
Abstract
Children with severe emotional or behavioral problems often present great challenges to parents, schools, and society because their emotional and behavioral reactions are unpredictable and extreme. When a child’s reactions are highly disproportionate to the circumstances, are frequent, and occur over a long time, they may be identified as having emotional disturbance (ED). The long-term risks associated with childhood ED include school drop-out, unemployment, and prison. These potential problems are frightening and stressful for parents to prevent or deal with the fallouts. Nevertheless, little is known about parents’ experiences raising a child with ED or how their child’s condition impacts them. This study used naturalistic inquiry to explore mothers’ experiences raising a child with ED. After institutional review board approval, eight mothers with 10 children with ED were recruited nationally through social media. Semi-structured interviews were analyzed for common themes. Mothers live in a state of high alert, trying to survive the stress and stigma created by their child’s ED. Mothers journeyed through escalating concerns to eventual confirmation that their child was not just difficult but had an ED. Mothers were overwhelmed by stress, cycles of escalating tension, hypervigilance, and isolation. Spouses often felt powerless to assist with the care of their child. Sibling bonds were strained or broken due to the unpredictable nature of ED. Finally, mothers shared ideas to help other families. This study provides details about families’ unmet needs and self-care deficits. Findings suggest needed changes in healthcare practice to better support families of children with ED.
Introduction
Children with severe emotional or behavioral problems are generally recognized to present great challenges to parents, schools, and society because of their intensely unpredictable emotional and behavioral reactions. In the literature, these types of significant emotional or behavioral problems may be identified by different names, such as emotional disturbance (ED), serious ED, or emotional or behavioral disorder (Williams et al., 2018). Regardless of the term, these children may have severe, unpredictable reactions which are dramatically out of proportion to the current circumstances. These reactions often create significant learning barriers for themselves and also their peers in school (Zionts et al., 2016).
The United States Department of Education (USDoEd) identifies children from age 3 to 21 years old as having “emotional disturbance” based on a list of criteria of observable, functional, and sustained learning problems in the school environment. The five criteria are (1) an unexplained inability to learn, (2) an unexplained inability to build peer or teacher relationships, (3) inappropriate behaviors or feelings under normal circumstances, (4) persistent, unexplained unhappiness, or (5) development of health symptoms or fears from school issues (U.S. Department of Education, 2020). Children may display one or more criteria, but the behaviors must persist for at least three months and be so severe that either the child’s learning or classmates’ learning is significantly impacted (U.S. Department of Education, 2020). Children with uncontrolled ED may wreak havoc in the classroom, disrupting not only their own learning but other children’s education as well (McKenna et al., 2019). Long term, children with ED have a high risk for dropping out of school, failed relationships, substance abuse, unemployment, and even prison (Lipscomb et al., 2017).
Given the seriousness of ED, it is not surprising that many researchers have devoted attention to this problem. In just one database, PsycINFO, a literature search using the terms “child or youth” and “emotional disturbance or emotional and behavioral disorders” found 74,000 articles published in the last 10 years. Despite this extensive body of research focused on children, literature focused on the child’s parents or families is scarce. Although some studies examined how parents themselves may cause or worsen a child’s emotional problems (Powers et al., 2022), few articles have explored the experiences of parents or families living with children with ED or how childhood ED affects family functioning.
The long-term problems associated with ED are clearly frightening. Multiple quantitative studies have reported parents of children with ED are highly stressed (Duppong Hurley et al., 2017; Green et al., 2020; Shenaar-Golan et al., 2021). Beyond being stressed, we know very little about parents’ experiences raising a child with ED or how their child’s condition impacts parents personally. Are parents stressed because of a lack of mental healthcare access? Do they feel ostracized by others? Are they or other family members in danger from their own child? We cannot build effective parental support programs without these contextual data about parents and what is happening in the home. Furthermore, this type of information cannot be accurately derived from quantitative data but is best studied with an exploratory qualitative research approach (Erlandson et al., 1993). Qualitative research can provide nuanced and detailed information to complement prior quantitative research and fill the current knowledge gap about parents’ experiences. Although parents are raising the children with ED, managing their treatments, and assisting with their schoolwork, there is a significant research gap focused on the impact of childhood ED upon parents or the family as a whole. This information could assist professionals to provide the supports that parents themselves identify that they need.
Background
Several quantitative studies have reported parents of children with ED are very stressed. Questionnaires have measured the level of parents’ emotional distress (Insa et al., 2021), if either externalizing behaviors or internalizing behaviors worsened parents’ stress levels (Shenaar-Golan et al., 2021), or if high parental stress could predict usage of a school-mediated support program (Duppong Hurley et al., 2017). Surveys of parents of children with ED found parents face employment problems, relationship tensions, or unempathetic healthcare or educational professionals, all of which led to higher stress levels (Green et al., 2020). Regarding different types of caregivers, such as parents versus grandparents, parents of children with ED report more stress than non-parental caregivers (Labella et al., 2020; Taylor-Richardson et al., 2006).
To gain a deeper understanding of parents’ stressful challenges, nuanced details and context surrounding parents’ experiences need to be studied. A few qualitative studies have explored the experiences of parents of children with general disabilities or mental illnesses, but not specifically those with ED. Leitch et al. (2019) conducted group interviews of parents with children who had either physical or mental disabilities. Parents reported feeling negatively judged and stigmatized, reporting there was “political backlash” when they advocated for their child’s needs, and that they were told to “belt it out” or if they “learned to control my kids, there wouldn’t be a problem” (Leitch et al., 2019, p. 6). Wiener et al. (2016) found mothers of children with ADHD often committed their whole lives to their child. Caregivers of individuals with various serious mental illnesses reported battling fear on multiple levels. Caregivers were terrified that their family member might commit self-harm, that the caregiver themself might be attacked, or constantly feared the unknown future (Johansson et al., 2010; Kalhovde & Kitzmüller, 2024). This prior research indicates parents are lacking in support or face outright hostility. These studies revealed more specific details about parents’ experiences, but they included children with physical disabilities or a mixture of different mental health issues. Children with ED are different than those with observable or more common conditions, so their parents may be impacted differently.
A literature search restricted to parents of children with ED found two recent qualitative studies. Both researchers used classic grounded theory. McKenna et al. (2024) explored how parents perceive their school’s special education services, while Tahhan et al. (2010) explored how extended residential treatments impact family dynamics. Parents who perceived their school was unwilling or unable to provide special education services reported high levels of stress and an overall distrust of educators (McKenna et al., 2024). Tahhan et al. interviewed mothers whose child required an extended residential stay. Mothers were physically, emotionally, and socially isolated. Some mothers were fearful their child may become violent with their siblings or the mother herself (Tahhan et al., 2010). Another important finding was parents reported their children’s behaviors at home were significantly worse than what others saw in public or school (Tahhan et al., 2010). This is a key finding for healthcare and educators to note: as difficult as the child’s behaviors might be in public, the situations may actually be worse at home. Neither study was directly focused on the home environment or how their child’s ED impacted their parents, but both studies suggest that the impact of childhood ED on families could be serious.
The literature gap surrounding ED in the home environment and prior reports of parents’ personal challenges suggest an exploratory investigation is warranted. Parents may experience self- or family-care deficits, aligning with Orem’s Self-Care Deficit Theory and the supporting theories of family and dependent care deficits (Taylor, 1989). Dorthea Orem postulated that nurses should anticipate and assist patients to overcome self-care barriers, which Taylor extended to include family and dependent’s needs. Taylor (1989) advises viewing the family as a unit, with specific needs in order to properly function as a unit. Parents frequently turn to healthcare providers for advice about their child’s emotional or behavioral problems. Unfortunately, parents and caregivers of mentally ill children report that the advice given is often unhelpful (Council for Exceptional Children, 2020; Kalhovde & Kitzmüller, 2024). Offering broad advice to reduce stress does not consider the root causes of parents’ stress or the other barriers they face. Without a clear picture of how parents living with the child are impacted by their child’s ED, it is difficult for professionals to give effective advice, support, or assist parents with overcoming self-care barriers.
It is vital we understand the nuances and context of parents’ personal challenges. By using a qualitative approach, prior quantitative results can be expanded to better understand the breadth of issues parents cope with, meet parents’ need for advice, and possibly reduce parents’ stress. The purpose of this qualitative study was to explore the challenges faced by parents raising a child with ED and gain a greater understanding of the impact of childhood ED upon their families at home.
Method
The lack of contextual information about parents’ experiences with childhood ED indicated the need for an exploratory qualitative approach. Various qualitative approaches have unique strengths. Lincoln and Guba’s (1985) naturalistic inquiry (NI) was selected because NI focuses on the context and perspectives of several people with firsthand experience to construct a composite of the group’s reality. NI is heavily dependent on the context of participants’ experiences and prioritizes maximum depth of data over uncovering broad generalizations or theory (Carl & Ravitch, 2018; Lincoln & Guba, 1985). Gathering context from people with firsthand experience of an issue allows researchers to “see what is happening” within the phenomenon (Erlandson et al., 1993, p. 9). “Seeing what is happening” with parents at home will assist professionals to better understand and address the self-care deficits of parents and families living with children with ED.
Historically, parents of children with mental disabilities have faced marginalization due to pervasive social stigmatization of mental illness, which extends from the child with the condition to also include their parents (Hernandez et al., 2017; Hinshaw, 2005). Parents struggle to decide if disclosing their child’s condition will bring greater assistance or stronger barriers (Eaton et al., 2017). Given the uniqueness of parents’ situations when raising a child with ED, using a NI framework can assist to accurately share the context of parents’ realities as well as give voice to a marginalized group (Curry et al., 2009).
The data presented here are part of a wider study exploring parents’ experiences raising a child with ED, the impact childhood ED has upon the family, and how parents manage day-to-day challenges related to their child’s ED. This article focuses on empirical data highlighting parents’ experiences before their child’s ED diagnosis and the impact of childhood ED on parents and siblings. At the time of the interview, all children had a formal diagnosis of ED. It is beyond the scope of this article to provide the entirety of the findings of this wider study. Further publications will address the methods used to manage their child’s emotional and behavioral outbursts, how the parent–child bond evolved over time, and techniques used to address the needs of parents’ other children. However, this article draws attention to specific sources of parental stress and provides guidance to effectively reduce self-care challenges for parents and families. In addition, the findings suggest pathways for improved collaboration between the nurses, healthcare providers, and educators who work with families of children with ED.
Study Design
The specific aim of this study was to explore parents’ child-rearing experiences as related to their child’s ED. The following questions guided the study: (1) What are the parenting experiences of parents of children with ED? (2) How does raising a child(ren) with ED impact the family as a whole?
The responses to these questions will give healthcare professionals insight about parents’ experiences at home, their challenges, and how childhood ED impacts the entire family. The resulting qualitative data also allow marginalized parents to be heard, and their voices included within the body of knowledge of ED.
The study design was guided by Lincoln and Guba’s (1985) theoretical view of NI, as described by Erlandson et al. (1993). Institutional review board approval was obtained prior to study initiation (University of Texas Medical Branch IRB, # 23-0049). Recruitment flyers were shared using national social media. Participation criteria were developed to ensure participants had recent, in-depth experiences to share. Participation was limited to parents (biological, adoptive, or stepparents) of children who had been diagnosed with ED or who had significant behavioral issues for at least 6 months. The children must be younger than 24 years old. Thirteen potential participants initially responded to the recruitment efforts. One respondent did not meet eligibility criteria, and an additional four respondents did not respond to follow-up calls or emails. The final sample was eight participants, all mothers, who were raising 10 children diagnosed with ED.
A naturalistic research study strives to construct a composite of multiple realities from the participants and retains a fluidity within the study processes (Lincoln & Guba, 1985). This fluidity encourages participants to share the experiences which participants feel are most important instead of requiring specific responses to pre-determined questions or scale items from the researcher. A semi-structured interview guide with four questions was created to guide the interviews, initiate topics, and prompt participants to remember situations they may have encountered. (1) When did you start noticing things that caused you to think your child might have an emotional or behavioral problem? (2) What were some everyday challenges that your child’s emotional or behavioral issues created for you and your family? (3) How have your child’s issues impacted you? (i.e., emotionally, work life, financially?) (4) How have your child’s issues affected other family members, such as your spouse or other children?
The questions were purposefully broad to allow each participant to focus on areas which were most important in the participant’s personal view.
Informed Consent
The protection of participants’ rights and ethics surrounding qualitative research is of paramount importance. Due to the study’s sensitive nature and to further protect participants’ confidentiality, participants did not sign a consent form but gave verbal consent. Since interviews were conducted remotely via Zoom or telephone, using a verbal consent process reduced the risk of a confidentiality breach than could occur with written signatures on an electronic consent form. It was hoped this verbal consent process would also reduce participants’ concerns regarding talking about their child’s mental health condition. Prior to the interview, each participant was sent study details as well as an informed verbal consent script. The script was read aloud before the interview began, and emphasized participants could decline any question for any reason or could end the interview entirely at any time. As part of the consent script, the author informed participants that she is a registered nurse and therefore mandated to report any child abuse or neglect in her state. If any information caused the author concern that a child was being abused or neglected, she would be required to stop the interview and report her concerns. After the consent script was read, all participants agreed to continue with the study and confirmed their verbal consent at the start of the recording. There were no indications of any parental child abuse or neglect during any participant’s interview.
Data Collection, Analysis, and Rigor
Individual, one-on-one interviews were conducted via recorded sessions over Zoom using end-to-end encryption or by telephone with a handheld digital recorder. Zoom recordings were downloaded to an encrypted flash drive and then deleted from the Zoom database. The interview began with collecting basic demographic data, including participant’s age, their child’s age, other siblings, ethnicity, and marital status. The interview portion began with an opening grand tour statement: “As you know, I am interested in learning about the lives of parents of children with emotional or behavioral difficulties. I would like to hear your story.” Participants could start and move through their story at their own pace. Additional data were collected by field notes which documented participant’s non-verbal reactions or impressions after each interview. The researcher kept a reflexive journal to monitor any potential researcher bias. Nurses are consistently viewed as “trustworthy” by the general public (Advisory Board, 2025), so the researcher’s status as a nurse may have increased participants’ comfort during the interviews. The researcher was careful to avoid a caregiving or advising role during the interviews, as her registered nurse status could create this type of bias during data collection.
Interview recordings were transcribed by Otter.ai, an artificial intelligence transcription service (https://otter.ai/). The researcher verified the accuracy of each transcription by listening to the recording and correcting any transcription errors. All potentially identifying information about participants and their family members was masked and de-identified. Only masked data were used for data analysis and stored in the researcher’s office. The original, unmasked transcripts, recordings, and participant contact data were stored on an encrypted flash drive, securely locked in a fire-safe storage box, and stored in a separate location from the researcher’s office. All transcripts were permanently deleted from the Otter.ai database. Interview recordings will be permanently destroyed at the conclusion of all written reports and manuscripts.
Data analysis was conducted using the constant comparative method. Although Glaser and Strauss developed the constant comparative method to derive social theory, Lincoln and Guba (1985) used constant comparative method to process data rather than generating theory (p. 339). In this way, NI’s data analysis can illuminate specific details, which gives a phenomenon’s context its “unique flavor” (Erlandson et al., 1993, p. 148). Microsoft Excel was used to store, sort, and re-sort data units into columns of groupings, and eventually into themes. The data were further analyzed by bridging and extending the data units into three overarching themes, each with supporting subcategories. Data collection and sampling is stopped when the data are saturated or “redundant,” which Lincoln and Guba define as when “subsequent interviews reveal scant or insignificant new information” (p. 234). Saturation was suspected after seven interviews and confirmed after eight interviews; therefore, further recruitment and interviews were halted.
Lincoln and Guba (1985) strongly emphasize the importance of rigor and trustworthiness in qualitative research, because trustworthiness determines if “the results are worth paying attention to” (p. 290). Trustworthiness is shown with evidence of data credibility, transferability, dependability, and confirmability. Several study processes were used to demonstrate rigor. All eight mothers recounted how every family member was altered by their child’s ED. Seven of eight mothers struggled to get their concerns about their child properly evaluated. This data triangulation provided strong credibility for the findings. Lincoln and Guba (1985) state that the purpose of naturalistic sampling “is to maximize information but not facilitate generalization” (p. 202). Because NI emphasizes context and constructed realities of a sample, broad transferability is not possible in a strict sense (Lincoln & Guba, 1985). However, transferability is enhanced with the creation of a rich, descriptive “data base,” including illustrative quotes, which allow readers to evaluate potential transferability to other settings and contexts. The researcher tracked participants’ specific experiences with a findings codebook, organized by constructs and themes. The codebook provided evidence of the findings’ dependability and confirmability. In addition, the researcher kept a reflexive journal and audit log to further enhance data credibility and dependability.
Results
Sample Profile
Sociodemographic Data: Mother Participants (n = 8)

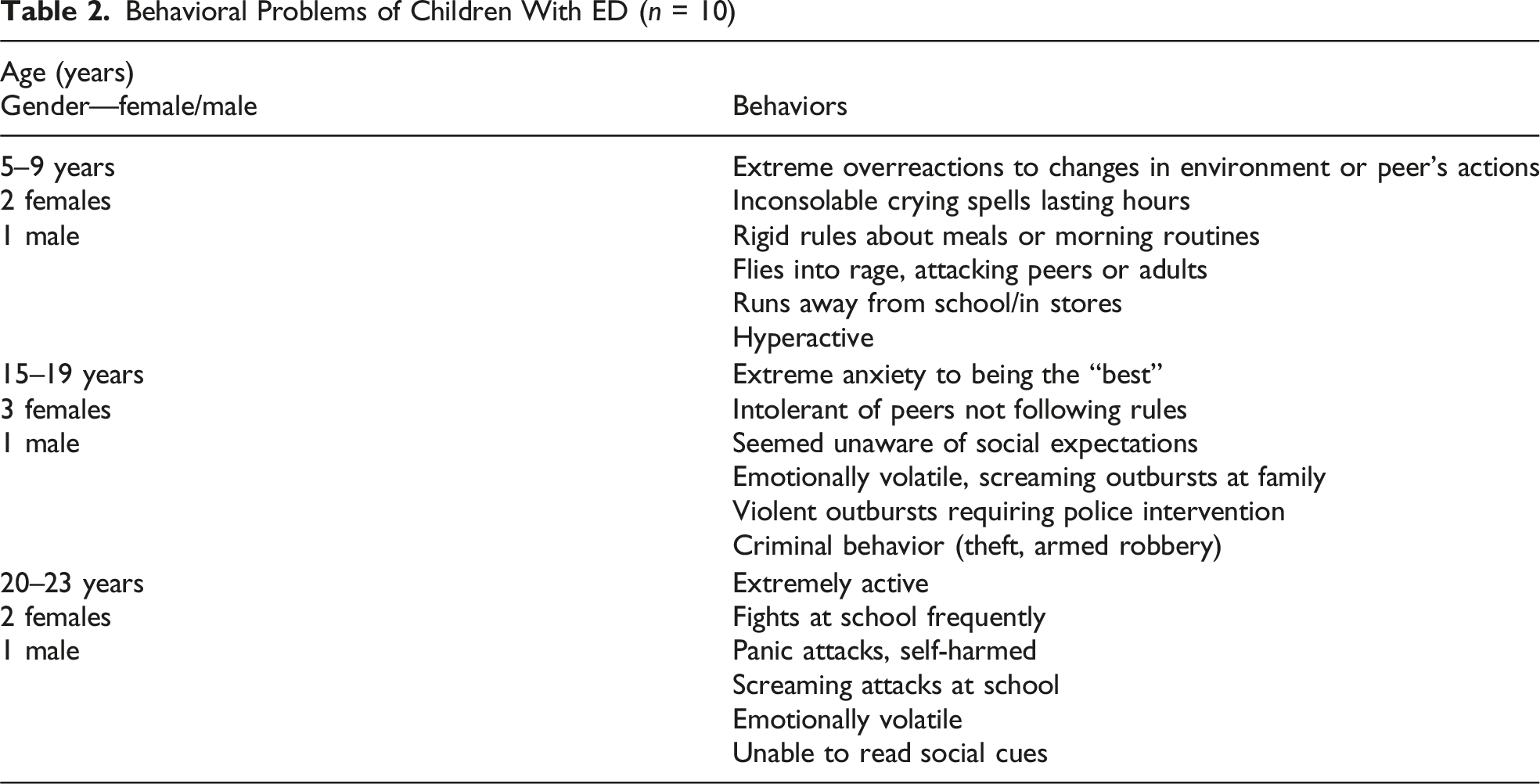
Behavioral Problems of Children With ED (n = 10)
Thematic Findings
Summary of Themes: How Childhood ED Impacted Parents
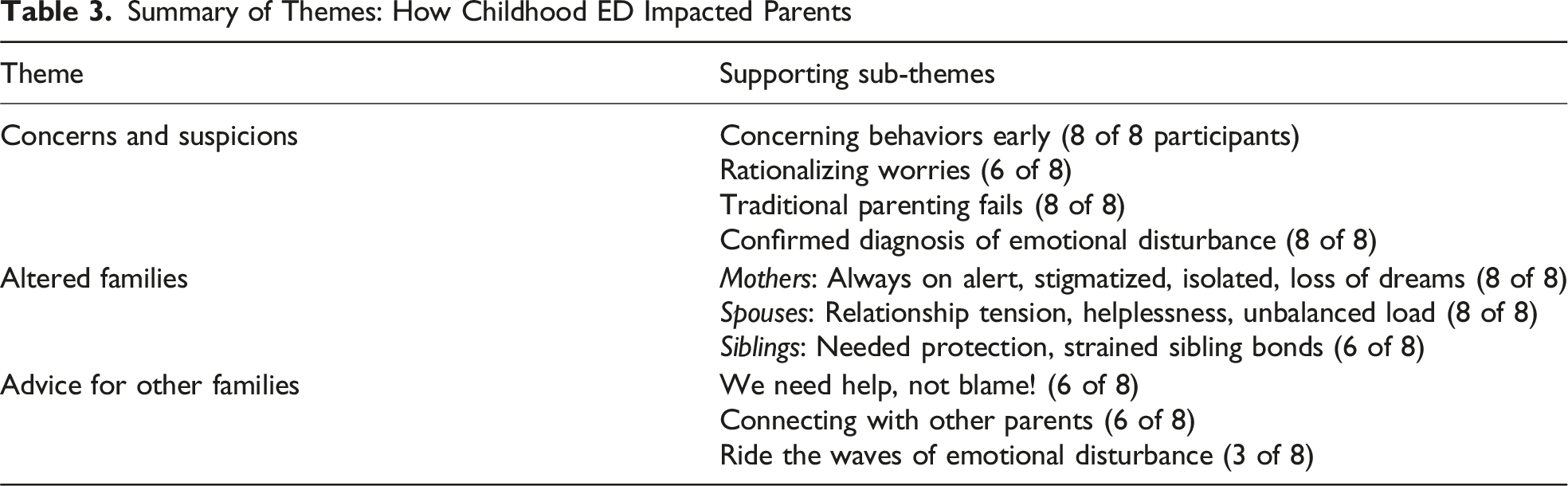
Concerns and Suspicions
A pattern emerged as mothers learned that their child had ED. All eight mothers saw early on—even in infancy—that their child reacted in ways that other children simply did not. Their children had explosive, violent outbursts to minor situations, were extremely intolerant of people not following rules, or displayed huge emotional reactions. One boy sobbed uncontrollably in a sad movie—at age 17. Another child (9) violently attacked a peer when he did not follow the rules of her make-believe recess game. This mother could “almost see the wires crossing” on her daughter’s face: “Her anger is…just hitting someone once isn’t enough. It’s like she hasn’t gotten her anger all the way out, so she has to keep going.” Mothers were shocked and dismayed at the sheer intensity of this child’s reactions.
The children were unable to empathize with others or consider a different perspective. The volatility and lack of perspective meant anyone could be blasted without warning. One mother’s child “controlled our house with her emotional outbursts,” while another mother said her child had no “concept of time, or others’ time, or even that anyone else was around!” Mothers struggled to understand their child’s outbursts when the irritating incident seemed so small or when their other children did not react to similar situations in the same way.
At first, most mothers (6/8) did not believe their child had a serious issue but rationalized their concerns instead. Mothers thought the problem was situation, such as changes in school routines, related to adoption, or being overly tired. As the primary caregiver, mothers observed more outbursts than their spouses. When spouses did not experience the frequency or intensity of the child’s reactions, some felt the mother might be exaggerating. Mothers then doubted themselves: “I started noticing things, but I was the only one noticing things.” When spouses did not both see a possible problem within their child, tension grew between spouses, causing mothers to doubt themselves and their own judgment. Liggins-Chambers (2023) noted that when family members do not believe or downplay a child’s disability, mothers feel “foolish,” “stupid,” and invalidated.
Nearly all mothers (7/8) initially wondered if their parenting style was the root problem. Mothers tried stricter rules with consistent consequences. Several mothers described this as the “old school” parenting which they grew up with, saying, “This is the rule … if you don’t follow the rule, this is your consequence.” However, all mothers reported that an authoritarian approach or consequences such as time outs, grounding, yelling/anger, or spanking were completely ineffective at improving their child’s behavior. Attempts to persuade the child to “make better choices” usually caused the child’s emotions to escalate rather than calm down. Although most mothers initially tried traditional, authoritarian parenting or verbal persuasion, these approaches were never successful for any of the children with ED, even when the styles worked well for their children without ED. The failure of traditional parenting methods worsened mothers’ feelings of stress and self-doubt.
The behavioral problems escalated when the child started school. The classroom also highlighted the dramatic differences between the reactions of the child with ED and other children. Schools reported their child was having major temper tantrums, extreme inflexibility, or an extraordinary need for control. The children flew into a rage from “0 to 60,” requiring teachers to separate the children or even call the police to lock down the classroom. As the behaviors worsened, mothers’ concerns grew. Despite mothers’ initial rationalizations and self-doubt, their concerns grew into deep suspicions that something was different about this child, even if the mother was not sure what it was.
Official confirmation of the child’s ED from a healthcare provider or child expert was lengthy and difficult. Challenges included long appointment waits, travel distance, high cost for mental health professionals, time away from work, other family health issues, or when the spouse did not believe the behaviors were truly abnormal. Pediatricians or other experts often continued rationalizing the child’s behaviors. Mothers were told that “it was just a phase,” “boys are delayed,” or were questioned about inconsistent home routines or disciplinary methods. One child would randomly scream or even bark at strangers, so her mother brought it up with her pediatrician several times. The pediatrician responded, “Well, she’s only two,” then, “Well, she’s only three.” She exclaimed, “Well, now she’s five and it’s worse, not improving!”
Responses like this caused mothers to vacillate between deep suspicion that their child had a problem and self-doubt in their parenting judgment. These mothers’ experiences support prior findings that despite seeking professional help early and often, interactions with pediatricians and child development experts are unhelpful or difficult (Council for Exceptional Children, 2020; Kalhovde & Kitzmüller, 2024). Eventually, all 10 children were diagnosed with ED, confirming their mothers’ suspicions. Receiving an official diagnosis was extremely important and cathartic to the mothers, concurring with Liggins-Chambers’s findings (2023). When their concerns and suspicions were confirmed by a diagnosis, mothers moved forward with researching the condition and treatment options.
Altered Families
Although the mothers handled the majority of daily childcare, every family member was significantly impacted by the child’s ED. In addition, the family dynamics and functioning were greatly affected by the child’s behaviors and by the actions needed to manage those behaviors.
All eight mothers voiced experiencing overwhelming stress, caused by cycles of tension and explosions, fear of violence, and social stigma. Their child with ED tried to adhere to social conventions when they were in school and public, but let “loose” when they reached their limit, usually just as they reached home. The pervasiveness of cyclical tension and explosions meant mothers were constantly “on alert” for the next crisis. Mothers panicked when they got an unexpected phone call, wondering if they needed to drop everything to go get their child. Because if things go wrong…I’m back on-call 24/7, just to make sure I keep her safe. For 23 years, I’ve been kinda waiting for the next crisis. Whenever I see the elementary school caller ID, I’m aways kind of deflated or panicked because I’m wondering, did she run away? Did she hit somebody? Do we need to go pick her up?
Even after a child had a stable period, her mother said, “If anything happened, I was right back there in my head.” Mothers were either managing a crisis, trying to prevent a crisis, or worried a crisis had occurred in their absence.
Some children with ED were violent toward siblings, peers, or the mother herself. Children flew into a rage over minor problems, making mothers so frightened for caretakers’ safety that they could not ask others to babysit their child. At this point, who can we leave her with? Who isn’t’ going to have to call us in a panic and tell us to come home? Who are we going to leave her with that she won’t … run away from?
Mothers could not get respite safely because they were worried what might happen if they were not present at all times. One mother tearfully admitted that she was petrified her child might kill someone in a rage. She feared her life will always revolve around keeping her child safe as well as keeping the world safe from her child, and she knew preventing violence could be impossible.
Nearly all mothers (7/8) struggled with stigma and isolation. Stigma could be blatant or subtle. One mother was shunned, watching other parent chaperones talking in a group during a field trip but excluding her. She saw her child’s desk was pushed into the corner of the classroom, and now she was pushed away from the other parents. Friends and family could be overtly judgmental. Family members told one adoptive mother to “do a better job!” or she should “just send her [child] back.” One mother was deeply hurt after revealing her daughter’s condition to a close friend, and years later, cried retelling the story. I thought [paused] this lady was my friend. She asked what was going on [with my child.] And so I would tell her because she was acting out. She looked me at me and said, “wow, well she looks really normal!” [mother crying] And I just thought, maybe if she had a deformity, it would make it ok? And you’d be sympathetic? …and I realized at that point, I’m alone.
Many mothers wondered if they would have been treated kindlier if their child had a physical disability, instead of a mental condition. These mothers’ experiences demonstrated the continued pervasiveness of mental health stigma, including the parents of children with mental health issues, as reported by Hinshaw (2005).
Some wounds were hidden, with seven mothers reporting deep grief and sadness. A child’s ED created problems during typical milestone achievements, such as fifth grade graduation or field trips. The loss of these anticipated memories were a great hidden loss because the milestones are so commonplace and expected for other children. The emotional wounds caused a death of motherhood dreams for several mothers, making mothers “grieve the loss of the vision, what you thought [being a mom] was going to be.” The mother–child bond was one-sided. Mothers of older children desired a two-way, adult connection between their child and themselves, but their child could not relate back to their mother in that way. One mother sadly admitted it was “a death of the expectation that you have, for who your kid is going to be.” Their mother–child bond lacked reciprocation and deeper meaning for their child, causing yet another loss in these mothers’ dreams of parenthood.
Mothers may have been the primary caregivers, but their spouses were also deeply affected by the child’s ED. Relationship tension was common, especially if the partner had not observed the outbursts as often, or believed the child was just “melodramatic,” or refused to adapt themselves to account for their child’s ED. A mother said her spouse “expects her to sit and be quiet, like the other kids.” As behaviors worsened, all the fathers eventually realized that this child’s outbursts were not “normal” and accepted their child had ED. Many mothers adapted themselves to better cope with their child’s reactions, but fathers were slower to adapt. Mothers reported that most fathers (6/7) struggled to handle the child’s explosiveness when the mother was not present. So, he tries…sometimes it’s great and it works. Other times, I get the call, “You’ve got to come home” or “I don’t know what to do, how do I make it better?”
This spouse wanted to give his wife a break to care for herself, but did not know how to handle his daughter and would text his wife to come back. Mothers knew their spouses felt helpless watching their wives’ mounting stress but also seemed unsure how to manage their own child. When spouses were unable to handle their own children alone, the caregiving burden for the mother became increasingly unbalanced, even at home. The child’s ED altered both parents individually and their relationship.
The imbalance of knowledge between spouses created a pattern of increasing burden and responsibility on mothers’ shoulders. Relationship tensions eased when spouses accepted that their child’s mental health problems were “real” and not just circumstantial, defiance, or “drama.” Despite the stress, most marriages remained strong. For the seven mothers originally married, six remained married to their partner. These six mothers considered their spouse their greatest supporter, it was “us against the world,” and relied heavily upon their spouse’s support. One mother and her spouse made a verbal agreement to always back each other’s decisions, agreeing that “whatever decision you make, is the best decision you can make [at that time].” This couple managed tension by deliberately dividing spheres of responsibility, from which parent will help with which school subject to which parent would attend what sporting event. The deliberate divisions and conversations allowed both spouses to be involved, yet also to let go of the things not in their assigned sphere.
Other children living at home were also deeply affected by their sibling’s ED. One family moved homes so the child with ED could attend a supportive school, which meant their siblings had to change schools also, with the subsequent loss of friendships and school groups. Some children needed physical protection from their sibling’s violence or theft, or had to live with relatives until things cooled down at home. They were in the same school. When she would misbehave, the cops would be called, and it was embarrassing because everyone knows that his sister’s having a breakdown. It was pretty mortifying for him.
Mothers knew their siblings were humiliated and embarrassed by the child’s explosive outbursts, especially when they occurred in front of the siblings’ peers. Another child with ED became so incensed when her brother wasn’t wearing a bike helmet that she attacked him. She did not care or differentiate that the younger brother was not actually riding a bike. Her mother had to physically protect her younger child, making the mother both angry about the situation and fearful for her younger child’s safety. Mothers were torn between the high needs of the child with ED, and siblings’ need for protection from physical and social harm, being caused by the mother’s own child.
Sibling bonds were difficult, because more even-tempered siblings could not understand the child’s unpredictable reactions. One mother revealed her other children spent “a lot of time placating to ‘P’ (the child with ED), because it was easier than arguing.” It was more peaceful to defer any decision to the child with ED than it was to voice an opinion. Voicing an opposing opinion meant the whole family could have a bad day. There were years and years where none of us slept through the night, because if “P” wasn’t sleeping, no one was sleeping.
When siblings feel they should give in to the whims of one child to keep the peace, resentment builds. Some sibling bonds were irreversibly broken due to violence or a vast incompatibility between their emotional make up. One child decided to cut ties from his two siblings with ED. He says to us [parents] that he doesn’t have a sister or a brother. They’ve been nothing but stress and trouble.
Mothers lamented the impact of one child’s ED on her other children, knowing she could not prevent the damage but understanding the needs and limits of both. However, vast emotional differences did not always break sibling bonds. A few siblings protected the child with ED by shielding their sibling from peer stigma or trying to smooth out their sibling’s emotional chaos. Overall, each individual family member and the relationships between family members were drastically altered due to the ED child’s behaviors or the treatments needed to support them.
Advice for Other Families
Qualitative research can give voice to hidden or marginalized groups or populations (Curry et al., 2009). During recruitment, many potential participants said they wanted to tell their stories because they hoped other families could learn from their experiences and lessen others’ burden. To capture this opportunity directly, the final interview question was, “If you could tell the world anything, what would you want others to know?” Mothers responded that (1) parents need more help, not more blame, and (2) shared “survival tips” for families.
Mothers struggled to raise their child without strong professional guidance but were often blamed for their child’s poor behavior in public. Reflecting on their journey, all mothers believed they did everything they could have done for their children. One mother, whose child committed violence and theft, shouted, “Stop blaming the parents! Stop blaming us because we tried!” Another shared how frustrating it was to be blamed when she was just lost without guidance. If I could just scream it to the world, it’s not the parenting. It doesn’t mean someone’s a bad parent just because their kid might be “bad.” The kids need help, not expulsion…there’s no one telling us what the right path is.
These sentiments correspond to prior reports of parents of children with ADHD who reported that they needed more than “coffee and Valium” (Leitch et al., 2019, p. 6). Mothers wished both professionals and society at large understood how hard they were working to raise their children well. Some segments of society still treated mothers as if their child’s problems were not “real.” They say, “It’s just in your mind!” and I say, exactly! In their mind, that’s a part of their body. The problem is in there! [pointing at her head].
Mothers want society to accept that their child’s problem was real participants wanted, and that problems which start in a person’s mind are just as legitimate as visible problems in the body. Parents of children with ED needed more help but often got more blame.
Mothers also shared survival tips for other parents. Mothers strongly encouraged other families to find similar families and “keep trying to find others you can talk to,” because finding connections eased these mothers’ feelings of loneliness and inadequacy. Learning about other parents’ experiences opened these mothers’ minds to potential ideas to try. Just have that openness to be like, I’m just gonna listen...or maybe, I don’t think that will work, but I could do this, tweak it, and then it might work.
Parents might hear an idea that may not work in its current form but might be changed for their child. Opening up to other people is emotionally risky, but mothers encouraged other parents to keep trying. Mothers acknowledged, “It seems scary, but the more you know, the more you can help [your child].” Mothers wanted parents with strong school partnerships to realize that teachers can provide astute observations in a different environment than parents themselves experience.
Lastly, several mothers suggested that other parents try viewing childhood ED situations as fluid waves that are constantly shifting, so parents can focus less on the current chaos and more on the path to the other side of the wave. One mother called it “riding the wave,” which became her personal mantra. The “wave” embodied her perspective toward the ever-changing situations she faced, with all of a wave’s unpredictability. She encouraged other parents to try it for themselves. We don’t know how long the wave is. We don’t know how short the wave is. Just…ride the wave.
Discussion
The unpredictable actions of these children with ED created a state of stress, stigma, and emotional chaos for their parents and families at home. This study’s findings extend the knowledge from prior quantitative studies of parental stress (Duppong Hurley et al., 2017; Insa et al., 2021; Kalhovde & Kitzmüller, 2024; Shenaar-Golan et al., 2021) by providing context and personal perspective from the stories of these mothers’ parenting journey. Mothers revealed that although their children with ED tried to adhere to social expectations for as long as possible, their children “let loose” when they could no longer hold it together, usually at home. For a few mothers, this “letting loose” could include a potential for violence from their child. These data support prior studies (Kalhovde & Kitzmüller, 2024; Tahhan et al., 2010) that despite the difficulties their child’s behaviors might cause in public, the behaviors may be worse at home. Several mothers felt both they and their child were socially stigmatized due to their child’s ED, confirming the ongoing challenge of mental health stigma. In this study, mothers bore the majority of the negative emotional impact of childhood ED, but no family member or relationship was unscathed by the experience. The information gained by this study should guide improvements on professional advice and support for parents raising children with ED.
Using Orem’s Self-Care Deficit Theory and Taylor’s family-care deficit theory as a framework, the findings demonstrate that mothers and families have immense self-care needs that are currently unaddressed by healthcare professionals. Mothers endured immense stress and exhaustion, leaving them isolated, doubting themselves, and desperately searching for help. Some parents and siblings have safety needs due to the potential for violence from their own child with ED.
The findings provide ideas to address parent and family self-care deficits. Several mothers emphasized that connecting with other people was vitally important for them and should be a major priority for other parents. Connecting to families with similar struggles helped the mothers know they were not alone in the world with this problem. Nurses, healthcare providers, and educators can assist families by emphasizing the importance of connecting with others and suggesting options for connecting. As previously reported (Kalhovde & Kitzmüller, 2024; Liggins-Chambers, 2023), mothers here revealed that obtaining an official diagnosis brought them a sense of peace, and they were desperate for positive affirmation of their parenting efforts. Healthcare providers must understand the power of affirmation for parents. Professionals working with families such as these should strive to purposefully praise parents for their efforts, even as parents search for the right methods, right environment, or best responses to their child’s ED. Providing affirmation of parents’ efforts and guidance to connecting with other families are two immediate study implications which healthcare and educational professionals could incorporate into practice immediately.
Another study implication includes assessing family functioning as a whole, rather than focusing solely on behavior modifications for the child with ED. Taylor (1989) advises that nurses look beyond the primary patient and consider the needs of the patient, caregiver, and entire family. Here, every member was deeply affected by the child’s ED, and the child with the condition is only part of the challenge which parents face. Due to a variety of factors, most mothers perceived they faced an unbalanced load of responsibility between themselves and their spouse. One couple made a deliberate choice to delineate the responsibility for specific jobs between each parent, which allowed each parent to focus on their assigned jobs and ensured all three children received nurturing and support. Nurses and healthcare providers could suggest other families that arranging responsibilities in a deliberate manner could strengthen partnership bonds, help provide for all their children’s needs, and help mitigate the extreme exhaustion when one partner is overloaded.
The study also suggests that nurses and healthcare providers examine their assessment practices of parents reporting behavioral issues with their children. All of the participants wished they had discovered their child’s problem earlier, so they could have been more proactive instead of reactive. Seven mothers consulted with multiple professionals over several years before getting a proper evaluation and diagnosis for their child. The participants’ healthcare providers frequently deferred mothers’ concerns, saying “it’s just a phase,” focused solely on a child’s immediate behaviors, or only advised strict traditional parenting techniques. Mothers wished providers would take a wider view for underlying causes. For example, one mother eventually related her child’s outbursts to an inflammatory response from gluten, leading the mother to find ways to reduce inflammation with diet changes, avoiding overheating, medications, and hydration. This finding supports research done by the Council for Exceptional Children (2020), who found that parents first turn to healthcare providers for help but come away feeling unheard.
Nursing assessment interviews often screen for intimate partner violence or parent to child abuse, but these mothers demonstrated that parents or family members may be in physical danger from their own child. This possibility is extremely concerning and correlates with prior studies that family members were worried their mentally ill loved one might harm a family member or the parent themselves (Kalhovde & Kitzmüller, 2024; Tahhan et al., 2010). Nurses and healthcare professionals should consider this possibility when working with families of children with serious behavioral issues. Unfortunately, mothers found there is still a stigma that mental health issues are not “real” but just a lack of will power or parental discipline. This stigma can be inadvertently reinforced when healthcare professionals repeatedly tell parents their child’s behavior is just a “phase.”
Limitations
Erlandson et al. (1993) caution researchers that NI research seeks to expand contextual understanding of a phenomenon but cannot fully describe a phenomenon’s complexity. Lincoln and Guba (1985) state that NI studies should strive to maximize information and impart thick description to enhance transferability of findings, but that broad generalizations are not the goal of an NI study. This is especially true when studying ED, which has a wide range of accompanying behavioral and emotional problems. This study conducted in-depth, individual interviews of a small sample size of eight mothers with 10 children with ED. Participant mothers were geographically widespread but fairly homogenous in terms of ethnicity and marital status. The level of context obtained here is not easily gathered with a large sample, but the findings should be viewed with caution until they are validated with a larger sample. Future research is also needed to explore fathers’ experiences as they are likely very different than mothers’ perspective.
Conclusion
Mothers shared vivid details about their parenting experiences raising a child with ED and the unique hardships they faced due to their child’s condition. ED manifests over a wide spectrum of behaviors, so there may be significant variability in families’ experiences. However, these findings correlate with previously reported typical ED behaviors and provide needed context surrounding parental stress related to raising a child with ED. Mothers here described living in a state of high alert, trying to survive the stress and stigma created by their child’s ED. Mothers struggled to obtain a diagnosis for their child’s condition, as well as dealing with constant chaos, social stigma, and isolation during their daily lives. The problems caused by the child’s ED were not limited to mothers, but each family member and the whole family unit were deeply affected.
Study findings revealed gaps in supports for parents of children with ED. Parents of children with ED are desperate for experts’ assistance, guidance, and affirmation of their efforts. The study should be used to guide further investigations into potential interventions, supports, and assessment guidelines by nurses and other pediatric experts. Nurses and healthcare providers must heed these parents’ cries for help. By improving the health and wellbeing of the whole family, we can also give the child with ED the best chance for a successful long-term outcome.
Footnotes
Acknowledgements
I would like to thank Dr. Virginia Tufano (Texas State University) for her exemplary critiques and editing assistance while preparing this manuscript. I am grateful to Dr. Patricia A. Blair (University of Texas Medical Branch) for her general support and guidance during the investigation. Lastly, I am deeply grateful to the study participants, who shared their deeply emotional experiences in an effort to ease the burdens of other families like their own.
Ethical Considerations
This study was approved by the University of Texas Medical Branch Institutional Review Board (IRB # 23-0049).
Consent to Participate
All participants were given written study information and provided verbal consent prior to study enrollment. Affirmation of verbal consent was re-confirmed and recorded at the beginning of each participant’s interview.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data which support these findings are available on reasonable request. Due to privacy considerations, data have been anonymized and will only be shared with appropriate safeguards.