
Abstract
Although female genital cutting, circumcision, or mutilation (FGC/M) can substantially affect survivors’ sexual health, there is limited research on the strategies they use to promote their sexual health. Using intersectionality, this interpretive description study aimed to explore and describe the perspectives and experiences of FGC/M survivors in Canada regarding their sexuality and their sexual health to identify self-driven sexual health promotion strategies. Based on semi-structured interviews with 27 women who underwent FGC/M and were currently living in Canada, we inductively identified three themes: (a) Challenging norms and striving for sexual liberation by educating oneself; (b) Cultivating sexual agency through resilience; and (c) Building a community of care to support sexual empowerment. This study offers guidance to both FGC/M survivors and their healthcare providers on potential sexual health promotion strategies based on education, action, and support. It is a first step toward understanding the sexual health of FGC/M survivors from a global and holistic perspective, moving beyond a narrow focus on anatomical and physiological functioning.
Keywords
Introduction
Background
The World Health Organization (WHO) defines female genital mutilation (FGM), sometimes also referred to as female genital cutting (FGC; Perron et al., 2020), as “all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons” (2025). Female genital cutting, circumcision, or mutilation (FGC/M) 1 is categorized into four types: type I (partial or total removal of the clitoral glans and/or clitoral hood), type II (partial or total removal of the clitoral glans and the labia minora, which may involve labia majora removal), type III/infibulation (creating a covering seal by repositioning and stitching the labia minora or majora to narrow the vaginal opening, which may also include the removal of the clitoral hood or glans), and type IV (other harmful procedures like pricking or scraping; WHO, 2025). FGC/M is practiced for various psychosexual (e.g., control of female sexuality), sociocultural (e.g., rite of passage into womanhood), hygiene, aesthetic, or religious reasons, although no religious texts endorse the practice (Momoh, 2017; UNFPA, 2025; WHO, 2025). Grounded in gender inequality and recognized as a form of gender-based violence, FGC/M constitutes a violation of sexual and reproductive health and rights (UN, n.d.; UN Women, 2017) and, more broadly, infringes upon fundamental human rights—including the rights to life, health, security, and physical integrity (WHO, 2025). Globally, over 230 million girls and women currently live with the consequences of FGC/M (WHO, 2025).
The health consequences of FGC/M are profound and multifaceted, impacting survivors’ physical, psychological, and sexual health. Physical consequences can include pain, hemorrhage, fever, infections, urinary problems, shock, and death in the short term and genito-urinary problems (e.g., urinary tract infections and vaginal infections), gynecological problems (e.g., painful menstruation), and obstetrical problems (e.g., prolonged labor, and higher risks of tears and lacerations) in the long term (Berg et al., 2014; Kimani et al., 2016; Klein et al., 2018; WHO, 2025). Studies examining the psychological consequences of FGC/M have documented a high prevalence of affective disorders (e.g., anxiety, somatization, and phobia), post-traumatic stress disorder (Mulongo et al., 2014; O’Neill & Pallitto, 2021; Reman et al., 2023; Sarayloo et al., 2019), neurosis, and psychosis (Klein et al., 2018) among survivors. Those physical and psychological impacts have repercussions on the sexual health of survivors, with studies reporting altered sexual function, dyspareunia, and decreased sexual desire and satisfaction among survivors (Berg & Denison, 2012; Berg et al., 2010, 2014; Kimani et al., 2016; Nzinga et al., 2021; O’Neill & Pallitto, 2021; Pérez-López et al., 2020; WHO, 2025).
Despite these well-documented consequences, critical gaps persist in the literature on FGC/M survivors’ sexual health. A systematic review of FGC/M-related published scientific literature revealed that only 3.5% of articles addressed the sexual and marital consequences of FGC/M (Mpinga et al., 2016). Much of this research adopts a narrow biomedical lens prioritizing physiological aspects of sexuality (Palm et al., 2019) while neglecting other important dimensions, such as body image and relationships (Abdulcadir et al., 2015). This focus is evident, as 64.1% of the articles related to FGC/M were published in biomedical journals (Mpinga et al., 2016). Furthermore, the majority of research on FGC/M survivors’ sexual health has been quantitative, concentrating on sexual function, genitality, and physiological processes, while often neglecting the perspectives of women, including those residing in Western countries (Pastor Bravo et al., 2018). Additionally, a bibliometric analysis of FGC/M literature found that the most-cited articles were those that emphasized the negative physical and psychosexual impacts of FGC/M (Sweileh, 2016), illustrating how the existing literature predominantly centered on harm and trauma rather than survivorship and agency.
While valuable and informative, the existing quantitative and biomedical literature on FGC/M survivors’ sexual health significantly lacks the inclusion of survivors’ voices, perspectives, emotions, and personal definitions of sexual health. This oversight is particularly significant given the deeply personal and subjective nature of sexual health (Čierna & Bianchi, 2024). Indeed, sexual health is a complex, multidimensional construct shaped by sociocultural, psychological, and relational factors; thus, purely biomedical approaches are insufficient to fully capture its multifaceted nature (Condran, 2014; MSSS, 2024). The limitation of such approaches becomes particularly evident when considering FGC/M survivors living in Western countries such as Canada. These individuals must not only contend with the stigma surrounding FGC/M (Jacobson et al., 2022; Johnsdotter, 2018; Johnson-Agbakwu & Warren, 2017) but also navigate a landscape where tailored resources and support are scarce or entirely absent (End FGM European Network, n.d.; Koukoui, 2017; Perron et al., 2020). In this context, qualitative inquiry emerges as a crucial approach for exploring the sexual health of FGC/M survivors. It allows for an in-depth examination between sexual trauma, healing, and resilience, while accounting for sociocultural and structural influences. Qualitative data are also essential for developing a deeper understanding of FGC/M survivors’ experiences of sexual health, ensuring that current and future sexual healthcare, services, and resources are adapted to align with survivors’ potential needs and actual priorities.
Purpose of This Study
The goal of this study is to describe the perspectives and experiences of FGC/M survivors living in Canada regarding their sexuality by addressing the research question: What strategies do FGC/M survivors implement to overcome potential impacts that FGC/M poses to their sexual health and well-being? We aimed to emphasize a survivor-driven and resilience-based approach, shifting from the deficit-focused narratives often presented when addressing the sexual health of FGC/M survivors. By focusing on the strategies survivors employ to navigate and overcome the challenges to their sexual health, we sought to uncover insights that go beyond biomedical or victim-centered perspectives, addressing both individual and structural factors through an intersectional lens.
Methodology
Research Design and Theoretical Grounding
This study is grounded in intersectionality. Developed by Black feminists to highlight gaps in social policies disadvantaging individuals with intersecting marginalized identities (Cho et al., 2013; Cole & Duncan, 2023) and first coined by scholar and civil rights advocate Crenshaw (1989), intersectionality provides a multidimensional lens to examine how individuals, and their experiences of oppression and resilience, are shaped by the interactions of various social locations (e.g., race, gender, socioeconomic status, and migration status) within broader systems of power (e.g., racism, sexism, classism, and xenophobia; Bowleg, 2012; Hankivsky, 2014). Applying this framework to FGC/M survivors’ sexual health allows for a nuanced and comprehensive understanding of both oppression and resistance mechanisms, considering both structural barriers and individual sexual agency, and advancing knowledge that can promote care, services, and resources that are responsive to survivors’ lived experiences.
We applied intersectionality through an interpretive description study design as delineated by Thorne and colleagues (Thorne et al., 1997, 2004). Interpretive description acknowledges the contextual and constructed nature of human experiences (Thorne et al., 1997) and seeks to identify patterns within subjective perceptions to generate a conceptual description of the study topic (Thorne et al., 2004). It also acknowledges individual variations to inform clinical understanding, reasoning, or practices (Thorne et al., 2004). By emphasizing the application of research to real-world contexts, interpretive description aligns with intersectionality’s commitment to social justice, ensuring that care practices are responsive to the diverse and intersecting needs of marginalized populations. As FGC/M survivors’ sexual health experiences might be shaped by various intersecting social, cultural, and structural factors, interpretive description enables a profound understanding of how these dynamics influence their health promotion efforts and the variations among them. This approach also supports the development of actionable recommendations directly aligned with survivors’ lived experiences and tailored to their realities.
In this study, interpretive description was used to guide the creation of a practice-relevant interpretive account of the sexual health promotion strategies of FGC/M survivors, and intersectionality was mobilized to contextualize those strategies within a broader perspective.
Recruitment and Participants
Recruitment was conducted from January 2021 to November 2024, utilizing a combination of targeted emails and poster distributions to healthcare providers, clinics, community organizations, colleges, universities, community centers, and laundromats. Social media and snowball sampling were also integral to the recruitment strategy. Participants were eligible if they had undergone FGC/M, self-identified as women, were 18 years or older, lived in Canada, and could communicate in English or in French. We recruited a total of 27 participants. Recruitment concluded when the research team reached a consensus that conceptual saturation had been reached—that is, subsequent interviews were no longer generating novel insights but instead reiterated patterns identified in earlier interviews. Saturation was assessed through ongoing reflective engagement with the data, involving iterative comparison between new materials and developing ideas.
Sociodemographic Information
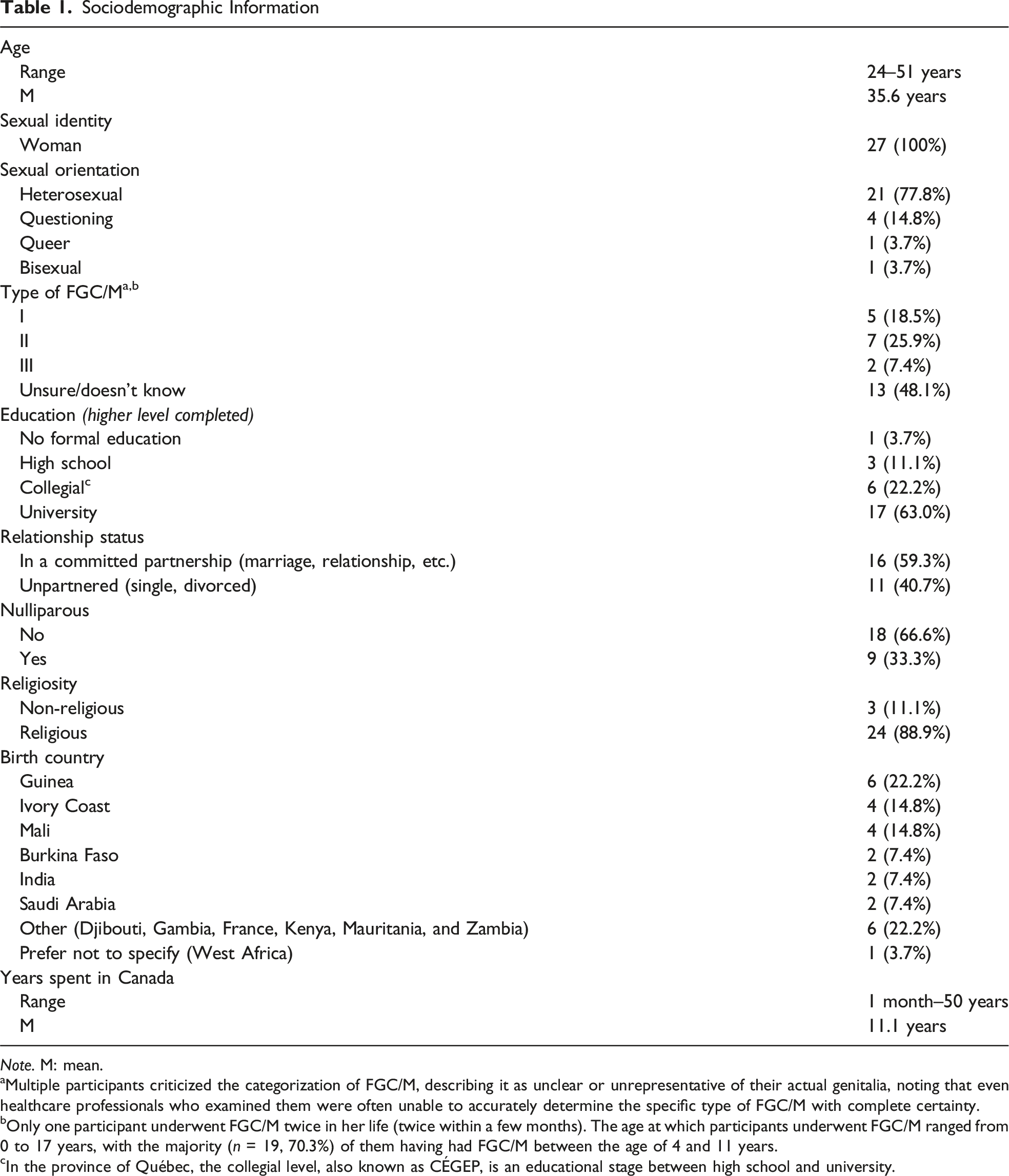
Note. M: mean.
aMultiple participants criticized the categorization of FGC/M, describing it as unclear or unrepresentative of their actual genitalia, noting that even healthcare professionals who examined them were often unable to accurately determine the specific type of FGC/M with complete certainty.
bOnly one participant underwent FGC/M twice in her life (twice within a few months). The age at which participants underwent FGC/M ranged from 0 to 17 years, with the majority (n = 19, 70.3%) of them having had FGC/M between the age of 4 and 11 years.
cIn the province of Québec, the collegial level, also known as CÉGEP, is an educational stage between high school and university.
Data Collection
An information form outlining the aim of the study, potential risks, benefits, and participants’ rights was sent out via email to women interested in participating in the study. Interested and eligible women were then invited to do an individual semi-structured interview on Zoom or over the phone. At the beginning of the interview, participants provided verbal consent and completed a short sociodemographic questionnaire. Participants were also given the opportunity to identify any topics they wanted to avoid. All interviews were conducted by the first author, and a semi-structured interview guide was used with open-ended questions about participants’ sexual identity, first sexual experiences, sexual education, past and current romantic and sexual relationships, sexual health, and access to sexual healthcare and resources. Interviews lasted between 47 and 106 minutes. Following the interviews, participants were provided with a list of resources and received a compensation of 45CA$. All interviews were audio-recorded, transcribed verbatim, and anonymized.
Analysis
Overview of the Reflexive Thematic Analysis Process
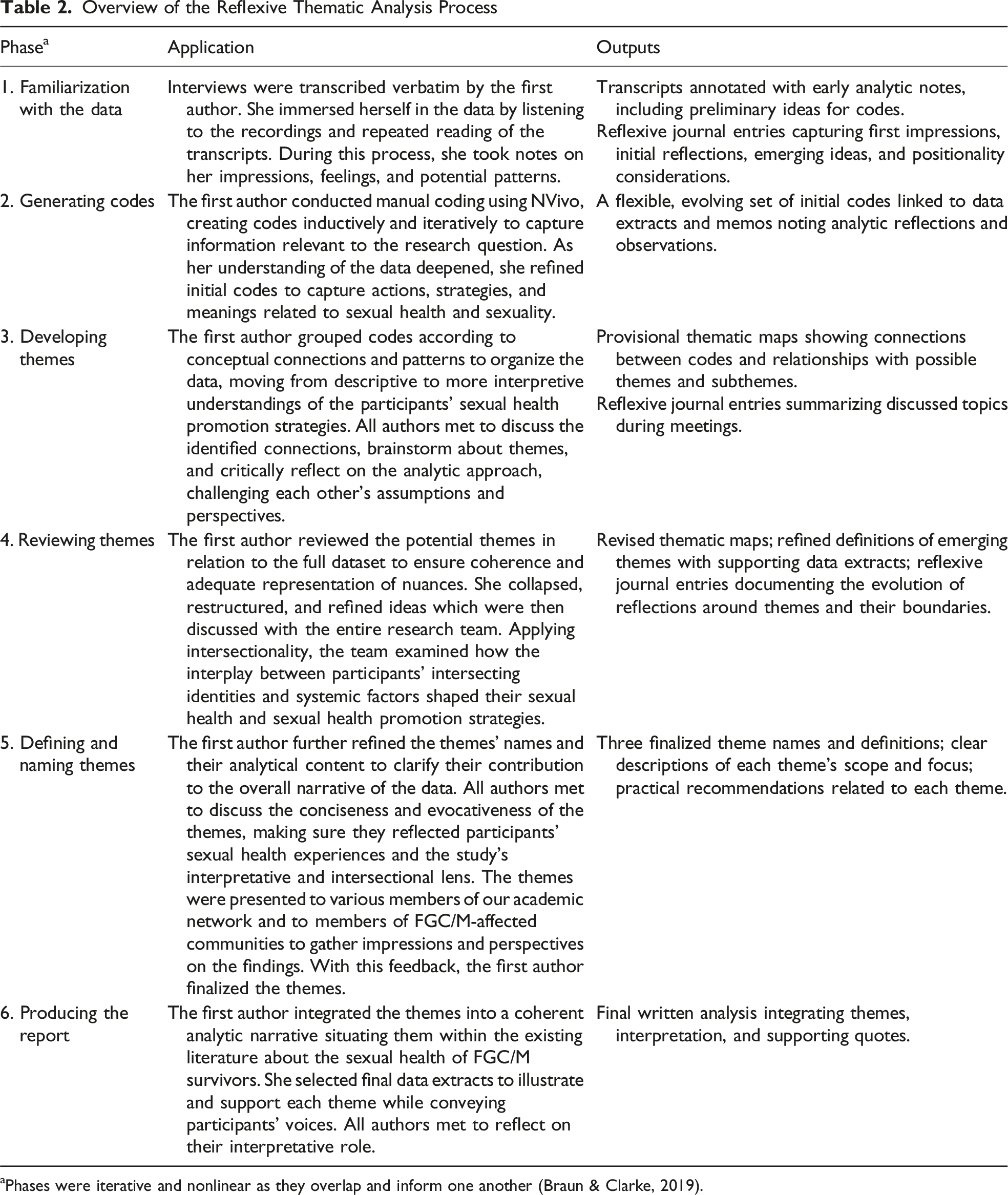
aPhases were iterative and nonlinear as they overlap and inform one another (Braun & Clarke, 2019).
Positionality Statement and Reflexivity Process
We acknowledge how our ever-evolving positionalities shape our engagement with this work. The first author—responsible for conceptualization, data collection, and analysis—is a committed feminist, community activist for sexual health and rights, and advocate for a sex-positive perspective. This illuminates why we emphasized a survivor-driven and a resilience-based approach in this research to shift from the deficit-focused narratives often put forward when addressing FGC/M survivors’ sexual health. While certain experiences and perspectives shared by participants resonated with our own, we remain outsiders—specifically, as white, non-migrant researchers who have not undergone FGC/M—and we acknowledge that we can never fully understand their unique realities. What we offer here is our perspective and insight on their lived experiences, presented as faithfully as possible. We also recognize our privileged social position and the potential impact this has on the research process such as biases, power dynamics, or cultural misinterpretations. Although this relational distance may have constrained our experiential insight into the cultural, bodily, and emotional meanings participants attached to FGC/M and sexuality, several participants noted that our outsider status made them feel more comfortable sharing taboo and non-normative sexual experiences without fear of judgment.
To acknowledge and address how our positionality influenced the research process and to help mitigate the impact of our outsider status, we employed several strategies to support an ongoing reflexive practice. The first author kept both written and audio reflexive journals to document her experiences, reactions, emotions, and perspectives throughout the research process, from study design to the writing of this article. Given the profound impact of participants’ narratives on EG, not only as a researcher but also as a woman, the audio journal proved especially valuable for capturing reflections and emotions that arose outside the workplace and in EG’s personal life. Authors also held bi-monthly peer debriefing meetings throughout the research process to critically reflect on emerging findings and challenge each other’s perspectives, interpretations, and assumptions. Additionally, although we did not conduct formal member checking, we engaged in the practice of member reflections (Braun & Clarke, 2024). EG prioritized discussions about the research process, reflexive practices, positionality, and preliminary findings, with members of communities affected by FGC/M (e.g., during commemorative and reflection days, and community events and workshops), researchers working on FGC/M or with related populations or topics (e.g., gender-based or sexual violence, during scientific conferences and meetings), and healthcare professionals working with FGC/M survivors (e.g., medical professionals and psychosocial workers, during workplace presentations or training sessions) to integrate their reflections and ensure resonance with lived experiences.
Ethical Considerations
This study was approved by the ethics review boards of three institutions: Université de Montréal (CERSES-21-002-D, #2020-1032), Centre Hospitalier Universitaire Sainte-Justine (#2022-3896), and Centre intégré universitaire de santé et de services sociaux du Centre-Ouest-de-l’Île-de-Montréal (#MEO-21-2022-3260; MP-21-2022-3896). As outsiders, we were deeply aware of the danger of not including survivors in the research process and of the risk that our work could inadvertently contribute to their marginalization. Although survivors were not formally involved in the study design, the research was ethically informed by prior consultations with community workers, healthcare professionals, and researchers with expertise on the topic. These consultations helped identify priorities relevant to survivors and those who support them, ensuring that the research focus remained respectful, ethically grounded, and responsive to community concerns.
Findings
Participants described three key strategies to overcome the impacts of FGC/M on their sexual health and well-being: (a) Challenging norms and striving for sexual liberation by educating oneself, (b) Cultivating sexual agency through resilience, and (c) Building a community of care to support sexual empowerment. These themes showcase the participants’ resilience and underscore the importance of explicitly addressing the challenges that give rise to this resilience. Many participants expressed their desire for their struggles to be reported in detail, to enhance understanding of both the depth of these challenges and the strategies they employ to overcome them. Each theme presented in the subsequent sections illustrates the challenges faced by survivors and the strategies they implemented, supported by direct quotes from participants. To respect participants’ individuality while avoiding the arbitrariness of pseudonyms or the impersonality of numbers, a random initial was assigned to each participant. Direct quotes translated from French are identified with an asterisk.
Challenging Norms and Striving for Sexual Liberation by Educating Oneself
Participants’ accounts revealed the significant role of sexual education in shaping their sexual health, well-being, and empowerment. Many participants expressed the profound impact of inadequate sexual education, which left them vulnerable to myths, misinformation, and internalized stigma. Despite these challenges, participants described several strategies they use to enhance their sexual health knowledge, including learning about their bodies, learning to recognize various forms of oppression, and questioning normative narratives to foster sexual emancipation.
Many participants navigated their sexual education independently, preparing for active sexual life without guidance. L. characterized this experience as “living in darkness.”* To address this, participants turned to online resources, allowing them to normalize their experiences and reject rigid definitions of “normal” sexuality. G. captured this realization: I was comparing myself to normality, but in fact, there is no normality. Every woman is different and every woman has problems too. It’s not just genital cutting.*
For many, learning about sexuality began theoretically (i.e., through reading or conversations), before evolving into personal exploration. This process often started with getting familiar with their sexual bodies (e.g., by using a mirror to see their genitals for the first time) and progressed to discovering what felt pleasurable (e.g., through masturbation and using sex toys). These experiences enabled women to identify their sexual preferences and assert boundaries, facilitating communication with their partners. M. reflected on how gaining sexual knowledge allowed her to advocate for her own pleasure: My second marriage came at a time when I was already mentally aware and I had a good rapport [to sex]. I was able to voice and say “you know what? I really want to know myself. I want to know my body, I want to know where are my [erogenous] points. What do I enjoy most?” So in that marriage, it was the first time that I experienced orgasm.
This ongoing learning process helped participants move away from preconceived notions about sexuality and reinforced their agency in defining their own sexual experiences.
Participants also highlighted how sexual education heightened their awareness of the intersecting forms of oppression that shape their sexuality. They described navigating gendered expectations, such as virginity, purity, and “marital duty,” reflecting the influence of broader systems of control policing women’s bodies. Recognizing these structures appeared as a crucial first step in challenging and breaking free from them, as K. explained: Understanding that because we have learned so much oppressive stuff, it’s natural that a few of those ideas are still circulating in the system and that these ideas are not actually important or true. So I lean a lot on that.
Participants elaborated on how this awareness involved understanding the nature of the oppressions, such as racial injustices and gender-based violence, and how these oppressions are enforced and sustained through mechanisms like the culture of silence perpetuating taboos around sexuality or misogynistic, patriarchal, and cultural norms. As S. bluntly said, “It’s a fucking man’s world.” Participants also reflected on the importance of understanding the impacts of these oppressions on sexuality (e.g., distrust of female sexual pleasure and rigid expectations about acceptable sexual practices) and the resulting consequences for women such as sexual submission and limited sexual autonomy. Many identified migration as a catalyst for questioning these norms, but also noted that oppression persists in Western contexts, albeit in different forms. As V. noted, gender-based oppression remains present in Western societies: When I moved here and I heard about the feminist movement, I didn’t understand why it was even a thing. I was only a teenager. I’m like “what are people talking about? Everything is so great here in Canada. I don’t know what they’re talking about.” And then actually going through your life and realizing there’s little things here and there. There’s all these subtle ways in which it starts [to] build up and then you’re like “oh actually, there is a need for feminism”. It was a kind of [a] turning point for me.
Additional strategies included accessing educational resources, engaging in therapy, and participating in feminist and social justice movements to develop a deeper awareness of the control imposed on women’s sexuality. Several participants noted that this awareness helped them reclaim control over their sexuality, enabling their sexual liberation.
Beyond awareness, participants described how sexual education allowed them to question cisheteronormative narratives around female sexuality. Many reflected on feelings of inadequacy or abnormality when confronting societal expectations of female sexuality and sexual standards, particularly those shaped by pornography. V. specifically noted that “mainstream sexuality” no longer suited her, describing it as “just catered to the male gaze.” Through access to information and education, participants redefined sexuality on their own terms, moving beyond traditional notions centered on penetration and genitalia to emphasize intimacy, pleasure, and emotional connection, like K.: My idea of sexuality has really widened. I would have said, even five years ago, that it had to be something genital, right? Now, I think that sexuality is really a lot of things. It can be when you give each other a really flirtatious look or grab each other’s bodies in a certain way when you’re in public. It’s the erotic. It’s really wide now for me.
For some, this journey intersected with their evolving sexual identities, as illustrated by J., who embraced her bisexuality through exposure to alternative sexual narratives: I had the opportunity to get more information. I discovered [name of health clinic] and I read the books they shared [on social media], the resources they give, and that enabled me to go a lot further and to know that in fact, nothing is really as complicated as they tell us in Africa. Nothing is as psychologically burdensome as what they teach us. […] I saw two girls kissing on the subway and it was amazing, I’d never seen anything like it except in porn movies of course [laughs]. So seeing this [in real life] opened up something […].*
Participants emphasized the importance of unlearning preconceived notions and sexual stereotypes ingrained from an early age through education and introspection. V. emphasized the importance of positively reframing sexuality in a manner that prioritizes their own needs and dismantles socially and culturally imposed limitations: I’ve been trying to maybe read some books that are positioning sex in this more positive way, talking about different types of bodies having sex and disabled people and women of color and just what you don’t see in the mainstream. You see a very airbrushed version of sex. So I’m trying to change my relationship with it [sex] slowly, trying to find things that I’m interested in or that excite me, but it’s hard. It’s not an easy answer.
By rejecting restrictive norms and redefining their own sexual narratives, participants reclaimed control over their sexuality, ultimately fostering empowerment and well-being.
Cultivating Sexual Agency Through Resilience
Participants highlighted the transformative role of resilience in cultivating sexual agency, identifying several interconnected processes. These included fostering body acceptance and reappropriation as foundational steps for reconnecting with their identities as sexual beings, transitioning from passive to active sexual agents by regaining control over one’s sexuality, and developing the capacity to articulate and advocate for their sexual needs in personal and institutional contexts.
Many participants recounted a profound disconnection from their bodies and sexuality, shaped by internalized stigma and dominant narratives that framed FGC/M as rendering them “incomplete” as women. For some, this led to struggles with negative body image, self-consciousness, and feelings of shame or self-disgust. These challenges underscored the importance of body acceptance and reappropriation as essential steps for reconnecting with their sexuality. One participant, A., emphasized the psychological aspect of this process: Sexuality isn’t just physical, it’s also psychological. So that’s what helps us. Cut women can [experience pleasure]. It still takes acceptance. You don’t have a choice; you have to accept your body. You have to find out for yourself what could help you enjoy your sexuality.*
For some, reappropriation was a process of redefining femininity and reclaiming ownership of their desires, challenging the narrative that FGC/M had irreversibly diminished their womanhood. This was illustrated by K., who reflected on the transformative role of therapy in regaining bodily ownership: I went and did more therapy around [genital cutting] and began to understand more about maybe how it had impacted me emotionally and sexually, and it was through doing that healing work that I began to feel like I owned my body more and more and more. And there’s something incredibly liberating about that. I wouldn’t have even said before that I didn’t have enough of that body ownership before. I didn’t realize it. But when I gained more of it, it was pretty clear to me.
Self-acceptance was highlighted as a strategy for coming to terms with their experiences of FGC/M and for fostering a sense of comfort, confidence, and appreciation toward their bodies. This was mainly achieved by participants practicing self-love and self-care, and was seen as a gradual process requiring significant emotional efforts. L. emphasized the importance of learning to accept and appreciate one’s body, despite challenges: Don’t stay in self-contempt, getting caught up in it. It’s hard to fight it, but you can do it with help, with solutions, with people who can help you appreciate yourself and your body.*
Another key element highlighted by participants was the challenging yet vital work of rebuilding a connection between body and mind—specifically the reintegration of physical sensations with emotional awareness, particularly after experiences that may have resulted in dissociation. This involved “being aware” (K.) of bodily sensation and feelings. V. explained how being mindful during sex enhanced her attunement to sensations and, ultimately, allowed her to find pleasure in sexual experiences: I’ve been reading this book, this Buddhist book about mindfulness, and I feel so much of that applies to sex. You need to be mindful, you need to be in your body rather than your head. I tried [to] kind of do that because when I find my mind wandering during sex, I try to bring my attention back to my body and how my body feels and how this feels good. The little details of brushing, my skin being brushed, or this and that, just like bringing myself back to the physical sensation of it.
Several participants shared experiences of evolving from being passive subjects in their sexual lives—merely “enduring it”*(U.)—to actively reclaiming control over their sexuality. Passivity was often shaped by resignation, compounded by experiences of gender-based violence or healthcare providers’ dismissal of their sexual health concerns. Others articulated a resolute determination achieving sexual fulfillment, a transformation characterized by a shift from simply “surviving”* sexuality (X.) to actively experiencing and embracing it. D. articulated this shift: Taking power over your sexuality. It’s important to have pleasure. It’s important not just to be a spectator. It’s important to be an actor. To try to get to know your body, to find out what gives you pleasure. So to really take power over it.*
Prioritizing pleasure was viewed by some as an act of resistance against patriarchal norms that expect women, especially women from FGC/M-practicing communities, to be sexually passive. B. highlighted the significance of sexual autonomy within intimate relationships: If you want [sexual] pleasure, you have to take it. That’s what I tell my partners: I’m here to take my pleasure, not to give it to you.*
Many, like D., channeled their resilience into actively seeking solutions and adopting a proactive mindset: To improve, you have to be proactive, to determine what I need. I just need to get out of my comfort zone, get out of my routine and look for resources.*
This journey often marked a shift from viewing oneself solely as a victim to embracing a more empowered survivor perspective.
The traditionally passive role assigned to women has often restricted their ability to articulate their emotions, needs, and boundaries. The stigma and taboos surrounding FGC/M compounded these communication barriers, making interactions with partners and healthcare providers particularly challenging. Additional complexities were present from intersecting vulnerabilities, such as experiences of gender-based violence, navigating migration and racism, or facing language barriers in a new country, complicating the advocacy for their needs. Despite the risks of reopening past trauma by discussing FGC/M-related issues, many participants highlighted the importance of self-expression as a key strategy for developing sexual agency. B. stressed the significance of breaking the silence: Don’t be embarrassed or shy to talk about it [FGC/M]. You should always talk about it. That’s all I can say. If you don’t talk about it, you can’t get the help you need. You can’t get support. If you suffer alone all by yourself, you’re going to suffer for nothing. You have to talk about it. You have to get it out in the open. There is plenty of help. You have to get it out, you have to talk about it without shame.*
Some noted that as they spoke about their experiences more frequently, it became progressively easier, ultimately contributing to the gradual strengthening of their sexual agency and fostering their sense of emancipation. T. described this feeling of liberation: [Talking about it] is an important step for me, where I’m starting to be more comfortable with myself. I feel free [laughs].*
For many, verbalizing their needs often acted as a catalyst for problem-solving. For others, speaking openly—sometimes as vocal activists—served as a subversive act in itself, allowing them to reclaim control over the narrative surrounding FGC/M survivors. This was the case for J. who, inspired by a longtime activist friend, had begun to speak out more freely and publicly about FGC/M: I want to talk about it, I want to push it. It’s almost provocative [laughs]. I do want to. I’m more open to talking about it precisely because of the anger [I feel]. There’s no reason why we should be the victims of this and we still have to keep quiet about it. No, we’re going to talk about it. And I know they don’t want us to talk about it, because a woman is supposed to be modest, she shouldn’t talk about these things, but it’s like I say, I’m going against the tide and I’m going to talk about it [laughs].*
By asserting their voices, participants actively resisted structures of oppression that sought to render them voiceless. Their experiences underscored that cultivating sexual agency was not just an individual journey but one deeply shaped by and in resistance to systems of power.
Building a Community of Care to Support Sexual Empowerment
Participants emphasized that while sexual empowerment must originate from within, it is also nurtured through supportive relationships. They described the importance of cultivating a network of peers, partners, and professionals who provided emotional support, validation, and guidance—collectively forming a community of care that played a pivotal role in their empowerment efforts.
Many participants shared feelings of difference and abnormality when comparing themselves to “other [uncut] women,” particularly following their migration to Canada. When pursuing steps to improve their sexual health or well-being, participants described feeling misunderstood, judged, or even ostracized by their families and entourage who disapproved of their efforts. These experiences reinforced a sense of isolation, with some participants perceiving their FGC/M-related challenges as unique, unaware that others had similar experiences. To mitigate this isolation, participants established a supportive community of care with peers who had similar experiences of FGC/M, serving as a vital source of solace and mutual support and understanding. Several participants emphasized the value of formal peer-led support groups, highlighting how such spaces fostered non-judgmental support and solidarity. V., who recently joined a support group, reflected on the significance of these groups in acknowledging intersecting identities and resisting reductive victimhood narratives: […] being in that group […], I could see myself reflected in so many of their experiences. They were all women of color, so there was an intersection. FGC is just one part of the entire experience. It felt like a little community, where your experience could be validated. Also, just having a space where you’re not seen as a victim is really good, because a lot of times, there is this Western gaze on FGC, of like “oh you guys are so oppressed!” And it’s almost used as a way to be racist towards some of our communities. […] So having a space where there is this understanding, […] like an empowering place and seeing us as full individuals… We are more than what happened to [us].
For many participants, these peer interactions fostered a sense of community and sisterhood, offering comfort and shared models of empowerment. R. described the safety and reassurance she found in peer support groups: We accepted everyone [in our support group]. It was a mix: religious people, old people, elderly people. A real mix. But it was the approach, it was the comfort. I don't know how to explain it, but it’s a very safe space. There’s no judgment. That helped me a lot.*
The validation received in peer spaces reinforced that participants were not alone, underscoring the critical role of peer support in healing and empowerment.
Participants frequently described their sexuality as deeply intertwined with marriage or committed monogamous relationships, emphasizing the pivotal role their partners played as members of survivors’ community of care in supporting their sexual empowerment. Many recounted emotional, psychological, and physical challenges related to FGC/M, particularly during penetrative intercourse—a practice often central to their relationships. These challenges sometimes led to marital conflicts, further straining their sexual well-being. Communication barriers, shaped by cultural taboos surrounding FGC/M and sexuality, compounded these difficulties, particularly when partners were uninformed or dismissive. To address these barriers, participants identified some strategies to foster partner support. Selecting an empathetic and respectful partner who demonstrated understanding of the impacts of FGC/M was deemed essential. Supportive partners fostered open discussions about sexuality and provided crucial emotional reassurance. E. recounted the solicitude of her current partner: Right from the start, the fact that I’d had FGM, he put his needs aside to look after me, to really know how I felt, how I lived with it. He really took an interest. He didn’t just run away.*
Several participants, like E., stressed that clear, open communication was key to navigating intimacy: Our partner is the one who really needs to know everything about our moods, everything about what’s going on in our bodies. When we decide to hide it, that’s where the danger lies.*
She also explained the importance of guiding her partner to show her preferences and needs: At the very beginning I was guiding him so he understood the way my body reacted. Of course, when you’ve been cut, it’s not the same as when you’ve not cut in terms of fragility, the products you can use to prevent irritation in that area. There are measures to take, positions to adopt so that it doesn’t hurt.*
Actively involving partners in the empowerment process, particularly through education about FGC/M, emerged as a critical strategy. B. shared how her partner took an active role in learning: And with him, really, I communicated a lot. I talked about everything. And he was someone who had also done a lot of research. Outside of my family, he was the first person I spoke to about genital cutting and clitoral issues. Because he was well researched.*
Involving partners in their empowerment journey helped distribute the emotional and cognitive labor of maintaining a fulfilling sexual relationship, fostering a more equitable dynamic.
A final essential component of a comprehensive community of care was professional support. Many participants reported living with various health issues stemming from FGC/M. Some participants had also endured additional traumas, such as rape, domestic violence, and gynecological and obstetric violence. Seeking professional support, whether medical, psychological, sexological, or psychosocial, was seen as an important step toward empowerment, as emphasized by R.: Finding resources, finding a centre, finding someone who’s been there and talking about it. Because on your own it’s difficult, but with two people it’s sometimes easier to find solutions and ideas. […] Don’t be alone. Don’t try to self-medicate, because sometimes that doesn’t help and makes the situation worse.*
Gynecological care, including clitoral reconstructive/reexposition/restorative surgery, and psychotherapeutic care were identified as transformative in promoting participants’ bodily autonomy and sexual empowerment. A. found that having access to psychological help was beneficial to her healing process: After I left my husband, I was in a centre for battered women. […] I had [access to] psychologists, so I was able to heal a lot of little wounds through that. Wounds that may not be linked to my sexuality, but everything is linked. Because when you’re subjected to domestic violence and you know that the root of it is sexual, by healing that, you heal a lot of things.*
However, many participants, including X., acknowledged the systemic inequities in accessing professional support, especially as racialized migrant women living in precarious situations: […] Despite all the qualifications I have, I experienced post-traumatic stress directly related to giving birth. People already suffer from postpartum depression. Even when you haven’t even had FGM. So imagine when you’re an immigrant woman, you’re vulnerable, you’re in a precarious situation, you have the burden of FGM, you have postpartum depression and on top of that you have post-traumatic stress because you didn’t get the support you needed and all that.*
As professional support was seen as an essential aspect of survivors’ community of care, participants stressed the need for accessible and adequately trained healthcare resources to ensure all survivors receive support, including those facing financial, cultural, language, or other types of barriers. Overall, empowerment was not a solitary process but one deeply embedded in relationships with peers, partners, and professionals.
Discussion
In this article, we used interpretive description to explore the strategies FGC/M survivors employ to overcome the potential impacts of FGC/M on their sexual health and well-being, providing an in-depth interpretive account of their experiences. To do so, we drew on intersectionality to account for power dynamics and broader structural factors shaping their experiences, while also considering how intersecting identities frame their sexual health experiences. We delineated three themes that illustrate the strategies FGC/M survivors use for fostering sexual empowerment. First, FGC/M survivors consider sexual education as a key strategy to learn about their bodies and understand the various forms of oppression and control shaping their sexuality. This knowledge helped them question normative sexual narratives and work toward sexual liberation. Second, survivors reported engaging in a body acceptance and reappropriation process, adopting an active posture within their sexuality and learning to express needs as ways to strengthen their sexual agency. Third, survivors expressed the importance of building a community of care, composed of peers, partners, and professionals, to support their sexual empowerment journey. Collectively, these strategies not only promote survivors’ sexual health and well-being but also demonstrate their resilience in reclaiming autonomy over their sexual lives while actively resisting the intersecting forms of oppression that shape their experiences.
Our findings highlight the importance of sexual education as a powerful tool toward sexual liberation. Many participants described bodily self-awareness as an initial step in this process, yet internalized cultural taboos and stigma frequently obstructed their journey. This aligns with the findings of a recent metasynthesis that found that the pervasive silence surrounding FGC/M and sexuality acts as a mechanism of control, reinforcing the sexual subjugation of survivors by limiting their access to sexual health knowledge (Gareau et al., 2025). Several participants of our study attributed their limited sexual education to being raised as women within African cultural contexts, where discussions of sexuality were heavily restricted. This absence of knowledge cannot be understood without attention to colonial and patriarchal structures that have historically regulated and constrained the sexualities of racialized women. Colonial interventions explicitly sought to reshape African sexual norms, constructing African women’s bodies as hypersexual while simultaneously imposing expectations of sexual restraint (Osha, 2004). The legacy of these colonial narratives persists today, shaping gendered norms that silence and marginalize discussions about sexuality (Osha, 2004), thus reinforcing women’s subordination by limiting their ability to access essential sexual health knowledge and assert sexual agency (Gareau et al., 2025; Villani, 2023).
Migration emerged as a critical factor in participants’ eventual access to more comprehensive sexual health education. Physical and cultural distance from their birth countries created opportunities to encounter diverse perspectives and alternative frameworks of sexuality. Prior research supports this finding, demonstrating that migration can influence how FGC/M survivors experience sexuality (Agboli et al., 2019), offering some freedom from restrictive gender norms and increased exposure to pluralistic perspectives on sexuality (Gray et al., 2022). However, this shift is not without tension. Dominant models of Western sexual health frequently fail to account for the intersecting oppressions faced by migrant women (Gray et al., 2021). These models often universalize sexuality through Western-centric, heteronormative, and biomedical frameworks (Palm et al., 2019; van der Toorn et al., 2020), overlooking survivors’ realities and reinforcing feelings of exclusion, as survivors must navigate both the restrictive gender norms of their birth country and the often homogenizing and pathologizing FGC/M-related discourses of the host country. Our findings reveal that survivors’ sexual empowerment involves an awareness and a critical examination of these intersecting systems of oppression. Becoming aware of how their sexuality has been shaped and often constrained by both pre- and post-migration forces plays a central role in their process of reclaiming agency. For instance, Western biomedical narratives frequently pathologize and victimize FGC/M survivors, defining their sexuality exclusively through pain, trauma, and loss of pleasure (Catania et al., 2007; Paakkanen, 2019; Palm et al., 2023). These narratives, rooted in colonial discourses, strip survivors of agency and reinforce representations of African and Muslim women’s sexualities as passive and in need of rescue (Paakkanen, 2019; Palm et al., 2023; Sarkar, 2017; Silverman, 2004). Yet, FGC/M survivors in our study resisted these narratives by actively seeking sexual health knowledge and generating alternative understandings of their embodied experience. This resistance was not just personal; it was a form of political subversion. By reclaiming sexual subjectivity and disrupting both traditional and Western pathologizing discourses, survivors challenge the very systems that have historically marginalized them, highlighting the resilience of survivors.
Our findings illustrate how FGC/M survivors cultivate sexual agency through body acceptance and reappropriation, transitioning from passive to active engagement in their sexuality and learning to express their needs. This process was not merely an individual transformation but a negotiation of systemic barriers impacting survivors’ sexual autonomy. Participants indeed reported encountering systemic barriers such as limited access to specialized sexual healthcare, restrictive gender norms, and external pressures to conform to prescribed sexual expectations—barriers well documented in existing research (Albert et al., 2023; Gareau et al., 2025; Ziyada & Johansen, 2021). These barriers were compounded by race, migration status, socioeconomic status, sexual orientation, and parental status (e.g., single mothers). Therefore, fostering agency is not solely a matter of individual will or resilience; it also necessitates structural support to address compounded forms of oppressions to ensure equitable access to resources that empower FGC/M survivors to build and exercise sexual agency. Furthermore, the transition from passivity to active self-advocacy emerged as a critical step in building sexual agency. Participants engaged in micro-acts of resistance, such as self-love and body acceptance. These acts should be understood within broader frameworks of reproductive justice and sexual rights positioning survivors’ agency within systems of power’s influences (Bay-Cheng, 2019; Cense, 2018). Indeed, though often individual, these acts carried broader sociopolitical significance, particularly within contexts where women are conditioned to perceive their bodies as abnormal, incomplete, or different. In this context, the exercise of sexual agency transcends personal empowerment; it constitutes a form of resilience against structural forces that constrain sexual autonomy. Addressing the structural determinants of survivors’ sexual health is therefore critical, as sexual agency does not emerge in isolation but within specific sociopolitical conditions that either enable or restrict the ability to reclaim sexual autonomy (Lang, 2012).
Our findings underscore the crucial role of the community of care—including peers, intimate partners, and healthcare providers—in participants’ sexual empowerment process. While Western models of resilience often emphasize individual responsibility (Ungar, 2008; Wang et al., 2014), our results highlight the collective and relational nature of this process. Peer networks and community spaces emerged as key sources of validation, offering emotional support that helped counteract the isolation produced by stigma and cultural taboos. These findings extend prior research demonstrating that community support fosters healing and empowerment for survivors of gender-based violence (Gregory et al., 2022; Konya et al., 2020; Ogbe et al., 2021). However, access to such support, particularly from formal health services, remains uneven and is shaped by structural inequities linked to gender, race, migration, and socioeconomic status (Baciu et al., 2017). Migrant and racialized women, for instance, often encounter culturally insensitive care in which their experiences are met with disbelief, judgment, or dismissal (Cabieses et al., 2024; Drewniak et al., 2017). These encounters reproduce gendered and racialized power dynamics in healthcare settings. In this context, intimate partners could either serve as a source of support—through understanding, encouragement, and open communication—or as a barrier, particularly when they held restrictive or uninformed views on sexuality. The findings presented here underscore how empowerment strategies must actively take partners into account to address the enduring influences of patriarchy that directly shape gendered dynamics within relationships. Healthcare professionals also play a vital role in survivors’ community of care. Yet, their approach is often shaped by medicalized discourses that reduce sexual health to a biomedical issue requiring correction (Palm et al., 2019; Villani, 2023). At the same time, a persistent lack of specialized training often leads providers to adopt either an invasive or dismissive approach toward FGC/M survivors (Evans et al., 2019a; Kawous et al., 2020; Ziyada & Johansen, 2021). This absence of specialized care has been identified as a critical barrier to sexual empowerment among FGC/M survivors (Evans et al., 2019b). Our findings highlight how the position of FGC/M survivors in Western contexts adds additional layers of systemic discrimination when accessing care, which is frequently either paternalistic or disregarding their agency altogether. Despite these challenges, many participants viewed healthcare providers as vital members of their community of care and as essential allies in their empowerment journeys, calling for improved training to ensure culturally competent, survivor-centered care in Western contexts like Canada.
Limitations
Our sample may reflect certain biases. First, recruited participants were largely motivated by a desire to contribute to change regarding FGC/M, which may exclude perspectives from women who support or hold neutral views on the practice. Second, since recruitment materials explicitly mentioned sexual health, it is likely that those who participated were already comfortable discussing sexuality, potentially leading to a more progressive perspective on sexual health and well-being. Third, the decision not to use interpreters limited participation to women fluent in English or French, potentially excluding newly arrived immigrants or those less integrated into Canadian society.
Conclusion
This article underscores the transformative potential of education, action, and support strategies in advancing survivors’ sexual health and well-being. Our findings illuminate the strength, resilience, and agency of FGC/M survivors, who actively resisted reductive and pathologizing narratives. Far from being passive subjects, participants actively promoted their sexual well-being by drawing on the support and care from peers, supportive partners, and informed healthcare providers. Yet, the path toward sexual empowerment of FGC/M survivors remains constrained by systemic barriers rooted in racism, sexism, and colonialism. Future research should prioritize the development, implementation, and rigorous evaluation of intersectional, survivor-informed interventions aimed at addressing the structural barriers that undermine access to comprehensive and affirming sexual healthcare. Such efforts are essential to supporting women in reclaiming their rights to sexual health, pleasure, and self-determination. Importantly, this work must recognize survivors not merely as individuals affected by gender-based violence but as active agents whose knowledge and leadership are central to advancing more equitable and responsive care frameworks.
Footnotes
Acknowledgments
We would like to express our deepest gratitude to the women who agreed to take part in this study. We hope to have offered an accurate interpretation of their experiences and, by highlighting sexual health promotion strategies, to have inspired hope among FGC/M survivors seeking improved sexual well-being and satisfaction. We also wish to reiterate that all survivors of gender-based violence deserve to feel sexually healthy, in whatever way they define sexual health. Our sincere thanks go to the community members and healthcare professionals who assisted in distributing recruitment materials and supported us throughout the challenging recruitment process, with special appreciation to Dr. Isabelle Boucoiran for her invaluable help.
Ethical Considerations
Our study was approved by the ethics review boards of three institutions: Université de Montréal (CERSES-21-002-D, #2020-1032), Centre Hospitalier Universitaire Sainte-Justine (#2022-3896), and Centre intégré universitaire de santé et de services sociaux du Centre-Ouest-de-l’Île-de-Montréal (#MEO-21-2022-3260; MP-21-2022-3896).
Consent to Participate
Informed consent was obtained from all individual participants included in the study. All participants provided verbal informed consent prior to beginning the interview.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fonds de recherche du Québec en santé [grant number 299194].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
While preparing this article, the first author utilized ChatGPT to assist with translation and to address grammatical, syntactical, and spelling issues typically encountered by non-native English speakers. Following the use of this tool, the authors carefully reviewed and revised the text as necessary and accept full responsibility for the final content of the publication.