
Abstract
Literature on racism suggests that Black physicians are acutely aware of how systemic racism influences the health and quality of care of their patients while being targets of that same racism. In other words, they are both observers and recipients of how systemic racism permeates US medicine. Yet, there exists no phenomenological inquiry which centers their experience to make known the systemic depth of racism on the experiences of Black primary care physicians. The goal of this study was to understand the lived experiences of Black primary care physicians and their perspectives on racism. We conducted a qualitative study based on hermeneutic phenomenology to examine the lived experiences of Black primary care physicians and their perspectives for advancing anti-racist actions in US medicine. Purposeful sampling was used to recruit primary care physicians identifying as Black or African American. In-depth, semi-structured interviews of one-hour duration were conducted virtually. A six-stage data analysis process for hermeneutic phenomenology was followed to convey their lived experiences. This study yielded a rich description of lived experiences of Black primary care physicians in the US and provides insights into participants’ ambition to pursue medicine as a career path as well as past and current experiences in practicing medicine. This description culminated in recommendations that the medical community can act upon to address the legacy of racism across the continuum of medical education to practice.
Keywords
Introduction
The US social uprising of 2020 in response to high-profile police killings brought into motion public calls to confront and address our nation’s historical legacy of slavery and systemic racism. This legacy is especially apparent in US medicine where inequitable access to quality care and poor health outcomes persist among racialized communities (Bailey et al., 2017) and the proportion of Black physicians relative to the general population remains marginal (Ly, 2022). Gaining a better understanding of the effects of systemic racism is important to advancing anti-racist progress as Black people remain the least healthy population in the US and suffer from higher rates of cancer, heart disease, obesity, diabetes, and end-stage renal disease relative to their White counterparts (Noonan et al., 2016; Sederstrom & Lasege, 2022). Recent evidence indicates that Black individuals experience a staggering number of excess deaths (relative to their White counterparts) within the past two decades, amounting to 1.6 million premature deaths and 80M potential years of life lost (Caraballo et al., 2023).
While the diversity of the US population has increased over time, the physician workforce has been slower to represent the general population – this is especially pronounced in the representation of Black physicians who are more likely to practice primary care and serve Black and underserved communities (Xierali & Nivet, 2018). The percent of Black physicians has barely risen over the past 100 years, remaining around 5% of the physician workforce, which is low compared to the percent of Black individuals in the general population (about 13%) (Ly, 2022). This percentage remains low despite statements and calls by medical associations to increase diversity of the workforce (Argueza et al., 2021; Clayborne, 2022; Clayborne et al., 2021). The percent of Black men physicians is even lower, lingering at around 2.6% of the physician workforce since 1940 (Knox & Seide, 2023). The persistent dearth of Black physicians creates an urgent need to understand and address systemic racism along the medical pipeline.
Prior studies have shown a link between racial concordance in the physician-patient relationship and increased trust as well as improved quality of care (Jetty et al., 2021; Wilson, 2022). More recent evidence suggests that a greater Black primary care physician workforce is associated with improved population health measures (e.g., survival-related outcomes) for Black individuals (Snyder et al., 2023). Additionally, physicians of color are more likely to care for disadvantaged and racialized patient populations, which is key to ameliorating long-standing racial health disparities (Marrast et al., 2014; Xierali & Nivet, 2018). However, the historical legacy of racism undermines who accesses and thrives in medicine as a career path. This legacy is associated with a number of historical factors, including events such as the publication of the 1910 Flexner report, which recommended US medical schools to emulate the European standard of medicine – one which prioritized lab and scientific training over experiential practice with patients, which led to the near erasure of historically Black medical schools (Hlavinka, 2020; Nguemeni Tiako et al., 2022, p. 2259; Ufomata et al., 2021). Further, Nguemeni Tiako et al. (2022, p. 2259) describe medical schools as a “racialized organization” whose processes “privilege certain racial groups at the expense of others.” These authors explain that “race-neutral processes and structures within medical education…may reproduce and sustain racial inequality among medical trainees” (Nguemeni Tiako et al., 2022, p. 2259), undermining the success of aspiring Black physicians. In this way, the meanings “encoded” in race effectively provide a “template for organizational action,” which systematically weakens the career prospects, outcomes, and well-being of Black physicians (Nguemeni Tiako et al., 2022, p. 2259).
Prior literature sheds light on the experience of pursuing medicine in a racialized organization. A study on Black and underrepresented medical residents revealed their experience is impacted by implicit and explicit racist encounters such as being mistaken for custodial staff by other clinical staff; the burden of being tasked to serve as “racial/ethnic ambassadors”; lack of mentorship and social support; inequitable performance standards and access to career advancement opportunities; and feeling stigmatized, “out of place,” and a low sense of belonging (Blanchard et al., 2022; Clayborne, 2022; Nguemeni Tiako et al., 2022). A study by Pololi et al. (2010) cites similar themes in the experience of being an underrepresented minority among academic medical faculty, including the experience of feeling isolated and invisible; lack of mentoring and role models; overt and covert bias and discrimination such as being stereotyped as uneducated; differential performance standards; being labeled as an “affirmative action or diversity hire”; and inequitable access to career advancement opportunities for leadership roles. Previous studies also found a negative influence of these experiences on the mental health and well-being of Black physicians and the decision to stay in the medical profession (Serafini et al., 2020; Williams & Cooper, 2023).
The adverse outcomes of this experience may be in part tied to the duality of both being a witness to systemic racism towards Black patients and staff members and a recipient of racism. Blanchard et al. (2022) describe this phenomenon as a “double consciousness,” a term coined by W.E.B Du Bois who first characterized it as a “sense of always looking at one’s self through the eyes of others, of measuring one’s soul by the tape of a world that looks on in amused contempt and pity” (Du Bois, 1897, p. 195). Blanchard et al. (2022, p. 968) used it to explain how Black physicians are “both providers of health care in a racist system and targets of this same racism.” This experience deserves critical scholarly inquiry as it serves to elucidate the influence of racism in US medicine and inform anti-racist action toward a more diverse physician workforce. We conducted a qualitative study, drawing on the tradition of hermeneutic phenomenology to examine the lived experiences of Black primary care physicians and their perspectives on issues surrounding race, racism, and inequity in US medicine. To our knowledge, this is the first hermeneutic phenomenology study to center and understand the lived experiences of Black primary care physicians in the US.
Methods
Design
To center and understand the experiences and perspectives of Black primary care physicians, we adopted the qualitative tradition of “phenomenology,” defined as “an approach to research that seeks to describe the essence of a phenomenon by exploring it from the perspective of those who have experienced it” (Neubauer et al., 2019, p. 91). The purpose of phenomenology is to study an individual’s experience of the world by examining it as it is subjectively lived (van Manen, 1997). The essence of the phenomenon we sought out to investigate was the lived experience of becoming and being a Black primary care physician in the US.
There is a broad set of phenomenological traditions, at least seven, rooted in different schools of philosophy; they each share the concept of studying the way we perceive and understand phenomena, an individual’s lived experience in the world but vary slightly in their approach to conceiving the contents of human experience (i.e., what was experienced and how) (Neubauer et al., 2019). The term “lived experience” (rather than “experience” alone) is used to describe how the person and the world are “co-constructed” that is, people are shaped by the world and are also actively constructing the world through their perceptions of everyday life contexts (Racher & Robinson, 2003). Among two common approaches to phenomenology, transcendental and hermeneutic, we selected the hermeneutic approach to phenomenology because of its emphasis on the lived experience being an interpretive process by both the individual experiencing it and the researcher observing it. In contrast, transcendental (sometimes referred to as “descriptive”) phenomenology defines the role of the researcher as a bias-free observer whose goal is to discover the “universal essences” of phenomenon by suspending his/her attitudes, beliefs, biases, previous understandings and knowledge, so they do not influence the object of study for example, theoretical knowledge, personal views and experiences of the researcher, etc. (Moustakas, 1994; Polkinghorne, 1989). The process of setting aside or “neutralizing” one’s personal background and knowledge is called “bracketing” (Moustakas, 1994; Polkinghorne, 1989).
The hermeneutic approach embraces the researcher’s subjectivity under the epistemological assumption that they cannot “bracket” off their personal experiences, and that their interpretation of the world is derived from their personal history and background (van Manen, 1997). With that acknowledgement, the goal of the researcher is to stay aware of how their experiences may inform data analysis. This means that rather than pushing their experiences aside in effort to reach a state of objectivity, the researcher should value them as the impetus for what drew them to a research question worthy of investigation in the first place. The analytical process then consists of iterative cycles of interpreting the data while simultaneously reflecting on one’s own experience and its influence on that interpretation. This tradition is aligned with the intent of the research question and allows the lead author to access her personal background as an individual who identifies as a woman of color of North African descent. In addition, several co-authors identify as Black and one as a Black physician.
Site and Participant Selection
We used purposeful sampling, specifically, chain referral sampling (also referred to as “snowball sampling) (Palinkas et al., 2015) of Black primary care physicians in the contiguous states. This sampling technique was used to maximize successful recruitment due to the low representation of Black physicians in the physician workforce relative to other racial groups and the difficulty recruiting primary care physicians due to time constraints of practicing physicians. The eligibility criteria consisted of physicians who identify as Black or African American who are currently practicing or have been in practice within the past 5 years in a primary care specialty, including internal medicine, family medicine, pediatrics, geriatrics, and obstetrics and gynecology. These criteria included primary care residents and retired physicians who have been in clinical practice within the past 5 years.
This sampling strategy was initiated through email outreach to physician contacts within the networks of the research team. This outreach led to the first few eligible participants. The nature of snowball sampling was explained at the conclusion of each interview until a point of confidence was reached around the researcher’s ability to convey a coherent story about the lived experience.
This study has been reviewed and approved by the George Mason University Office of Research Integrity and Assurance on August 17, 2023.
Data Collection
In-depth, semi-structured one-on-one virtual interviews of 60-min duration, using Microsoft Teams, were conducted. The lead author conducted the interviews in an enclosed space in which only she and the participant could be heard to ensure privacy and confidentiality. The virtual format was used to increase the convenience of participating given the time demands on physicians as noted earlier. To collect sociodemographic data on the participants, we developed and distributed an online pre-interview questionnaire using Qualtrics via email prior to the interview. Informed consent also took place prior to the interviews. Participants who completed the interview received a monetary incentive of $100 in the form of a digital gift card as compensation for their time. Participants were also offered the option to request their transcript for the opportunity to review and retract any part of it.
The lead author facilitated the interviews using a semi-structured interview guide, which consisted of questions on the following topics: the motivation to and experience of pursuing medicine and primary care; the day-to-day experience of caring for patients; the patient population characteristics; the experience of being Black in a historically, predominantly White professional field and of potential experiences/encounters with racism, implicit/explicit biases, and the feeling of double consciousness; perspectives on the medical education curriculum; and anti-racist suggestions for increasing inclusivity in medicine and building a pipeline of Black physicians. See Supplemental Appendix 1 titled “Semi-structured Interview Guide” for the list of questions.
The interview guide was reviewed by two researcher team members, a physician and a subject matter expert, respectively, who both identify as a Black woman, in addition to two other research team members with expertise in qualitative research.
Unlike other qualitative methods, reaching saturation (i.e., significant reoccurrence or redundance in concepts, arguments, and sentiments captured) is not the measure for when to conclude recruitment in hermeneutic phenomenology as one cannot “uncover” all meanings in a phenomenon and the process of understanding does not reach completion (Smith et al., 2009, p. 51; van Manen, 1997). A “final” interpretation about the lived experience is not achievable given that it will change over time by both the participant experiencing it and the researcher interpreting it (Alsaigh & Coyne, 2021). Likewise, the goal of producing generalizable knowledge is also not conducive to the intent of this tradition. Rather, the “stopping point” for data collection is when the researcher can produce a clear description of the phenomenon under study (Alsaigh & Coyne, 2021) – in this case, the experience of being a Black primary care physician. On that basis, the research team concluded that confidence to convey this experience was reached at 18 participants.
Data Analysis
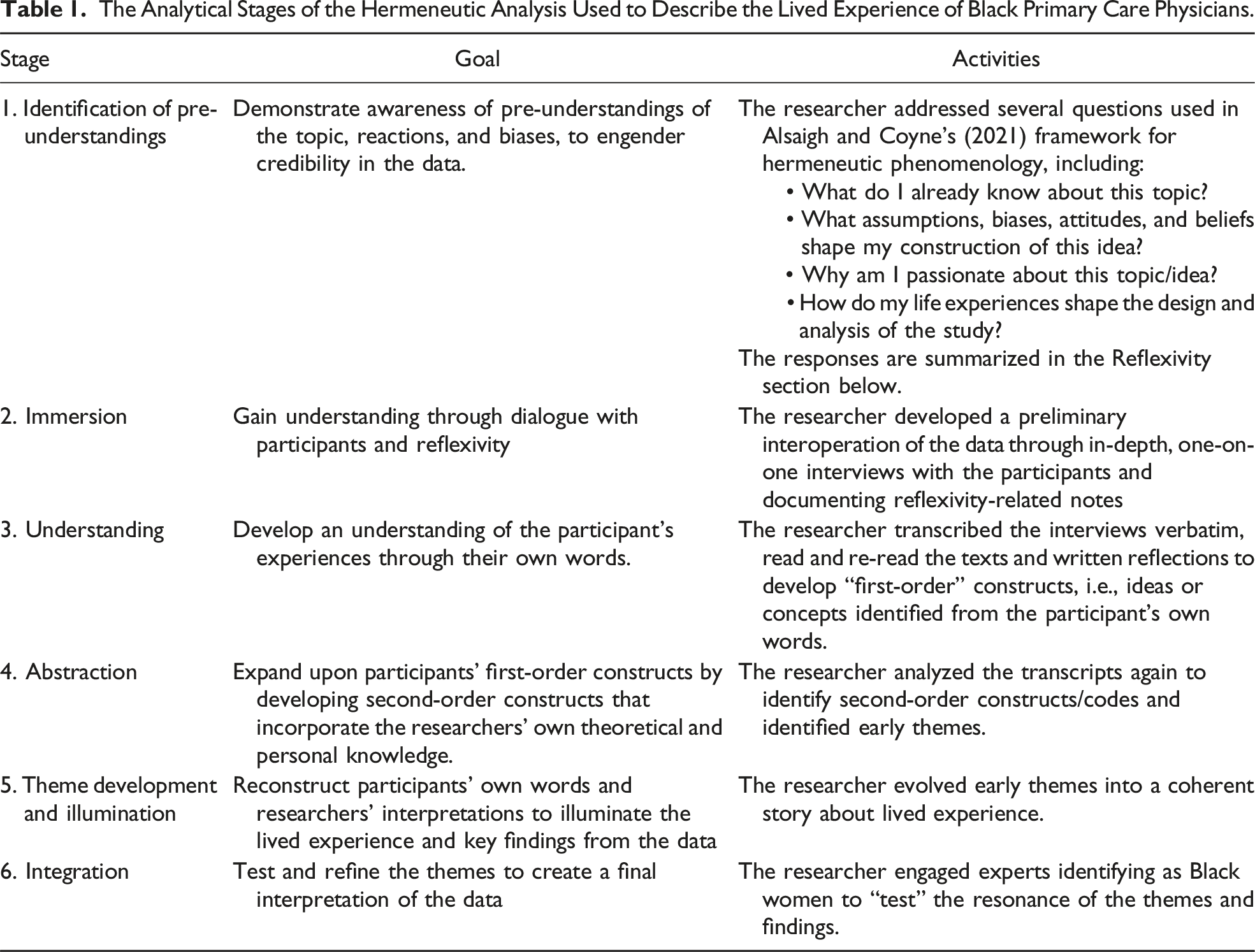
Our data analysis approach was adapted from Alsaigh and Coyne’s (2021) and Bynum et al.’s (2019) description of hermeneutical phenomenology stages. Alsaigh and Coyne (2021) provide a framework for applying Gadamer’s version of hermeneutics based on Fleming et al.’s (2003) explication. Similarly, Bynum et al. (2019) provide a detailed description of stages of hermeneutic analysis.
The Analytical Stages of the Hermeneutic Analysis Used to Describe the Lived Experience of Black Primary Care Physicians.
Reflexivity
As conveyed above, the lead author engaged in reflexivity throughout several stages of the analysis to remain cognizant of how her overlapping experiences, perceptions, and potential biases influence the interpretation of the participant’s feedback. As such, she acknowledges that her personal history and racial identity shaped her interest in understanding the experience of being at the “margin.” The lead author also has an extensive theoretical knowledge base on concepts and contemporary issues surrounding race and racism.
The lead author, therefore, brings a perspective shaped by empathy and experience, and a depth of related background knowledge. This background introduces potential biases in interpreting the lived experience of being a Black primary care physician. The hermeneutic phenomenology tradition does not agree with the “bracketing” of one’s personal background (i.e., divorcing personal beliefs and priori assumptions) from the interpretation of data. To ensure that the interpretation of the data is reflective of individual lived experiences, the lead author engaged two members of the research team – one who identifies as Black woman physician and another who identifies as a Black woman with professional experiences in predominantly White institutions (PWIs), including academia. Their input during the process aided in affirming or clarifying interpretations that are consistent or inconsistent with the experience of identifying as Black in medicine and predominately White institutions (PWIs).
Results
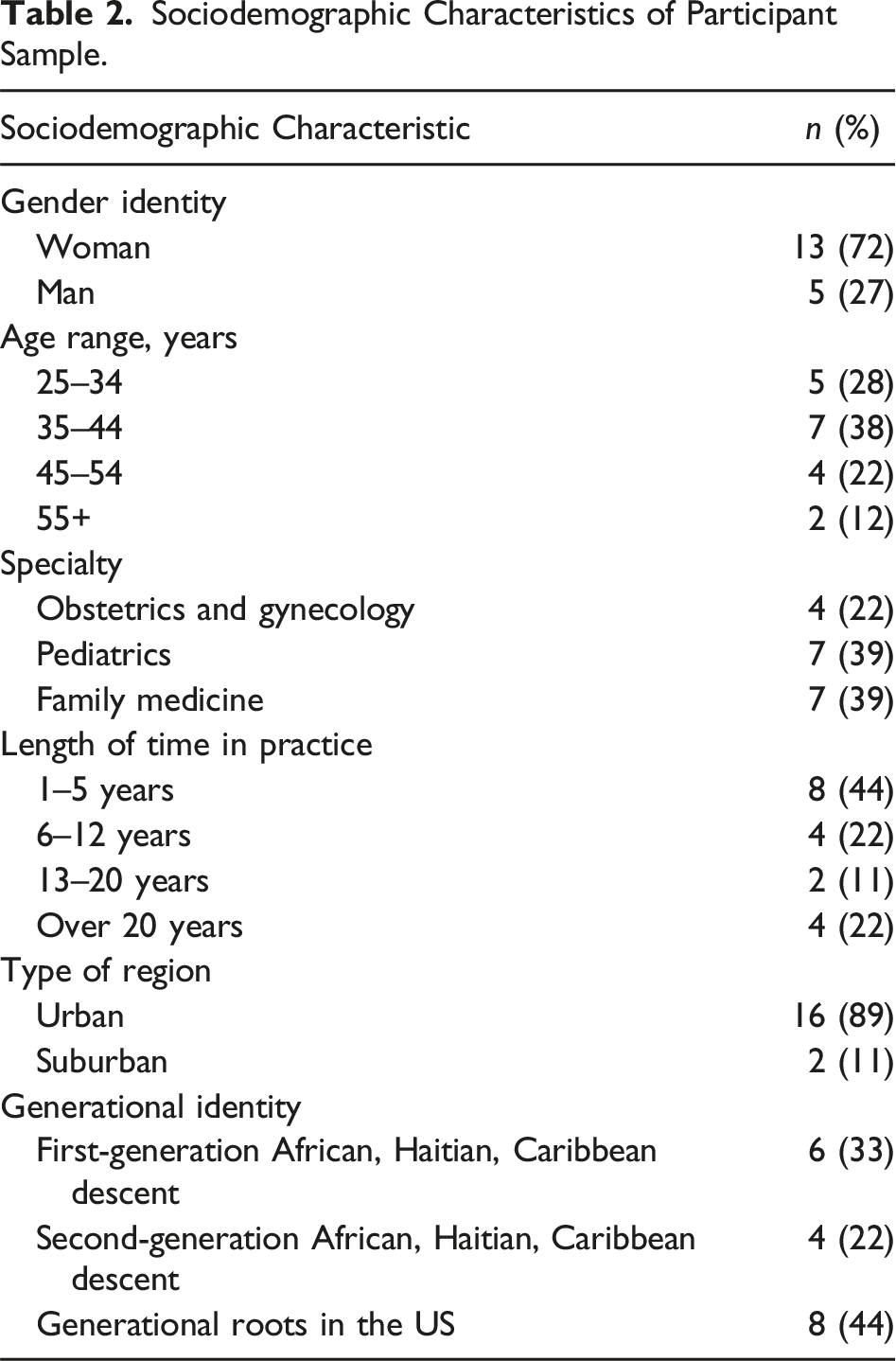
Sociodemographic Characteristics of Participant Sample.
The data analysis informed a description of the lived experience across the journey of pursuing and practicing medicine. This description consists of five overarching themes related to the experience of selecting primary care as a professional goal, the experience of practicing primary care in a clinical setting, the experience of double consciousness, and perspectives on anti-racist actions to reconcile with the legacy of racism in medicine, as follows.
Choosing the Path – The Call to Serve the Underserved
When asked to describe one’s motivation to pursue the path of becoming a primary care physician, all participants described early instances of encountering people or the health care system that instilled a drive to serve underserved populations. Several participants described either a negative or positive experience with physicians at an early age that became a motivating factor to pursue medicine later in life and pursue primary care, more specifically. And you know, my doctor growing up was also a family medicine doctor, and it was the same doctor as my parents for a long time. So this one doctor cared for all of us. And you know, that’s the doctor that I had in my mind that I wanted to be. And then going through the process of medical school, there were really no other specialties that spoke more to my inner passions, and my desire for advocacy, that really drove me to family medicine to do things a little upstream than the clinic environment.
Participants honored this intrinsic motivation to serve in that capacity despite coming to understand that this desire is not valued or perceived as “worthy” in the culture of medicine, with other specialties (e.g., surgery) perceived as more lucrative, competitive, or prestigious. However, several participants noted that they had a lot of clarity in their pursuit of primary care given their knowledge of the systemic factors influencing the health of underserved communities. They shared that they valued the “continuity of care” in primary care, building long-term relationships with patients, and the ability to serve as “advocates” and use their positions to seek out necessary resources and care for their patients. Several participants noted that this dissonance between this internal call and the culture of medicine became a source of alienation and at times created a lack of belongness among their peers. I felt like if I do medicine, I really want to work with the underserved and so that led me to [Medical school name retracted]. I felt like [Medical school name retracted] was the only medical school that was very clear about and their push for primary care. Literally, our model is service to all mankind basically and to serve the underserved. And that really spoke to me. Being there, you absolutely saw it. And so I ultimately feel like I have one of the greatest privileges in medicine to be able to not only bring life into this world, but to also advocate for women and birthing people. I really, really love the continuity of care with my patients and the broader things that I get to do.
Participants’ desire to serve the underserved was evidenced by their explanations of their patient population characteristics. Many participants discussed spending most of their careers serving low-income and socially disadvantaged communities. Several participants indicated that most of their patients are publicly insured with the majority being immigrant and Spanish speaking individuals as well as African American patients. Some added characteristics of the surrounding community for example, how their patients live in food deserts, and many are from single-parent households. Examples of settings that participants worked in included school-based settings, federally qualified health centers, public hospitals, etc. So, I actually work in a care setting that predominantly serves African American and immigrant populations, usually from South America and Central America, for our immigrant populations and African American populations, because I work in a city hospital where people who are usually underinsured or not insured. So currently I’m at the [descriptor retracted] clinic which is in [city name retracted] and is predominantly under-resourced, underserved patients overall, but probably Hispanic, largely immigrant, otherwise predominantly Mexican. There’s also a fair amount of other immigrants, a variety of Asian cultures, so Korean, Vietnamese, Taiwanese, some Cambodian and then you know, some Caucasian patients as well as Black.
Pursuing Medicine – Do you Really Want to Become a Doctor?
In recollecting the process of learning about the path to and pursuing a medical career, participants often indicated that their experience with being racialized became more apparent and a larger part of their lived experience than their previous academic career in grade school through college. Several participants indicated that in simply trying to learn about the process and consulting with academic advisors or educators, or in expressing their interest/intent to go to medical school, the reaction received was characterized as one of questioning or doubting the participant’s capability – a reaction perceived as racially prejudiced. Several participants provided examples of these types of comments for example, hearing that they should consider other paths such as social work, nursing, physician assistant, etc., and being asked if they really wanted to become a doctor. It started as early as when I decided that I wanted to pursue medicine. Just people’s questions or assumptions or judgments about if this was a path that I could actually achieve, and this was regardless of their knowledge of how I did in school or what I could accomplish. They questioned, you know, if I should actually try to be a doctor? Or maybe consider doing nursing or being a physician assistant instead.
Once in medical school, participants recalled encountering racist incidents in the classroom environment with both students and faculty. Participants shared sentiments of disappointment over how these incidents were or were not handled. Examples of comments and interactions included a student using the N-word, students asking or assuming that the participant was accepted into medical school in a non-meritocratic way such as through affirmative action or special diversity programs, and students openly talking about Black people or communities in an insensitive way.
In addition, participants relayed that they felt that they were constantly scrutinized, doubted, and judged to be less competent, and that this experience was heightened through certain microaggressions and interactions that left underlying racist messages. I think my first interaction, I actually just shared this with the mentee yesterday about a professor I had a question in anatomy and I asked if I could stay after lecture and the professor responded, “I’m happy to answer any questions, I’m always helping the Black students”, and so I, you know, I was certainly taken aback, but I was hearing from that professor that Black students always needed help and that he did not regard the Black students to be having, whether it’s the same intellectual capacity or the same success as other students that weren’t Black.
Practicing Medicine – Where is the “Real” Doctor?
In the context of clinical practice, participant comments demonstrated that forms of racism, including interpersonal racism and systemic racism are ubiquitous and part of the day-to-day experience of being a Black primary care physician. These instances of racism were not concentrated early in residency, but rather, followed participants throughout their careers in medicine from training to senior roles. A common experience relayed as an obvious expression of racial bias is the experience of being asked if the Black physician is indeed the physician and provider of care for a patient/family, confusing them as a nurse or other clinical or non-clinical staff member. Participants communicated that this confusion has frequently occurred across their journey from training to becoming an experienced physician and it occurs despite wearing a white coat and a badge with their name and credentials, and explicitly introducing themselves as a medical doctor. This persistent form of explicit bias may come from patients and their families or caregivers, and other staff and colleagues in the health care setting. So people always confuse me as the nurse or nursing student. And I’m like, I literally just did your surgery 2 seconds ago. I am the surgeon. You know, I mean, I still have supervising, you know, privileges, but I literally do this people’s surgery by myself. And people still think so. I’m like is that because I’m a Black? Is that because I’m a woman?… I definitely still get mistaken for nurses or something like that, particularly when I work in urgent care. Because that’s different economic statuses, so if I’m just providing just regular routine care and I will I find myself sometimes, particularly if there’s a man like a White man in the room, I mean, I get interrupted when I’m trying to explain something, there is a kind of an attitude of arrogance that that they have and almost resentment of the fact that I’m in there providing information, that I am in that capacity…but I refused to, you know, let it determine how I’m going to behave and certainly not how I’m going to treat the kid. That’s really what it’s all about. I definitely had times where I would come into a room and introduce myself as Doctor [last name retracted] and people would make comments of ‘ohh, so when is the doctor coming in?’ and I would say I am the doctor, or they would say ‘ohh nurse, you know, when am I going to see the doctor?’
Several other experiences of racism were recounted by participants – these are experiences that altogether define the Black experience in medicine as one of being an “outsider” or “foreigner” in a system in which they have dedicated extensive amounts of time and training in service of others. Participant comments revealed that these racialized experiences include instances of patients both White and non-White rejecting the care of Black physicians and requesting White physicians; encountering racist attacks from patients; and experiencing racially biased behavior from staff reporting up to the physician for example, nurses who question or challenge the authority and direction of the physician. The funny thing is, I think still, there’s a perception that White is better. I mean, I think this is just, you know, in our world period, but you know there’s still that innate, we’re all kind of taught subconsciously that there might be something more that they have so and I’m like, well, you know, I actually would have empathized with you more than this other person who is lovely person as well…But the patient was like no, no, I want to, you know, see, the White doctor. So, you know, I mean, I had to just kind of you know let that one go. So, I feel there are those kind of perceptions even amongst our patients, they want to be seen at the White Clinic… I think what bothers you anymore is the ancillary staff, because I’m technically in a role that is more senior to you and I give the orders. And so, I, as part of my role, I feel like they should be more accommodating and you find they’re more likely to question you as a Black woman, question your decision making about the patient. There are times you know, you can be wrong and maybe call the wrong thing, but they’re more likely to push back with women who look like me versus other women who don’t look like me.
A more insidious or subtle experience shared was one of perceiving disparate performance and professionalism standards that are unreasonable and unrealistic to meet and as such, suggest either conscious or unconscious racial bias towards Black residents and physicians. Similarly, several participants shared how they are stereotyped or “boxed” into a certain persona due to biased assumptions around what Black people are like – examples including withholding small talk on certain topics that White people perceive to be foreign to Black people for example, certain sports, or music genres, and selectively talking about things that may be considered a part of “Black culture.” So, I came in at an early time, but not super early. Basically, he texted me while I was maybe 15 minutes away and he was like, I’ll meet you in five like 5 to 10 minutes and I need this, this, this…. And I was like, OK, well, I’m not even there. I don’t know this. You know, I don’t know this hospital. I don’t know where to find all of those things that you need you get, and I didn’t know I was rounding with you, so I don’t even know what your case list is like. I don’t know who your patients are. I’m very unprepared for this. Basically umm…long story short, I got yelled at in front of everybody, and I was told I was not contributing to the team and I needed to be more useful. And I think this is my second week…I didn’t even have EMR access…. they should have been more understanding and that is no way to speak to someone…
Navigating “Double Consciousness” – Seeing and Experiencing Racism Simultaneously
The racialized experiences described above are of the Black physician being a recipient of racism. As providers of care, participants discussed the duality of witnessing and interrupting racism as they care for patients and the effect that this “double consciousness” has on how they navigate their environments. This witnessing of racism includes seeing both the effects of interpersonal racism between other staff and Black patients and systemic racism on their patient population. In this context, the participant’s role became one of advocacy and education to interrupt racially biased behavior for example, using different language with Black patients and other racialized patients, providing a potentially disparate standard of care; and serving as an example of delivering “structurally competent” care (i.e., recognizing the upstream factors that lead to downstream health outcomes). … So if we’re looking at pediatrics and we’re looking at BMI and we might have concern for child being overweight or obese, right, the conversations you know is that we immediately look to or the child’s, you know, not getting nourished or the mom only cooks this type of food. But we’re not thinking about food insecurity, right as an extension of poverty rate, and because it’s families growing up in a low wealth income, we’re immediately questioning the parents understanding of nutrition, right? But not understanding that this might be, you know, the only approach or a food resource or nutrition. So I see that commonly and I’m always having to correct and say, what did we ask first? Are we making a presumption, but that presumption is built on biases that for some have become the norm. Difficult is more used…. It’s, well, you never asked, you’re saying ‘ohh she well she never gets her medication’. Did you ask her? Did she have a car to get it? Did you ask her? Did you ask her if she has the money to pay for it?
Participant comments lent themselves to some insight on the complexity of navigating both seeing and experiencing racism simultaneously. This complexity is shaped by the day-to-day need to advocate and defend both oneself and others against racism, and the need to modify and over-regulate one’s thinking and behavior to participate in an environment which constantly signals who belongs and who does not. The comment below conveys the nature of trying to shield oneself from racist stereotypes and biases in order to continue positioning oneself as an advocate for Black patients and individuals who may be on the receiving end of that same racism. I mean literally, literally I’ve seen, I’ve seen physicians throw bloody gloves across the room, yelling the F bomb or whatever. But if I say listen, it wasn’t appropriate for you to call at 2:00 o’clock in the morning to ask me if the dose of Tylenol was correct, in that case, I was really, very aggressive. So, I honestly have to make sure that I say that in a way that’s not considered aggressive. So how can I defend and advocate for my patients in a way that I ensure their heard without then also suffering the angry Black woman myth? And how do I show up in the world for myself? It’s a very interesting dance. And how do you do the dance? Because it is a dance. How you do the dance can impact how effective you are or how your messages are received or not received.
Participants described several additional examples of the effects of double consciousness, including the need to over-exert oneself and work twice as hard to be considered equal to their White counterparts, and overanalyze the intentions and behaviors of others to understand whether to attribute potential biases to racism. Several participants also mentioned the effect of the “minority tax” in needing to play an outsized role in participating in diversity-related efforts to help create a more inclusive space for Black physicians and individuals.
Moving Towards an Anti-Racist Agenda in US Medicine – Centering Black Primary Care Physician Perspectives
Participants reflected on actions to move towards an anti-racist approach to medicine – these perspectives largely centered on two major domains: (1) informing anti-racist pedagogy in medical education, and (2) improving efforts to build a pipeline of Black physicians.
Addressing Limitations of Medical Education
All participants conveyed that longstanding issues exist with the way they were taught and the way that current students learn about race and racism. The overarching model of educating on these issues is still to pathologize race as a risk factor for disease and a determinant of genetics—that is, medical education reifies race as a biological rather than a social construct. I think we are studying for all of our exams and you’re going through, you know, the bank of questions and you’re just pounding through them, you’re just going through a ton of questions and you start to find patterns…certain ethnicities are always the same type of cases., it’ll be COPD or it’ll be at type 2 diabetes, you know, with an annotation situation…it’ll be pretty consistently the same types of things. I mean, not just for Black. I mean, we’ll see it for Latinx as well, too…. So, I definitely think that’s part of the training.
Participants urged revision to the curriculum consistent with findings from the Ghanem et al. (2024) study with Black women medical students, including to provide the historical context behind present-day racial disparities, and ensure that components of the curriculum are mandatory, evaluated, and longitudinal. Participants further stressed that extending and embedding this content into practice across a physician’s career is necessary to facilitating one’s unlearning related to racial biases and learning of structural competence, as explained in the following comment. So you know, I think it doesn’t just stop with medical school because medical school is 4 years out of a you know, 60-year career. However, when people stay in medicine, there definitely needs to be some ongoing, you know integration so that when you’re really out in practice, you know how to practically apply and implement the tools that you’re learning, realizing this is a big one that you know, there needs to be a humility to keep learning.
Building a Pipeline of Black Physicians
Participants overwhelmingly voiced that a critical step to addressing the sparse numbers of active physicians in the physician workforce is to devote resources to pipeline efforts which expose young Black individuals to the profession at an early age, starting in kindergarten when one starts to become aware of their racialized identity. Participants emphasized that one cannot aspire towards a profession if they don’t see themselves represented and that repeated exposure to Black physicians’ overtime is essential to inspiring ambition to become one. In addition to exposure, participants suggested that these efforts should incorporate long-term mentorship, and Science, Technology, Engineering, Mathematics (STEM) programming. It should start in kindergarten, which is when most children start to identify or realize the difference is based on race and so you know programs that like that give that additional support and mentorship and that is focused on marginalized children, Black children, children of color, to give them a healthy sense of self. Because at every stage you see, people drop out, right…So, every and every step of the career there needs to be mentorship. I know specifically since I came to the US and definitely since I started my practice, had I not had mentorship from other Black male physicians, I would not have been given certain opportunities… A lot of these STEM program start in high school, but it’s kind of too late by then, sometimes people already think that they can’t do math or they’re not good at science, they’ve been kind of counted out or they’ve counted themselves out, you know, pretty early on. So to make a shorter answer extending the pathway to consider, younger exposure and you know all the way up through supporting residents, supporting Black physicians along each step of the path is really crucial… If a group of professionals are routinely brought into the classroom who look like the students, they’re going to see that at an early age. You begin to believe that you can own a company. You can run a business because you’ve seen folks who’ve done it. Each and every day, because you might not see it at home, but you’re in school all the time, more than you’re at home… It sounds kind of unfair. I saw it every day. But some kids don’t. And if you don’t see it, if you don’t see someone who’s doing it, who looks like you. Oftentimes, because we’re in such a negative racist environment, I don’t think a child would think they could do it either…so I think if we started earlier with that whole introduction of kids seeing adults doing some wonderful, great and positive things.
Several participants added that structural barriers disadvantaging Black and other racialized individuals need to be addressed. These include the financial cost to attend medical school, the over-reliance on standardized exams, and the lack of access to certain resources. With regard to the latter, participants alluded to how there exists a “selection effect” among Black individuals due to structural racism that is, only Black/African American individuals with greater access to resources (both material and immaterial) along the path will apply to medical school and succeed throughout the process. A few participants indicated that this reality disadvantages individuals with generational ties in the US relative to first- or second-generation African Americans and as a result, this group is an even smaller minority (a “minority within a minority”) within the physician workforce. I tell you my path because it’s important coming from a place where I never felt restricted. When you look at the Black physicians, it is a lot of Caribbean American, African Americans coming from other places…what does the pipeline look like?…To truly ask where are the Black American physicians and what those numbers look like, I don’t I think it’s easy to say, and it’s not accurate to say that we have 5% Black physicians, my friends are literally Caribbean African. The diaspora is heavier in medicine relative to Black Americans who come from the US.
Please see the Appendix for additional participant quotes by theme in Table 4 titled “Illustrative Participant Quotes by Theme.”
Discussion
This phenomenological inquiry fills a gap in the literature by uncovering the ubiquitous and consuming nature of implicit and explicit racial biases experienced by Black primary care physicians in the US. The experience of being a Black primary care physician is one that creates a heavy psychological toll and further validates prior evidence from Blanchard et al. (2022), Clayborne (2022), Clayborne et al. (2021), Nguemeni Tiako et al. (2022), and Pololi et al. (2010), who identify the ways that medicine as a racialized institution disadvantages Black and other racialized individuals and is characterized by an exclusionary culture that otherizes Black physicians as “outsiders” and “foreigners.” Black primary care physicians experience layers of de-valuing; they are performing a critical service for underserved and marginalized communities within a specialty that is de-valued and under-compensated relative to other specialties while being simultaneously de-valued on the basis of their skin color.
Within this state of “less than,” Black primary care physicians must contend with the duality of being both an observer and recipient of racism and learn a delicate balance of being a defender and educator against racism while not potentially behaving in a way which may confirm a racial stereotype or make them a target of racial biases among their peers and patients. The latter creates the risk of undermining their credibility and longevity in the profession and their personal mission of giving back to communities in most need of their care. This experience of double consciousness creates added stressors associated with constantly being evaluated and targeted on the basis of one’s race and acting as an educator and advocate for other racialized individuals to ensure that their care experience meets a standard of care and is not negatively impacted by the racial biases of other health care professionals. The stress of this experience is likely to contribute to a low sense of belonging, feelings of being isolated and invisible, and poorer mental well-being as Pololi et al. (2010) found in the context of underrepresented academic medicine faculty.
The understanding of this experience lends itself to several insights. First, the historical legacy of slavery and racism in this country permeates medicine through the assigning of biological meaning to race in fluid ways as Byng (2012) explains, where racism is reproduced at various levels and operates independent of individual prejudices or individual intentions. The meanings encoded in race shape every aspect of medicine, including what is taught; who is taught in medical education; and who is represented, included, and accepted in the physician workforce. Second, this experience calls for a need for comprehensive anti-racist actions along the continuum of education to practice – the perspectives of Black primary care physicians conveyed in this study offer a starting point. Third, the systemic nature of racism cannot be solved within the walls of the medical system, and a broader, societal consciousness around these issues is needed to address the structural factors which contribute to inequities across racial lines. Overall, the lived experience, and perspectives on anti-racist change inform several recommendations that the medical community can act upon, to move toward changing the face of medicine and reconciling its enduring legacy of racism (1) Medical education stakeholders (educators, administrators, and accrediting bodies) should evaluate or add new content related to race, racism, and racial disparities to educate students on the historical context behind disparities, correct the conflation of race as a biological construct, and develop structural competency in future physicians. The Ghanem et al. (2024) study centering Black women medical student perspectives on anti-racist reform in medical education provides new guidance to act on this recommendation. Similarly, health care organizations should engage in continuous learning and unlearning around the use of race in practice. (2) Health care organizations should foster a culture of accountability over discriminatory behavior and unfair norms or standards towards Black and other racialized individuals. This includes creating an environment where physicians feel empowered to openly discuss and confront these behaviors without fear of consequence. (3) To address the dearth of Black physicians and the declining proportion of Black men physicians, medical education, community, and diversity-focused organizations should learn from exemplar efforts to expose young Black individuals to Black physicians starting in grade school. This includes investing resources in long-term mentorship programs, preparatory STEM and standardized exam programming. This study encourages the organizations to further explore ways to address the unique barriers that Black individuals with generational roots in the US face to pursuing medicine. (4) Lastly, the medical community, including medical education and health care organizations, should look to evidence-based strategies to create inclusive climates, for example, designing and implementing implicit bias interventions shown to produce positive effects. Key features of these interventions include communicating positive messages about inclusive behaviors, integrating skill-building tasks to practice mitigating bias, and using real-world case studies to facilitate learning (National Institutes of Health [NIH], 2021).
As noted earlier, this study agrees with existing literature examining the experience of underrepresented physicians and adds to this literature by illuminating the lived experience of being Black in primary care, specifically, from the point of identifying the aspiration to serve underserved populations to practicing medicine and navigating double consciousness. The results of this study also strengthen existing literature on long-standing limitations of medical school curricula and emphasize the need for anti-racist pedagogy. To our knowledge, this is the first hermeneutic phenomenology study to examine the lived experiences of Black primary care physicians in the US and to center their perspectives on actions to address the effects of systemic racism in medicine.
Implications for Policy and Practice
The significance of primary care to the nation’s health system cannot be overstated. Primary care is often the first contact a patient will have with health care workers, and it has been shown to improve population health outcomes, preventing illnesses and injuries from becoming severe and difficult to treat (National Center for Health Workforce Analysis [NCHWA], 2024). Over the past few years, challenges in the primary care workforce have been well-documented. These challenges include a shortage of primary care providers, geographic maldistribution of providers, high rates of burnout, lower compensation relative to other specialties, and a changing demographic (NCHWA, 2024). With regard to the latter, the proportion of minority patients is expected to increase by around 10% from 2020 to 2060, yet the racial makeup of the workforce remains mostly non-Hispanic White across all subspecialties (NCHWA, 2024).
As noted earlier, racial concordance between physicians and patients is associated with improved trust and quality of care (Jetty et al., 2021) and areas with a higher percentage of Black practitioners are linked to higher life expectancy among Black individuals (Snyder et al., 2023). The primary care community should use the results of this study to inform actions towards cultivating a physician workforce that is as diverse as the nation’s population and inclusive of Black individuals. The lived experiences brought to light in this study demonstrate that Black primary care physicians are intrinsically motivated to serve underserved and minoritized communities and are especially empathetic and sensitive to the ways in which structural factors affect health outcomes in disproportionate ways. The US health system will benefit from their increased entry into and inclusion in the primary care workforce – the recommendations offered in this study provide an impetus for action.
Limitations
Though this study has several strengths, there are limitations worth noting. This study is not generalizable or representative of the Black or African American primary care physician population, though this is not the intent of phenomenology.
Conclusions
This study provides insight into the day-to-day lived experience of being a Black primary care physician and the complexity of the double consciousness that shapes it. We hope this study promotes greater awareness and empathy for Black and racialized individuals and an urgency to participate in anti-racist actions in medicine.
This study inspires several areas of future inquiry. First, the sociodemographic characteristics of the participants reflects that Black individuals in medicine with generational ties in the US are a smaller minority as compared to individuals with first or second-generation immigrant backgrounds. Comparative studies focusing on the within-group differences in experiences and perspectives would advance an understanding of racism and anti-racism along the continuum of medical education to practice. Second, the gender disparity in our sample is reflective of a larger trend of declining Black men physicians relative to Black women. An understanding of the experience of being a Black man in medicine is worthy of future investigation.
Supplemental Material
Supplemental Material - Critical Phenomenological Inquiry on the Experiences of Black Primary Care Physicians in the US
Supplemental Material for Critical Phenomenological Inquiry on the Experiences of Black Primary Care Physicians in the US by Nouran Ghanem, Debora Goetz Goldberg, Eldesia Granger, Jennifer R. Warren, and Gilbert Gimm in Qualitative Health Research
Footnotes
Acknowledgments
The authors sincerely thank the participants for their willingness to participate and share their thoughtful and insightful perspectives.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study participant incentives were funded by the George Mason University Mentoring for Anti-Racism and Inclusive Excellence (MARIE) program.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.