
Abstract
The concept of saturation was originally developed within grounded theory. It has since been extended and widely adopted as a marker of rigor throughout qualitative health research. Although saturation can prove useful, there are growing concerns regarding its uncritical adoption as a universal standard of high-quality analysis. While this critique is not new, we ground our argument within the concept of epistemic injustice, to contend that the inappropriate use of saturation risks enacting epistemic injustice by marginalizing certain forms of data and certain methodologies. This, in turn, limits what can be known about health and illness, with the potential to cause material harm and produce and sustain health inequities. First, we introduce the concept of epistemic injustice, following which we provide an overview of saturation to describe the different models, discuss their contingent nature, and call attention to the underlying positivist logic embedded in saturation. Next, we analyze the exclusionary effects of saturation in qualitative health research through the lens of epistemic injustice. We conclude with recommendations for a more context-sensitive and reflexive engagement with saturation, and a shift away from procedural adherence to checklist-based standards that enforce its use in academic knowledge production.
Introduction
First introduced to qualitative research by sociologists Glaser and Strauss (1967), saturation has gained status as a marker of rigor for qualitative research writ large (Fusch & Ness, 2015; J. M. Morse, 2015; Saunders et al., 2018). Conceptualized as the point at which no new information may be gleaned from the data, saturation has been described as critical to qualitative health research (Buckley, 2022) and “the key to excellent qualitative work” (Morse, 1995, p. 147). Similar claims are made in other disciplines. For example, in management studies, failure to reach saturation has been pronounced potentially fatal (Bouncken et al., 2025), and saturation has been characterized as not only a guarantor of high-quality but of ethical research as well (Chitac, 2022). In tourism research, saturation has been described as essential (Andriotis, 2024), while others in philosophy have begun to advocate for its use to enhance the rigor of philosophical research (Hiah et al., 2025).
Although a potentially useful concept to determine when one’s data can support their analytic goals, we argue the uncritical adoption of saturation in qualitative health research has the potential to enact injustice and harm by limiting what we can know about health and illness. While there is an array of critiques regarding how saturation is conceptualized and used (Braun & Clarke, 2021; Jennings & Yeager, 2025; Saunders et al., 2018; Sim et al., 2018; Thorne, 2020; Tight, 2024; Varpio et al., 2017), and these are not new (Caelli et al., 2003; O’Reilly & Parker, 2013), we make a novel contribution by contextualizing our critique through the lens of epistemic injustice (Fricker, 2007). Specifically, we reference Dotson’s (2012, 2014) concept of epistemic oppression, and Fricker’s (2007) concepts of hermeneutical marginalization and hermeneutical injustice, to theorize how the uncritical use of saturation can create knowledge gaps with the potential to harm peoples’ health and produce and sustain health inequities.
We have several goals in writing this critique. We add our voice to the growing number of qualitative health researchers who advocate for a more intentional and circumspect use of saturation. Not unlike O’Reilly and Parker (2013), we were motivated by our experiences navigating proposal evaluations and peer review, where our methodological designs and analyses have been questioned because saturation was either not referenced or employed. In this spirit, we hope to provide a theoretically oriented yet approachable critique that researchers, especially those new to the field, can reference to help articulate the potential epistemic and ethical implications of using saturation and to help justify why it might be incongruent with their study.
Another concern—prompted by reviewer comments—is that as artificial intelligence proliferates, there may be renewed interest in using saturation to determine and establish the rigor and validity of machine-generated analyses (De Paoli & Mathis, 2025; Mpofu, 2025). This development is not inherently problematic; rather, ensuring machine-generated analyses are rigorous is much needed. While we do not examine machine-generated analyses here, this example highlights the relevance of our critique: renewed interest in using saturation to determine the rigor of these analyses may risk reinforcing it as a universal standard—again—sidelining previous critiques and introducing new epistemic harms (Humphreys, 2025).
We structure our paper as follows. First, we briefly introduce epistemic injustice to establish the conceptual terrain for our critique. Then, we overview saturation, describing its varied conceptualizations, contingent nature, and use. Next, drawing on the work of Dotson (2012, 2014) and Fricker (2007), we theorize the process through which academic knowledge production practices can enact epistemic injustice. We use this to analyze the exclusionary effects of saturation in qualitative health research. This lays the groundwork to rethink saturation not as a hallmark of rigor but as a construct that must be used intentionally. Finally, we provide recommendations for the intentional use of saturation, with the lofty hope of advancing epistemic justice in qualitative health research.
Epistemic Injustice and Health
The concept of epistemic injustice was coined by Fricker in 2007 and refers to wrongs done to people when their ability to share, understand, or contribute to knowledge is unfairly dismissed or undervalued. Fricker distinguishes between two types, testimonial and hermeneutical injustice. The former occurs when people’s testimony is discredited based on their social identity, while the latter arises either when people lack the interpretive (i.e., hermeneutic) resources needed to make sense of their lived experiences or when their interpretations are discredited because they do not align with what others commonly believe, expect, or consider possible (Fricker, 2007). Importantly, as Bufkin (2024) highlights, scholars from diverse fields had already been grappling with questions regarding whose experiences, ideas, and voices shaped knowledge (see, for example, Collins, 2000; de Sousa Santos, 1998; Foucault, 1980; Haraway, 1988; Spivak, 1994), similar to those Fricker would later articulate. What Fricker managed to do was create renewed interest and significant momentum regarding the politics and philosophy of knowledge production, “[sparking] a veritable cottage industry” (Bufkin, 2024, p. 2). Since publishing her book in 2007, epistemic injustice has since been clarified, revised, and expanded on by Fricker (2017) alongside many others (see, for example, Catala, 2024; Coady, 2017; Dotson, 2012, 2014; Nikolaidis, 2021; Pohlhaus, 2017, 2020).
Taking the above into consideration, our overview of epistemic injustice is meant to be illustrative, not exhaustive. For comprehensive reviews of epistemic injustice in psychiatry, for example, see Kidd and colleagues (2025); and in patient–provider interactions, see Jonas and colleagues (2025). We use studies by Mezza (2025) and Kerr and DeMichelis (2025) to demonstrate some of the ways in which epistemic injustice has been examined in qualitative health literature, to help establish the conceptual terrain for our critique.
Mezza (2025) thematically analyzed a signal assessment, a type of report which comprehensively documents the evaluation of the causal relationship between an intervention and an adverse event (i.e., signal), produced by the European Medicines Agency. The assessment examined the potential causal link between the Pfizer COVID-19 vaccine and heavy menstrual bleeding. The evaluators had difficulty assessing if heavy menstrual bleeding was a potential side effect to vaccination because there was no formal definition and it was difficult to evaluate (i.e., what differentiates normal from heavy menstrual bleeding for an individual, for a population?). Mezza (2025) identified two epistemic mechanisms that underpinned this “difficulty.” The first was the lack of research on menstrual health, something which has been historically enacted and collectively sustained, resulting in a knowledge gap or what Fricker (2007) calls a hermeneutical gap. The second was the agency’s use of evidence-based medicine as a framework to determine what counts as reliable evidence. This positioned lay person (i.e., subjective) reports as less credible, constituting an example of testimonial injustice.
Although Mezza (2025) focused on epistemic injustice, we can extrapolate from her analysis to imagine material implications. For example, if menstrual changes following vaccination are not taken seriously, they may go uninvestigated, potentially resulting in prolonged symptoms, or delayed diagnoses and treatment either for vaccination side effects or other underlying issues. This could risk reinforcing long-standing inequities experienced by women and people who menstruate (Kerr & DeMichelis, 2025; Mezza, 2025). Similarly, if reports of menstrual changes are disregarded, this could erode confidence in regulatory and medical systems, as people who feel unheard may be less willing to report adverse events or seek future care.
While Mezza (2025) demonstrates how epistemic injustice may be enacted institutionally, Kerr and DeMichelis (2025) examine how epistemic injustice is enacted interpersonally during clinical encounters. Drawing on ethnographic observation of an online community for women with fibromyalgia and in-depth interviews with its members, Kerr and DeMichelis (2025) explored how women navigated and resisted epistemic injustice as they sought treatment for their fibromyalgia. Women’s self-reports of chronic pain were often discounted by clinicians who did not consider fibromyalgia a legitimate condition, and constructed these women as exaggerating or unstable (i.e., uncredible). The result was restricted access to treatment for their fibromyalgia. In response, community members shared their diagnoses and biomedical language they encountered during clinical encounters, such that the group functioned as a “real-time crowd-sourced database” (Kerr & DeMichelis, 2025, p. 5). Other members could thus use this language to resist experiences of testimonial injustice and legitimize their suffering and need for treatment.
As these examples illustrate, epistemic injustice can be enacted through institutional practices (Mezza, 2025) and interpersonal interactions (Kerr & DeMichelis, 2025), and has tangible consequences on people’s health.
An Overview of Saturation
Saturation is closely linked to the ideas of sample size, data adequacy, and information redundancy (Guest et al., 2020; Hennink & Kaiser, 2022; Saunders et al., 2018; Sim et al., 2018). That is, saturation is reached when enough data have been generated such that additional data generation and/or analysis is unlikely to yield new insights into the phenomenon under study. Understood another way, saturation is achieved when a researcher can understand the underlying logic and anticipate the broader narratives embedded in participants’ stories, and recognize how meaning is being constructed (Susan Cox, personal communication, December 2024). Decisions about when saturation is achieved also implicitly shape which perspectives, experiences, and interpretations are considered legitimate evidence, influencing the knowledge produced through qualitative health research.
An overview of saturation models
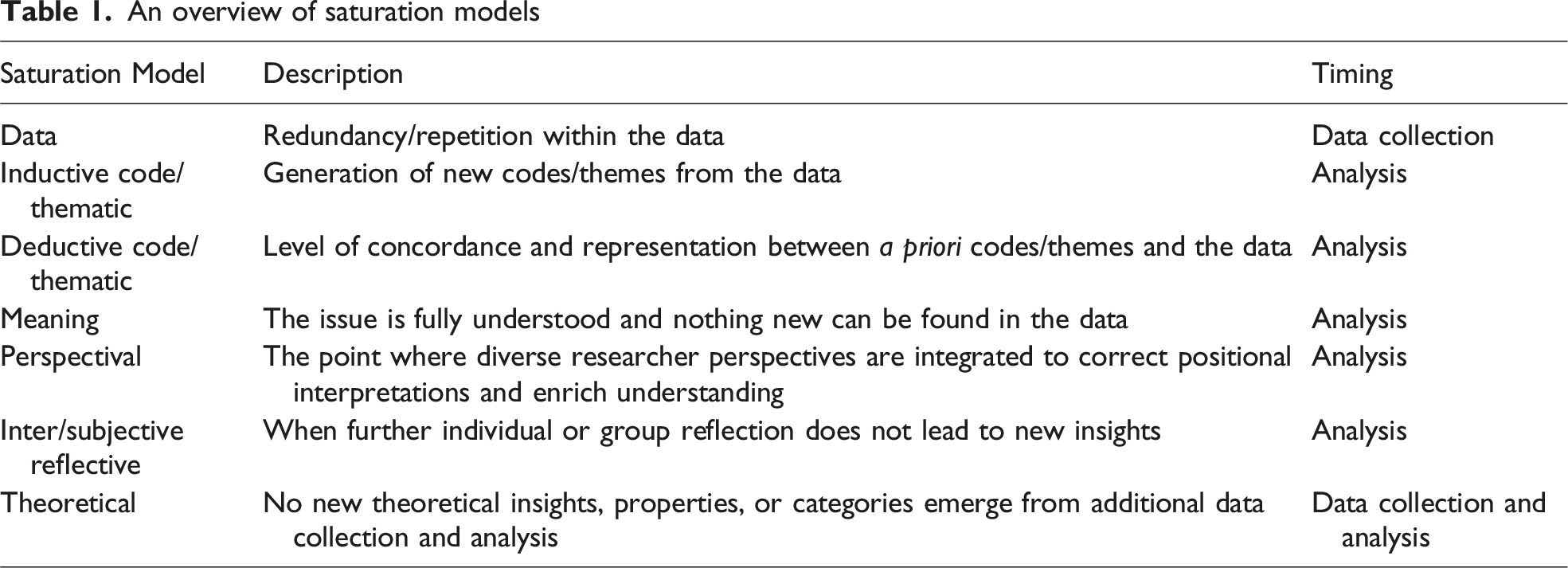
Data saturation occurs when no new information is identified during data generation. Code and thematic saturation are identified during analysis, and can be further categorized as inductive and deductive (Saunders et al., 2018). The former describes when no new codes or themes are generated, while the latter refers to the level of concordance between a priori codes or themes and how well these are represented in the data. Meaning saturation is likewise identified during analysis and refers to when the phenomenon under study is fully understood and “no further dimensions, nuances, or insights of issues can be found” (Hennink et al., 2017, p. 594). Perspectival, subjective, and intersubjective reflective saturation also occur during analysis. The former is achieved by integrating perspectives from a diverse team of researchers to address potential limitations owing to each person’s positionality, while reflective saturation occurs when individual (i.e., subjective) or group (i.e., intersubjective) reflection produce no further insights (Hiah et al., 2025). Given how they are conceptualized and when they might be “achieved,” different types of saturation will influence which data are examined and the knowledge generated through analysis. For example, an emphasis on data saturation may highlight patterns that recur across participants, whereas inductive thematic saturation may emphasize seemingly discordant cases that contribute to analytic depth.
While saturation has been conceptually expanded, we believe it is difficult to distinguish and use these different formulations in practice. For example, Hennink and colleagues’ (2017) definition of meaning saturation—the point at which an issue is fully understood and nothing further can be found—is little different from theoretical saturation, barring the emphasis on codes (Saunders et al., 2018). In fact, their conceptualization appears to align with inductive code/thematic saturation. The recently proposed subjective and intersubjective reflective saturation (Hiah et al., 2025) also seem near identical to meaning saturation, though we find the explicit use of subjective valuable for highlighting the role of the researcher or researchers in shaping and determining saturation.
Hood (2007) offers another example, writing about substantive saturation which she says is commonly used in generic inductive qualitative methods. However, Hood fails to provide a clear definition, referencing Maxwell (2005), who does not make any reference to substantive saturation. What complicates this is that saturation is often poorly defined and simply justified by a “throw-away line about achieving saturation” (Jennings & Yeager, 2025, p. 2). Caelli and colleagues highlighted this persistent lack of clarity over two decades ago, warning the concept’s “ubiquitous and non-selective use risks rendering the term meaningless to the qualitative research community” (2003, p. 9). Indeed, saturation attempts to cover a wide range of related albeit distinct ideas, assumptions, and processes into a single term. Thus, while it may be invoked as a marker of rigor, such claims are difficult to assess when it is not clearly defined or justified (Jennings & Yeager, 2025; Vasileiou et al., 2018).
As Saunders and colleagues (2018) note, the type of saturation adopted in a study has implications both for what it means to reach saturation and when it might be reached. For instance, data saturation suggests that data can be categorized as either unsaturated or saturated, and there is a discrete point at which the former becomes the latter (Saunders et al., 2018). In contrast, code, thematic, meaning, and theoretical saturation occur once coding and analysis are underway, and this suggests saturation may be better conceived as a matter of degree rather than a clear-cut instance (Saunders et al., 2018).
Another key consideration is the level of analysis at which saturation occurs. It is very different to saturate semantic or surface-level description than latent or underlying meaning (Braun & Clarke, 2021). Consider a hypothetical qualitative study exploring chronic pain management strategies, with analysis being guided by thematic saturation. Participants report several different treatments—such as medications and alternative therapies—each with unique considerations such as cost, access, and side effects.
If we are interested in descriptive themes (e.g., pharmacological, rehabilitative, and behavioral interventions), the dataset may appear far from saturated, with each account introducing seemingly novel information. Of course, as Morse clarifies, “we do not saturate particular details of individual events and random incidents. Rather, we saturate characteristics within categories” (2015, p. 587). Yet, it may be that participants have predominantly described medications, with only limited or passing references to other pain management strategies. This may reflect who was interviewed, such that further and targeted data generation would identify as yet unencountered or underrepresented data. However, latent or interpretive themes may be better substantiated by the data. For example, one theme could speak to the piecemeal and often improvised nature of pain management, and another, the emotional and financial impacts of living with inadequately controlled pain.
Hennink and colleagues (2017) demonstrate this distinction between descriptive and interpretive analysis, though they came to the opposite conclusion. They assessed when (inductive) code saturation occurred compared to meaning saturation, concluding that code saturation (i.e., “hearing it all”) occurred after analyzing nine interviews while meaning saturation (i.e., “understanding it all”) occurred between 16 and 24 interviews (Hennink et al., 2017). While they empirically examined saturation and we used a hypothetical scenario, we believe the fact we arrived at different conclusions underscores the inherently subjective nature of determining saturation. Indeed, saturation is contingent upon the model used, the desired level of analysis, the quality of the data, and the researchers conducting the study (Fusch & Ness, 2015; Guest et al., 2006). As Braun and Clarke write, the “judgements about ‘how many’ data items, and when to stop data collection, are inescapably situated and subjective [emphasis added]” (2021, p. 201).
It is also important that the choice of saturation model align with the study’s analytic aims (Tight, 2024). Data saturation appears to most closely align with descriptive analysis, given the focus on identifying new information during data generation. Meaning and theoretical saturation are concerned with depth and richness of understanding and involve highly interpretive analytic work, thus aligning best with latent analysis. Code and thematic saturation can align with either. All of this suggests that, if we use saturation, it should be done so intentionally.
Scholars have also proposed alternative concepts, such as information power (Malterud et al., 2016), recognizing the potentially inappropriate use of saturation in methodologies other than grounded theory. The concept of information power suggests a smaller number of participants can generate the appropriate amount and quality of data if the aim of the study is narrow, in-depth, and theoretically driven; the sample is well-defined; and the dialogue is detailed and nuanced (see, for example, Amri et al., 2025). Conversely, a greater number of participants will be needed should the study aim and/or sample be broader (see, for example, Liberati et al., 2021), atheoretical, or theoretically underdeveloped, and/or the quality of the dialogue weak.
Despite the availability of alternatives like information power—also facing critiques (Sim et al., 2018)—saturation remains widespread in qualitative health research (Braun & Clarke, 2021; Guest et al., 2006; Jennings & Yeager, 2025; Saunders et al., 2018), with some referring to it as “the gold standard” for high-quality qualitative research (Guest et al., 2006; Hancock et al., 2016). For example, in a review of 214 qualitative health articles collated from one journal each in the disciplines of psychology, sociology, and medicine, Vasileiou and colleagues (2018) found that 55% of articles justified their methods and analysis by invoking saturation. More recently, Jennings and Yeager (2025) reviewed 152 articles from the six nursing journals with the highest impact factors and found that roughly 45% of the articles mentioned saturation.
Although health phenomena are multifaceted and encompass myriad dimensions, we believe the preoccupation with saturation in qualitative health research reflects how positivism maintains an ideological hegemony in health research (Park et al., 2020; Varpio et al., 2017). That is, positivism is the dominant set of ideas, beliefs, and values which influences and shapes what is considered legitimate scientific inquiry and what is not (Held, 2023; Tight, 2024; Varpio et al., 2017). As a philosophical orientation, positivism asserts the existence of a singular, objective reality that can be studied and understood through value-free science based on empirical, and primarily quantitative, evidence (Park et al., 2020). The appeal to quantification embedded within saturation assumes the superiority of numbers, such that qualitative findings are legitimate only if they are numerically supported. Such appeal is evidenced by the strategies proposed for determining when saturation is achieved, such as through code or theme frequency (see, for example, Guest et al., 2020), and reinforced by reporting guidelines and checklists (see, for example, Standards for Reporting Qualitative Research [SRQR; O’Brien et al., 2014]; COnsolidated criteria for REporting Qualitative research [CORE-Q; Tong et al., 2007]).
By adopting saturation, we assume there is a stable truth embedded in participants’ accounts that can eventually be exhaustively known (Braun & Clarke, 2021; Sim et al., 2018). However, this framing imposes a standard of scientific rigor that does not appropriately account for methodologies which view social phenomenon as multiple and situated (Sim et al., 2018). Moreover, it ignores the role of context within which research actors and research processes are embedded and upon which meaning is contingent (Held, 2023).
It is important to note that qualitative research spans a range of paradigms. Some approaches, including certain postpositivist or pragmatic orientations common in health sciences, may adopt saturation as a criterion for rigor in ways that align with their assumptions. Our critique is not directed at these approaches nor with positivism itself. Rather, we are concerned by the superiority afforded to positivist health science which has pressured qualitative researchers to adopt saturation to legitimize their work (Braun & Clarke, 2021; Jennings & Yeager, 2025; Varpio et al., 2017). We believe it is this ideological hegemony of positivism vis-à-vis saturation (for emblematic examples, see Guest et al., 2020; Lowe et al., 2018) that creates the structural conditions by which saturation may enact epistemic injustice, which we discuss below.
Analyzing Saturation Through the Lens of Epistemic Injustice
In this section, we theorize the relationship between epistemic oppression (Dotson, 2012, 2014) and hermeneutical marginalization and hermeneutical injustice (Fricker, 2007). Recall our earlier examples which demonstrated how epistemic injustice can lead to material harm, such as prolonged symptoms, delayed diagnoses, and limited or absent treatment (Kerr & DeMichelis, 2025; Mezza, 2025). Building on these examples, we suggest that the uncritical use of saturation has a similar potential to enact epistemic injustice and in turn material harm, by limiting what data and analyses are recognized as legitimate and rigorous bases for making claims about health and illness. We draw on an article by Howard and colleagues (2021) to consider how saturation might enact epistemic injustice when we have “thin” data. We then explore the implications of privileging data that can be repeated or corroborated across multiple instances, which may marginalize singular, one-off narratives that nevertheless offer important insights. This leads us to consider how methodological choices shape what is recognized as data and how some methodologies may not be compatible with saturation.
Epistemic oppression refers to the exclusion of people and groups from participating in knowledge production practices (Dotson, 2012, 2014). For our purposes, we are interested in third-order epistemic oppression, which refers to the structural conditions—the ideological hegemony—that lead to the exclusion of certain people and groups (Dotson, 2012, 2014). As mentioned above, positivist assumptions continue to influence what is considered legitimate scientific inquiry in qualitative health research (Held, 2023; Tight, 2024; Varpio et al., 2017), even as other paradigms have challenged and broadened definitions of legitimate science. When people and their interpretations are excluded from knowledge production practices, this can be described as hermeneutical marginalization (Fricker, 2007). That is, they are excluded from and thus cannot contribute to the creation of shared interpretive resources. Persistent exclusion results in gaps in the resources through which we make sense of individual and collective life. Hermeneutical injustice thus occurs when certain people or groups experience difficulties understanding or communicating their social experiences, or their interpretations are discredited because they do not align with what is considered possible (Fricker, 2007). These dynamics become evident in the methodological challenges described by Howard and colleagues (2021), whose study illustrates how assumptions about what constitutes adequate data (i.e., data that can be saturated) can marginalize certain interpretations and insights.
In their article, Howard and colleagues (2021) describe methodological challenges they faced conducting a qualitative study with participants who had various chronic, critical illnesses and who all required mechanical ventilation. Chiefly, the data were “‘thin’ by conventional qualitative health research standards” (Howard et al., 2021, p. 9) given participants’ ventilation-related communication impairments. They used the following example to illustrate this thinness: Interviewer: What makes a bad day? Resident: The nurses. Interviewer: The nurses. And what are the types of things that they do to make it bad? Resident: [Long breath] it’s either their way or [mouthed the word nothing] Interviewer: Their way or nothing? Resident: [inaudible] Interviewer: So what types of things? Can you give me an example? Resident: Everything and anything. [long breath] so that you have to. [long breath] it’s a vicious setting. Interviewer: It sounds incredibly frustrating. Is there anyone you talk to about that? Resident: [participant nodded head no] Interviewer: No? Resident: It would get back to the nurses. Interviewer: And what would happen if it got back to the nurses? Resident: I’ll get the look. Interviewer: You’ll get a look? Resident: You did it. Interviewer: A look of, I know you did it? And is that? Correct me if I’m wrong, but to me it sounds like a form of punishment? Resident: It is. I get the silent treatment. It’s really hard and it’s [long breath], “you did it.” [long breath]. Cause they’re [the nurses] mad at me. [long breath] over and over and over. (Howard et al., 2021, p. 9)
This example demonstrates the challenges faced by Howard and colleagues (2021), arising from participants’ communication impairments which often resulted in stilted narratives characterized by short or inaudible answers and punctuated by long breaths and slight nods. To respond to the constraints of their data, they adopted a narrative analytic approach rather than using line-by-line or segment-by-segment coding to organize and analyze the data, noting the thinness of the data would have made it difficult if not impossible to reach saturation.
Recall that saturation privileges data that can be repeated, corroborated, and/or generalized across multiple instances. Had Howard and colleagues decided to prioritize data that could be saturated, the voices of participants with more severe communication impairments would be “relegated to the sidelines” (2021, p. 9). This exclusion can be understood as a form of hermeneutical marginalization, and persistent marginalization of this kind would create gaps in shared interpretive resources, contributing to the potential for hermeneutical injustice and material harm. For example, care practices might be based on incomplete evidence, leaving the needs of patients with communication impairments unmet or misunderstood.
Alongside thin descriptions, the emphasis on saturation may also marginalize narratives which are singular, are complex, or resist neat categorization into thematic patterns. Singular stories may offer profound insights into the health phenomenon under study by potentially challenging dominant narratives and generating important nuances. Yet, the drive for saturation may push researchers to overlook these insights in favor of those that fit into coding frameworks and contribute to data redundancy and analytic consistency.
Similarly, methodologies that are incongruent with saturation may be discredited or devalued. This is in part because our choice of methodology actively shapes what we consider data in the first place. Ethnography, for example, often relies on observational fieldwork, but when observations concern events that occur infrequently or under highly specific conditions, it raises questions about how such observational data could be saturated. Likewise, a discourse analysis of a single policy document presents a bounded text. In both instances, we are challenging the conventional application of saturation, which emphasizes and privileges data and insights that can be generalized across multiple instances.
Saturation may also be fundamentally misaligned with the ontological and epistemological assumptions of certain methodologies, especially those which embrace multiplicity, contextuality, and emergence. Indigenous paradigms, for example, have long critiqued colonial epistemic regimes that systematically devalued Indigenous ways of knowing (Hart, 2010). Historically, these regimes discredited Indigenous people (i.e., testimonial injustice) and prevented them from contributing to shared interpretive resources, rendering their experiences unintelligible or discrediting their interpretations (i.e., hermeneutical injustice) (Hart, 2010). Thus, relying on saturation to validate and legitimize research findings can risk reproducing inequities in knowledge production by favoring positivist-aligned epistemologies while sidelining or “blinding” (Hart, 2010) relational, emergent, or contextually situated ways of knowing. This selective design is not a neutral process; rather, it reflects what Spivak (1994) calls the epistemic violence through which predominantly Western researchers filter and erase the agency and voices of their marginalized subjects, which has been and continues to be a major tool of colonial violence (Hart, 2010).
Rethinking the Role of Saturation in Qualitative Health Research
Echoing Tight (2024), we believe saturation has become overworked and overused in qualitative health research. It is invoked so broadly and flexibly that it compresses a range of distinct ideas, assumptions, and processes into a single, ill-defined term, and as a result is doing a disproportionate amount of conceptual work. However, the meaning and operationalization of saturation are highly contingent and require careful alignment with the ontological, epistemological, and methodological foundations of the research project.
Viewed through the lens of epistemic injustice, the uncritical use of saturation has serious implications for academic knowledge production. By privileging data that can be repeated, corroborated, or generalized across multiple instances, saturation can delimit the interpretive resources available for understanding and representing peoples’ experiences of health and illness. Resulting knowledge gaps can further translate into material harms, such as prolonged symptoms, delayed diagnoses, and restricted access to treatment (Kerr & DeMichelis, 2025; Mezza, 2025).
To address the potential limitations and harms associated with the uncritical use of saturation, we suggest changes at two levels: research design and publishing. First, researchers must approach saturation as a methodological choice, not a requirement. Its use should be intentional, and only when saturation aligns with the epistemological commitments of a project. Moreover, researchers should adopt reflexive, context-sensitive practices consistent with their methodology rather than rely on procedural adherence to checklist-based standards to ensure and indicate rigorous analysis (Morse, 2021). Otherwise, by relying on procedural adherence to checklist-based standards, we may inadvertently reinforce the use of saturation and risk perpetuating epistemic injustice and material harm.
Second, peer reviewers, editors, and other academic knowledge production gatekeepers must interrogate their assumptions about saturation. Rather than treating saturation as a universal benchmark for rigor, gatekeepers should consider whether saturation is conceptually compatible with the aims and orientation of the work they are evaluating. These are important steps to help prevent the enactment of epistemic injustice through academic knowledge production practices, thereby ensuring a broader range of knowledge and experiences are legitimized and represented in our shared interpretive resources about health and illness. We believe this will have direct implications on material experiences of health and illness, and support efforts to redress health inequities.
Footnotes
Acknowledgments
We extend heartfelt thanks to our colleagues at the W. Maurice Young Centre for Applied Ethics, who provided helpful feedback in the early stages of conceptualizing and writing this paper. We particularly appreciate Dr. Susan Cox, whose qualitative expertise and thoughtful suggestions further advanced this manuscript. Michelle Amri would also like to acknowledge the donors to the Mary and Maurice Young Professorship in Applied Ethics.
Ethical Considerations
Ethical approval was not required as this manuscript is not the product of research involving participants.
Author Contributions
Jackson P. Loyal conceptualized the paper and led drafting of the manuscript. Michelle Amri contributed to conceptualization of the paper and made critical revisions to the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.