
Abstract
While men’s mental health help-seeking has received increased clinical and research attention, little information exists regarding men’s perspectives and experiences of peer support and mutual help for mental health challenges. Drawing on qualitative photovoice interviews with 65 men living in Canada (M = 37; SD = 15.5 years), thematic analyses were conducted to explore the gendered barriers to men’s mental health peer support. Two inductively derived themes were identified. Dual paradoxes fuelling men’s silence revealed a complex interplay of tensions and alignments with traditional masculine norms, often leading to concealment and therefore inaction. Men struggled to reach out to male peers, despite their willingness to help others and broader societal encouragement to seek help. Relational masculine norms driving misaligned support revealed risks and vulnerabilities for men seeking peer support, with concerns about asking for too much or over-disclosing when opportunities arose. Men’s requests for support were often implicit or vaguely defined, which contributed to their unmet support needs, despite well-intentioned efforts from peers. When men did receive support, it was often conditional and contextually bound within acceptable masculine milieus. Findings highlight how men’s intentions and actions toward mental health peer support can be constrained by perceived normative masculine identities and relations. To reify the potential of men’s peer support, gendered barriers must be thoughtfully considered and addressed to promote men’s mental health and informal help-seeking.
Introduction
Globally, male suicide rates are more than twice that of females (World Health Organization, 2021), and in Canada, 75% of suicides are men (Statistics Canada, 2023). Complicating matters is that many male suicide decedents are not known to have mental health conditions (Fowler et al., 2022), with only 10% of men >12 years old seeking professional help for their emotional and mental well-being (Statistics Canada, 2020). These results underscore the prevalence of undiagnosed mental health challenges in men and the complexities for seeking mental health care. Research has revealed a series of barriers to men’s mental health help-seeking with an emphasis on the role of masculinities (Seidler et al., 2016). The assertion has long been that men’s alignments to traditional masculinity, characterized by strength, self-resilience, and emotional stoicism reduce and impede help-seeking for mental health challenges (Chatmon, 2020; Tang et al., 2014). Men’s reticence for seeking professional help is exacerbated by barriers including lack of familiarity and compatibility with care providers, fear of judgment, and pressure to divulge ordinarily private information as the entry point to treatment (Seidler et al., 2020). In light of the complexities of men seeking and sustainably engaging professional mental health services, alternative informal help resources have emerged. Foremost among these is men’s peer support (Sharp et al., 2024), whereby mental health is idealized as adeptly promoted with the company of other men (e.g., sharing and troubleshooting personal challenges). Despite a broader societal understanding of and advocacy for mental health promotion, considerable barriers persist to restrict men’s informal peer supports. Herein, we examine complex structure and agency interplays to report men’s barriers for engaging mental health peer support.
Men, Masculinities, and Mental Health Peer Support
There is growing interest in peer support as a viable avenue for promoting men’s mental health (Cyr et al., 2010). For example, programs including BuddyUp have built communities of practice by raising awareness and norming conversations around men’s mental health challenges (Sharp et al., 2023). Movember, a global charity, is known for its annual fundraising campaign engaging men to grow moustaches and have conversations to raise awareness and funds for men’s suicide prevention (Movember, 2023). While BuddyUp and Movember are part of a growing suite of community-based efforts to socially connect men and advance their collective mental health, the everyday practices of men accessing mental health peer support are poorly understood. Peer support acknowledges the importance of interpersonal connections in mental health and provides a platform for open discussions (Darby, 2018), potentially reducing the stigma associated with seeking help. There is evidence that peer support aids men in navigating mental health challenges, foremost improving depressive symptoms (Pfeiffer et al., 2011; Sharp et al., 2023). Herein, peer support has emerged as a valuable source of assistance, providing accessible and practical information exchange to foster belonging and facilitate mutually beneficial direction for individuals seeking help (Mead et al., 2001). Originating in organizations such as Alcoholics Anonymous and other peer-run recovery services, peer support has grown in popularity in recent years offering various forms of support and assistance (Gagne et al., 2018). Common to these predominately community-based offerings has been men sharing their experiences with the goal of providing understanding, support networks, and mutual aid (Tracy & Wallace, 2016). With a growing number of interventions and programs (Shalaby & Agyapong, 2020), there exist significant opportunities to harness these health promotion initiatives for the purpose of encouraging and coaching men to actively participate in mutual help.
Research indicates that men tend to seek emotional support from individuals with whom they share familiarity, emotional closeness, trust, and confidence in receiving assistance (Burke et al., 2022). Support interventions may appeal to men when they have a clear purpose, are action-oriented, and provide practical strategies seamlessly integrated into daily life (Sagar-Ouriaghli et al., 2019). Notably, an environment fostering shared understanding seems highly appealing to some men in seeking support (Galdas et al., 2015). The exchange of personal experiences within these contexts serves to normalize men’s individual experiences and facilitate their exploration of diverse ways to construct personal and relational narratives (Vickery, 2022). In these supportive environments, men can redefine help-seeking within the framework of normative masculinities as strength-based, requiring attributes like courage, action, and resolve. Moreover, such reframing positions help-seeking as masculine capital, exemplified by the sharing of vulnerabilities to affirm and aid others (Gough & Novikova, 2020). Nonetheless, mental health stigma continues to be a significant barrier for men seeking help, potentially influencing their participation in mental health and peer-related initiatives (Burke et al., 2022).
Despite extensive research exploring and evaluating peer support across various contexts (Penney, 2018), little information exists regarding men’s barriers to peer help-seeking. Additionally, there is limited knowledge concerning the gendered challenges for engaging mental health support. Understanding men’s complex help-seeking patterns is essential to informing mental health promotion and suicide prevention strategies (Oliffe et al., 2021).
Methods
Study Recruitment and Procedures
Following university ethics approval (H23-00301), English-speaking men (18+ years) living in Canada were recruited to participate in a virtual photovoice study regarding men’s perspectives and experiences of peer support and mutual help for mental health challenges. Canada-wide recruitment was conducted predominantly through social media as well as e-flyers distributed by individuals and organizations for circulation via their respective communication channels (e.g., newsletters and mailing lists). Potential participants contacted the project manager via email and were invited to attend a brief eligibility/intake Zoom meeting to receive additional study details including the research objective and procedures. Eligible participants were asked to complete a Qualtrics consent and demographics questionnaire, and take 5–10 photographs that depicted their perspectives and experiences of social connection and mutual help for mental health challenges, ahead of undertaking an individual Zoom interview. In line with best practices in photovoice ethics (Creighton et al., 2018), all interviewers were trained and experienced in conducting topic-sensitive qualitative research and attentive to signs of participant distress. At the end of each interview, participants were reminded of support resources, including national crisis lines and mental health services. Additionally, a follow-up email containing these resources was sent to all participants. Each participant received a $100 e-gift card to acknowledge their time and contribution to the study. The amount was chosen to fairly recognize the time commitment of participating in the study (i.e., attending intake meeting and semi-structured interview, completing demographics survey, and taking and submitting photographs).
Study Participants and Data Collection
Participant Demographic Characteristics.
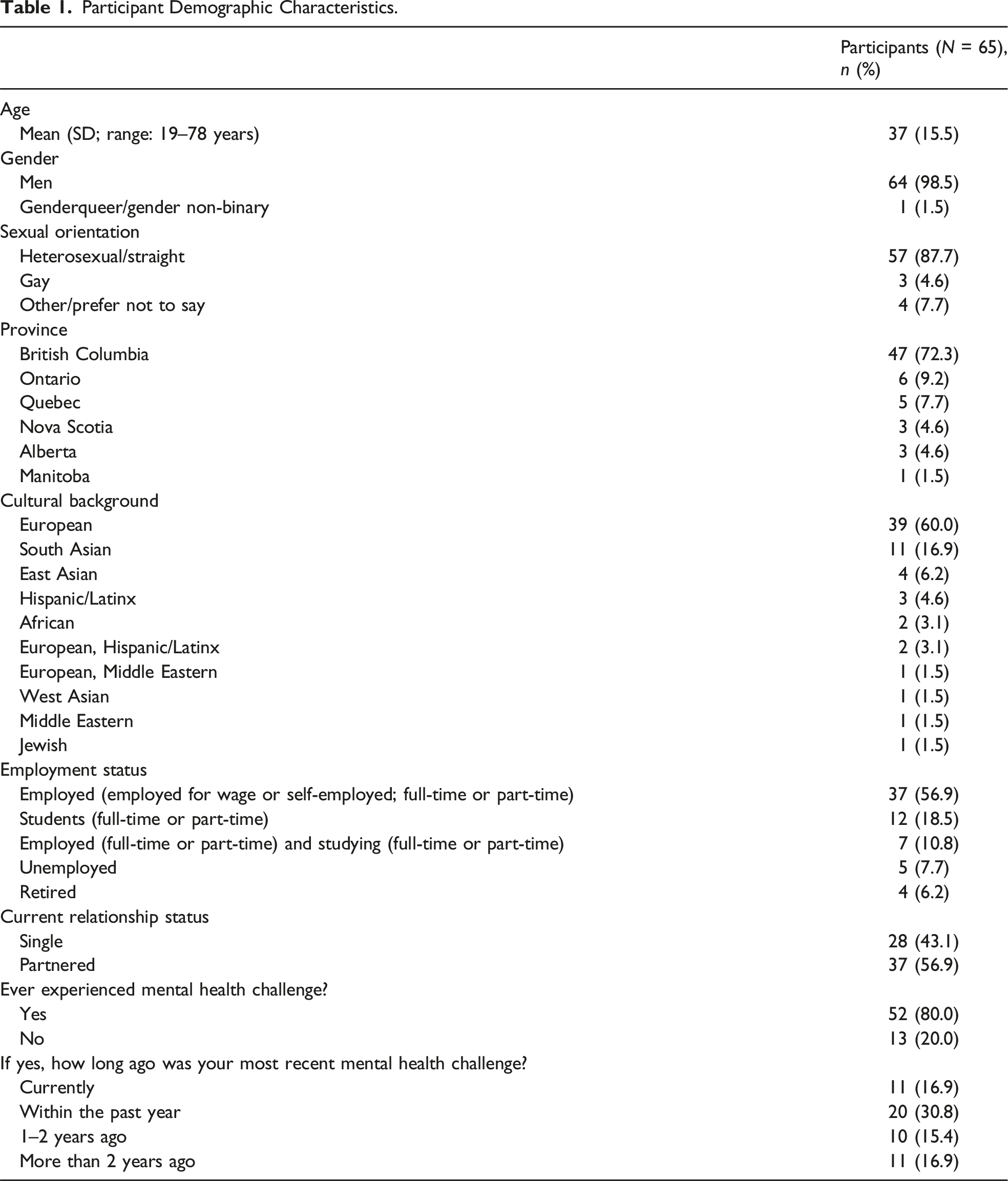
Strategic social media recruitment and e-efficiencies for conducting virtual photovoice interviews (Oliffe et al., 2023) helped us work with participants from six provinces across Canada. Individual Zoom photovoice interviews were conducted by four Canadian-based researchers (three men and one woman) from June to October 2023, and the interviews ranged from 35 to 262 minutes (M = 76 minutes, SD = 32.2 minutes). Prior to the interview, participants titled and submitted their photographs via Qualtrics. Each photograph was discussed during the interview, and participants were asked to describe the image and explain its meaning, leveraging the visual prompts to elicit in-depth narratives and reflections. Semi-structured interview questions were used to guide the conversation including “What would prevent you from seeking peer support?” and “Tell me about a time when you reached out or sought help from other men when dealing with a challenge in your life?” The Zoom interviews were audio-visually recorded and transcribed verbatim. Participant photographs were inserted to their accuracy-checked anonymized interview transcripts and imported to NVivo 12 for coding. A written summary highlighting key insights from each interview was completed for all participants to aid the organization and preview of the data. While the overarching aim of this research was to explore men’s perspectives and experiences of peer support and mutual help for mental health challenges, the current analysis focused on identifying and interpreting the barriers to peer support that emerged as shaped by gendered norms and expectations. The analytical focus on gender was formalized as a primary research question in the research proposal and operationalized to guide the analytics and analyses of the photovoice data collected.
Data Analysis
We adopted a reflexive thematic analysis approach as described by Braun and Clarke (2022), grounded in a constructivist epistemology that understands masculinities as relational, context-dependent, and socially constructed (Connell, 2005). This approach centers the researchers’ active role in generating themes through interpretation, rather than treating themes as emerging passively from the data. In the initial analytic phase, two researchers independently read and re-read the first 20 interviews. This subset was pragmatically selected due to the large size of the qualitative dataset, an approach aligned with past photovoice research involving sizeable samples (Oliffe et al., 2024b). The rich photovoice data were used to inductively derive preliminary codes and tentative themes. Two inductively derived themes, (1) dual paradoxes fuelling men’s silence and (2) relational norms driving misaligned support, were refined and further developed through abductive analyses (Timmermans & Tavory, 2022), wherein the remaining 45 participant interviews were closely reviewed and coded to identify consistencies, divergences, and gendered patterns. Connell’s (2005) masculinities framework was then applied to theorize and conceptually advance gendered understandings within the findings and delineate how participants aligned with and resisted masculine norms. This process ensured the analyses remained grounded in the data amid applying theory to build gendered explanations to the findings. In line with reflexive thematic analysis, we did not seek data saturation as a marker of analytic completeness. Instead, we aimed to produce a rich and nuanced account of meaning patterns in the dataset, guided by the evolving interpretive process and theoretical lens (Braun & and Clarke, 2021; Clarke et al., 2024). Reflexivity was embedded throughout the analytic process to enhance the credibility and depth of interpretation. Team members regularly met to reflect on how their positionalities, disciplinary perspectives, and assumptions about gender and mental health influenced the coding and theme development (Braun & Clarke, 2021).
Results
The findings are presented through two overarching themes, each supported by representative participant quotes and photographs. These individual accounts were selected as illustrative examples that reflect patterns across the dataset and ground the findings in men’s lived experiences while representing broader social and gendered dynamics shaping men’s peer support practices.
Theme 1: Dual Paradoxes Fuelling Men’s Silence
Evident in men’s narratives were two entwined paradoxes that compounded and contextualized their reticence for seeking peer support. These paradoxes reflect a tension between men’s intentions and actions, shaped by traditional masculine norms and relational dynamics.
Ready to Offer Help, Reluctant to Seek Help
The first paradox comprised self-contradictory statements wherein the intricate dynamics and high endorsement of giving peer support sharply contrasted participants’ reluctance for seeking the help of peers themselves. Max, a 20-year-old man, suggested this was normative, suggesting men are “way more open to help someone else than to get help for [themselves].” Aligning to masculine ideals for providing and protecting, many men spoke to their readiness and ability to help peers. Lucas, a 37-year-old man, elaborated: When someone opens up to me, I’m actually quite comfortable with it. I don’t mind talking to someone and hearing what they’re going through and offering a bit of reflection or just an ear to listen.
Contrasting this ease, Lucas shared his discomfort and feelings of “vulnerability” and “embarrassment” when asking for help, positioning this paradox as learnt and deeply engrained: “from the generations of being brought up thinking that you just have to deal with it yourself, pull yourself up by your own bootstraps.” Here, despite the gendered reasonings for help-giving and the self-referential reticence for being helped, their co-existence and double standard was logically unacceptable. This paradox was, however, commonplace and often explained away as men’s alignments to masculine norms for providing (i.e., protector) but not needing help (i.e., self-reliance) from peers themselves.
These contradictory positions were somewhat reconciled with men responding to self-pressures to uphold masculine norms in denying their need for help, thus bypassing the marginalizing risks for transgressing manly self-reliance scripts. Liam, a 28-year-old man, explained these norms as socially constructed and persuasive: We’re used to this image of, oh, guys are sort of rocks, right? And, you know, they’re supposed to be the rocks that people lean on. Once they crack, it can be like, you’re not really fulfilling your gender role, in a way. Like, you are not really being a man, I guess.
The duality of being strong and self-assured for others prevailed as the time-honored masculine script to which Liam and many participants narrated themselves as complicit. The net effect was men’s self-management of life transitions through concealments of mental health challenges that accompanied their shifts. Jayce, a 53-year-old man, critiqued the senselessness of this, highlighting the futility of buying into these unachievable and inauthentic masculine norms: In things like sports, jobs, relationships, we’ve got an expectation to perform, to be the best … and at the end of the day, we may not be happy with that, and we might find ourselves sitting back and thinking, “How do I step away from all that, when I’ve created this perfection—or tried to create it—and it’s a façade, it’s a mask.”
Normed masculine competitiveness, combined with carefully curated public images of success over social media, isolated many men in their struggles, concealing their challenges and rendering moot the reaching out to peers for help. Being seen as less than or weak within masculine hierarchies drove these defenses in ways that were often positioned as requisite to giving peer help. That is, men’s displays of self-reliance served as assurance and evidence that they were legitimate candidates to support other men. Jayce later qualified that giving into peer help was reserved for and indicative of crisis and being rock bottom when self-resiliencies were replete: I don’t want to end up sleeping on other people’s couches and sleeping in their guest rooms to try and get back on my feet … Do I want to call a friend? No, I should be going to the gym instead.
Here, Jayce questioned whether to ask for support, weighing his need for help against the fear of appearing vulnerable or powerless in the face of his challenges. Ultimately electing self-management through exercise, Jayce took the well-worn masculine path for independently and physically working through his mental health challenges.
Relatedly, not wanting to burden peers diminished the potential for men calling in a favor for help from male friends. Again, needing help was synonymous with debility, and these relational discomforts were often linked to the nature and limits of specific friendships. Jack, a 23-year-old man, explained, “unless it’s one of your very close friends … you may be nervous yourself, ‘am I overextending my boundary as a friend, is this too far.’” Emphasizing these uncertainties in contemplating who he could reach out to, Jack suggested trust and deep connection determined the feasibility for asking another man for help. Interestingly, Jack did not employ these criteria in suggesting he would provide peer support to anyone who needed it.
These relational paradoxes were also lifted into broader social norms and discourses, where some temporal shifts were espoused as slowly growing to offer easements for exchange and mutuality in men’s help-giving and taking. Kevin, a 22-year-old man, submitted Photograph 1 titled Fragmented and commented on emerging changes in societal attitudes toward men’s help-seeking: I titled it, fragmented. Just because there’s so many branches coming off. I really thought, the broken branches near the bottom represented current societal attitudes towards men’s peer support. It dug into the ground, broken. And a few branches that are still growing up are a changing of attitudes, in terms of, progression. Fragmented.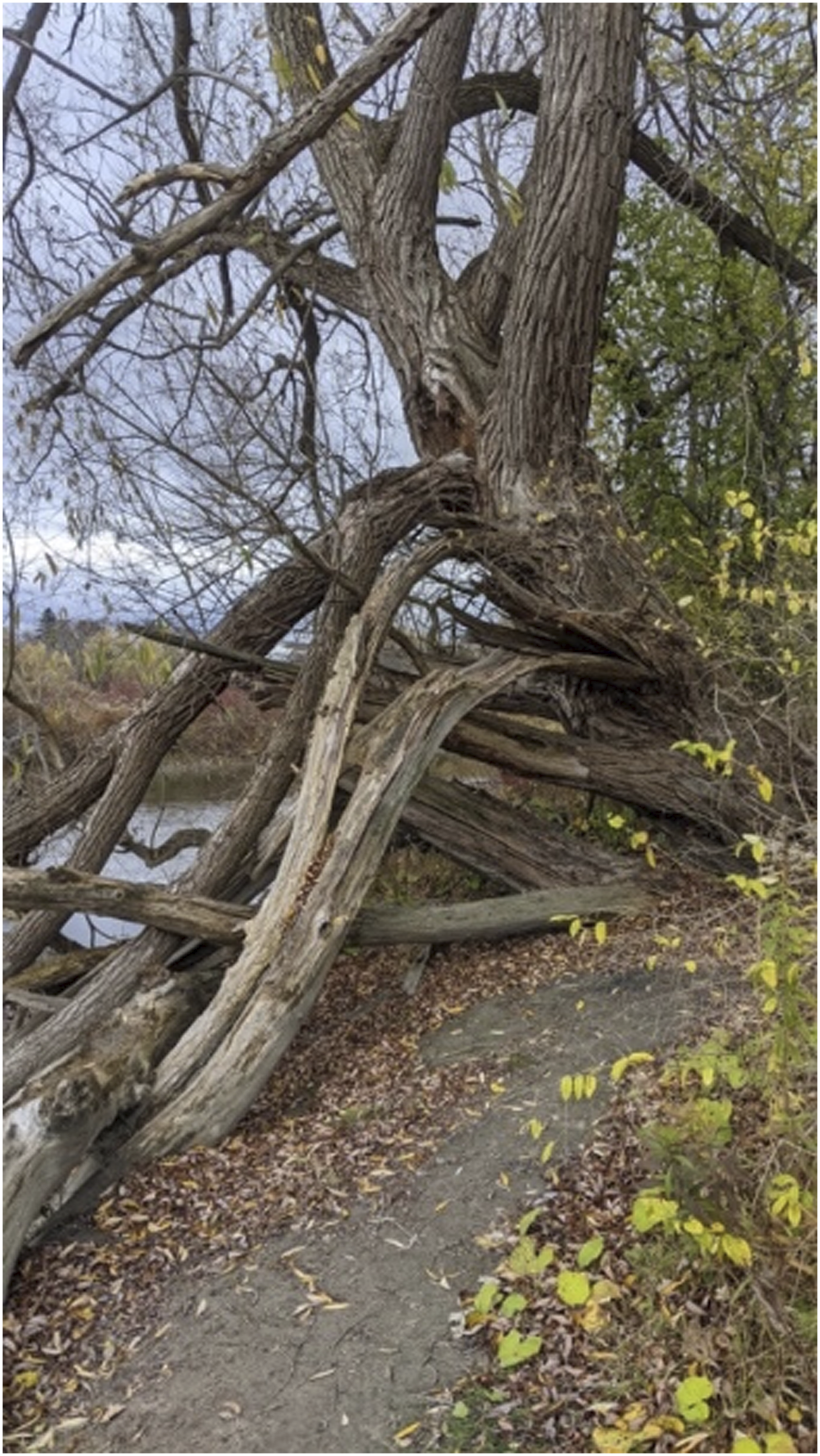
Speaking to the pull of traditional masculinity, Kevin metaphorically pointed to the deep-rooted structures characterizing sturdy oak men as saying and needing less. Also claimed were some visibilities of men’s contemporary masculine offshoots for openly and authentically speaking with one another. Symbolically, traditional masculinity was depicted as an anchor and undertow, albeit amid some northbound reaches visibly pulling against those limits. There is evidence of a struggle here with the trunks and branches twisted directionally—a tension reflected in Kevin’s uncertainty for the new masculinities he craved.
Permitted to Open Up, Unequipped to Disclose
These structure and agency tussles were perhaps even more evident in the second paradox, which contrasted the growing public awareness of and de-stigmatizing work for promoting mental health by authentically speaking up about those challenges with men’s reticence to self-disclose specificities about what they were feeling. Ryan, a 25-year-old man, elaborated on the lag and discord between what could be discursively said and relationally done: Even if we’re in an era where most, but not all folks our age are open to, and even actively saying that, we should be talking about our feelings, that still doesn’t represent all of society, including parents, siblings, co-workers, there’s still remnants and feeling that you shouldn’t be soft.
Here, expressing what was felt was troubled relationally with the paradox of being socially affirmed to speak up, but without the resources for doing that. Ryan and many men spoke to their silences as relationally policed outside male peers amid the public discourse for them to be more emotionally expressive. Building on this point, James, a 31-year-old man, spoke about using alcohol to break with the non-disclosure rules for mental health when talking with other men: So, I think even though it’s [mental health] been much more destigmatized … at the same time, it’s just not comfortable, I guess. I’m much more open with alcohol. I probably should’ve started drinking before this interview.
Countering his wry quip, James went on to concede that “drink[ing] to have a chat when your mind is less clear is counterintuitive.” Noting the entrapped self-stigma for disclosing his own mental health challenges, and the shortfalls for using alcohol to ease that, James took some solace in those efforts. The silences arrested, James’ uncertainties were indeed momentarily remedied only to be amplified later in the aftermath of his alcohol use and its empty promise of agential liberation. This offers some context to men’s widespread use of substances to self-medicate, wherein it can facilitate mental health help-seeking with peers—even though the risks and redactions thereafter are heavily set.
For some men, the reluctance to open up to peers about mental health challenges underscored their lack of mental health literacy. Louis, a 20-year-old man, explained: Mental health probably popped up more prominently in the last three, four years. When I was in high school, it was not something guys talked about. So, if you brought it up, nobody knew what would happen … we didn’t understand how big of a problem that was.
The generalizing of mental health and the lack of specificities for how to recognize or support the challenges limited Louis’s efforts for disclosing his own struggles. Spencer, a 32-year-old man, submitted Photograph 2 titled Sunset shared with friends as we reflected, which spoke to the disconnects between men knowing mental health was important but lacking the ability for securing that with their male friends: I think a lot of the time it’s going to be just trying to process everything in your own head, knowing that you’re not really going to be that great communicating it, getting it, because you don’t really fully understand it yourself … managing the awkwardness of that conversation from the very beginning of having to try and overcome that, it just becomes a bit overwhelming to even begin to have that conversation. Sunset shared with friends as we reflected.
Contrasting the tranquil and idyllic Vancouver sunset, Spencer spoke to being in the company of men but without the cadence to start the conversation he needed. The awkwardness for incoherently stumbling through a struggle narrative that he himself did not fully understand left Spencer silent. The sunset came and went, as did the moment to deeply connect and share what he was really feeling. Interestingly, Spencer claimed that he did not expect anything different, but in the interview, it was clear that he needed and wanted more than the ascetics of and superficial banter around their shared sunset.
In summary, the dual paradoxes fuelling men’s silence reveal a complex interplay of tensions and alignments to prevailing restrictive traditional masculine norms with the net effect of men struggling to reach out to male peers amid their willingness to help others. While many men also bought into contemporary changes for seeking peer support, their concealments and inactions for reaching out and opening up revealed a lack of knowing how to connect and the strong potential for being isolated in and by their mental health challenges while in the company of other men.
Theme 2: Relational Masculine Norms Driving Misaligned Support
Compounding men’s silences were relational masculine norms driving misaligned support wherein specific needs were vaguely shared and awkwardly unmet, with those miscues having long-lasting effects.
Implicit Help-Seeking and Conditional Care
Men’s efforts to seek support were often communicated implicitly, leading to unmet needs and relational disconnects. Even well-intentioned peers frequently missed or minimized these subtle cues, reinforcing norms of stoicism and emotional self-reliance. Joshua, a 51-year-old man, discussed a text conversation he had with a close friend where he disclosed his recent intimate partner relationship breakup: This friend of mine is a very kind-hearted man. He’s a very gentle soul, and he takes care of the other female friends. I have to own my part, I did not explicitly say, “I’d like to talk to you about it.” I felt awkward asking for this. So I sent him this long message hoping that he would offer, “hey, do you want to meet, or do you want to talk about it or even call me?” And I was surprised by the answer he gave me which is, “Sorry to hear that. Too bad when things don’t end up well, big hug my friend.” And that was it. He never called to check on me, he never wondered after a few days, “Are you doing okay?” This is a two-and a half year relationship that just ended. And I was really surprised and part of me said like “maybe you should ask for more,” then part of me says well, “he should know.”
Joshua’s disappointment for failing to connect was evident, especially having carefully selected a friend he believed to be compassionate and caring. Joshua’s friend’s gendered approach to supporting friends was also made apparent wherein it seemed he was more attuned to supporting female friends but missed the implicit (perhaps subtler, less normed masculine) calls from male friends. While Joshua’s friend was sympathetic to the situation, the shortfall of support left Joshua pondering his own text, and lack of directness in not explicitly asking for help. Likely at play was the norming of men’s emotion resiliencies, intimate partner relationship breakups, and the need to privately work through the many life transitions when partnerships end. Clearly disappointed, Joshua nonetheless fell in line with what he was being implicitly asked to do—move on from the pain by self-managing (rather than talking about) it. Like Joshua, many participants, while knowing they needed help, found themselves shutdown, wishfully waiting for permissions that never materialized and help that never came. The support men did receive was often pragmatic and operational, wherein peers would provide outcome-oriented assistance within well-defined parameters. Such approaches to peer support were reliant on and guided by traditional masculine relations between men, the sum and parts of which were experienced by men as restrictive and limiting. Jayce, introduced earlier, described the support he received from his friends after separating from his partner: I went through a rough period, a breakup—and the solution with a bunch of my friends was … “We’re going to get Jayce and we’re going out to the bar. We’re going to get him back on the saddle. We’re going to introduce him to the next girl, and all of his problems are going to be solved.”
While Jayce’s friends were well-intentioned, their strategy focused on distracting and downplaying his emotional pain with alcohol and conquest, synonymous with masculine ideals. Jayce described this type of support as a “quick fix,” suggesting the counterproductive effects of not providing the space or safety to process all that happened in the relationship and the breakup: “Suddenly, those issues that you’re dealing with get pushed down and hid. It’s kind of you’re just ignoring it.” Like Jayce, many participants questioned the therapeutic value of this type of support and problematized it as driven by traditional masculine norms, which prize action over emotion—doing rather than thinking.
Other life transitions also featured wherein the support from other men was also focused on feeling less and downplaying the circumstances underpinning participants wanting help. Noah, a 40-year-old man, submitted Photograph 3 titled Only cuz you asked me 5 weeks in advance, describing his dismay for the lack of emotional support he received from his friend, as he navigated a potentially life-changing health scare: I went to the first treatment alone, but I asked a friend of mine to drive me there because they’re gonna dilate my eyes … And I said, “hey, thank you, man, I really appreciate that you drove me to the hospital today.” And he’s like, “no, don’t worry I can always be here for you, as long as you ask me in advance.” It was a very peculiar moment for me, because sometimes you don’t know you’re gonna need somebody. How can you ask in advance, right? Only cuz you asked 5 weeks in advance.
Noah began by qualifying his need for help as justifiable given his risk for going blind, and the anxiety he had about the impact of that possibility on his life and partner. As Noah sought a moment to share his fears, his friend’s response closed off that possibility by offering only conditional, practical help—limited to situations where advance notice was given. Sharing the image of his friend’s hands upon the wheel referencing his straight-ahead gaze on the road, Noah was taken aback and silenced. Compounding fears about the impending treatment[s] and uncertain future were left unsaid, with rational and practical assurances that his friend would help out by driving him to the hospital if he could. In fairness, the friend may have been downplaying his help to reduce the potential for Noah feeling indebted. However, a heaviness ensued in their shoulder-to-shoulder silence for the commute home, leading Noah to whimsically remark, “I wanted somebody that made me feel safe, with compassion, without making me feel like less strong or less worthy.”
The examples above highlighted the relational, co-constructed nature of men’s peer support experiences wherein the unvoiced implicit asks for emotional support are missed or intentionally avoided in ways that could potentially heighten the mental health challenges of some participants. Jayce, introduced earlier, similarly noted an implicit temporal expectation of progress lightening mental health challenges, and thus paving the way for problem-free, fun-orientated get-togethers: There’s an expectation that everything always moves forward. “Come on, it’s been a couple of weeks or whatever. You’re not passed that? I thought we talked about this already. You’re still not through it yet? Come on, man.”
Evident were mismatched expectations that men’s mental health challenges were time-bound and likely situational in their progress toward a resolution.
Over-Disclosing as a Trustfall Fail
Men often perceived an unspoken threshold in emotional disclosure, whereby sharing too much risked overwhelming the listener, resulting in silence, discomfort, or shame. Throughout men’s narratives, there was an ever-present risk to men who “overdid it” by belaboring their problems or sharing too much emotion about their struggles. Lucas, a 37-year-old man, submitted Photograph 4 titled The feels, describing his ruminations and doubt after sensing he had over-disclosed to a friend: So, I took it [the photograph] thinking about after you have those conversations, how do you feel? It’s kind of embarrassed. It’s like, you want to hide for a second. Again, it’s that vulnerability thing. It’s, you’re vulnerable in the moment, and if the moment’s passed, you’re like, “Oh, was that too much? Did I say too much? What are they going to think? What are they going to say next time?” and you just want to hide for a second. The feels.
Hiding from himself, as well as veiling from the potential judgments of others, Lucas physically and emotionally recoiled from being “exposed.” The safety or affirmations in those disclosure moments with peers were gone, and Lucas’s fear of judgment and self-doubt took hold, exacerbating his worry about burdening others as well as concerns for damaging his masculine identity by over-disclosing his challenges. Here, Lucas’s vulnerabilities were for what was said, and the depth of the feelings shared, rather than any concerns about explicitly asking for or receiving help. In essence, the concerns are about breaking the masculine code and following through on a departure from what men do and reasonably can disclose and talk about with each other.
The effects of men’s mismatched attempts to solicit support and potential over-disclosures recursively flowed to and from trustfall issues and being negatively seen. Louis, introduced earlier, bluntly stated, I don’t want people looking at me different. When I do tell people how I feel, like the times I have, they leave, so I don’t want people to leave.
Evident here was the confidentiality and off-the-record nature of men’s disclosures, and the muting effects that breaking that trust can have. Differentiated here also were the public nature of men’s social connectedness where lightness for doing rather than feeling contrasted the more private deep introspections and disclosures. Louis’ account indicated he had some transgressions wherein he misread opportunities about when and how to authentically show up among peers to talk about mental health challenges.
In summary, relational masculine norms driving misaligned support revealed the fragilities for men seeking and perhaps interpreting the support of other men. Seeking help was often implicit, with concerns about asking for too much and/or over-disclosing when those opportunities arrived. The support men did receive needed to be understood and accepted contextually within masculine milieus.
Discussion
While informal peer support has been suggested as a promising avenue to promote men’s mental health, the findings from the current study highlighted the gendered challenges for its uptake and effectiveness. In what follows, we situate the two thematic findings in the broader literature of masculinities, and men’s mental health and help-seeking, ahead of discussing the potential implications of this research for reducing the barriers to men’s engagement with peer support for promoting mental health.
The dual paradoxes featured in men’s peer relationship performativity highlight the bidirectional outcomes of aligning to traditional masculinities. So, while men’s willingness to provide peer support sharply contrasted their resistance to asking for help, these contradictions both clearly respond to masculine norms. At the fore were participants’ self-reliance and stoicism along with accommodations and protections for helping (rather than further marginalizing) men experiencing mental health challenges. While there was evidence of an easement in traditional masculinities, and more awareness and acceptance of men’s mental health disclosures, the idealized masculine-self was consistently portrayed as giving rather than taking help. As previously discussed by Gough et al. (2021), the discursive tensions between traditional masculine norms and contemporary discourses for men to be emotionally expressive challenge men’s engagement of mental health peer supports. The dual paradoxes illustrate how both social and self-stigma can contribute to men feeling burdensome, disempowered, or excluded—dynamics that reinforce traditional masculine norms and discourage help-seeking (Ogrodniczuk et al., 2023).
Sustained self-stigma, in particular, seems to challenge the optimism that men’s peer support might be the utopia for bypassing and/or connecting men to professional mental health care services. Absent, at least in the findings presented here, were the ideals for reciprocity and mutuality to overcome barriers to men’s help-seeking and stake claims for the emergence of new contemporary masculinities (see Sharp et al., 2024; Mansfield et al., 2003). The nuanced challenges reveal the limits of one-on-one peer support within established friendships, in line with the ideals of peer support being provided by someone who is an equal, has similar demographic and social backgrounds, and can share knowledge from experiencing similar challenges (Penney, 2018). These paradoxes reveal that men’s peer support experiences are shaped by complex and often contradictory dynamics. To ensure community-based peer support initiatives are effective, it is essential to consider and address these nuanced challenges.
Despite men clearly wanting to be there for their peers, the relational masculine norms driving misaligned support highlight an array of mismatches and discordances for what help is and how it is received. While men acknowledged masculine discourses legitimizing the expressions of what is felt on route to securing peer support, in line with previous findings from Migliaccio (2009), the gendered dimensions of male peer relationships characterized by shared activities rather that self-disclosures limit the depth of those connections. From a symbolic interactionist perspective (Carter & Fuller, 2016), understandings about the where, when, and how of men’s peer support for mental health are lagging behind the discourse and their collective willingness to help each other. Said another way, men’s expectations of, and cravings for, deeper social connections with other men rupture (even momentarily) the superficiality that characterizes many men’s friendships. Echoing findings from Sweeney et al. (2015), when confronted with uncomfortable mental health conversations, male help-givers, similarly challenged by the men’s relationality norms, tend to dismiss or disapprove help-seekers’ subtle requests for help. These mismatches might constitute the intentional avoidance of femininities stereotyped as ever-nurturing by some men, as well as men’s perceptions of being unprepared or unskilled to respond effectively to other men’s mental health disclosures. Men’s mental health stigmas also prevail to limit the expectations and disclosures in men’s peer supports, wherein safety and trust for self-disclosures are paramount. Similar patterns have been observed in men’s use of domestic spaces as both refuges and sites of despair, underscoring the importance of place and privacy in shaping how men engage with their mental health (McKenzie et al., 2025). The misaligned support also underlined the gendered challenges for men’s peer support. Research from Gough et al. (2021) indicated that when men engaged informal mental health support, they were more likely to reach out to significant women (e.g., female partners), a finding echoed by Burleson et al. (2005) 16 years earlier. For many participants, men’s mental health challenges are experienced and expressed as embodied emotional distress, rendering intimate partners the most likely confidant and help (Oliffe et al., 2024a). The current study, while not explicitly delineating those practices, might reasonably reveal unique challenges for men’s mental health peer support. That said, also evident are the need for other help resources including and perhaps especially male peers. As Shaw et al. (2021) suggest, the lack of accessible emotional support is a key risk factor for men’s self-harm and suicide.
Notwithstanding the gendered barriers detailed here, there is strong potential to leverage emergent cultural shifts in mental health and masculinities to shift men’s peer support in terms of mutuality and reciprocity. Bromance research by Robinson et al. (2017)—wherein the tenets of men’s peer relationship was marked by emotional intimacy, trust, and cohesion—suggests positive effects for men’s mental health and social well-being. Not to undervalue the benefits of organic connections (e.g., fun and light chats) between men, the normative framing of peer support, including mental health check-ins, might usefully extend the activity-based connectedness of men’s friendships.
While it is possible that the identified themes could have been accessed through other qualitative methods, photovoice added value to this study. Specifically, participant-generated photographs provided evocative prompts grounding the interviews in concrete, often deeply personal experiences. For many men, the act of taking and selecting photographs facilitated reflexive practices and meaning-making in advance of the interview, fostering engagement and explanations in our conversations. In some cases, images allowed participants to express difficult or otherwise ineffable aspects of their mental health experiences. As such, photovoice not only supported data richness but also aligned with the participatory ethos of the study by actively promoting participant agency in shaping their narratives (Oliffe & Bottorff, 2022).
Men’s well-intentioned peer support needs to be reinforced with increased mental health literacy (Sampaio et al., 2022) to aid the recognition of and assistance with men’s inevitable life challenges. Recognizing this need, the current study has also informed the development of tailored resources to enhance men’s social connections and promote help-seeking behaviors. The In Good Company with Dr. Paul Sharp podcast has featured along with a collection of participant-submitted photographs and narratives on the In Good Company website (www.ingoodcompany.menshealthresearch.ubc.ca/) with the express goal of discussing and depicting men’s struggles and strategies for engaging peer support. Resources are similarly available elsewhere. For example, the Men’s Health Forum offers Men’s Health Champion training courses with the goal of equipping male volunteers with the knowledge and skills to champion men’s health (Baker & Pollard, 2024). Incorporating gender-responsive training aimed at bolstering peer mental health literacy and communication skills may help men recognize signs of distress in themselves and others, and effectively respond in supportive ways consistent with masculine norms (e.g., shared activities, goal-oriented conversations, and expression of solidarity) (Sharp et al., 2025). Such capacity building can be influential in men recognizing stoicism and emotional avoidance as unhelpful masculine states. Moreover, catalyzing men’s social connection skills to proactively and mutually enhance the mental health of themselves and their peers through existing programs (e.g., sporting groups, men’s sheds, or workplace initiatives) can help normalize help-seeking and giving.
Study limitations include the broad definitions of both mental health and peer support in the research design, which meant we relied on participants’ interpretations of the two concepts in offering more general narratives of their gendered challenges. Future work might usefully differentiate the various contexts of peer support and specific mental health challenges (including severity) to nuance understandings about what works in peer mental health support and how it can best be mobilized. As peer work models gain traction globally, it will be particularly important to examine how these distinct dynamics transpire within more formalized mental health peer work settings.
In conclusion, men’s uptake of mental health peer support—both intentions and actions—can be constrained by normative masculine identities and relations. With the shifting discourses on masculinities, mental health, and men’s help-seeking, the gendered barriers thematically revealed men’s lived experiences to thoughtfully consider and strategically build capacity in framing and guiding gender-responsive peer support initiatives to promote men’s mental health.
Footnotes
Author Contributions
Study conceptualization and design: PS; data collection and analysis: PS, NG, PZ, and RC; draft manuscript preparation: PS, NG, PZ, RC, and JLO. All authors reviewed the results and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Government of Canada’s New Frontiers in Research Fund (NFRF) (NFRFR-2022-00308). Sharp is supported by a Michael Smith Health Research BC Research Trainee award, Canadian Institutes of Health Research Fellowship, and SSHRC project grant (NFRFR-2022-003080). Seidler is supported by an Investigator Grant Fellowship from the National Health and Medical Research Council of Australia (2008170). Oliffe is supported by a Tier 1 Canada Research Chair in Men’s Health Promotion.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
This study received ethical approval from the University of British Columbia Behavioral Research Ethics Board (UBC BREB) (approval # H23-00301).