
Abstract
Patients on dialysis develop unique relationships with their providers, fellow patients, and the broader healthcare system. This network of relationships is a well-established key factor influencing both their healthcare experience and mortality rates. Yet, despite ongoing efforts to improve these networks of relationships, health outcomes remain unfavorable for dialysis patients. Investigating the formation of these relationships through a social media platform provides valuable insight into patients lived experiences, shedding light on pervasive power dynamics as seen from the patient perspective while addressing methodological gaps present in the literature. Analyzing social media platforms helps identify critical areas for improvement that may have been overlooked to enhance the experience and outcomes of patients on dialysis. In this paper, we use Foucauldian discourse analysis to examine 41 posts and their associated comments from the r/dialysis forum on Reddit, focusing on the first year of dialysis initiation and exploring how societal discourse shapes and is shaped by peer-to-peer interactions, impressions, communities, and frameworks. In this study, we highlight how power and resistance are reflected in the discursive choices made by patients, as well as its influence on their conceptualizations of the patient–provider relationship as they begin their dialysis journey. These insights add to the dearth of current literature that use social media platforms and discourse analysis in investigating healthcare experiences. They lay the groundwork for better supporting a vulnerable clinical population and provide a foundation for future academic research using this methodology.
Introduction
The patient–provider relationship is fundamental to quality healthcare (Hreńczuk, 2021; Kohatsu et al., 2025; Shay & Lafata, 2015), which is particularly true for patients with chronic disease, who are profoundly impacted by their interactions with nurses and physicians. Clinicians have leveraged this knowledge across various populations to support patients throughout their healthcare journey. Renal patients, for example, experience heightened vulnerability during dialysis initiation as they adjust to a strict new lifestyle (Wachterman et al., 2019), prompting the development of Transitional Care Units to facilitate their adaptation (Bowman, 2019). This transition is pivotal to the course of their clinical journey as patients begin to shape not only their sense of identity but also their perceptions of the providers, peers, and healthcare system they will engage with over time.
Research on supporting this transition for dialysis patients has expanded rapidly as the concept of patient empowerment gains increasing recognition. This empowerment involves “shift[ing]… the balance of power and can be seen as both a process and a state of being” (Hickmann et al., 2022, p. 4). Researchers have thus far focused on the importance of shared decision-making, with the majority relying on interviews as their primary method of data collection (Sedin et al., 2023). Insights from other methodologies may be overlooked, as reflected in the persistently high dissatisfaction of care in the population (Bear & Stockie, 2014; Kuo et al., 2024; Song et al., 2013) and lack of meaningful documented change (Attalla et al., 2020). This study contributes to the dearth of literature by approaching these issues from a different perspective: specifically by analyzing a dataset from the r/dialysis forum on Reddit and applying discourse analysis to examine posts and comments shared by dialysis patients on a public platform. Examining the broader societal discourse embedded in these patients’ posts can help us learn how providers in the healthcare system can better support patients on hemodialysis as they begin their journey.
Using social media datasets presents unique methodological considerations. Retrospective bias and social desirability effects are influenced by the online and often anonymous nature of these platforms. Users exercise significant autonomy over what, when, and where they choose to share, leading to highly curated narratives shaped by both individual self-presentation and the moderation practices of the communities they engage with. While anyone with access to the internet can read the public posts, those who actively engage in the forums form an audience sharing specific needs. The presence of “upvoting,” peer judgment, and platform norms can contribute to the development of “echo chambers,” influencing the tone and content of both posts and comments (Cinelli et al., 2021; Dosono et al., 2017; Gaudette et al., 2021). The authenticity of the narratives and claims by each post is difficult to verify. Despite these limitations, social media data offer valuable, relatively “real-time” insights, particularly when users post shortly after their experiences, and provide a window into interactions and narratives that occur outside of formal institutional contexts.
In this Foucauldian discourse analysis (FDA), we explore the following research question: How do patients receiving hemodialysis understand their relationships with healthcare providers, as reflected on the r/dialysis subreddit?
Background
Patient–Provider Relationships in the Hemodialysis Population
The relationship between patients and providers, identified in this study as nurses and physicians, is dynamic and often complex. Patients on hemodialysis rely on their providers to deliver life-sustaining treatment, in addition to essential education on managing their disease in the community (Stavropoulou et al., 2017). Providers can play a vital role in supporting patients to build their capacity for self-management, centered conceptually on the ability to retain a sense of normalcy in their daily lives (Curtin et al., 2005). By leading their lives independently outside the hospital, patients report feeling more satisfied, more empowered, and more capable of participating in their own care (Angwenyi et al., 2019; Carlin et al., 2012; Fox & Chesla, 2008; Harvey et al., 2008). A positive patient–provider relationship can therefore influence healthcare trajectories and encourage patients to exercise control, where possible, in their lives.
Establishing trust during the initial stages of dialysis can be crucial in encouraging compliance to treatment (Krot & Sousa, 2017; Sihvonen et al., 1989) and an openness to share concerns with their providers (Chandra et al., 2018; Salt et al., 2012). Researchers show that first impressions have significant impacts on a relationship, even years after they are formed (Rimondini et al., 2019). Change in relationship dynamics is possible, but often slow, and requires focused intention (Cone et al., 2017). Hence, patient perceptions of their provider created in this stage of their journey are vitally important to their consequent trajectory. Studies show that these perceptions are influenced by multiple factors; and while many are related directly to providers, others are gained through shared experiences and frameworks endorsed by peers (Ziebland & Wyke, 2012).
Patient Forums in Dialysis
While patients’ empowerment and knowledge were traditionally gained through providers and the healthcare system, use of the internet has shifted these dynamics (Tan & Goonawardene, 2017). Patients now have the ability to not only search for healthcare information independently but also discuss thoughts and emotions globally with others. Social support is known to be a significant factor in the development of self-management capacity (Li et al., 2014). Patients on dialysis traditionally had their social circles limited by location, both due to physical frailty and their need to attend dialysis sessions multiple times a week. The advent of online forums addresses this challenge by providing a platform for sharing information, experiences, and emotional support. These forums can offer a supportive space for patients and their families to ask questions and express emotions that might otherwise go unnoticed by providers (Ahmed et al., 2017).
Beyond the connections that form between peers, reading and sharing in others’ experiences can influence a user’s understanding of the interactions with care providers and help them navigate a difficult time (Ziebland & Wyke, 2012). Peer dialogue can assist in sense-making as the patient transitions into a new lifestyle (Ziebland & Wyke, 2012). Patient forums can therefore provide a unique snapshot of peer interaction and emotions in relatively “real time” as patients choose to share their stories shortly after their medical experiences, and often throughout their year-long transition period.
Methodology
In this study, we collect data from the r/dialysis subreddit (https://www.reddit.com/r/dialysis), a forum dedicated to supporting dialysis patients and their caregivers throughout their renal journey. A machine-learning tool named Teleoscope was used to select relevant posts by patients on hemodialysis posting within the first year of initiation. An FDA was then applied with a focus on patient–provider relationships.
Teleoscope and the Dataset
Teleoscope is described as “an interactive web-based system for exploring large datasets (100K-1M) of short documents such as social media posts” (Bucci et al., 2024, p. 2). Created by Paul Bucci, it aims to assist qualitative researchers in exploring relevant data from a large dataset through the evolution of document similarity. Machine learning is used to refine the system’s schema based on the documents identified as appropriate, and the tool will suggest increasingly relevant data accordingly (Bucci et al., 2024).
Search Terms Used in the Selection of Posts From the r/dialysis Forum Through Teleoscope
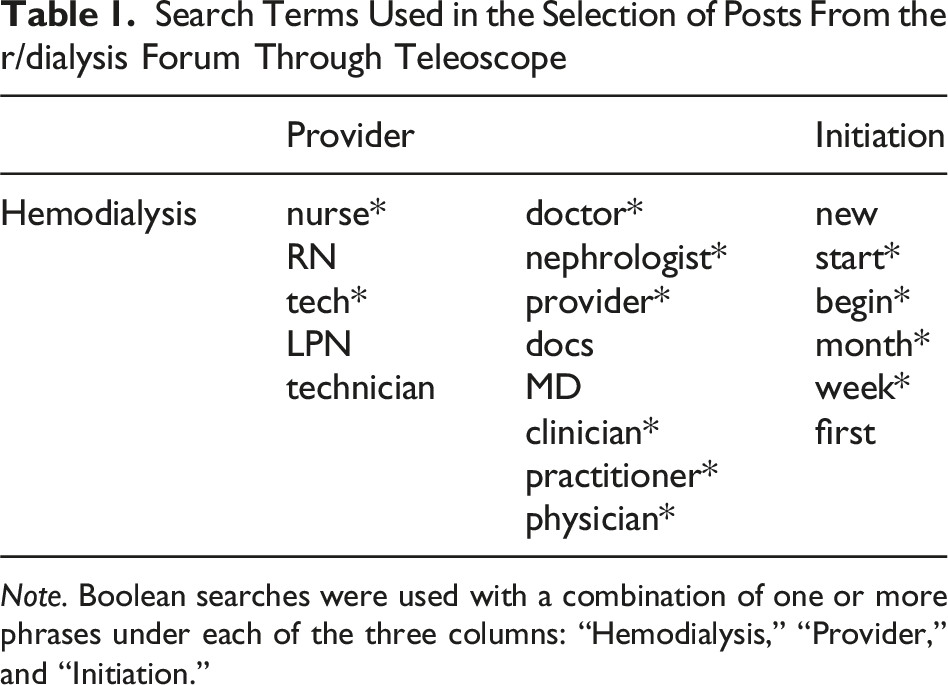
Note. Boolean searches were used with a combination of one or more phrases under each of the three columns: “Hemodialysis,” “Provider,” and “Initiation.”
Foucauldian Discourse Analysis
Foucauldian discourse analysis has its foundations in Foucault’s theory of power, which emphasizes the pervasiveness of power in society and its interconnectedness with knowledge and discourse. It positions discourse as a productive phenomenon that reinforces the form and nature of knowledge through interactions between individuals (Foucault, 1972). Social realities are constructed when knowledge is reiterated over time and normalized, ultimately creating a dominant discourse for the particular era (Foucault, 1980). In this process, certain knowledge is made visible and internalized while others are discursively excluded. Discourses of truth are produced in this way through mechanisms of power embedded in and exercised through institutions (Foucault, 1972). Power and knowledge are thus reciprocal and fundamentally intertwined and made most visible at an interactional micro-level on the fringes of society (Foucault, 2020).
Implementing FDA can be a challenge due to the lack of analytic guidance offered by Foucault (Ong et al., 2024). This has led to the varied application of the methodology in modern literature (Hook, 2001), with all research arguably using a “Foucauldian-inspired” approach. After considerable investigation into prior approaches to FDA, the current study uses a framework modeled after a study by Ahl (2007), combined with guiding principles set by Arribas-Ayllon and Walkerdine (2017). Ahl (2007) details the core principles of FDA and creates multiple smaller objectives under an overarching research question to help guide analysis. Principles include reversal, discontinuity, specificity, and exteriority, which are used to ensure that both the “said” and “unsaid” are examined appropriately. Objectives are created in an iterative manner as data are collected and reviewed. Arribas-Ayllon and Walkerdine (2017) approach their analysis by first selecting a corpus of statements, before assessing its formation, problematizing the text, and considering technologies of power and self that assert influence on the discursive object. Their process highlights the need for technologies in driving the researcher’s frame of reference.
In this study, five guiding objectives were iteratively formulated throughout the data collection phase: • What assumptions are made about providers and healthcare institutions in these texts? • In what ways do institutionalized practices influence how narratives are shared? • How are discourses co-produced by dialogue between posts and their comments? Who is allowed to speak, and what is allowed to be spoken? • What is implied in the ways users of r/dialysis refer to their healthcare team? • How is power displayed and discussed in the posts shared on r/dialysis?
Given the nature of FDA, research findings were discussed among all authors throughout the collection and analysis process. A journal was kept by the first author for reflexivity as well as transparency in decision-making.
This study was exempted by the Human Research Ethics Board at the University of Victoria, as Reddit posts are considered public data. However, the ethics of using social media as datasets has been an increasing concern in academic circles (Fiesler et al., 2024; Golder et al., 2017; Hunter et al., 2018; Moreno et al., 2013; Norman Adams, 2024; Stommel & Rijk, 2021; Webb et al., 2017); hence, ethical concerns that could arise were thoroughly discussed prior to the study. Topics of discussion among the research team included implied consent, autonomy over posts, patient vulnerability, anonymity, contextual importance, and the risk versus reward of conducting this study. To mitigate the potential harm to users on the forum, particular attention was placed on the context of each post and annotations attached accordingly throughout analysis. Furthermore, all quotes used in this article are paraphrased to maintain anonymity, and researcher triangulation was leveraged to ensure meaning is preserved for academic integrity.
Findings
This study generated valuable insights, driven by the five objectives. The findings were organized into three discursive categories: The “Good” Patient and Peer, Positions of “Us” and “Them,” and Empowerment in Medicalization. In this paper, we explore the findings that both align with the identified research topic and hold potential to inspire meaningful change. While we acknowledge the presence of other discourses in the data, they are not discussed here.
In the analysis, we pay particular attention to the technologies of self and power that are present within the three discursive categories and reflective of the ways in which technology shapes discourses. Foucault defines “technologies” as the methods and techniques humans use to interpret and control both themselves and others. He identifies four types: production, sign systems, power, and self (Foucault, 2005). While these technologies are distinct, they rarely function in isolation, instead operating through ongoing and interconnected interaction. Technologies of self explore the tools used by humans to define and produce an ethical self-understanding, and the practices by which individuals can influence their way of being to attain certain states of “happiness, purity, wisdom, perfection, or immortality” (Foucault, 2005, p. 18). Technologies of power have an external focus and operate from a higher-level perspective. Power is exerted through these technologies to shape the subject’s conduct and objectify them. In our study, two technologies of power play significant roles in the shaping of patient experiences: disciplinary power and biopower. Disciplinary power is asserted through regulation and constant observation to create “docile bodies.” A classic example is Foucault’s panopticon, where the structure itself is the technology that channels the disciplinary power of surveillance (Gane, 2012). Biopower refers to the regulation asserted on a population to subjugate and control “life,” for example, public health policies on vaccines or birth control regulations. Many mechanisms are so intertwined that they can arguably be varied forms of the same—for example, technologies of self may ultimately be a form of internalized disciplinary power, while biopower may be enacted through forms of disciplinary and sovereign power. Regardless, the mechanisms of power pervasive to the healthcare system have been studied extensively in the literature, often driven by the need for equity and improved patient outcomes for vulnerable populations (Mattioni et al., 2021).
The “Good” Patient and Peer
Being a “good” patient and peer is a fundamental driving force for many new dialysis patients, as it allows them to be accepted into the new social circles that come with their new lifestyle. What constitutes as “good” is discursively determined by their communities and the societal discourses they are situated in. Many posts by patients in their first year of hemodialysis began with an introduction, typically including details such as age and gender. These introductions were frequently accompanied by a statement of how long they had been undergoing hemodialysis, with some expressing lack of familiarity and identifying as new to the process. As one user stated, “I’ve not been long in the saddle yet.” Similarly, certain comments by more “veteran” patients responding to these posts would explicitly identify themselves as having years of experience being a patient on hemodialysis.
Positioning themselves in subject positions of “novice” and “veteran” patients afforded each party certain privileges within the forum: for example, the novice patient could request for help and ask questions without being judged on their lack of knowledge by their peers, and display vulnerability as others empathized with the challenges of dialysis initiation. For some patients, it may also allow them to defer power to others with expertise when they feel unsure about how to proceed. This positioning is highlighted as new users chose to present themselves as friendly and inviting, often sharing their stories with notable use of emojis, gratitude, and humor. In one post, gratitude was emphasized with a heart emoji when a user thanked responses to their story “in advance,” while humor is seen when another user stated his “fat butt” was the reason for a prolonged stay in the hospital, accompanied by an eye-roll emoji. Even in the occasional instance when the user presented as emotional or upset, their positioning as a novice patient afforded them the grace of patience and understanding from the more veteran patients who had shared similar frustrations in the past. These posts did not use emojis and instead used punctuation to portray their urgency. One patient, for example, used multiple question marks when asking if they were the only patient experiencing a certain symptom, while another wondered if being dead was “any worse than [life on dialysis]???”. The subject positioning as a new patient provided them the space to express their emotions in a “safer” way that is met with sympathy. This can be interpreted as a form of power, allowing access to the knowledge and support held with their veteran peers.
On the other hand, the veteran patient position is empowered by the respect of their newer peers and granted a voice of authority on dialysis-related topics. Experience is equated to knowledge, a fundamental assumption of the “lay expertise” discourse that encourages patient voices and values the lived experiences. This activist approach challenges the traditional “book” expertise held by providers in a medical system steeped in biomedical discourse, looking instead to peers as “experts” with accumulated and shared experiences of the illness. Borne out of frustration over being dismissed by their providers, and propagated through the increased visibility of such experiences through the internet, this “lay expertise” supports the patients’ desires for more power in the interactions and decision-making processes related to their treatment and care. This is a form of subjugated knowledge, or forms of knowledge excluded by the dominant discourse (Foucault, 1980), that has, in part, been given space to grow through the use of online forums such as r/dialysis. What it means to be a “good” peer—and, in extension, a “good” patient—is enforced in the forum by positive and negative reinforcement of specific actions. Friendliness is rewarded by support and knowledge in the comments, encouraging new users to contribute in similarly positive ways in the community. Concepts of how a “good” patient should act appeared to be commonly shared across the Reddit posts and reinforced: for example, “doing … what the nurses and doctors want” is framed with pride, while missing appointments is associated with shame. Comments echoed this, as other users respectively praised or criticized the action. Patients would further report doing “everything right” by “cleaning up their diet,” having good blood work, or being patient with new nurses. Not complying with treatment regimens was then labeled as something “stupid” to do. While the novice position allowed them the power to freely seek support, it may have precluded them from resisting against their veteran peers in these notions of “right” and “wrong.” Veteran patients reiterated certain pieces of knowledge to their newer peers, such as advice to always gather information to “make informed decisions” or the need for “[us] dialysis patients [to] stick together.” There was an overwhelming theme of optimism, with shows of support such as “hang in there,” “you got this,” and “it will get better.” This optimistic discourse consequently resulted in the discouraging of other, more negative narratives, and may have buried narratives that otherwise could be shared by newer patients. This “silencing” can be seen as patients starting dialysis would often apologize in their posts for “complaining” or acknowledge that they were feeling the “wrong” way. Sometimes this was illustrated through expressions of regret and justification of posts that shared a pessimistic outlook. For example, one user apologized for their “incoherent rant” and explained that it was due to their fatigue, while another finished a post with “anyway” as a means to shift away from their perceived negativity. Users often expressed feeling temporarily “sorry” for themselves or acknowledging that they “should be” more positive by continually “trying … to not let everything get [them] down.” These acts of self-monitoring are displays of disciplinary power or internalized norms of not only the r/dialysis subreddit but perhaps larger biomedical discourses of “good patients” as a whole. This absence of negativity is just as significant as the overwhelming presence of positivity, suggesting that, conscious or not, patients on the forum may feel unable to share all aspects of their story.
This micro-level community and its participants are ultimately influenced by the greater biomedical societal discourses, and patients on dialysis can hold multiple subject positions that create spaces of tension. Outside of the forum, where they are “novice” and “veteran,” they hold positions of “patient” in relation to providers and lay people not on dialysis. One prominent discourse is the ideal of patients being “fighters” and an expectation of these patients to face their “fights” with endless determination. The use of warfare imagery in relation to disease has been extensively documented, particularly in the field of oncology, and is deeply ingrained in current Western discourse. Military metaphors have appeared in medical contexts for centuries, first entering Western thought in the mid-seventeenth century and becoming dominant in the 1800s (Hansen, 2018). Through this positioning as “fighters” against their enemy of “dialysis,” patients are perceived as “winners” if they continue to persevere and “losers” when they begin to feel doubt and express pessimism. Although initially intended as empowering, such discourses may remove the patient’s ability to seek support for fear of being “beaten” by their disease. The paternalistic biomedical discourses reinforced by Western healthcare institutions intersect with this “fighter” discourse as patient positions demand compliance in exchange for access to care. When viewed through a broader lens, the behaviors promoted by veteran peers as markers of a “good patient” form part of the healthcare system’s exercise of societal biopower, delineating the acceptable limits of patient conduct for those seeking continued access to life-sustaining treatment. Even in the acts of resistance patients have, such as gathering information, they must work within the rules created to receive these institutional privileges.
Positions of “Us” and “Them”
Language is an inseparable part of our daily lives that enables us to communicate ideas in both direct and indirect ways. Linguistic choices made in forum discourse can inform interpretations beyond the stated content, as the deliberate or unconscious use of specific pronouns has been shown to facilitate “othering” through mechanisms of inclusion and exclusion (Alinezhad & Nemati, 2019), while also indicating how speakers position others within their social circles (Yates & Hiles, 2010). The ways in which patients position their healthcare providers may reveal underlying perceptions of power relations, as well as their sense of trust or community.
In the r/dialysis forum, newer patients would refer to their providers as a collective, using “them” or “they” over professional designations. For example, one post reported that “they created a fistula” and “they pricked me,” with no acknowledgement of who “they” are or that the two “they” refer to different people. Another stated that “they are removing the stitches on their central line” but is unclear on who the “they” refers to. At times, it seems that “they” is not a single person but instead the healthcare system as a whole. This anonymous “collective” is positioned in opposition to the patients, who are referred occasionally in posts as “we.” For example, some comments stated that “we are all in the same boat” and that “we dialysis patients” must support each other. Original posters may even respond to these comments using “we” as well, as a user did by saying “thank you … we got this.” By forming a sense of “us” and “them,” and creating divisions between the two groups, trust and loyalty are more rapidly formed which can be vital for patients acutely experiencing transitions and looking for immediate support. These patients then empower themselves by gaining collective knowledge and experience from other patients on the forum.
The linguistic choice of “they” by these patients suggests both distance and anonymity, and perhaps a lack of warmth. This echoes the paternalistic nature of biomedical discourse, where the provider is traditionally seen as the sole decision-maker and patients are the passive “recipients.” New dialysis patients can seek to contribute more fully to these decisions by finding support in peer communities and learning to resist this discourse over time. This desire to seek out power and alternative knowledge is evidenced within the forum, where new patients often requested advice from the “veterans” of the community. Patients choosing to consult their peers may be looking to take back power that they feel was lost to the healthcare institution, turning it into an ability to choose and trust an alternative, less paternalistic source of information. This sense of powerlessness was a significant theme in many posts. For example, one user stated that they “had no choice” when it came to treatment compliance to avoid being “kicked off” the transplant list, while another reported being “being attached to … the centre” and simply “not knowing what to do.” Another post asked if anyone had advice or if they just “have to live with this [feeling].” A common phrase used across narratives was the statement of feeling tired, not in reference to physical fatigue but rather being weary of certain situations. For example, one post described being tired of “being awake as … tubes [were] put in and out [of their body]” while another recounted being tired of people looking at them “like they’re dying.” Yet, another reported simply being “tired of dialysis.” The sharing and support provided by the forum, and the development of lay expertise on this platform, can help newer patients reduce their feelings of powerlessness and instead help empower them to resist the biomedical lens.
Of note, “we” does not always refer to the dialysis community when used in the forum and may instead indicate the patient’s healthcare team. This is more commonly adopted by the veteran patients responding in the comments. Patients may also refer to their providers as “my” provider instead of “the” provider, suggesting that these providers are being included in that patient’s “in-group.” For example, some posts speak about “my dialysis/healthcare team,” “my doctor,” and “my nurses.” Some used “we” in reference to their team as well, stating that “we had to add a day” to their dialysis schedule and “we looked into a fistula,” implying collaboration between the patient and provider. Therefore, while the use of “they” may suggest that the providers were still primary decision-makers, using “we” may point to a relationship of shared decision-making that has developed in that patient’s journey. In these scenarios, power is being shared across the healthcare team, encouraging the patient to view them as now being “on their side” and no longer in opposition to their “in-group.” Advice provided by the r/dialysis community to cooperate with healthcare providers supports patient autonomy while working within the confines of the system, allowing them to reinforce their own discursive norms while acknowledging the prevalence and constraints of the more dominant discourse. It may feel necessary for them to work within the biomedical discourse given their vulnerability to the biopower enacted by the healthcare institution’s rules and procedures. By utilizing smaller acts of resistance, such as asking questions to make informed decisions, they enact resistance in safer ways that continue granting them the privilege of access to dialysis treatment.
Patient empowerment and lay expertise are growing counter-discourses against the biomedical discursive patterns prevalent in Western countries, which can be seen in the differences between posts by novice patients and the more veteran responses. While novice patients are still steeped in the paternalistic approaches offered by their providers as extensions of the healthcare system, veteran peers may encourage them to consider alternative, more holistic, and more empowering perspectives. This is made possible with the space provided by the increasing neoliberalism of healthcare, which has risen in response to dissatisfaction with traditional approaches, an increasing need for self-management in a society of resource scarcity, and the growing acceptance of digital and online technologies.
Empowerment in Medicalization
The power of language is further evident when looking at the medicalized terminology used by patients within the forum. Medicalized terminology refers to terms that a lay person may not typically be aware of or use on a regular basis. For example, one user reported having “multifocal stenoses … increased flow through the palmar arch … [and] compression of [their] fistula” while another used the term “hemoglobin” over “red blood cells” and “BP” over “blood pressure.” Use of terms such as “acute,” “interstitial inflammation,” and “atrial flutter” suggests that these users are more attuned to specific medical processes than the general public. However, these terms were usually mixed with other lay terms, such as being “plugged in” to the machine, “hooked up,” having a “fistula cleaning,” or a “shoulder catheter.” Medicalized terminology therefore appears to be informally learnt through interactions with their providers, resulting in their “fractured” use of the verbiage.
Medicalized terms are significant as a symbol of the institutional power held by providers, particularly as the biomedical discourse grants power through medical knowledge. Multiple reasons may influence the patient’s use of medicalized terminology; for example, it may be a subconscious decision stemming from the internalization of their passive patient positions relative to their providers. Patients may begin seeing themselves in reductionist ways reflective of the larger biomedical discourse. This process is objectifying, and they may refer to their treatment experiences in similar distancing language, for example, reporting that they “did 1.7, 1.3 … then 1 … but [then only] got to .5” (in reference to the fluid volumes removed during hemodialysis). However, this same positioning may arguably create the absence of medicalization seen in some posts, as patients accept their objectification but remain in the “naive” and “unknowing” state ascribed to them by their provider. Medicalized terminology may also be naturally picked up over time, as patients become more immersed in biomedical discourse. This is particularly salient with dialysis patients, who are exposed to the healthcare system and their providers multiple times a week for many years, and therefore are likely to learn these terms. If medicalized terms are also used in forums such as r/dialysis, then even their social support outside of the hospital may reinforce the use of the same terminology. A patient may also make a conscious decision to empower themselves by intentionally using these terms in conversation, as a means of signaling medical knowledge and demanding more respect. Establishing this may elevate their position from a passive patient to one on more equal terms with others such as veteran peers, but also their providers within a healthcare interaction. In this way, it takes a technology of power wielded by providers to establish the institutional hierarchy and uses it against them to better equalize the power disparity.
These intersections of traditional biomedical discourse and contemporary patient empowerment create spaces of tension, which in turn may impact the way providers are framed and spoken about in the forum. Despite the inclusion of providers into veteran patients’ “inner circle,” many posts by more novice patients were centered around asking questions or expressing doubt about their providers. Questions were typically about peer experiences, either directly related to dialysis or their interactions with the healthcare system. Users would also question the veracity of their providers, preferring instead to check with their peers for guidance on what to do. For example, one post asked if they could ask their provider to “continue using [their] central [line]” and another stated that they still felt like something was “terribly wrong with their heart” despite provider reassurance. This tension remains as users continued to ask their peers for advice regardless of what was given by providers; one post, for example, reported that their providers recommended a switch to peritoneal dialysis, but that they would only trust someone that had “personally gone through the experience.” Discourses in the media may contribute to this trend of distrust in providers, especially for newer patients who have limited personal experience with the healthcare system. Both sensationalism in traditional media and the increased visibility of negative experiences online can contribute to a discursive trend of distrust, which intersects with the “lay expertise” discourse to place significant value on the patient’s lived experiences. This, in turn, ascribes increased respect and power to the veteran patients on the forum, who have the ability to frame their providers and influence these newer patients in positive or negative ways.
While using medicalized terminology may be an effective technology of power during healthcare interactions, its use within an informal, peer-dominant setting warrants consideration. Such terminology can be seen as a symbol of the biomedical discourse, which may not necessarily be welcome or needed within a community endorsing its counter-narrative. Perhaps the issue, then, lies within the positioning of this patient empowerment discourse as “counter” to the biomedical discourse. Instead, it may be seen as one more “adjacent” to it. While it was developed in response to dissatisfaction in the biomedical system, and continues to actively work toward its change, it does not necessarily seek to completely dismantle it or replace it. Instead, these patients are enacting resistance toward certain parts of a comprehensively large discourse, while accepting other institutional practices that fall under it. In this way, use of such medicalized terminology can be seen as empowering, as it not only acts as a signal of the patient’s experience in the system—valued significantly within the community—but also as a way to teach others the means to navigate it.
Discussion
Findings from the selected posts on the r/dialysis subreddit were viewed through a macro lens of power, in accordance with the FDA approach. The iterative process of analyzing each post uncovered multiple overarching discursive categories, which were then filtered to focus on those most relevant to our study. Patient–provider relationships were frequently observed to both shape and be shaped by the discursive power that influences their development. Further analysis revealed the significant role of peer-to-peer interactions within the forum in shaping these relationships. The unique dynamics between posts and their comments provide valuable insights into how patients develop frameworks and concepts during their transition into hemodialysis. Our analysis therefore explores not only findings that speak directly to the patient–provider relationship but also those on the quality and influence of their relationships with their peers.
A Digital Panopticon
The first impression plays a crucial role in establishing the foundation of a relationship (Cone et al., 2017). As a result, the way a user presents themselves in their post can reveal pre-existing frameworks and underlying intentions, both deliberate and subconscious. Self-regulation of digital presentation is an effective strategy for users to achieve their goals, whether they aim to simply get their questions answered or cultivate a more enduring presence in the community. Online forums have created a novel context in which this management occurs, due in part to the anonymity and disinhibition that is afforded with this distance (Shelton et al., 2015). The rise of the internet in the 1980s spurred the proliferation of virtual communities centered around diverse interests and purposes. In the 1990s, scholars recognized these platforms as spaces for connection, empowerment, and even the subversion of traditional power structures, while also acknowledging their potential to foster alienation (Wilson & Peterson, 2002). As we progress further into the 21st century, especially in the wake of the COVID-19 pandemic, these early observations continue to hold true as society increasingly shifts its interactions to cyberspace (Norman Adams, 2024). The ability to form connections and communities across the world online has provided significant opportunity for creation, exposure, and adoption of less dominant discourses, allowing users to use impressions as a means of resistance. This introduces spaces of tension that provide opportunity for change, such as the subversive use of medicalized terminology as a technology of power in biomedical discourse.
Novice patients were observed to engage in self-discipline as a form of impression management. They apologized for “incoherent rants” and expressed that they “should” maintain a more positive outlook, both in their initial posts and in the dialogue within the comments. Despite the presence of moderators on the forum, they did not intervene or comment on any of the selected posts. This lack of direct oversight suggests a classic panoptic setting, where individuals regulate themselves without overt coercion in response to the knowledge of being monitored. Multiple layers of “watching” are likely in play to craft this need to impress: veteran peers on the forum, who may or may not step in to criticize their words and exclude them from the community; moderators of the forum and on Reddit, who can enact the institutional power granted by the platform to remove them from the website; and the larger, discursive societal ideal of patients being ever-optimistic “fighters.” This macro-level discourse can be internalized by those in the patient position and reinforced by friends, family, and even providers who offer well-intentioned encouragement. Despite the veneer of anonymity offered by Reddit’s forums, the initial fear of being monitored may have transformed into a technology of self and resulted in patients striving to be society’s “good patient.”
Self-regulation and the silencing of negative narratives serve to reinforce an optimistic perspective on the illness journey. This outcome is desired on two levels: a micro-level, by dialysis peers and non-medialized “lay people,” and a macro-level, by the biomedical institutions. Dialysis patients may choose optimism to combat the inherent fear of uncertainty that comes with a life-limiting chronic illness such as kidney failure, using it as a mechanism to empower themselves and focusing on choices that remain in their control. Friends and family may also use it as a coping mechanism, again taking power when confronted by uncertainty and reiterating stories of hope and positivity. Optimism therefore serves as a means to reclaim power when feeling powerless against an incurable disease. To the healthcare system, reiterated optimism is a technology of biopower that serves to improve the population’s health. Studies have shown the benefits of self-management and the impacts mental health can have on the physical body; consequently, providing hope and preventing despair can help support the population’s health on a larger scale.
Creating a Community
The r/dialysis forum presents itself as a space where patients can ask questions about kidney failure and dialysis, as well as share personal experiences related to kidney issues. It positions itself as an inclusive community, open to anyone who engages with good intentions. According to Foucauldian theory, the sustainability of any community—regardless of its focus—relies on power dynamics that naturally give rise to a dominant discourse (Philo & Whitworth, 2019). The interactions between peers in the forum serve to both include and exclude certain narratives, thus preserving the integrity of the communal space. The power to silence comes not only from the explicit criticism of certain actions but from the reinforcement of dominant discourses accepted within that community.
Foucault links his concept of othering closely with technologies of power and knowledge (Philo & Whitworth, 2019). Communities are built on divisions that emphasize the strengths of the “in-group” and expose the flaws of the “out-group.” While this process can be overt, it is more often manifested through subtle mechanisms (Adlam & Scanlon, 2010). For example, certain knowledge can be made visible, or specific language repeatedly used, to establish a dominant discourse that circulates within the community. Users reinforce these ideas over time, shaping them into accepted truths. This dynamic is both an exercise of power and a form of resistance against external discourses, as the in-group unites against what they perceive as an unfair narrative (Essex, 2022). These mechanisms are visible in the dialysis forum. Veteran patients, for example, often refer to the community as a team, with statements like “we dialysis patients must stick together.” Discourses emphasizing positivity, perseverance in the “fight,” and the empowerment of asking questions are frequently reiterated. An emphasis of the shared similarities between dialysis patients is used to situate users in the position within the intersecting discourses and encourage acceptance of communal norms.
“Othering” requires positioning of an “in-group” against an “out-group.” The use of pronouns such as “they,” “we,” and “our” can be interpreted as indicators of where an individual is situated within both personal and communal hierarchies. When patients refer to providers as “they” or “them,” they position their providers on the outskirts of their social circle. Conversely, referring to providers as “we” brings them closer to the center, implying a more integrated relationship. The use of “my” and “the” has similar implications, where the former is more personal and the latter more distancing. This movement of the provider between layers of inclusion may reflect the evolving nature of patient–provider relationships over time. For example, novice patients were often observed using “the” and “they,” while veteran patients in the comments were more likely to use “my” and “we.” This pattern mirrors existing understandings of chronic disease patients, who, through frequent interactions with the healthcare system, develop unique relationships with their providers (Drossman & Ruddy, 2020). Novice patients position providers on the outskirts, seeing them as an anonymous extension of the healthcare system (“they”) and experiencing a greater power imbalance than their peers due to their lack of knowledge. The power associated to their providers is situated as immense and institutional. However, with the rise of online forums and increased access to information, patients can shift this power dynamic and gradually separate the provider from the system. As a result, providers become distinct entities with which positive relationships can be built, and the previously conflated sources of power are separated in the patient’s worldview.
The initial positioning of distance between a patient and provider can be attributed to the paternalism of the Western biomedical healthcare system. Although there is power invested in providers by the institution, an increasing scarcity of resources and rise of “patient experts” has resulted in the space for power to be negotiated. Patients find sources of knowledge in their peers and online websites, use technologies of power such as medicalized language, and capitalize on the space that develops alongside the patient–provider relationship to take more power over their treatment decisions. The trust and respect in these relationships may be foundational to shared decision-making, reducing the overwhelming dominance of the biomedical discourse and inviting an otherwise silenced discourse to be heard in the interaction.
Tension Between Discourses
As novice patients engage with posts and comments in the r/dialysis forum, their perceptions of what it means to be a “good” patient, the role of healthcare providers, and the nature of the patient–provider relationship begin to shift. While numerous factors influence this framework, including those outside the peer and provider relationship, the advice and stories shared by peers carry significant weight. The r/dialysis community places a strong emphasis on the shared experiences of hemodialysis patients, sometimes cultivating an “us vs. them” mentality that distinguishes dialysis patients from others. In this environment, novice patients start adopting these discourses, aligning themselves with the perspectives of more experienced peers and shaping their own views based on the collective experiences shared in the comments.
Dialysis patients may experience a tension between the narratives shared by their healthcare providers and those endorsed by the dialysis community. As they transition into their new identity as dialysis patients, they may begin internalizing certain aspects of the healthcare system, particularly through the adoption of medicalized terminology. Medicalization refers to the framing of non-medical issues within a medical context, or the transfer of self-determination and decision-making from individuals to the medical profession for the purpose of social control (Van Dijk et al., 2019). By adopting medicalized terminology, patients may internalize the medical gaze, a concept Foucault describes as the process through which the body is constructed and understood through clinical observations and discourse (Greenhalgh, 2001). This gaze starts from the moment the patient enters the healthcare system and can influence the way the patient views themselves. It objectifies them, reducing them to clinical terms and concepts, such as fluid volumes. Using this medicalized language is powerful, as, in Foucault’s (2002) words: “The eye that knows and decides, [is] the eye that governs” (p. 88–89). Over time, patients may start to see themselves in the way their providers view them. This can lead to a conflict between their internalized medical identity and the self-concept shaped by their peers within the r/dialysis forum. Arguably, even those who consciously choose to use this terminology as a means to reclaim their power may begin seeing themselves with the medical gaze, as their framework adopts to the language they use over time.
Traditionally, the healthcare system has exerted institutional power through providers who act as intermediaries (Cody, 2003), and providers held sole decision-making power within the system. Scholars have coined the term “expert patients” to describe the phenomenon of patients with significant experience, knowledge, and confidence, a concept that has sparked both support and criticism from medical professionals (Tattersall, 2002). Patients may be perceived to be demanding, unreasonable, or subversive in their use of medical terminology and alternative knowledge sources to assert authority in their decision-making (Shaw & Baker, 2004). These strategies challenge the passive role traditionally assigned to them by the medical gaze and are supported in forums such as r/dialysis that emphasize empowerment and lay expertise as technologies of power. The dialysis community, with its emphasis on shared lived experiences, offers an alternative framework that can be at odds with the clinical lens. The tension between discourses allows the patient space to question and consider both sides but may also lead to uncertainty until their identity as a dialysis patient is better formed.
Making Way for Resistance
Foucault (2020) emphasizes a bottom-up approach to analyzing discursive power and highlights the importance of investigating the fringes of society, where institutional power filters down to the micro-level. In the case of the r/dialysis forum, peer-to-peer interactions function as spaces of both power and active resistance, existing alongside the broader dynamics between patients and the healthcare system. Veteran patients hold authoritative power within the communal hierarchy due to their extensive lived experiences, shaping the dominant discourse present in the forum. Despite the potential for resistance, observations of the forum suggest that novice patients often embrace, and even perpetuate, these power dynamics. The readiness with which they accept peer opinions without questioning points to a marked difference in quality between patient–provider and peer-to-peer relationships. As one patient noted, many “only trust those with personal experience,” signaling the elevated credibility placed on peers over providers. This may reflect a broader societal shift in how healthcare providers are perceived, as counter-perspectives to traditional biomedical discourse become prominent. Peer communities have historically been studied to develop counter-narratives as forms of resistance (Essex, 2022), creating an alternative discourse grounded in shared dissatisfaction with the existing system. These discourses place value on concepts traditionally trivialized in biomedicine, such as the patient voice and experience, giving power to those who feel dismissed by providers in the healthcare system. In this way, they find approval from those on the “fringes” of the current dominant discourse.
As expectations grow for patients to actively participate in their care, the internet has become a valuable space for empowerment through the exchange of knowledge. Self-management has become both a practical means to address resource scarcity and a way to address the growing dissatisfaction with the paternalism of traditional medicine. Online forums like r/dialysis have created a space for dialysis patients around the world to engage in a discourse that centers on empowerment and resistance to the medicalized system. Foucault discusses how knowledge can become a site of resistance, where power structures are contested and challenged (Medina, 2011). Subjugated knowledge is often rendered invisible over time but can be reclaimed as a tool for resistance (Foucault, 1980). Historically, it was challenging to combine and strengthen such counter-knowledge, but the rise of online forums has eased the process. Patients sharing experiences that were once overlooked are now empowered by their peers to mobilize this knowledge. This dynamic is evident in the r/dialysis forum, where the supportive and protective nature of the community fosters empowerment and collective resistance. Comments may urge the novice patient to “BE CONCERNED” and ask more questions, or encourage them to speak up and “fight it hard!” In many cases, patients become advocates for their own care, using their accumulated knowledge to challenge the traditional medical narrative. One patient, for example, thanks the forum for suggesting they get a second opinion and explains that they advocated for more than a simple fistulogram: “If he had done only that, my steal syndrome would be even worse.” For these patients, the r/dialysis community may serve to reinforce discourses of patient empowerment and lay expertise to encourage peers to take up spaces of tension and enact resistance.
Conclusion
As patients progress in their renal journey, their perception of the patient–provider relationship may evolve, alongside shifting power dynamics and peer influence. In the early stages, patients can rely heavily on the discourse endorsed by their providers and perceive them as extensions of the larger healthcare system. When questions or concerns arise, they may bring them to their peers, whose shared experiences lend credibility that providers may not possess. A strong sense of community forms quickly as patients connect over common struggles and emotions that are difficult to express to those outside the group. As novice patients continue to interact with veterans, they may begin adopting the perspectives and frameworks of their more experienced peers, often fueled by disenchantment with the healthcare system (Thorne & Robinson, 1988). This shift in perception leads to a sense of camaraderie among patients and a shared desire to resist the medical institutional discourse. This study has highlighted the significance of how engaging with an online community of peers shapes development of patient–provider relationships, but also the relative absence of providers in easing the transition into hemodialysis. Patients were observed to turn to their peers to potentially fill gaps in knowledge and support left by the healthcare system. Despite this, a healthy patient–provider relationship was endorsed by many veteran patients, where the provider was seen as distinct from the larger healthcare system and an active partner to the patient for their care. This allowed for a more individualized relationship to develop, where trust and collaboration could evolve and providers were perceived as a supportive actor within the patient’s community.
Footnotes
Acknowledgement
We thank Paul Bucci for his assistance and support in using the Teleoscope machine-learning tool.
Ethical Considerations
Our study was exempted by the Human Research Ethics Board at the University of Victoria as Reddit posts are considered public data.
Authors Contributions
S.H.O. designed the study, collected the data, and performed qualitative analysis with support and guidance by A.S. and V.C. S.H.O. took lead in writing the manuscript. All authors contributed to critical feedback, review, and edits to the final paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.