
Abstract
Black same gender loving (SGL) men in the United States continue to experience mental, physical, relational, and financial health inequities due to the impact of various systems of oppression. Despite this fact, there are few health interventions developed specifically for Black SGL men that address health outcomes beyond sexual health. Despite strong evidence that spirituality is a cultural strength associated with positive health outcomes for Black SGL men, it has seldom been incorporated into health interventions as a central mechanism for facilitating this group’s well-being. The present qualitative study utilized a hybrid (i.e., codebook and reflexive) approach of thematic analysis to analyze data from individual semi-structured interviews with 29 Black SGL men across the United States. Three themes were generated: (1) Harmful and Nonresponsive Institutions; (2) Diversity, Detail, and Black SGL Men’s Preferences in Intervention Design; and (3) Multilevel Positive Holistic Impact. Findings from this study may be used to develop spirituality-based holistic health interventions for Black SGL men in the United States. Such interventions have the potential to effectively reduce health inequities among this population.
Keywords
Introduction
Black same gender loving (SGL 1 ) men are male-identified people of African descent who experience same-sex or bisexual attraction and embrace their Black culture and values (Lassiter, 2014). In the United States, these men are subjected to routine marginalization due to experiencing intersecting systems of oppression (e.g., racism, heterosexism, and poverty), which have adverse effects on their overall health (Follins & Lassiter, 2017; Lassiter, Follins, et al., 2020). Regarding their mental and physical health, research has indicated that exposure to experiences of oppression is associated with adverse health outcomes such as psychological distress, perceived burdensomeness, heavy drinking, sleep disturbance, and risky sexual behaviors (Caceres et al., 2019; English et al., 2021; Hatzenbuehler et al., 2009). The health effects of oppression are broad and far-reaching.
In terms of relational health, extant evidence has suggested that experiences of interpersonal heterosexism can manifest in the form of violence, bullying at school or work, expulsion from families, and strained familial relationships (Barton, 2010; Boykin, 1996; Griffin, 2006). These experiences make it difficult for Black SGL men to share their sexuality with others. This difficulty increases experiences of social isolation and loneliness (Lapinski et al., 2010). Black SGL men have also reported experiencing internalized racism which has contributed to them perceiving other Black SGL men as unsuitable sexual partners (Wilson et al., 2009). Such internalized oppression makes Black same-sex relationships difficult to develop and sustain.
Black SGL men often experience financial oppression in the form of poverty. Empirical data indicates that approximately 31% of Black lesbian, gay, bisexual, and transgender (LGBT) people live in poverty compared to 25.3% Black cisgender heterosexual people (Badgett et al., 2019). Findings also indicate that 48% of Black SGL men live below the poverty line compared to 44% of Black cisgender heterosexual men (Choi et al., 2021). Poverty has been found to be significantly associated with sexual risk behavior and decreased pre-exposure prophylaxis use (Burns et al., 2021; Mena et al., 2017) among Black SGL men. Taken together, the oppressive systems of racism, heterosexism, and poverty negatively impact Black SGL men’s health in profound ways.
Unfortunately, most of the health research conducted with Black SGL men predominantly focuses on their sexual health, while neglecting Black SGL men’s holistic health. Evidence suggests that 90% of the existing literature on Black SGL men has focused on sexual health–related research (Wade & Harper, 2017). More research on Black SGL men’s strengths and resilience is warranted given their ability to successfully adapt and thrive in the face of multiple forms of oppression. Spirituality has been found to be one culturally relevant strength—of several—that has helped Black SGL men navigate oppression and achieve good health (Lassiter, Saleh, et al., 2019; Smallwood et al., 2017; Taggart et al., 2021; Watkins et al., 2016). Of note, spirituality overlaps with, yet is distinct from, religion (Hill & Pargament, 2008). Black SGL men have identified spirituality as a form of personal and multidimensional connection with the sacred that is inclusive of religious practices and beliefs yet not exclusive to them (Lassiter et al., 2020). Black SGL men reported that spirituality is a guiding force that is shaped by their experiences of intersectional oppression and ancestral connections, which in turn influences their thoughts, feelings, and behaviors. Black SGL men have disclosed that in moments of high spiritual consciousness they are able to harness their spirituality to positively impact their mental and physical health (Lassiter & Mims, 2022). Given the strong influence of spirituality in Black SGL men’s lives, spirituality-based health interventions may be an appropriate avenue for increasing holistic health among this group.
Spirituality-based health interventions have been found to be beneficial in improving health outcomes among the general American population. For example, spirituality-based cancer interventions were found to have positive effects in terms of reducing fatigue, chronic pain, anxiety, depression, sleep disturbance, hospitalizations, and enhancing one’s spiritual well-being, faith, and meaning of life (Izgu et al., 2024; Torabi et al., 2024; Zhang et al., 2024). Research with Black Americans has found that church-based health programs have positively affected myriad health outcomes such as hypertension, asthma, cardiovascular disease, and HIV/AIDS (Campbell et al., 2007; DeHaven et al., 2004; Hankerson & Weissman, 2012). Relatedly, health interventions that have been designed using African-centered values (e.g., Nguzo Saba), including spirituality, have been found to significantly improve Black American’s people’s health outcomes (Belgrave et al., 2004; Gilbert & Goddard, 2007; Grills, 2003). Prioritizing spirituality and African-centered values in health interventions has promising implications for Black SGL men.
Spirituality-based and African-centered interventions have a strong body of efficacy research to support them (Izgu et al., 2024; Lateef et al., 2022). In Black communities, many of these programs are implemented as faith-based programs in church settings (Anderson et al., 2015). However, too many of them neglect holistic health beyond pathological foci and focus predominately on sexual health and substance use problems. Such features may unintentionally reinforce, instead of counter, the anti-Black and hypersexual stereotypes and demonization many Black SGL men face given the homonegative religious messages and sexual stigma to which they are exposed (Lassiter et al., 2019). To our knowledge, there is no empirical study that has investigated the potential impact of a spirituality-based health intervention exclusively for Black SGL men’s holistic health. The current article aims to provide stakeholders with insights and recommendations to design behavioral interventions that are spirituality-based and culturally informed by Black SGL men to improve their health.
The study was conceptualized and guided by the principles of participatory action research (PAR; Baum et al., 2006) and optimal conceptual theory applied to sexual and gender minorities (OCT-SGM; Lassiter & Mims, 2022; Lassiter et al., 2023). PAR is an approach to research with the goal of social transformation through addressing inequity (Rumsey et al., 2022). Aligned with PAR, we designed the present study with an emphasis on shared power (via co-construction of knowledge with our participants) and reflexivity. OCT-SGM is a culturally specific theoretical framework with the goal of prioritizing African-centered ways of being among sexual and gender minorities, thereby empowering Black SGL people to define themselves and thrive in environments where they are holistically affirmed. OCT-SGM proposes that life occurs in a spiritual context and that one’s health is influenced by one’s degree of attunement to the spiritual nature of life (Lassiter et al., 2023). Spiritual attunement influences one’s perception of intersectional oppression, and vice versa. The framework asserts that among Black SGL people low spiritual attunement may contribute to greater susceptibility to interpreting experiences of intersectional oppression in ways that are not conducive to good health. Relatedly, experiences of intersectional oppression make it difficult to remain spiritually attuned. Thus, good health is achieved by developing and maintaining high attunement to the spiritual nature of life, including how one’s own spirituality influences their sense of self and others. This assumption about the intertwined associations of spirituality, oppression, and health informed the study’s research questions, methods, analysis, and interpretation.
Study Aim and Research Questions
The present study aims to examine Black SGL men’s recommendations for developing a spirituality-based holistic health intervention. Our research questions were (a) Why is a spirituality-based health intervention needed for Black same gender loving men? (b) How should a spirituality-based health intervention function for Black same gender loving men? (c) What is the potential impact of a spirituality-based health intervention on Black same gender loving men’s lives?
Methods
Study Overview and Participants
The qualitative data presented in this article are from the Spirituality and Stress Study (SSS), a cross-sectional multi-method online study conducted from 2019 to 2022, that aimed to examine how spirituality and oppression-based stress influenced Black SGL men’s health (Lassiter et al., 2024). A total of 169 participants provided quantitative data for the study, and a subset of 29 participants also provided qualitative data. SSS was approved by the institutional review boards at the institutions where the research was conducted.
Selection criteria for the study included (a) being 18 years or older, (b) identifying as African American or Black, (c) identifying as a cisgender male or transgender male, (d) having romantic attractions to men or participating in same gender sexual behaviors, (e) engaging in a weekly spiritual practice (e.g., prayer and listening to inspirational music), (f) recognizing the importance of spirituality and stating it was at least “somewhat important,” to them, and (g) having reliable Internet with the ability to participate in a face-to-face video call. Respondents who did not meet all study criteria were excluded from participation.
Recruitment
Recruitment was conducted online using ads and posts on social media apps, websites, and blogs with large Black SGL male readerships. The ads and posts consisted of culturally specific graphics that included the study’s name, purpose of the study, and a hyperlink that led to a short screening survey hosted on Qualtrics (see Lassiter et al., 2024 for more details). Respondents were informed that after completing all study tasks, they were eligible to receive $45 (i.e., $15 gift card for completing an online survey and a $30 gift card for completing a qualitative interview). Participation was voluntary and all participants were able to opt out by contacting the principal investigator.
Procedures
After completing the screening survey, research assistants (RAs; five undergraduate and two graduate students)—trained by the first author—called and assessed respondents for eligibility. If eligible, respondents were first invited to complete a survey with 14 psychometrically validated measures and 21 sociodemographic questions. A random subset of 33 participants who finished the survey were also invited to participate in the qualitative interview. Twenty-nine accepted. Qualitative data were collected using a semi-structured qualitative interview guided by a 23-question protocol. The first author and RAs conducted all interviews, with the first author conducting 41% of the interviews. Participants provided written consent before the interviews were conducted and gave verbal consent at the start of all interviews. The interview questions focused on Black SGL men’s insights about (a) participating in research studies where they would donate biological samples and (b) developing a spirituality-based health intervention. The findings presented in the current article are from analyses conducted with the data generated from the second topic area. Interview questions were informed by literature review related to the topics of interests, optimal conceptual theory applied to sexual and gender minorities (OCT-SGM), and a constructionist ontological approach that assumes that reality is subjective and context dependent. Interviews were conducted via a Health Insurance Portability and Accountability Act (HIPAA)–compliant version of Zoom to ensure confidentiality of the interviews. The mean length of the interviews was 58 minutes and 36 seconds. All recordings were professionally transcribed.
Sample Size
As recommended by Braun and Clarke (2021b), we used the concept of information power—having enough participants enrolled in a study to develop new knowledge—to determine sample size. We assessed the sample size’s ability to provide high information power by considering five factors: sample specificity, study aim, use of established theory, quality of dialogue, and analysis strategy (LaDonna et al., 2021; Malterud et al., 2016). The current study (1) only enrolled U.S.-residing, spiritually conscious Black SGL men who were 18+ years old at the time of the study; (2) had a narrow aim; (3) was guided by OCT-SGM; (4) utilized interviews conducted by qualitative interviewers trained specifically in thematic analysis and the cultural realities of Black SGL men; and (5) analyzed the data across cases. Previous qualitative studies have achieved moderate to high information power with samples ranging from 10 to 30 participants (Kruithof et al., 2024; Midtsund et al., 2023). Based on these factors, we are confident that our sample of 29 participants allowed us to achieve strong information power.
Data Analysis
We utilized a hybrid approach to thematic analysis that intentionally combined elements of codebook (Braun & Clarke, 2021a; Roberts, 2019) and reflexive thematic analysis (RTA; Braun & Clarke, 2022). We used a codebook to facilitate expedient team coding of a substantial dataset. The reflexive approach was used to guide a longer, more in depth process of theme generation that aligned with OCT-SGM and PAR (i.e., our guiding theoretical framework and research approach, respectively). Our process started with the first author (who has 10+ years of experience conducting qualitative research) familiarizing himself with the data by reading and re-reading transcripts and watching video recordings of the interviews (phase 1). He wrote memos about insights that occurred during this familiarization phase. At weekly data analysis team meetings, the first author shared these insights with the other members (five undergraduate and two graduate-level research assistants, trained by the first author). These team members were also responsible for reading portions of the dataset and sharing their insights in the meetings. After this initial phase, the first author coded six transcripts openly and organically using an inductive approach (phase 2). An initial codebook of 18 codes was developed. Using the codebook, the other team members coded five to seven unique transcripts each. Each transcript was coded twice. This process was iterative and resulted in six more codes being added to the codebook. The codebook was a method for providing a starting point for organizing the data into legible chunks of meaning. Differences in coding were discussed, and in some cases all coders’ categorization of qualitative data were included (i.e., the same part of a transcript was coded with multiple codes). NVivo 1.7.2 software was utilized to store and organize data.
After all transcripts were coded, the first author independently continued analyzing the data beginning with generating initial themes (phase 3). This decision was made to more effectively track researcher subjectivity and facilitate deep reflexivity. The first author also had the most expertise related to qualitative methods and the guiding theoretical framework and approach (i.e., OCT-SGM and PAR). Theme generation commenced with collating similar codes together based on how well they responded to the research questions and aligned with OCT-SGM and PAR. The first author utilized memos throughout this process to document analytic decisions, reflections about the data, and standout quotes for later use. From this process, eight themes were generated. Next, we used the OCT-SGM and PAR lens to further develop and refine codes (phase 4). Specifically, we re-read the data in the context of the transcripts to determine how well they supported the themes and made sense within the OCT-SGM framework and PAR approach. This process resulted in one theme being removed. We further refined our themes by shifting some data from one theme to another as appropriate. The resultant seven themes were reviewed by outside qualitative research experts who recommended additional refinement to ensure “thick” themes. This re-analysis resulted in three themes (phase 5). Finally, this article represents phase 6 of our thematic analysis.
Trustworthiness of Results
Several steps were taken to ensure trustworthiness of our findings. The researchers focused on ensuring credibility, dependability, and confirmability (Nowell et al., 2017). To bolster credibility, member checking was used (Shenton, 2004). The research team emailed participants a list of extracted themes and de-identified supporting quotes. Participants were asked to email back with their thoughts about how well the quotes supported the themes. We also asked them to tell us how well they believe the themes matched what they intended to say. Overall, participants expressed no major concerns and indicated that they believed their thoughts on the subject were captured appropriately by the themes. Member checking allowed the researchers to include the participants in the co-construction of the interpretation of the data. Regarding dependability and confirmability, the authors have reported all decisions about research design, analysis, and interpretation in a way that is logical, traceable, and clearly described throughout the article (Braun & Clarke, 2022).
Researchers’ Positionality Statement
The first author is a Black American SGL cisgender man with a PhD in clinical psychology and advanced training in disease prevention science. With a career of 10+ years, he is highly experienced with qualitative methods including thematic analysis. The values that guide his work are informed by his background growing up in a working-class, Christian, Southern family highly aligned with African-centered values such as (a) belief in God and the spirit world, (b) respect for ancestors and elders, (c) high racial salience, and (b) prioritizing education as a method of liberation. The assumptions that guided the current study were (a) the unseen world (i.e., spiritual) influences the material world (including health beliefs and behaviors) and (b) Black men are the experts on their lives.
The second author identifies as a cisgender Muslim woman raised in a religious family in Pakistan, and her racial and religious identities are central to her sense of self. She is currently a fifth-year doctoral student in the first author’s lab and has a foundational understanding of conducting RTA. Through her own reflexive process in this study, she has gained key insights, including the understanding that “one size does not fit all” when it comes to increasing spiritual consciousness. This process has deepened her appreciation for the cultural nuances and diverse expressions of spirituality in Black SGL people.
The third author identifies as a Vietnamese American, a spiritual atheist, and a cisgender, sexually fluid woman. As a graduate research assistant in the first author’s lab, she has academic knowledge of African-centered spirituality and African American people’s experiences with oppression but very limited in-person interactions with Black SGL men. While interviewing the participants for this study, she took the stance of an outsider and primarily used an experiential approach to understanding the participants’ lived experiences.
The fourth author is a first-year doctoral student in clinical psychology, also a member of the first author’s research lab. She identifies as a Black West Indian from the island of St Maarten. She acknowledges that she has a novice understanding of and skills related to qualitative methodology. As a researcher who was born and raised in the Caribbean, she acknowledges that her cultural background both enriches and complicates her relationship with the research participants. While she may have a unique cultural perspective, she recognizes that her cultural lens may lead to misinterpretations of participants’ lived experiences.
The fifth author is a Black American cisgender SGL man with a PhD in public health and more than 20 years of experience in health promotion and disease prevention, particularly related to HIV in the southern United States. His approach to this work is informed by multiple factors, including his upbringing in a Black Christian tradition in the rural South, being an ordained minister in a mainline Black Protestant tradition, and a critical lens informed by critical theory and intersectionality. He currently directs several projects aimed at integrating theological education and public health principles to promote health equity achievement strategies in southern faith communities using interfaith and ecumenical approaches. All members of the research team worked together to intellectually and emotionally process and document their subjectivities related to this study to ensure that their perspectives were harnessed as a strength and did not overshadow the meaning making of the participants.
Results
Participant Demographics (N = 29).
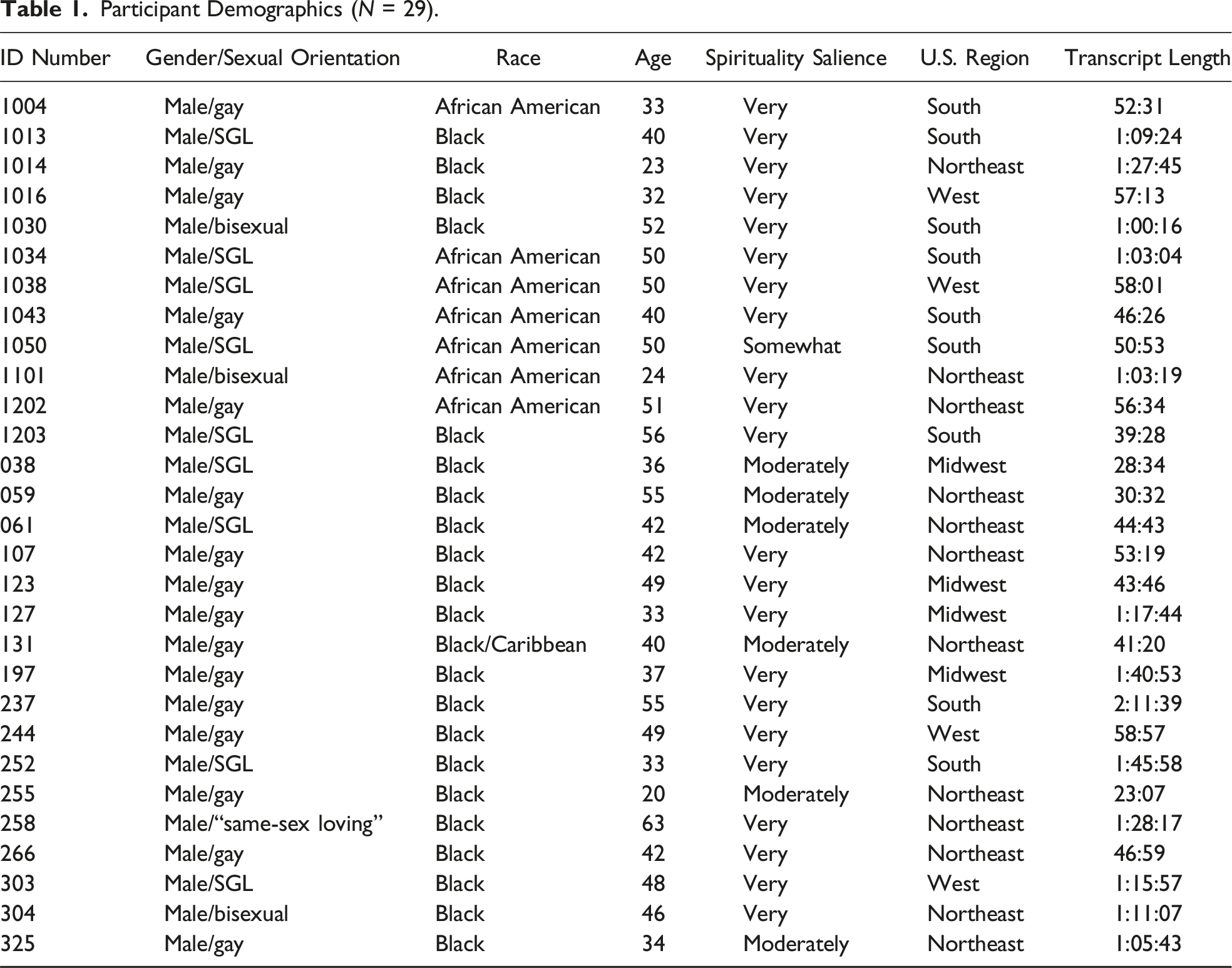
Three themes were generated. Overall, the themes provided essential information for guiding future intervention development. The themes were (1) Harmful and Nonresponsive Institutions; (2) Diversity, Detail, and Black SGL Men’s Preferences in Intervention Design; and (3) Multilevel Positive Holistic Impact. See the Supplemental Material for more details about each theme including definitions and additional supporting data. The themes are organized by the research question that they helped us answer. Participant ID numbers are in parentheses to provide context about who provided each quote.
Why Is a Spirituality-Based Health Intervention Needed for Black Same Gender Loving Men?
Many participants discussed the need for a spirituality-based health intervention in their interview responses. Their perspectives are represented by theme 1.
Theme 1: Harmful and Nonresponsive Institutions
This theme highlights that currently available institutions (e.g., churches, healthcare organizations, and non-profit social services) are ill-equipped and poorly designed to effectively meet the needs of Black SGL men. In some cases, these institutions perpetuate harm through heterosexism, racism, and other oppressive forces that negatively impact Black SGL men’s health. Participants highlighted that traditional Christian and Muslim religious spaces (e.g., churches and mosques) have perpetuated heterosexist stigma and discrimination against Black SGL men. These spaces have often demonized and rejected Black SGL men, causing trauma and sexuality-related guilt among them that contribute to negative health beliefs and behaviors. Many Black SGL men are living with spiritual wounds that affect every aspect of their lives. One participant (1034) shared, … the majority of the people that you’re gonna deal with … have had … some awful experiences in church settings. … they’ve been told, um-- we’ve been told that, you know, “You’re not right. … There’s something wrong with you.” … And so you are dealing with the walking wounded …
This participant reveals that church settings often turn Black SGL men against themselves and cause them to internalize beliefs that they are fundamentally flawed.
Another participant (1004) disclosed, I have to go back to the church and religious structure. I think that there’s a lot of, um, guilt-tripping and fear-mongering that happens and has happened, particularly with, um, organized religion historically. And I think that Black, same-gender-loving men have experienced a lot of that and have been traumatized by a lot of that for, for many of us.
This participant emphasized that religious organizations are the site of emotional trauma for many Black SGL men.
A third participant (1202) stated, They have self-criticized themselves not being able to fit into the mold and model that the Black church is. And then they’ve either stayed and lived just the craziest existence of the Black church and/or they have built a new spiritual model for themselves …
Participants described a need for new spiritual models given the negative impact Black American religious spaces (e.g., Christian and Muslim) have had on Black SGL men. Some participants spoke to the potential of Black religious spaces to be places of healing for Black SGL men. One participant (304) hypothesized that if Black SGL men are affirmed in their religious spaces, they may engage in fewer health risk behaviors. He said, Their willingness to take, um, rik-risks in sexual situations. There are-- there are a lot of implications, um, due to homonegativity. So if you have the opposite, hopefully, and, and based upon the numbers-- so if you have affirming congregations, affirming clergy, then the opposite-- the opposite happens.
Another participant (197) disclosed that he believes religious spaces should help Black SGL men embrace their sexuality, not shun it. He said, … what I realized for me is that … when your sexual-social relations are kept in that place. Like, there—something is happening to you as a person … when the only place you can express your sexual self is in the dark or at night. … I think that religious institutions can push against that, like, and give—if they were smart, they would do it … because I think the closets are ultimately spaces of death …
Overall, participants expressed that Black American Christian and Muslim spaces have contributed to harmful and traumatic experiences for Black SGL men across their lifetimes. They also believe that these same spaces have the potential to be beacons of affirmation and transformation if they encourage Black SGL men to be their authentic selves.
Participants reported that they perceive the currently available healthcare services and spiritual/religious spaces to be ill-equipped or poorly designed to effectively meet the distinct needs of Black SGL men. One participant (038) shared, … the healthcare system in general, right? We’re expected to be able to successfully navigate and operate through a system that wasn’t designed for us to be able to navigate, and when we encounter challenges or barriers, then we’re looked at as if we’re to fault for why we were unable to access or navigate that system, instead of them saying, “Okay. The system itself is broken”.
Another participant (123) reported, We don’t discuss this in church. … my church is now discussing mental health, yes, but … it’s been more related … to COVID and whatnot, but we don’t do this as an ongoing thing to talk about, yes, even as Christians, we do get stressed out, ‘cause we’re like everybody else. … it is something that needs to be discussed.
How Should a Spirituality-Based Health Intervention Function for Black Same Gender Loving Men?
Participants had several recommendations for how a spirituality-based health intervention for Black SGL men should function. Their suggestions are described by theme 2.
Theme 2: Diversity, Detail, and Black SGL Men’s Preferences in Intervention Design
This theme emphasizes that Black SGL men have diverse needs that require flexible, accessible, and culturally tailored curriculum development, content framing, and interactions between facilitators and participants so that spirituality-based health interventions may reach as many Black SGL men as possible. Participants believed that interventions should be specific in prioritizing Black SGL men who are interested in using their spirituality to improve their health while also being as inclusive as possible of Black SGL men from varied backgrounds. One participant (061) recommended that the program “puts them at the center of … the program, rather than just general health that’s for everybody.” Another participant suggested that we be open to the spectrum of sexuality. … I mean from monogamy to open relationships from … butch men to femme men to transgender to cisgender … having an understanding of the spectrum that may show up, and then how that gets blended, … So … there has to be a way to, to make us all understand we are one … in our individuality … and that everyone’s accepted here. … I think that’s [a] very important aspect … It’s a Black gay spirituality group.
Participants also provided recommendations about strategies to reach the target audience and potential barriers. The importance of building relationships and developing a good reputation with the community were highlighted as essential. One participant (325) advised, … it would take some time getting it off the ground ‘cause people aren’t gonna trust it just because. … it will take time to build relationships with people and institutions and organizations to get buy-in.
There was an emphasis on the intervention having cultural relevance and being developed and staffed by community insiders. One participant (123) recommended, Critically, [it] has to be culturally sensitive and-- to attract them … and that could even include … using images that look like us. … have to be friendly. … see someone that looks like me, someone that looks like him, you know? That’s what’s … gonna attract people to it.
Participants warned of potential obstacles interventionists might encounter in developing a spirituality-based health intervention. Such barriers included concerns about privacy, misconceptions about spirituality, and some participants not following through with the intervention due to lack of motivation.
In terms of intervention design, there was diversity across participants about preferences for duration, frequency, format, and setting. However, participants were clear that whatever the design, the intervention should be as accessible as possible to attract as many participants as possible. Across 28 responses to a question about the format of the intervention, a hybrid format with in-person and electronic (i.e., online or app) components was the most endorsed, followed by solely in-person, and then solely electronic. One participant (237) exemplified the plurality of participants’ preferences: I think it could be in different formats … It could be online, and it could be in person … and it could be-- the different, um, activities could be … in different formats … So you could have one-on-ones, and you could have the group sessions … a speaker, certainly, you can do, um, just … on video. … it would be nice to have … the group setting, just to be … growing, feeling like you’re growing with the group would be nice, um, and people can share their experiences … and learn from other people’s stories as well. … ’Cause kind of that spiritual connection is … easier in person.
Participants named several potential settings to gather for an in-person version of the spirituality-based health intervention. They named a diverse variety of places such as community centers, LGBTQ+ affirming churches, college campuses, doctor’s offices, gyms, bars, meditation spaces, research facilities, and health fairs. Overall, participants stated that regardless of the specific setting, it should be a place that is confidential, accessible, and engenders a feeling of physical, mental, emotional, and spiritual safety.
Participants also reported myriad preferences for how long the spirituality-based health intervention should last. One participant (123) said that the program should last one day, some said one year, and others expressed that it should continue indefinitely. Overall, participants shared that the intimate and spiritual nature of the program along with personal preferences should determine the length of the program. Furthermore, the spiritual work of the program was perceived as lasting longer than any formal sessions and was “lifelong work” (Participant 266).
Participants varied in their preferences for frequency of the group. Responses ranged from twice a year to weekly. The majority of participants expressed a preference for weekly meetings. The second most endorsed meeting frequency was monthly. Participants made arguments for each decision citing the importance of working on one’s spirituality and health, needing time to process information and emotions, and avoiding feeling burdened by the program. See Supplementary Materials for additional supporting data.
Participants suggested that interventionists be intentional in their curriculum development, how they frame content for participants, and how intervention facilitators interact with participants. Suggested curriculum topics included holistic health (i.e., mind, body, and spirit), differentiating the differences between religion and spirituality and emphasizing the benefits of the latter, and including a history of African and African diasporic spiritualities. Participants also discussed the importance of not making the program religious but helping Black SGL male attendees understand, emotionally and intellectually process, and heal from homonegative religious trauma. One participant (107) recommended, … let them know that they were created the way they were supposed to be created. There’s nothing wrong with them … and that … we are all gifts … from God, so let’s use everything to the best of our abilities. You know … there’s no defect … in us.
Participants also noted that some Black SGL men would need to unlearn and redefine who they are in their bodies outside of sexual spaces. One participant (1038) stated, “… you’re gonna have to help people to re-educate themselves about who they are and what’s allowable where their bodies are concerned.” Another (258) shared, There is absolutely nothing more beneficial health-wise than a hug. And there are people that, literally, don’t get that, don’t know what they are. … especially as [same]-sex-loving men of African descent, you will find that people are not familiar with … love or any type of touch that isn’t sexual. So I do believe that that’s an important part of teaching people not only to love their bodies, but to, to keep their bodies healthy.
Participants recommended using books, storytelling with lots of sensory words, and intergenerational discussions to facilitate conversations. Afrocentric, Black feminist, and Black queer perspectives were mentioned as potential theoretical frameworks to guide curriculum development.
Participants emphasized that the people who facilitate the intervention should not be judgmental, not force participants to believe or act in any prescribed way, avoid making assumptions about the participants’ lives, and respect the within-group diversity of Black SGL men. One participant (304) summed it up when he said, … we’re not monolithic. We do not go to Pentecostal churches. You know, you have Blacks. You have African traditions. You have Islam. You have Hindu. You have Buddhists, practicing Buddhists. You have nontheistic, so like ethical culture. … Black thinkers, which that-- for some reason, that does kind of fall within the spectrum of a religious movement. Freethinkers. Black freethinkers. Um, we’re not monolithic, and our backgrounds are significantly varied. Um, so be aware and, and make space.
When asked about what activities the intervention should include, there were a multitude of responses. Although participants suggested various activities, all of them were meant to help Black SGL men harness the power of spirituality for their well-being. Meditation was mentioned the most along with other mind–body practices. One participant (303) stated, It should look like, uh, meditation. It should look like a bit of yoga. It should look like anything that … gets your body in tune … spiritually, mentally, and emotionally-- as physically in tune with yourself but also with the environment that you’re in.
Another participant (197) suggested activities that focus and quiet the mind. He said, … you need, like, a more contemplative space, whether it’s journaling or prayer or, like, listening to music that helps you … Forget yourself or lose yourself sounds weird … I don’t really want to say entrancing. But, like, music that, that helps you to be open rather than, um, hyperaware and anxious …
Other activities that were suggested included lots of discussion, spiritual reading groups, affirmations, using singing bowls, having quiet time, watching videos and media about spirituality and health, listening to music, free writing, walking, laughing, and using psychedelic mushrooms. Another participant (244) suggested artistic methods of connecting to oneself. He said, … people don’t consider art therapy to be spirituality, but it is. From a culture where a lot of our history was oral where it couldn’t be written or it’d be destroyed, there are a lot of things that we express artistically, but it’s really our spirit. Poetry is a way for me to be able to express what’s going on in my spirit to the world.
Participants also advised that attendees be granted easy access to as much information as possible related to spirituality and health, including referrals to health services.
What Is the Potential Impact of a Spirituality-Based Health Intervention on Black Same Gender Loving Men’s Lives?
Participants’ perspectives about the potential effect of a spirituality-based health intervention are illustrated by theme 3.
Theme 3: Multilevel Positive Holistic Impact
This theme captures that many participants believed that a spirituality-based intervention can potentially have a positive holistic impact on Black SGL men’s lives at the individual, interpersonal, and structural/societal levels. Black SGL men in the study expressed that (a) spirituality can help Black SGL men prioritize self-love and self-care by attending to their individual mental, physical, financial, and spiritual health; (b) spirituality helps Black SGL men connect with something greater than themselves and develop healthier relationships with others; and (c) spirituality provides a framework for addressing oppression and its associated negative outcomes. One participant (061) expressed that a spirituality-based health intervention could help Black SGL men with “… unlocking healthier ways of living and being.”
Highlighting the potential holistic impact, Participant (1031) shared that he thought having a spirituality-based holistic health intervention that was designed specifically for Black SGL men could make them feel renewed. He said, Have you ever seen The Wiz? … When you get to that end part where … it … kind of pans out, and they sing that Can You Feel a Brand New Day, and they peel off the skins. Yeah. I feel like that would be the impact.
Another participant (059) reported that he believed the intervention could definitely give a more positive outlook to men who are feeling unheard … or seen. … it would give space for new opportunities to meet people, and to do stuff. And to just … to live a normal day-to-day life without the stress of whatever illness you’re going through, or whatever trouble you’re dealing with.
Participant (1202) emphasized one benefit of a spirituality-based health intervention is helping Black SGL men enhance their spirituality which is connected to increased self-worth and better self-care. He said, … the stronger [Black SGL men’s] spiritual connection, the more likely they are to have a higher, um, sense of worth. And when you have a higher sense of self-worth, you’re more likely to go to the doctor, to take your medicine, to protect yourself, to do behaviors that are healthy and not unhealthy, right, uh, when you have a sense of spirit because, you know, spirit is all around you.
Several participants highlighted that a spirituality-based health program could help Black SGL men use their spirituality to improve their physical and mental health. Participant (123) noted that “… spirituality encourages me to want to have a healthy body. Um, and so therefore, it, it does. It plays a huge role, um, in who I am.” Participant (1016) also shared, “… I definitely feel like God helps me make decisions in who I want to be with … in bed …” Several participants reported that they believed spirituality could be used to decrease depression, anxiety, loneliness, stress, shame, anger, suicidality, and drug use (see the Supplemental Material for additional details).
Increasing spirituality was also noted as a way for Black SGL men to improve their interpersonal relationships. Participant (1004) disclosed, I think the … biggest thing would be interpersonal relationships, whether it be romantic or otherwise. Um, if you feel like everyone is connected to God in some way or connected to the universe in some way, we are all one, you feel a greater sense of duty also to treat them with respect and … namaste to the god in you if you’re sort of really living that and not just thinking it’s a yoga phrase, then, um, your relationships benefit greatly.
One participant (038) noted his belief that if Black SGL men could harness their spirituality, they could better navigate oppressive healthcare systems. He offered, I think spirituality can be used to … help us overcome our problems by creating a framework for us to be able to have something to fall back on. I think the healthcare system in general is very heteronormative and is very White and patriarchal. The providers fit that mold. The systems fit that mold. And nothing is really created or ascribed for us to be able to be successful or navigat[e] those fears. But we’ve always historically and traditionally had a spiritual faith base or spiritual foundation. And so incorporating those two will be a beneficial means to be able to ensure that there’s a safer space for us to access and navigate those systems.
Overall, Black SGL men expressed that they believed that enhancing their spirituality could be beneficial for many facets of their health. A spirituality-based health intervention has promise for improving this group’s health.
Discussion
This study utilized a hybrid approach to thematic analysis that intentionally combined elements of codebook and RTA to generate and makes sense of patterns of meaning across a sample of Black SGL men related to their recommendations for developing a spirituality-based health intervention. The results of the study fit well with the guiding theoretical framework and approach of the study (i.e., OCT-SGM and PAR) in that they illustrate Black SGL men’s (1) centering of spirituality and themselves to achieve better health; (2) addressing intersectional oppression; and (3) exercising power in sharing their stories. Our findings indicated that Black SGL men believe that currently available health and spiritual services are inadequate and have perpetuated harm in their communities. Participants expressed a need for a widely accessible spirituality-based health intervention that honored their lived experiences, treated them with respect, and incorporated several activities that helped them harness their spirituality to enhance their holistic health. Most health interventions have largely excluded or failed to center the intersectional realities of Black SGL men (Fish et al., 2016; Huang et al., 2020). The current study represents sorely needed attention to the holistic health of Black SGL men beyond the context of HIV. Findings from the present study can be used to address multiple health concerns among Black SGL men.
Although this study is unique in scope, its findings are supported by extant literature. For example, participants suggested a comprehensive spiritually-based intervention addressing multiple factors, including individual, community, and institutional, would be most effective. This finding is in line with previous health promotion research positing that multilevel interventions have the potential to have maximal impact on health behaviors and health outcomes (Glanz & Bishop, 2010). Also, participants’ calls to be seen accurately, recognized as more than just their sexual identities, have been echoed in previous research critiquing the oversexualization of Black gay men, and Black men in general, throughout history (Jones & Ferguson, 2020).
Study participants provided diverse preferences for intervention design. For example, participants differed when discussing the duration of a spiritually-based intervention; some suggested a short-term intervention, while others recommended a longer-term, ongoing intervention as the most effective approach. This finding shows that the needs of Black SGL men are diverse, and so offering a range of interventions tailored to individual needs may be most useful. Similarly, a nuanced understanding of the relationships between religion and spirituality should also be considered when developing and implementing spiritually-based interventions for Black SGL men. Theme 1 summarizes participants’ beliefs that while religious spaces have been sites of harm, they also have the capacity to serve as healing. This observation suggests that the affirmation that accompanies healthy spirituality can be realized through more traditional Black Christian and Muslim pathways for some Black SGL men. This finding highlights that not all Black SGL men choose to eschew Christian and Muslim Black religious spaces, but rather find comfort and community in traditional practices (e.g., music and liturgy) when paired with inclusive theologies. That said, the experiences of Black SGL men are varied, with many choosing to leave religious communities that have been antagonistic to them, opting for personal spiritual practices that affirm them as complete beings (Miller, 2007).
Implications for Future Practice
Using the recommendations of the participants in our sample can result in the development of holistic health interventions that would be distinct in the psychological, public health, and wellness spaces for Black SGL men (Gilbert et al., 2009). Spirituality-based interventions would be informed by African-centered principles, strengths-based with a focus on well-being, and target multiple health and social conditions. African-centered psychology emphasizes the mutually influential relationship between spirit(uality) and the human experience/material world (Awosogba et al., 2023). An intervention developed based on the recommendations in this paper would integrate a core component of African-centered approaches (i.e., spirituality) to address first and foremost spiritual consciousness and alignment as the pre-requisite for mental, physical, and relational health in the midst of intersectional oppression. The goal would be to increase holistic health and well-being, not just promote a decrease of symptomology or absence of disease. There is evidence that spirituality can help Black SGL men (a) achieve mental and physical health and (b) harness their spirituality to cultivate meaning making and self-knowledge to thrive in the face of oppression (Lassiter & Fulton, 2024; Lassiter & Mims, 2022). The combination of these features represents a potentially powerful holistic health intervention created for and by Black SGL men.
Our findings have both strengths and limitations to consider. One strength is that we recruited a national sample of diverse, spiritually conscious Black SGL men who provided perspectives that may be relevant for men across a range of U.S. geographical regions. Another strength is the high level of reflexivity of the researchers as well as the cultural insider status of the lead researcher that guided study design and data interpretation. Our findings demonstrate intersectional generalizability in that they illuminate the particular ways of meaning making related to health concerns, spirituality, and culturally appropriate treatments for intersectionally oppressed people (Fine et al., 2008). It also possesses provocative generalizability in that through the co-construction of our findings, the researchers and participants provoke scientists and interventionists to imagine a spirituality-based holistic health intervention currently not in existence (Smith, 2018). One limitation is the cross-sectional nature of the analysis that does not necessarily capture the ways in which recommendations might change across time. Another limitation could be that we did not query participants about how the occurrence of the COVID-19 pandemic, which happened during the data collection phase, could have influenced their recommendations. These strengths and limitations should be considered.
This study provides recommendations for a spirituality-based health intervention for Black SGL men that has the potential to holistically impact their lives. The intervention does not center HIV, sexual health, substance use, or other disease and deficit-based outcomes. Instead, its target is increasing mental, physical, relational, and financial well-being in the context of intersectional oppression and cultural strengths. If well implemented, the recommendations could lead to an (or intervention) that cultivates new opportunities for decreasing inequities and enhancing expansiveness among Black SGL men.
Supplemental Material
Supplemental Material - “Unlocking Healthier Ways of Living and Being”: Black Same Gender Loving Men’s Insights into Developing a Spirituality-Based Holistic Health Intervention
Supplemental Material for “Unlocking Healthier Ways of Living and Being”: Black Same Gender Loving Men’s Insights into Developing a Spirituality-Based Holistic Health Intervention by Jonathan M. Lassiter, Kainaat Anwar, Khanh Pham, Muraiye Pierre, and Stacy W. Smallwood in Qualitative Health Research
Footnotes
Acknowledgments
The authors thank Ashley Foye and Caitlyn Clarke, former members of the SPIRiT Lab who contributed to participant recruitment, enrollment, and interviewing for the Spirituality and Stress Study, which provided data for this manuscript. The authors thank all participants who shared their stories with the research team, allowing them to highlight their voices in the goal of decreasing health inequities among racial and sexual minoritized people.
Author Contributions
Jonathan M. Lassiter conceptualized the study that provided the data for this manuscript; supervised data collection; conceptualized ideas for this manuscript; led data analysis; and contributed to data visualization and writing the original draft of the manuscript. Kainaat Anwar conducted individual interviews with participants and contributed to writing the original draft of the manuscript. Khanh Pham conducted individual interviews with participants and contributed to writing the original draft of the manuscript. Muraiye Pierre contributed to data visualization, data analysis, and writing the original draft of the manuscript. Stacy W. Smallwood contributed to writing the original draft of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jonathan M. Lassiter is the principal investigator of the study and was supported by faculty research startup funds. Kainaat Anwar, Khanh Pham, and Muraiye Pierre were supported by doctoral graduate assistant funds. Stacy W. Smallwood reported no funding for this project.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.