
Abstract
Head and neck cancer (HNC) includes a diverse group of cancers, involving complex care pathways and life-altering side effects, including changes to how people communicate. Patient experience is an important outcome of HNC care; however, to date, little research has been conducted to explore the healthcare experiences of those individuals with HNC and associated communication changes. We sought to explore how people with HNC and associated communication changes understand their healthcare experience. An interpretative phenomenological analysis framework was employed, using data from nine individual interviews. Six group experiential themes were identified: (1) Assembling and reassembling supportive scaffolds: The role of significant others and peers in the healthcare experience; (2) Human connectedness in an overwhelming system: Reverence in presence, turmoil in absence; (3) Gathering, disengaging, or epiphany: The fluxing relationship with information; (4) Continuum of healthcare navigation: From frustration to relief; (5) A quest to reclaim self after upheaval; and (6) From confronting to seeking: The desire for professional expertise. Findings show that healthcare engagement and navigation are ongoing for years post-primary treatment. The healthcare experience is often traumatic, but there are moments that bring people from vulnerability to safety with families, peers, and healthcare workers all contributing different roles. This group of people value expertise in their healthcare, have a fluctuating relationship with healthcare information, and begin to rebuild themselves early in the healthcare experience. This research helps to understand the healthcare phenomenon and can guide practices to support people with HNC throughout their continuum of care.
Introduction
Head and Neck Cancer
Head and neck cancer (HNC) comprises a heterogeneous group of cancers affecting the upper aerodigestive tract including lips, oral cavity, salivary glands, pharynx, sinuses, and larynx (Australian Institute of Health and Welfare, 2014; Cohen et al., 2016; Massa et al., 2018). HNC care involves complex pathways, involving multiple healthcare providers (HCPs), healthcare episodes, and treatment options (Cancer Council Victoria and Department of Health Victoria, 2021; Checklin et al., 2024; Cohen et al., 2016; Foley et al., 2022). Treatment modalities may be single or multimodal, including surgery, radiotherapy, chemotherapy, and/or immunotherapy (Cohen et al., 2016; Cramer et al., 2019; Mody et al., 2021). The care continuum spans symptom presentation, diagnostics, primary and adjunct treatment, rehabilitation, surveillance, survivorship support, and sometimes palliative care (Cancer Council Victoria and Department of Health Victoria, 2021). Over the last two decades, HNC has shifted from being primarily associated with tobacco and alcohol use to being increasingly linked with the oncogenic human papillomavirus (HPV) (Mody et al., 2021). HPV-related cancer affects younger people and has better survival rates, meaning that people are living longer with the side effects (Mody et al., 2021). Lasting side effects include xerostomia, decreased dental health, swallowing impairment, shoulder and jaw dysfunction, lymphedema, pain, and communication difficulties (Taylor et al., 2023; Verdonck-de Leeuw et al., 2022).
HNC-associated communication changes (ACCs) arise when cancer and its treatments disrupt the anatomical structures for verbal communication (speech, voice, hearing, and cognition) and are often confounded by pain and fatigue (Bolt et al., 2016; Chen et al., 2015; Fletcher et al., 2019; Heijnen et al., 2016; Mujica–Mota et al., 2013; Piai et al., 2022). These communicative disruptions not only impact the person with HNC but also their families, with consequences stretching across many aspects of life (Nund et al., 2015). Changed communication abilities often persist, impacting directly on return to work, quality of life, family relationship and roles, intimate relationships, and healthcare experiences (Gibson et al., 2022; Nund et al., 2015; O’Brien et al., 2012; So et al., 2012; Tsai et al., 2023).
Patient Experience and Ability to Communicate
Patient experience is defined as “the sum of all interactions, shaped by an organization’s culture, that influence patient perceptions across the continuum of care” (The Beryl Institute, 2025). Excellence in person-centered healthcare can be achieved by being grounded in patient experience (Abid et al., 2024), which is positively correlated with safety and outcomes (Doyle et al., 2013). Patient experience informs strategic decision-making, enhances safety, and supports clinical improvements (LaVela & Gallan, 2014). Positive experiences may also encourage patients to return to their HCP, particularly important in HNC given the risks of recurrence and long-term side effects (Browne et al., 2010; Haring et al., 2023; Verdonck-de Leeuw et al., 2022).
Despite communication being an important human right with legislation in place to support a person’s right to communication supports when accessing healthcare, people with communication disabilities report negative healthcare experiences (McEwin & Santow, 2018; McLeod, 2018; U.S. Department of Justice Civil Rights Division, 2020). Such negative experiences include, but are not limited to, being unable to communicate basic needs on the ward, greater risk of hospital falls, frustration and stress in accessing emergency care, not receiving pain management in critical care, and inequitable healthcare outcomes (James et al., 2022; Nyhagen et al., 2023; Stransky et al., 2018; Sullivan et al., 2024, 2025). Despite this recognition in the broader healthcare literature, recent reviews highlight that people with HNC-ACCs are rarely included in research on communication disability and healthcare experiences and an ACC is rarely a focus in the HNC healthcare experience literature (Checklin et al., 2024; Oshita et al., 2025). One scoping review of qualitative research on the experiences of people with HNC reported limited studies specifically examining the impact of ACCs on HNC patients’ healthcare experiences (Checklin et al., 2024). More studies excluded people with significant communication issues rather than specifically investigating this topic (Checklin et al., 2024). Although some studies reported on communication, only two explicitly reported investigating the healthcare experience of people with HNC-ACCs. One mixed-methods study reported that people with HNC-ACCs experienced communication difficulties when requesting pain medication in the post-operative phase (Rodriguez & VanCott, 2005). A qualitative study investigating the HNC patient experience reported that communication with HCPs was hurried, leaving them feeling silenced and disempowered (Gibson et al., 2022). These two studies illustrate that people with HNC-ACCs experience unique challenges in their healthcare experiences, but knowledge in this area is limited.
Limited understanding of the healthcare experience of patients with HNC-ACCs hinders efforts to improve patient experience for this cohort, and by extension patient safety and clinical outcomes (Doyle et al., 2013). To make informed clinical recommendations, we must first understand how people with HNC-ACCs interpret and make meaning of their complex healthcare pathways. This study aimed to investigate the healthcare experiences of people with HNC-ACCs to understand their experiences.
The Present Study
Ethical Considerations
This study was approved by the Monash Health Human Research Ethics Committee (approval no. RES-23-0000-155A). All participants provided written informed consent, obtained by the principal investigator.
Methodology
A qualitative study informed by interpretative phenomenological analysis (IPA) was chosen. IPA focuses on uncovering deeper meanings and understanding how individuals make sense of their experiences within their broader contexts (Smith et al., 2021; Spiers & Smith, 2019). Employing IPA is particularly suited to exploring the healthcare experiences of people with HNC-ACCs, a phenomenon not yet examined using this methodology, enabling this topic to be seen through a new lens, while providing essential methodological rigor (Checklin et al., 2024). An IPA approach allowed for the collection and analysis of rich and detailed information without predefined categories. A key component of IPA is that the researcher engages in “double hermeneutics,” meaning the researcher attempts to make sense of the participants’ own sense-making of the phenomenon (Smith et al., 2021). IPA has a microexperiential focus, so it advocates for a small purposive homogenous sample, with rarer health conditions such as HNC tending to generate their own homogeneity (Spiers & Smith, 2019).
Recruitment
Participants were recruited from three health metropolitan networks across Victoria, Australia, and Australian HNC patient support groups. Local clinicians not involved in the study approached eligible participants, or participants responded to adverts via support groups.
Participants
Eligible participants were adults with a confirmed diagnosis of HNC, had self-reported communication changes from treatment/HNC, had undergone curative-intent treatment (and not under palliative care) in an Australian healthcare context, and were unknown to the researchers. Australia has a hybrid model of both public services (funded through taxation) and private services (funded through private insurance and/or individual contributions) (Dixit & Sambasivan, 2018). Participants were included from either system. Additionally, participants completed the Communicative Participation Item Bank (Baylor et al., 2013) prior to the interview to inform the interviewer of current participant-reported communicative participation abilities.
Data Collection
Semi-structured, one-to-one in-depth interviews were conducted using a flexible guide (see Appendix 1). This guide was constructed by the research team, piloted with someone with HNC-ACCs, and modified based on feedback from the pilot themselves and from the research team after watching the recorded pilot interview. The interviewer had formal training in qualitative study interviewing. Questions focused on exploring sensory perceptions, mental phenomena (i.e., thoughts, memories, associations, or fantasies), and individual interpretations on the healthcare experience (Pietkiewicz & Smith, 2014).
In-depth, semi-structured interviews can be used effectively with people with communication disorders, provided participants’ communicative abilities and preferences are accommodated (Bickford et al., 2022; Lanyon et al., 2019). All interviews were video-recorded. Data collection strategies included interviews conducted by an experienced speech pathologist with HNC expertise, use of a microphone connected to participant hearing aids, face-to-face interviews to improve speech intelligibility, online interviews that allowed electrolarynx connection to the audio system (extending battery life), scheduled breaks, and opportunities for all participants to provide additional written thoughts post-interview. The interviews were transcribed verbatim externally, checked by the interviewer for accuracy, and returned to the interviewee for any further amendments.
Data Analysis
Data analysis followed a seven-step IPA framework (Smith et al., 2021), with notetaking, field notes, and reflection journaling throughout each stage. The analytical process was dynamic and nonlinear, with iterative deepening of analysis. Personal Experiential Themes (PETs) were created for each participant; these PETs were merged into Group Experiential Themes (GETs) to generate the overall findings.
Quality was enhanced by designing and conducting the research in line with IPA principles (Smith et al., 2021), adhering to the eight “big tent” criteria for quality across qualitative research (Tracy & Hinrichs, 2017), and ensuring IPA-specific quality markers were followed (Nizza et al., 2021). Member reflections (in-situ checking and participant transcript review), audit trails of data collection and analysis, peer data review, and team debriefing all assisted with establishing credibility.
Results
Participant Details (n = 9)
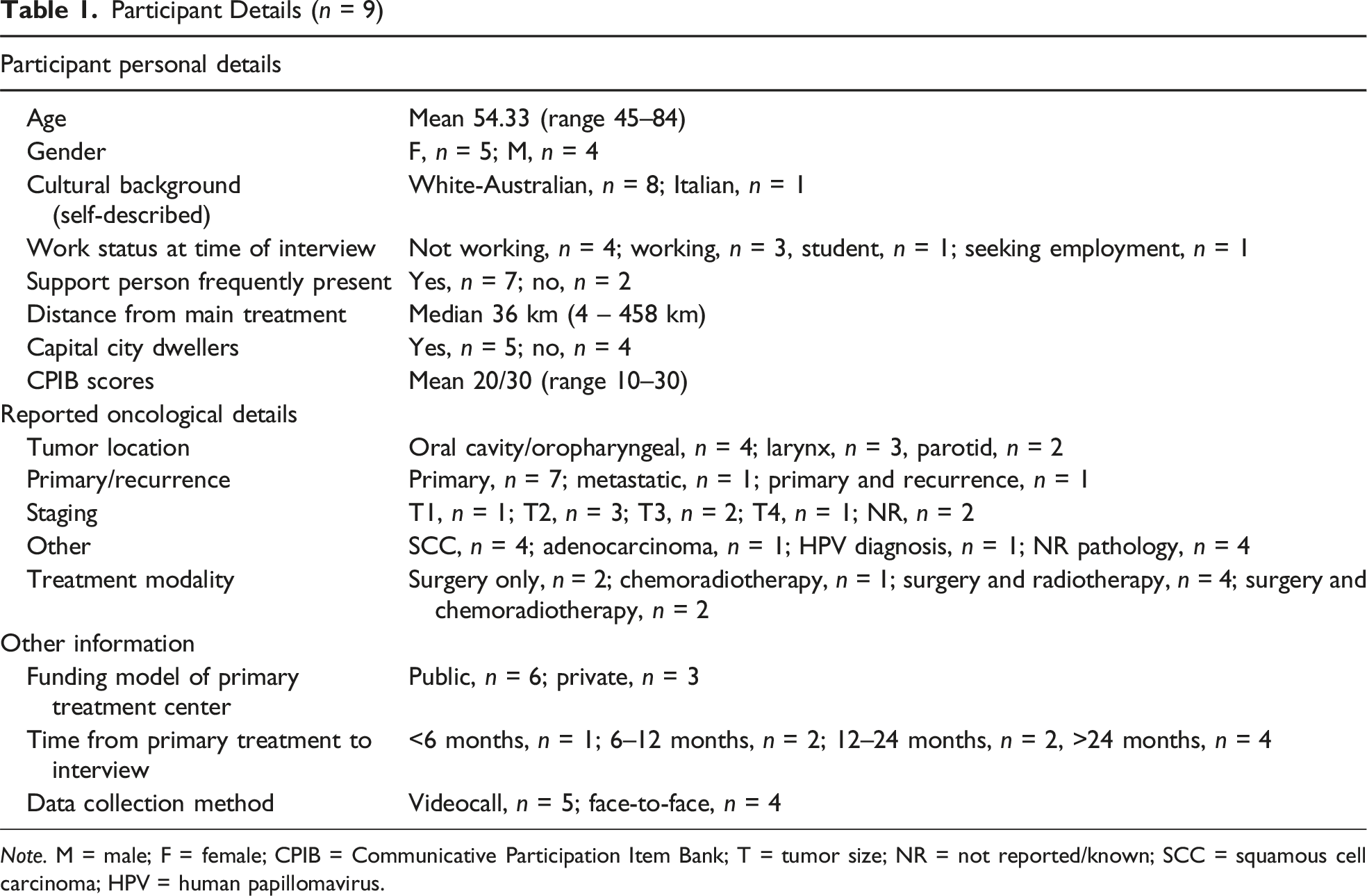
Note. M = male; F = female; CPIB = Communicative Participation Item Bank; T = tumor size; NR = not reported/known; SCC = squamous cell carcinoma; HPV = human papillomavirus.
GET 1: Assembling and Reassembling Supportive Scaffolds: The Role of Significant Others and Peers in the Healthcare Experience
Seven of the nine participants reported having a significant other (SO) frequently accompanying or visiting them during treatment. People with HNC-ACCs deliberately built support networks, primarily consisting of close SOs and, to a lesser extent, peers. These scaffolds provided emotional, practical, and advocacy support, particularly during the vulnerable initial stages of treatment. Participants expressed immense gratitude for SOs, who helped them navigate complex healthcare systems, interpret medical information, and regain a sense of self. These relationships often reflected pre-existing dynamics. For example, Susan described having “my husband there the whole time, thank goodness. Because he was sort of like an advocate,” reflecting that a pre-morbid loving family provided strong, cherished support.
Such advocacy often extended to interactions with HCPs, with SOs stepping in to ensure that the needs and wishes of the person with HNC-ACCs were communicated during time-limited medical interactions: “I just felt like [family] needed to be my advocate, because I couldn’t speak” (Maria). Brian described relying on a friend to clarify medical terminology after his hearing declined: “I heard it as ultrasound … but it was an ultrasound-guided FNA biopsy … so that’s the major motivation for getting [friend] to come with me.” Support needs transcended healthcare settings, with help also required in social settings. As Craig noted, “Even when we’re out in public, if she sees me struggling, without even interrupting, she’ll just basically help me talk … without her, I’d be feeling a lot more socially isolated.” This experience contrasts with Wayne, who had less social support, describing being “at the pub when a lot of people are talking, everyone tends to get louder … people can’t hear me. So … I tend not to communicate. I put my earphones in.”
Some participants benefited from SOs with extra skills to support their healthcare, such as a naturopath (Elizabeth), a paramedic (Susan), a nurse (Kate), or a speech pathologist (Maria). Kate described being “quite lucky with Mum being a nurse … [because] I’m not sure other people would have the same support,” while Maria’s friend, a speech pathologist, “would … just listen to me when I was speaking … Also gave me some exercises to do.”
Peer support was also valuable, particularly in the context of adapting to communication changes. Sharing similar experiences offered invaluable practical advice and strategies for managing complex communication challenges. This shared understanding fostered a sense of camaraderie and reassurance, providing participants with lived experience insights. Wayne, a laryngectomee said, “you don’t become as fearful as what you would just going through it on yourself. Seeing other people that have gone through it and seeing what they’ve been able to accomplish.” Kate found emotional support at a time of great vulnerability from “the lady in the bed next to me … we started communicating with our whiteboards to one another through the curtain.” However, as support needs changed over time, so did participants’ need for peer support, especially when they were trying to move away from a focus on cancer. For example, Jennifer initially wanted connection: “I really wanted to talk to these people [cancer buddies],” but later distanced herself: “I want to put cancer to the side … this cancer group that I belong to … I’ve stopped going the last two or three months because I get sick of listening to these people in the group who complain.” This illustrates how peer support fluctuates based on personal needs and healthcare time points.
GET 2: Human Connectedness in an Overwhelming System: Reverence in Presence, Turmoil in Absence
Among the traumatic challenges of healthcare, there were moments of human connectedness that were profoundly meaningful and transformative. Through reassuring, comforting, and personal interactions with HCPs, people moved from vulnerability to safety. Maria recalled reassurance from an HCP’s words: “He said, ‘It’s just a bump in your road, it’s not the end of the road.’” Such words offered a sense of safety amid health uncertainty. Elizabeth reflected that her oncologist “was amazing, I haven’t met many men as amazing as my father … he just made you feel—he was very reassuring.”
While not every interaction required such connectedness, its absence at vulnerable moments increased fear, anger, distrust, and trauma therefore leading to further turmoil. For example, Keith and Susan both talked about moments with and without human connectedness, demonstrating the differences that human connectedness can bring. Keith said of his surgeon that “He was too big headed and arrogant to talk to a patient … he shot us down the first day we went in there,” contrasting with being with a nurse: “We’d go out there and sit in the sun and … he made ya feel as comfortable as he could.” Susan stated, “Well, he [surgeon] was just talking, like, as if I’m the specimen there that all the learning staff are looking in on. I mean at one stage, I had 10 people looking in on my mouth,” and then compared a different encounter: “She just said we’ll just have a chat. So, I’m sure in that chat, she was also giving me some ideas. But I didn’t feel like I was this sort of specimen that needed to be changed.” Elizabeth while suffering distress and seeking medical help reported that a receptionist’s demeanor exacerbated the stress, stating, “But when I tried to get this appointment, she was a bit short with me,” which resulted in her calling a different healthcare network to get follow-up care.
Human connectedness transcended newly acquired communication barriers for people with HNC-ACCs, even using non-verbal means. Maria described a critical moment: We ended up having this magnificent conversation through a whiteboard … how amazing [a nursing student] is in the way that she shows such compassion and kindness … It was a deep conversation … I don’t know if it would ever happen if it was just a verbal conversation.
Such experiences reinforced the power of connection, illustrating that the impact of ACCs could be mitigated by creating a shared humanity between patients and HCPs. For individuals with HNC-ACCs, these connections foster more than a sense of being cared for. Participants developed meaningful connections with HCPs during traumatic times, enriching both parties reciprocally. Brian discussed the emotional connection: It is possible for the patient and the healthcare professional to find a degree of kindredness of spirit, to the benefit of their professional relationship, and perhaps even to their individual lives beyond that relationship. We all gain from shared reminders of our common humanity.
However, Craig reflected on contributing back positively to the care dynamic, sharing feedback with HCPs on communication solutions he discovered after treatment, showing his wishes to support clinicians’ knowledge.
GET 3: Gathering, Disengaging, or Epiphany: The Fluxing Relationship With Information
People with HNC-ACCs had a complex relationship with healthcare information, leading to varied levels of preparedness and understanding. Participants recalled moments of successful delivery, enabling them to prepare better for treatment. Wayne reported that his surgeon “pretty much told me before the operation what would happen. And—and obviously I was a bit worried about being on the table for 12 hours. I rushed around and tidied things up before I went down.” Craig described having “been prewarned about the fact that I wouldn’t be able to communicate. So, I got a range of little [digital writing boards] and blackboards.” Additionally, being informed provided psychological reassurance for participants, with Brian describing that “the more information that I got, the better I felt,” and Elizabeth sharing that she “didn’t know that I would get that information, so that was sort of … comforting.”
Despite HCP-delivered information, participants accessed additional sources. Craig noted, “I used to spend hour or two hours like ‘avin’ a bit of a Google … to see why I was havin’ the problem with the [voice prosthesis] leakage,” reflecting a need for internet-led guidance on managing voice prosthesis leakage when HCP advice was absent. Similarly, Jennifer also sought online information on many aspects of her healthcare such as symptoms, surgeon reputation, and what she may look like in the future. However, not all internet-sourced information was valued. Susan shared her experience: “I’ve joined a Head and Neck Facebook [group]. Which is the whole world … Then they are just reliving it all the time and I’m thinking, ‘My goodness’. But I don’t think that’s that healthy.”
In contrast, other participants felt unaware and underprepared for what happened after surgery, feeling that the information provided by HCPs was irrelevant or not applicable to them. Jennifer reflected on her initial naivety of future changes, saying, “I didn’t think about [side effects] … OK, I just thought … they’re gonna operate here. They’re going to take it out, and I’m going to be OK.” Similarly, Susan described her initial shock when she learned she would have a tracheostomy post-operatively: “I was a bit sort of naive and unaware … the speech pathologist came in and said, ‘No I think you’re going to have one of these’, and I’m like, ‘What?’”.
Many felt that while they had been given some information, it was not always sufficient to fully prepare them for upcoming realities. Keith mentioned, “There’s a little bit of unexplaining … I don’t think once that any of ‘em ‘ave mentioned, um, smell,” indicating that critical outcomes, such as anosmia, were overlooked. Similarly, Kate post partial glossectomy highlighted that clearer information would have helped: An area for improvement could be really seeding that it’s likelihood that you will need speech therapy … some more definite language and some reference to how many people do, or how long … they would be out of action for.
For some, receiving information did not always translate to understanding. Kate, while acknowledging that she had been warned about the possibility of speech pathology, expressed that the actual impact was far more significant than anticipated: So not being able to pull much of a sentence together was quite a shock. I think in understanding before the surgery, it was you might need some speech therapy, and in my mind I was like, “Ohh it’s only a small ulcer, I’ll be fine,” but actually the impact was quite a lot.
Others avoided absorbing information as it was too overwhelming. Susan candidly remarked, “I think at that time I just thought more information for me wasn’t the way to digest this.” Similarly, it was difficult for people to digest diagnostic information due to the stress of being confronted by cancer, with reflections including “There’s prob’ly a lot of things explained to me previously, but well [I’m not] in the mind frame of what is goin’ on” (Keith) and “half the time I wasn’t in the mindset to listen to what they were telling me” (Jennifer).
Many only fully understood information after experiencing treatment firsthand. Maria encapsulated this experience: “Not until probably about two months after my visit—I understood what they did. I was then able to just come to terms with it and work with it differently.” Jennifer added, “You just don’t know until you go through it.” Elizabeth noted how she only engaged with written material after treatment: “The handouts you get given at the very start … it wasn’t until probably towards the end I started reading stuff.”
GET 4: Continuum of Healthcare Navigation: From Frustration to Relief
Participants did not perceive their healthcare pathway steps as separate healthcare components but saw their healthcare experience as a sum of their encounters across the continuum of care, even when involving multiple health providers and networks. The ongoing challenges of managing side effects and navigating multiple healthcare services for people with HNC-ACCs reflect varied experiences with both coordinated and disjointed care. Coordinated care provided confidence and reassurance to participants, while its absence led to stress and frustration. Not only were participants seen by multiple clinicians within the same professional group and across a range of differing roles, but individuals needed to access different health networks, accessing both public and private providers. This therefore had a major impact on coordinating and navigating HNC healthcare.
Participants described organized care as calming and supportive. Brian shared how coordinated care resulted in feelings of confidence and relief, reflecting that “Committed professionals … inform the patient as to what is being done, what is to be done, and why … coordinate smoothly, and keep the flow of things.” Similarly, Jennifer valued coordinated care, saying, “Everything was organized. You go here, you go there.” For Keith, relief came from organized professionals who “come through to see if you’re okay and how you’re going to be when you’re home; ‘Have you got this at home? Have you got that at home?’”, highlighting reassurance when HCPs follow up on future needs. These experiences illustrate how healthcare pathways that are perceived as accessible and well-structured healthcare provide relief, provide emotional security, and, ultimately, foster trust.
Within her experience, Susan experienced relief but at other times expressed frustrations with navigating the system across her surgical and radiotherapy hospitals. She described a nurse coordinator as “super important. Just to make that contact and to help us navigate this big system,” but even with that help, when managing late side effects, she added: Once you get outside the system where they’re all talking a little bit, they’ve got access to the same scans, and it worked. But the moment you step out of that, you’ve got to go and get your own scans, and you just feel like you’re spending so much time running around doing all this stuff.
Craig echoed this frustration, noting the lack of care coordination between the HNC treating team and his other HCPs “that was one of the rare cases where my GP got notified of the results.” Participants requiring surgery and additional treatments (e.g., radiotherapy) or care across multiple health networks faced greater emotional toll in navigating care. Kate, who had acute care outside her geographical cancer care catchment, noted that her healthcare journey could have been enhanced by “a stronger handoff point for people to know their options. I kind of fell into my physiotherapist through the wound nurse.”
Re-engagement with healthcare was a recurring event in participants’ narratives, reflecting continuous needs. Susan was still re-engaging five years post-initial treatment, Jennifer two years post, and Brian following up concerns regarding a “new lump.” The participants who had undergone a laryngectomy as part of their HNC treatment (Wayne, Keith, and Craig) also described constant needs; Keith described a time he had to re-engage with the healthcare system “[my voice] was getting worse and worse, and I’m thinking, like, you know, I don’t know what’s going on here, but anyhow, I went back, and they had a look. Sure enough, the skin had grown over.” Wayne, also a laryngectomee, explained: “I have trouble with [voice prosthesis] leaking. I can’t socialize like I used to … I just have to let the doctors know.” Due to the nature of laryngectomies and voice prosthesis changes, a clearer pathway for re-engagement with healthcare services was in place compared to other HNC subpopulations. This contrasts with Kate, who had tongue cancer and experienced delays in accessing speech pathology, stating, “Perhaps it was delayed through the system, so I then made my own inquiries to secure an appointment and find out who would be available.”
The need to constantly re-engage with healthcare systems to manage ongoing issues, sometimes without clear pathways, can leave patients feeling overwhelmed. One way of controlling this was by enacting agency to address their needs to rebuild their lives. Many participants described moments when they took control of their care. Kate actively sought the type of speech pathologist she wanted, saying, “I knew speech pathology as a career was quite varied, and I didn’t necessarily think my situation was aligned with pediatrics or aged care requirements. So, I wanted someone who’d perhaps had hospital or acute experience.” Maria described a similar experience: The speech therapist through the hospital was brilliant, but they only have, obviously, a certain time that they work with us. Once I left out the hospital, their recommendation was to either wait until I could get into the public system or see my own … I said, I don’t want there to be long-term changes. Who can I work with?
In response to seeing another person with HNC whose appearance did not align with her aspirations, Jennifer felt that she did not want to become like her and actively sought further surgery, reflecting, “She’s let herself completely go, and I could see that. And, um, I decided, no, that’s not me.” Elizabeth reflected on her choice to access alternative therapy without telling the medical team, sharing that she “just thought I don’t know if this will sit well with the medical people … but I was just keen to, um, just to see how that would help.” More desperately, Craig recalled the time when he was not getting the follow-up care he felt was optimal, so “I lied on my next appointment … I said, ‘I’ve been coughing up a bit of blood’” which led to the discovery of further tumors.
GET 5: From Confronting to Seeking: The Desire for Professional Expertise
Gratitude for specialist expertise was evident, especially in the initial diagnostic and primary treatment phases. However, participants required ongoing expertise, particularly when long-term side effects persisted, with Jennifer stating her “side effects are ongoing … you need to stay in the healthcare system to utilize the help out there for a better outcome mentally and emotionally.” Perceptions of HCP expertise provided participants with relief and reassurance. Wayne described being treated by “a tradesman … not a labourer,” emphasizing the value he placed on skill and experience. Keith shared, “one of the male nurses wasn’t new to laryngectomies, he was pretty good and I actually think that that’s what made the experience prob’ly pretty good,” contrasting to his experience with speech pathology: “[speech pathologist at a different hospital] was a fair bit more experienced in what she was doin’ than what they two of ‘em [speech pathologists at treating hospital].” Craig also felt the HNC ward had expertise in communicating with people, but this expertise was absent elsewhere in the hospital: I was basically just standing in an x-ray machine … It’s just people in that scan room obviously weren’t dealing with larys all the time, so they could usually talk to the person and ask them to do something, ask them a question from another room and get an answer.
Appreciation of expertise was reported by others, such as Elizabeth, who was impressed that her speech pathologist had “seen it all before,” and Jennifer, whose surgeon had “the opinion of his colleagues.” Some participants were relieved at being offered other services, like “the opportunity to have a psychologist” (Maria), “a referral to [speech pathologist] to do the esophageal speech” (Craig), and “one word of mouth referral I got from the wound nurse was if I had private health, was a recommended lymphedema physio” (Kate).
Access to expertise often necessitated compromises: tolerating brusque demeanors; long travel distance; lengthy waiting times; or being confronted by the vastness of the HNC teams. Susan articulated the tension: “He knows his work and I do really trust him but he’s a bit gruff … what can I do when I’ve been advised that this is what you need to do?” Four participants were non-metropolitan residents and had to travel to access expertise, which was often their preference over accessing services from HCPs perceived to be less experienced in regional centers: “It’s like with the nurses in [the city hospital]. Like I’ve got more confidence in them, and they understood more about my predicaments than the ones in [local hospital]” (Wayne). Jennifer added, “Access to these needs were easy as my treatment was in the city at a great hospital with amazing health professionals guiding me.” At times, the level of specialists and expertise was overwhelming, Maria described, “So within 15 minutes … we had probably about 20 to 30 people coming into the room, all from different teams. So, whilst that was overwhelming and extremely confronting, there was also a sense of assurance.” Others reflected on the conflicts within the need for expertise: “I guess it’s that idea that I’m dependent on people’s expertise … and yet I’m also saturated with it as well” (Susan) and “You can easily concede to what these people tell you, and I know they call them specialists, I just call them advisors, because they’re trying to help me get better” (Craig).
The need for high-level expertise was not always met within the treating primary health network, creating stress and leading to participants seeking solutions independently elsewhere. Craig expressed frustration with the lack of technological support he had when he was non-vocal, reflecting, “I think they’re [speech pathologists] dragging the chain a bit as far as that’s concerned … The speechies are really just handing on the knowledge from one speechie to the next.” Susan expressed her distress when denied the expertise she wanted “but straight away, there’s all these assumptions. I said no, I just need … somebody who can help me out with lymphoedema. That’s all I wanted. But they wanted me to have all these other services.” Participants demonstrated agency in seeking expertise independently. Elizabeth recounted seeking PEG (percutaneous endoscopic gastrostomy) expertise: “I rang [different health network] and I said you guys didn’t put this PEG in, but I would like it out.” Some participants referred to expertise outside of medical healthcare to help them cope and manage the impacts of HNC, such as naturopathy (Elizabeth) or meditation gurus (Maria), or peers (Jennifer, Craig).
GET 6: A Quest to Reclaim Self After Upheaval
The diagnosis of HNC was shocking and stressful for patients and their families. Brian described it as “dealing with ah what turned out to be a crisis situation.” Maria expressed the emotional toll, describing that she was “just so emotional. I am crying constantly because, intuitively, I think I was feeling something.” Jennifer recounted how the diagnosis affected her entire family in that “We haven’t had cancer in the family. It was worrying.” Following diagnosis, participants described the treatment phase as brutal and traumatic, forcing them into vulnerability. Those who underwent a tracheostomy felt intense shock. Susan recalls “the treatment was really quite traumatic. Waking up with a trache … listening to other people choking, it was really traumatic.” Kate added that “the hospital stay was the most traumatic part. Not just physically … As an acute ward, they have the trache patients, all who can’t speak and are using whiteboards.” She reflected on the vulnerability of losing fundamental functions: “You don’t realize how much swallowing, breathing, and speaking make you vulnerable until they’re taken away.” Treatment also deeply impacted their sense of identity. Maria shared: I felt like it was effin’ barbaric … Only mafia people cut tongues off. How the fuck am I getting half my tongue cut off? I didn’t know what I was going to look like or what it was going to do to my family.
Other highly traumatic aspects of treatment included facial disfigurement (Jennifer and Susan), mask-fitting for radiation therapy (Jennifer and Susan), pain (Elizabeth, Keith, and Susan), radiation side effects (Wayne, Elizabeth, and Keith), and PEG presence (Elizabeth).
From these low points, people with HNC-ACCs began to rebuild themselves early in healthcare settings, including how they functioned as communicators. Many initially became non-vocal communicators due to swelling, tracheostomy, or laryngectomy with adjustment to written communication being manageable: “They were patient enough while I was writing on the blackboard” (Craig) and “I was always prepared with a notepad” (Wayne). However, they learned to deal with communication inefficiencies. Keith explains, “You shorten it up. You don’t say what you normally would if you were talking, because you’re textin’ and thinkin’, well, they haven’t got all day to wait.” Wayne adds, “It just took a little bit longer to tell them what you wanted.”
Hospital environments played a role in easing this transition and learning adaptive communicative skills. Kate recounts, “[My mum] couldn’t understand me, so we reverted to the whiteboard. With staff, it was generally okay.” Wayne wrote with pen and paper for over six weeks while in hospital and added that “[staff] were great … [staff] were so amazed at the neatness of the writing.” Craig highlighted how skilled staff adapted: “Writing on the [writing tablets] was minimal because they expected me not to speak and asked yes/no questions instead.” However, there were also moments of frustration. Maria, who lost her vision due to chemical exposure and could not use her arms due to IV access, describes, “I couldn’t write or speak … I remember saying to the universe, ‘What the hell do you want from me? You’ve taken all my senses except hearing.’” Even when she regained writing abilities, challenges persisted:
You have a bell to call staff, a pen, and a board, which usually works—unless they take the bell or the board away, which did happen. Then you feel like, ‘Hang on, you’ve just taken my only way to communicate!’
Craig shared similar frustration at being sent to scans without his communication board and not being taught esophageal speech for simple communication.
After hospital discharge, people continued to rebuild their communication skills using healthcare services. Speech pathology was often a key part of this. Kate reported that for her, “face-to-face was better. Over time, it became a good accountability checkpoint, making sure I was getting out of the house and connecting.” Others engaged later, like Jennifer who accessed service two years post-treatment and emphasized the importance of self-management: “In the first few weeks, you cover most of it. Then it’s up to you to practise.” Some require ongoing support, such as managing voice prostheses. Beyond speech pathology, interacting with HCPs to rebuild their communication skills extended to surgery/dentistry (Jennifer and Susan), audiology (Brian), and lymphedema management (Susan).
Reintegration into society was another communicative challenge. Participants described steadily re-engaging in socialization as key to overcoming anxieties. Brian recalls, “I found that my facial changes, which I was acutely aware of, didn’t seem to register with others. That realization eased my anxieties.” Maria shared, “I felt like I had to constantly apologize for my sound. I didn’t want to explain, so I’d just say, ‘Hey, I had some mouth surgery.’” Long-term communication rebuilding also occurred, including adjusting to using an electrolarynx (Craig) or voice prostheses (Wayne and Keith), using hearing aids (Brian), managing fatigue’s impact on communication endurance (Brian), and dealing with confidence issues (Susan). Reflecting on recovering, Maria captured the essence of rebuilding her identity and communication: “Our sense of self and purpose, whether we want to admit it or not, is so reliant on these faculties. When they’re taken away, we need strong resilience and self-compassion to continue living with these changes.” She developed the mantra “Face Everything And Reclaim (FEAR) … But now I can look at myself and think, ‘Wow—I’m healing, and yes, I’m sounding better.’”
Discussion
We investigated the healthcare experiences of people with HNC-ACCs, employing an IPA methodological framework. From nine semi-structured, in-depth interviews, six GETs were generated, describing the healthcare experiences of people with HNC-ACCs. The use of IPA enabled a deep understanding of the phenomena through the iterative and multiple levels of analysis including contextual and linguistic features underlying the participants’ statements (Smith et al., 2021). Using IPA with a focus on HNC-ACCs, we were able to further our understanding of communication changes within the healthcare context. However, in HNC, communication is not the sole variable that changes. Within the interviews, participants often segued to other changes to themselves, such as eating and drinking, airway management, pain, aesthetics, and psychological well-being, suggesting that they did not delineate changes to discrete clinical areas. Using supported one-to-one interviews enabled the participants to talk at length, providing detailed recall of events creating rich data for analysis. Conducting interviews post-primary treatment enabled an understanding of the “ongoingness” of HNC and a need to constantly (re-)engage with healthcare well after primary treatment.
The primary treatment phase is marked by brutal changes to self and communication abilities especially when tracheostomized or with inadequate ways to communicate. This leaves participants vulnerable and traumatized but valuing human connectedness as a coping mechanism. Such experiences can be likened to other non-vocal hospitalized populations (i.e., those in critical care) who experience anger, withdrawal, reduced communicative effectiveness, and changes to identity (Carroll, 2007; Foster, 2010; Freeman-Sanderson et al., 2018; Happ et al., 2011). In our study and others, there are mixed descriptions of the experiences and effectiveness of alternative communication methods, whereas stronger relationships and meaningful interactions with HCPs support this non-vocal period, making patients feel safe and less anxious (Carroll, 2007; Foster, 2010; Freeman-Sanderson et al., 2018; Karlsen et al., 2019).
Upon becoming a patient, people with HNC inhabit an unfamiliar world with fear and uncertainty dominating, and are dependent on HCPs. Treatment-induced functional impairments can result in erosions of self-image and a catastrophic attack on sense of self (Lang et al., 2013; Turpin et al., 2009). A cancer experience involves two stages of liminality: first, “acute liminality” when patients undergo unpredictable existential changes upon diagnosis (Little et al., 2022). This is followed by “sustained liminality,” a prolonged state extending beyond hospital discharge where patients oscillate between disturbance and resolution while developing into their new post-treatment selves (Little et al., 2022). By focusing on ACCs, our study found that one part of this self-image change is in the role as a communicator. From the initial existential changes of being a changed communicator, individuals start to rebuild their communicative selves within healthcare settings before transferring these adaptive skills to more complex, naturalistic social environments. In our study, family support during healthcare was pivotal, providing not only advocacy and emotional support but also assisting with liminality. Participants with infrequent support often turned to HCPs or peers to assist with liminal adjustment. For people with HNC, hospital environments serve as safe spaces where they begin liminal adjustments to changes in appearance, eating, drinking, and speaking (Dawson et al., 2019). This study found that the healthcare environment facilitates supported adjustment, providing individuals with opportunities to practice communication skills in a structured and accommodating space buoyed by clinical expertise and compassionate care, therefore setting up adaptive and resilient skills for broader social interactions. Importantly, participants described a need to re-engage with healthcare services at various points post-treatment—sometimes weeks, months, or years later—as communicative challenges persisted, new ones arose, or new liminal adjustments emerged.
Gulliver et al. (2023) found a major issue facing cancer survivors in Australia was difficulties accessing services for both their mental and physical health, with care coordination challenged by complex funding models. Our participants appreciated coordinated care, but even when participants had access to care coordinators, they still encountered difficulties navigating services. Inconsistencies navigating healthcare resulted in increased patient burden, distrust, and frustration, resulting in patients choosing to access different health networks when needs were not met in the primary treating service.
Lalazaryan and Zare-Farashbandi (2014) investigated various models of health information seeking and concluded there were three categories of patients. The first was “active seekers” and the second was “passive recipients.” In our study, active seekers engaged with multiple sources of information to achieve their informational needs (e.g., HCPs, peers, the internet, social media, and written materials), whereas passive recipients tended to receive information during healthcare consults. A third category was information “blunters,” those who actively avoid gaining information (Lalazaryan & Zare-Farashbandi, 2014). While this category is represented by participants reporting avoidance of information as it was overwhelming or they were not in the right mindset, there are information-related behaviors which sit outside these categories. First, there were those who reported not being told of potential outcomes (which may be true, rather than being blunters) while others did not relate the information given to their situation, due to not realizing its personal relevance, and they had to actually live through the treatment to be fully capable of understanding what they had been told. Importantly, participants were not always consistently demonstrating the same behavior within or across time points, suggesting great fluidity in how people react to information across the healthcare continuum and how people with HNC-ACCs are not limited to a certain behavior. This study reinforces previous findings that information-seeking behaviors vary depending on a patient’s position in their cancer journey (Eheman et al., 2009). There was a notable gap in how HNC treatment, especially for non-laryngectomees, may change someone’s communication abilities. Non-laryngectomy participants rarely recalled discussions about communication outcomes. There are many factors which may impact communication abilities post–HNC treatment, for example, surgery variable, tumor details, co-morbidities, radiation side effects, or access to speech pathology services, so outcomes may be challenging to exactly predict for people (Dwivedi et al., 2009).
Patient–provider therapeutic connection is made up of a variety of dimensions including shared mind, shared power, shared deliberation, caring nature, authenticity, trust, respect, and emotional support (Rathert et al., 2022). In our study, patient–provider connectedness encompasses all these but also such connection elevates individuals with HNC-ACCs from vulnerability to safety. In contrast, the absence of this connection can lead to deeper despair. The connectedness felt by participants is intertwined with the desire for expertise, resulting in a sense of being in the right hands. This is similar to findings in a laryngectomy-only cohort who wanted HCPs to not only be competent but to also understand their needs and respect them as people (Bickford et al., 2018). Gibson et al. (2022) reported that compassionate communication gives patients a sense of being heard and respected, and that a single compassionate HCP can assist with coping. This study builds upon those findings, emphasizing the importance of human connectedness in overcoming isolation and fear associated with HNC treatment. Even simple, empathetic gestures or conversations can provide comfort and reassurance. The absence of connection has detrimental effects, evoking feelings of fear, anger, and distrust, lingering well past treatment. Patients and HCPs can form meaningful connections, even non-verbally, suggesting that communication changes can be overcome. Additionally, there is hope from patients that these connections can improve the lives of HCPs through mutual bonding, therefore leading to not only enhanced patient experience but also enhanced human experience within the healthcare setting.
Limitations
Participants who were mid-treatment either requested to wait for completion of treatment or did not consent at follow-up; therefore, interviews were all retrospective in nature, although many were still engaged in healthcare services. Participants identified themselves as White or Anglo Australian with one participant describing themselves as Italian. No participants identified as First Nations People of Australia, who experience higher incidence, higher mortality rates, higher burden of HNC, and also poorer access to HNC services compared to non-Indigenous Australians (Gupta et al., 2016; Khan et al., 2024). Despite interview support strategies in place, funding for interpreters, recruiting from four demographically different hospitals, and multiple support groups, people with permanent non-verbal forms of communication or people with limited English proficiency did not participate. However, the pilot participant did not identify as White-Australian, one non-verbal participant began palliative treatment prior to interview, and two non-English speakers initially agreed but could not participate due to life circumstances unrelated to the study, suggesting that the recruitment strategy was inclusive of these groups. Other studies which focus on these vulnerable populations would be critical to understand how these groups may experience healthcare differently. Other data collection methods (e.g., observational methods and art-based methods) may be more inclusive for people who may have been deterred by interview methods (even with support strategies in place) or even capture those who are too overwhelmed to share their experiences, who may not have been deemed approachable by recruiting clinicians or not involved in support groups. Additionally, we did not seek the experiences of people undergoing palliative care, despite this group being less represented in the literature and these people may have different experiences (Checklin et al., 2024).
Clinical Implications
The findings highlight the need for healthcare systems and HCPs to be aware of the vulnerabilities of people with HNC while in their care. While it is acknowledged that not all health services can provide for every single individual’s need and some subdisciplines of expertise may not be core members of the team (e.g., dental services and lymphedema therapists), timely onward referral pathways to external services may mean patients can easily navigate the system and can have their needs met to rebuild themselves. It has been recommended that HCPs working with individuals with HNC undertake advanced communication skills training (such as trauma sensitive training) (Homer & Winter, 2024). Based on our findings, we would add that communication training incorporates supporting communication with people with ACCs. Additionally, HCPs need to ensure people with HNC-ACCs always have the required means to communicate based on their individual needs to not only interact with HCPs and family but also to support liminality and reduce anxieties. Given people with HNC-ACCs build a village of support including SOs who can help interpret medical information, it is essential that they are included in such counselling, even though they may have different information needs (Hoesseini et al., 2020).
Future Research
As per the limitations, there are future opportunities to explore the experiences of different ethnic groups, disenfranchised patients, or people with more severe communication deficits. This may be completed by incorporating other methods less reliant on lengthy interviews. Given the discussed concept of liminality and self-image as a communicator, further studies may investigate how these transitions occur and how patients can be best supported. Phillips-Salimi et al. (2012) suggest that to help HCPs understand behaviors that foster connectedness, staff education programs should be developed. Future research could investigate how tailored programs for HCPs working with people with HNC-ACCs may improve connectedness and create meaningful impact. Finally, the patient experience movement is moving beyond purely the patient’s perspective but to a more “human experience” of healthcare. Healthcare is not just about diagnosis or disease but must take an integrated view of what matters not only to patients but also to families and care partners, and the needs and vulnerabilities of HCPs (Adams et al., 2024). To fully understand the human experience of HNC-ACCs and healthcare, further research on the perspectives of others (i.e., families/HCPs) may provide valuable and different insights.
Conclusion
The study employed IPA to explore the healthcare experiences of people with HNC-ACCs, providing rich insight into the phenomenon. Findings illustrated that the healthcare experience is complex and a traumatic time for people with HNC-ACCs. However, there are also moments of human connectedness and gratitude for expertise which enable them to cope. Additionally, people begin to rebuild themselves safely within the healthcare system, preparing themselves for a changed future.
Footnotes
Ethical Considerations
This study was approved by the Monash Health Human Research Ethics Committee (approval no. RES-23-0000-155A).
Consent to Participate
All participants provided written informed consent, obtained by the principal investigator.
Author Contributions
Martin Checklin led the development and design of the study, coordinated recruitment, collected data, and led the analysis and the preparation of the manuscript for submission. Robyn O’Halloran, Rebecca Packer, and Abby M. Foster supported the lead author in the conceptualization of the study and throughout the conduct of the research, analysis of the findings, and preparation of the manuscript. Benjamin Dixon supported the lead author in developing the study, securing funding, recruitment, and preparation of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible thanks to the generosity of donors to the Epworth Medical Foundation, grant number EH2022-924. This research was completed in partial fulfillment of a PhD and further supported by La Trobe University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.