
Abstract
Advance care planning involves understanding and sharing values and goals to ensure people with serious illnesses receive treatment that is consistent with their preferences. With the growing treatment options available to patients living with advanced heart failure, advance care planning is regarded as a means of preserving individual autonomy. Despite significant public awareness campaigns, research, and interventions to increase advance care planning, it remains under-utilized in heart failure care. The aim of this research was to gain an understanding of how patients with heart failure understand and express their autonomy through the process of advance care planning. Critical qualitative multiple-case study methodology was used. Cases were constructed using data from 19 interviews with seven patients, eight caregivers, and nine healthcare providers from across two institutions. Constructions of autonomy were developed using within- and across-case analysis guided by a relational conception of autonomy based in feminist ethics. There were three key findings: (1) advance care planning is understood as external to treatment decision-making within the current biomedical landscape; (2) the experience of autonomy in advanced heart failure is incongruent with the dominant individualistic approach; and (3) advance care planning is influenced by interpersonal relationships and responsibilities as well as interpersonal and social power dynamics. Although advance care planning is considered a practice that preserves individual autonomy, interpersonal, institutional, and societal level relationships were all heavily influential in this practice. Future research should consider the advancement of advance care planning, and the enactment of autonomy, using a relational framework that acknowledges autonomy is shaped by institutional, social, and interpersonal relationships.
Introduction
Heart failure (HF) currently affects more than 64.3 million people worldwide and is rapidly growing in prevalence due to an aging population and improvements in cardiovascular disease diagnostics and management, leading to increased survival rates (Groenewegen et al., 2020; Khan et al., 2024; Savarese et al., 2022). HF is considered “advanced” when patients continue to experience symptoms such as shortness of breath, fatigue, and palpitations at rest and display marked limitation of physical activity even with optimal medical therapy. Despite the advanced stage of disease, a number of treatment options exist including surgical and minimally invasive interventions, device implantations (i.e., pacemakers and cardioverter-defibrillators), heart transplantation, mechanical circulatory support, and inotrope infusions (Heidenreich et al., 2022). Patients with advanced HF face many complex decisions along the illness trajectory related to medications, device options, and the pursuit of various therapies and procedure (Maddox et al., 2021; Matlock et al., 2017). Yet, research has found that patients often have limited involvement in these decisions and may not have an in-depth understanding of the risks and benefits of each medical option, reducing their ability to participate in decision-making (Matlock et al., 2017).
Advance care planning (ACP) is a practice that enables individuals who have decisional capacity to identify their values, to reflect upon the meanings and consequences of serious illness scenarios, to define goals and preferences for future medical treatment and care, and to discuss these with family and healthcare providers (J. Rietjens et al., 2021; J. A. C. Rietjens et al., 2017). Current clinical guidelines for HF management recommend that ACP be initiated early and often in the disease trajectory; most recommendations favor a proactive approach and suggest discussing ACP during specific milestones such as with each hospitalization, change in health status, or device implantation (Allen et al., 2012). Participating in ACP has been associated with increased quality of life, fewer acute care admissions, lower rates of depression and anxiety in caregivers, and lower healthcare costs at the end of life (Detering et al., 2010; Dixon et al., 2015; McMahan et al., 2021; Zhang et al., 2009). Increasing ACP engagement for HF patients could lead to decreased rates of hospital admission, decreased stress and anxiety, improved patient–provider communication, and increased patient and family satisfaction with end of life care (Houben et al., 2014; Nishikawa et al., 2021; Teno et al., 2007). Currently, the majority (76%) of HF patients do not participate in ACP, despite educational interventions and clinical guideline recommendations (Bose Brill et al., 2024; Evangelista et al., 2012; Habal et al., 2011). However, there has been a shift in how ACP is understood, from being a document-driven practice focused on specific treatment decision-making to being a process that involves communication regarding personal goals, values, and preferences (J. Rietjens et al., 2021; Sudore & Fried, 2010). Despite this conceptual shift, both research and clinical practice continue to focus on the role of formal medico-legal documentation in the process of ACP, and ACP continues to be provided in an individualized manner with limited impact on patient outcomes (Malhotra et al., 2020; Nishikawa et al., 2020).
The last six months of life for HF patients are often associated with frequent hospital admissions, invasive procedures, and intensive care admissions (Bose Brill et al., 2024; Goodlin, 2009; Ko et al., 2008; Romanò, 2024). This trajectory most often results in a hospital death, despite evidence that many HF patients may prefer supportive care over intensive intervention at the end of life and want to die at home (Formiga et al., 2004; Kitakata et al., 2021; MacIver et al., 2008). ACP is often framed as a practice that can mitigate negative outcomes by ensuring care providers are aware of patient preferences prior to entering the end-of-life phase. However there remains very limited patient engagement and low ACP participation rates in patients with HF despite clinical guideline recommendations, public awareness campaigns, and over 30 years of research and intervention development (Bose Brill et al., 2024; Fried et al., 2006; Habal et al., 2011). This low level of engagement highlights the need for further understanding of how patients, families, and healthcare providers view, understand, and approach the practice of ACP in relation to their experience of autonomy (Killackey et al., 2019a, 2019b; J. Rietjens et al., 2021). The purpose of this study was to gain an understanding of how patients living with HF understand and express their autonomy through the process of ACP. An additional aim was to characterize the way social location mediates the experience of autonomy and participation in ACP for patients with advanced HF.
Theoretical Framework
Feminist Bioethics and Relational Autonomy
Feminist bioethics developed within philosophical thought as an alternative to the principle-based approach of traditional bioethics, which is the ethical framework most commonly employed in the healthcare setting (Sherwin, 1992). Feminist ethical theory brings attention to the social location of moral agents in general with an explicit focus on vulnerable and oppressed groups (Mackenzie et al., 2014; McLeod, 2002; McLeod & Sherwin, 2000; Sherwin, 1992) but, as opposed to mainstream feminist theory, does not necessarily prioritize gender over other social factors (Dodds, 2000). Relational conceptions of autonomy are driven by feminist concerns that people are embodied and develop and exercise their autonomy within social contexts (Stoljar & Mackenzie, 2022). Within feminist bioethics, relational autonomy is the name for a cluster of approaches to autonomy that emphasize the socially embedded nature of agents (Sherwin & Winsby, 2011). This approach attends to the social, political, and economic conditions that influence the identities and decision-making of moral agents and considers the embodied social location and experience of people (Sherwin & Winsby, 2011). Relational autonomy can be understood as the recognition that self-governance is both defined and pursued in a social context, and that this context influences the opportunities an agent has to express or develop autonomy skills (McLeod & Sherwin, 2000). Relational autonomy also seeks to identify the ways in which the ability to be self-directed is affected by social and political forces and rejects the idea that autonomy is an achievement of individuals (McLeod & Sherwin, 2000). Previous work has outlined the merit of using relational autonomy as a new framework for understanding and approaching the process of ACP for those who are chronically ill (Killackey et al., 2019b). Research suggests that ACP is often enacted as a process of negotiating values and meaning throughout the trajectory of an illness in order to maintain social identities and relationships (Johnson et al., 2016; Robinson, 2011; Singer et al., 1998). Drawing on the conceptualization of relational autonomy developed by feminist ethicists (McLeod & Sherwin, 2000; Sherwin, 1992, 1996, 1998; Sherwin & Winsby, 2011) which views autonomy as a dynamic capacity shaped by social context, we explored what can be understood about the experience of ACP using this alternative model that is rooted in relationships as opposed to traditional individualized understandings of autonomy (Beauchamp, 2016; Dworkin, 1981). We were specifically interested in the role of social location and how this influenced the availability of meaningful opportunities to develop autonomy skills.
Methodological Approach
Design
We employed a critical qualitative multiple-case study approach, guided by the concept of relational autonomy. The multiple-case study design was used to explore differences within and between cases (Baxter & Jack, 2008; Yin, 2009); this approach allowed us to develop a richer and more focused understanding beyond what is already known related to ACP in HF care (Dooley, 2002). ACP research has been taking place for several decades without producing significant uptake or improvement in participation rates (Habal et al., 2011). By using a critical perspective to highlight relationships of power and taken for granted assumptions (Kincheloe & Mclaren, 2005) and employing a case study approach, we developed an in-depth understanding of the relational and social context of ACP which builds on the significant, yet largely post-positivist, extant literature.
Reflexivity
Case study explicitly supports a flexible and responsive relationship between the researcher and participants, which allowed for enhanced examination of theoretical concepts in an empirical setting (Sandelowski, 2011). All authors are registered nurses, with several years of experience working with the various populations including cardiovascular patients, oncology patients, and psychiatric patients. As a team, we examined our positionality in relation to the research topic and research participants (Doyle, 2013) and the effect that our situatedness may have had on the setting and the people being studied, as well as examine how the research question was developed and what influenced this interest (Berger, 2015). Western society values autonomy, and within healthcare systems the principle of autonomy is frequently given priority over other relevant bioethical principles such non-maleficence and justice. Working in an individualized healthcare system influenced our interest in autonomy as well as our view that ACP has a role in chronic illness management from the perspective of healthcare providers. It is possible and perhaps even likely that participants did not share this viewpoint for any number of reasons, and therefore we were open to differing perspectives and ensured we approached interviews and engaged with participants in a way that encouraged them to share their unique and potentially converse perspective on this practice.
This study developed from the perspectives of healthcare professionals who work with chronically ill patients and their families, which is a relationship with an inherent power imbalance. Therefore, it was imperative to acknowledge the influence of our positionality in relation to the research topic and participants, and maintain flexibility with our versions of reality (Doyle, 2013). Doyle suggests that authentic contact with both the other and the self is necessary for a reflexive research process, and therefore in order to promote rigor, the primary author developed a reflexive journal to document evolving perspectives as this project developed (Doyle, 2013). The critical social paradigm also sees the researcher as a tool toward empowerment and advocacy (Guba & Lincoln, 2005). This goal resonates strongly with our nursing identities, as advocacy and empowerment are part of our professional values and moral obligations to our patients.
Setting and Sample
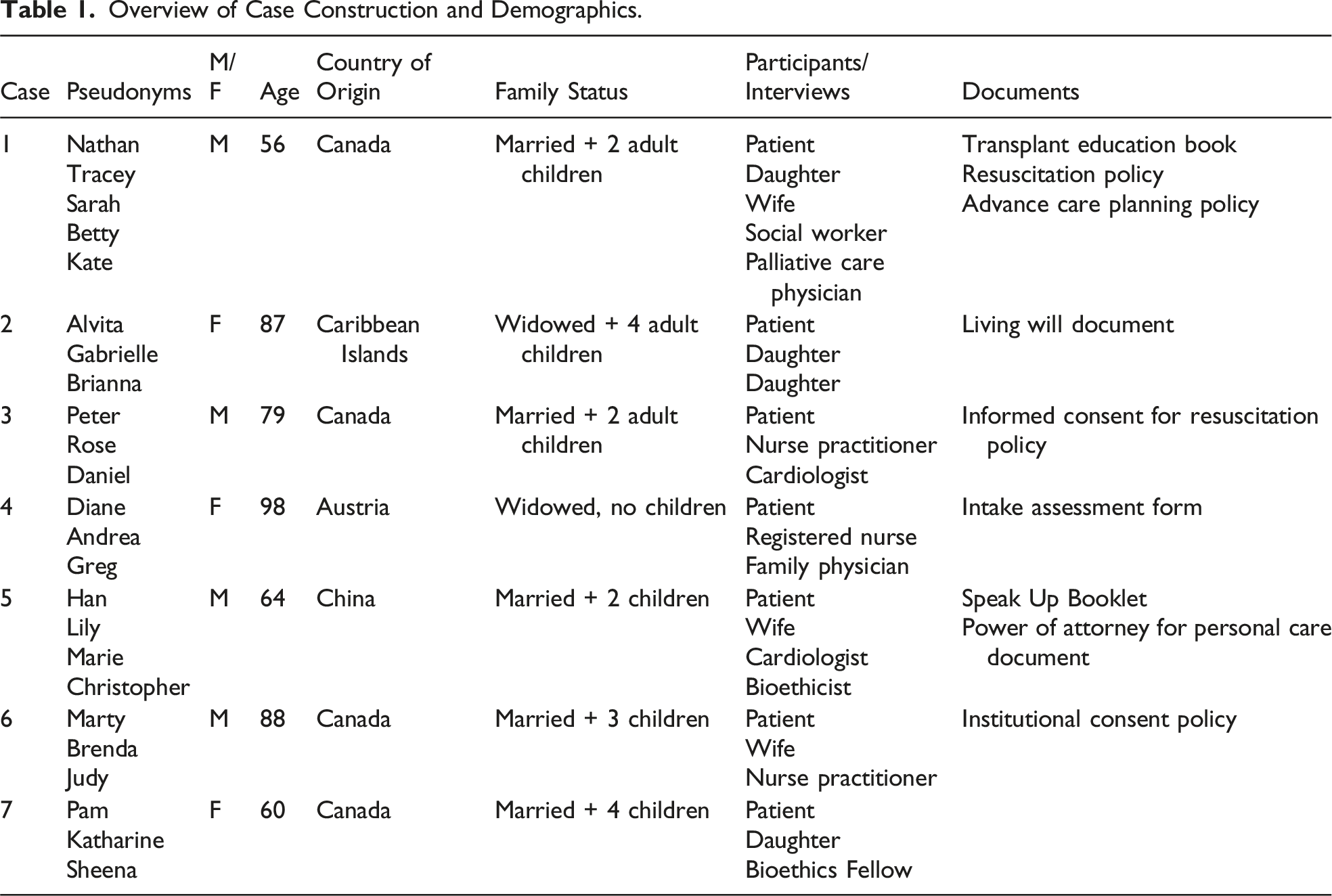
Overview of Case Construction and Demographics.
Data Generation
Cases were constructed beginning at the individual level by recruiting the person with advanced HF to participate in a semi-structured interview and then moved outward to capture the interpersonal level which involved family members and healthcare providers. Cases were also expanded to examine the institutional and social level, which involved analyzing relevant policies, legal documents, and educational materials. This approach facilitated the examination of multiple relationships among different types of participants and different types of data. We employed a variety of data collection techniques, including semi-structured interviews with participants, observation and field notes, and document analysis. Semi-structured interview included questions such as “What has it been like for you/your family to live with heart failure? What decisions have you made about your/your loved ones’ healthcare? What decisions have you made regarding your life since being diagnosed? What were some important factors you considered when making these decisions?” to unearth the realities of exerting autonomy within healthcare decision-making. Interviews were audio-recorded and transcribed verbatim, with identifying details removed. Interview transcripts were uploaded to NVivo 12 (NVivo Leading Qualitative Data Analysis Software (QDAS) by Lumivero, nd) to support data management and coding.
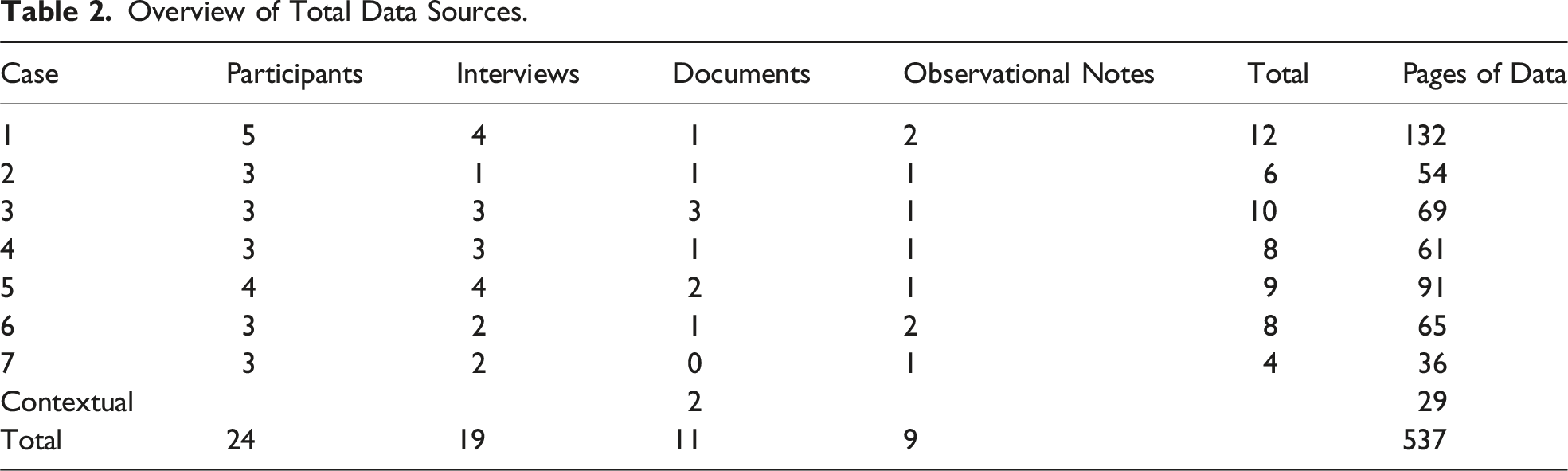
Overview of Total Data Sources.
Data Analysis
A critical case study analysis was undertaken to identify aspects of the ACP experience that may be common across cases or unique to an individual case. Using the principles of both within-case and cross-case analysis (Ayres et al., 2003), each case was constructed starting with the individual patient and working outward to include interpersonal relationships with family members and professionals. Once each case was constructed and analyzed, a cross-case analysis followed, where patterns, or similarities, as well inconsistencies across the various cases were identified and explored (Patton, 2002; Ritchie et al., 2013; Ritchie et al., 2003; Spencer et al., 2003). We undertook several rounds of coding, using both inductive and deductive analytic techniques to interpret the study data (Reichertz, 2014), moving between the empirical data and emerging analytical concepts to develop an overarching codebook. The first rounds of coding progressed inductively and were grounded in terminology employed by participants themselves (Elo & Kyngäs, 2008; Reichertz, 2014). Further analysis utilized a deductive approach to examine tensions within data, with specific attention to the relationship between the participants’ experience and the key documents being analyzed.
Documents can be thought of as physical evidence of social settings and provide a mechanism for understanding social and organizational practices (Coffey, 2014). Documents were analyzed not only for their content but also to better understand the circumstances under which such documents were created (Coffey, 2014) by examining the language used, what the purpose is of each document, and the relationships that are present both within an individual document and across documents (Coffey, 2014).
This critical case study analysis was guided by the concept of relational autonomy. In keeping with relational conceptualizations of autonomy, a critical feminist lens was used to explore power differences in the context of ACP. Combining a case study analysis with a critical feminist lens allowed power dynamics within social processes and relationships to be made visible so that they could be addressed (McLeod & Sherwin, 2000; Sherwin, 1992). In case study research, data from a variety of sources are analyzed together instead of examined individually, to provide a holistic understanding of a phenomenon and to incorporate an exploration of relevant relationships (Baxter & Jack, 2008). This strategy further strengthens the findings and credibility of case study research by allowing findings to inform one another to more fully understand the case being studied (Baxter & Jack, 2008). Data collection techniques (i.e., interviews, observations, and document analysis) and data sources were triangulated by incorporating the perspectives of patients, family members, and healthcare providers in order to support the study’s methodological rigor (Patton, 2002). As discussed by Baxter and Jack, each data source can be viewed as one piece of a puzzle that enhances the researcher’s understanding of the phenomenon as a whole, and study findings can by strengthened by “strands of data [being] braided together to promote a greater understanding of the case” (Baxter & Jack, 2008, p. 554). Therefore, what participants reported was not necessarily verified through triangulation but was used to encourage a more nuanced and holistic understanding of the experience of ACP in HF.
Results
Case Construction
Overall, there were 7 cases that were composed of 24 participants, 19 interviews, 11 documents, and over 500 pages of data (see Table 1 and Table 2). Pseudonyms were created to protect confidentiality. Patient participants ranged widely in age from 56 to 98 years and were equally split between men (n = 4) and women (n = 3); most cases also included additional family members such as spouses and/or children. In addition, relevant healthcare provider participants (i.e., nurse practitioners, physicians, and social workers) were included as well as key documents (i.e., heart transplant patient education booklet, living will document, and informed consent policy).
Key Findings
Three key findings were developed from this work: (1) ACP is understood as external to treatment decision-making within the current biomedical landscape; (2) the experience of autonomy in advanced HF is incongruent with the dominant individualistic approach; and (3) ACP is influenced by interpersonal relationships and responsibilities as well as interpersonal and social power dynamics. Each of these findings will be explored in depth.
ACP Is External to Treatment Decision-Making
First, ACP was found to be a complex social process, often positioned outside of standard treatment decision-making within the biomedical model. Although ACP is outlined in theory and in research as an attempt to overlap the biomedical and legal models of decision-making and incorporate personal preferences, values, and goals into treatment decision-making, in clinical practice, ACP was often reduced to decisions regarding resuscitation.
ACP as a Legal Process: ACP as an Idealized Application of Informed Consent
Current models for ACP are built upon the practice of obtaining informed consent and therefore follow a process of providing information to patients, with which they and their SDM may discuss potential future situation to allow SDM to provide informed consent on the patients’ behalf in the future. The following is an excerpt from the Speak Up Ontario work book, which is an educational resource and guided document for families wishing to engage in ACP: In Ontario, the law requires all health care providers to get informed consent, or refusal of consent, before providing a patient with any treatment or care. Health practitioners must tell you about your illness and what may be done to treat you. You then have the right to make a decision and agree to or refuse the treatments offered. This is called health care consent: it is a basic patient right to decide what health care to receive. Only in emergencies, to save a life or to reduce suffering, can people be treated without informed consent. Consent always comes from a person: either the mentally capable person or their substitute decision maker(s). If you are not mentally capable, the health practitioner will turn to another person, your substitute decision maker, who will then speak for you and make the decision about your care. Advance care planning lets you know who would speak for you. (Excerpt from Speak Up Ontario Booklet)
Analysis of this document highlighted that being informed is a necessary component of individual autonomy and is therefore a key aspect of ACP. In the Speak Up Canada Framework for ACP, “Learn” is the second component of ACP which involves “learning about different medical procedures and what they can or can’t do” (Speak Up, Case 5). As highlighted in earlier chapters, ACP is based on the process of informed consent, and the two requirements of informed consent are agency (or voluntariness) and information (Stoljar, 2011). Excerpts from both hospital center policies on informed consent cited four specific requirements:
For consent to be valid: (1) it must relate to the treatment; (2) it must be informed; (3) it must be given voluntarily; and (4) it must not have been obtained through misrepresentation or fraud. (Consent to Treatment Policy Document)
These four requirements can be reduced to the provision of accurate information and the existence of voluntary agency by the person providing consent. Additionally, Hospital Centre B outlined that to have informed consent, the health practitioner must: • Give the patient information that a reasonable person in the same circumstance would require in order to make a decision. • Provide the patient with information on the following matters and respond to the patient’s requests for other information about these matters: (1) the nature of the treatment(s), (2) the expected benefits, (3) the material risks, (4) material side effects of the treatment, (5) special or unusual risks, (6) the alternative courses of action, and (7) the likely consequences of not having the treatment. (Consent to Treatment Policy Document)
Our document analysis identified that these requirements are met when consent for surgery or medical procedure forms are signed, indicating that a patient had exercised their individual autonomy by actively making an “informed decision” or “informed choice.” HCP participants in this study acknowledged that being informed included providing good information on the life limiting nature of the HF and was a necessary requirement for patient autonomy. However, the type of information that was considered “good” was seldom identified: Hmm, like any other healthcare decision I think what’s important is that people have good information and have time to reflect, have the capacity to make a reasoned decision, which with some people can kind of wax and wane. Christopher (HCP, Case 5)
In his interview, Christopher (HCP, Case 5) minimized the import of ACP by comparing it to “any other healthcare decision” and applies the principles of informed consent, which includes patients being fully informed and competent to make a voluntary decision. In reality, healthcare decisions are rarely made in a way that aligns so closely to theory, as Greg (HCP, Case 4) described that patients and their families rarely “grasp everything that was said” which limits their ability to be truly informed. So, often patients will come to me after they see their specialist and they might have decisions to make … they will bring in one or two kids, or a close friend and discuss what the oncologist said about choices or the neurologist said about dementia. There’s always a specialist involved. So, it’s usually discussing what the specialist is saying or has written to me or called me and told me. Rarely that a patient really grasps everything that was said. Greg (HCP, Case 4)
HCP participants highlighted the tensions between the requirement of an autonomous person to be “informed” and the reality of how challenging it is to truly inform people of their disease process in a meaningful way. HCPs act as the gatekeepers of important health information and may actually reduce opportunities to develop capacities that are necessary to exercise personal autonomy (Dodds, 2000; Meyer, 1989). As Greg noted, patients and their families rarely “grasp everything that was said,” which limits their ability to be truly informed. Additionally, despite Christopher’s optimistic picture of the decision-making process, there is not always freedom to exercise careful consideration and reflection within the time-constrained structure of the healthcare system (Sherwin & Winsby, 2011; Meyers, 1989) and capacity often is not questioned unless there is a cognitive diagnosis or an obvious reason to examine capacity (i.e., the person is disagreeing with the care plan or is at the end of life). Therefore, ACP is based on an idealized application of informed consent.
ACP as a Personal Process: Wills, Personal Finances, and Burial Arrangements
Participants’ understanding of ACP was also related to the social conditions under which families manage and plan for death (Sherwin & Winsby, 2011) and the legalities associated with death such as wills, as mentioned by Judy (HCP, Case 6). Both provider and patient participants described how they associated ACP with personal family experiences where there was a strong focus on finances and funeral arrangements, as these were understood to be aspects of life that participants or their family members had clear control over. ACP was primarily understood as a personal process related to after-death legalities of finances and wills. As an example, when asked about her experience with ACP, Judy (HCP, Case 6) immediately relayed her experience supporting her mother and aunt through the financial and funeral planning process: Researcher: How did you learn about advance care planning? Judy: My mother is going to be 99 in January—my sister’s been my executor and power of attorney for my aunt who passed away and my dad who passed away and she is looking after our mother’s financial affairs. She has got everything on spreadsheets and transfers money here and there. Yeah, so it’s just the whole process I think, my parents have always been sort of proactive in sort of that regard. They, they bought, they bought pre-planned funerals, not the funerals but they have made arrangements too for cremation and, and plots and stuff and when they were in their 60s. Researcher: Do you have any experience having these kinds of conversations with patients and families that you work with? Judy: Hmm, nothing recently comes to mind.
Judy was not the only healthcare professional who related ACP to personal experiences; many HCPs used examples to describe end-of-life decision-making in their own families as opposed to providing clear examples of their professional role in ACP or their experiences integrating patient goals and values into their treatment decision-making. Taken together, this understanding reflects how ACP is often seen as external to treatment decision-making. Participants connected ACP to aspects of life outside of the healthcare system (i.e., pre-paying funeral expenses) which may have influenced their ability to approach and participate in ACP within the context of clinical relationships.
Although many participants were not familiar with the specific terminology of “advance care planning,” there were two types of future care decisions people generally referenced: (1) HF treatment decisions (i.e., medications, devices, and therapies) which were driven by the healthcare team and were guided by overarching treatment protocols, guidelines, and candidacy criteria, and were understood as largely outside of the control of patients. (2) Personal decisions (i.e., after-death legalities related to finances, wills, and burial arrangements) which were guided by a legal model and were understood as things that participants had control over.
When the legal and biomedical models of decision-making did overlap, the process of ACP was reduced to obtaining code status or determining resuscitation preferences. For example, when discussing ACP with Andrea, the director of care at an assisted living facility, she noted that during her initial assessment she asks what the residents’ “wishes” are, but then immediately dictates that this means they either sign for CPR or no CPR: Yes, I ask them during the initial assessment. We ask them about what their wishes are so they sign either a CPR or no CPR, so that was what we put in place so on their full assessment and care plan—we put the code status. Andrea (HCP, Case 4)
During this interview, Andrea also highlighted this section of the standard intake assessment form at the assisted living facility, which clearly prioritized documentation of code status as the primary method for communicating patient preferences. Many patients also initiated discussions of “do not resuscitate” (DNR) orders with the research team during interviews and were clearly familiar with this concept. Marty: My doctor knows that it’s DNA [DNR] [referring to existing ACP documentation]. Researcher: Oh okay, what does that mean? Brenda (wife): Do not resuscitate. Marty: Do not resuscitate. Researcher: Okay and when did that decision take place? Marty: Many years ago.
The healthcare decisions that patients viewed as under their control related specifically to refusing resuscitation but seemed to exclude decisions about the treatment plan leading up to the resuscitation point or involvement in conversations regarding consent to treatment. Documentation of a DNR underpinned by the overarching power of the legal model was seen as the only way for patients to exert their autonomy in the healthcare system, both by healthcare provider and patient participants. The legalities of consent combined with the dominant view that biomedical treatments should be pursued until the time of death together created a very limited role for patients looking to participate in ACP, and the only method available to help them enact their autonomy was DNR documentation (see Figure 1). ACP is external to treatment decision-making.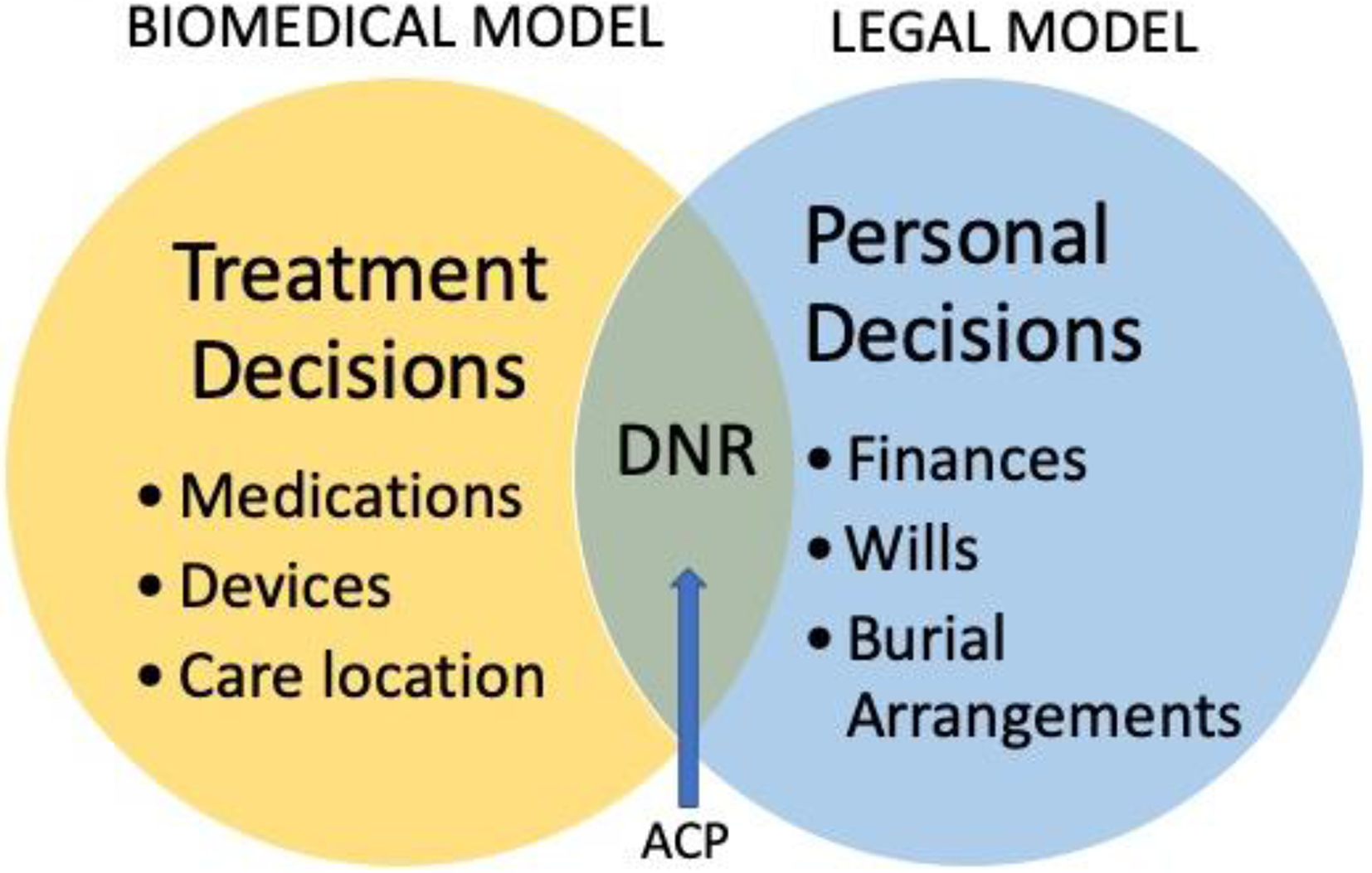
Agency Is Constrained in Advanced HF
Second, the agency of patients was constrained in advanced HF due to the limited understanding of complex information, limited treatment options, and the protocolized nature of decision-making. In addition to this constraint, ACP did not align with the individualistic view of autonomy that it is traditionally associated with (see Figure 2). For example, Daniel’s experience as a cardiologist stood in sharp contrast with Han’s experience as a patient trying to determine whether to move forward with a heart transplantation: Explaining the standard deviation of prognosis in heart failure and that we say 50% are dead in 5 years, but of course 50% in 5 years doesn’t mean that everyone is concentrated around that 50%, like some live 4 or some live 6 years. […] Heart failure is this thing that even I have trouble teaching internal medicine residents like—what is heart failure? It’s a syndrome. It’s a description of syndromes that partially relates to heart, partially relates to kidney and, and the prognosis is highly variable and even in experts we’re not that precise in being able to accurately estimate prognosis. Daniel (HCP, Case 3) To be honest, one of the big issues I am struggling with right now, yes, I am taking medication, but I can run around, go everywhere. Yes, my heart is weak, but at least I am not dying yet. Or maybe I am dying. I don’t know. Han (Case 5) Agency is constrained in advanced HF.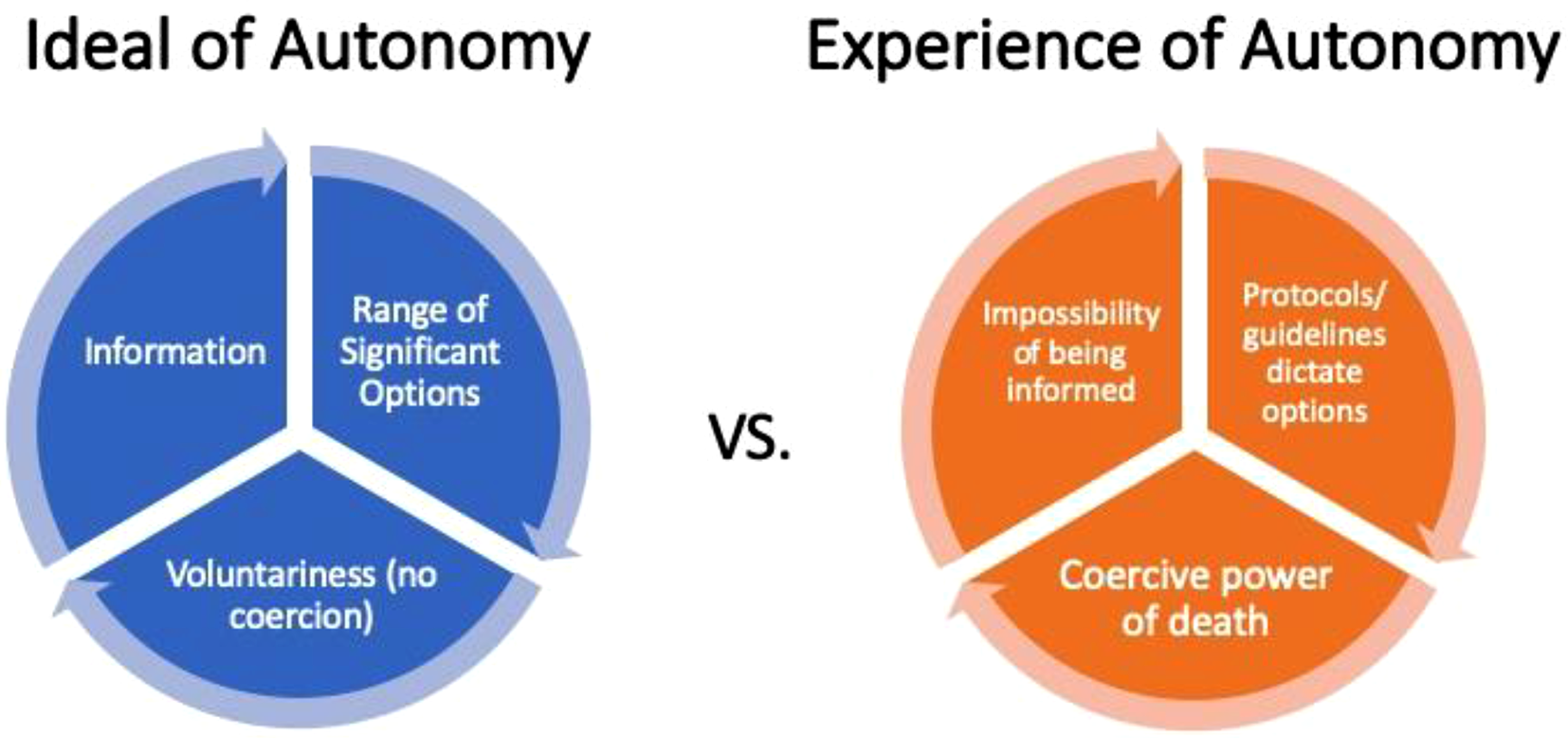
Daniel described the challenges he faces explaining prognostic curves and mortality rates to patients and expresses that he even struggles to teach medical residents about HF, stating that even experts are unable to accurately estimate prognosis for patients. At the same time, Han struggled with this uncertainty, as he rationally knew he was sick because he was taking medication, but he generally felt well and did not know if he was dying or not. This overall demonstrates the impossibility of being informed and the way patients have to make future care decisions with limited information.
Heart failure treatment decisions also were shaped by strict candidacy criteria. Decisions were not based on preferences or values of the patient or were even understood to be under the control of individual healthcare providers. Instead, they were framed as decisions dictated by the larger power of candidacy criteria (i.e., guidelines for determining which patients are able to receive specific therapies such as surgeries or devices) that deemed specific patients as “candidates” for various therapies. Because of the power of these guidelines, there were limited opportunities for participants to develop their autonomy related to healthcare decisions, as candidacy criteria and guidelines were viewed as the only legitimate way to address or respond to the illness, as highlighted in this quote by Peter: Peter: They have the stress test to determine that I am more likely a good candidate for a valve replacement, but they can’t do it yet. They have to wait and get the fluid off of my legs before I can do that. Researcher: So, they are trying to figure out whether you are a candidate? Peter: Well, I think that’s been decided. (Patient, Case 3)
In this instance, Peter frames the decision to pursue a valve replacement as having “been decided” by clinicians in conjunction with meeting the candidacy criteria, and was unrelated to his personal values or wishes. Because of this structure, patients often viewed themselves as having a passive role in healthcare decision-making and having no choices. Their options were limited to accepting treatments proposed by their clinicians, or refusing. Yet, the risks of refusing treatment often meant certain death, as Nathan outlined his “non-decision”: Nathan: Deciding to have a transplant was a big decision for me, but it was actually a non-decision in the end because I didn’t really have a choice, so. Researcher: Can you tell me a little more about that? Nathan: Well, um … [Long pause] yeah, I mean, there was a decision process in whether or not I was going to have the transplant at all, and that was after I had gone through the work up and I had to decide that myself, but then when you hear what the options are, the second option wasn’t very good. Researcher: Which was what? Nathan: Was to … I don’t know how much time I would have had but maybe a year, maybe two and that was it. (Patient, Case 1) Researcher: When you are thinking about this valve surgery and what this procedure will entail, is there anything that is important to you when you are making that decision? Peter: Hmm … {Long pause} well it’s basically that or nothing right? It comes down to that - not being given any options. (Patient, Case 3)
In addition to Nathan and Peter who highlighted they had no choice or limited available options presented to them, other participants noted that even when they did not wish to receive a certain therapy, such as Han who did not want an ICD insertion, they were told they had to move forward with the treatment or else they were at risk of dying at any time. This demonstrates how even when patients did have specific preferences in relation to treatments, they were often disregarded or rejected in favor of prolonging life at any costs.
Choosing between various medical treatments was not something that patients and families saw as within their domain of control, and patients described how they were not asked about their wishes or treatment preferences. In fact, patients didn’t have specific desires or preferences for care but instead they had preferences for how they would like to live the remainder of their lives, and often this involved merely trying to stay alive for their loved ones.
Autonomy Is Experienced Relationally
Finally, the findings indicated that autonomy in ACP was shaped heavily by interpersonal relationships and responsibilities as well as power dynamics and broad social forces. This last set of results demonstrates how autonomy is deeply connected to family roles and responsibilities, relationships with healthcare providers, social location, and social identities and is influenced by meanings attached to social constructs of ageism, individualism, and self-management. Han and Nathan outlined the role that life-stage and family considerations played into their health decision-making: Another thing I am considering is age. That time [implantable cardioverter-defibrillator insertion time] I was 50 okay, now I am 64 going, turning to be 65—this is another concern. When I was 50, I was more positive. I have to get it done. Why? My kids were still young, I still have to pay the bills, mortgage everything. Now, they are grown up, they have their own life. And financially we are okay. That’s why—my role changed. Han (Patient, Case 5) Researcher: What specifically were important factors in thinking about whether you want to move forward with it [heart transplant] or not? Nathan (patient): {Long pause} Well … just living I guess is the primary thing and I think that even though the family was leaving that choice up to me, they probably would rather have me around. I don’t know why. {Laughter} Sarah (daughter): Yeah, we wanted you around. Nathan and Sarah (Patient and Daughter, Case 1)
These excerpts from Han, Nathan, and Sarah’s interviews demonstrate how decisions were constructed in family life, and the way people made decisions was based on what was best for their family and not just for themselves. Families were expected to “want” to have each other around, and patients were expected to want to continue living to spend more time with their family members.
Age and ageism were also highly influential in ACP. Despite being defined as something that should be relevant for all adults, there was an underlying discourse of ageism that targeted ACP specifically at those who were older. There was a sense that when patients were younger, ACP was not relevant because “everything possible [should] be offered” or they were “not yet at that point” to discuss ACP. For example, in the case of Nathan, age 56, his wife stated: Yeah, so in his case I think it’s a little bit different like everybody almost wants to kill you with kindness. It’s a little bit of a different environment I think than your average person. But there wasn’t a lot of talk about that [DNR], of course with his age it was like well yeah, you know, full code, we will do everything, all that kind of stuff. Tracey (Nathan’s wife, Case 1)
Rose, a healthcare provider also emphasized Tracey’s point: I say nowadays lots of people they know exactly—we have patients that even at a younger age they come in with a living will or something right? Yeah, sometimes we don’t have to have another conversation. We don’t think it’s at that point yet, right? And to say, “definite no” to resuscitation, but you are only 40 years old right? Rose (HCP, Case 3)
These excerpts help highlight how if young patients did not want extensive treatment (i.e., implantable cardioverter-defibrillator or resuscitation), this was seen as the wrong decision by healthcare providers and was not easily accepted. Comparatively, when patients were older and had fewer responsibilities, there was a different assessment of the moral and social value of their lives and the value of keeping them alive with intensive interventions, as Betty suggests: And you know, we, they might have more of an effort if they have younger children obviously then they want everything possible to be offered to power of attorney. Betty (HCP, Case 1)
For Alvita (Patient, Case 2) and Diane (Patient, Case 4) who were two of the eldest study participants, age was seen as something that dictated treatment decisions and was extremely relevant to the discussion of treatment benefits. Diane (Patient, Case 4) explained that she did not see the point in invasive testing such as angiography because she did not see herself living much longer, and also did not have the desire to live much longer: They tested me for all kinds of things, he [cardiologist] wanted to have an angiogram and of course I had the test for that and my niece had to stay overnight and all that. Then I said: “I am not going to have that angiogram”—forget about it, at my age? Forget it. I also have now starting a breast cancer on my right side, forget it, I said at this age what are you going to do with it. For what should I go through? I mean I can’t live much longer {Laughter}. And if I have to live much longer I will probably lose my marbles too like the rest of them here. Diane (Age 98, Case 4)
Simultaneously, Daniel (HCP, Case 3) highlighted the variability between patients and the fact that judgements cannot be made broadly based on age due to the different perspectives people have regarding their own mortality. He pointed out that treatment guidelines largely do not have age cut-offs, so although this should be factored into treatment conversations, it may not be routinely addressed because it has been excluded from guidelines. Despite the importance that Alvita and Diane placed on their age and how this factored into their decision-making, Daniel (HCP) again highlighted that this is not necessarily the same for all elderly patients, and that age must be examined at a personal level in relation to what the patient and their family value and how they understand mortality and death: I think there’s such variation in terms of what people expect and their preparation for end of life, like I’ll have a 70 year old who is like nope, lived long enough I don’t care if I die suddenly, I don’t want a defibrillator not interested if I die in my sleep I am fine with that and I have 90 year old’s who are not. Daniel (HCP, Case 3)
Daniel also highlighted the limited data available to make decisions regarding HF therapy for older adults: We know that the data for older therapy is more modest. It’s a little bit opaque to find out exactly how many older patients with comorbidities are studied in clinical trials, like they usually have ranges and we spend a fair bit of time saying listen we don’t really know for sure. We think this works. We have some subgroup analysis but intentionally the drug companies and the device companies intentionally make it opaque to figure out exactly what kind of patients are enrolled because they would rather have over inclusion than under inclusion and so that’s the kind of data that we’re stuck with. Daniel (HCP, Case 3)
This quote is a direct example of the way ageism functions in current society and that it is not seen as worthwhile for drug and device companies to provide analyses specifically for older demographics of patients. These choices then can influence the way decisions are made in healthcare and can potentially lead to negative health outcomes due to this lack of data. Patient participants in this study recognized that receiving healthcare and treatments was a physical burden. After a certain point in their lives, they did not see the pursuit of treatment as something that was worthwhile for them; however, it was unclear whether this was explored routinely with their HCPs in the context of treatment decision-making, especially considering the lack of acknowledgement of age in many of the cardiovascular care guidelines.
In conclusion, autonomy was shaped by relationships with family members and healthcare providers, who were powerful and deeply influential in decision-making. Factors such as age, gender, and culture as well as broader social and political forces heavily shaped the experience of ACP (see Figure 3). Overall, conceptualizing autonomy as a relational experience that captures these factors may allow people in a variety of social locations to participate in the process, as opposed to only those who identify with a traditional, individualized approach to autonomy and decision-making. Autonomy is relational.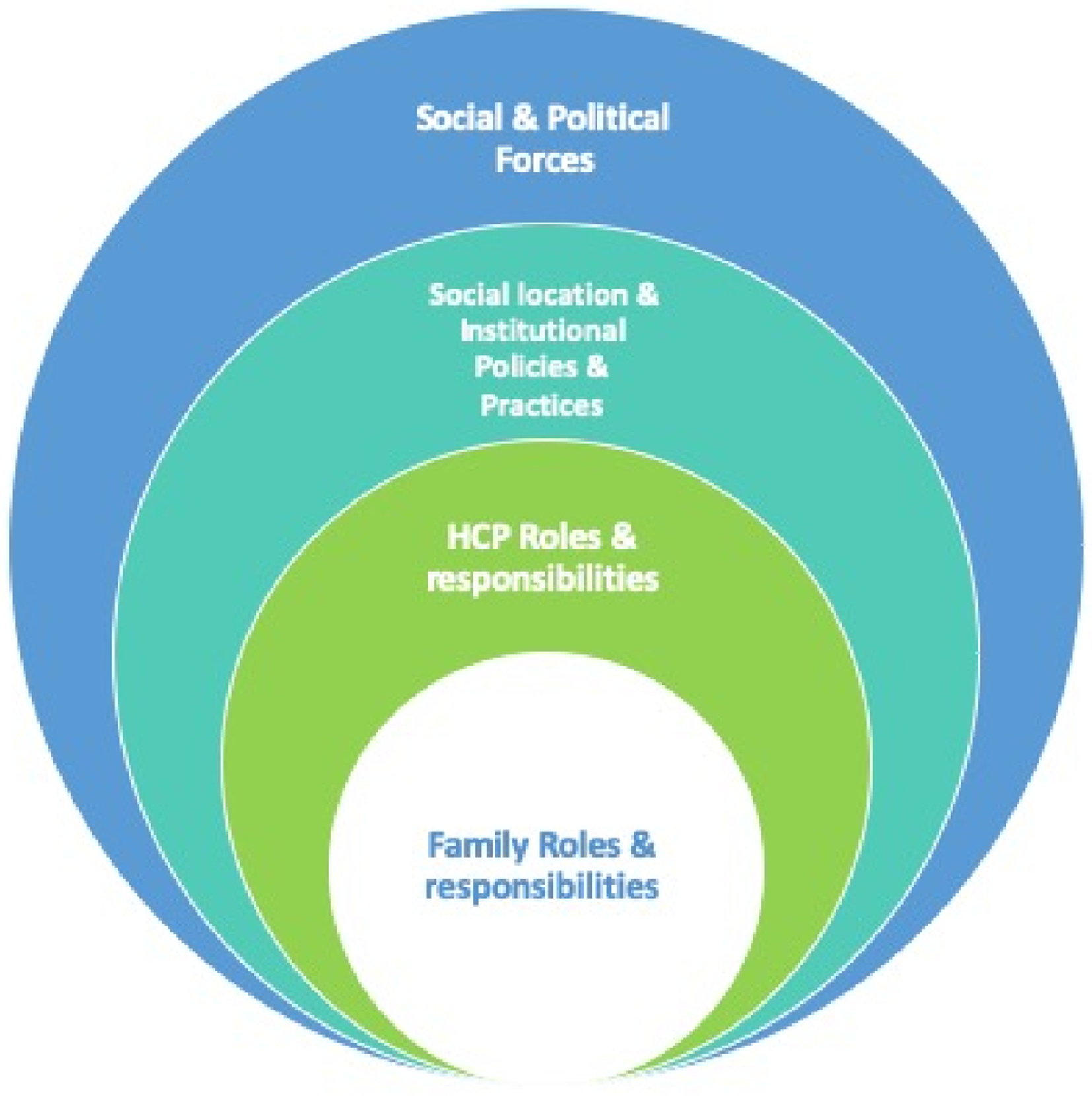
Discussion
Overall, patients’ experience of autonomy was incongruent with the dominant individualistic approach that is used currently to structure ACP interventions and instead was a relational experience. The results suggest that there are diverse ways of understanding ACP in advanced HF, yet there is little connection between the traditional individual model of autonomy and the realities of decision-making experienced by participants. ACP is included in the current practice standards for cardiovascular care and is recommended as something that should occur early and often in the HF disease trajectory (Allen et al., 2012; Ezekowitz et al., 2017). However, a key finding in this study was that the majority of participants did not view ACP the way that it is defined in the literature, as a process of “identifying values, reflecting upon the meanings and consequences of serious illness scenarios, defining goals and preferences for future medical treatment and care, and discussing these with family and health-care providers” (J. A. C. Rietjens et al., 2017, p. 543). Rather, both provider and patient participants associated ACP with end-of-life and death, and accordingly understood ACP as the personal, legal, and financial decisions that surround the end-of-life process. Although ACP is outlined in theory and in research as an attempt to overlap the biomedical and legal spheres of decision-making and bring personal preferences, values, and goals into treatment decision-making, in clinical practice, ACP was often reduced to decisions regarding resuscitation. This meant that participants (patients, family members, and healthcare providers) focused specifically on determination of resuscitation status as well as financial and social end-of-life concerns, such as will preparation and burial arrangements. These decisions were unrelated to HF management or day-to-day clinical decision-making regarding current or future care. These findings highlight the ways people exercise autonomy in the context of HF decision-making and demonstrate which aspects are understood to be under personal control, such as financial affairs and social arrangements, compared to aspects that are under medical control, such as treatment decision-making.
Diminished personal agency in decision-making may lead to discrepant understandings between patients and HCPs of what constitutes ACP and how autonomy is enacted within the clinical setting. The legalistic perspective of ACP involves identifying patient preferences or previously expressed wishes, which leads practitioners to understand ACP as patients’ ability to identify specific types of life-sustaining treatment they would consent to receive (or not consent to receive) in advance, which is then often reduced to merely a “yes/no” determination of resuscitation status. Schwarze and colleagues described the way clinicians attempt to elicit this type of information about patient preferences to recommend treatments by asking the substitute decision maker: “What would they [the patient] want?” (Schwarze et al., 2016). Our findings reflect this phenomenon, where HCPs understood ACP to focus on determining the types of medical interventions patients would “want” (such as surgeries, new medications, or deactivation of cardiac devices) if they were to become unable to speak for themselves.
However, our findings highlight that this construction of ACP as a process of extracting wishes and preferences from patients in advance of deterioration does not resonate with patients’ experiences. Decontextualized preferences and goals rarely aligned with the actual goals and values held by patients; patients rarely (if ever) framed their preferences around specific treatments or interventions they would accept or would not accept. Rather, they focused on their personal and social values, which often revolved around the basic desire to continue to live to support their family members. Previous research aligns with this finding by outlining that attempts to extract patient preferences tend to encourage a focus on various medical strategies, as opposed to a discussion of the value of different outcomes, such as length and quality of life, which would help patients plan for the future (Schwarze et al., 2016). Consequently, Schwarze and other authors recommend moving away from framing decision-making in relation to patient preferences because it encourages the patient and family to reflect on specific treatments, such as life support or comfort care, rather than the goals or outcomes of these treatments (Schwarze et al., 2016).
In the case of ACP in the context of HF patients, it seemed impossible to be informed of and understand all the potential treatments that could be offered (Schwarze et al., 2016; Shapiro, 2015; Sudore & Fried, 2010), which is a major flaw in the current paradigm of ACP. In response to this challenge, researchers recommend shifting toward a model that best prepares the patient and SDM to work with HCPs to make decisions in a shared decision-making model (Lin & Fagerlin, 2014). However these recommendations still center on an individualistic model which encourages patients to “communicate their values and needs” in advance (Sudore & Fried, 2010, p. 259) while the findings of this study suggest that this is likely insufficient, as this individualistic model may still be incongruent with the experience of autonomy in chronic illness (Schwarze et al., 2016; Shapiro, 2015).
We also found that agency is constrained in advanced HF, and patient and family experiences did not align with the traditional model of individual autonomy. Participants recognized the impossibility of being completely informed given the complexity of HF and choices were limited (or non-existent) as decision-making was guided by clinical guidelines, protocols, and candidacy requirements, with little to no room for patient preferences or values to factor into the process. Assessment of therapeutic candidacy is a ubiquitous aspect of the HF care journey (Lala & Mentz, 2022); patients are continually assessed and determined to be candidates (or not) for various interventions such as cardiac transplantation (Peled et al., 2024), cardiac surgeries (McCarthy et al., 2023), device implantations, and more. Recent research has characterized this constant assessment and re-assessment of candidacy as “negotiating a vicious cycle of heart failure care” (Higginbotham et al., 2021, p. 3148). Further research may consider integrating frameworks such as the Candidacy Framework (Koehn et al., 2024) to better explore the experience of navigating candidacy from the perspective of healthcare access.
Beyond the process of candidacy, patients expressing that they had “no choice” but to pursue biomedical treatment is not limited to this study; indeed, researchers that have examined the experience of patients receiving cardiac devices such as implantable cardioverter-defibrillators and left ventricular assist devices have also found very similar results (Fowler et al., 2018; McIlvennan et al., 2014). In similar research regarding the decision-making process of patients with advanced HF who were offered a ventricular assist device, patients often felt they “had no choice” (p. 8) in the decision (Dillworth et al., 2019; Kitko et al., 2016; Ottenberg et al., 2014). Agency is constrained when patients construct consent to treatment as their only choice, as is the case in advanced HF. Researchers report that patients generally understand medical decision-making to be an emotional process of coming to terms with the recommended plan of care, often requiring intensive support from family members or a spiritual community, and that for some, “the desire to live supersedes reflective processing” that should accompany an autonomous decision (McIlvennan et al., 2014, p. 374). Considering that reflective endorsement of authentic desires is a requirement of autonomy (Mackenzie, 2008), it becomes clear how chronically ill patients may not always be able to fulfill the conditions required to exercise individual autonomy the way it is currently constructed. Although ACP is branded as a means to understand patient desires and support voluntary choice and autonomous decision-making, when treatment decisions are consistently framed as life-or-death decisions to the patient and family, a continuous cycle of accepting treatment can occur (Higginbotham et al., 2021).
Overall, clinicians and researchers are beginning to understand the limitations of using individual accounts of autonomy as the foundation for critical healthcare practices such as ACP. Recent debate in the palliative care context has begun to shed light on the numerous complex steps required to align in order to successfully engage in ACP and meaningfully impact patient outcomes (Morrison et al., 2021). Multiple studies in the HF population have demonstrated that current approaches to ACP are not producing improvements in relevant outcomes (Malhotra et al., 2020; Nishikawa et al., 2020) Additionally, relational approaches to ACP have been suggested in recent research, specifically in the context of dementia (Phenwan et al., 2024; Van Rickstal et al., 2022). From a policy perspective, the Pan-Canadian framework on ACP (Advance Care Planning in Canada (SpeakUp), 2020) shifted from using an individualized to a relational understanding of autonomy, but more research is needed to determine how this can be fully implemented within the Canadian healthcare setting and beyond.
Limitations
A limitation of this study was that it was conducted at two sites within one large city; the first site was a specialized cardiac care center, and the second a smaller, academic urban hospital, both within the publicly funded Canadian healthcare system. Because of the location and proximity to specialized cardiovascular care, the possibilities for patients to obtain a variety of treatment options were potentially greater than in a smaller institution in a rural area, and much greater than the options available in a lower-income country, which may limit the transferability of results to other countries or settings. Healthcare institutions with limited budgets may not be able to offer patients the types of therapies that characterized the HF trajectories in this study, such as access to cardiac transplantation, new and expensive technologies and therapies, and specialized interdisciplinary HF care teams.
Another important limitation of this study was that the participants did not represent a wider range of social locations, despite efforts to recruit a broader sample. The sample was heterogeneous in terms of demographic criteria such as gender, ethnicity, diagnosis, and experience of HF, as well as HF treatment trajectories. However, overall, participants had supportive social networks, were relatively health literate, and were able to advocate for themselves in English. With the exception of Peter (Case 3), who described the personal consequences of having advanced HF by having to move homes to be closer to family and to treatment, participants appeared to be relatively stable socially and financially. Moreover, several participants seemed to have a relatively high socio-economic status based on field observations during interviews which took place in their homes. Future work could expand on this topic by focusing specifically on groups such as newcomer or immigrant populations, non-English-speaking HF patients and families, or families in more rural and remote locations.
Conclusion
In conclusion, this study challenged the current conceptualization of ACP as a healthcare practice grounded in individual autonomy. By using a new approach to studying ACP based on relational autonomy, we developed an understanding of the complex intersecting web of relationships and forces that shape people’s ability to participate in ACP. Further empirical work is required to explore how this relational approach can improve the experience of ACP for patients with a diverse range of chronic illnesses, and beyond ACP, how this approach could improve health decision-making in a broader context throughout the illness trajectory.
Footnotes
Acknowledgments
We would like to thank the staff of the Heart Function clinics at Toronto General Hospital and Sinai Health for their support in this research.
Ethical Statement
This study was approved by the Research Ethics Boards at both University Health Network (#17-6162) and Sinai Health Systems (#18-0063-E), and all participants provided written informed consent.
Author Contributions
Conceptualization: Tieghan Killackey, Elizabeth Peter, Jane Maciver, and Shan Mohammed. Methodology: Tieghan Killackey, Elizabeth Peter, Jane Maciver, and Shan Mohammed. Formal Analysis: Tieghan Killackey, Elizabeth Peter, Jane Maciver, and Shan Mohammed. Writing—original draft preparation: Tieghan Killackey, Elizabeth Peter, Jane Maciver, and Shan Mohammed. Writing—review and editing: Tieghan Killackey, Elizabeth Peter, Jane Maciver, and Shan Mohammed. Supervision: Elizabeth Peter.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by scholarships from the Ted Rogers Centre for Heart Research, the Peter Munk Research Scholar Award, and the Ontario Graduate Scholarship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.