
Abstract
Research indicates a positive correlation between residential treatment duration and residents’ positive outcomes. Between 2015 and 2019, a New Zealand residential drug rehabilitation service noted a rise in premature program exits, leading to an in-depth investigation into the individual and therapeutic community factors that impact residents’ completion of the 18-week program. The aim of the study was to understand how to enhance support mechanisms that promote longer treatment stays with the view to improving well-being outcomes. The authors conducted a two-phase, mixed-methods study. They applied quantitative secondary data analysis to data collected between 2015 and 2019 from 796 participants and did follow-up qualitative data collection in 2023, where 15 former residents participated in focus groups. Six were then randomly selected to participate in an in-depth interview. This article reports findings from the interviews of that study. The aims of this article are threefold. The authors introduce data from a New Zealand drug rehabilitation service as a case for using ChatGPT to support AI-assisted thematic narrative analysis. Steps in the analysis are detailed through a reproducible prompting process. Second, the authors present findings highlighting factors influencing residents to leave treatment and those that influenced them to stay. The authors position AI as a complementary tool for qualitative data analysis that enhances methodological rigor and practical applications in addiction research.
Keywords
Introduction
Substance use disorders (SUDs) continue to affect a significant portion of Aotearoa New Zealand’s (Aotearoa NZ) population, with the Ministry of Health (2024) reporting that more than a quarter of New Zealanders over 15 years of age face moderate to high risk for such conditions. Despite the harm substance misuse inflicts on individuals and communities (e.g., strained family relationships, greater mental health disorders such as anxiety and depression, increased crime rates, adolescent developmental issues, academic challenges, and future dependency), access to treatment remains uneven. Extended wait times, limited service availability, and societal stigma impede recovery pathways (Jackson et al., 2023). Māori, the Indigenous people of Aotearoa NZ, face disproportionate rates of SUDs (26.5% compared to 12.3% for the total population [Clifford, 2020]), making the stakes particularly high. Structural inequities such as the lack of culturally specific health messaging and the failure to integrate Te Reo Māori (language) and Mātauranga Māori (knowledge) in public health campaigns create compounding challenges contributing to widening inequalities as well as early exposure to substances (Clifford, 2020; Huckle et al., 2024). Yet, research shows that the solutions are as diverse as the challenges. Treatment for problematic substance use in Aotearoa NZ spans a continuum, from abstinence-based to harm-reduction models. Longer retention in treatment is closely linked to better outcomes, including reduced substance use, improved psychological well-being, and lower reoffending rates (Ashdown et al., 2023; Mulder et al., 2009).
The findings reported in this article concern one treatment approach: therapeutic communities (TCs). TCs, in the context of substance use, are drug-free residential treatment facilities where the community (i.e., its residents and staff) plays a central role as the primary therapeutic tool. The approach emphasizes mutual accountability, peer-driven learning, and collective responsibility, contrasting with clinician-led or individual-focused therapies like CBT (De Leon, 2015). Beyond abstinence, TCs aim to instill values like honesty, self-reliance, accountability, and responsible social behavior to focus on the concept of “right living” (De Leon & Unterrainer, 2020, p. 60). This makes the goal of recovery broader than just ceasing substance use. Residents move through a hierarchical structure, gaining responsibilities and rewards as they demonstrate personal and social growth while serving as positive role models for one another under staff supervision and guidance (De Leon & Unterrainer, 2020).
TCs show promise, but their success often hinges on factors like duration of treatment, cultural alignment, and social support systems (De Leon, 2015; De Leon & Unterrainer, 2020; Shaver et al., 2023). A substantial body of research points toward the fact that people who finish the full duration of treatment have the best outcomes (De Leon, 2000 cited in King et al., 2016; de Leon et al., 1982; Hubbard et al., 1997), making treatment completion an important indicator of success in therapeutic rehabilitation.
The longer someone stays in a TC, the better chance the person has of meeting their recovery goals (Bell et al., 1996; De Leon, 2010; Inciardi et al., 2004; King et al., 2016; Welsh, 2007; Welsh & McGrain, 2008), whereas leaving treatment early can diminish the likelihood of sustained recovery, exacerbating the cycle of addiction (Vanderplasschen et al., 2013). The method of entry into the TC (coerced or voluntary) has also been known to influence engagement, with Haviv et al. (2024) illustrating how legal coercion can enhance early treatment retention as intrinsic potential builds over time. This is also supported by local evidence from Ashdown et al. (2023), who indicated a higher level of retention among court-mandated participants in an Aotearoa-based TC.
Program quality and organizational structure are important retention factors. A predictable routine and clear program expectations have been linked to higher levels of retention, with Smith and Lawson (2017) noting this provides a sense of safety and predictability for residents. Although peer learning and accountability remain important in the TC setting, client-level variables such as drug use severity and mental health strongly predict dropout (Evans et al., 2009; Ravndal & Vaglum, 1991). Haviv and Hasisi (2019) found TC programs that blend addiction treatment with mental health services enhance retention. Furthermore, Strauss and Falkin (2000) in their US-based study on women offenders indicated perceived fairness and quality of staff support influence program retention.
Research shows that consistent peer affirmation and structured social dynamics within TCs contribute to retention and may support relapse prevention (Campbell et al., 2021; Warren, 2020). Peer connection is a key protective factor. Research underscores that empathy, shared lived experience, and role modeling (whether by staff or residents) can support engagement and self-efficacy (De Leon, 2000; Knight, 2021; Moos, 2007). However, these dynamics must be managed carefully, as peer interactions can also reinforce unhelpful behaviors.
Gender-specific needs also impact retention. Women in treatment often face complex trauma histories and caregiving responsibilities, and evidence indicates separation from children can disrupt recovery (Stanley, 2023). Family-focused interventions that support maternal identity have been linked to increased retention (Conners et al., 2006; Madden et al., 2022; Suchman et al., 2011), by allowing residents to maintain a connection with their children while receiving care, thereby reducing distress and strengthening motivation to remain engaged in treatment.
This article serves three purposes. We explore the application of artificial intelligence (AI), specifically ChatGPT 4o, as a tool for assisting narrative analysis. ChatGPT (i.e., generative pre-trained transformer) is an advanced AI language model that generates human-like text by utilizing knowledge from a large dataset (i.e., open-source content across the entire Internet) to produce contextually relevant responses to the user’s prompts. Using an Aotearoa NZ residential drug rehabilitation service as a case study to demonstrate how ChatGPT can assist in narrative analysis, we build on the work of other researchers exploring AI-assisted qualitative data analysis (QDA). It showcases our approach to AI-assisted narrative analysis as adapting Chubb’s (2023) and Hamilton et al.’s (2023) AI-assisted QDA. The approach to analysis involved the triangulation of themes generated separately by researchers and ChatGPT, and was then confirmed by participants. Second, this study explores the interplay of structural, cultural, and interpersonal dynamics that shape retention and early exit in TCs, drawing on both local and international research. Finally, the study is an example of how AI-assisted narrative analysis can be used to organize and present findings in a way that upholds the integrity of participants’ lived realities of SUDs while uncovering themes critical to understanding treatment exit and completion. Service providers can consider our findings to inform interventions and service design to increase engagement, potentially reducing relapse rates and improving long-term health outcomes.
Therapeutic Communities in Aotearoa: A Brief Introduction
Aotearoa NZ’s TCs, including Odyssey House, Higher Ground Papa Taumata Drug Rehabilitation Trust (henceforth Higher Ground), and Moana House, demonstrate the impact of culturally informed and family-inclusive models. For example, Higher Ground integrates te ao Māori (Māori worldview) principles and practices alongside its 12-step framework, acknowledging the importance of cultural identity in recovery (Higher Ground, 2024). Meanwhile, including children in treatment settings (e.g., Odyssey House Family Centre) has been shown to improve retention rates by addressing the practical needs of parents (Conners et al., 2006). Outcomes from these approaches are encouraging. Residents completing Higher Ground’s 18-week program report significant reductions in substance use and improvements in physical health, mood, and relationships (King et al., 2016). Similarly, programs incorporating tikanga Māori have demonstrated efficacy in reducing recidivism and fostering deeper engagement among participants (Adamson et al., 2010).
Despite the growing recognition of TCs as effective treatment models for SUDs, attrition remains a pervasive challenge internationally. In Aotearoa NZ, research outcomes of TCs remain underexplored. This fact makes it crucial to determine whether Aotearoa NZ TCs yield similar results and face comparable challenges of TCs internationally, ensuring that practice is guided by the best evidence and is fit for context. Existing studies in Aotearoa NZ, point to the complexity of this issue. For instance, research at Moana House in Dunedin, which provides a nine-month long residential program and an additional three months of aftercare, emphasizes the interplay between cultural relevance, mandated participation, and retention rates, evidencing participants with court-mandated treatment are more likely to remain in the program for at least three months (Ashdown et al., 2023). Meanwhile, evaluations of programs like Higher Ground in Auckland demonstrate the need for tailored, culturally inclusive models but also underscore the logistical and emotional barriers that can disrupt treatment continuity (King et al., 2016). The evidence also highlights how integrated approaches addressing broader psychosocial needs can support retention. Parenting-focused rehabilitation services, for example, have demonstrated the benefits of coupling substance misuse recovery with parenting support, allowing parents to prioritize both their health and their families (Stanley, 2023). However, gaps remain, particularly regarding the structural factors that influence retention across therapeutic settings for SUDs and resident narratives about early exit.
Methodology
Compelled by our commitment to answer a question raised in practice, “Why do people leave our treatment program early?” our research followed a qualitative narrative research design that views stories as central to how individuals construct, interpret, and communicate their experiences. As an approach, it guided the entire research process, including data collection, analysis, and interpretation. Narrative research considers stories as fundamental to understanding human experience, emphasizing stories as the primary form of data collected as well as the output of the analysis (Riessman, 2005). We focused on gathering stories about participants’ identities, relationships, and cultural and societal influences in relation to a particular experience (e.g., a recovery journey) to explore how individuals made sense of their treatment journeys. Their journeys included challenges, turning points, and decisions to continue or leave, with the analysis specifically looking for the individual and structural contributors to treatment retention or early exit. The story outputs in this study are presented as narrative moving vignettes.
Narrative Moving Vignettes in Data Analysis
Vignettes are a method of presenting participants’ stories in a concise yet impactful way that maintains the depth and complexity of their experiences while focusing on specific, meaningful moments. Qualitative studies often employ vignettes as a methodological instrument, presenting fictional narratives to participants to elicit their reflections on specific subjects during data-gathering sessions, occasionally using vignettes based on actual events (Sampson & Johannessen, 2020). However, vignettes derived from interviews and other textual sources as a means of organizing and presenting findings of a study are gaining popularity across various fields that utilize qualitative research approaches (Chubb, 2023).
The story outputs in our study are presented as narrative moving vignettes to capture the trajectory of a single person’s experiences over time. Given (2008) previously discussed the idea of moving vignettes as a longer narrative being presented to garner responses from a participant in an interview. Instead, we use the idea as a means of presenting data where the narrative arc of change was central to portraying participants’ experiences as evolving rather than single-dimensional. Chubb (2023) employed AI tools to condense interview transcripts into engaging, concise narrative vignettes—a method that significantly speeds up data analysis and enhances the clarity of presenting complex participant experiences. Our study expands on Chubb’s (2023) use of AI to transform qualitative data into narrative vignettes, building an understanding of how AI can be used as a supplementary tool in data analysis.
Research Setting
Modified TCs emerged in the 1990s, offering greater staff involvement and a broader range of support, often delivered within a shorter timeframe (De Leon, 2015; Melnick et al., 2000). These programs incorporate individualized therapies, family inclusion, and services such as medical care, mental health support, and vocational training (Ashdown et al., 2017; De Leon, 1995). Participants were recruited from an Aotearoa NZ–based modified TC, Higher Ground, which reflects similar environments to other TCs through its shorter 18-week residential program, increased staff involvement, integration of 12-step recovery principles (Gamble & O’Lawrence, 2016), and a mandatory Māori cultural program for all tāngata whai ora (i.e., people seeking wellness). The TC incorporates a holistic approach to rehabilitation, emphasizing spiritual dimensions such as honesty, open-mindedness, and respect as foundational elements for healing. Admission to Higher Ground is primarily for Aotearoa NZ residents, with priority given to those living in specific regional areas unless dealing with methamphetamine addiction, in which case residents from anywhere in the country can be admitted. Individuals looking to enter the program must undergo an intake interview to ensure the program’s suitability for their needs. Most residents qualify for financial support through the country’s social welfare provider, Work and Income New Zealand, to supplement the program’s cost, although those who do not qualify may pay a weekly charge. Emphasizing peer support and personal development, the TC aims to equip residents with essential tools for long-term sobriety to improve both social and psychological well-being while maintaining abstinence.
Participants, Data Collection, and AI-Assisted Qualitative Data Analysis
Participant Demographics.
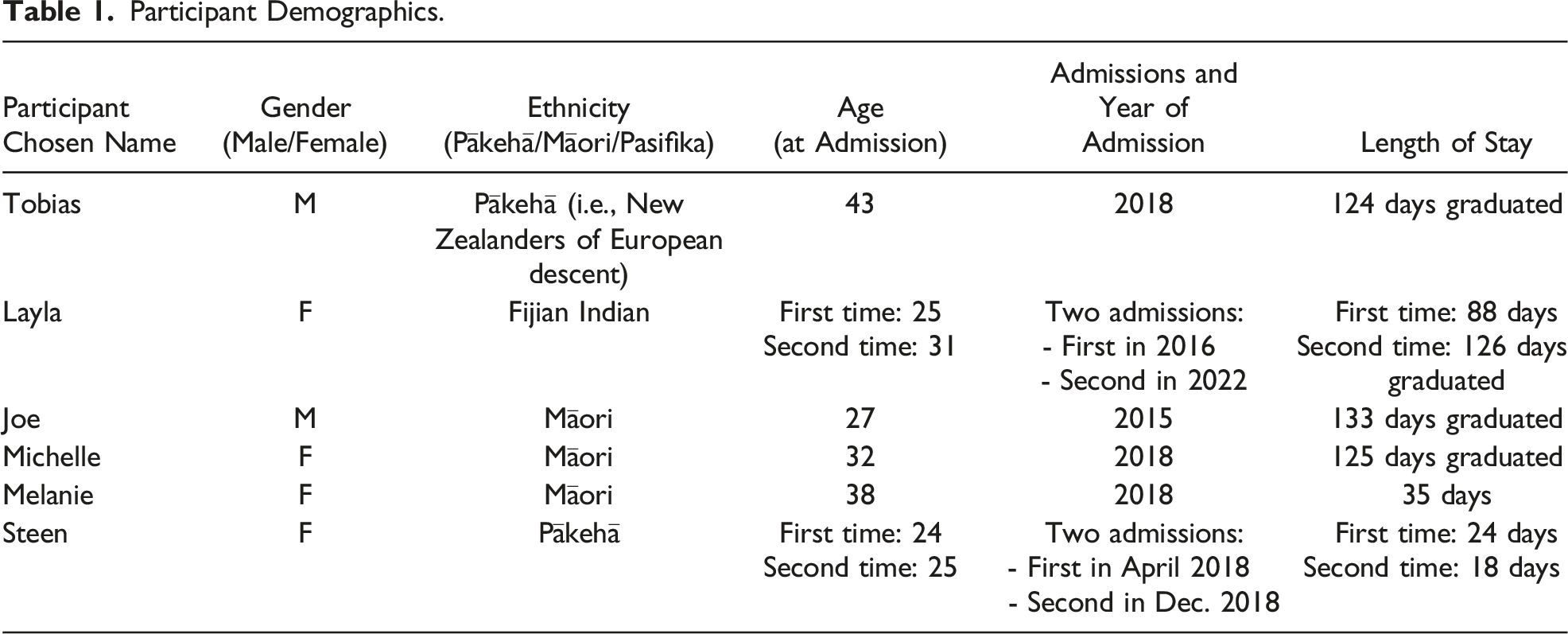
Given the sensitive nature of the interview topic and the potential for re-traumatization during the interview, participants were informed of their right to stop or fully withdraw from the interview at any time without giving a reason. Prior to starting the interview, participants were given the contact information for an independent trauma-informed registered counselor with experience in addiction should they need the extra support. Participants all chose their pseudonyms so they could see themselves reflected in the data. We determined the interview questions following an analysis of the focus groups for dominant themes. Ethical approval was obtained through Aotearoa Research Ethics Committee—Te Roopu Rapu i te Tika (Approval #: NZEC22_44).
Using interviews conducted with participants of guaranteed income pilots, Hamilton et al. (2023) compared emerging themes from qualitative analyses that were executed collaboratively by humans and ChatGPT. The authors highlighted overlaps and discrepancies in themes identified by human coders and ChatGPT, noting specifics missed by each. Their findings suggested that ChatGPT could effectively help supplement human tasks in complex research scenarios. Their conclusion anticipated the broader use of such AI tools in research, with the authors suggesting that future studies could involve directly inputting raw transcripts into ChatGPT and using AI-generated themes in discussions between researchers to detect overlooked aspects, perspectives, and personal biases. Our analytical process aimed to trial that suggestion by feeding ChatGPT our de-identified interview transcripts as part of the simple 10-step vignette creation protocol for an AI-assisted thematic narrative analysis illustrated in Figure 1.
1
We focused on looking for recurring themes and patterns across each participant’s narrative and producing a narrative devoted to those themes. Riessman (2005) defined thematic narrative analysis as examining stories by identifying and interpreting themes within the text, focusing on what is said rather than how it is told or what are the structural elements of the narrative. Vignette creation protocol for AI-assisted thematic narrative analysis.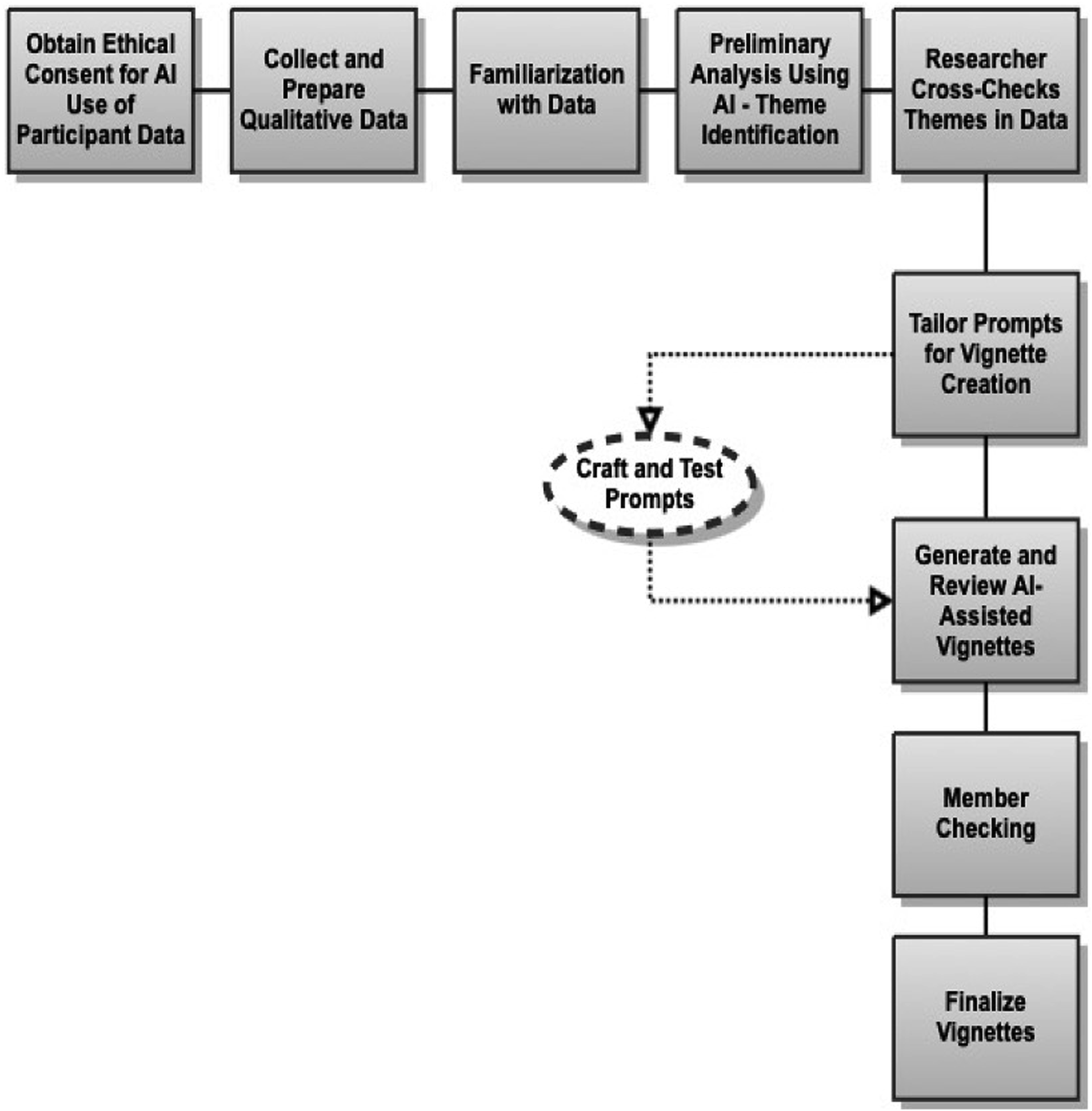
The initial plan for analysis was to create each participant as a case in NVivo 14 and then thematically analyze each before manually developing a vignette for each person aligned with the themes. However, the first author had previously developed an AI-assisted QDA process using a generative AI tool to present findings in the form of vignettes for a different study (Chubb, 2023), and we decided to explore this as an option for their dataset. This involved first obtaining ethics approval from Higher Ground and developing new Participant Information Sheet and consent forms before reaching out to the participants to perform a reconsenting process (from which they could opt out). The second author contacted each participant via email, explaining the proposed use of AI for analysis, and offered the option to review their AI-generated vignettes. Participants were also assured that should they opt out of their data being used in ChatGPT, we would continue manual analysis, and a researcher-crafted vignette would be sent to them for confirmation. Upon reconsent, the transcripts were checked for full anonymization (i.e., stripped of names, locations, and any identifying information) prior to analysis. This is consistent with standard practice when uploading data into software like NVivo. We then ran their de-identified transcripts through ChatGPT 4o, with memory disabled—meaning the chatbot did not retain any information about the conversation beyond that session, ensuring the interaction was completely temporary and the chat would be deleted after analysis was completed. All six interviewee participants consented and were asked to review an AI-generated version of their vignette (i.e., member-checking) (Schurink et al., 2021). This process established a foundation of transparency and respect for participant autonomy over their final narratives. We prepared qualitative data by anonymizing all transcripts, removing any names (except participant pseudonyms) and identifiable details (e.g., locations) and disabling the memory function in ChatGPT 4o.
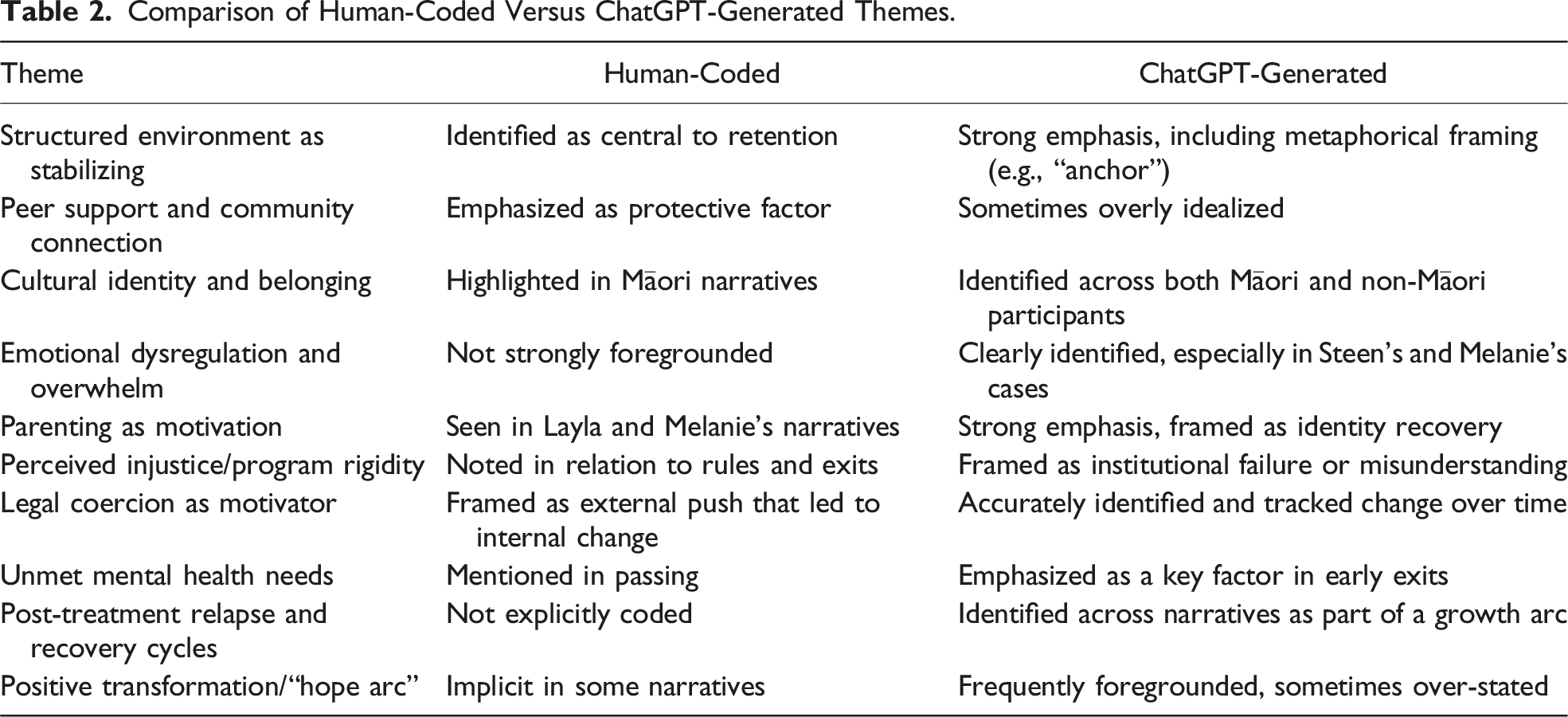
We then familiarized ourselves with the data by reading and annotating transcripts and coding initial patterns to build a foundational understanding of participant narratives through preliminary themes around factors influencing why people chose to leave treatment and why they chose to stay.
Comparison of Human-Coded Versus ChatGPT-Generated Themes.
Prompt-Design Steps for AI-Assisted Vignette Creation: Tobias’s Vignette Example.
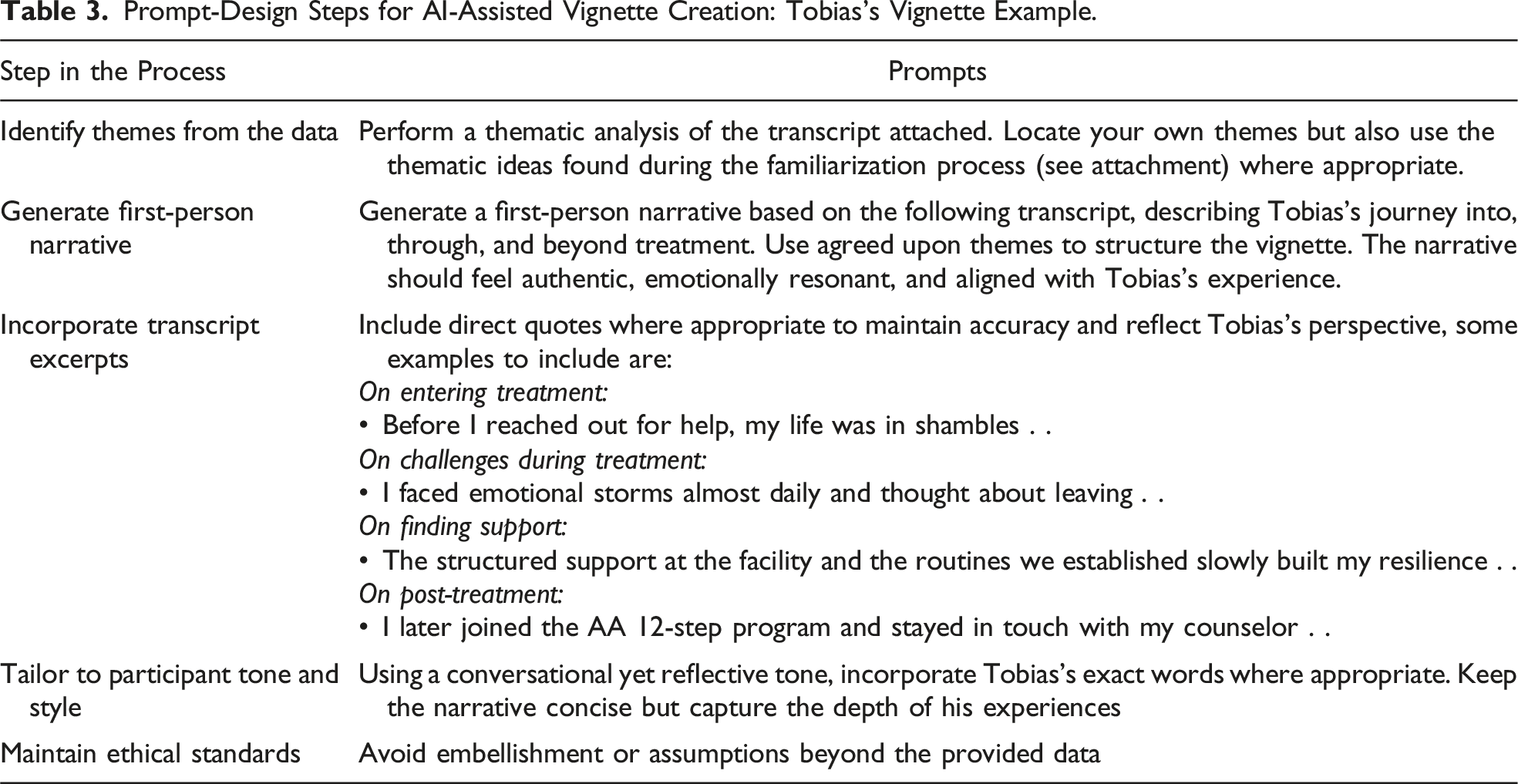
Combining the finalized instructions as one prompt, ChatGPT generated draft vignettes for each participant. The first two authors reviewed the drafts and compared the outputs with the original transcripts to ensure accuracy and alignment with participant voices. Where discrepancies or inaccuracies arose, we revised the vignettes manually to better reflect participants’ stories.
Member-Checking Response Email Text From Participants.
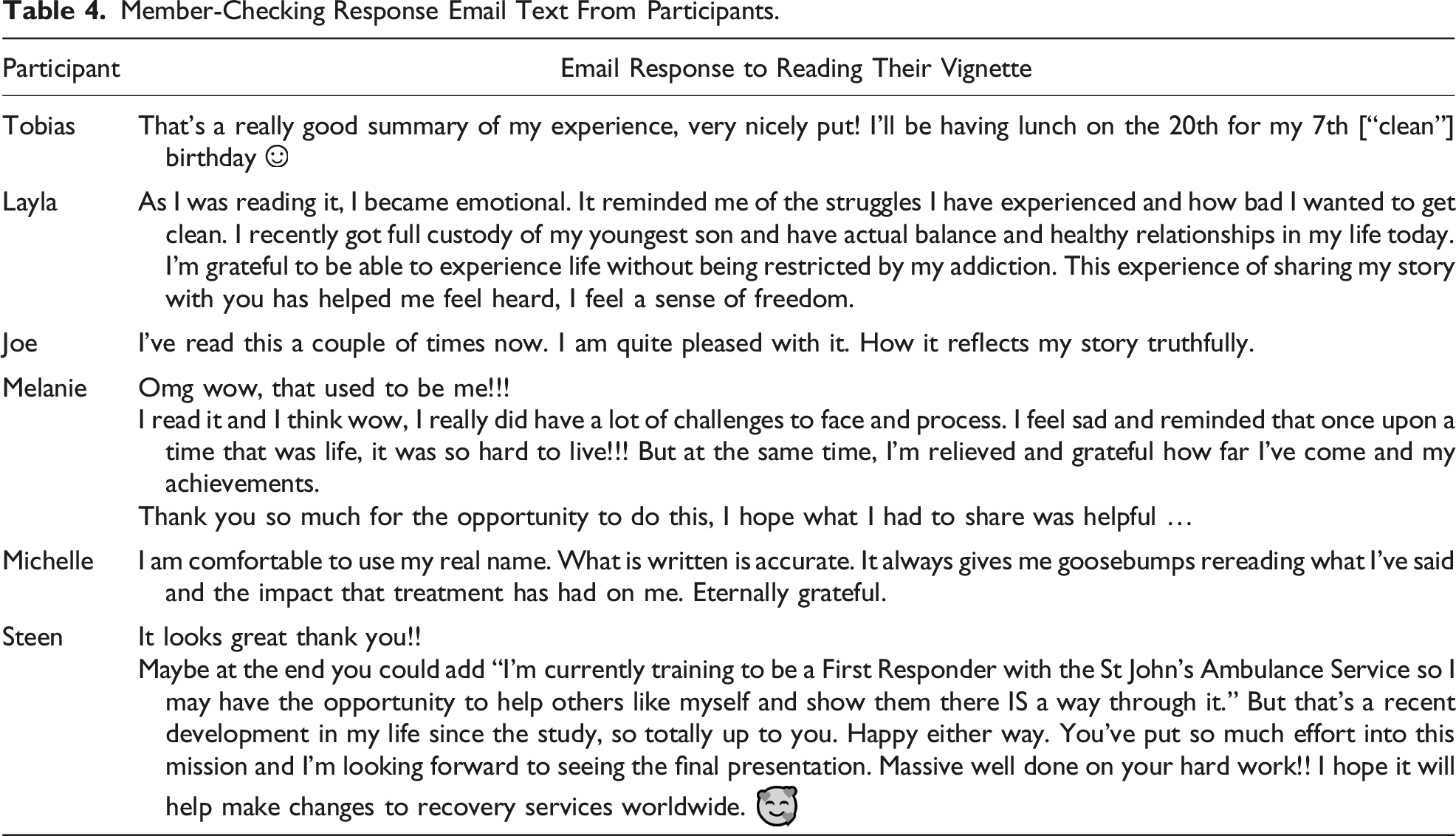
The process presented an opportunity to assess the impact participating in the project had on residents—or what Koelsch (2013) referred to as transformational validity. The process represents a counter to harmful research practices that distort the original intent or meanings behind what participants share during data collection, where the process not only prevented harm but also provoked catharsis. It also demonstrates a concrete example of the process of member-checking, something Harvey (2015) asserted is lacking in reports of research.
The authors assert that Hamilton et al.’s (2023) conclusions were correct as engaging ChatGPT for the purpose of analyzing raw qualitative data facilitated rapid coding, organization, interpretation, and presentation of data in our study. The final outputs are a combination of AI-generated content, our refinements, and participant confirmations that the vignettes represent an account grounded in the stories they shared. Through this process, we balanced the efficiency of ChatGPT with the depth and ethical considerations essential to any qualitative analysis.
Findings
Residents’ Main Reasons for Leaving or Staying.

Tobias: Emotional Storms and Anchors
Tobias’s entry into treatment was driven by a deep personal crisis, including family separation and a subsequent abusive relationship, leading to severe isolation and a life he described as “meaningless.” Initially, Tobias found the social aspect of the treatment challenging yet rewarding, as it reintroduced positive social interactions into his life. However, he also faced significant emotional upheavals, including suicidal thoughts and anger, which were addressed within the treatment setting. Tobias engaged in a structured Higher Ground’s post-treatment program and later lived with someone from treatment, highlighting the importance of continued support. He also maintained a relationship with his counselor and actively participated in an Alcoholics Anonymous program. Tobias credits the treatment with life-changing improvements in his emotional regulation, personal responsibility, and overall life management. His vignette summarizes why he entered treatment and what factors supported him to stay: Before I reached out for help, my life was in shambles. I felt isolated and sad. My entire life just became kind of meaningless. I had no real connections with anyone anymore. At least that is what I used to think. The overwhelming pain finally pushed me to seek treatment, hoping for some relief. At first, the transition was tough. I had been alone for such a long time, completely isolated, and all of a sudden, I was surrounded by these people. The community at the treatment center was a stark contrast to that loneliness, and initially, it was overwhelming! But, staying wasn’t easy. I faced emotional storms almost daily and thought about leaving more than once. My go-to in a case like that is to make a quick exit, but the structured support at the facility and the routines we established slowly built my resilience. The program gave me a lifeline when I most needed it, and the tools I learned there became my foundation for recovery. I knew if I left early, I’d lose not just the support of peers and counsellors but potentially my life. That kept me going when things got tough.
Layla: A Rocky Road to Recovery
Early exposure to drugs and the criminal activities were part of Layla’s family, which she came to view as normal. Her experiences of trauma and neglect in this environment profoundly influenced her perceptions of safety and belonging. She detailed the evolution of her substance use, recounting cycles of domestic violence and legal troubles. These experiences played a significant role in her decision to seek help, motivated by the need to provide a better environment for her children. Layla’s recovery journey was marked by periods of relapse with varied experiences in TCs and support services, but Higher Ground offered her structure, support from peers and counselors, and a sense of safety that was critical for her recovery, as illustrated in her vignette: From as early as I can remember, the world around me was filled with chaos, my family’s parties, and the harsh realities of substance use . . . they called it “normal.” I started using meth at 12, believing it gave me control, a twisted inheritance from my family. My uncles they had businesses, and they liked to party, so I just didn’t understand what was happening in the household. But later in life, as the violence at home with my partner escalated and my kids got involved, I knew I had to reach out. I felt bad as a mother. We were both using. I wasn’t giving them the best that they deserved. My first cry for help with a support service felt like shouting into the void. No support, just silence. It was just really annoying. Treatment centers like Higher Ground and several others became my sanctuary, a place where, despite my struggles, I found a framework to rebuild. Yet, every step forward seemed shadowed by setbacks, from systemic failures to personal relapses. I would stay clean, then I had a lapse, got back up and then stayed clean for about two and a half, nearly three, years. It was a rocky road, but the drive to give my children a better life and the unwavering support from my counselors kept me going. They reminded me of my strength, even when I forgot.
Joe: Engagement Under Compulsion
Joe’s substance use began at a young age within a family environment where drug use was normalized. His substance use escalated to harder substances, and the legal troubles that ensued largely prompted his treatment. Joe’s account indicated a pragmatic approach to treatment, marked by compliance with legal obligations and driven by the necessity to avoid incarceration rather than a genuine commitment to recovery. Joe reflected on his improved self-awareness and control post-treatment, highlighting personal and professional growth. He acknowledged the indirect benefits of the treatment despite his initial reluctance, as demonstrated in his vignette: When I first walked through the doors of Higher Ground, it was under the heavy weight of a court mandate. I wasn’t there because I wanted to be. I was there to avoid going back to jail . . . a get-out-of-jail-free card. So, I thought I would get out of jail and go. My whole mindset was about survival, not recovery. As I navigated the days, my approach was minimal—do just enough not to get kicked out. It was all a bit crazy, and I had no intention of going through a program, but the flip side wasn’t the best option. But while I was keeping my head down, something unexpected happened. I began to pick up on things, and I think the biggest impact has been giving me awareness of everything, like understanding how my reactions to others were shaped by my past and a new awareness of people and their behaviors and what I can control. This was new to me, realizing how much of my behavior was about control and how letting go could actually feel liberating. The real support came from the structure of the program itself. The daily routines and the peer support during group sessions, even though I resisted participating, provided a constant backdrop against which I could measure my progress. And gradually, my reasons for staying shifted. It wasn’t just about avoiding jail anymore.
Melanie: “Staying Stopped”
Melanie had an extensive history of meth addiction and involvement in criminal activities to support her habit. Melanie’s decision to seek help was influenced by the realization that her lifestyle was unsustainable and harmful, particularly after her partner’s incarceration and subsequent relapse. During treatment, she experienced highs, such as gaining self-awareness, and she experienced the emotional lows of confronting her SUD. Melanie detailed her struggles and successes after leaving Higher Ground, highlighting the importance of ongoing support, therapy, and personal growth. Her vignette captures the challenges with institutional rules, the impact of being discharged early, and her views on how the program could better support residents: I was a meth addict for 25 years. I did crime to pay for my habit. I was doing burglaries 24/7 and putting needles in my arm. Violence was a constant companion. At one point, I was left partially blind after a brutal beating by my partner. That relationship was really abusive . . . stabbed me, would beat me continuously. When my youngest children’s father was released from prison, we used together. I abandoned my children with my mother, spiraling further. I knew that I needed help because I just could not stop, especially with the crime. A person from a support service pushed me to seek help. Entering Higher Ground was tough. It turns out stopping is the easy part, staying stopped and being comfortable in my own skin was a whole other story. I knew I needed to be there to confront and do the things that I needed to do. I felt traumatized the whole time I was there, but it woke me up to how unwell I was. I was literally exhausted the whole time I was there, and I couldn’t help but wonder if they do that on purpose. The main reason I left was because my kids weren’t coming to visit me, which really got to me. But the final straw was when I called out another peer for a major rule break. She denied it, and I was called a liar. That was it for me. I thought, fuck this, this isn’t going to work. And even though I wasn’t at all prepared for life after treatment, that early discharge pushed me to stay committed to my sobriety. Post-treatment, I found purpose working for the support service that helped me initially. Regular therapy and NA meetings have been vital. My kids were my initial motivation, and their absence made things harder. If Higher Ground could have picked them up and supervised them with another adult, and brought them in to visit, that would have been more helpful. Now, celebrating two years of sobriety, I see the importance of structured support and family involvement in sustaining recovery.
Michelle: From Spiral to Structure
Michelle started using drugs at a young age and resisted several attempts by her family to go to rehab. The loss of her children and the impact this had on her led to multiple relapses, periods of recovery, and eventually incarceration. She shared the difficulties within various institutions, including lack of proper support during her remand period and the programs offered—or not offered—during her sentence. Michelle spoke of her eventual entry into Higher Ground, her experiences there, the support she received, and the challenges she faced, including dealing with her past, the stigma associated with her actions, and the dynamics within the treatment setting. She also discusses life after leaving, focusing on personal growth, rebuilding relationships, employment challenges, and her ongoing therapy and recovery journey. I started using drugs around 15, rebelling against everything, including my family’s attempts to get me into rehab. By 17, I cut off contact with them completely. Having my son was a turning point. I got clean for 18 months, but losing custody of him to my ex’s mother shattered me. My addiction just absolutely spiraled at that time; it was really bad. I faced legal troubles, including a kidnapping charge that led to almost three years in prison. There, I struggled to find support. There were no courses in remand, and I wasn’t able to get any until I got sentenced. Finally, I was transferred to a drug treatment unit, and it was there that I saw a way forward. I rang my mum and said, “Mum, I am going to Higher Ground.” Navigating Higher Ground was tough. I felt lost at first, but the structure and cultural aspects, like learning the haka, gave me confidence. While not all staff were supportive, the cultural leaders really guided me through the program. There were lows, like being humiliated in family group sessions, but the therapy and support I received helped me separate my identity from my past. Post-treatment, reintegrating was challenging. I sought out therapy once I left and have been in therapy ever since. What kept me in treatment? The realization I needed to change for my children and myself despite the struggles. The structured support, even with its flaws, provided a foundation I could build on.
Steen: A Seed for Recovery
Steen’s story is one of turning a challenging past into a future of recovery and healing. She traces her descent into problematic substance use as a coping mechanism rather than a habit. Her story highlights factors beyond addiction, like trauma, social environment, and pivotal life events, that can influence a person’s path to seeking help. Steen’s experiences within the program capture the emotional and psychological rollercoaster that residents often face. Her story also demonstrates how the environment, despite its challenges, can plant the seed that starts the road to recovery: I grew up in church, deeply involved in youth work, but my life took a drastic turn at 19 when I left and ended up in a brothel. Drugs came into my life not to fuel a habit but to cope with the trauma of my new reality. I ended up doing them to deal with the work that I was doing . . . made it easier to block it out. The gang rape and subsequent abortion pushed my usage to dangerous levels. The birth of my nephew was a wake-up call. My sister’s ultimatum “get clean, go to rehab, or lose contact with him” was the push I needed. Wanting to reconnect with my family, I sought help. At first, I tried to quit everything cold turkey and ended up having a seizure but managed to get myself into detox. Then, I chose Higher Ground, knowing others I trusted had said it was my best chance at recovery. My time there was a rollercoaster. The first time is very daunting, obviously. I was so anxious and was unmedicated for ADHD and probably a lot of PTSD at that point too that I hadn’t dealt with. Despite the anxiety, there were moments of connection with others who shared my experience and clarity and some supportive staff. I went to my first NA meeting ever, and I just loved it. I felt like I found my people. Unfortunately, I was discharged twice. The first time, I was told to leave for saying that I felt like hitting a staff member. I was just overwhelmed after sharing something traumatic and felt dismissed. After fighting to return, I was discharged again for mentioning a past mental health event to a peer. I didn’t know that wasn’t allowed, but they said I should’ve known. Both discharges felt like a mix of my misunderstanding and Higher Ground not understanding my mental health and emotional dysregulation. After each discharge, relapse was almost immediate, but the seed of recovery had been planted. I sought out therapy once I left Higher Ground. The structured support and community I was exposed to planted the seed for recovery. Working on a dairy farm also helped me build a routine, and reconnecting with NA meetings showed me I didn’t have to do it alone. Now I am celebrating my two years . . . I’m currently training to be a First Responder with the St John’s Ambulance Service so I may have the opportunity to help others like me and show them there IS a way through it.
Discussion
AI-assisted narrative analysis using ChatGPT, as demonstrated in this study, offers health care practitioners and service providers an efficient tool for identifying and cross-validating patterns between human-coded and AI-generated themes in research on patient/service user engagement and attrition. Using ChatGPT enabled long interview transcripts to be synthesized into meaningful narratives, allowing the researchers to promote specific themes that might either be missed through traditional methods or be less emphasized. The analysis process gave researchers more time to connect with participants and discuss the presentation of our findings, confirming its alignment as being rooted in their lived experiences. The findings illustrate how emotional, social, and environmental factors shape residents’ decisions to leave treatment early.
Structured routines were a key factor in encouraging residents to continue treatment, a well-documented characteristic of TC environments (Adamson et al., 2010; Jason et al., 2015; Mutschler et al., 2022; Shaver et al., 2023; Smith & Lawson, 2017). Some studies have even suggested increasing structure within TCs to improve retention further (Mills et al., 2024). Participants in this study echoed these findings, reporting that clear rules and routines gave them a sense of security and predictability. Such environments also support psychological safety, which is particularly important for residents with past experiences of chaos or trauma (Lomas, 2024).
Adding to previous research, the cultural program, supportive staff, and connection to children emerged as significant factors promoting retention. These elements helped residents feel connected, valued, and empowered—an experience many had not previously encountered. While the program was based on Māori values, non-Māori participants also expressed high satisfaction, stating that it helped strengthen their identity and sense of belonging as New Zealanders. This aligns with Stanley’s (2023) study of Odyssey House Family Centre, which demonstrated that cultural, racial, and religious diversity within TCs contributed to residents’ sense of inclusion. This finding also builds on the work of Haviv and Hasisi (2019) who demonstrated that integrative interventions with a cultural aspect enhance retention and decrease attrition.
All residents highlighted connection and peer support (either through paid staff or other residents) as protective factors for staying engaged in treatment. This aligns with broader research recognizing peer support as a foundational element of TCs to enhance engagement and accountability in recovery, as it provides empathy, encouragement, and shared lived experiences that support recovery (Knight, 2021; Neale et al., 2018; Welsh & McGrain, 2008). De Leon (2000) described this as the “community as method” approach (p. 92). However, Knight (2021) noted that peer interactions could sometimes lead to negative dynamics, particularly if group members reinforce unhelpful behaviors. Despite this, many former residents in this study reframed difficult peer experiences—such as feeling humiliated in a group session, as essential to their growth and recovery. In this way, peer support in TCs not only offered empathy and connection but also contributed to improved self-efficacy and encouraged positive behavior change through modeling and reinforcement (Moos, 2007).
Legal mandates also played a role in treatment retention. In Joe’s case, external legal pressure initially drove his engagement, but over time, behaviors modeled within the TC helped him develop internal motivation. This shift from extrinsic to intrinsic motivation has also been observed in other service settings, including a TC in Dunedin, New Zealand, where Ashdown et al.’s (2023) analysis of 240 tāngata whaiora admitted between 2011 and 2020 found that court-mandated residents were more likely to complete at least three months of treatment than those who voluntarily entered the program. This finding is consistent with international research. For example, Haviv et al. (2024) examining the Hartuv TC in Israel found that residents who entered as an alternative to detention had a 4.67 times greater likelihood of completing treatment compared to voluntary participants, suggesting that external legal pressure can bolster engagement and extend the duration of stay. Similarly, a large US study analyzing data from the Treatment Episode Data Set-Discharges from 2015 to 2017, which examined 43,437 cases of individuals with opioid use disorder, found that court-mandated participants had higher completion rates (Lucabeche & Quinn, 2022). Evans et al. (2009) also highlighted program structure and the availability of staff support as critical for retention, especially in court-mandated programs.
Despite supportive elements within the TC, many residents faced barriers that led to early program exits. Residents also identified unclear expectations, inconsistent enforcement of rules, and inadequate communication as major barriers to engagement and treatment success. A few participants reported feeling misunderstood because the TC’s strict, consequence-oriented model failed to address their mental health needs and trauma histories. Steen’s narrative reflected this dynamic—she described feeling unsupported, emotionally overwhelmed, and unable to regulate under ongoing scrutiny, ultimately leaving after just 10 days. Steen’s experience suggests that for some individuals with complex trauma histories, highly structured environments may unintentionally intensify distress rather than promote stability. Residents with co-occurring mental health conditions such as anxiety, depression, and complex PTSD sometimes felt unsupported within the TC framework, which contributed to their decision to leave. This demonstrates the need for trauma-and-violence-informed (TVI) methods beyond traditional trauma-informed care. These methods are particularly crucial in examining how interpersonal abuse, historical oppression, and systemic discrimination collectively impact individuals’ trauma experiences. A TVI approach prioritizes emotional safety, adaptability, and choice, which are essential aspects of maintaining retention of residents such as Steen who need structure and psychological sensitivity in order to fully engage with and benefit from treatment (Lomas, 2024; Short et al., 2019).
These findings are particularly relevant for the women in this study, all of whom had experienced significant family violence and carried complex trauma histories that further complicated their mental health needs. Building on this, research suggests that shifting from traditional trauma-informed care to a TVI approach can better meet the needs of individuals affected by both interpersonal and structural forms of violence. TVI frameworks emphasize emotional safety, empowerment, and context, acknowledging how trauma is shaped by intersecting systems such as colonization, poverty, and gender-based violence (Short et al., 2019). Incorporating TVI principles into residential treatment can help mitigate distress and improve engagement by promoting flexibility and relational trust. Lomas (2024) emphasized the importance of integrated mental health care within treatment programs including specialist support and pharmacological interventions, as key to improving outcomes for residents with co-occurring conditions.
Participants’ children were a significant motivating factor in entering treatment, but separation and limited visitation meant some residents left the program early. This was evident in Melanie’s case. She left the program after prolonged separation from her children and infrequent visits, stating, “I needed to be with my babies.” Research supports this finding, showing that parents, particularly mothers, frequently experience emotional distress due to separation from their children during treatment (Substance Abuse and Mental Health Services Administration, 2007). Melanie’s narrative reflects these broader gendered dynamics, where maternal identity and the emotional stress of separation intersect to influence treatment retention. These patterns are echoed in Strauss and Falkin’s (2000) study of women in drug treatment programs, which found that perceived fairness, emotional security, and the ability to maintain family bonds significantly influenced retention among female participants. Programs with family-centered approaches, such as on-site accommodations for children or regular visitation, have been associated with higher retention rates (Madden et al., 2022).
This study recognizes the challenge of providing person-centered care within TCs that can respond to individual needs while maintaining a shared structure. Findings emphasize the importance of the TC in considering these factors, reinforcing the elements that support sticking to the program while mitigating those that contribute to early exits. To promote retention, programs can integrate specialist and pharmacy care with TVI care that is sensitive to residents’ lived experiences. A clearer articulation of aims and objectives could reduce misunderstandings, and more flexibility and downtime could reduce exhaustion. Increased access to children through supported visits or increased virtual communication could help reduce the psychological toll of disconnection for parents. Finally, transparent processes for grievances and fair treatment protocols can promote trust in the therapeutic community. Implementing these strategies can help sustain residents’ engagement in treatment, reduce premature exits, and contribute to more positive recovery outcomes.
Limitations
Despite anonymization and participant approval, publishing detailed narratives carries a risk of indirect identification, especially in small communities. We mitigated this by altering identifying details and using member-checking, but we acknowledge that participants may later feel differently about their stories being public. Reaching former residents was also a challenge for this study. The absence of email addresses during recruitment hindered our ability to reach a diverse pool of potential participants, as issue compounded by reliance on postal addresses, frequent house moves, and address details collected up to eight years prior. Another potential limitation was retrospective bias, which refers to the tendency of people to remember past events inaccurately due to their current knowledge, beliefs, or emotions (Markman & Dyczewski, 2013). When interviewed about their time in treatment, most residents had not engaged with the facility for over four years, with the longest period since admission being six years. This means their memories may be distorted by forgetting details or unintentionally altering the narrative.
Conclusion
This study extends the existing literature by providing a deeper understanding of why individuals leave treatment programs prematurely. It demonstrates the utility of AI-assisted narrative analysis as a means of sharing recovery narratives and the required cross-validation and member-checking processes to uphold ethical commitments to participants, which prioritizes transparency and collaboration to ensure the final outputs resonate with participants. The study positions AI-assisted methods as an innovative analysis technique in addiction research that can be used to share stories. By addressing both methodological rigor and practical application, the authors’ approach to analysis contributes to ongoing discussions about the role of AI in reshaping qualitative methods to produce findings that can improve the delivery of care.
Findings demonstrate treatment programs should evolve and adopt more holistic approaches that reflect the complex realities of those they aim to serve. They should also incorporate compassionate treatment models capable of supporting sustained recovery. The findings suggest several practical changes that could improve retention across treatment settings. Enhancing communication about available support, offering more flexible family contact, easing rigid scheduling, and providing robust mental health support are all potential strategies to enhance outcomes. Programs should aim to be adaptable, with the recognition that recovery is not a linear process but a long-term pathway. This understanding is essential for developing systems that meet people where they are to enable lasting change. Implementing these adjustments could help residents feel more connected, supported, and capable of completing their treatment journey.
These findings should prompt TCs to consider how they answer the following question: Can an abstinence philosophy coexist alongside harm reduction? Higher Ground and other TCs that operate using similar abstinence-based approaches to recovery should consider the experiences of these former residents and their implicit calls for an approach to recovery that is increasingly framed through a harm-reduction and patient-centered lens. The research offers concrete suggestions for policy and practice reforms by exposing the reasons behind early treatment exit. Programs might improve retention by integrating more adaptive approaches to policymaking and program structure, such as increasing the flexibility of treatment phases based on individual progress and responses. Furthermore, the findings suggest enhancing the cultural competence of treatment programs, especially in diverse societies, to improve engagement and outcomes for all participants, particularly indigenous and minority groups.
Understanding why people leave treatment requires examining the interplay of personal, social, and systemic factors. Therapeutic approaches that align with cultural values, address logistical hurdles, and provide robust aftercare services may serve to improve treatment outcomes. However, ongoing investment in research and infrastructure is needed to ensure these solutions reach the communities most affected by substance misuse. Future research could test targeted interventions across different settings to measure their impact on retention rates and overall recovery outcomes. By doing so, addiction services can build a clearer evidence base for strategies that sustain engagement and improve outcomes throughout the treatment sector.
Footnotes
Acknowledgments
The authors would like to thank Elisabeth Price for her assistance in conducting interviews with residents in this study.
Ethical Statement
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Maree Matthews is the Program Director of Higher Ground. She was not involved in the recruitment, data collection, and analysis (i.e., zero contact with raw data), but did review and edit this manuscript for accuracy in relation to the therapeutic community environment, given her in-depth knowledge of the field of practice.