
Abstract
Food allergy (FA) is a potentially life-threatening condition which is associated with poor quality of life and psychological distress in patients and caregivers. Although FA is often seen as a condition that affects children, increasing numbers of adults have FA, either as a condition they have grown up with or they were diagnosed as an adult. No recent research has explored the lived experiences of adults with FA and how they manage this condition. In response, this study aimed to qualitatively assess the current lived experiences of adults in the UK with FA, and how they manage this condition. Adults aged 18 years or over, with medically diagnosed FA, living in the UK were recruited through patient organisations and interviewed (n = 22). Data were analysed using template analysis. Two main themes were identified from the data. The first theme explores the influence of FA on the participants’ lives, in particular on their ‘psychological’ and ‘social’ well-being. The second theme unpacks the strategies participants employed to cope with and manage their FA, specifically participants’ deployment of ‘avoidance’, ‘control’, ‘self-monitoring’, and ‘adaptation’ to manage their FA and their anxieties around it. Clearly, FA has a profound, ongoing effect on the lives of adults. Few adults in this study were able to access any support to manage their FA and accompanying anxieties. Ways in which effective support can be made available to adults with FA must be identified and implemented.
Background
Food allergy (FA) refers to an abnormal, and potentially life-threatening, immune response following consumption of a particular food (Santos et al., 2023). Symptomatology can be varied and ranges from relatively mild symptoms such as itching, tingly mouth, vomiting, and hives; to severe reactions such as anaphylaxis. Anaphylaxis affects multiple systems and can lead to breathing difficulties, a rash, vomiting, decreased blood pressure, and loss of consciousness, and, in rare occasions, is fatal (Hammond, 2023). At present, there is no cure for FA, although a range of desensitisation-based treatments appear effective for increasing thresholds for immune-reactivity to food allergens (Sindher et al., 2022). As such, the primary pillar of FA management involves strict avoidance of the food and preparation to administer rescue medication as needed (e.g., anti-histamines for mild reactions and adrenaline/epinephrine for more severe reactions including anaphylaxis) (Muraro et al., 2014).
FA is often diagnosed during infancy and early childhood and those with allergies to cow’s milk, egg, or wheat may outgrow these. However, this is less likely for allergies to peanut and tree nut, where many children have these for life (Savage & Johns, 2015). Systematic reviews estimate the self-reported lifetime prevalence of FA in Europe to be between 0.4% and 6% (Nwaru et al., 2014; Popov et al., 2020; Spolidoro et al., 2023). Furthermore, emerging evidence from the United States (US) indicates that among respondents with ‘convincing FA’ (defined as self-reported symptoms to specific allergens that were consistent with IgE-mediated reactions), 27% developed their first FA during adulthood and 48% reported developing at least one of their convincing FAs as an adult (Gupta et al., 2019). This indicates that for many, FA is not isolated to childhood and must be managed throughout adulthood.
Considerable research effort has been directed to explore the experiences of children with FA and their parents. Evidence from systematic and scoping reviews universally indicates the detrimental impact of FA on quality of life (QoL), and management of FA is associated with increased burden, isolation, and significant FA-specific anxiety (Golding et al., 2021, 2022; Westwell-Roper et al., 2022). Research centred on the experiences of adults with FA is less abundant, but accumulating evidence from QoL surveys indicates the constant vigilance required to manage FA is a significant burden irrespective of age. For example, university students with physician-diagnosed FA in the US reported higher levels of anxiety and depressive symptoms than those without FA (Chen et al., 2020). Similarly, 31% of adults with physician-diagnosed peanut allergy surveyed in the United States agreed that FA interfered with their life ‘very much’ or ‘completely’ (Nowak-Wegrzyn et al., 2021). Nowak-Wegrzyn et al. (2021) reported all domains of health-related QoL were significantly worse for people with peanut allergy than population norms, with the impact on psychosocial health identified as being more problematic and deleterious to well-being than physical health.
In a multi-national study on adults with FA and caregivers of children with FA across more than 20 countries, 68% of the 1329 adults responding to the survey reported experiencing psychological distress related to their FA (Knibb et al., 2024). Of the 21 types of distress reported, anxiety about an allergic reaction (reported by 64%) was the most common. Sadness about FA, fear of trusting others, and bullying were among the other types of distress reported (Knibb et al., 2024). Adults with FA also incur substantial economic costs (Warren et al., 2020).
Qualitative research has further elucidated the experiences of adults living with FA. Participants have suggested General Practitioners (GP) are typically not well informed about FA, frequently dismiss or minimise patient symptoms, and act as gatekeepers to the limited number of specialist services (Peniamina et al., 2014). Once diagnosed, the demands of managing FA for adults are considerable. Eating out and other food-related social events can be particularly burdensome (Peniamina et al., 2014) with participants facing potentially unwanted attention from fellow diners and accusations of being an “attention seeker” or an unjustifiably “fussy eater” (Leftwich et al., 2011; Nettleton et al., 2010; Tsoumani et al., 2022). Research on young adults at college in the United States (US) reported their feelings of fear, anxiety, and disconnection, amplified as they respond to interpersonal, environmental, and intrapersonal changes in their lives (Lee et al., 2023; Schelly et al., 2022; Yuan et al., 2024). Two studies have explored the experiences of adults with anaphylaxis, including anaphylaxis to food (Knibb et al., 2019; Walklet et al., 2018). In both studies, adults discussed the fear and anxiety caused by anaphylaxis and the need to maintain some control over their environment to manage their allergy.
Further insight and support for findings from previous research has been provided by a recent study exploring the lived experience of adults, teenagers, children, and caregivers of children with multiple FAs in the United States (Ciaccio et al., 2024). In semi-structured interviews, adults described the loss of spontaneity from having to avoid foods they are allergic to, which required constant effort. Adults discussed their stress and anxiety and how managing multiple FAs changed the way they interacted with others, with the need to speak up about their allergies and trust others when participating in events involving food.
Despite this more recent attention on adults, these qualitative studies have focused specifically on a younger age range or those managing multiple allergies or anaphylaxis to a range of different allergens, not just food. Some research, particularly on eating out, was carried out some years ago and the landscape for FA has changed over this time. For example, the introduction of legislation in the United Kingdom (UK) in 2014 regarding information required on allergens for prepacked food and mandatory allergen labelling on non-prepacked food (such as that sold in cafes and restaurants) has changed the experiences people with FA have when eating out (Begen et al., 2018). In the present study, we therefore aimed to explore the current lived experiences of adults in the United Kingdom with FA and how they manage this condition. We addressed some of the gaps of previous literature by not having any restrictions on age of the adult, how many foods they were allergic to, or severity of their reactions.
Methods
Participants and Recruitment
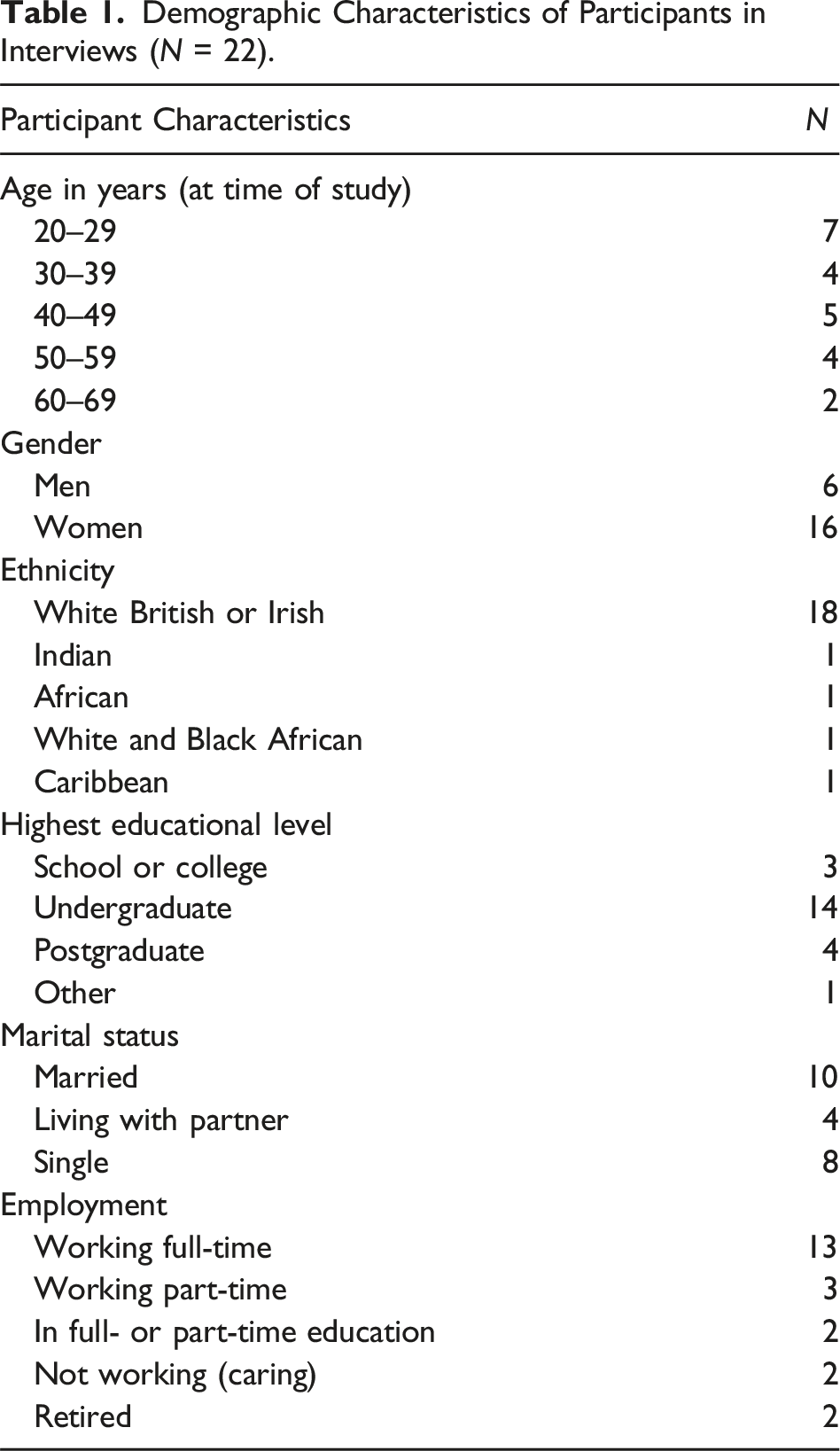
Participants were recruited as part of a larger mixed-methods multi-phase Global Access to Psychological Services for Food Allergy (GAPS) study examining the psychological health experiences and needs of adults living with FA and caregivers of children with FA. Participants for this interview study had to have a self-reported diagnosis of FA by a medical professional, live in the United Kingdom, and be aged 18 years or over. The study was advertised by the patient organisations Allergy UK and Anaphylaxis UK. Prospective participants were asked to click a link to an online participant information sheet and if interested, complete an expression of interest form consenting to be contacted and interviewed by the research team. These participants were then emailed a link to an online consent form and a short questionnaire to capture demographic information and FA characteristics.
Demographic Characteristics of Participants in Interviews (N = 22).
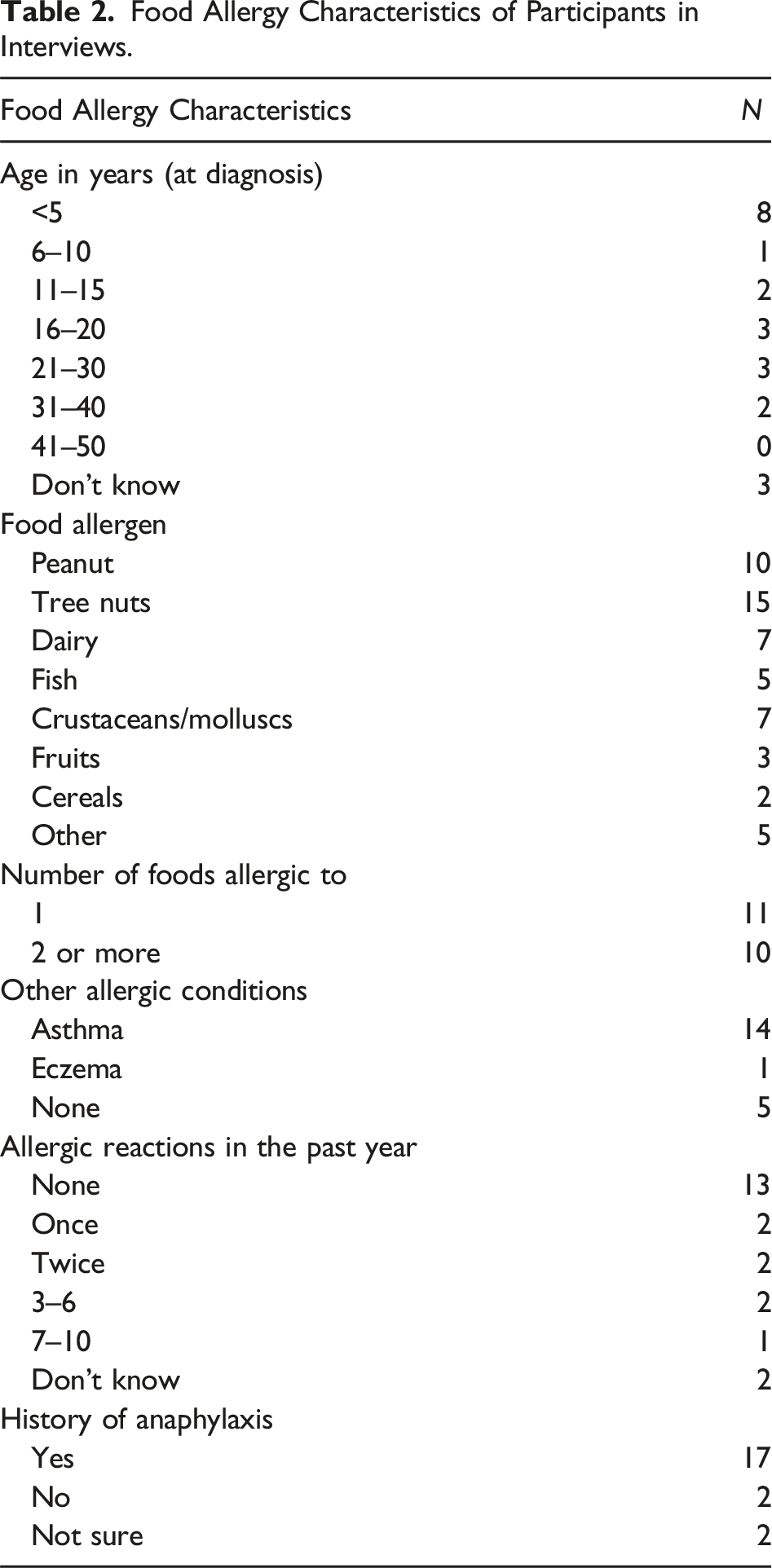
Food Allergy Characteristics of Participants in Interviews.
Data Generation
An interview schedule was devised, informed by the current literature. Questions explored the impact that FA has upon an adult’s life, how they cope with FA-related distress, experiences with healthcare professionals (including GP, dietician, nurse practitioner, and psychologist), and resources to improve management of their FA and/or their FA-related anxiety (see Supplemental File). Consistent with semi-structured interview guidance (Kvale, 1983), the schedule guided conversation but was applied flexibly to allow for follow-up questions to unexpected responses. Interviews were conducted online using Microsoft Teams® by masters students (1 male, 1 female) trained in qualitative methods with a background in FA psychosocial research. Participants and researchers were unknown to each other prior to interview and researchers had no personal experience of FA. Interviews lasted between 10 and 43 minutes (mean = 28 minutes), were audio recorded, and transcribed verbatim with identifying features removed. Participants were assigned pseudonyms. All data were stored securely, compliant with data protection laws. All participants received a £10 e-voucher for their time.
This study was given a favourable ethical opinion by Aston University Research Ethics Committee (REC approval number #1819). All participants gave informed written consent using an online consent form and verbal consent at the start of their interview. Participants were debriefed, and advised they could withdraw at any time during the interview and up to 14 days afterwards. No participants withdrew from the study.
Data Analysis
Data were analysed using Template Analysis (Brooks et al., 2015). The analysis was performed by CR, an experienced qualitative researcher (PhD) with expertise in health and illness experience (but not FA specifically) and RCK, an experienced Health Psychologist and expert in FA. Neither had a personal diagnosis of FA. CR read all interview transcripts with adults living with FA and selected three, which captured a range of participant characteristics, on which CR and RCK then performed preliminary coding. Three topics served as tentative a priori themes to organise the original template and guide analysis, based on the aims of the GAPS study: (1) the psychological impact of living with FA; (2) what support had been provided and accessed and the perceived utility of the support(s); and (3) how support could be improved. After preliminary coding, meaningful clusters were identified and discussed and an initial coding framework was agreed upon. To do justice to the richness of the data generated, the framework was expanded beyond the three a priori themes to ensure participants’ wider experiences of living with FA and how management intersected with and affected various aspects of their life. CR applied the template to five more transcripts, and any modifications or additions were made and agreed upon before it was then applied to the full data set for adults (see Supplemental File for the template). During this analysis, the researcher kept a reflective diary to note any potential biases for discussion. The researcher did not have expertise in FA or personal experience; however, knowledge of previous research in the area may have influenced the analysis process and this was noted and discussed. The results and interpretation of quotes were circulated for review by the multidisciplinary GAPS team (which includes psychologists, allergists, methodologists, primary care physicians, health services researchers, patients, and patient organisation representatives). Any possible misinterpretations were discussed within the team and transcripts and audio recordings were reviewed where needed. This process occurred iteratively until there was consensus agreement on interpretation of the results from the team. Frequencies were calculated for demographic and FA information.
Results
The results presented here concentrate on two main themes from the template analysis. The first theme ‘The Psychosocial Burden of FA’ explores the influence of FA on the participants’ life, and in particular the effect on their ‘psychological’ and ‘social’ well-being. The second theme ‘Coping with Uncertainty’ unpacks the strategies participants employed to cope with and manage their FA. Specifically, attention is afforded to participants’ deployment of ‘avoidance’, ‘control’, ‘self monitoring’, and ‘adaptation’ to manage their FA and their anxieties around it.
Theme 1: The Psychosocial Burden of FA; “FA Makes It Very Difficult to be Spontaneous”
Participants indicated that FA affected all aspects of their life. In particular, the influence on their ‘psychological’ and ‘social’ well-being was the most salient and frequently endorsed by participants in this study (see Figure 1). Thematic map of the burden of living with food allergy in adults.
Psychological Well-Being
Ensuring their safety while eating presented participants with a significant and enduring challenge that resulted in considerable fear around food preparation and consumption, as Sian reflected, “it’s kind of a lifelong fear that’s always in the background and sometimes [it’s] very prominent.” Participants’ fear of dying, “you know you get really worried that you’re going to eat the wrong thing and die” (Monica), or having another reaction, “I suppose the other thing is the impact on my life is when I do have an allergic reaction and just how terrifying that is for me and the people around me” (Dawn), was palpable, irrespective of participant age, time since diagnosis, number of allergens, or severity of reaction.
The uncertainty surrounding food safety was a potent and perpetual peril for participants and they frequently referenced experiences where they had been confronted by the very real threat of anaphylaxis. For some, these were “close calls,” and consumption of their allergen was narrowly avoided, as Daniel explained, we were getting some fish and chips and I casually mentioned that I have a nut allergy and they said, “well you can’t have anything we serve here; we fry stuff in the chip oil which has got hazelnut in it.” So yeah, even stuff like that, places where you’d never think you know has nuts sort of thing, but it seems to be everywhere.
Participants who had lived with FA since childhood were not immune to feeling anxious about their FA. On the contrary, they explained that experiencing an anaphylactic reaction then triggered considerable fear around food and a more cautious and indeed anxious approach to management. Heather’s anecdote typifies this experience, [as] I’ve gotten older and as these, I guess for me appeared to have more severe reactions, I’ve got far more cautious and worried. It completely changed the way that I live my life.
Despite having lived with FA all their lives, these participants reflected that the transition to adulthood and independence was a “tricky time” for managing their FA, with most becoming overly reliant on avoidant behaviours that isolated them physically and socially, “depending on how things were going in my life at certain times I’d avoid going out with my friends because I was anxious” (Priya), and for others marked an ongoing struggle with their mental well-being, “it’s made life so unbearable for me” (Nathan).
There were marked differences in the ramifications of their anxiety among participants. For example, some developed social anxiety that resulted in withdrawal from social situations which “can be quite an isolating thing” (Isla). Others approached their fears head on, “it doesn’t hold us back because I do still do it [go out to places food is served]” (Monica), while others reported feeling gaslit and began to question whether their condition was as severe as they believed it to be, “I just wanted to know if I was being OCD [obsessive compulsive disorder] with all my worrying and anxiety” (Andrea).
Rosie, who experienced angioedema (swelling) on her face, described how FA had robbed her of her self-confidence and self-esteem which had resulted in her withdrawal from family life, when it’s bad I can’t look you in the eye, like during [COVID-19] lockdown I wouldn’t even FaceTime with my family because I didn’t want them to see me.
She went on to explain that she avoided being photographed on holiday by offering to take the photograph but reflected she was “missing out on making memories” as a consequence.
Social Well-Being
The social aspect of FA was often described as being the most painful and challenging for participants to manage. As reported in the preceding sub-theme, at some point in their lives, participants experienced anxiety around food which culminated in their withdrawal from social situations and often led to feelings of loneliness and isolation. Despite this, participants were determined to have rich and fulfilling social lives but noted this was often difficult because of societal attitudes towards FA. I suppose it’s people that I’ve just met for the first time or some people even that I’m friends with can be kind of like brush it aside like “oh it’s not that big a deal” or “if you eat this, nothing will probably happen.” I don’t think they realise that it is deadly. (Kate)
Most participants noted there were people in their lives who do not take their allergies seriously, “it doesn’t feel like an illness it feels like a bit of a joke” (Monica), or else “they think you’re being picky” (Sian) which made communal eating uncomfortable at best, and risky at worst. Having an FA necessitates disclosure if one is to access safe food. Yet, many participants emphasised the acute embarrassment they felt outing themselves as having an FA. This embarrassment was discussed as being most pronounced during adolescence and young adulthood, but for some participants, it endured throughout their life and was something they still struggled with, “even as an adult, I do understand that sort of level of embarrassment and that kind of nervousness around it” (Sian).
The root cause of the embarrassment varied across participants. Some were concerned they were “putting other people out” (Lucy), others felt awkward displaying their difference, “you desperately want to just fit in and not have anything that makes you unique” (Lara). Some resented the fuss and questions that inevitably followed, “I’m mortified I just don’t like, I hate the fuss it causes and the questions it leads to” (Shannon), and some recalled “embarrassing situations (…) in smart restaurants and the waiter has brought out the catering size ice cream box to the table with the lid so that I could check the ingredients for myself” (Dawn).
Although most participants reported they were well supported by friends and family, there were nevertheless points of tension within families. For example, Isla was concerned her partner was annoyed they were unable to go to small independent restaurants and instead returned to the same chain restaurants time and again, and both Monica and Daniel struggled to enjoy Christmas because of the proximity to nuts at social gatherings during this holiday. However, none of the participants recounted an argument or rift with family members as a result of their FA; instead, they channelled their efforts into (re)educating them on the risks or else accepting that, at present, “there is a lot of misunderstanding about allergies and how they can affect a person, not just physical health but mental health” (Kate) and so they determine to “just get on with life” (Sian).
A point that was consistently identified across participants was that their life opportunities had been limited because of their FA, “it can be life limiting and you have to work quite hard to make sure it isn’t” (Lara). This was most often framed in terms of limited dining options, “it can limit your options as to what you can and cannot eat so obviously that is missing out as well” (Priya) or restricted travel opportunities, “it reduces choice of where you can travel (…) it makes it very difficult to be spontaneous” (Lara). Participants longed to experience the world more fully but lacked the confidence and appropriate support systems to do so.
Theme 2: Coping With Uncertainty; “You Have to Be Vigilant, Constantly Vigilant, Which Can Be a Bit Draining”
This theme captured the ways in which participants coped with FA as a physical condition and the steps they took to protect their mental and emotional well-being. This included avoidance strategies to help manage their FA, strategies to maintain control over their environment, self-monitoring, and positive adaptation. In particular, this theme seeks to unpack coping strategies that are recommended and valued but are mentally and emotionally demanding and have unintended consequences that affect well-being.
Avoidance
Avoidance of allergens and carrying an adrenaline/epinephrine autoinjector is the primary treatment for FA, and ‘avoidance’ was endorsed by all participants as their main strategy to cope with and manage their FA. However, participants discussed the lack of guidance from healthcare professionals in how to do this. As Agatha succinctly summarised, “[I was told to] just stay away from what you can’t eat and that was it.” While some framed avoidance matter-of-factly, “I guess the main strategy is I’ve just avoided [their allergen] (…) and I guess I’m not sure what else I could have done really” (Heather), for others avoidance was more complex, “the doctor’s always just like, ‘you have to avoid nuts’ and I’m like, ‘well that’s harder than you think, you try it’” (Martha).
Most participants explained avoidance was easier within their own homes but became more difficult and stressful when eating outside the home. In an effort to counter the anxiety, worry, or embarrassment they experienced or anticipated when eating communally, participants reported their avoidance behaviour extended beyond avoidance of their specific allergen. Common strategies included avoiding specific cuisines because they frequently include peanuts, tree nuts, fish, and/or shellfish in their dishes, “I just avoid Indian food, Asian, Thai anything sort of like that” (Andrea); unfamiliar dishes or cuisines, “just any cuisine that I don’t know I wouldn’t take the risk, even if I saw an allergen list” (Andrea); travelling to particular countries such as India or Thailand, “there are some places that I just don’t think I would travel to because of the risks” (Lucy); social or work events, “if it’s a work do [work event] where maybe there’s a dinner involved I might avoid it (…) [sometimes it’s] easier to avoid something than it is to go and feel anxious and uncomfortable about it” (Isla); and avoiding conflict with friends, family, and colleagues by attending meals but not eating, “I’ve been to places where I’ve not been able to eat anything” (Rosie).
Participants acknowledged that avoidance had become a de facto response to uncertainty and ameliorating their anxieties whilst eating out but that this strategy was not without consequence, as Sian reflected, “I’ll make changes which really helped me but have a knock-on effect of slightly isolating me.” Indeed, for some these anxieties were insurmountable and had resulted in them being unable to advocate for themselves or negotiate their safety in social situations. I didn’t want to be the person who goes “oh no, I can’t eat that can we go somewhere else.” I suppose that it’s really led me to people pleasing and going along with something even though it scares me. (Kate)
Control
In order to navigate the risks and uncertainty inherent to living with FA, participants developed techniques to control their environment and others which permitted them to ameliorate their anxiety and engage more fully in life. For example, participants were vigilant about what products entered their house, “it’s checking ingredients of everything that we buy in the house of course (…) it’s a permanent struggle to manage it really” (Richard), and most reported that keeping their home free of their allergen(s) provided them comfort and confidence to enjoy their meals. Although this was framed as a necessity to keep themselves safe, some participants such as Shannon lamented the cascading impact this had on her family, which were difficult to reconcile: “you make choices and you keep yourself as safe as possible, but it does completely change things, like my husband hasn’t eaten fish for over 20 years, my son has never tasted fish.”
Negotiating shared living spaces presented unique logistical and social challenges. Sophie, for example, noted, “when I moved into a shared house, so I had my own crockery and cutlery. You know, I was trying to keep safe,” and Sian likewise approached workplace kitchens cautiously, “so little things like I take my own mug to work so I’m not using one in the kitchen because people don’t clean them very well.” On the surface, these may appear to be small strategies participants employed to control their environment, but they were often fraught with anxiety that “people might feel like [it] excludes them somehow” or else that it would be viewed by others as “making a fuss.”
Advanced planning and preparation were also prized strategies, particularly when eating out. For example, participants frequently reported viewing restaurant menus online, carrying emergency food supplies in their bags, and returning to restaurants and selecting dishes they perceived to be ‘safe’ in an effort to mitigate their anxieties eating out. Trusting others to purchase, prepare, and cook their meals was a perpetual challenge for almost all participants. Kate, for example, explained that she had so frequently been misled by people handling her food she had lost confidence and trust in what they said which had “spread into other parts of my life and I feel that when somebody says something I can find it difficult to believe them or trust them.” This degree of mistrust was not reported by all participants, but many reported watching over kitchen staff to alleviate the anxiety that stemmed from not being able to trust their food was being prepared safely, “I manage it because I can see it, I can literally watch them [laughs] watch them doing it” (Monica).
While mistrust and anxiety were particularly acute within the context of restaurants and takeaways, participants also continually monitored and challenged the behaviour of their family and friends: I have to remind my mom, you know, don’t cook with this and this or you know, just double check the ingredients list (…) [it] feels like you’re imposing yourself on other people, which is a bit difficult at times. (Sian)
Participants described the constant effort of having to negotiate their own physical safety without causing offense to their friends, family, and colleagues as tiring, which Sian concluded “you have to be vigilant, constantly vigilant which is a bit draining.”
Self-Monitoring
For some participants, the “constant vigilance” required to manage their FA had made them “hyper aware of food and what you’re eating” (Dawn) such that they admitted to being “a little OCD about checking [labels]” (Andrea). While participants were cautious about using the term OCD when they had not received a formal diagnosis, it served to signal their awareness that their checking and controlling behaviours were perhaps maladaptive. As Monica described, constantly checking the ingredients of something when you’ve already checked it, but you know you sort of question yourself because you don’t want to make a mistake so that sort of thing is day-to-day and not quite 100% normal.
Among some participants, obsessive checking behaviour extended to their own body which catalysed and compounded their health anxieties, as Olivia recounted, “I was just finding it really hard to not obsess about every tiny thing my body was feeling which I think stemmed from my allergies.” While those affected were aware cognitively there is a “difference between anaphylaxis and panic, I think they can feel very similar” (Lara), they reflected, “I think mainly my issue is around the anxiety and being able to tell the difference between anxiety or if it is an allergic reaction” (Lucy). Most participants had been unable to access appropriate psychological care to support the development and use of more adaptive coping strategies.
Positive Adaptation
Although less frequently discussed, participants did share examples of positive adaptation that had permitted them to live life more fully. In particular, participants highlighted that going on self-catered holidays (accommodation with a kitchen so you can prepare and cook all of your own meals) enabled them to feel safe and in control whilst in an unfamiliar environment, “I do self-catering on holiday a lot, we have a motor home, so we go camping” (Isla), and focusing on outdoor pursuits provided valuable family time and connectivity that did not rely on food, “we’re quite into being outdoors and doing outdoorsy things you know like biking and walking which don’t involve being inside and being around food” (Monica). Technologies such as translation services and digital allergy cards also opened up travel possibilities that had been hitherto fraught with anxiety.
Discussion
This study provides novel findings regarding the experience of living with FA for adults, how it affects their day-to-day life and how they cope. In an in-depth exploration involving semi-structured interviews, adults discussed two main areas in which FA affected them: the psychosocial burden of FA and coping with the uncertainty of FA. The psychosocial burden of FA was the most important factor affecting the daily lives of adults and one they spoke about most often across all interviews. Adults spoke about the anxiety and fear that is accompanied by FA and the effort required to avoid allergens that may cause a serious and potentially fatal reaction. This anxiety has been reported in the literature for children and adolescents with FA and for caregivers of children with FA (Golding et al., 2021, 2022; Westwell-Roper et al., 2022). It has also been reported in quantitative research, with Knibb et al. (2024) reporting FA anxiety as the type of distress endorsed most frequently by adults in their survey of adults with FA. Our more in-depth qualitative study provides further insight into why the impact of FA on psychological health does not diminish as someone grows older, with adult participants explaining that FA is an ongoing struggle, a finding supported by recent qualitative research by Ciaccio et al. (2024).
Adults in the present study also spoke of a lack of self-confidence and self-esteem, with some developing anxiety about social situations, leading them to withdraw from events where food is involved. If they did eat out, adults spoke of the embarrassment of having to ensure their FA is catered for and not wanting to appear different. Eating out seems to be a particular difficulty, no matter one’s age, a finding reflected in a mixed-methods study by Barnett et al. (2018) who reported that adults with milk allergy in particular did not find their needs catered for when eating out. Not wanting to be different from friends is something that has been reported for children and adolescents with FA (DunnGalvin et al., 2009; Vazquez-Ortiz et al., 2020). Our findings show that this may not be limited to the adolescent age-group but may be a consequence of the nature of FA, due to the need to behave in a different way to others in social situations involving food.
These findings can be explained within the context of the developmental pathway for children and adolescents with FA developed by DunnGalvin et al. (2009). This theoretical framework aims to explain the onset, development and maintenance of FA-related cognitions, emotions, and behaviour. The model suggests that during adolescence, cognitive appraisal and coping behaviours become habitual and continue into adulthood. This includes the integration or rejection of an FA identity, which can lead to feeling different to others. Appraisals made regarding the threat to health are associated with an emotional response to that threat. If that response involves high levels of anxiety, avoidant strategies and withdrawal from situations involving food may be used to manage and reduce the distress. These experiences and behaviours were described by adults in our study, with avoidance a habitual response for many.
The second theme found in our data describes and explores the ways in which adults coped with FA. Some of these coping strategies involved avoidance and restriction of activities they would have liked to be involved in. This was discussed as necessary to keep them safe but was also isolating. Avoidance of situations involving food has been reported for adolescents with FA (DunnGalvin et al., 2009) and, as noted above, DunnGalvin’s developmental pathway suggests that this way of coping could become habit as the person grows into adulthood. Our data show that this type of strategy is also used by those diagnosed later in life. This avoidance helped adults manage the anxiety related to FA and the risk of having a reaction, but this can have an impact on QoL (Polloni & Muraro, 2020). Avoidance as a coping strategy, particularly in managing long-term conditions, has been associated with poorer QoL and greater anxiety or depression (McCoy & Theeke, 2019). Avoidance can lead to poorer self-care or adherence to medication (Albai et al., 2017). In the context of FA, avoidance may also perpetuate feelings of anxiety due to the lack of exposure to anxiety-provoking situations. This may be due to increased threat appraisal and threat avoidance, an impaired regulation of avoidance, habitual avoidance, and attempts to increase psychological distance from the threat (Arnaudova et al., 2017). Interventions that address coping strategies before they develop into habitual behaviours that might have a detrimental influence on quality of life and anxiety are therefore important.
Controlling their environment was a further strategy discussed by adults, which has been discussed in other qualitative studies with adults with anaphylaxis (Knibb et al., 2019; Walklet et al., 2018). The constant vigilance was described as draining, and some adults worried that their checking behaviour could be excessive. Frequent checking of food labels and menus and asking staff about ingredients when eating out has been shown to predict poorer QoL in adults with FA (Knibb et al., 2021). However, this is seen as a behaviour that is needed to keep them safe. Adaptive strategies such as forward planning and preparation helped some adults reduce their anxieties and enabled them to do things such as eating out. These more problem-focused strategies have been related in the literature to less psychological distress and better QoL (McCoy & Theeke, 2019).
The way in which adults in our study coped with FA and the effect on emotional outcomes such as distress can be further explained through the Common Sense Model of Self-Regulation (CSM-SR) (Leventhal et al., 2016). The social cognition model suggests that coping responses are guided by cognitive representations of the illness and how threat-related information is processed. Research has consistently shown that representations or beliefs that a health threat has serious consequences, is difficult to control, has a chronic timeline, and has a high emotional burden are related to illness-related outcomes such as anxiety and poorer QoL (Hagger & Orbell, 2022). They are also associated with less adaptive coping strategies such as avoidance or emotional venting. Whereas a feeling of control and a good understanding of the condition is related to more adaptive coping such as planning or active problem-solving, and less distress (Hagger & Orbell, 2022). In support of this, a study on people with allergies found that strong personal control beliefs and strategies such as positive reinterpretation were associated with less psychological distress, whereas a higher emotional burden from the allergies was associated with greater overall distress including anxiety, stress, and depression (Knibb & Horton, 2008). Adaptive illness beliefs and coping strategies should therefore be fostered in intervention strategies for adults with FA.
This study has some limitations to consider. The majority of participants interviewed were well educated White British women in the United Kingdom. Although proportions in terms of ethnicity may be similar to the UK population (England and Wales Census, 2021), experiences discussed here may be different to people from different ethnic or socio-economic groups. Participants from countries with different societal views or knowledge about FA, or different FA labelling laws that could affect experiences when shopping or eating out, may not experience the same impact as the current participants. Additionally, this study relied on convenience sampling recruited through patient organisations which may have introduced selection bias. Adults with FA who engage with such organisations may have different coping strategies or levels of awareness about their condition compared to those not affiliated with such communities. Care must therefore be taken making generalisations.
Our findings provide some guidance for healthcare practice. It is clear that FA affects the psychosocial lives of adults and this should be considered by healthcare professionals, in particular the anxiety and fear of FA, the control it can have over people’s lives, the impact on self-esteem, and the hyper-vigilance and checking behaviour that can result from constant efforts to avoid accidental allergen exposure. Where necessary, adults with FA should be referred for further support to help them manage their FA distress. Planning and positive adaptation should be encouraged so that adults with FA can maximise their quality of life.
Supplemental Material
Supplemental Material - “It’s a Permanent Struggle to Manage It Really”: Psychological Burden and Coping Strategies of Adults Living With Food Allergy
Supplemental Material for “It’s a Permanent Struggle to Manage It Really”: Psychological Burden and Coping Strategies of Adults Living With Food Allergy by Caity Roleston, Jennifer L. P. Protudjer, Linda J. Herbert, Christina J. Jones, Chris Warren, Helen A. Brough, Mahboob Miah, Nicola O’Donnell, Mary Jane Marchisotto, and Rebecca Knibb in Qualitative Health Research
Footnotes
Acknowledgments
We would like to thank Allergy UK and Anaphylaxis UK for their help in providing comments on study materials and questionnaires and for advertising the study for recruitment of participants.
Authors Contributions
Study concept and design: R.K., L.J.H., C.J.J., J.L.P.P., H.A.B., C.W., and M.J.M.; data collection: R.K., N.O., and M.M.; analysis of data: C.R. and R.K.; interpretation of data: all authors; drafting of the manuscript: C.R. and R.K.; and critical revision of the manuscript for important intellectual content: all authors. All authors approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.K.: research funding from the National Institute for Health Research, Aimmune, National Peanut Board, Novartis and the Food Standards Agency and honoraria from Nutricia, Viatris, and Stallergenes and DBV Technologies. R.K. is also Chair of the British Society for Allergy and Clinical Immunology Psychology Special Interest Group for Psychology. J.L.P.P.: Section Head for Allied Health, and Co-Lead, Research Pillar, for the Canadian Society of Allergy and Clinical Immunology; sits on the steering committee for Canada’s National Food Allergy Action Plan, and reports consultancy for Ajinomoto Cambrooke, Nutricia, Novartis, and ALK-Abelló. H.A.B.: research funding from the NIH (NAIAD) and speaker honoraria from DBV Technologies. M.J.M.: sits on the National Peanut Board Food Allergy Advisory Council and reports consultancy for Novartis. C.J.J.: research funding from the National Institute for Health Research and the Food Standards Agency and honoraria from the National Institute for Health Research, Nutricia, Mead Johnson, and Allergy UK.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Aimmune Therapeutics, Novartis, National Peanut Board, and European Academy of Allergy and Clinical Immunology.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.