
Abstract
In peasant livelihoods, families are regularly exposed to ectoparasites such as ticks, and thus to the diseases they carry. Little is known about how rural families’ knowledge influences health in domestic and community environments. We applied reflexive thematic analysis (RTA) to family preventative and curative strategies for tick exposure and bites in a Maya community in Yucatan, Mexico. Data were collected over six months via participant observation and 26 semi-structured interviews with fifteen women homemakers, five peasant farmers, three traditional healers, and three biomedical professionals. Three themes became apparent via RTA: “Socialization and normalization of tick management,” “Pragmatism and observation,” and “Women Caregivers.” A principal finding is that local participants only associated tick bites with skin ailments, which they treated at home using mostly homemade remedies, as well as some biomedical products. Based on their knowledge of and experience with ticks, their preventive strategies in the domestic sphere focused on minimizing tick contact with the skin, preventing ticks from entering the house, and protecting children. All family members contributed to implementing anti-tick strategies, using knowledge created through communal processes influenced by economic factors and experiences with similar illnesses. One biomedical professional commented that the study population’s lack of awareness about the magnitude of the disease risk from ticks is alarming, referring to tick-borne Rickettsia as a “sleeping giant.” Our findings underscore that acknowledging and understanding domestic knowledge and strategies is vital to developing programs to assist rural populations in better controlling this and other disease vectors.
Introduction
In rural societies, people with peasant livelihoods are regularly exposed to wildlife-related pathogens such as ticks. Bites from ticks and other live organisms (known as vectors) can transmit potentially deadly diseases. Due to the clear risks associated with their outdoor occupations, qualitative research on infectious diseases transmitted to humans by insect bites (known as vector-borne diseases) has focused entirely on rural, male populations (Dzul-Rosado et al., 2020; Ghane Kisomi et al., 2019). This ignores the knowledge other members of a population, such as women and children, possess about how to protect their families from vector attacks.
Domestic medicine, understood as the set of therapeutic knowledge, resources, and actions present within households, recognizes women as protagonists in their work as healers and the primary agents of health care in the family environment (Zolla-Luque & Sánchez-García, 2016). In the community sphere, mothers tend to be the main recipients of social programs, as well as the main participants in educational, health-related, and religious spaces (Arenas-Monreal et al., 2015). These experiences contribute to their role as caretakers. This female primacy in caretaking may diminish in urban settings due to greater availability of, and access to, medical services but remains significant in rural contexts.
Vector-borne diseases are a critical worldwide public health problem (Hill et al., 2005). They are contracted with greater frequency by populations in contact with wild environments and those with demonstrable gaps in social well-being (Namusisi et al., 2021). These types of diseases are responsible for more than 17% of all infectious disease cases worldwide, and more than 700,000 deaths annually (Organización Panamericana de la Salud [OPS], 2017).
Mexico’s climate, geography, ecology, and sociodemographic conditions are similar to those of other developing countries in that they foster transmission risk of many vector-borne diseases (Nava-Doctor et al., 2021). Another key proliferation factor for vector-borne diseases is lack of health care access (Hotez et al., 2015). Between 2018 and 2020, the percentage of Mexico’s population in poverty increased from 41.9% to 43.9%, while lack of access to medical services in rural areas increased from 15.3% to 32.8% (Consejo Nacional de Evaluación de la Política de Desarrollo Social, 2022).
Ticks are vectors for critical infectious diseases throughout Mexico (Hotez et al., 2015) and are associated with diseases such as rickettsiosis. The initial clinical profiles of rickettsial diseases (e.g., typhus, Rocky Mountain spotted fever, and rickettsial pox) include fever, headache, and changes in skin color and texture; they share enough similarities with more commonly known febrile illnesses like dengue as to mask and delay their diagnosis (Santamaría-Arza et al., 2018). Increased incidence of rickettsiosis poses an important social problem given that the majority of those exposed to the disease have limited knowledge, or are merely unaware, of the risks of contracting illnesses from tick bites (Álvarez-Hernández et al., 2017; Santamaría-Arza et al., 2018).
Rickettsia tick species are known to be present in wild, domestic, and peri-domestic animals in the state of Yucatan, Mexico. These animals participate in the pathogen transmission cycle in both urban and rural areas, representing a potential risk for the human population in this region (Braga-Ordóñez et al., 2016; Dzul-Rosado et al., 2017, 2021; Martínez-Ortiz et al., 2019; Panti-May et al., 2015; Peniche-Lara et al., 2015; Rodríguez-Vivas et al., 2016; Vázquez-Guerrero et al., 2023).
Zolla-Luque and Mellado (1995) emphasize the importance of understanding health-related practices performed inside the home, a place where “numerous illnesses are caught, diagnosed, treated, and eventually cured” (p. 73), without the involvement of medical specialists. A large-scale study in Mexico found that over 60% of those studied, particularly the poorest, tended to self-manage their illnesses rather than seek medical care, regardless of condition acuteness (Leyva-Flores et al., 2001). The present study objective was to analyze the preventive and curative strategies implemented by families when faced with tick exposure and bites in a Maya community in Yucatan, Mexico.
Materials and Methods
Study Design
We chose a qualitative design within the constructivist paradigm with the purpose of building a bidirectional understanding of the relationship between language and experience (Byrne, 2022). Constructivism assumes that findings are created as research advances due to continuous interaction between researchers and study participants (Guba & Lincoln, 1994). Both in-person semi-structured interviews and participant observation were done between September 2020 and January 2021. We decided to use inductive RTA to focus on the latent meaning of the data (Braun & Clarke, 2019; Braun et al., 2022) in the interviews and field notes. We present stories of participant experiences and our interpretations. Reflexive thematic analysis is characterized by the organic nature of its coding and the active role that researchers play in the analytical process (Trainor & Bundon, 2020). Initial data collection and coding was done by the first author in close dialogue with the corresponding author. Group meetings were held among all co-authors to review and discuss progress and, rather than seeking consensus, to achieve “richer interpretations of meaning” (Byrne, 2022, p. 1393). The themes generated initially were modified during this collaborative and reflexive process, maintaining internal consistency to ensure accurate data representation.
Study Area
The study was done in the municipality of Teabo, in the state of Yucatan, Mexico, located approximately 87 km (90 minutes’ drive) south-southeast from the state capital of Merida. Regional climate is subhumid warm with a 26°C average annual temperature, summer rains, and a marked dry season (Instituto Nacional de Estadística y Geografía, 2010). Of the approximately 262 km2 surface of Teabo municipality, 1.31% is urban area and 98.69% vegetal cover. Its total population in 2020 was 6921 inhabitants (49.8% men and 50.2% women), of which 97.2% was classified as indigenous. Almost 70% of the population five years of age and older speaks an indigenous language (Instituto Nacional de Estadística y Geografía, 2021). The municipality has one health center, a primary care facility for diagnosis, follow-up, and control of out-patient cases. This municipality was chosen for three reasons: (1) its inhabitants have been reported to be unaware that ticks are vectors for human diseases (Dzul-Rosado et al., 2018, 2022); (2) evidence in blood tests has shown rickettsiosis in some inhabitants (Dzul-Rosado et al., 2022, 2025); and (3) their peasant livelihoods require inhabitants to interact with wildlife far from human settlements.
Participants
We used sociodemographic data from the community health center to contact potential participants and key interlocutors. We included families in which heads of household worked in agriculture, women did domestic work, and at least one child was under the age of 15; the latter criterion was used because children younger than 12 years have been reported as more prone to severe clinical manifestations of tick-borne diseases (Dzul-Rosado, Lavín-Sánchez, et al., 2024; Dzul-Rosado, Panti-Balam, et al., 2024; Zavala-Castro et al., 2008). Using the snowball sampling technique, we invited family members to participate in the study. A total of 26 people chose to participate in the study, including fifteen mothers, five peasant farmers, three traditional healers, and three biomedical professionals. All participants were from Teabo and currently living there at the time of the study. All participants, save one biomedical professional, were Maya/Spanish bilingual. The three traditional healers were elderly: one was a woman and two were men. All three biomedical professionals were men: one was a physician, one a nurse, and one the state-wide coordinator for the Yucatan Zoonosis Program. The mothers’ median age was 34 years (range = 25–42 years), and all had children under 15 years of age (median = 2 children, range = 1–8). They generated extra household income by embroidering clothing and weaving hammocks. The peasant farmers were all men, 41 years median age (range = 36–44), and combined farming with construction work outside Teabo. Most of the non-professional participants (93.3%) were peasants engaged in agriculture, although some (6.7%) were engaged in informal business.
Data Collection
Data were collected via semi-structured interviews between September 2020 and January 2021. Due to the COVID-19 pandemic, interviews were initially conducted by telephone to protect the research team and participant health. When pandemic preventative measures were partially relaxed, we made in-person visits to the village, still following the preventive measures recommended by health authorities. We asked participants to answer questions about (a) ticks, (b) their knowledge of disease transmission, (c) their information sources, (d) dynamics and routines, and (e) treatment of tick bites and general ailments. Interviews were 50–90 minutes long. All were conducted in Spanish, except for two interviews with traditional healers for which we required local Maya–Spanish translators. Interview guides were written in colloquial language with appropriate Maya terms to ensure clarity and understanding. As part of the ethnographic method, we did rounds in the community to become familiar with it and better understand the study environment. We also engaged in participatory observation when in homes and non-participatory observation at the health center and with a traditional healer. These observations provided valuable contextual information for understanding other data, such as those from the interviews.
Study site sociopolitical conditions, and the consequences of the COVID-19 pandemic, required modification of the fieldwork plan. Informed consent was provided by participants verbally because local political pre-campaigns had begun months before the official dates and people in Teabo refused to sign any documents at this time. We only recorded interviews after receiving participant consent. All participants were fully aware that their participation was voluntary and that they were free to not answer any questions or stop participating in the study at any time. Audio recordings were made of all interviews, and these were transcribed to text documents (Word®). We took notes during participant observation, conversations, and interview audios, subsequently organizing them into a fieldwork diary. The research protocol was evaluated and approved by the bioethics committees of the two participating institutions.
Data Analysis
Using recording transcripts and fieldnotes taken during observation, we implemented RTA as a way to identify, analyze, and communicate patterns of meaning (Braun & Clarke, 2023). In RTA, researcher subjectivity is perceived as a resource to be applied in producing knowledge (Clarke & Braun, 2018). The themes identified therefore arose from the intersection between our reflexive commitment and our personal experience and theoretical knowledge.
We initially familiarized ourselves with the data by reading the transcripts; we identified key elements which became the initial codes that guided development of the main themes. Once initial manual coding was complete, we refined the codes by reviewing all the transcripts and fieldnotes, highlighting important aspects such as a silence or changes in participant tone of voice during an interview. Based on participant experiences, we generated three central themes. The first is “Socialization and normalization of tick management,” which describes how participants acquired and shared their knowledge about ticks during their lives, and is addressed in two subthemes: (a) Socialization with ticks and (b) The tick bites, the poison makes you sick. The second is “Pragmatism and observation,” which addresses how participants applied their knowledge and expertise to prevent tick bites and treat the discomfort they cause; it is divided into the subthemes of (a) Prevention and (b) Care. The third is “Women Caregivers,” which presents how women incorporate their health care experience and implement it as caregivers in their family and community.
Reflexivity
The co-authors are professionals from various institutions with scientific backgrounds and professional experience at the intersection of health, disease ecology, and cultural anthropology. All are open to dialogue and reflection. The first author is a human ecologist focused on sociocultural health practices. The second is a biological pharmaceutical chemist and pathologist specializing in rickettsial diseases. The third is an anthropologist experienced in community health and gender violence. The fourth is a biomedical scientist studying neglected diseases and biodiversity. The corresponding author is a social anthropologist interested in gender and community processes. Using a reflexive, iterative analysis, we navigated challenges like COVID-19 restrictions and early election campaigns, and adapted our fieldwork to changing conditions at a study site 90 minutes from our home base city.
Findings
Socialization and Normalization of Tick Management
Study participants understood what ticks (peech in Maya) are from an early age. They are present in their daily lives, which involves contact with wild and domestic animals. Participants and their children learned about ticks when young by listening to those who work in the fields and through their own experiences with ticks and those of their relatives. Based on the documented conversations, we found that they could identify three to five tick species, which are named in Maya based on morphological traits and the kind of place where they abound.
Socialization With Ticks
Places and Activities With Greatest Exposure to Ticks.
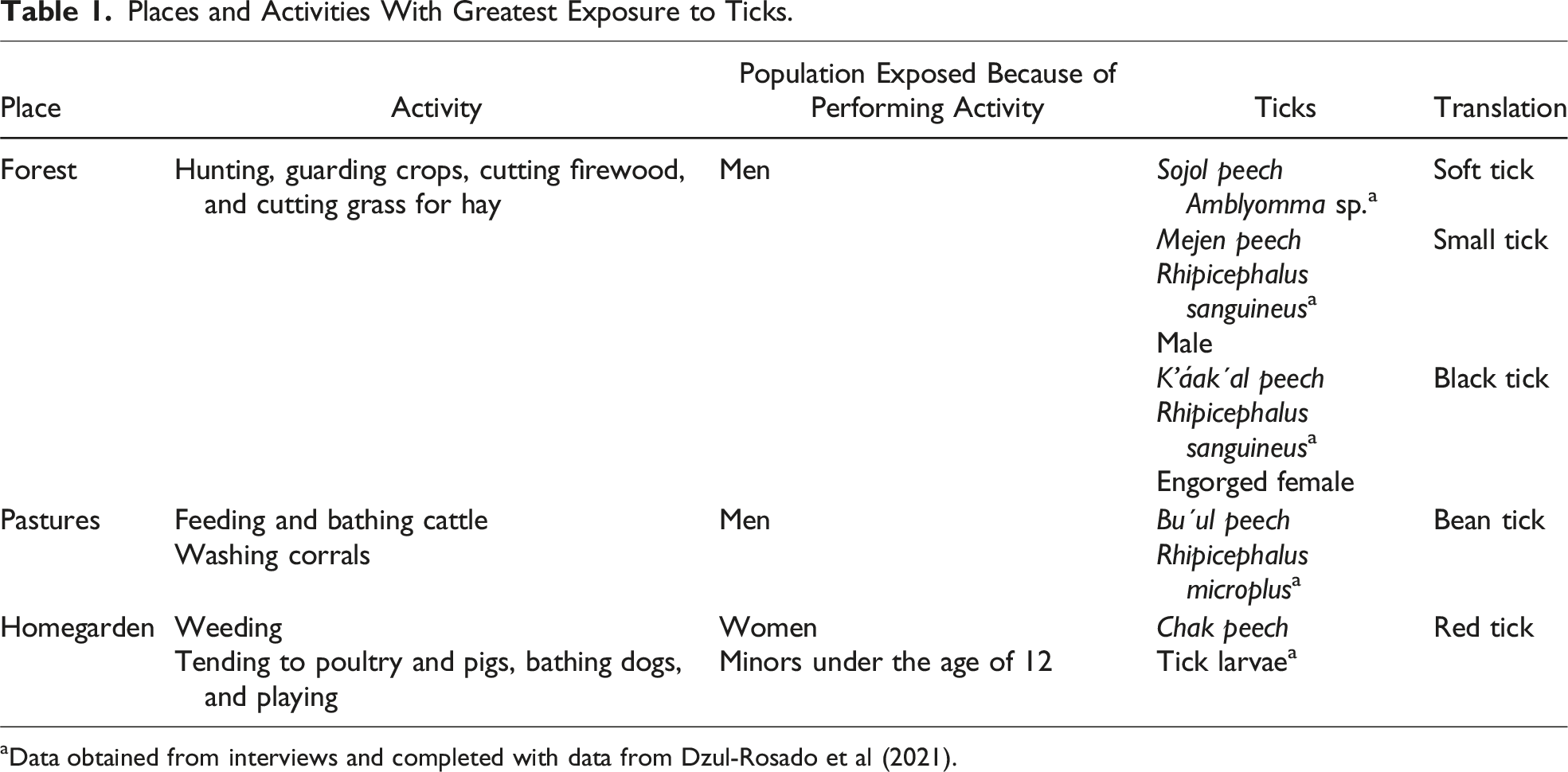
aData obtained from interviews and completed with data from Dzul-Rosado et al (2021).
People who walk through pastures or areas where wild fauna is found can carry ticks attached to their bodies or clothes. These ticks can be carried into the home: (…) sometimes they [male relatives] carry ticks (…) from … deer, cattle… from everything … the animals in the woods. They can’t go straight into the house like that! They have to remove them … shake them off … or … change their clothes or bathe so that they can come in the house, because … sometimes they even lie in the hammock, it will stick to the hammock! Sometimes when they come like this, if there is a tick where they went … yeah, a tick sticks to his [nephew’s] skin. He’s going to swell up! He’s allergic to ticks! (26-year-old woman)
Children learn about ticks; they observe them and listen to the adults around them talk about them. Sometimes their relatives talk to them about ticks to prevent them from getting bitten and experiencing discomfort. Despite their young age, adults assume that children will eventually implement what they have seen and heard: He [her son] was a kid. He didn’t know what it was. He was just scratching himself (…) my sister explained it to him. “When you see something like that”—she tells him—“it’s a tick! And if it bites you, it’s going to itch”—they tell him. She explained it to him and everything. Well, now you know, it may have gotten on him again (…) but since now he knows (…) they’re going to remove it (…). They are not going to tell me. (26-year-old woman)
Contact with ticks seems to be something normal and expected when interacting with relatives who work in the fields or enter the forest. When asked if her children had been bitten by a tick, one woman said, “Yes, because their father is always in from the forest” (38-year-old woman). Indeed, children have no compunction in helping relatives remove ticks from their bodies. When he [her husband] comes in, if I’m making tortillas, he says like “[in Maya] is the food is done,” “[in Maya] almost,” I tell him “Well hurry up because I got ticks” he says. But because I almost can’t see (them) because (they’re) so tiny [referring to tick size], I tell the kids … The kids already know. So, he grabs it, detaches it, kills it, then he [her husband] goes to bathe. Once he bathes, they also fall off, but you gotta take [them] off first. (41-year-old woman)
If children are still unclear as to what ticks are, they are vulnerable. As family caregivers, women are mainly the ones who notice any ticks on their children’s bodies. They identify ticks when examining their children or if the children express discomfort from bites: Sometimes they [ticks] get on them [children], because sometimes when he [her husband] lays in the hammock, I think (…) if we don’t remove it [the tick] it stays in the hammock. For example, they removed one from the baby [two-month-old grandson] (…) they were breastfeeding him (…) his mother noticed (…) she removed it and saw that it was a tick, yep! [nodding] (…). That’s also how she healed … my little granddaughter, the girl (…) she’s barely talking, she’s just learning to speak (…) she speaks Maya, she speaks Spanish (…) she comes like this and says to her grandfather “grandpa, there’s an ant [siinik in Maya]” (…) she doesn’t say like, “ants bit me,” “there’s ant.” And she’s showing him (…) that there’s an ant on her back. Then her grandfather lifted up her shirt and told her “It’s not a siinik, it’s not an ant that’s biting you—he says—, you have a tick,” my husband started to remove it (…) but it was already deep, it couldn’t be removed. (37-year-old woman)
We observed that children know about ticks, and they even expressed what they had learned. A participant’s son, who accompanied him to the field, interrupted the conversation with his father to describe what it feels like to be bitten by a tick: “When you are walking or hiking, when it bites you, you don’t feel it. When you lie down for a while, even if it’s only 20 minutes, you feel the pain” (12-year-old boy).
The Tick Bites, the Poison Makes You Sick
All participants mentioned that the main discomforts caused by tick bites were itching and redness around the bite area, reactions also associated with mosquito bites (another insect in the community, responsible for transmitting dengue, chikungunya, and Zika). They observed that children and allergic people may have more intense reactions to bites, such as skin sores and persistent itching; they expressed this as “it doesn’t suit them” or that the bite does them no good: “There are children for whom tick bites don’t suit them, there are children who are bitten, but nothing happens to them, but this one [her daughter] tick bites don’t suit her (…) but ever since she was a child it’s like that” (41-year-old woman). After growing up and experiencing tick bites, adults (mainly men) apparently become tolerant to the discomfort; they say they do not feel anything, or only itching: Yes, ticks bite him [her husband] but nothing happens to him (…) he just bathes with alcohol and that’s it, it goes away where they bit him. But my son, wow!, the last time he was bitten by ticks from animals, from cattle (…) on the ranch …; he got some pimples everywhere! On his hand, on his feet, I tell him “I don’t know why you went; I’m telling you not to go” I tell him “You know that nothing happens to your dad when they bite him.” I put a little salt water on them, so he could bathe and that was it … he had a few pimples, but they’re gone now. (36-year-old woman)
They also observed that when bites cause more discomfort than usual, it may be because the ticks had bitten animals in the woods before biting the person: “Sometimes you get sick, if it bit a snake, you get infected” (43-year-old man). This was emphasized by one of the traditional healers and his son: Interviewer: So, the k’áak’al peech are the ones that can make you sick if they bite you? Participant: Yes (…) you can also become paralyzed (…) if you are bitten at 15 years old [that is, if younger than 15 years old] and you begin to have back pain, your feet lose strength, [the tick] has bitten a snake and it transmits it to your body. Son: The poison. Participant: The poison stays in your body and little by little your defenses decrease, then you start to get sick (…) First it will bite you and you will swell up, then it will be red (…) finally (…) it’s purple, scarring, but it’s always itchy. Son: It leaves its tooth (…) You’ll take them out with a needle. (Traditional healer, 54 years old, and son, 12 years old)
Ticks are often removed with the fingernails, although participants did report using other available resources: “… for example, my grandmother, that’s what she tells me, ‘you pinch it with the nail clipper, and you kill it’, that’s what she says, ‘so that it’ll let go of the skin’” (26-year-old woman). If a tick is found on someone’s body, it must be removed completely; if not, the bite can become irritated and the skin can develop sores or become infected: “When they kill the tick, you put salt with lemon [on the bite] so that it … gets rid of the poison!” (traditional healer, 81 years old). Participants mentioned using citrus fruits to eliminate the poison, or whatever may remain on the skin that causes the discomfort.
Pragmatism and Observation
When asked, participants said they took no preventive measures to avoid contact, bites, and tick infestation. However, in our analysis of their responses, we identified ways in which participants did protect themselves, their family, and their home.
Prevention
Based on their knowledge of areas and activities with increased tick exposure, participants implemented various strategies to minimize tick contact and the amount of time a tick remains attached to the skin. These preventative strategies are practiced by the entire family. For example, if men know they are going hunting or will be working with livestock or will be anywhere with a high probability of contracting ticks, they ask their wives to prepare a bath of hot water with salt and alcohol to bathe themselves upon returning and thus prevent ticks from entering the home. If he goes far out there, this is what he tells me, “Heat up some water. When I get home, I’m going to take a bath.” And when he gets back, I get his water warmed up and he gets in the bath, because he has lots of ticks on him; sometimes I put alcohol in the water for his bath (so that) they fall off. (35-year-old woman)
This mixture (hot water with salt and alcohol) was said to prevent any ticks not found during physical inspection from remaining on the skin and to minimize itchiness from any bites. One participant described what happens when her husband arrives from the fields: “When he gets back (…), we’re all [she, her children, and her grandchildren] picking ticks off his back, his arms, his feet” (37-year-old woman). In addition, the man changes into a clean set of clothes and separates the dirty clothes used in the field from the rest of the family’s clothing.
A preventative strategy used by men before tick exposure was to rub tobacco (Nicotiana tabacum, k’úuts in Maya), alone or mixed with water or alcohol, onto their clothes and skin. This is believed to be a general repellent for work in the bush or hunting. They said they use it mainly to ward off snakes, but that it has the indirect effect of preventing ticks from attaching to their clothes or body: …before (…) pure tobacco. My deceased father when he took me [to the plot] when we have ticks, he chews tobacco (…) he rolled it up, you put it in your mouth, you chew it, you taking out saliva and you putting it on the clothes (…) raise your pants like this (…) you put it underneath, so they don’t climb up you. (61-year-old man)
Traditional methods of preparing k'úuts are still used, especially by older people, although less frequently. They prepare a mixture of dried tobacco, Maya breadnut (Brosimum alicastrum, Family: Moraceae), and bastard cherry (Ehretia tinifolia, Family: Boraginaceae) leaves mixed with medicinal alcohol (or moonshine) and honey.
Some participants explained that to save time younger men opt to buy cigarettes, crush them up, and mix them with water to prepare a mixture to spray on their clothing and body: Alcohol (…) with a cigarette, that’s just what he [her husband] uses (…) I watch him prepare it [laughs]. He bathes … his hand or his foot in it so they don’t climb up on him, because those things [ticks] do climb up on their own, uh-huh! but it doesn’t stick (…) it falls right off. (41-year-old woman)
Still others just smoked cigarettes as they entered the bush to impregnate their clothes and body with the smell. Apparently, they feel the time saved is worth the extra cost.
Homegardens were described as an area for everyday activities such as clothes washing, cleaning of domestic utensils and equipment, resting, and children’s play. For this reason, participants stated that they kept this space clear of dried leaves and fallen trees or branches to protect against ticks and other potential dangers: It gets weeded, but then everything grows back thick again (…) even just from walking, going to the bathroom [open-air defecation] there are little ticks. When you squat down, well, since they’re [the ticks] walking around, they climb up onto you; those are the ones that swell up [chak peech tick bite]. (61-year-old man)
Care
How bite reactions were treated varied depending on who had been bitten. If a young child was bitten, their mother treated the bite quickly and carefully with the understanding that children were more likely to have an allergic reaction, develop skin sores, or experience persistent itchiness. The women participants stated that when treating their children, they alternated between traditional medicinal resources and biomedical products; the latter included creams such as Barmicil® or other ointments sold at pharmacies: “If he has a tick on his ear (…) I put Barmicil cream on it (…), I always have Barmicil, that’s what I put on it” (34-year-old woman).
The women observed that the men were more accustomed to discomfort from bites and overlooked them. However, if itchiness persisted, they might treat it with salt, medicinal alcohol, ointments such as Vicks VapoRub®, or tobacco (Table 2). Alcohol (…) because if not, it’s like it gets infected (…) when you take [it] off, you get itchy if you’re allergic (…) one of those bites (…), like a pimple forms on you (…) but now we [use] alcohol or hydrogen peroxide (…) ¿you know what my father did too? Well, that’s how he taught us, you put tobacco in the alcohol and take that to the parcel. When you get there, before going in [to the parcel] you put it on. When he knows there’s weeds he puts it on and they don’t stick to him, [it’s] alcohol and tobacco in his remedy. (44-year-old man) Resources Used to Relieve Cutaneous Reactions to Tick Bites. Note. M=men; W=women.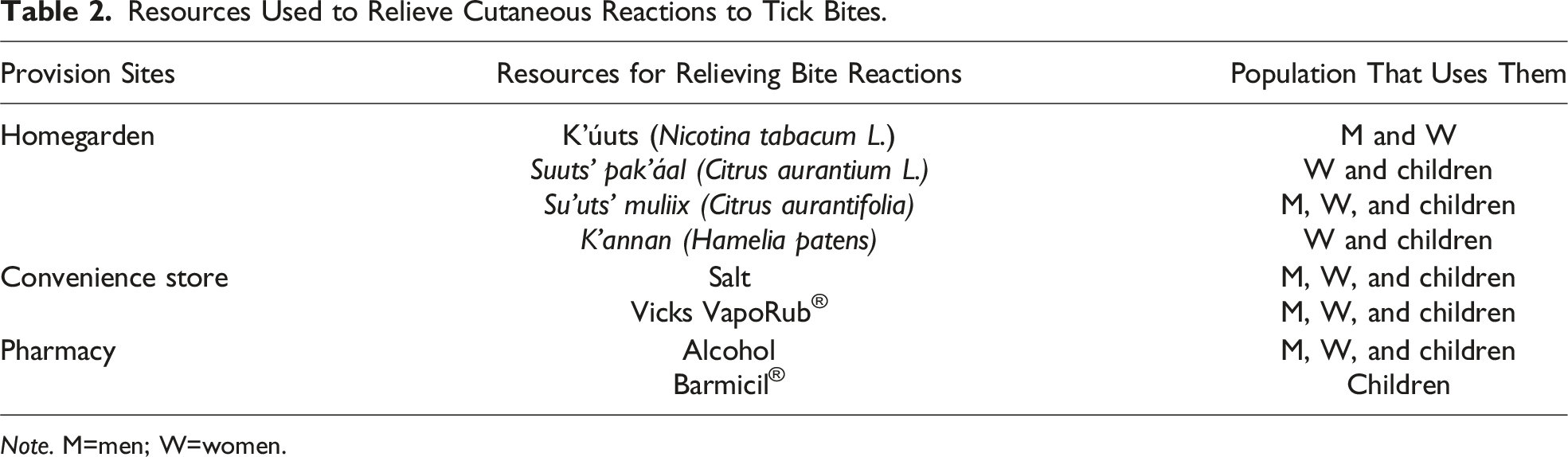
K’úuts was also used as a medicinal resource by other household members to reduce itchiness and other skin reactions to bites, as well as to mitigate muscle pain. One woman participant mentioned using firebush Hamelia patens (K’annan in Maya) when her daughters felt itching.
Woman Caregivers
The participants’ families largely had a peasant lifeway, with a clear gender-based social division of labor. From a young age, women are socialized to do household chores and, as wives and mothers they acquire new responsibilities such as caring for their family’s well-being. Their ability to care for and cure transcends childhood illnesses, especially when they have contact with biomedicine: I do worry about him [husband] (…) since (…) they gave me talks in the hospital about how you feel when you are diabetic, how you feel when you are hypertensive, how you feel when your sugar or your weight is too high, so I tell him “you’re already diabetic, I tell him, your triglycerides are high and he doesn’t want to accept it. You’re already way overweight,” but they don’t believe me. So I tell him, “why do I keep telling you things if you don’t believe me?” I even say it to my mother-in-law. I treat my mother-in-law like a little girl, “don’t eat too much salt, don’t eat too much butter! Why? because you eat too much salt and your blood pressure goes up and if you don’t stop eating salt, your blood pressure won’t go down.” She suffers from colitis too (…) it’s her nerves, she gets upset and her blood pressure goes up, her colon gets congested (…) she tells me “my stomach hurts, I have diarrhea” you know what? (…) she’s going to cook just a little bit of salt I’m going to put in the vegetables and that’s what you’re going to eat, and sometimes she says “it’s not good, it’s not salty” (…) my husband is like that, when he eats, tons of salt, after a while “Ouch! My hand hurts, ouch! I don’t know what’s wrong with me (…)” So I tell him (her husband) sometimes it bothers me because I’m (…) trying to take care of them. (40-year-old woman)
Based on the documented experiences of the participants and biomedicine professionals, we found that the local health center, through government programs, was a space where women obtained information on family health care, outside of the doctor’s office. Prospera was a federal social program which addressed health, nutrition, and education issues, and conditioned a financial stimulus on regular participation in program activities. This program asked mothers to care for their own health and that of their families. To do so, they attended talks at the health center, where a health promoter functioned as a link between the institution and the community. The promoter was told “if we have a case of Rickettsia in town, we’re going to address rickettsiosis [a group of infectious diseases associated with tick bites], if it’s the rainy season, we’re going to talk about dengue, the vaccination campaign is coming, then we’re going to talk about (…) anti-rabies vaccination” (…) That was the mechanism we had (…) the promoter is the one who trains the people, the one who if there is a probable case of dengue (…) goes to visit [the person], or if there is a case of some disease (…) goes to follow up but outside the clinic. He’s the one who carries out the activity with the community, and he in turn relied on women, block chiefs (…) that were part of that program. (Head of Yucatan Zoonosis Program)
The articulation attained between the different institutional and community agents created a favorable scenario for working to improve health in rural communities; local problems were addressed with key agents accepted in the community. Although the stimulus for participation was financial, the women participants also said there were other benefits from participation in the program, such as health knowledge, medical control, and constant check-ups. When we had (…) Prospera (…) they told us, we have a booklet, … a paper where we had to go to our talks every month (…). If we did not go to our talks, they took away the program from us and we said, “so they don’t take away the program, we attended the talks” (…). (…) this month there was a talk about diabetes, the next month there were talks about hypertension, the following month there were talks about … about, for example, triglycerides or pregnant women or something like that, about diseases (…). I learned a lot there, more or less I think I learned the symptoms of each disease and that’s what I use as a base (…) sometimes when I go to consult or to my appointments, to appointments like that, I ask the doctor things. Why? I like to know (…) Because then I know what medicine it is, what medicine I can give (…) or I can’t give to my patient. (40-year-old woman)
The women valued these spaces where they shared information. They said they learned about personal hygiene, pregnancy, contraceptive methods, and vector-borne diseases, even about chronic-degenerative diseases: Before, in Prospera they demanded that you have to go to your appointment. You have to go to your check-up if you have diabetes, and today nobody goes to their check-up. Before, they do go, because if they don’t go, they are marked a missed visit, and they don’t get their grant. But today, no. Today, yes, if you want to take care of yourself, you go (…) it was better [before] because they pressured you. (34-year-old woman)
In this biomedical space, women interacted with other women of different ages. In addition to sharing knowledge and experiences as wives and mothers, networks of relationships were created that extended into the community. Communication was helped by the fact that the promoter spoke Maya, and thus the participants felt comfortable speaking in Maya at the meetings. The COVID-19 pandemic and changes implemented by the federal government affected meeting continuity; the program was cancelled in 2019: “Then came the change and all that, there was no longer any talk, and we were left hanging [laughs]. The president of the republic changed, all that and there was no more” (40-year-old woman).
The participating women had been regularly exposed to biomedical spaces; in contrast, the adult men had remained distant from biomedicine, avoiding medical appointments and opting for home remedies for any discomfort, including tick bites. This, despite being more exposed to vectors due to their work: He [her father-in-law] told me “Pull this off,” but it was already engorged, the tick looked fat (…) but the little head stayed in (…) and they told him to go to the Health Center so they could check it (…) no, he says. With alcohol, with VapoRub. But it started to hurt, and my mother-in-law told him, “I told you to go, and you didn’t want to go!” (…) he started to put warm VapoRub on it and that’s it, I think it died, that’s when his pus came out. It never got better, it’s always red. It hurt for a long time; I think more than a month. That’s why she [his mother-in-law] was scolding him that he should go to the appointment. (40-year-old woman)
The physician in charge of the health center agreed with the participants, who stated that their husbands and fathers avoided going to the doctor when physically ill, unless it prevented them from working or when they suffered a chronic illness. It is not that men don’t get sick … I don’t know how they do it, or they send their wife, right? “Go get my medicine and say it’s yours” I don’t know, but men don’t … they hardly go to the doctor. The majority … the men who go to the doctor are those who are over 50, 60 years old (…) the elderly … when younger, the majority (…) are women, (…), they also bring their children, they bring their older children, that is, the mothers, the women are the ones who come to appointments most. (General physician at local health center)
As part of their role as caregivers, women accompanied men to the doctor—they generally did not to go alone—and then they cared for them at home, applying their knowledge. Men informed women of their ailments: “When I get a fever, it hits me hard, and I tell her [wife] to take me … so we go to the doctor” (36-year-old man). Wife: “Why would he go alone?!” (34-year-old woman).
The local medical personnel did not mention having treated patients with tick bite–related symptoms. They know that tick bites occur in the local population, and that people do not seek medical care for them. The head of the Yucatan Zoonosis Program characterized this as a potentially significant problem, referring to tick-related diseases, specifically Rickettsia, as a “sleeping giant.” When we wake it up, we won’t know what to do, because it is such a huge monster much more complex than dengue, than rabies (…), given the scope of dealing with a rickettsiosis outbreak. We need to work with the person (…), examine the environment where they are, in this case the home, [use] control activities in the home and on [tick] reservoirs (…), dogs or cats (…), rats, mice, rodents, (…) opossums. (Head, Zoonosis Program, Yucatan)
Discussion
This study is one of the first studies in Mexico to explore household practices for tick bite prevention and management in an indigenous community. Unlike previous research focused on tick-borne disease epidemiology, our approach highlights local knowledge, everyday strategies, and intergenerational knowledge transmission. Our findings provide a novel perspective on the intersection of traditional knowledge, community health, and risk prevention in rural and indigenous contexts. They show how members of the domestic group transmitted knowledge and know-how about tick control and bite treatment in their daily lives. All participants were aware of how ticks attach themselves to people and the discomfort caused by tick bites. Even children participated in the conversations and shared their experiences about ticks. However, they were generally unaware that ticks are vectors for various diseases. This has also been reported in a previous study of men and women heads of household of Mayan ancestry in Teabo aimed at documenting their knowledge, attitudes, and practices related to exposure to and prevention of tick-borne diseases (Dzul-Rosado et al., 2018). Although participants in this study were very knowledgeable about ticks and where they were most frequent, they were largely unaware of the disease transmission risk posed by ticks. This is similar to how cattle ranchers in Eastern Cape Province, South Africa, didn’t associate tick bites with any human diseases in a study of local knowledge, attitudes, and practices related to African ticks, their bites, and consequent infections in a cattle ranching area where contact with wildlife is frequent (Katswara & Mukaratirwa, 2021). Another study done in Teabo, of Maya farmers’ traditional knowledge about tick-borne diseases, found that the farmers believed that tick bites require no treatment at all (Dzul-Rosado et al., 2020). The same held true in a qualitative study of agricultural workers at eight farms in Malaysia aimed at understanding their experiences, knowledge, health-related beliefs, informational needs, and preventive practices related to tick bites and tick-borne diseases (Ghane Kisomi et al., 2019).
We found that the study participants and their families had developed preventive strategies that were accessible given their household budget and functional in their everyday lives; they resorted to local resources to prevent contact with, and bites from, ticks. The prime example in the present results is the use of k’úuts (tobacco) to keep snakes away and prevent ticks from attaching to clothes and skin. Similar findings were reported in a study of rural and urban inhabitants in southern Poland aimed at identifying how the occupational risk of working in tick-infested areas, in conjunction with previous experience with ticks, influenced participant awareness and behavior (Bartosik et al., 2008). Rural inhabitants preferred to protect themselves using resources from their immediate environment, such as smoking cigarettes and rubbing gasoline or essential oils on their clothing and skin. In the present study, the most common tick preventive strategy used by men was self-inspection of their clothes and body. They did this after being in areas with high tick abundance to prevent ticks from attaching to their bodies. Self-inspection after tick exposure was also one of the main preventative strategies reported in a study of inhabitants of endemic tick regions in the states of Connecticut and Maryland, United States, evaluating participant knowledge, attitudes, and behaviors regarding prevention of tick-borne diseases (Niesobecki et al., 2019). In a case–control study of Connecticut residents evaluating the effects of peri-domestic preventative measures on the risk of contracting Lyme disease (a tick-borne disease), self-inspection after vector exposure was recommended as part of a wider preventative strategy for improving protection against ticks and their diseases (Connally et al., 2009).
In the studied families, domestic medicine included multiple preventative and curative methods. Participants used resources from traditional medicine as well as from biomedicine to treat the cutaneous symptoms of tick bites, mostly itching. Biomedical products (e.g., Barmicil®, which contains gentamicin, betamethasone, and clotrimazole) were most often used to relieve dermatitis in children. These were purchased by the mothers, who used them and stored them in their medicine cabinets. Domestic medicine is a self-aid practice, although the way it is applied within a household responds to structural elements that transcend basic first aid and healing practices (Zolla-Luque & Mellado, 1995). The decisions made as part of domestic medicine transcend pragmatism, stemming more from the cultural and historical processes by which types of aid and their meaning are constructed (Menéndez, 1994). Cultural and historical processes were also structuring elements in a study of women in northern Tajikistan seeking medical services during pregnancy (Nabieva & Souares, 2019). Decision-making was permeated by cultural factors such as family organization and gender roles.
We found that even though almost all participants were bilingual Maya–Spanish, Maya was used to discuss health-illness-care topics with other members of the domestic group. In addition, adherence to recommendations from outside the domestic sphere was taken more seriously if shared in Maya, the language used by the health promoter and doctor in charge of the health center (both members of the community in which they work). This was also the case for traditional healers, because a healer is a member of the same community, shares its worldview, speaks the patient’s mother tongue, and “…works like the others: most of the men in their cornfield, the women taking care of their children and home, as vendors, embroiderers” (Gubler, 1996, p. 13).
We found that economics was also a structural element of domestic decisions about health care in Teabo. When men were not at home due to their work, mothers decided how to treat health issues, and, under the guise of not wanting to worry their husbands, would not inform them. Any costs incurred were covered from the household budget or from their own financial resources. They generated their own income by selling handcrafts (e.g., embroidered clothing and hammocks) or gathering firewood for sale. These activities were done in addition to their regular domestic responsibilities. They also used the financial incentives from the Prospera government social program.
In their roles as mothers, wives, husbands, and children, we observed that household members had learned to care for each other. Their knowledge and know-how in addressing family health issues had come from observation and acquired experience. In their study of the therapeutic practices of housewives in Valdivia, Chile, and the value they attribute to their role as family caregivers, Jara-Araneda and Soto-Retamal (2021) found that disseminating knowledge in the domestic sphere occurs through “feminine transmission.” It unfolds in an orderly, hierarchical fashion in which elderly women are immediate reference points for younger women. This coincides with Tabong et al. (2021), who explored the reasons women preferred traditional midwives to free maternal health clinics. They used a phenomenological approach with 31 women in northern Gahan who had decided to use a traditional midwife to give birth. The women preferred midwives because they provided care during birth but also supported the women in the process. In addition, since they shared a cosmovision, greater value was assigned to the care they provided to the women and their newborns.
This coincides with our results in which older women shared the knowledge they had acquired while married, as well as that gleaned from other elderly women who passed knowledge on to them during their lives. Of note is that young women in the present study, using their own judgment, were deciding how and in what situations to use the information provided by their elders. This is similar to patterns observed by Peniche-Moreno and Angelotti-Pasteur (2018) in their study of San Pedro Juárez, a Maya community in the municipality of Tizimín, Yucatan, during a chikungunya fever epidemic in 2015. They underscore that, much as we observed in our study, therapeutic knowledge expressed by women emerges from internalization of their experiences as mothers, daughters, neighbors, and guardians of family and community health.
As part of the self-aid model, many authors see domestic medicine as the first true level of health care (Menéndez, 2003, 2018; Osorio-Carranza, 2001; Zolla-Luque & Sánchez-García, 2016). Within a household, women occupy the role of “domestic authority on health-related topics” (Szasz, 1995, p. 22), since they are in charge of noticing, diagnosing, and initially treating some ailments affecting family members. This was clearly the case with tick bite–associated maladies in Teabo: all women participants in this study had dealt with tick bites at least once in their lives. Within their homes, women primarily treated children still in the process of familiarizing themselves with ticks. In Teabo, we observed that the Prospera program reinforced the division of labor by gender, because women represented their family in the program, adding to their daily activities and those of their older daughters or female relatives on whom they relied to meet the requirements that the program demanded to receive financial incentives. This coincides with Gil-García (2015), who conducted an ethnographic study in La Gloria, a settlement of indigenous Mayan refugees from Guatemala in Chiapas, Mexico, focusing, among other things, on the gender equality component of Prospera. Among the findings is that program participants negotiated maintaining family care to remain in the program and that women exercised their capacity for action beyond hegemonic neoliberal forms of government (Gil-García, 2015, p. 462). In a study of autonomy and reproductive rights among indigenous women in the Prospera program in a Mayan community in Chiapas, Mexico, Abarbanell (2020) found that the program had produced many positive results, but it was definitely not the path to female empowerment.
Conclusions
This is one of the first studies in Mexico to highlight the importance of recognizing the families’ active role in health-related issues, especially the knowledge of women, in health management and disease prevention in communities vulnerable to ticks. It highlights the importance of incorporating an intercultural approach into public health programs if they are to be effective. These programs could benefit from including local knowledge in campaigns to raise awareness about tick-borne diseases and their risks. Current preventive measures are clearly insufficient considering the potential disease risk and that many of the symptoms of tick-borne diseases can be confused with those of potentially mortal arboviruses such as dengue, chikungunya, and Zika. If health education programs are to be truly effective, they need to understand local health practices and knowledge, and then use them to adapt their approach to the realities of the target communities.
Footnotes
Acknowledgments
The authors thank the women of Teabo and their families for participating in this study, as well as the authorities and staff at the Health Center for their hospitality and support during the period of field work. The authors express gratitude toward community members Karina Mutul and Magdalena for their accompaniment, and Ligia Uc and Ameyali Rios for aiding in interview transcriptions.
Authors Contributions
J.P.-V. contributed to study design, data acquisition, and analysis, K.R.D.-R. and M.T.C.-B. contributed to conceptualization, study design, and data analysis. L.A.-M. and C.N.I.-C. contributed to design and validated the study. All authors reviewed and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Informed Consent
Due to community political context and the COVID-19 pandemic, participant informed consent was provided verbally prior to study participation.