
Abstract
Although grief is an unavoidable aspect of the human experience, it remains largely unspoken in the workplace, including healthcare. Physicians, in particular, minimize their grief due to professional norms and broader societal discourses, often viewing it as trivial or incomparable to the suffering they witness at work. This study examines how physicians narrate their grief to see which discourses are represented, enacted, and sometimes resisted in clinical practice. Physicians (n = 12) and residents (n = 5) from Atlantic Canada participated. Two rounds of interviews, 6 months apart, were conducted. Critical discourse analysis was utilized to make sense of the language participants use to describe their grief experiences. Two dominant discursive framings were identified: grief as an interference and grief as an invitation for meaning making. For many, navigating professional responsibilities while experiencing grief generated tensions and contradictions, evoking feelings of disequilibrium and frustration. For some, however, grief prompted deep self-reflection, leading to a shift in mindset or a realignment of values. Residents grappled most with the discursive boundaries of grief expression, unsure about when and with whom it might be acceptable. More experienced physicians articulated greater ease in discussing grief, often framing it as a source of deepened wisdom. Participants’ discursive framing of grief appeared to change alongside their maturation as physicians, suggesting that status and hierarchy influence the extent to which physicians feel empowered to engage in grief-positive discourse. Formal education and institutional support to foster “grief literate” clinical environments could play a valuable role in supporting physician well-being.
Introduction
Although grief, defined here as “the experience and natural feelings that come with loss” (Kessler, 2019, p. 13), is inherent to the human experience, it remains largely unspoken in most workplaces. Healthcare environments are no exception, especially when the person grieving is a physician. Beginning in medical school, learners are socialized into the cultural norms of the medical profession and over time begin to recognize and inhabit the language, behaviors, and commonly agreed-upon values attributed to being a “good” physician. They learn through role modelling and workplace culture which emotions are deemed appropriate to display during patient encounters (Helmich et al., 2014), when to distance themselves from situations that may hinder their efficiency or clinical decision-making (Webster et al., 2015), and how to avoid vulnerability to intrapersonal distress (Bynum et al., 2019). Once in practice, they assume responsibility for the patients within their care while at the same time having to remain sensitive to challenges in the healthcare environment that are largely beyond their control. As a result, physicians’ grief is often overlooked, reinforcing the false belief that they are impervious to it, or not permitted to grieve (Frank, 2022; Kim, 2019).
A prevalent discourse interfering with the acknowledgement of physician grief is the assumption of invincibility—the notion that physicians are superhuman and therefore must “keep on keeping on” with their clinical responsibilities, regardless of the serious harm this may have on their well-being (LaDonna et al., 2022). Another powerful discourse shaping the extent to which physicians engage with their experiences of loss is the biomedicalization of grief. A substantial body of literature both situates and critiques grief as a medical or mental disorder necessitating intervention. The language associated with this discourse serves to warn and inform about the potential physical, psychological, and organizational costs incurred if grief is perceived as too prolonged or too intense (Bento, 1994; Granek, 2015; Macdonald, 2019). Consequently, physicians often struggle to acknowledge their own grief, partly due to prevailing discourses that deny them the privilege to process and partly because what they may be grieving is not always understood or is disenfranchised in the clinical workplace (Kim, 2019; Kittleson, 2018; Lathrop, 2017). This makes it difficult for physicians to recognize that they may be grieving, let alone freely name aloud all of what they are experiencing to the outside world.
The discursive construction of grief as solely tied to death-related loss further complicates our understanding of physician grief. And yes, in many cases, the loss a physician may be mourning might be physical—for example, exposure to patient death or the loss of a family member or a cherished colleague. However, a grief response can occur in response to instances of loss unrelated to death, such as shifts in the practice of healthcare (Lathrop, 2017; McAlearney et al., 2015), and more existential losses related to aspects of an individual’s identity (Burm et al., 2025).
Current Barriers to Acknowledging Physician Grief
Given the demands of medical training and the mounting pressures healthcare systems continue to withstand, it may not be surprising that discussions of physician grief happen infrequently. While well-being interventions and organizational policies have been developed to support physicians with navigating difficult experiences such as grief (West et al., 2016, 2018), these measures are often elective, irregularly offered, and challenging to meaningfully implement in the clinical workplace. As a result, opportunities for physicians to engage in conversation about grief remain limited (Granek et al., 2017; O’Connor & Breen, 2014; Sikstrom et al., 2019). Moreover, many proposed coping strategies, while well-intended, place the responsibility on the griever to balance their work obligations amid the depths of their grief, overlooking the systemic organizational factors that discourage physicians from disclosing grief or seeking support (Funk et al., 2017; Hancock et al., 2020).
The repercussions of avoiding acknowledgement of grief in medical practice are serious. Current scholarship paints a dim picture, one that shows physicians’ overwhelming tendency to soldier on, and in so doing, compromising their psychological and physical well-being (Kim, 2019; LaDonna et al., 2022; Laor-Maayany et al., 2020) and the sustainability of the healthcare workforce, a reality that became particularly evident during the COVID-19 pandemic and continues to be a pressing issue today (Burm et al., 2025; Rabow et al., 2021; Yazden et al., 2023). Unacknowledged grief exacerbates burnout, compassion fatigue, moral distress, and reliance on maladaptive coping strategies, often leaving physicians to internalize the belief that they themselves are the root of the problem (Barnes et al., 2020; Srinivasa et al., 2019).
Grief is an inherent aspect of medical practice, yet it is often overlooked or considered inappropriate to discuss. To challenge this silence and provide a more humanizing perspective on the issue, we undertook a qualitative inquiry into the various types of losses that physicians grieve. The focus of this study was on the discursive construction of grief at the individual level to examine underlying assumptions influencing physicians’ perceived ability to acknowledge their personal or professional losses and express grief in the workplace. Our central research question was: How do physicians’ discursive constructions influence the extent to which grief can be freely experienced? By asking this question, we aimed not only to bring to light the broader discourses that may be limiting conversations about grief within the clinical workplace but also to explore opportunities to challenge and reshape them.
Methods
Critical discourse analysis (CDA) (Fairclough, 2003) was utilized to make visible the ways physicians use language to describe their grief experiences and its impact on their clinical work. Recognizing that “discourse” is understood differently, depending on theorist, philosophical stance, or academic discipline (MacLeod et al., 2024), we provide a rather uncomplicated definition to situate our understanding and rationale for using CDA. Broadly speaking, the term discourse refers to “ways of representing aspects of the world—the processes, relations and structures of the material world, the ‘mental world’ of thoughts, feelings, beliefs and so forth, and the social world” (Fairclough, 2003, p. 124). CDA, by extension, enhances this exploration by drawing on a critical theory framework to reveal how dominant discourses infiltrate physicians’ beliefs and practices, establishing an “acceptable” way to grieve—one that, over time, becomes perceived as “normal” and “the ways things should be” (Gee, 2014). Applied to medicine, this framework reveals a discursive ideal of emotional neutrality and detached concern, which previous work in medical education has shown to be reinforced through medical training (Beagan, 2000; MacLeod, 2011). If we consider these discourses in the context of physician grief, emotional investment and outward displays of emotion would be regarded as undesirable and an impediment to clinical decision-making. Through the lens of CDA, we can begin to expose the expectations and boundaries of acceptable physician grief, while creating the space to explore other discursive possibilities. This study was approved by the Institutional Review Board of Dalhousie University (REB File #: 1028381).
Data Collection
We recruited physicians (n = 17) from across Atlantic Canada via our research team’s professional networks and Dalhousie University’s Postgraduate Medical Education office during 2023–2024. We had a total of nine male-identifying and eight female-identifying physicians’ consent to participate in our study with participants representing diverse specialties including surgery, family medicine, palliative medicine, pediatrics, infectious disease, internal medicine, pathology, emergency medicine, anesthesia, urban and rural practice locations and career stages, practice locations, and career stages, ranging from residents (n = 5), mid-career physicians (n = 7), and late-career physicians (n = 4) to those recently retired (within 12 months of data collection) (n = 1). Data collection involved two rounds of semi-structured online interviews with each participant, conducted 6 months apart. Unfortunately, one participant from our dataset did not complete a second interview due to scheduling constraints. Team members TB and VL were responsible for obtaining verbal consent from participants at the start of each interview. The first round of interviews focused on the discursive construction of grief in physicians’ personal and professional lives. The second-round interviews involved revisiting key discursive constructions identified during initial data collection. Participants were invited to weigh in on what was shared and if so inclined, to contribute additional insights into the social and cultural aspects of discursive practice surrounding physician grief. This meant asking pointed questions that arose for us after the first round of interviews (e.g., when is it okay to share grief and with whom?) so that they could help us better understand why physicians construe grief in specific ways. Follow-up interviews served dual purposes: first, as a strategy to enhance the quality and credibility of our analysis (Patton, 1999), enabling participants to engage in the co-interpretation of the data, and second, as an avenue for gaining insider understanding into the discursive practices that shape how grief is perceived, discussed, and managed. Across both interviews, participants were encouraged to share their diverse experiences of loss, including experiences with personal bereavement, exposure to death in the clinical setting, and non-death-related losses. Our decision to focus on a range of losses aligned with the broader aim of this study: to deepen readers’ understanding of the diverse spectrum of losses that physicians carry with them into the clinical workplace each day. This choice was also shaped by the timing of our study. Having begun interviews not long after the height of the COVID-19 pandemic, an event that starkly illuminated the many forms of loss experienced across the healthcare system, we felt a responsibility to honor and hold space for all the experiences participants chose to share with us, regardless of where they might fall on the spectrum. We approached this inquiry with the view that loss, in any form, is significant. All interviews were approximately 60 minutes in duration and were conducted over Microsoft Teams to accommodate physicians’ schedules. All interviews were audio recorded with participants’ consent and transcribed verbatim by a professional transcriptionist to ensure accuracy.
Data Analysis
Throughout our analysis, we remained sensitive to the productiveness of discourses (Carabine, 2001), meaning that we sought to understand how the clinical environment reinforces certain discursive ideals of grief. We also placed special attention to “counter-discourses, noting that individuals are not passive recipients of discourse” (MacLeod, 2011, p. 378). To do this, we had to give serious consideration to how ideas about medical professionalism, the healthcare system, and psychological safety may be giving meaning and force to how physicians narrate their experiences with grief. We were equally interested in identifying moments of resistance, where participants questioned or outwardly rejected specific perspectives and normative ways of speaking about grief. We remained attuned to how these discursive constructions influenced physicians’ expressions of grief at work, while staying open to potential shifts in discourse especially since the COVID-19 pandemic. We utilized Carabine’s (2001) 11-step process to discourse analysis as our guiding framework. The process began with members of the research team (SB, TB, and VL) each choosing a few transcripts to review. During this initial phase, our focus was on familiarizing ourselves with the data and the various discursive strategies participants employed as they narrated their experiences with grief. At this stage, we made notes on participants’ language choices (e.g., the use of specific metaphors or euphemisms), the stories they chose to share, and participants’ tone or demeanor while narrating these stories (e.g., whether they spoke adamantly or cautiously about grief). We also attended to absences and silences in the data, instances where anticipated topics were noticeably under-discussed as well as intertextual references (e.g., mentions of policies, publications, or codes of conduct). Concurrently, we remained sensitive to the institutional contexts and participants’ self-reported identities (e.g., gender, race, career stage, and clinical specialty) considering how these elements influenced the ways in which different discourses produced particular “truths” about what it means to be a “good” physician. Following our individual reviews, we convened to discuss our interpretations and together began organizing our initial observations into preliminary thematic clusters, such as grief as a teachable moment or grief as an equalizer between physicians and patients. From there, we developed a codebook comprising a set of codes and their corresponding definitions, which we used to help us categorize the data during subsequent stages of analysis. Data were coded in ATLAS.ti by TB. Since our analysis followed an iterative process, our codebook evolved as our analysis progressed. Additionally, we revisited relevant academic literature to compare participants’ discursive strategies with how the subject of grief is currently represented in scholarship. SB, TB, and VL met on a regular basis throughout the analysis stage to ensure consistency in coding and to review any new themes that were identified within the dataset.
The larger research team (AD, LH, SM, and AM) were invited to review transcripts throughout the analytical process and to share and reflect on their individual impressions of the data based on their positionality within the clinical and educational spaces they routinely inhabit. Our team includes members from various professional and academic backgrounds, unified by a shared commitment to creating grief-positive spaces in medical education and clinical practice. SB and AM are PhD researchers who bring a critical social science perspective to issues in medical education. AD, LH, and SM are physicians who hold or previously held leadership roles at Dalhousie University. VL is a doctoral student, and TB is a trained research associate with expertise in health informatics.
Results
Examples of Loss in Physicians’ Lives
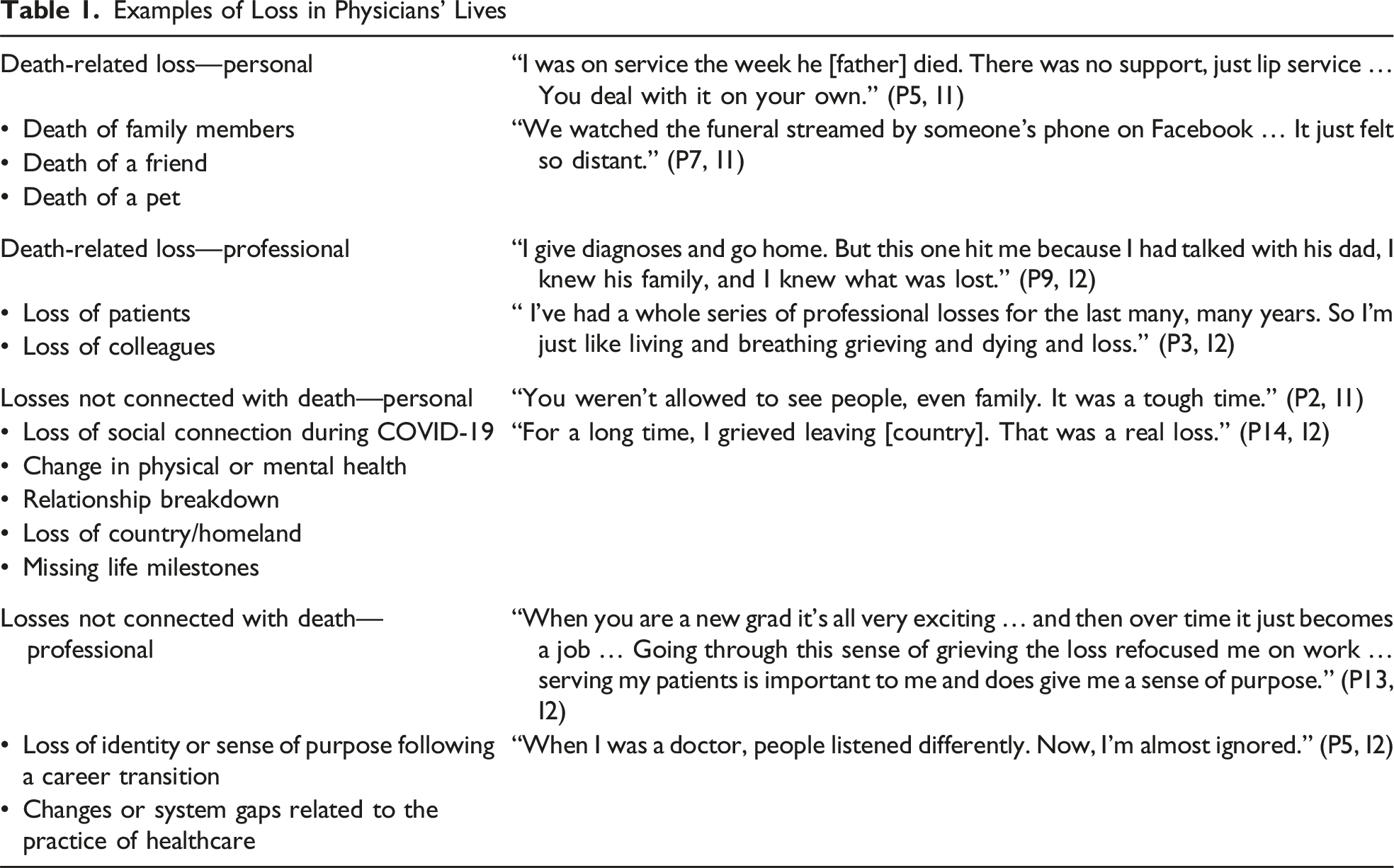
Many spoke about their grief in somewhat elusive terms, characterizing it as an experience that never truly ends but rather “eases, waxing and waning” (P5, I1). One participant described a physician’s grief much like the continuous swinging of a pendulum: “You want to be empathetic enough, and you want to feel enough, but you don’t want to feel so much that you basically get destroyed by it” (P13, I2). This language choice showcases the inner tug of war that physicians must navigate in the context of their daily work—searching for balance between reacting compassionately to their own losses or those they observe others endure, and the need to contain their grief in order to respond to the needs of the moment. Perhaps to no surprise then, the topic of grief was broached with carefulness by participants. We observed them toiling over whether grieving was, and should be, permissible at work or whether it was easier and safer to keep it tightly contained. What stood out to us was participants’ positioning of grief in dualistic terms, with the most pervasive discursive framing being grief as an interference. Depending on the circumstances, grief generated tensions and contradictions, evoking feelings of disequilibrium and frustration. For a few participants, however, their grief experiences prompted deep self-reflection and a reawakening of sorts. In such cases, participants recognized the harm that stigmatizing and pathologizing grief can have on physician well-being, leading them to undergo a mindset shift or a realignment of values when it came to grief in general and physician grief more specifically. We labelled this discursive framing grief as an invitation for meaning making. We explore these two discourses in more depth in the sections that follow.
Grief as an Interference
Participants often described their experiences with grief as an inconvenience, hindering their ability to fully concentrate on their clinical work. Understandably then, participants were driven to interrupt their grieving process, regardless of the potential effects on their well-being. Participants across clinical practice fields found that their work demands made it near impossible to carve out space to fully experience grief, and thus the only viable option they felt they had was to set it aside. As one critical care physician reflected: “You want more humanity and more warmth [in healthcare], but then you have 15 patients to see and three consults, and one person might need to get intubated … it all gets pushed” (P17, I1). Here, we recognize the physician’s desire to uphold a professional identity rooted in discourses of care. They use words like “humanity” and “warmth,” evoking a vision of healthcare many of us hope for: a system where expressions of grief are acknowledged and supported. Yet, this ideal is swiftly replaced by the harsh realities of clinical practice and discourses of efficiency, where grief is deemed not as a necessary part of professional life but as a luxury that time and workload do not afford.
Others attributed their tendency to suppress grief to the belief that displays of strong emotionality are unprofessional and violate accepted norms: “Our strength is seen in how well you suppress your emotions and how objective you can be” (P10, I2). Some participants reasoned that grief needs to be “handled appropriately” (P9, I2) so as not to compromise the deeply entrenched discourse of the good doctor—one who is expected to consistently and capably uphold their duty of care.
Participants repeatedly referred to a discursive ideal dictating how physicians “should” handle grief. Statements akin to “buck up and carry on” (P7, I1) were commonly shared, reinforcing that outward expressions of grief were often disregarded or socially unsanctioned in the clinical setting. This was particularly the case in relation to grieving death-related losses experienced while at work. Many participants, driven by concerns of appearing weak, mentally unwell, or facing “medical legal repercussions” (P1, I2), were admonished to keep a “stiff upper lip” (P14, I1). As one physician noted, medicine fosters a culture where “you need to be strong … it’s hard to show weakness around other people because of fear of judgement” (P16, I1).
The overwhelming stigma surrounding the expression of grief, combined with its perceived disruptive nature, placed a heavy burden on participants, leaving them to err on the side of invulnerability. Open conversations about grief were reported to be rare. As one surgeon noted, “not a lot of people talk about [grief] … at work, we’re a little bit superficial” (P1, I1). Residents especially grappled with the discursive boundaries of grief expression, unsure of when it was appropriate to do so or with whom. This reluctance was particularly resonant among the female-identifying residents we interviewed and often stemmed from gendered expectations that continue to shape medical culture. As one resident shared, When I step into work … I have to come across a strong like alpha … it makes me feel vulnerable when I show emotions at work. I kind of feel like I will be attacked … or that people would think that I’m like inadequate or incompetent. (P15, I1)
Another resident echoed this sentiment, expressing concern that “if [they] cried or expressed grief … [they would be] seen as less serious, or less of a real doctor” (P4, I2). In both accounts, the language conveys a presumption that female-identifying physicians operate from an emotional place versus one of reason, where any visible expression of feeling is viewed as unprofessional or destabilizing. As a result, they are not only expected to conform to the emotional norms of the clinical environment but also to overcompensate by constantly signalling their competence and emotional control.
Participants across all career stages and specialties frequently engaged in or observed others perpetuating discursive practices discouraging the expression of grief in the clinical setting. These messages often resulted in emotional turmoil, with participants’ grief remaining largely unexpressed and therefore unacknowledged.
Grief as an Invitation for Meaning Making
We identified a second discursive construct, which we refer to here as grief as an invitation for meaning making. This discursive framing resisted the biomedicalization of grief and was oriented toward a more humanist representation of a physician, one that revealed the value that lies not only in showing emotional vulnerability in clinical practice but also how the experience of grief can quickly put things into perspective. This shift—from merely acknowledging their grief to embodying it—not only seemed to help participants grow into more compassionate physicians but lead them to find greater fulfillment in their work. This is not to suggest that participants found their grief experiences any easier to navigate. However, their attempts to reorient their experiences of grief from a problem to fix to one met with empathy and validation appeared to deepen the quality of their connections with colleagues and patients and the world around them. This was the case for one junior resident, who recalled a particularly difficult case while working in the neonatal intensive care unit that resulted in the deaths of both the mother and the infant. Struggling to cope with the emotional impact of the case, they found themselves unexpectedly breaking down weeks later in the resident lounge. The resident shared how this moment of emotional outpour, while initially leaving them self-conscious, sparked a productive conversation that had residents across different levels of training recalling similar experiences and relaying words of comfort. The participant commented that they left the interaction feeling “really supported and like [they weren’t] alone in having these tough experiences so early on in residency” (P4, I1).
We noticed that physicians further along in their careers articulated greater ease in discussing grief, often framing it as a source of deepened wisdom. This process, they noted, often required a conscious effort to let go of the discursive ideal that “being emotionally present is equal to breaking down” (P10, I2). Through this journey, they gained new perspectives, including a greater understanding of themselves. Some of the physicians with whom we spoke to had confronted a great deal of loss, be it in their personal or professional lives, which they attributed to making them “more aware of the foibles of the medical profession” and “a sense of the other side of the equation—what it [is] like to be a patient and a family member, and the importance of openness and transparency” (P5, I1). Another physician described their experience with grief as “post-traumatic growth” and how they now “have a much more empathetic approach to people that experience trauma, having firsthand experience of how much it can derail your life” (P8, I2). This reframing of grief as an invitation for ongoing meaning making, both individually and in relation to others, was recurrently discussed. As one physician remarked, Is it unprofessional to shed a tear when you see grieving family members having their last moments with [their loved one] … I don’t think so. I think it shows that you’re human. We are human. We’re not machines. And you can acknowledge that and say that, you know, I’m touched by what’s happening here, and I’ve suffered similar losses, and I know it’s difficult … I don’t think it [has] made me less professional … I feel it maintains my humanity. (P11, I2)
In these examples, participants introduce an alternative discourse that pushes back against the dominant discourses of competence and infallibility that prevail in medicine. They highlight how, in certain circumstances, grief enlightens physicians about “the humanistic aspect of what they do” (P2, I1). Through this discursive framing, physicians are more than their professional role; they too are entitled to grieve, be it as patients or loved ones or simply because they are embedded in professional contexts where death, dying, and loss occur. While not always easy, physicians resisted the notion that grief gives way to weakness. Instead, they recognized its value and, in the process, came to realize that grief need not be vilified but can serve as a powerful teacher.
Discussion
Participating in our study offered physicians the opportunity to reflect on their experiences of grief and critically examine how the professional culture of medicine supports, or, in some circumstances, fails to support, grieving physicians. Discourses of competence and uniformity, coupled with the expectation to prioritize patient care above all else, often compelled physicians to conceal their grief, a finding supported by previous literature around professional identity formation (Frost & Regehr, 2013; MacLeod, 2011; Sawatsky et al., 2023). Our findings also revealed that physicians’ inability to grieve was largely influenced by systemic pressures rather than clinical specialty. In the face of staff shortages and budget constraints, there was simply no time to grieve. The busyness and inefficiencies of the current healthcare climate left many feeling that embracing self-sacrifice was the only viable choice. For some, this was a conscious decision—they willingly set their grief aside for their patients, perpetuating the enduring ideal of the virtuous physician as one who prioritizes duty over their humanity. However, an increasing number of physicians acknowledged that working in a broken system—let alone grieving within it—was growing tiresome and escalating into a serious occupational risk.
Still being trainees, residents often felt the most pressure to appear unbreakable and therefore were less inclined to lean into their grief. For many, their professional environments offered few outlets to have their grief acknowledged by others, fearing that any display of vulnerability would be perceived as professional weakness—or worse, a lack of competence: an enduring dilemma among medical learners that has been previously reported (Bynum et al., 2019; Nichol et al., 2024). Interestingly, we found that participants’ discursive framings of grief appeared to change alongside their maturation as physicians, suggesting that status and hierarchy influence the extent to which physicians are able to question and even resist dominant discourses of neutrality. Yet, years of experience did not always serve as an impenetrable shield; even seasoned physicians admitted to struggling with the notion that they deserved time and space to grieve. However, when participants took the proverbial leap and gave themselves permission to grieve, this bold step proved rewarding, even liberating for some. Participants reported a greater sense of emotional well-being, maintained patient-centered care, and developed deeper, more meaningful connections with their colleagues, and perhaps even with their chosen vocation.
Admitting to being in the throes of grief—whether to colleagues, mentors, or even oneself—requires tremendous courage, and we are not naïve to the fact that striking a balance between personal disclosure and professional responsibility can be a delicate dance (LaDonna et al., 2022; Parsons Leigh et al., 2021; West et al., 2018). We also recognize that engaging in discourses related to grief expression varies significantly depending on the person, the loss being grieved, and the unique dynamics one is working within (Breen et al., 2022; Harris, 2019). More so, as our data reveal, there exists a discourse of fear that acknowledging grief aloud may not be met with compassion and support. However, the prevalence of professional burnout, compassion fatigue, and moral distress in the medical community is a powerful indicator that the “tough it out” mentality is increasingly unsustainable (Khan et al., 2023; West et al., 2018). It is imperative that we openly interrogate discursive practices that construct grief as something to be suppressed or “gotten over” and consider other discursive possibilities. An opportunity exists to leverage the inevitable experience of grief, not as something to be endured in isolation but as an experience from which physicians can learn, deepen their understanding, and strengthen the support they offer to others and the support they may one day need themselves.
Rethinking Physician Grief: Opportunities and Next Steps
How, then, can we better support physicians navigating grief and loss? A starting point lies in education and stronger institutional support aimed at creating “grief literate” work environments (Breen et al., 2022). Macdonald (2024) writes that “grief literacy starts with the premise that grief is a typical, expected experience” (p. 367) and, as such, should not go unobserved or be stigmatized in the communities where we live and work. In a grief literate workplace, both new and experienced physicians, regardless of specialty, would have access to, and be encouraged to engage in, grief training opportunities. These opportunities would help physicians navigate encounters with death and bereavement in everyday clinical practice while also helping them process personal losses that inevitably influence how they show up professionally. By extension, we advocate for grief training to adopt a broader scope—one that explores the wide range of non-death losses physicians experience, as well as the role each of us play in shaping everyday discourse around grief.
While education is undoubtedly at the heart of building a grief literate milieu, there are more immediate steps that can been taken in the short term. What this will look like will depend on the clinical context, but ultimately, it comes down to holding space for the griever “without judgement, platitudes or an agenda” (Cacciatore et al., 2021, p. 9). We urge readers to be both creative and flexible in their approaches to making space for physician grief. This may take the form of specific emotion-focused debriefs or mourning rituals, seeking community and connection with like others, improving both the accessibility and inclusivity of employee assistance programs, and advocating for community-driven activities designed to help physicians recognize, understand, and process their grief. These types of initiatives have been shown to provide tremendous value in the clinical workplace and, over time, can help challenge stubborn discourses that continue to influence the medical profession (Yazdan et al., 2023). Even a subtle acknowledgement of grief—through comforting words, a moment of silence, or non-verbal gestures like offering a hug or holding a hand—is a means to resist the denial of grief (MacDonald, 2020) and can hold profound meaning, particularly for physicians in training who often look to their preceptors for guidance on navigating emotionally charged experiences (Bombeke et al., 2010; Helmich et al., 2012). Though they may seem insignificant, these small acts of compassion can serve as powerful reminders to the grieving individual that they are not alone in their experience.
Let us be clear that by advocating for physicians to have the space and psychological safety to discuss and share their grief, we are not suggesting that maintaining emotional detachment in certain circumstances is not a useful—or at times, necessary—self-protection mechanism. Nor are we advising readers to disregard concerns about a person’s fitness to continue with, or return to, work after an experience of loss. Rather, we seek to emphasize the importance of ensuring that physicians do not navigate these uncharted waters in isolation or face stigma for expressing grief when appropriate to the circumstances. Navigating loss, regardless of type, or whether unforeseen or expected, is devastating enough for a person to work through without needing to agonize about how their workplace will respond. It is essential that workplaces and education programs take due diligence to safeguard the health and safety of grieving individuals, their colleagues, and ultimately patients.
Study Limitations
Grief can be a challenging topic for many to discuss. We recognize that physicians who were unable to participate in our study—whether because of time constraints or emotional capacity—may be underrepresented in our dataset. The physicians in our study who chose to participate likely did so because they had reached a stage in their grieving where they felt comfortable speaking about their experiences. Some may have even found the process cathartic, appreciating the opportunity to have their grief—regardless of its source—acknowledged and validated. However, we recognize that our participants’ perspectives do not represent all physicians, let alone the experiences of other health professionals. Future research that considers issues of intersectionality in the study of grief may facilitate a more nuanced understanding of how physicians’ experience or speak about grief.
Conclusions
Our study reveals that physicians experience grief as a dynamic, shifting phenomenon—at times seen as a professional liability and at other times a source of strength or an opportunity to seek moments of emotional authenticity. Yet, despite physicians’ acknowledgement that grief can take many forms and that no one should have to navigate it alone, challenging deeply ingrained cultural norms remains a daunting task for many physicians, particularly those earlier in their career, reinforcing a discourse of fear that grief needs to be swiftly and discreetly resolved. Consequently, many physicians in our study quite willingly set their grief aside for their patients, aware of the detrimental impacts on their well-being but viewing such self-sacrifice as part of their commitment to medicine.
Given the demands of the clinical environment, it is understandable why discussions of grief are often avoided. However, evading grief may pose an occupational hazard. Our findings suggest that recognizing and addressing grief, rather than pathologizing and avoiding it, is crucial for physicians at all stages in their career. Formal education and institutional support to foster “grief literate” workplaces could play a valuable role in supporting physician well-being.
Footnotes
Acknowledgments
The authors wish to thank the study participants for generously sharing their experiences of grief, allowing us to deepen our understanding of its impact within the medical profession.
Ethical Considerations
Our study received approval from the Institutional Review Board of Nova Scotia Health (REB File #: 1028381).
Consent to Participate
All participants provided verbal informed consent prior to their involvement in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided through the Nova Scotia Health Research Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.