
Abstract
Sexual health and well-being (SH&WB) in late midlife is an important yet underexplored aspect of healthy aging. Satisfying sexual activity contributes to psychological and relational well-being, yet midlife is marked by physiological changes, health issues, and social transitions that can affect sexual functioning. Existing research has mostly focused on adults over 60 or on clinically diagnosed sexual problems, leaving late-midlife experiences largely overlooked. This qualitative study addresses that gap by examining how late-midlife adults (50–64) in Poland perceive and navigate SH&WB challenges, shedding light on their experiences. Forty participants (25 women, 15 men) took part in semi-structured, in-depth interviews, and reflexive thematic analysis was applied. Many participants did not identify themselves as belonging to the “aging” group, often describing themselves as “too young” to experience age-related sexual concerns. Consequently, common changes (e.g., lower libido, vaginal dryness, and erectile difficulties) were seldom perceived as distressing or problematic. Participants typically managed these changes independently through creative, tactful strategies and by addressing psychosocial factors, reserving help-seeking for instances of severe distress or disruptions to sexual activity. These findings suggest that healthcare providers should respect late-midlife adults’ perspectives and avoid over-medicalizing normal sexual changes. Instead, SH&WB should be integrated into routine care in a supportive manner that encourages open dialogue and proactive engagement, laying the groundwork for assistance if future needs arise.
Keywords
Introduction
Sexual activity remains an important aspect of life across the lifespan, and evidence shows that many individuals in midlife and beyond continue to express interest in sex and engage in partnered and solo sexual behaviors (Lee et al., 2016; Smith et al., 2019; Træen et al., 2019). Maintaining a sexual life during middle and older age can significantly contribute to psychological well-being and relational satisfaction. However, midlife is also marked by the emergence of various physiological changes, health conditions, and life transitions—such as career developments, widowhood, and care-giving responsibilities—which can affect sexual expression and pleasure, for example, through fatigue or stress, impacting sexual desire (Briken et al., 2020; Burghardt et al., 2020; Hendrickx et al., 2015; Wellings et al., 2023). Although adequate information, education, and care regarding sexual health are essential for a satisfying sex life—and have been recognized as a fundamental right across all ages and life stages (WAS, 2008)—adults in midlife and older often report low usage and limited access to sexual health services (Agochukwu-Mmonu et al., 2021; Hinchliff et al., 2020; Hobbs et al., 2019).
In this paper, we examine how adults in late midlife perceive and navigate challenges related to their sex lives, with a focus on their experiences of sex and their help-seeking behaviors regarding sexual function and well-being. Late midlife can be viewed as an important phase in the life-course, offering opportunities to sustain a satisfying sex life into older age, while also presenting challenges related to shifting personal and professional circumstances, including changes in health, family roles, and work responsibilities. Existing scholarship on sex and aging tends to concentrate on individuals aged 60 and older or those with clinically diagnosed sexual dysfunctions. There is a paucity of research evidence on how late-midlife adults without such diagnoses experience their sexual lives and tend to their sexual well-being.
Midlife as a Unique Phase in Life
Midlife, also referred to as “middle-age” or “middle adulthood,” is typically defined as the period between ages 40 and 60 and represents a critical yet understudied stage of human development (Lachman et al., 2015). To counter the dominant cultural narrative of the “midlife crisis,” recent scholarship reframes this life stage as one marked by complex and unique transitions “that include a focus on balancing gains and losses, linking earlier and later life periods, and bridging generations” (Infurna et al., 2020, p. 470). Research suggests that many adults in midlife experience this period as a mix of opportunities and challenges: freedom from expectations, plethora of possibilities, and a maturity-driven self-acceptance are often intertwined with a growing awareness of life’s finitude and elevated levels of stress and anxiety (Arnett, 2018; Dolberg & Ayalon, 2018; Melinda et al., 2023; Thomas et al., 2018).
Late midlife in particular may bear a pivotal period for sustaining sexual satisfaction into older age. For many adults in midlife and beyond, sexuality remains a meaningful aspect of life, with a fulfilling sex life closely linked to overall well-being and indicators of successful aging (Buczak-Stec et al., 2019; Štulhofer et al., 2018 Træen et al., 2019). However, this stage is also marked by gradual physiological and health-related changes, including hormonal and reproductive transitions—such as menopause—and a rising prevalence of chronic illnesses (Boyd & Bee, 2019). As many long-term health conditions that impact sexual functioning are diagnosed during this life phase (Lee et al., 2016), important questions emerge around how individuals in middle adulthood navigate their sexual well-being in the context of potential sexual difficulties. 1
This article uses the term sexual health and well-being (SH&WB) to encompass both clinical and experiential dimensions of sexuality, particularly as they relate to individuals in late midlife. SH&WB includes not only the clinical aspects typically associated with sexual health—such as disease prevention, infection management, contraception, and safe sex practices—but also the more holistic and subjective elements captured by sexual well-being, including feeling good and functioning well within one’s sexuality (Mitchell et al., 2025; WAS, 2008). While these facets are often discussed separately, this integrated framing reflects the need to approach SH&WB as a comprehensive concept, essential for supporting a satisfying and healthy sex life throughout midlife and beyond (Bauer et al., 2016).
Research on Sexual Functioning in Midlife
Amid rapid global population aging, healthy aging has gained prominence as a key international priority, with healthy sexual aging recognized as one of the core components of this agenda (Træen & Villar, 2020). This recognition has contributed to a growing body of research on sexuality and SH&WB in older adulthood (Sinković & Towler, 2019; Træen et al., 2016). However, much less attention has been paid to sexuality in midlife as a distinct and unique life stage. Within existing studies on late-midlife adults (typically aged 50–60), two notable tendencies emerge: first, research often concentrates on individuals with clinically diagnosed sexual problems, commonly recruited from medical settings; second, studies frequently group middle-aged and older adults together, treating them as a homogeneous population and obscuring the unique experiences of those in late midlife.
The first approach is evident in a substantial body of clinically oriented research that focuses on specific health conditions or sexual health concerns, such as menopause, erectile dysfunction (ED), hypoactive sexual desire disorder, and dyspareunia or vaginismus. While these studies acknowledge the distinctiveness of midlife, they are predominantly framed through a biomedical lens, positioning gendered sexual issues as defining aspects of this life stage (Avis et al., 2017; El Khoudary et al., 2019; Waetjen et al., 2018). Probably due to the medicalization of menopause and ED, these topics dominate midlife literature which is, as a result, skewed toward single-gender studies.
The second approach, where middle-aged individuals are “bulked up” with older adults, can be seen in studies that focus on people aged 50 and over. The term “older adults/men/women” frequently appears in study titles and bodies of text, even when participants include individuals in their early 50s (e.g., DeLamater, 2012; Schick et al., 2010; Stowell et al., 2023). While broad age ranges facilitate age-based comparisons, many of these studies draw conclusions about “older people” or “later-life sexuality” based on analyses of the entire sample (James et al., 2023; Lu et al., 2020; Schafer & Upenieks, 2023). This lack of differentiation limits our understanding of the nuances in SH&WB across different stages of later life (Hinchliff, 2016).
Sexual Problems in Midlife
While it is widely accepted that sexual activity and function tend to decline with age (Lee et al., 2016; Mitchell et al., 2016; Schick et al., 2010), research shows that only a few sexual problems—namely, ED and vaginal dryness—become consistently more common with age (Hendrickx et al., 2015; Mitchell et al., 2016; Moreira et al., 2008; Quinn-Nilas et al., 2018; Richters et al., 2022). For other sexual difficulties—such as low interest or arousal, trouble reaching orgasm, pain during sex, or anxiety about performance—the picture is less clear. Some research indicates that the prevalence of specific problems increases consistently with age or peak in (late) midlife (Briken et al., 2020; Hendrickx et al., 2015). Conversely, other studies suggest that they become less common in people in their 50s or show no significant age effect between midlife and older adulthood (Mitchell et al., 2016; Quinn-Nilas et al., 2018; Richters et al., 2022). In a study by Fischer and Træen (2022), Norwegians aged 45–59 were actually less likely to report sexual problems than those aged 30–44. These inconsistencies may stem from variations in how studies define and measure sexual problems (e.g., wording, symptom duration, and perceived severity), which age groups are used in analyses, or cultural differences (such as how much emphasis people place on intercourse versus other forms of sex; see Gore-Gorszewska & Ševčíková, 2023).
In addition to symptoms, according to the Diagnostic and Statistical Manual of Mental Disorders, sexual issues are only problems if they cause distress. Research shows that distress is generally reported less frequently than symptoms themselves, across both genders and age groups (Briken et al., 2020; Lee et al., 2016; Richters et al., 2022), and tends to decrease with age (Briken et al., 2020; Graham et al., 2020; Hald et al., 2019; Hendrickx et al., 2015). However, findings on sexual distress during midlife are mixed. Some studies suggest it peaks in this period, while others find it remains steady or declines from midlife onward (Briken et al., 2020; Hendrickx et al., 2015; Mitchell et al., 2013). For instance, the UK-based Natsal-3 survey found that sexual distress peaked among men aged 55–64 but did not vary by age for women (Mitchell et al., 2013). Still, many studies do not break down distress data by specific age groups (e.g., Richters et al., 2022), and most are quantitative, limiting what we know about middle-aged adults in particular.
Seeking Information or Support Related to Sexual Health and Well-Being at Midlife
Research consistently shows that few adults seek help for sex-related concerns as they age, with less data available on midlife populations than older adults. In a cross-national study of people aged 40–80, only 20% in Europe and the non-European West had sought medical or psychological help for a sexual problem (Moreira et al., 2005). More recent data from four European countries found that among adults aged 60–75 experiencing a sexual problem, just 12% of men and 7% of women had sought professional help within the past five years (Hinchliff et al., 2020). Similarly, only 17.3% of community-dwelling U.S. adults aged 65–80 reported discussing sexual health with a healthcare provider in the past two years (Agochukwu-Mmonu et al., 2021).
Research points to several reasons why older adults may avoid seeking help for sexual problems. These include low levels of distress, viewing symptoms as a normal part of aging, hoping the issue will resolve on its own, and feeling embarrassed, ashamed, or anxious about how doctors might respond (Bauer et al., 2016; Fileborn et al., 2017; Gore-Gorszewska, 2020; Hinchliff et al., 2020; Teo et al., 2022). Some also worry that healthcare professionals (HCPs) lack the necessary training and knowledge (Ezhova et al., 2020). Instead, individuals may turn to online sources for information or support (Ševčíková et al., 2023). However, research specifically exploring how middle-aged adults experience and address SH&WB concerns remains very limited.
The Current Study
As noted, late middle adulthood is often accompanied by emerging health issues that can impact sexual functioning. While a decline in sexual frequency with increasing age and the chance of experiencing sexual issues increase, these changes are not universal—their timing, severity, and the distress they may cause can vary. There is limited research on how midlife adults experience the changes and respond to challenges in their SH&WB. Studies that rely solely on clinical populations or combine middle-aged and older adults, as noted above, risk overlooking the unique experiences of this life stage. To help fill this gap, the present study explored how late-midlife adults perceive the changes and navigate existing (or prepare for anticipated) SH&WB challenges, and whether they view them as problems that require help.
Materials and Methods
Sample Characteristics (N = 40)
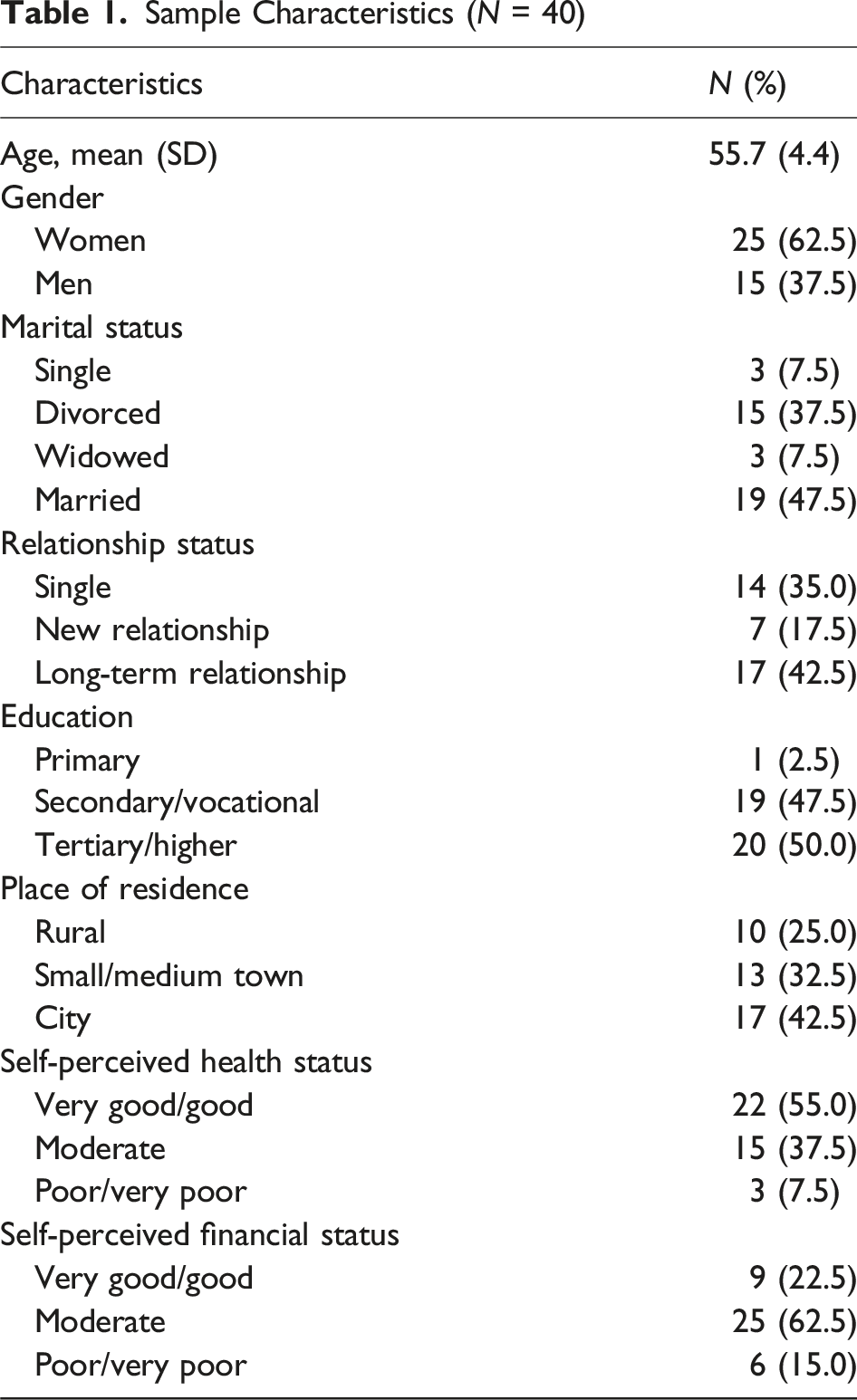
Semi-structured, face-to-face interviews were conducted by the first author and two trained research assistants (graduate psychology students). Using a broad interview guide (see Table 2, supplemental material), the interview covered a range of topics but followed a conversational format that allowed participants to introduce topics important to them and enabled interviewers to explore experiences unique for each individual’s biography. Interviews took place at a location chosen by the participant—typically either a private university office or their home—and lasted between 1.5 and 2.5 hours. All interviews were audio-recorded.
To establish trust and credibility, each interview began with the interviewer introducing themselves and clearly explaining the study goals and procedures of qualitative data collection. This also included outlining participants’ rights, such as the ability to withdraw at any time, decline to answer specific questions, and the measures in place to protect their anonymity. Interviewees were assured that pseudonyms of their choosing would be used instead of names and any identifying information removed from transcripts. After signing informed consent and completing a brief demographic questionnaire, interviews began with general questions about the participant’s background and relationship history. This approach helped build rapport, essential for discussing sensitive topics, before moving toward more sensitive questions about their sex life. Participants received PLN 150 (approx. EUR 35) as compensation for their time.
During debriefing, none of the interviewees expressed discomfort or distress; on the contrary, many reflected on the conversation as pleasant, thought-provoking, or personally meaningful. They frequently emphasized the interviewers’ respectful and tactful demeanor as key to fostering rapport and encouraging openness. The interviewers’ younger age (20s–30s) did not appear to inhibit participants’ disclosure, nor did gender—participants were given the option to choose a female or male interviewer. Many stated they were motivated by a desire to contribute to scientific knowledge, viewing the interviewer as a professional rather than focusing on their demographic characteristics. To ensure confidentiality, during the data collection and analysis, no third party was present during the interviews, no personal details were retained, and recordings were anonymized by the interviewer prior to transcription by the professional service. Only the first author had access to the full set of transcripts, which were kept on a password-protected computer. All study procedures were reviewed and approved by the Research Ethics Committee at the Institute of Psychology of the Jagiellonian University.
This paper focuses on the themes identified through qualitative data analysis that addressed the question “How do middle-aged adults perceive and navigate existing—or prepare for anticipated—SH&WB challenges?”. The data analysis adhered to the principles of reflexive thematic analysis (Braun & Clarke, 2021), following established steps required to ensure analytic quality and the trustworthiness of findings. The first author familiarized herself with the data through multiple readings of a subset of transcripts (n = 10) and noted down initial ideas. The coding process followed. The initial coding categories, as related to the research question of this paper, encompassed (i) planned codes, for example, experiencing sexual problems/difficulties, interest in one’s SH&WB, and ways of addressing sexual concerns, as well as (ii) the notions that emerged from the interviews, for example, reasons for lack of interest, component of distress, and changes but not problems (deductive–inductive approach). To ensure the validity of the coding, selected transcript excerpts relevant to the current research question were independently coded by the coauthors and outcomes were discussed collaboratively. Codes were then consolidated into a set of candidate themes, reviewed for internal homogeneity and external heterogeneity. The reviewed themes were organized into a thematic map with illustrative quotations, reviewed and refined in discussion with coauthors, and subsequently applied to the remaining transcripts by the first author. Additional in vivo codes identified in the process (e.g., Too young to think about these topics, No sex so no problems) were then reviewed and used to modify the existing structure, forming the final thematic map (Figure 1), which was again discussed and agreed upon by all authors. Final Thematic Map: Participants’ Ways of Perceiving and Navigating SH&WB Challenges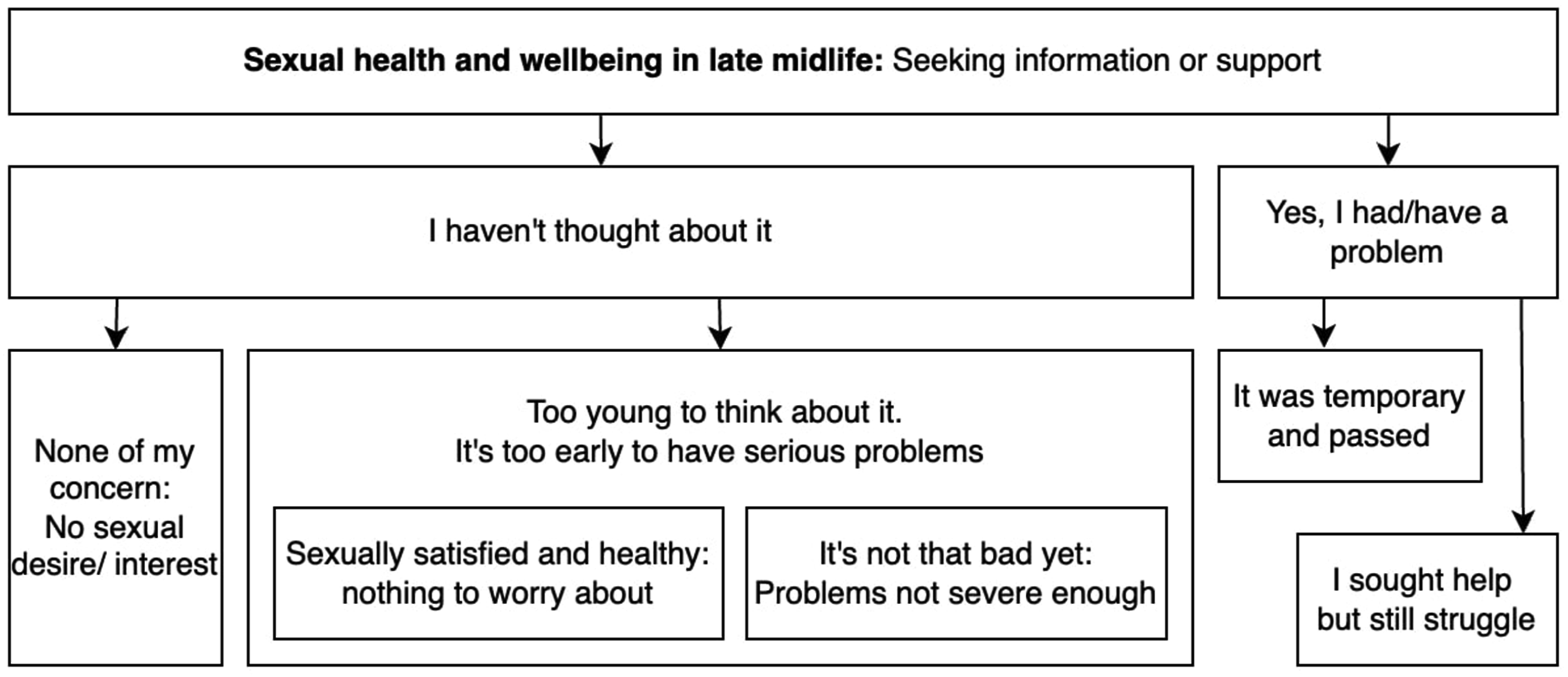
Analytical rigor was maintained throughout the recurrent discussions between the coauthors and by keeping a transparent audit trail in the form of detailed analysis notes. To ensure analytic transparency and data richness, and to allow the reader to evaluate the elements of the analysis and its interpretative conclusions, participants’ direct quotes have been provided. All quotations were translated by the first author and verified by an English native speaker.
Results
The dominant theme identified during analysis was a lack of consideration of sexual health or addressing sexual concerns. Indeed, “I haven’t thought about it” was a leitmotiv, a recurrent point the participants made when discussing SH&WB, including changes in own sexual functioning, concerns about sexual functioning in the context of aging, or experiences with help-seeking behaviors. Participants differed regarding rationale for not paying attention to these topics, to some extent reflecting their life situation and relationship context. Responses ranged from being single and simultaneously not interested in sex to being in a long-term relationship with a satisfying sex life. Only six interviewees mentioned experiencing distressing sexual problems.
Too Young to Think About It: Us Versus Them
The participants almost unanimously said no when asked whether they actively sought any information about sexual functioning for their age. It was clear from the analysis that many considered themselves too young to think about this topic. One respondent, Evo, mother of two, encapsulated this sentiment by stating, “At 50, I don’t feel my age yet and don’t view myself as part of an aging generation or approaching older age. It’s still too early” (W50, married, satisfying sex life). Another participant, Adam, enthusiastically approved the interviewer’s introduced terminology (i.e., middle adulthood) when addressing his age range: “Excellent! I love it! It used to be called ‘older age’, which I totally do not identify with” (M51, remarried). Also, Atydorfa, woman in her 50s, expressed an internal disapproval of linking the 50+ age with terminology typically associated with older age, a disapproval shared by many interviewees: “I sometimes hear about ‘geriatric sex after 50’ in the media, or comments like ‘how is it possible that people over 50 still have sex?’, it gives me angry shivers” (W56, separated, new living-apart-together relationship). Participants, thus, did not associate themselves with being “older” and certainly not with the sexual problems they believed “older adults” could experience.
Indeed, an “us versus them” discourse was evident in the data. For example, Timothy dismissed the idea of seeking information or advice about SH&WB at his age: “I think there is such literature. I didn’t get to it because I wasn’t interested in the topic yet. I don’t experience changes of this kind [age-related]. But certainly, when it begins, I will look for it [information]” (M56, separated, searching for new relationship). He then elaborated on the changes he had mentioned by referencing the overall health deterioration he observes in his parents and admitted being concerned about the “prospect of old age.” On a similar note, Happy, satisfied in her marriage, drew from her daily experiences with the older individuals she supports at work to illustrate how differently she perceives her current sex life: I am aware of what it can be like. I work with seniors; I know what it is like, and I expect it will get worse [for me] one day. But if time would stop right now, it would be perfect (W53, long-term marriage).
Interestingly, interviewees often used the term “seniors” or “old(er) people” (seniorzy or starzy/starsi ludzie in Polish) when referring to individuals in their late 60s or older: a categorization which emphasizes the distance they felt, psychologically, from their own middle-age group. One participant commented on how, in his opinion, the aging process significantly impacts (sexual) capabilities only at later stages of life: “Well, it is known that when people are 65 years or older and have actually lost their sexual abilities …” (M56, divorced, single). This suggests that such an age difference may be enough for some individuals to maintain a sense of distance from the concept of “aging.” Overall, the lack of identification with the older or even aging generation was a recurring theme in participants’ narratives. 2 This sentiment, usually raised when discussing general sexual functioning or their approach to addressing sexual problems, can be therefore understood as one of the reasons for participants not taking SH&WB topics into consideration.
Sexually Satisfied and Healthy, So Nothing to Worry About
Many participants who did not reflect on their SH&WB narrated their current sexual life as satisfying. For instance, Alexander, a 56-year-old man married for 30 years, content with both his overall health and the quality of his sex life in marriage, reported never consulting any specialist and never being asked by any HCP about sexual problems. He concluded, “It’s not the time yet to have any [problems of this kind],” hence his lack of concern. In a similar tone, Bala, a 58-year-old woman in an informal, long-term relationship with a partner 10 years younger, expressed her deep satisfaction with their sex life, which she described as “great.” She firmly and merrily stated that she has not observed any impact of current menopause on her sexual activity or sex drive: “Definitely not. In my case, it [menopause] may affect other aspects [of my life], but not this one [sex life] (laugh)” (W58). On top of satisfaction with their sex lives, interviewees like Bala and Alexander also considered their overall health and well-being as contributing toward their indifference regarding sexual health–oriented behaviors. The prevailing sentiment was that as long as the participants’ (sexual) functioning does not substantially differ from earlier experiences and they are satisfied, the need to proactively address SH&WB remains minimal.
Interestingly, it was clear from the analysis that several participants did not perceive it necessary to actively engage with their SH&WB (e.g., by seeking information or consulting specialists) despite acknowledging age-related changes in their own sexual functioning. Once again, the pivotal factor was the presence of a fulfilling sex life. Book_Lover, a 56-year-old man, divorced for many years and currently in a new relationship for two months, reported that he had not encountered any sexual problems so far. Despite the acknowledgment that his erection is “less firm than it used to be,” he expressed satisfaction with his current sexual functioning. Consequently, he did not consider consulting his sexual health with anyone. Another interviewee, Irene, a 55-year-old married woman, concluded that she “feels like a princess” after describing how her husband tends to her sexual needs through massages, intimate touch, and kissing. Reflecting on her ongoing menopause, Irene acknowledged a decrease in libido but clarified that it does not bother her: “I think it always decreases [during menopause], but not enough to [bother me]. I’d say it is completely irrelevant to me. I like being [intimately] touched. Always” (W55, married for 33 years). This sentiment was echoed by another female participant, Happy (53), also in a long-term relationship. Happy received vaginal globules prescribed by a gynecologist for menopause-related vaginal dryness. Despite the medication having a rather weak effect, Happy claimed not being troubled by this and explained, “There are so many ways to manage it and have fun […] I experience it rarely, and if, there are myriads of alternative forms [of sexually satisfying each other], so it does not pose any problem” (W53, married for 30 years). In both accounts, applying a wider repertoire of sexual behaviors proved beneficial when faced with age-related changes in sexual functioning. Even after experiencing recent health problems and medical procedures that she and her husband underwent, Happy still did not perceive any sexual issues: “You know, I haven’t thought about it because I don’t have any problems. Probably, if there was a problem, I would have started thinking about it” (W53). Apart from another instance of this study’s leitmotif (“I haven’t thought about it”), Happy’s account of not viewing occasional vaginal dryness as a sexual problem highlights the crucial role of subjective interpretation, a concept elaborated further below. Collectively, the participants’ perspectives suggest that when individuals experience a subjectively satisfying sex life, even acknowledged age-related declines in sexual functioning are not perceived as problematic and therefore do not prompt further engagement.
“It’s Not That Bad Yet”: Problems Not Severe Enough
The findings demonstrated that behaviors like seeking information or consulting specialists tended to be absent unless the sexual changes reach a subjectively severe level and cause notable distress. Adam, a 51-year-old married man, highlighted this perspective through observations of his peers. In friendly conversations, some expressed concerns about being “on a slope of decline”—still “functional” but past their sexual peak. The issues they experienced, however, were not perceived as severe enough to prompt action. Adam’s and some other participants’ voices suggest that the ability to engage in penetrative intercourse may define this threshold of perceived severity.
The comparative severity of changes in sexual functioning was illustrated by Terry, a 58-year-old female married participant, who mentioned experiencing decreased libido and vaginal dryness. She accepted a lubricant gel as per her gynecologist instruction; however, she did not raise the issue of her decreased libido, even though she described this gynecologist as reliable and “like a friend.” Terry explained how she found ways of managing the situation by occasionally “pretending not to understand” when her husband signals his sexual interest or by orally satisfying him during sex, although the way she narrated it indicated not being very comfortable with oral sex. She gave a comparative example of her female friend, whose intense pain during intercourse makes penetration impossible, effectively preventing that person from enjoying sex. By comparison, Terry considered her problems as minor, thus not requiring intervention. A similar account came from Joseph (53), married for over 30 years, who shared insights regarding his own and his wife’s health problems and medical procedures, and discoveries of potential sex-related side effects of pharmacotherapy he was prescribed in the past. Joseph concluded, “Many people have problems. In my opinion we do not have such severe problems, right? Nothing that would cause severe discomfort or eliminate… Our ability to have sex” (M53, married). He expressed openness to the idea of actively seeking information or support, like he had in the past, but indicated that their current situation (i.e., wife’s post-surgery occasional pain during intercourse and his mild erectile problems) can be managed without external consultations, via adjusting sexual positions and engaging in longer foreplay. These accounts demonstrate that some participants find a way to manage the changes in sexual functioning or prefer not to pay attention to them. They consider seeking information or professional support only when the situation becomes subjectively severe and distressing.
Interestingly, some participants were somewhat skeptical about discussing less-than-severe sexuality-related concerns with healthcare providers, sensing that doctors’ clinical orientation largely overlook the emotional and relational dimensions of sexual well-being. Encounters mentioned by several interviewees who otherwise reported no severe sex-related problems suggested that consultations were narrowly confined to anatomical or physiological aspects, often at the expense of a more comprehensive conversation. One participant recalled that her doctor talked to her “strictly… strictly about the physical [aspects]” (W53) omitting any reference to sexuality itself. Kunegunda, a 58-year-old woman in a new relationship, echoed this viewpoint, remarking that a gynecologist “does his job, checks, that’s it” (W58), with “checking” understood as screening for serious illnesses like cancer or endometriosis. This left her unconvinced that they would be open to discussing any aspect of her sexual life beyond basic physiological function or dysfunction. Such experiences apparently fostered some of our participants’ impressions that HCPs are rather reluctant or unable to engage beyond strictly physiological assessments, possibly also contributing to their stance that seeking professional medical help is reserved for severe sexual difficulties.
None of My Concern: No Sexual Desire/Interest
Several female participants were not sexually active and had no interest in the SH&WB-oriented behaviors. From their perspective, if they were not engaged in any sexual activity, neither partnered nor solo, and had no intention of resuming such activity, addressing their SH&WB was irrelevant. While Monique, a 57-year-old widow, expressed disinterest in sex following her husband’s death four years ago, Bea (58) navigated the challenging terrain of endometriosis cancer and divorce with an unsupportive husband, prioritizing pain relief during illness over any sexual desires. Both emphatically stated that the sexual chapter of their lives had concluded, and therefore, they saw no reason to maintain any interest in their sexual health.
Two other women explicitly voiced their (almost) non-existent sexual desire, with a notable lack of distress associated with it. Agnes, aged 55 and in good health, narrated embracing her post-menopause loss of interest in sex which she viewed positively: - Agnes: That [sex] doesn’t interest me at all. I don’t think in terms of sex at all, to be honest. For example, I used to look at a man and think to myself “he’s pretty cool, I could consider him.” Now I think “you’re handsome, and that’s it. I’m not interested in you at all.” That’s the stage I’ve reached (laughs). - Interviewer: Okay. Do you see this change as something problematic, bothering you? - Agnes: No, no! Not at all. As a natural process. It’s just the way I am and I’m happy with it.
Similarly, Cloud (52, divorced, single) went through a decade of singlehood marked by very low libido with occasional masturbation. She awaits menopause, expecting these sporadic needs to vanish completely. These women’s accounts were devoid of any notion of discomfort, sadness, or other negative feelings related to their low or lack of desire, which may explain why they did not view it as a problem. From their perspectives, engaging in any behavior oriented toward SH&WB, such as seeking information or advice for the changes they experience, was unnecessary.
Yes, I Had/Have a Problem…
Six participants expressed genuine concern about their self-reported sexual problem that required some level of intervention, while another participant narrated more general struggles. Five cases related to erectile problems—self-reported by men or by women about their partners—while one case involved low desire reported by a female participant. The latter was shared by Beatrix (58), who remarried eight years ago to a younger partner. She articulated her diminished desire in these words: My husband wants, and I simply don’t want. I don’t have the drive like I used to. Don’t get me wrong, we do have sex, and I like it, but it takes me a very, very long time to get aroused (W58, remarried).
While she declared contentment in her current relationship and expressed great enjoyment of partnered intimacy, she admitted distress over the decrease in desire. After discussing this problem with her husband, she tried to consult a gynecologist during a menopause-related visit. However, without being asked for details she was promptly prescribed a lubricant, which helped with vaginal dryness but did not address the main issue of low desire/arousal. Beatrix was uncertain about the course of action: “I don’t know what to do now, it is really bothering me,” and throughout the interview, she sought reassurance on whether and how to raise the topic again during the next gynecological consultation.
An intriguing perspective was voiced by a male participant, Roman, aged 63, divorced and seeking a new relationship. While Roman vaguely mentioned that “we all have some problems” without delving into the specifics of his own challenges, he highlighted that his major struggle lies in “how to express yourself, how to ask” about sexual issues. It was observable throughout the interview, as Roman frequently paused in search of words, resorting to metaphors and euphemisms. He recounted his experiences with HCPs, including a urologist and a psychologist, who asked generic questions and offered brief recommendations without providing ample space to elaborate on the matter that Roman was struggling with: They check if you’re OK, if you’re sleeping, if you want any pills. They may even say “make love as much as possible to live long.” Such short comments! But anything more … There is no further information, no advice. Just “goodbye, off you go.” (M63)
Consulting healthcare specialists may prove challenging for individuals like Roman or Beatrix who, possibly due to their limited experience in discussing sexual topics, struggle to articulate their queries quickly and precisely and leave without resolution or concrete support for their concerns.
In contrast to the above, distressing erectile problems mentioned in several interviews were all resolved, without seeking specialist consultation. They were universally interpreted by the participants as transient, usually linked to stressful life circumstances. Two male participants recounted how an exceptionally stressful work situation had preoccupied their minds to the extent that they were unable to relax at home and focus on sexual interactions. After successfully addressing the work-related issue, their sexual functioning returned to its previous level, as in case of Aleksander: It was generally just a problem that I had to solve at work, and it affected my psyche, unfortunately, yes? It was such a difficult task that it absorbed me too much. And the moment it got resolved at work, it all [sex life] went back to normal. (M56, married)
The other male participant recalled some online reading on the topic. In a similar vein, three female interviewees narrated their male partners experiencing temporary erection problems, which they attributed to fatigue and work-related stress, or an elevated blood sugar level (onset of diabetes) in case of Letta’s (51) partner. Evo, a 50-year-old woman married to a man several years older, described it as follows: [My husband] handled the problem. He said “I know it’s the stress, it’s related to the stress,” because he actually works a lot. I think that was the major factor in all of these problems. […] He couldn’t finish [ejaculate]. And he was a bit scared about it. But I said “we’ll see, take it easy for now.” When we approached the subject a second time [had sex again], it was no longer a problem. We talked it through, I said “relax, no stress, I don’t know, let’s buy some lube gel.” So, we bought the gel, tried again and there was no more problem. Everything was ok.
Strategies to address the issue, as remembered by female interviewees, included “taking it slowly,” advocating for some rest, and abstaining from sex for a brief period; in case of suspected onset of diabetes, diet and exercise was introduced by Letta’s partner. These approaches proved successful in resolving the problems without necessitating further action. Evo and Letta added that should their partner’s erectile problems reappear and become persistent, distressing for them, they may consider consulting a sexologist. These findings highlight how late-midlife couples navigate the landscape of distressing sexual problems, preferring often to deal with it on their own. Clearly, addressing a sexual problem within the relationship was done tactfully and in support of the partner.
Discussion
Contrary to what the literature on the high prevalence of sexual problems and distress in late middle-adulthood led us to believe, the majority of participants in this study had not felt the need to seek SH&WB information or support. Reasons for not seeking sexual health advice highlighted in research with older adults include stigma, ageist stereotypes, embarrassment, and strained patient–provider relationships (Bauer et al., 2016; Ezhova et al., 2020; Teo et al., 2022). Yet, the current study found a different, more nuanced rationale for midlife adults not seeking SH&WB information or support, namely, not thinking about it, not considering it relevant in their current life situation, or successfully managing some mild changes without external professional help. These findings raise several points worthy of further research and clinical consideration.
First, our results indicate that some late-midlife adults do not consider that they belong to the “aging” group and do not feel old at all (Dolberg & Ayalon, 2018). It resonates with Hinchliff and Gott’s (2008) observation of their midlife female participants (mean age 62) rejecting the “asexual discourse of aging for themselves” but accepting it when discussing women older than themselves. Corresponding to findings by Shinan-Altman and Werner (2019), where middle-aged participants said that old age begins around the age of 68, the term “older people” was frequently used by our interviewees when referring to individuals in their late 60s or 70s, emphasizing the psychological distance from their own age group. In the context of this study, participants who did not feel they were aging simply did not think about sexual health issues, often saying they were “too young to have any problems” at all.
“Not feeling like aging” was often mentioned in the context of the participants’ self-perceived good health and satisfactory sex life. This aligns with research showing that sexual problems may be not necessarily more common in midlife than earlier (Fischer & Træen, 2022; Quinn-Nilas et al., 2018; Richters et al., 2022) and that physical activity and self-rated health correlate with better sexual function and fewer reported problems in midlife and beyond (Cabral et al., 2014; Lee et al., 2016; Smith et al., 2019). Declining health, together with retirement and widowhood, is a life event typically associated with the transition-to-older-age period (Jecker, 2020; Melinda et al., 2023), and chronic illness can be a particularly strong biographical disruption (Bury, 1982). In the absence of such events or disruptions, some late-midlife adults may not perceive age-related processes as affecting their sexual functioning. Others may notice some changes but successfully manage them independently, often through creative, tactful strategies. Several participants demonstrated a resourceful and supportive approach to navigating these changes—especially when the issues were transient—allowing them to maintain a subjectively satisfying sex life without seeking professional assistance.
Second, findings from this study revealed an intriguing phenomenon where many interviewees did not view themselves or their partner as having any sexual problems, while throughout the interview they mentioned experiencing lower libido, less firm erections, vaginal dryness, or decreased frequency of sex. Several explanations for this discrepancy are possible. If the changes in sexual functioning do not disrupt relationship interactions or quality of sex life, reappraisal strategies, such as viewing the changes as minor inconveniences rather than major problems, may help late-midlife individuals ensure they do not become a source of worry. If people can engage in subjectively satisfying sexual activities with some adjustments like the ones narrated by our participants (using lubricants, wider sexual repertoire of non-penetrative behaviors, new ways to maintain intimacy; Fileborn et al., 2015), they might legibly not view some changes as problematic. Additionally, the narratives on closing the sexual chapter of life suggest that when a person’s priorities and interests shift, and sexual activity becomes marginal to their overall well-being (DeLamater & Koepsel, 2015; Gore-Gorszewska & Ševčíková, 2023), symptoms, which might otherwise be seen as problematic in different life circumstances, may lose relevance and thus may not be experienced as problems at all.
The absence of distress was notable in participants who experienced sexual changes but did not consider them problematic. This observation aligns with existing research documenting that the levels of reported concerns (distress) about sexual functioning are substantially lower than the prevalence of sexual difficulties reported by women and men in midlife and beyond (Briken et al., 2020; Fischer & Træen, 2022; Graham et al., 2020; Hald et al., 2019; Richters et al., 2022). In the context of this study, the absence of distress corresponded to the participants’ belief that no SH&WB-related intervention was necessary. This perspective could be advantageous by preventing unnecessary anxiety and avoiding the pathologization or medicalization of natural, age-related sexual changes (Briken et al., 2020). Additionally, this study is unique in demonstrating that some midlife adults possess the competence and creativity to address sexual challenges independently, thereby maintaining a subjectively satisfying sex life without any need for external professional help.
Still, it may be relevant to consider that because these individuals have not yet needed to seek sexual health support, their experience in navigating such services is limited. Indeed, while many participants confidently expressed that they would intuitively recognize and address distressing problems should they occur, it is worth mentioning that a couple of interviewees dealt with communication issues that made their help-seeking less straightforward. This finding is in line with prior research documenting the presence of communication, personal, and systemic barriers in seeking professional help (Ezhova et al., 2020; Teo et al., 2022). For instance, Hinchliff et al. (2021) found that middle-aged and older adults’ pathways to getting help for existing self-reported sexual problems are often characterized by delay, and mired with stops, starts, and uncertainty, a reality echoed by some accounts in this study. This indicates that even if one plans to act when a problem becomes severe, one may be occasionally tempered by healthcare system realities. Therefore, in order to facilitate midlife adults’ navigating relevant services should more distressing sexual health issues arise in the future, it would be beneficial to ensure that accessible and supportive pathways are in place.
Third, consulting an HCP regarding sexual health concerns was, in our participants’ opinion, conditional upon facing a significant sexual problem versus experiencing manageable changes in sexual functioning. This mirrors a pattern observed in research on healthcare-seeking behavior among midlife women in other health domains, where greater severity of symptoms encouraged treatment seeking (Du et al., 2020; Waetjen et al., 2018). The current focus on time-effectiveness and efficiency in the healthcare sector often results in brief, to-the-point visits during which patients are expected to describe specific symptoms and ideally leave with a prescribed treatment or referral. It can be argued that this structure does not easily accommodate discussions on SH&WB (Hughes & Lewinson, 2015; Kingsberg et al., 2019). Future research could explore the possibility that individuals without severe or urgent symptoms (“not bad enough”) may hesitate to consult an HCP. A case could be made that concerns which are perceived as less tangible by a person may be difficult to articulate or may be seen as falling outside the HCP’s domain of interest, as signalled by some of this study participants. Overall, the perspective that only severe and specific sexual problems legitimize consultations with an HCP may discourage those who would otherwise be interested but feel less comfortable in expressing their sex-related queries under time pressure.
Finally, our findings demonstrated that participants considered psychological and emotional factors as contributing to their sexual problems, which they addressed by tackling underlying causes (e.g., stress). This suggests that late-midlife individuals acknowledge the biopsychosocial context of sexual functioning and may prefer “whole person”–centered support (Hughes & Lewinson, 2015). Consequently, they might avoid seeking sexual health advice or treatment from HCPs perceived as narrowly specialized or focused on pharmacotherapy. Thomas et al. (2017) found middle-aged women with sexual difficulties preferred non-pharmaceutical treatments and emotional outcomes over purely physiological improvements. Our findings align, indicating that some midlife women, as well as men, may seek alternatives to the “here is a prescription” approach, reflecting the rising interest in non-pharmacological interventions overall (Mestre-Bach et al., 2022). This preference may shape their expectations of consultations with HCPs who lack a holistic approach, driving midlife adults to other resources, like the Internet. Further research is needed to better understand midlife adults’ needs regarding SH&WB information and support.
Implications
As our findings suggest, some adults at late midlife do not experience SH&WB problems or believe that such concerns are only relevant for older populations. Not viewing themselves as “older” and without encountering major life transitions that prompt a reconsideration, they may not see a need to seek out or engage in sexual healthcare. While many do not require external information or support, those who might otherwise take interest could be put off from engaging with materials labelled “for older age/in later life.” Thus, such materials should be tailored and advertised specifically for (late) midlife adults. Importantly, researchers and practitioners must carefully consider their language because referring to late-midlife individuals as “older” may create resistance, reducing their engagement in discussions about sex.
Notable distress appears to be a prerequisite for seeking sex-related information or support among late-midlife individuals (Gore-Gorszewska et al., 2025). Regrettably, distress as a crucial component is not always assessed in sex research (e.g., Quinn-Nilas et al., 2018). Even the authors of the widely used Female Sexual Function Index, considered a gold standard for assessing clinical sexual dysfunction, acknowledge the absence of a distress measure in their scale as a limitation (Meston et al., 2020). Moreover, our findings support existing recommendations about how HCPs should frame their questions during consultations (Kingsberg et al., 2019; Parish et al., 2019). A generic question like “Do you have any sexual problems?” may yield a negative response from midlife patients, while tactful prompting on specific changes and, critically, on related distress (or an absence thereof) would facilitate exchange of information regarding more nuanced experiences of midlife patients.
For these late-midlife adults who are not distressed about their current sexual functioning, a proactive style adopted by HCPs may be advisable. Research indicates that patients who have been asked about sexual function are more likely to present help-seeking behavior in the future (Moreira et al., 2005). Therefore, introducing SH&WB topics during routine appointments (e.g., health checks and medication reviews), especially in the absence of immediate concerns, could serve as a preventative health strategy and facilitate open dialogue should a need arise. Offering suggestions or advice on behavioral and communication-oriented strategies for managing changes in sexual functioning would align closely with preferences clearly expressed and successfully adopted by this study’s participants. Midlife adults may appreciate signals that an HCP goes beyond pharmacotherapy toward a more holistic approach. For those who may be discouraged by past difficulties in articulating their concerns to a clinician, HCPs’ acknowledgement and support would be beneficial. Offering respectful, patient guidance to those less experienced in expressing their concerns clearly in medical terms could improve healthcare accessibility.
Conclusions
This study offers nuanced insights into how late-midlife adults experience changes in sexual functioning and when they perceive these changes as problematic enough to warrant seeking help. Individuals in this life stage might not seek SH&WB information or support because they do not identify with the concept of being older, do not view sexual changes as problems, or do not experience distress about them. This study challenges existing assumptions on inevitability of sexual dysfunctions in late midlife by showing that many individuals successfully manage the changes on their own, preventing those changes from becoming problems. By using creative and tactful partnered strategies, they maintain a subjectively satisfying sex life. Healthcare providers and researchers should acknowledge and respect this perspective, recognizing that many late-midlife adults neither require intervention nor desire the medicalization of normal sexual changes, often preferring non-pharmacological support. Still, even in the absence of urgent concerns, clinicians can proactively create space for open dialogue and lay the groundwork for supportive interactions should a need arise. Viewing midlife not as a time of decline but a preparatory phase—an opportunity to foster awareness, strengthen communication skills, and provide knowledge about available resources—can help individuals be more empowered and competent in managing potential challenges in the future. Future research should investigate how late-midlife adults decide to seek help and which sources of information and support they prefer, especially beyond traditional healthcare settings. Finally, including late-midlife adults in research on later-life sexuality necessitates careful consideration. This demographic’s life situation may be distinctly different from those in their 60s, 70s, or 80s, warranting separate age groups for analyses and conclusions. Such delineation can yield more accurate scientific data and, ultimately, better-targeted support for all age groups.
Supplemental Material
Supplemental Material - “We Are Too Young to Worry”: Late-Midlife Adults’ Voices on Sexual Changes, Distress, and Help-Seeking Behaviors
Supplemental Material for “We Are Too Young to Worry”: Late-Midlife Adults’ Voices on Sexual Changes, Distress, and Help-Seeking Behaviors by Gabriela Gore-Gorszewska, Anna Ševčíková, and Sharron Hinchliff in Qualitative Health Research
Footnotes
Acknowledgements
The authors would like to thank all individuals who agreed to participate and shared their perspective, as well as Zuzanna Sommerfeld and Paweł Jemioło for help during recruitment and data collection.
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Research Ethics Committee at the Institute of Psychology, Jagiellonian University (approval number KE/51_2022).
Consent to Participate
Written informed consent to participate and publish anonymized excerpts was obtained from all interviewees.
Author Contributions
GG-G conveyed the idea for the study, collected the data, and drafted the first version of the manuscript. All authors were involved in the process of data analysis and contributed to writing of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection and analysis was supported by the National Science Centre in Poland (grant number DEC-2021/41/N/HS6/02193), grant awarded to the first author. The study is also from the project, Research of Excellence on Digital Technologies and Wellbeing CZ.02.01.01/00/22_008/0004583 which is co-financed by the European Union.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.