
Abstract
This study was conceived by nurse researchers working throughout the pandemic on a COVID ward, aiming to explore in depth the experience of ward staff. Full ethical approval was obtained and in-depth unstructured interviews were conducted with staff members (two doctors, two healthcare assistants, two allied health professionals, and four nurses). Data analysis followed a psychosocial approach using psychoanalytic theory as a tool for examining data. Whilst previous research has identified the emotional labor of work during the COVID pandemic, with subsequent impact on staff mental health and well-being, this is the first study to demonstrate the usefulness of psychoanalytic methodology in this context. Deeper consideration of the internal world and affective experience of the participants in relationship to external events and context enables a complex interpretive understanding of the phenomena. This study therefore provides valuable insight on a different level to that attained through traditional quantitative and qualitative research methods. A psychoanalytic lens of analysis enabled us to develop a model of the elements which combined to lead to psychological disturbance, the institutional defences that inadvertently compounded the experience as traumatic, the personal meaning derived from the experience, which staff members relied on to survive, and the lasting impact. We add to the evidence base around experience of the COVID pandemic, highlighting the profound and long-lasting impact on staff and demonstrating the value of psychoanalytic research methodology. We conclude by discussing the implications of our study for future practice, particularly in terms of leadership and staff well-being.
Introduction
The impact of the pandemic on staff mental health and well-being was unsurprising, given the lack of mental health support for NHS (National Health Service) staff identified several years previously (Boorman, 2009). Pre-COVID, nurses were already at increased risk of burnout, post-traumatic stress disorder (PTSD), and suicide (Maben et al., 2022). During the pandemic, negative effects on mental health were identified at a population level in the United Kingdom (Newman et al., 2022), with healthcare workers (HCWs) in particular reporting profound emotional, behavioral, and cognitive impact. Many experienced difficulties such as anxiety, anger, disrupted sleep, stress, and increased alcohol intake (Chotalia et al., 2022). More severe psychological distress included de-personalization, self-harm, and suicidal thoughts (Majumder et al., 2021). Emotional distress led to burnout, compassion fatigue, moral distress, and increased attrition (Boland et al., 2023).
Literature Review
We undertook a narrative literature review regarding the impact of the pandemic on HCWs. Studies typically utilized surveys to produce large descriptive data sets and statistical correlations; some qualitative studies, largely phenomenological, explored lived experience in greater depth. We synthesized both qualitative and quantitative findings to highlight key findings relating to external and internal factors. Many studies listed individual factors affecting HCWs’ mental health, along with subsequent coping mechanisms. One systematic review exploring mediators of psychological well-being among HCWs during previous pandemics worldwide found that self-efficacy, coping ability, and altruism were protective factors (Schneider et al., 2022). Other studies associated mental well-being with psychological flexibility, tolerance of uncertainty, and resilience (Johns et al., 2022). Demographic factors associated with greater risk of emotional distress, anxiety, and depression include being young, being female, or being a less experienced or part-time worker (Beck & Daniels, 2023; Dai et al., 2020; Lancee et al., 2008; Matsuishi et al., 2012; Nickell et al., 2004; Zhang, Wang, et al., 2020; Zhu et al., 2020). Lower educational level was found to have an impact on insomnia symptomatology (Zhang, Yang, et al., 2020) and mental health more generally (Lung et al., 2009). A pre-existing physical illness predicted psychological outcomes such as depression, anxiety, insomnia, and PTSD (Shacham et al., 2020; Zhang, Yang, et al., 2020; Zhu et al., 2020). HCWs with physical symptoms of the pandemic disease were more likely to report depression, anxiety, stress, and PTSD (Chew et al., 2020; Schneider et al., 2022).
With regard to external factors affecting HCWs during the pandemic, survey data highlighted perceived and actual support received and the effect of this on psychiatric symptoms. All report similar factors with increasing anxiety levels during the pandemic such as fear of contagion, lack of personal and protective equipment (PPE), uncertainty, perceived social support, struggles to connect with patients, and being overworked and isolated (Ariza-Montes et al., 2022; Beck & Daniels, 2023; Mitchinson et al., 2021; Newman et al., 2022; Siddiqui et al., 2021). Perceived and actual support received had a powerful influence on mental health and well-being of staff. Perceived support had a positive effect; support from the hospital, supervisors, colleagues, or the government was protective against psychiatric disorders such as depression and anxiety (Zhu et al., 2020); characteristics considered important were being heard and being valued (Gordon et al., 2022, p. 516).
Studies reported an overwhelming sense of “lack of control,” highlighting issues with policies and guidelines being inconsistent and at times in tension with HCWs’ values (Ariza-Montes et al., 2022; Pilbeam & Snow, 2022). Response to the pandemic included a direct Mental Health Recovery Action Plan from the UK Department of Health (DHSC, 2021) for frontline workers. NHS Trusts implemented psychological support provisions, the response to which varied; whilst appreciated, many staff could not access support or were concerned with stigma attached to doing so (Clarissa et al., 2021). Some staff found participation rewarding (Olabi et al., 2022) whilst others felt it was not necessary (Weston & Nordberg, 2022). Resilience was a concept used frequently during the pandemic and not always viewed favorably; one qualitative study of nurses’ conceptualization of resilience during COVID-19 and the impact on their mental well-being emphasized that nurses felt blamed for experiencing workplace stress when perceived not to be resilient “enough” (Conolly et al., 2022). This is particularly relevant when considering what reaction would be “normal and appropriate” in the extreme circumstances and context of the COVID-19 pandemic.
Many lessons learned from the pandemic have been well documented. First, interventions are needed to address the lack of adequate PPE and the burden of being considered a hero during a pandemic (Ball et al., 2023; Chegini et al., 2021; Gunawan et al., 2021; Nelson et al., 2021). Second, support required for the mental health and well-being of staff is multifactorial, including supportive environments, equal treatment of staff, access to support services, and ensuring the safety of self, colleagues, and loved ones (LoGiudice & Bartos, 2021).
In summary, the internal and external factors which predisposed staff to mental distress during the pandemic have been identified and elaborated in previous studies. Large-scale surveys have elicited descriptive data, with a smaller number of qualitative studies of lived experience adding a richer insight into these factors. What is missing from the extant literature is a detailed analysis of the dynamic interaction between the responses of frontline HCWs, healthcare organizations, managerial staff, and the public, applying a robust theoretical framework in order to understand the cumulative impact on HCWs’ sense of identity and their capacity to continue to provide effective and life-saving care, in the face of previously unimaginable stress, and the long-term implications for sustaining the well-being of the health and social care workforce. This is important, as future global pandemics or similar are an almost certainty, and awareness of risk factors alone cannot guide or inform effective strategies for reducing the risks of HCWs developing mental health conditions. This is particularly relevant in the current climate of “the toughest winter in NHS history” (Toynbee, 2025); again, the impact of this has yet to be realized.
An interesting perspective identified in previous studies is the comparison between working in COVID and war environments. Horton (2020) collected accounts from NHS workers: “as distressing as they have been horrifying”; these referred to “humanitarian crisis” and “total carnage” (p. 1022). Glasper (2021) compared the NHS at the start of the pandemic “to a war-zone casualty station… analogous to that faced by Florence Nightingale… in the Crimean War” (p. 252). The devastating impact on staff emotional well-being was unsurprising. As Glasper described, “Nightingale herself was a broken woman by the end of the Crimean War, suffering years of ill health attributable to PTSD” (2021, p. 252). Psychotherapeutic expertise in identification and treatment of post-traumatic stress emerged from doctors and nurses treating soldiers psychologically damaged by their battlefield experience in WWI; the whole field of study derives from their initial work with this cohort (Temple & Wadell, 2002).
We recognize that references to war are set against a political landscape, underpinned by the state of the NHS at the time of the outbreak. The UK Government was already under significant pressure with staff shortages, long waiting lists, insufficient beds, and buildings unsuitable to contain infection, already creating the perfect storm (Ramsey, 2025). The analogy of war also emerged as the overarching theme from our inductive analysis; we took this as a starting point to contextualize and develop several illuminating sub-themes such as “command and control.” As shown in Figure 1, we examine how the “frontline” experience was traumatic for participants on several interconnected fronts, explored through themes of fear, chaos, chinks in the armor, and dealing with death. Taking a data-driven approach, we utilized psychoanalytic theory from the British school of object relations (otherwise referred to as Kleinian and post-Kleinian theory)—led by the content of participant interviews, which repeatedly contained motifs relating to being in a fight for life, fear of death, and having ones resources overwhelmed by fundamental anxieties—to elaborate a more nuanced analysis beyond a straightforward description of the work experiences that created duress, to understand the dynamic interaction between external events, the environment, and social, organizational, and personal threat/coping responses. Overarching theme and sub-themes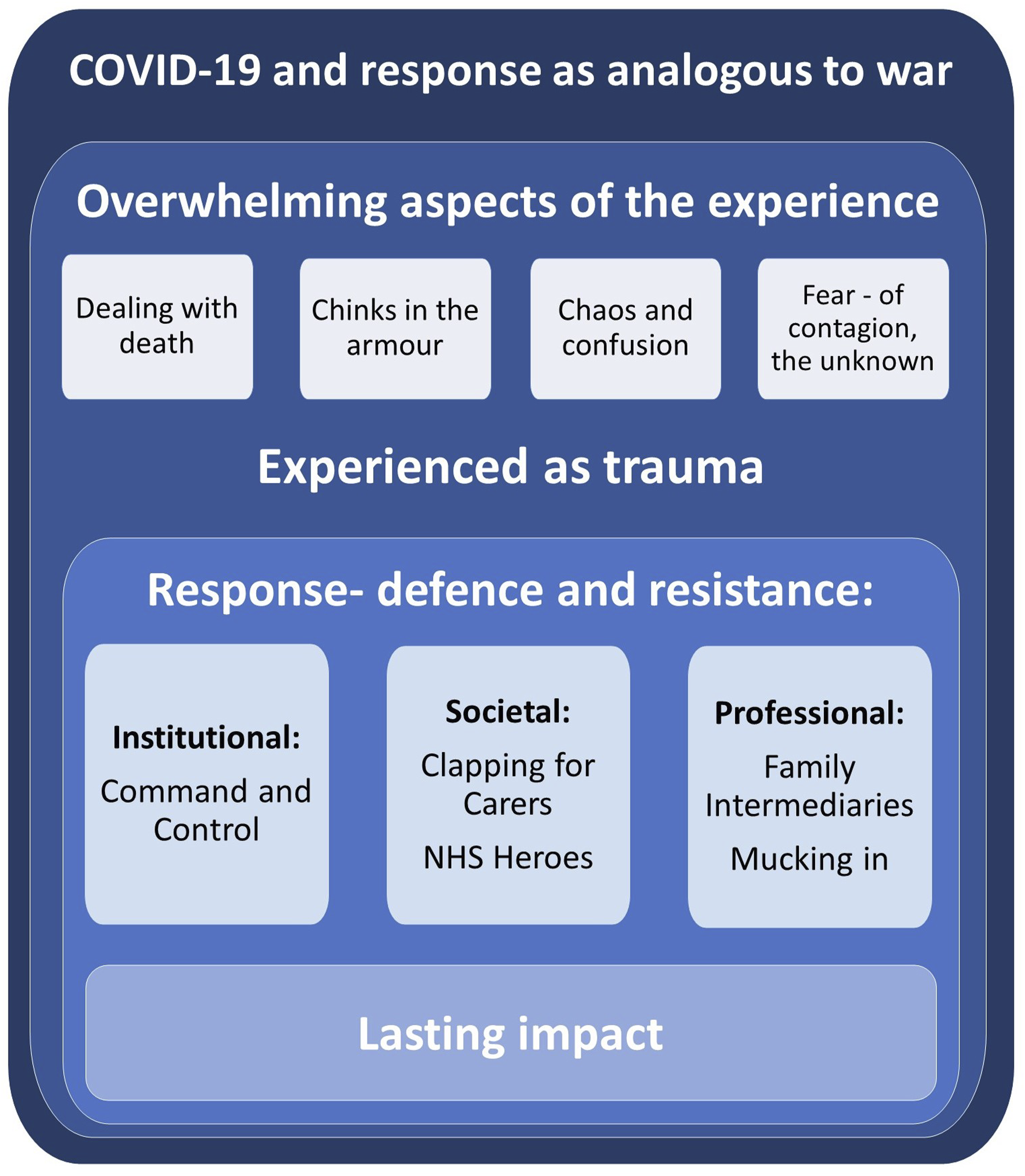
The British Object Relations movement rose out of another great existential threat in our recent history—World War II (Baraitser & Salisbury, 2020)—and was refined and expanded through the analysis of those experiencing severe illness (Bion, 1962; Klein, 1959). It is a theory of human development that, whilst originally derived from analysis of individuals, has been applied at team, community, organization, and societal levels in both seminal and contemporary work seeking to understand the unconscious effects of existential threats faced within health care settings (e.g., Baraitser & Salisbury, 2020; Foster & Smedley, 2019; Garland, 2002; Klein, 1937; Menzies-Lyth, 1988; Ramsey, 2024; Stamenova & Hinshelwood, 2018). Our study is in keeping with this tradition.
Research Aim
The aim of the study was to use a qualitative methodological approach incorporating application of contemporary psychoanalytic object relations theory: • To address an important gap in the extant literature regarding the COVID experience. • To understand the psychosocial, intra-, and intersubjective processes underpinning response to the COVID pandemic among HCWs. • To bear witness to the long shadow that COVID has cast on HCWs’ experience and identity; now COVID wards have disappeared and there are no sites of disturbance to return to, or relics to sustain institutional and social memory. • To counter the potential for unconscious repetition in healthcare organizations as social systems, through learning from experience. • To identify learning for ongoing care and support of the work force, both for future pandemics and during periods of seasonal pressure, when respiratory virus cases overwhelm capacity for care provision.
Methodology
Psychosocial research methodology was adopted (Clarke & Hoggett, 2009) utilizing psychoanalytic research methods, particularly for the data analysis process. Described as a hybrid existing between clinical practice and social science within a psychosocial research framework, psychological and social domains that make up the focus of investigation are sought and “thought together” (Frosh, 2003, p. 1547). Domains are the individual, system, and structure plus connections between them, including that which is not measurable, the “extra-rationale” of emotional dynamics and the unconscious (Taylor, 2017). Psychoanalysis considers the internal world of the subject (in this case the HCW) in the context of their psychosocial experiences, along with their family structure, social group, institutional structures, and so on. Psychoanalytic perspectives have been used to facilitate qualitative data analysis to understand the relational components of healthcare delivery (Foster & Smedley, 2019; Gough, 2009) and in organizational studies (Stamenova & Hinshelwood, 2018). In this study, data from unstructured interviews with members of staff who were part of a wider study of patient, staff, and carer experience on a COVID ward were analyzed utilizing an inductive process to identify themes. This was followed by application of Kleinian and post-Kleinian object relations theory, and its application to traumatic experience in adulthood (Garland, 2002) facilitating elucidation and meaning-making of deeper inter/intrapersonal factors and the dynamic iterative relationship with the external context in which participants were situated.
Healthcare work involves physical and emotional elements hard to define and invisible to others (De Frino, 2009). A psychoanalytic theoretical lens was employed for secondary analysis to address this, as it provides a high level of magnification of detail, seeking to track and understand moment-to-moment changes in states of mind (Bion, 1962). Under an ordinary level of magnification, the work may appear domestic and ordinary; detailed scrutiny reveals it to be highly complex (Deacon & Cleary, 2012). Psychodynamic theory has a language for intra/interpersonal and relational processes that can be used to illuminate and understand HCWs’ emotional experience of their work and of the care contexts they occupy, as they described it within the data. This is important to provide an enhanced level of insight into the psychosocial context of work during the pandemic and resultant response of staff members.
Researcher Positionality and Its Implications for Research Methods
Within the epistemic frame of psychosocial and psychoanalytic research methods, the researcher’s subjectivity must be located and considered in relation to effects upon the knowledge produced whilst accepting that absolute transparency is not achievable (Pillow, 2003). The knowledge we generate as qualitative researchers is situated, specific, and partial, shaped by the focus of our own interests and the specific circumstances within which research is conducted (Corlett & Mavin, 2018), but is no less important as a result. The new meanings and understanding generated by psychoanalytic research methods contribute to a larger field of knowledge, patching our specific and partial views together in order “to see together without claiming to be another” (Haraway, 1988, p. 586). The initial research was conducted by two female researchers (SR and HH), both post-doctoral with previous experience of qualitative research. Having worked clinically on the ward in question throughout the pandemic, they were previously known to the participants and had first-hand experience of the subject and setting they were seeking to interrogate. Choice of research subject and setting often reflects the inner dynamic of the researchers themselves (Clarke et al., 2008). SR and HH identified personal motivation to understand and bear witness to the specific emotional and psychological experience of working within a COVID ward; now they have disappeared and there are no sites of disturbance to return to, or relics to sustain institutional and social memory. Data analysis can, in this case, become a closed system of confirming one’s own internal reality, without systematic interrogation of positional reflexivity and use of an analytic third, that is, someone with a greater psychological distance from the subject of analysis, who could assist the primary researchers with distinguishing between participant and researcher voice/perspective in the analysis (Davies & Eagle, 2013). At the point of data collection, unstructured interviews were employed that centered the participant’s account of their experience rather than the researchers (see below). At the data analysis phase, the third author, a registered mental health nurse, registered psychotherapist, and academic, provided methodological consultation and an overview of the data analysis theoretical abstraction process, outwith of direct experience of the context of the study. Psychoanalytically oriented research supervision enables the researcher to identify their own motives and blind spots in relation to the project, allowing different perspectives to emerge (Tietel, 2002).
Sample and Setting
Ten members of staff were interviewed as part of a study of patient, staff, and carer experience on a 65-bedded COVID ward at an NHS hospital site in England. COVID wards were make-shift arrangements, repurposing ward environments usually used for other specialties, to which staff who did not usually work together were deployed to look after large numbers of acutely ill COVID-positive patients. Two participants were allied health professionals (AHPs), two were medical staff of different seniority, and six were nursing staff of varying levels of experience and seniority. Pseudonyms have been used to refer to participants to maintain confidentiality. Details of setting and sample have been previously reported (Hurst & Ramsey, 2025).
Data Collection
Generation of situated, narrative data is at the heart of psychoanalytic and psychosocial research methods (Taylor, 2017). The full methodology of the wider research study, from which raw data for this analysis were drawn, has been published and provides further detail of the interview process (Hurst & Ramsey, 2025). Data collection took the form of open-ended interviews, with participants invited to tell their story with limited prompting from the researcher. The opening question therefore asked the participant to talk through their experience of COVID. The interview approach was similar to that of the psychoanalytically informed research interview (Holmes, 2013), involving use of free-flowing attention and empathic sensitivity along with demonstration of curiosity through summarizing, clarifying, and playing back the researcher’s understanding, respectful exploration of complexity and ambiguity, and allowance for free associations to the interview material (Long & Harding, 2013). Interviews varied in length, typically lasting between 30 minutes to an hour, with audio recording and subsequent verbatim transcription.
Data Analysis
Themes were derived from the data in a double/triple hermeneutic process of analysis, enabling consideration of the internal world of the participants rather than focusing only on their conscious presentation (Stamenova & Hinshelwood, 2018). SR and HH conducted the primary analysis. To understand the data as a coherent whole, all transcripts were read and re-read as a complete data set, before an inductive examination of each interview transcript in depth, firstly in isolation, giving priority to holistic analysis of each interview, and then in relation to the participant group as a whole. Such movement between parts and the whole is integral to psychoanalytic and psychosocial data analysis (Clarke & Hoggett, 2009), allowing core themes to emerge whilst retaining individual meaning and experience. Emergent themes and concepts were defined by combining related topics and content areas from the open coding process.
Psychoanalytic theory, specifically object relational and its application to both individuals and social and organizational contexts, was applied as a theoretical lens, to illuminate and elaborate findings from the primary data analysis and generate a conceptual model of HCWs’ intrapsychic, interpersonal, and psychosocial experience. Theory was used to conceptually reinforce the interpretations of the researcher, to ensure they are logically and methodically consistent (Clarke & Hoggett, 2009).
Rationale for Selection of Kleinian/Post-Kleinian Object Relations Theory as the Theoretical Framework
Emergent themes for inductive primary analysis of data related to fundamental fears, psychological defences, and coping mechanisms in the face of overwhelming stress, and the specific individual impact and meaning that participants made of their experiences of patient care and their organizational and societal context. Central to Kleinian and post-Kleinian object relations theory is the concept that experiential learning from our most formative relationships in early life continues to be encoded in our responses to others in adulthood, often re-activated in everyday encounters, and especially so by the experience of injury and extraordinary illness (Barratt, 2021). Klein conceptualized the experience of being ill as a return, often in ways outside of our conscious awareness, to the earliest pre-verbal anxiety and danger situations experienced in infancy, activating defences (threat responses), and latent wounds from early childhood when we were reliant upon others for our survival (Klein, 1937). Within this model, the experience for professionals of having their attempts at help thwarted by the magnitude of the problem or environmental and organizational challenges can be equally re-activating of primitive defence mechanisms. This can create a cycle of escalating distress and dysfunction, including splits between individual staff members and within organisational and social systems (Adshead & Guthrie, 2015). Object relations can offer a tool for unpicking and resolving this cycle. Importantly it is also a theoretical framework that views the physical environment as an active player in unconscious processes; it has a specific contribution to make in relation to understanding the dynamics of traumatic stress. Its utility to elaborate deeper meaning of themes in the data was therefore three-fold.
Ensuring Process for Trustworthiness and Rigor
The third author, with knowledge of the clinical context from which data were drawn, but independent of the process of data collection, theme identification, and abstraction, was identified to establish relative trustworthiness of the emergent themes and rigor of analysis and to ensure themes remained grounded in the data. This was done by systematically working backward from the identified themes and theoretical elaboration of data pertaining to these, and into the raw data (interview transcripts). Data analysis methods have been systematically applied and rigorously adhered to, as a means of being accountable for how particular readings of the data were reached (Frosh & Emerson, 2005). Presentation and reporting of results were undertaken in accordance with the recommendations for reporting qualitative analysis by O’Brien et al. (2014).
Findings Conceptualized Through Application of Psychoanalytic Theory
Overarching Theme: COVID-19 and Response as Analogous to War
The bay looked like a bomb site. The patients just looked like carnage, this auxiliary took one look at me and I said, “what can I do?” They just burst into tears, ripped their visor and all the rest of it off and went “I’m going. I just need to get out.” (Andrea, Nursing)
HCWs providing direct patient care were described both by themselves and others as working on the “front line” of the pandemic: “[frequent policy changes] made it harder for us who’s on the frontline” (Andy, AHP). In common with studies highlighted in the literature review, several of our participants used language evocative of the trauma of war. Alan (Medical) described “having to fight” management to maintain social distancing among staff, whilst Theresa (Nursing) described the “fight” against COVID: “You know people are not going to recover from this but at the same time the fight is on, trying to get them to recover.” Colette (Nursing) described finding work on the COVID ward: “Quite traumatic. I asked not to go back. I’m an [acute medical] nurse. We make people better. And I just didn’t feel we’d got anywhere with some of them. I felt quite defeated almost.”
Along with references to working on the “front line,” participants described fighting a battle against COVID, with subsequent feelings of defeat when patients succumbed to the virus. Within the next themes, as shown in Figure 1, we articulate how this war-like experience of working in the pandemic came to be traumatic for so many.
In object relations theory, we all survive a kind of developmentally ordinary original trauma that sets the conditions for developing capacity to cope with difficult emotions and states of mind, built on across the life course. Infants, helpless and adjusting to the terrifying new, post-birth reality, experience overwhelming “life and death” anxiety. These fears produce instinctual defences against what feels to be life-threatening attacks (Klein, 1959). Primitive defences include splitting objects (good/bad) and feelings (love/hate), projection of hostile or unmanageable feelings on to others, and avoidance and denial (Klein, 1946). In good-enough circumstances, our fears are ameliorated by the loving handling and responsiveness of our carers (Bion, 1962), which in time gets internalized as one’s own ability to tolerate and cope with anxiety—a kind of internal container for holding worries—but our most fundamental fears of dying or being at the mercy of hostile external forces are never fully let go. Stressful circumstances in adulthood can re-activate fundamental pre-verbal anxieties and the primitive coping mechanisms we employed to cope, particularly in moments where our self/ego feels under threat (Klein, 1959).
HCWs are relied upon to tolerate physical, psychological, and environmental stress beyond the ordinary, using knowledge and experience to cope with the demands of their work. Their sense of competence in a crisis acts as a form of armor, their knowledge base enhancing their internal container, supporting them to take in and make sense of raw experiences which on the face of it seem intolerable (Foster, 2009). However, our first four themes demonstrate how chaos, confusion, and ill-preparedness intersected to produce the specific characteristics of psychological trauma for participants, the raw anxieties this provoked, and the primitive psychic defence mechanisms re-activated in response. The experience of having one’s more mature capacities to cope overwhelmed by something that simultaneously reawakens one’s earliest worst fears (helplessness, death, annihilation, attack) has been conceptualized by Garland (2002) as the defining features of a trauma. Subsequent themes track the development over time of more organized unconscious social defences, before the lasting impact reported by participants is explored. Under each theme, we introduce concepts from object relations theory as they emerged from the data. The case vignette in Figure 2 demonstrates how our themes came together in a moment of overwhelm for a participant, greater than the sum of its individual parts; this will be discussed further toward the end of the Findings section. Case Vignette illustrating intersection of themes.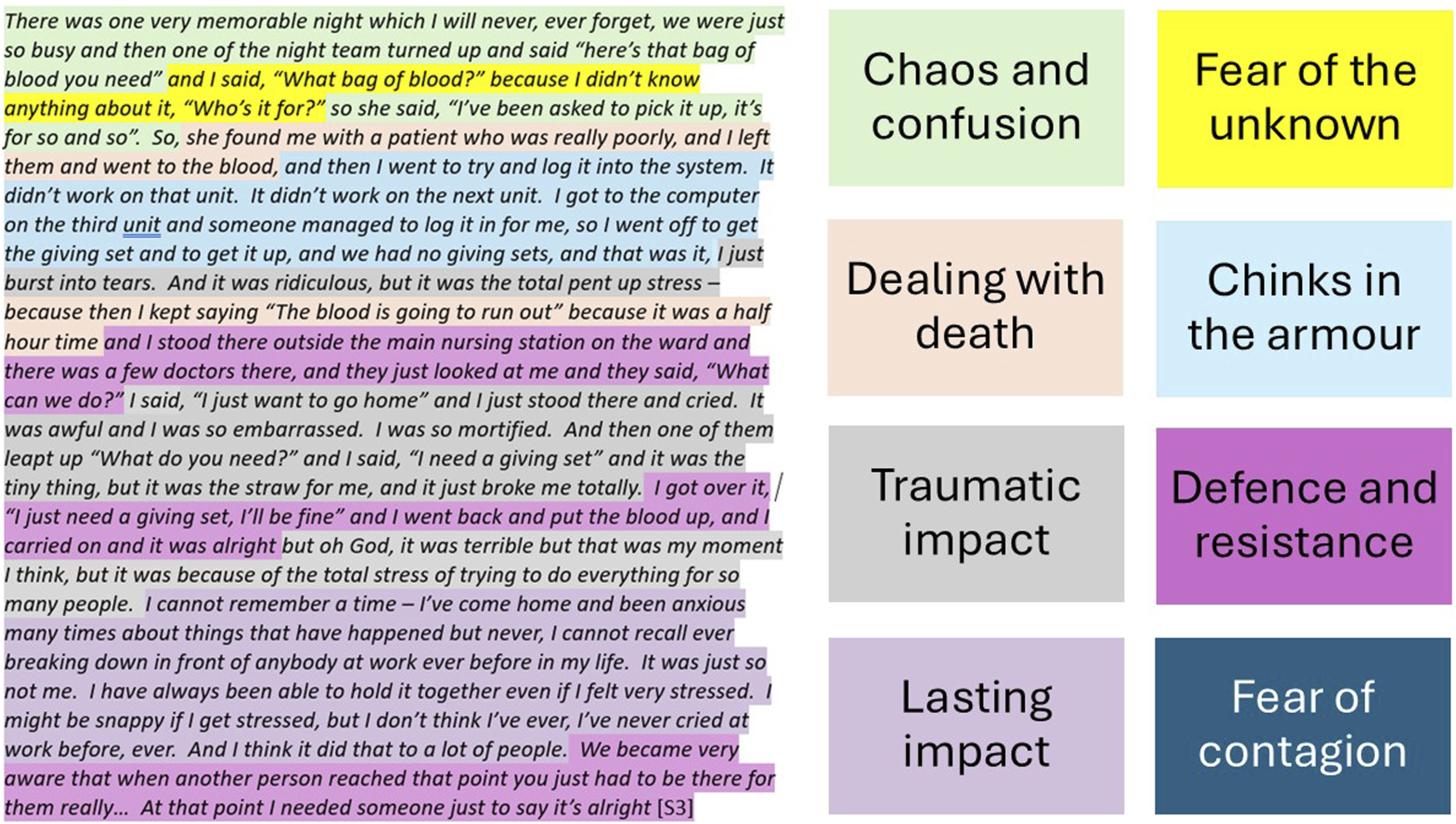
Fear of the Unknown
In an unprecedented situation with little in the way of guidance or protocols, the COVID wards were an ad-hoc solution born out of necessity. Participants described chaos and confusion as new teams were assembled, infection control guidance frequently changed, the media predicted overwhelm of the NHS by the “mystery virus,” and an atmosphere of fear predominated. There were a significant number of seriously unwell patients: It was completely overwhelming at the beginning … every single [patient] was so ill—[usually] you might get one or two that go off, but you don’t get everybody going off on the shift, do you? Thank God. But for these patients, there were none that you thought “they’ll be alright, so we’ll come back.” Everything was hit and miss, and nobody really knew which way it was going. (Theresa, Nursing)
Theresa felt an “overwhelming fear of gosh what will we find, and can we cope?” on hearing that the COVID ward was to be opened; Rebecca (AHP) described “walking into the unknown” on her first shift. Quotes demonstrate how something of the danger situations experienced in infancy was echoed in the circumstance (Klein, 1959), awakening primitive fears of being overwhelmed and left helpless (Garland, 2002; Klein, 1946).
Rebecca (AHP) described how she felt the presence of COVID … It was almost like walking into a veil … we didn’t know what we were dealing with. My first reaction was to open all the windows to let the air circulate. I was thinking, this is crazy, get the windows open.
“Walking into a veil” evoked the presence of COVID, hanging in the air, felt but not seen, a shadowy hostile force that clung. Staff on the front line were fighting an enemy both unknown and unseen.
Fear of Contagion
The “veil of COVID” caused significant fear of contagion and transmission: “Everybody was scared … they didn’t know if they were going to be safe [or] if they were going to get COVID or if they were going to go home with it on them …” (Dawn, Nursing). Alan (Medical) observed HCWs’ reluctance to spend time with patients to support them to eat and drink: “I think they were terrified to do that.” This led to conflict between staff, some feeling forced to shoulder an increased workload, exacerbating the fear and unrest on the ward. Some participants worried about becoming ill with COVID, or dying themselves; others feared taking it home to their dependents. For example, Colette (Nursing) described being paranoid that you’re going to get it all the time. I wouldn’t go near me dad … it was being transported on paper, then it was cardboard, then it was your shoes. I became a little bit obsessed.
Returning to Klein (1946), we see that hidden fears of annihilation were stirred up, becoming the primary concern. This led to the use of defences such as splitting, avoidance, and projecting aggression onto others to maintain both physical and psychological survival, as reflected in the conflict over fair workload distribution.
Dawn (Nursing) described an additional fear, evocative of being a “Typhoid Mary,” the infamous disease spreader: “We used to say, ‘everybody I’m looking after is getting COVID, is it me? I’ve got no symptoms.’” The other side of fear of annihilation, activated when traumatic experience collapses our capacity to contain our worst fears, is fear of our own destructiveness (Klein, 1946). In moments of overwhelming stress, capacity to symbolize, that is, to distinguish between fear and reality of the situation—it’s “as if” I am COVID/death versus “I am COVID/death”—can be damaged (Garland, 2002). HCWs rely on symbolic functioning to master the anxiety inherent in their work (Menzies-Lyth, 1988), particularly tolerance of feelings of guilt (Di Ceglie, 2001). Temporary collapse of this function exacerbated the traumatic quality of the experience, as staff experienced themselves as a danger to patients.
Chink in the Armor
HCWs are supported to tolerate anxieties, limiting reliance on primitive defences, through availability of guidelines, protocols, and equipment required to perform tasks effectively. Such resources produce a different kind of protective skin or “container,” protecting the individual’s psychic skin from unmanageable attacks (Foster, 2009). Fear of contagion may have been better contained if staff felt protected from COVID; instead, difficulties regarding PPE increased anxiety levels. Participants described ever-changing PPE guidelines: Rules were changing about PPE nearly every single day, one minute the full gowns and then the next day people were like, “Oh you don’t have to wear that now,” and it’s like, What’s happened in 12 hours? to say that you’re not allowed to wear gowns? and it turns out that it’s because we were low on stock, well that’s not good is it? (Sue, Nursing)
Uncertain environments can be experienced as persecutory, exacerbating anxieties of disorganization, disintegration, and/or death (Lawrence, 1995). Participants also described the inferior quality of the PPE: Supposedly full-length gowns … if you stretch your arm out, it rips … PPE was a shambles … and that business of pulling out masks with an expiry date three years ago, that didn’t go down well. (Alan, Medical)
Freud (1926) described the mind as enveloped by a kind of skin, a protective shield constituted of our coping skills and resilience which filters and limits that which gets through, both externally and internally. The word trauma, from the Greek for “wound,” denotes a piercing to one’s “psychic skin” through which frightening and potentially dangerous objects can flow in and out, as demonstrated in Alan’s account of PPE ripping. An actual chink in his armor is created, also representing a psychic wound in terms of failure of the reliable protection that is meant to have been afforded. Fear of contamination is made concrete as the anxiety and that which symbolizes it can no longer be differentiated (Segal, 1957). This situation regarding PPE was incredibly distressing to staff “on the frontline” who were experiencing public expectation to be an “NHS Hero” whilst feeling unprotected, uncared for, and almost disposable.
Dealing With Death
Participants identified encountering the death and dying of others at unprecedented levels as traumatic. Unpredictable disease progression was challenging; patients deteriorated and died very quickly: “This chap, we’d washed him and five minutes later he’d died. And nobody was there with him. And those things, they’re not right, in my mind. So, I found all of that very, very difficult” (Lisa, Nursing). Deaths which participants found particularly traumatic were those where they felt patients had been neglected, leading to feelings of moral injury: People were dying and we weren’t able to get to them, and you never forget that. You can’t forget that. It’s a hideous feeling because you knew when you were leaving somebody who was very ill that they may not still be alive when you got back to them … it went against everything we’ve ever been able to do in our careers … that doesn’t go away and it doesn’t get any less really, that terrible guilt feeling. (Theresa, Nursing)
Guilt around failure to provide patients with a “good death” was prevalent across participants’ accounts, particularly relating to patients who died alone. The traumatic nature of this comes through from Alan’s (Medical) difficulty with describing the experience: “There were some really sad things—I mean, we put—It put people in—things that were really, you know—People dying without their families there. People were dying on their own.” Encountering unprecedented levels of death appeared to lead to fracturing of the internal container built through professional training and experience to manage the distress associated with being close to death. Impotency to intervene left a long shadow of lingering guilt, even though nothing could have been done. Self-blame protects against a worse existential horror of realizing you were actually completely helpless in the situation, and so could be again, as it implies that through working on yourself, you can prevent the situation recurring (Levy & Young, 2012).
Nicole (Medical) provided a different perspective, describing medical treatment as going “too far” at times: “if they had just been on a normal medical ward and had a really bad pneumonia or something we would have stopped a lot earlier, but because it was COVID we were like, ‘We’ve got to keep going.’” This was perhaps inevitable in a situation where the battle against COVID was a victory to be won at any cost, a response to the expectation that the NHS would “save us all,” an understandable drive to reduce the number of deaths, or an omnipotent defence against the overwhelming anxiety of helplessness in the face of an unrelenting death toll.
Traumatic Impact
Participants experienced symptoms characteristic of those encountered post-trauma. For example, Lisa (Nursing) described feeling ill and anxious every time she went onto the ward: “putting your scrubs on and not knowing what you were going to encounter.” Sue (Nursing) found it difficult to put the experience into words: “honestly I don’t know how I felt … one word to explain it all was just surreal, and I feel like it’s still surreal now.” Several participants’ sleep was disrupted, as Rebecca (AHP) noted: “People were having disturbed sleep, in the form of, like, nightmares, or just very vivid dreams. And I absolutely experienced that.”
Rebecca (AHP) also described seeing a nurse “sat on a chair with her head in her hands and looking completely just exhausted. She was close to tears and I thought, oh my goodness. I found that very, very overwhelming, to see the emotion of that nurse.” From a medical perspective, Nicole described “watching these people who couldn’t really breathe and you didn’t really know what to do, like, ‘What’s this crazy thing?’, which added to the stress and made you feel down.” Being impotent to cure patients also re-enforced the anxiety-provoking truth that death is ultimately unpreventable.
When trauma pierces our “psychic skin,” we feel vulnerable to overwhelm by external stimulus, but also by internal worries and vulnerabilities, which the “psychic skin” was holding in check. The mind floods with stimulation far greater than it can make sense of; past and present, inside and outside, me and not-me can all become confused and blurred, to the extent we feel as if we are going mad (Garland, 2002). Over time, more adaptive or social defences (Menzies-Lyth, 1988) emerged to replace the initial, raw response to the situation, elucidated in the following themes.
Individual Social Defences—Finding Meaning
Mucking In
Staff valued feeling needed, for example, Rebecca (AHP): You really just did have to help out where it was needed … there was a lot of pulling together and that was a nice experience … feeling that you had a role to play and you were helping others.
Nursing staff derived pleasure from providing basic nursing care, which was hard work but rewarding; Andrea (Nursing) described it as an “old fashioned” kind of nursing. Staff bonded quickly, supporting each other, pulling together, and having each other’s backs. There was a sense of camaraderie across nursing, AHP, and medical teams, where “everybody did muck in together” (Lisa, Nursing), all working “like trojans” (Theresa, Nursing). Finding meaning proved a more adaptive defence against feeling powerless, overwhelmed, and impotent than the primitive defences initially employed.
Family Intermediaries
Staff found it difficult that patients were separated from their families. They described challenging phone calls with relatives: It was very tough when relatives were so emotional over the phone, it was like they were putting a bit of that into you and you were then going and being with the patient whilst they were passing and you were thinking, oh god, I know how upset so and so’s daughter is. (Dawn, Nursing)
Sue (Nursing) described the emotional impact of assisting a patient to call his family: “His daughter was on the phone on loudspeaker and I didn’t expect her to start saying her last words to him, and it absolutely broke me … and then when I was going home I just burst into tears.” Dying patients separated from relatives left a lasting impression: Some people were dying alone, and I found that really, really difficult. Because you put yourselves in the position, don’t you? Of the relatives and the person that’s poorly. And I think that was extremely traumatic … that will always be something that I think about. (Lisa, Nursing)
Participants described how the situation affected the care they provided; one recalled “treating them like they were my grandpa or grandma” (Dawn, Nursing). Another described “how much we are involved not just in providing therapy but from being that person, that patient’s relative, friend” (Andy, AHP). This role intensified the emotional impact of the work, but also increased feelings of being needed, adding meaning to otherwise desperate and barren work.
Institutional Social Defences
Command and Control
Whilst individual adjustments focused on finding meaning, the data points to implementation of omnipotent unconscious defences (Klein, 1946) at the organizational level. Participants described leadership in terms such as negligence and incompetence; information provided was felt to be opaque, misleading, and lacking in rationale. Participants felt de-personalized, merely resources to be used by the organization; many staff were redeployed to the COVID ward without consultation: I didn’t really have a choice. I didn’t know whether I was being asked or I was being told … [someone] kicked him under the table, at which point I thought absolutely, you’ve definitely all had this conversation outside the room. (Andrea, Nursing)
From the outset, national defence against the pandemic sought to control chaos and unpredictability through information gathering, reduction of transmission, and development of treatment and vaccination. Governmental response to the crisis was to take a “command-and-control” approach, issuing explicit directions which NHS Trusts were expected to follow; concerns regarding the implementation of this strategy were identified, for example, failure to use communication structures effectively and ensuing difficulties for clinicians (Davies et al., 2020).
Participants expressed derision regarding the command-and-control concept: “You are being commanded to do something you know is wrong. The things they asked us to do were beyond stupid, you know …” (Alan, Medical). Participants felt decisions made were senseless, inconsistent, and ever-changing. They felt cut off from the decision-making process, their knowledge and experience dismissed and devalued by distant leaders. According to Andy (AHP): If they just talked to the people [on] the frontline, they could have come to a better decision … we had to deal with the brunt from the families and patients. Whereas the people who made those decisions made them from a distance so they wasn’t seeing the impact.
Alan highlighted the difference between military and NHS employment: “In the army, if your commanding officer sends you into a situation where you might die, you have to go. That’s what being in the army involves. That is not what being an NHS employee involves.” HCWs are trained to work autonomously and take personal responsibility; the corollary of “command-and-control” is denigration of individual capacities, producing internal conflict. HCWs were placed in a situation of high responsibility yet low autonomy, increasing feelings of moral distress.
Public Social Defences
NHS Heroes
There was significant public support for “frontline” NHS staff, demonstrated through weekly clapping and generous donations: “People were sending in free food, you did feel like you were being supported” (Dawn, Nursing). Whilst food was appreciated, participants were less complimentary regarding the clapping, describing it as derogatory, a publicity stunt, an empty gesture, tedious, and cringeworthy. Several participants felt it was undeserved as they were “just doing their job.” Theresa (Nursing) did appreciate the applause initially: I did go out and clap because I felt a real rallying feel about the first wave. A bit of a wartime spirit, when everybody rallied round, and was patriotic. It just felt like everybody was joining in and feeling the goodwill—it was a boost that people were applauding what we were doing and were grateful for it.
Participants also expressed discomfort with representation of NHS staff as “heroes”: “a man up the road said, ‘I think you’re a hero’ and I said, ‘I’m not a hero’” (Theresa, Nursing). Andrea (Nursing) disagreed: “We were probably heroes at first because we were challenging something we’d never ever done before. The NHS rose to the challenge, the biggest challenge it had probably faced for quite a while.” A nurse interviewed by Davey et al. (2022) described a move to “stop calling NHS workers heroes. Because if you put the title of hero to someone, you stop asking if they’re okay and if they can cope” (p. 7).
Lasting Impact
Participants discussed the lasting emotional impact of the pandemic, several feeling scarred by the experience. Some described emotional responses to mention of COVID, and others experienced lingering guilt. Theresa (Nursing) described a “hideous feeling” of guilt and “filling up” as she recalled her experiences. Participants had vivid, lasting memories; one was experiencing flashbacks. Lisa (Nursing) could still “bring back that feeling of how ill and anxious I felt … it takes no effort, when you talk about it, that feeling is there.” Andrea (Nursing) could “still see some of them, the panic on their faces with those bloody masks.” Participants highlighted a lack of opportunity to process the experience, despite availability of well-being support: We’ve not had a break to just say, “Right how is everyone feeling after that?” … people might need counselling, but we’ve not had the time… we’ve not even had the time to have ward meetings or anything … people are expected to just come back and crack on. (Dawn, Nursing)
The Blood Is Going to Run Out
In order to synthesize the themes presented, a case vignette is provided (Figure 2). This illustrates the cumulative interaction between elements of the experience which produced a profound impact. The participant noted that many staff on the ward had reached a “breaking point” before going on to describe her own. She described a busy, stressful night shift; she was interrupted whilst caring for a seriously unwell patient and asked to administer a blood transfusion to a different patient; she had not been aware this was required. The scene brings together themes from the data analysis including chaos and confusion, the unknown, and dealing with dying patients. Pressure builds for the participant as she makes multiple attempts to find a computer which will enable her to log the blood transfusion, required prior to administration. A further environmental constraint (Chink in the armor) causes the final overwhelm—upon finding no giving set (the tubing required to administer the blood to the patient) was available, she burst into tears and repeated the words “the blood is going to run out.”
The participant’s choice of words at the moment of overwhelm is highly evocative. Symbolically, blood may be viewed as representative of lifeforce or emotional nourishment, vital sustenance, or an extension of the good internal object. In terms of “running out,” the participant was referring to the time interval by which it is safe to administer blood once it has been removed from the fridge. However, as the patient was dependent on the transfusion to stay alive, time was running out for the patient as well as the blood. By being out of the fridge for too long, the blood is in danger of becoming unsafe—resonating with fundamental anxieties of annihilation via contamination or destruction of the good object through neglect or aggression.
Through an object relations conceptualization of trauma, “the blood is going to run out” could be viewed as symbolizing a psychic wound through which something essential is seeping away, a loss of sustaining internal presence. In other words, a recognition - at some level - of our internal container or 'resilience' being breached. We can see how the participant’s significant competence and nursing experience—“I have always been able to hold it together”—are overwhelmed by “the total stress” (Traumatic impact). The participant described a wish for external holding and containment at the moment of overwhelm: “I just want to go home,” and “I needed someone just to say it’s alright.” She then described how her colleagues responded to her need for containment by providing immediate support, and how this became routine practice on the ward: “When another person reached that point you just had to be there for them” (Mucking in).
Discussion
Whilst previous studies highlighted the symptomatic impact on staff of working through the COVID pandemic, through a psychodynamic lens of analysis we have developed a model of the elements which combined to lead to psychological disturbance, the institutional defences that inadvertently compounded the experience, the personal meaning which staff members relied on to survive, and the lasting impact. In relation to our initial aims, this analysis addresses a pre-existing gap in the literature and considers the psychosocial processes underpinning response to the COVID pandemic among HCWs.
Davoine (2022) likened the pandemic to “wartime, when time stops owing to the destruction of symbolic bearings” (p. 30); a doctor she interviewed described their work as “trench warfare… it’s war and it’s not war, we surpass ourselves, we do things we wouldn’t normally do, and we do them over a long period of time” (p. 14). Military terms such as “deployed” and “mobilized” were increasingly used within healthcare during the pandemic (Webster, 2020). A nurse interviewed by Ball et al. (2023) described how “healthcare workers deaths are being treated like soldiers at war, dying doing what they loved, instead of a failing of the public health system to protect us” (p. 347). Those joining the armed forces acknowledge injury and death as a potential occupational hazard; the fact that this is not the case for HCWs was omitted in media representation of the frontline heroes of the NHS. Such idolization through the defence of splitting and projection allows denial of suffering and sacrifice, or the costs of having the NHS available, whilst potentially also providing convenient cover for a state/government who are not protecting their staff—reducing the risk of being held to account by the public.
Themes have been described separately; though as the case vignette illustrates, it was the intersection of all the themes which together produced a traumatic experience. Helplessness was considered by Freud (1926) to be the prototype of the traumatic situation (Nicolò, 2021), linked to the theme of chaos and confusion and echoed in descriptions provided by other HCWs. For example, “there’s been no guidelines, it’s chaos” and “we are literally making it up as we go along” (Horton, 2020, p. 1022). One doctor noted, “we are fragile beings. As long as everything is fine, we feel omnipotent. But one virus is enough to destroy our entire system” (Bohleber & Leuzinger-Bohleber, 2021, p. 132).
Participants experienced the stress of unprecedented circumstances, their worst fears realized as their skills and experience proved inadequate weapons against the onslaught. In relation to fear of contagion, they described “the persecutory feelings caused by an invisible element that generates anxiety” (Nicolò, 2021, p. 209), anxiety regarding contracting COVID and potentially dying, plus the possibility of becoming conduits of COVID. Splitting and projection of aggressive impulses were identified through conflict regarding workload equity and necessity for someone to tend to the contagious. As in other studies, participants described the emotional labor of encountering patient death on an unprecedented scale (Dowrick et al., 2021; Hanna et al., 2021). Overwhelm derived from fracturing of their internal container, built through professional training and experience to manage distress associated with proximity to death. Similarly to our participants, a nurse interviewed by Pilbeam and Snow (2022) said, “that first death where the family weren’t able to be there was probably one I’m never going to forget… I just cried the whole way home that day” (p. 465).
As identified in multiple previous studies, trauma was ubiquitous among HCWs; one doctor wrote: We had to leave the unit. We needed distance from the sticky blood on the floor. We needed not to see …their supplicant posturing still silently begging us to save them. We walked away, shaking and nauseated. It wasn’t a choice. Our bodies knew to rescue us from the scene. (Rudden, 2022, p. 281)
When trauma overwhelms the mind, functioning becomes massively disrupted, resulting in a collapse of routine, of belief in the world's predictability, and of the mental structures and defences which support stability. It leaves the individual vulnerable to intense and overwhelming anxieties from internal sources as well as actual external events. Primitive fears, impulses, and anxieties emerge. Trust in the fundamental goodness of the world itself is shattered—who after all let this terrible event happen? Failed to protect you from it? Worse, might even have wished for or provoked it? (Garland, 2002). What is crucial is the collision of anxieties, where the external event is perceived as confirming the worst of the internal fears and phantasies—in particular the reality and imminence of death, or personal annihilation, through the failure of those good objects (internal and external) to provide protection from the worst. Thus, a trauma is an event which overwhelms existing defences against anxiety (for HCWs, this may be knowledge or competence) in a form which also provides confirmation of those deepest universal anxieties.
Viewing trauma as a psychic wound, we might consider what would escape through the piercing: underlying fears, sense of competency/resilience, ability to cope. We could also consider what would more easily get in: the fears of contamination, media stories of doomsday, and the perceived callousness of managers and organizations. Through difficulties with PPE, an actual chink in one’s armor, fears were made concrete. As the case vignette demonstrates, “the suffering that derives from these traumas will then be at the center of a crucible formed by the intrapsychic, the interpersonal, and the transpersonal” (Nicolò, 2021, p. 209).
The traumatic experience evoked primitive defence mechanisms, particularly at the start of the pandemic when fear of overwhelm was prevalent. Over time, more mature defences started to emerge; later themes track the development of more organized unconscious social defences. This included sublimation or feeling useful; in a large-scale Welsh study, Pink et al. (2021) found HCWs reported lower levels of distress than the wider population, highlighting the “potential benefits to one’s mental health of playing a crucial societal role during crises” (p. 789). A former Military nurse working on a COVID ward “witnessed what I can only describe as a military-type mentality amongst the staff… They were all pulling together, making their contribution for the greater good and feeling empowered for having done so” (Dyson & Lamb, 2022, p. 82). Straker (2021) linked feeling like a valued member of society with symbolic immortality and reduction in anxiety; feeling part of something greater than ourselves brings meaning and permanence, reducing death anxiety. Supporting patients in the absence of family members was one such way to make a difference, as also identified in studies conducted by Hanna et al. (2021) and Dowrick et al. (2021), where a nurse described being their patients’ “only point of contact with the human world… you’re like an extended family member to them” (p. 2168).
Mitigating the impact of perceived powerlessness, the state and organization adopted a command-and-control position, akin to what Klein (1946) called “manic” defences against helplessness, exacerbating the traumatic situation of staff members. As Atkinson et al. (2020) described, the responsibility typically devolved to the NHS itself “was replaced by a ‘wartime’ model in which control was centralised in government” (p. 4), leading to central and local tensions. An NHS worker quoted by Horton (2020) stated, “rigid command structures make decision making impossible” (p. 1022); participants in this study felt resentful, dismissed, and devalued. Doctors interviewed by Jabbar and Marshall (2023) also described changes of guidance exacerbating uncertainty. When staff experience disintegrating effects of trauma, a “command-and-control” approach would potentially create a containing structure to mitigate against anxiety. However, for this to be effective, a high level of trust must be placed in those giving the commands. Participants in fact experienced increased anxiety as they did not feel listened to or acknowledged by those in control, adding to the powerlessness and threats to identify/ego they were already experiencing. Similarly, a nurse interviewed by Abrams et al. (2023) stated, “we weren’t asked. We were told… I didn’t volunteer. I haven’t fallen on this sword” (p. 2193).
Consciously and unconsciously, for the public, the NHS was the first line of defence against the pandemic. “Clapping for carers” highlighted societal strength of feeling; this might be viewed as a quasi-religious/magical “ritual” in support of the service which would “save us all.” Moore (2020) highlighted the strong psychosocial attachment developed by the British public toward the NHS. Osserman and Lê (2020) described societal transference toward the NHS as a supportive parent; as an institution, it serves as a container for anxiety around suffering, illness, and death (Hoggett, 2006). Obholzer describes how the health service “might be more accurately called a ‘keep-death-at-bay’ service” as it serves as a societal defence against death anxiety (1994, p. 171). Whilst participants were skeptical regarding the ritualized clapping, they did appreciate the voluminous donation of food to the hospital, sacrificial offerings, or sustenance for the troops; an army marches on its stomach, after all.
One qualitative interview study of nurses’ experiences was titled “Thank you for helping me remember a nightmare I wanted to forget” (Pilbeam & Snow, 2022). Our participants described the lasting impact of COVID in a variety of ways, such as the feelings evoked by television coverage of COVID or mention of the pandemic in conversation. No participants in this study found it helpful to engage with health and well-being initiatives. Positivity-focused initiatives had the unintended consequence of implying to staff that something was wrong with them for having a negative emotional response to the pandemic. Other studies reported different experiences of interventions allowing for expression and processing of negative experiences and emotions; for example, group therapy facilitated processing of the experience including mourning, acceptance, and healing (Rudden, 2022). In a study of 6120 HCWs, increased resilience was linked to positive perception of the organization’s understanding of emotional support needs, positive perception of leadership support, and a higher level of psychological safety (Munn et al., 2021).
One aim of our study was to consider the need for ongoing care and support of the work force, both for future pandemics and during periods of seasonal pressure. According to Anzieu (1993), the psychic wounding of trauma may be reduced “if someone can be found as quickly as possible to function, both by the words they speak and the attention they give, as an auxiliary or substitute skin ego (or envelope) for the [psychologically] injured person” (p. 140). Here, Anzieu is describing emotional containment, taking-in of the full horror of the experience, digesting it, and giving it back in a form which helps the wounded person feel seen and held (Bion, 1962). It is apparent from participant accounts that staff played this role for each other, whilst the organization itself did not. A well-run organization can serve as a powerful container of distress, though anxiety and inability to tolerate painful feelings impair this capacity for containment (Lucey, 2022; 1967). Bion describes how anxiety which is not contained is re-introjected in the form of “nameless dread” with the individual feeling on the edge of catastrophe (1962, 1967), as described by participants.
To recover from a traumatic experience, events must be worked through rather than walled-up, the personal meaning for the individual identified, so they can make sense of and think about their response; recovery from trauma can be seen as the capacity to “get on with it” rather than to “get over it” (Garland, 2002). Castrillón and Marchevsky note that “proceeding as ‘normal’… is full-on death. We must… name the losses we have incurred, mourn them, and work to… re-inhabit those spaces forbidden to us by the infectious logic of the virus” (2021, p. 8). Though our study participants had access to well-being services, there was no encouragement to access these. Nurses interviewed by Davey et al. (2022) similarly identified limited opportunity to process the experience; they were not encouraged to take advantage of well-being services or offered time away from their work to do so.
Traumatic events change us; survivors will never be the same again. The question is “whether in the end the survivor will be less of a person than before, a more disturbed person, or… more of a person, the disaster becoming a focus for growth” (Garland, 2002, p. 6). Given the limited opportunity for growth offered to so many HCWs who worked through COVID, significant levels of trauma have been buried and defended against. If required to work through a future pandemic, such staff members are likely to become overwhelmed incredibly quickly and will require a great deal of support.
The ability to “think about” the meaning and implications of one’s experiences, practices, or policies is central to surmounting overwhelming and unprecedented situations, whilst limiting the risk of sustained and lasting psychic and moral injury to the workforce and those it cares for. Responding to Baraitser and Salisbury’s (2020) call to pay detailed attention to conditions that prompt action and can close down thinking, this study has produced implications for how staff can be supported to sustain their capacity to think while “under fire” (Bion, 1962), if employing managers, organizations, and governmental departments recognize the possibilities that come from containing the unbearable anxiety that such conditions inevitably produce. That is: (1) To really register and think about the unavoidable impact upon staff, rather than to deny, or minimize it through employment of dehumanizing conceptualization of them as “super-human” heroes and (2) To use the insights that come from engagement with the realities, to develop support strategies that discourage coping based on “soldiering” and privilege spaces for staff to recognize, work though, and mourn their experiences, promoting growth of a more realistic, sustainable, and flexible type of resilience that can be drawn on in future situations.
Conclusion
Previous studies have highlighted the individual symptomatic impact on staff, such as anxiety, stress, and PTSD. Using a psychodynamic lens of analysis has enabled us to develop a model of the specific elements which came together to lead to psychological disturbance and traumatic stress for the staff; the institutional defences that inadvertently compounded the experience as traumatic for staff; the personal meaning derived from the experience, which staff members relied on to survive; and the lasting impact: “people are expected to just come back and crack on” without an opportunity to process the experience, feeling scarred, with vivid memories and lingering guilt.
One limitation of the study may be that the interviews were conducted at one hospital site with a small number of staff. Whilst we can make no claims to generalizability, the in-depth perspectives and transferability of this new knowledge are significant. Further, as highlighted in the Discussion section, participant accounts resonated on multiple levels with those of staff interviewed in other qualitative studies. We add to the evidence base around staff experience of COVID, highlighting the profound and enduring impact on staff and demonstrating the value of psychoanalytic research methodology. Rather than simply demonstrating that working through the COVID pandemic was disturbing to staff’s mental health, we illuminate why and how this disturbance occurred. This deeper exploration enables suggestions to be made for promotion of staff well-being in general and particularly in the case of a future pandemic. We have identified how the failure of both internal and external containment combined to exacerbate traumatic experiences. Consideration of quantitative evidence regarding levels of burnout and PTSD, along with NHS staff turnover rates and participant accounts, leads us to conclude that some staff now experience the NHS as not a good-enough employer/mother/container; it cannot be relied on to support or protect them, which has undoubtedly impacted staff well-being and workforce retention.
The authors hope they have achieved their aim of bearing witness to the participants’ experience and ensuring memories endure. To counter the potential for repetition, we provide a basis for the development of strategies for care, both for the workforce who have survived this traumatic experience and those working through a future pandemic.
Footnotes
Ethical Considerations
All participants provided written informed consent, and the study was subject to full UK Health Research Authority ethical clearance (HRA, Wales Research Ethics Committee, REC reference 20/NE/0188). The study was carried out in accordance with the ethical guidelines of Manchester University.
Author Contributions
SR conceived and designed the study, collected data, performed analysis, and wrote the paper. HH designed the study, collected data, and contributed to writing of the paper. CF provided supervisory support, performed analysis, and wrote the paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Manchester University Foundation Trust (MFT) Charity and the Houghton Dunn Charitable Trust. MFT WTWA Complex Heath Directorate provided funding for transcription of interviews. The funding body had no involvement in the design of the study, the collection, analysis, and interpretation of data or in writing the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.