
Abstract
This study investigated the use of group body mapping as a methodological tool to explore experiences of obstetric violence among migrant women from Senegal, Morocco, and Pakistan in Catalonia. The research aimed to assess the effectiveness of group body mapping in identifying the barriers these women faced during pregnancy, childbirth, and the postpartum period, while also highlighting the intersectional dimensions of obstetric violence. The study identified seven key codes—Issues/Barriers, Trust, Gender, Body/Embodiment, Significant Relationships, Employment, and Gender-Based Violence—which were analyzed from an intersectional perspective. Group body mapping was presented as an effective strategy to visualize structural and invisible barriers, offering a deeper understanding of the sociocultural dynamics that affected migrant women’s access to and experience of sexual and reproductive health services. This technique complemented traditional research methods by capturing complex narratives and revealing systemic structures tied to social status, gender, religion, language, and age. It empowered women to reclaim agency over their experiences within historically medicalized and colonized healthcare systems. Ultimately, the research highlighted the transformative potential of group body mapping in advancing healthcare equity and promoting culturally and gender-sensitive sexual and reproductive health services for marginalized populations.
Keywords
Introduction
This article presents a methodological reflection on the use of group body mapping with migrant women in vulnerable situations. The vulnerability of these women does not arise from their status as foreigners or from the processes of pregnancy, childbirth, and caregiving per se, but rather from the passive roles assigned to them, which limit their ability to express themselves, be heard, vote, or participate in civic, cultural, and territorial aspects (Adlbi Sibai, 2016).
The study underscores the methodological potential of the intersectional dimensions of obstetric violence (OV) experienced by migrant women (Brigidi, 2022). By employing group body mapping, the research highlights the experiences and barriers faced by these women during pregnancy, childbirth, and the postpartum period.
The article introduces the qualitative technique of group body mapping as a valuable strategy for overcoming obstacles related to the research process itself, such as time, space, political conditions, and the role and appearance of the researcher, as well as cultural barriers, values, and traditional norms faced by women both within and outside the biomedical system.
In this context, the central research question guiding this study is: How effective is group body mapping as a methodological approach for investigating OV experiences among migrant women in vulnerable situations in Catalonia? The aim is to evaluate its effectiveness in highlighting the barriers and experiences of OV faced by migrant women during pregnancy, childbirth, and the postpartum period. Moreover, this study seeks to analyze its capacity to explore the intersectional dimensions of OV and examine its potential as a complementary tool to traditional methods in sexual and reproductive health (SRH) research, along with a brief reflection on the a-therapeutic nature linked to the proposed technique (DiGiacomo, 2016).
Despite ongoing debates regarding the term in biomedical contexts (Ayres-de-Campos et al., 2024; Brigidi et al., 2024), there is consensus in European policies and laws that OV refers to dehumanizing treatment, abuse, disrespect, and neglect or excesses within healthcare settings (Committee on the Elimination of Discrimination against Women, 2020; Directorate-General for Justice and Consumers & Quattrocchi, 2024; Llei 17/2020; Parliamentary Assembly of the Council of Europe, 2019; Simonovic et al., 2019). This includes physical, verbal, psychological, and spiritual mistreatment, as well as non-consensual medical interventions (Brigidi et al., 2023; Sadler et al., 2020).
In recent years, academia has increasingly incorporated artistic techniques such as theater, body-storming, performance, podcasts, and comics (Boydell, 2020). These narrative tools allow for greater representation and recognition of experiences related to illness and motherhood, contributing to a deeper understanding of these phenomena. Body mapping exemplifies this trend (Henderson et al., 2023), integrating art therapy elements to collect data efficiently (Solomon, 2007). This creative process utilizes drawing, painting, collage, and writing to visually represent individuals’ lives (Gastaldo et al., 2018; Mayra, 2022). Historically utilized since the 1970s (Coetzee et al., 2019), body mapping has adapted to various cultural contexts (Mayra et al., 2022; Skop, 2016).
Body mapping is typically employed when speech or memory challenges arise, or when participants have experienced trauma, fostering non-verbal communication skills (Gastaldo et al., 2012). It offers an alternative storytelling method that complements reflections by incorporating symbols unique to collective experiences. Importantly, it allows individuals to reclaim agency over their histories (Ryan et al., 2022).
This study focuses on group body mapping with migrant women as a critical tool for examining the medicalization, colonization, and objectification of their bodies (Ladeira & Borges, 2022). These bodies, often perceived as fragile, lack voice and presence in Western contexts (Adlbi Sibai, 2016; Davis, 2019). Group body mapping enables participants to reclaim their corporeality within historically marginalizing environments (Ryan et al., 2022).
By applying an intersectional approach aligned with the United Nations 2030 Agenda (Crenshaw, 1989, 1991; UN, 2015), this research addresses OV, cultural diversity, and the use of group body mapping. It examines how ethnicity intersects with SRH experiences among migrant women from countries such as Senegal, Pakistan, and Morocco in Catalonia. Intersectionality facilitates the identification of vulnerabilities across different dimensions.
Personal reflections highlight how privilege influences research understanding, especially when navigating diverse languages and cultural contexts as a migrant researcher. A feminist situated approach (Haraway, 1988) has been essential. This study explores how intersecting factors such as gender, culture, social status, language, and religion shape the childbirth experiences of migrant women (Rodó-Zárate, 2021). Body mapping, as a participatory methodological tool, offers a comprehensive way to examine these intersecting axes and reveal systemic barriers to accessing SRH services. By visually representing their experiences of OV and the challenges they faced, migrant women in Catalonia provided valuable insights into hidden obstacles within the healthcare system. This approach promotes a deeper understanding of the physical, emotional, and systemic difficulties these women endure.
Migrant Women’s Access to Sexual and Reproductive Health Services in Catalonia
Promoting access to SRH services is key to reducing health inequalities (Candeias et al., 2021). This area not only facilitates inclusion in the healthcare system but also strengthens trust in it, highlighting the importance of inclusive and rights-based public policies. The implementation of screening programs grounded in cultural competence, as well as any other self-care intervention, requires the adoption of culturally appropriate strategies (Lurgain et al., 2024; Schouler-Ocak, 2023). In Catalonia, despite the political agenda addressing SRH (Llei 19/2020; Llei 17/2020), barriers to SRH access persist for migrant populations, particularly affecting migrant women (De la Torre et al., 2006; Llamas & Brigidi, 2022; Lurgain et al., 2024). According to data from the Catalan Institute of Statistics (IDESCAT, 2022), the foreign female population in Catalonia displays notable diversity in terms of nationality. Specifically, there were 16,800 women of Pakistani nationality, 100,543 of Moroccan origin, and 60,006 of Senegalese origin (IDESCAT, 2022). In total, foreign women represented 10.9% of the female population in Catalonia, underscoring the importance of migrant communities in the region’s demographic structure. In 2022, foreign mothers accounted for 32.7% of births (IDESCAT, 2023), highlighting the need for care that is better adapted to the linguistic, cultural, and socioeconomic diversity of the population (Brigidi, 2022; Llama et al., 2023). The limited available studies on SRH among migrant women in Catalonia do not reveal statistically significant differences in treatment compared to native women (Gallardo Martínez et al., 2021). Catalonia has some of the most favorable maternal and child health indicators in Europe, with low maternal (3.6/100,000) (IDESCAT, 2023) and neonatal mortality (2.52) (IDESCAT, 2023), as well as stable rates of low birth weight (7.4%) and prematurity (6.4%) (Vidal et al., 2021). However, qualitative studies reveal concerns about excessive medicalization, body control, and obstetric and institutional violence, issues that disproportionately affect migrant women (Brigidi, 2022; Lazzerini et al., 2022). Research also shows that migrant women are more vulnerable to gender-based violence (GBV), experiencing discrimination and racism that erode their trust in SRH services (Davis, 2019; Kingsberg et al., 2019). A significant portion of organizations, specifically 65%, report that their members do not receive respectful treatment during pregnancy, childbirth, and postpartum, particularly concerning care for functional and cultural diversity. Major areas for improvement include specialized counseling, personalized care, and respect for diversity—areas that, according to 60% of organizations, are not adequately addressed (Escuriet Peiro et al., 2023).
Current SRH challenges related to migration are linked to several factors: (1) the increasing number of migrant women of reproductive age, which will significantly influence public health in the next decade (Eurostat, 2024); (2) the lack of culturally competent care for issues such as chronic cystitis, infertility, or endometriosis (Nunez-Badinez et al., 2021); (3) the impact of practices like childbirth and breastfeeding on global sustainability (Nommsen-Rivers et al., 2010); (4) the relationship between SRH and mental health, particularly in chronic conditions like vulvodynia or the aftermath of OV; (5) the need for women to make informed decisions about their SRH (Castro et al., 2019); (6) the urgency of addressing sexually transmitted infections (Geretti et al., 2022); (7) the importance of comprehensive care during pregnancy and postpartum to prevent complications (Lazzerini et al., 2022); and (8) the removal of barriers related to GBV and racism in the healthcare system (Nelson et al., 2023).
Methodology
Participants
Author’s Elaboration, Sociodemographic Characteristics of the Women Participants (Excluding Cultural Mediators).
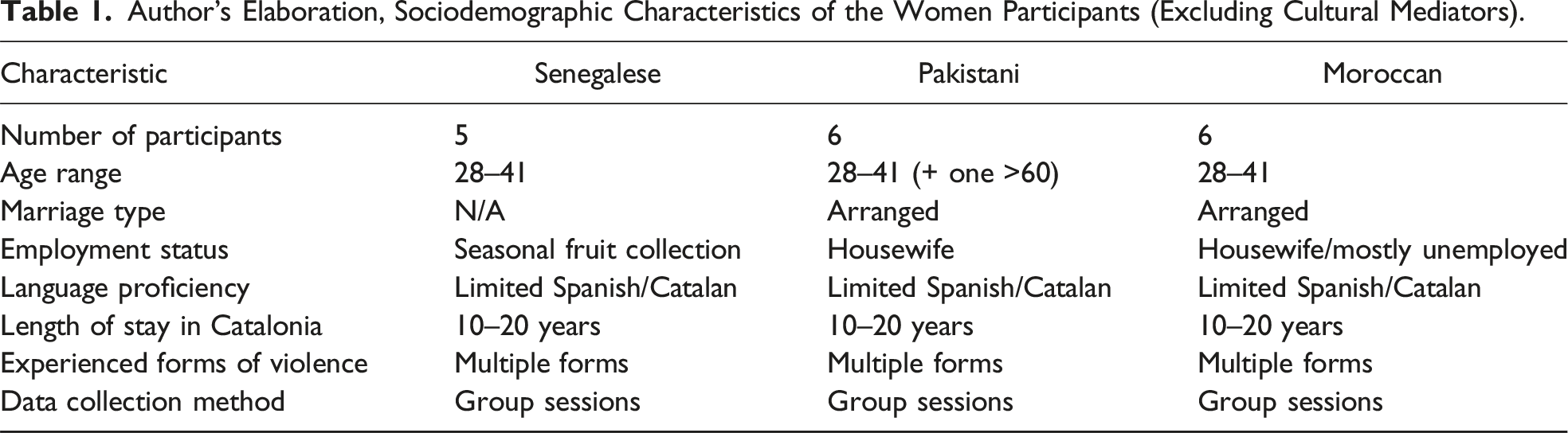
These nationalities were selected based on data from the Statistical Institute of Catalonia (IDESCAT, 2021), choosing groups with the most significant territorial presence in Catalonia and those about which there was a lack of scientific knowledge in terms of healthcare and social services according to a previously unpublished study conducted with health professionals. Additionally, the significant presence of women of childbearing age among these groups was considered. It is important to clarify that these official data only account for women with administrative stability, not reflecting the entire foreign female population in the territory.
For inclusion in the focus groups and body mappings, the criterion was that participants be mothers who had given birth within the last 5 years in any hospital of the Catalan public network. To recruit informants, contact was established in Catalan and Spanish with associations in Catalonia that focus on health, migration, and women’s issue. Furthermore, these associations provided the space to conduct the groups and body mappings, and store the necessary materials for the mappings. The cultural mediators were women and mothers, well-known to the associations, some having collaborated in previous health studies (Table 1). All had lived in Catalonia for over 20 years, held qualifications as cultural mediators in health, spoke Spanish, and understood Catalan. The cultural mediator played a crucial role in facilitating communication and understanding between researchers and participants.
The COVID-19 pandemic profoundly affected the research methodology and participants’ experiences, requiring adaptations due to health restrictions. It disrupted spatial dynamics, social interactions, and healthcare delivery, particularly in pregnancy, childbirth, and postpartum care. These changes heightened existing socioeconomic disparities and healthcare challenges throughout the project. The women involved in this study have been and continue to be in a position of vulnerability. It is important to emphasize that the groups themselves are not inherently vulnerable but are in a situation of vulnerability due to the process of wealth concentration, economic exploitation, segregation in political participation, and inequality in access to cultural heritage. Migrant women, in particular, face situations of deficiencies and inequalities in multiple aspects, such as social, cultural, economic, and emotional.
On the other hand, although the biomedical system demands profound knowledge about various communities, including their cultural, ethnic, social, economic, and political characteristics, and individual resources, it is crucial to avoid hasty generalizations. Culture, with its diverse traditions and customs, is transmitted through a complex process of socialization that defines the beliefs, values, and customs of those exposed to it, impacting both subjective and collective levels. The field results and records obtained during the research pertain exclusively to the women with whom the body mappings were developed. However, they can offer a valuable perspective and support to healthcare or childbirth personnel, though they should not be understood as a rigid guide of tools applicable indiscriminately to any individual from the mentioned territories.
Multiple forms of violence include physical, economic, psychological, sexual, vicarious, obstetric, and second-order violence as recognized by Catalan law (Law 17/2020). The body mappings have also revealed evidence of these forms of violence.
Procedure
The study involved 13 sessions of body mapping with three groups of 4–5 migrant women, along with a cultural mediator, the principal investigator, and occasionally a research technician. Sessions lasted 3–4 hours and continued until information saturation or participant fatigue. Each group completed 4–5 sessions focused on specific themes: migration, fertility, and body perception; conception and pregnancy; childbirth; and child-rearing practices. The themes, drawn from prior literature, aimed to construct a comprehensive narrative of migration, pregnancy, and maternal care. Instructions were repeated in each session, and participants collectively embodied their experiences on the silhouettes, prioritizing shared experiences over aesthetics. With participants’ help, I prepared the materials—scissors, colored pencils, pens, glitter, crayons, magazines, and more—ensuring everything was child-friendly. I encouraged participants to bring their own magazines, as Catalan media often lacked diverse body representations, particularly for Black women. Despite these limitations, the women adapted the images and added words or symbols to complete their collages, often involving their children in the process. Typically, women participated with their children. Except for Moroccan women, with whom we arranged groups during school hours and who had daughters older than 3 years, other women participated with their children: some newborns, others a few years old and not yet schooled within the Catalan education system. This created a lively and tender atmosphere among all participants, characterized by crying, laughter, drawings, scuffles, loving words (and scolding) in native languages interspersed with some words in Spanish and Catalan, diaper changes, food on the floor, and breastfeeding. On one hand, creating a safe and welcoming space for the children was fundamental for the research; without it, the women would not have agreed to participate, and it also allowed for deeper observation and understanding of their child-rearing realities and kinship relations. On the other hand, it cannot be denied that this changed the timing of the group development as conversations were often interrupted by the children, their desires, and their needs, which also created challenges in transcribing text for the interns due to the background noise. In each session, something was purchased for a snack, keeping in mind the dietary restrictions and customs of each community. These moments turned into a collective snack time, where a mother would offer pieces of dates to her daughters, enjoy a piece of dried or fresh fruit herself, and discuss recipes and traditions. Food is an element that unites people and softens language and cultural barriers more easily. Exclusively with the Senegalese women, this conviviality did not generate a participative and unified atmosphere; generally, they maintained a position of respect for “our food” and caution toward the research team. It is worth mentioning that this was the only group in which one of the husbands of the participants, also a prominent figure within the community, entered during a session to ask if everything was going well and the next time, waited outside the association until the group finished. It can be affirmed that, for all women, regardless of ethnic background, the sense of control and judgment was always present and was a challenging element to manage externally.
The strategies to support women in cases of distress during the study included the ability to directly contact the principal investigator, engage with the assigned cultural mediator for a trusted and supportive environment, and access further assistance and security through the facilitating association. During the body mapping, we were all in the same position in front of the paper, where our shared experiences as women and mothers in the realm of SRH came together through both lines and words. For many women, learning about my own migration story eased the telling of their own experiential journeys. Many of them saw parts of themselves in me, asking me how I had lived through it, how I had managed to obtain my “papers,” considering I belong to one of the most prevalent migrant communities in the area. They identified me as an ally. This was not the case with the Senegalese women, who initially showed significant resistance and criticism toward the position of Western women. However, during the final mapping session, the experience flowed, and, surprisingly, as we discussed childbirth, they began to open up.
The Room and Body Positioning
A critical aspect proved to be the characteristics of the room: it needed to be welcoming, allow movement while fostering elements of circularity, and contain a large piece of paper and all the artistic materials used, without them being too far away. Since there were often children present, the room should not have stairs or furniture with sharp corners. This aspect also presented challenges to the group of Senegalese women. The room was one of the largest, filled with many tables and chairs that hindered circularity and the straightforward use of artistic materials. Typically, I would arrange the roll of paper on the floor. The silhouette was made from a roll of paper that was cut to size; sometimes, to make it aesthetically more appealing, colored paper was used. A roll of cardboard could have been used to make it more durable, but one of the features of this project was mobility: the ability to travel to communities in different cities across Catalonia (about 200 km), and the transportation of materials was done using my private car. The need to fold the paper into a roll was essential to facilitate movement and transportation.
Each session, after re-explaining the session’s theme and discussing some points that seemed important to address, I asked the group in which position they wanted to draw the woman: sideways, squatting, lying down, etc. This is an important issue and what sets this work apart from other body mapping studies. I never used predefined bodies or models for the research, allowing the choice of position, material, and color used to be collective acts of awareness and themselves material for analysis: why choose this position to represent childbirth? After selecting the position, one of them would lie down on the paper (Images 1 and 2). This was a moment characterized by much hilarity: tracing the body with a pencil, respecting the shapes of traditional clothing, and enhancing the profile by adding biographical and aesthetic elements like curly hair emerging from under a hijab, or nipples, represented moments of unity and sharing. Silhouette preparation: outlining the body. Decorative detail of the hand, reproducing henna and nail polish decoration.
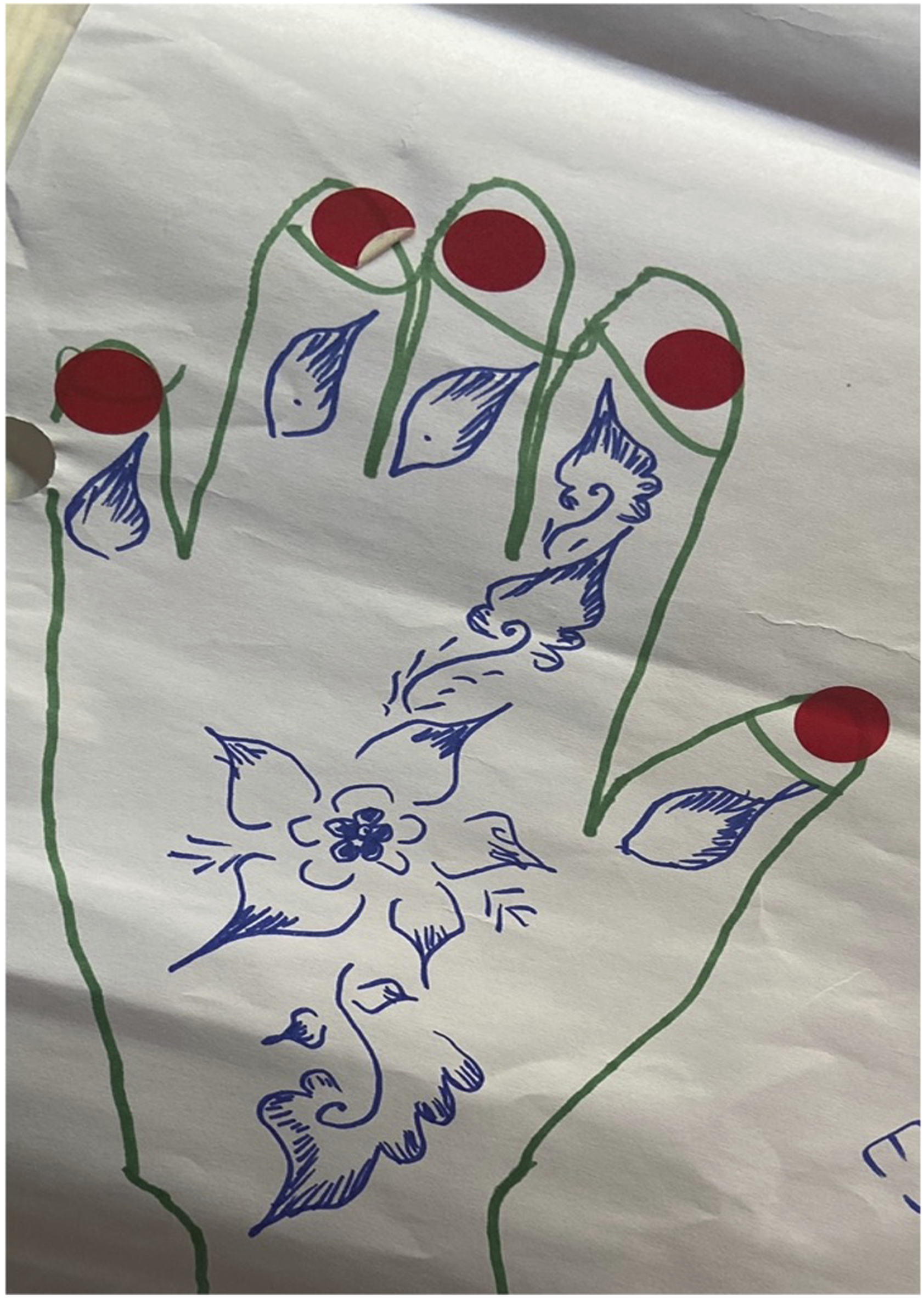
Initially, I would remind them to include sexual elements, and then they would draw them, representing their breasts with golden glitter (the maternal milk), bellies and vulvas with stretch marks and scars, cuts (episiotomies), and hands that penetrate them (repeated examinations), knees that press down on them (Kristeller maneuver), or decorating the hands with henna.
The Floor, Listening, and Words
The decision to position ourselves on the floor stemmed from the intent to emphasize key ideas central to the trial-and-error nature of fieldwork, which every researcher encounters. Initially, my focus was on the spatial distribution of the silhouette, aiming to ensure free circulation of participants, materials, and food for snacks. These silhouettes, measuring about 1.80–2 m by 1.20 m, were bulky and delicate. I found meeting rooms, often designed without a feminist or gender-sensitive perspective, restrictive due to tables and chairs. To me, this spatial arrangement was crucial. I would arrive early to rearrange the furniture, stacking chairs, and arranging food in a simple and practical way (Image 3). Using the collage technique to find figures and writings to use in the collective bodymapping.
Children were present as well, which reminded me of my own experience with my children when they were small, often sitting on the floor with them. This setting allowed for more flexibility, particularly for mothers, by reducing the stress of monitoring young children. Finally, comfort played a role in my choice. Since these workshops were lengthy, sitting on the floor allowed us to stretch or bend our legs, making the experience more comfortable for everyone involved. I will not elaborate on the qualities of the circle (office tables are usually square, creating separating corners) to allow for the creation of a safe space of trust and active listening. I will only highlight that the use of different languages, the translations, and mediations that took place required extreme attention and a great capacity for containment on my part. The use of non-verbal language, despite being mediated by cultural meanings, was essential: my gaze, my attention, and my body inclined toward the woman speaking (Cavarero, 2016). She could laugh, draw, and cry without me having the comprehension codes to understand and respond verbally, yet there I had to be: with gaze and body. The floor allowed closer proxemic proximity.
Another point I wish to emphasize is that, surprisingly, each of the women traced her experiences related to the topic without the fear of not knowing how to draw (a common occurrence among native women or health professionals), always displaying fascinating elements of ethnoanatomy. A strength of the study was the ability to artistically mix many languages and forms of writing (because they, despite not mastering Spanish or Catalan, come from countries where more than one language is spoken).
Finally, the last session with all the groups reproduced all the body mappings made, to retrace a narrative line between the experiences and the drawings and to enhance the sense of shared creation, discuss the preliminary results shown in the mappings, and gain their approval, and to also meet the credibility criterion of the research.
Data Collection
Each group meeting was recorded using an audio recorder and documented through various photographs of the process: hands drawing, hands massaging the uterus, and the ways in which elements were cut and pasted onto the silhouette. Faces or minors were never photographed. Prior to this, each woman and the cultural mediator signed an informed consent form for voice recording during the mappings, photographic images, and for the use of the body mappings (primarily for research and training purposes). Each information sheet provided a detailed explanation of the research project and the duration of use for each material. None of the participants expressed any resistance and engaged with enthusiasm and hope. The idea of being able to change the healthcare system to include their voices, already perceived as silenced, greatly motivated the women.
Three interns participated in the project with the role of transcribing the focus groups. They signed a confidentiality agreement.
Data Analysis
In this context, only the data collected through reflection groups and body mappings are presented: - Audio recordings of each session, followed by literal transcriptions in Spanish. - The body mapping techniques will be detailed further.
The qualitative data analysis was conducted using both NVivo software and manual methods, particularly for the body mappings. This approach allowed for the coding, categorization, and thematic analysis of the transcripts, facilitating the identification of patterns and the systematic organization of emerging ideas.
How to Compile and Condense Data From Body Mapping
After completing the fieldwork with the women, the 13 body maps were assembled in a designated space at the university. Each map was displayed sequentially based on thematic content—focusing on meanings attributed to the pregnant body, couple relationships, or obstetric experiences—rather than by ethnicity. The space was reserved for several days to prevent damage from repeatedly hanging and removing the materials. During this time, some materials were restored, as they had deteriorated due to storage conditions, usage, or wear, with some collage elements coming loose.
Several interns participated in the analysis, creating a co-creative learning experience. The analysis began by moving from general to specific themes, then from specific to general, identifying both visual and conceptual relationships between the different maps. Codes were assigned, each with a specific theoretical focus, and these were used to define what were termed “embodied units of corporeal registration.” Seven key codes were identified: Issues/Barriers, Trust, Gender, Body/Embodiment, Significant Relationships, Employment, and Gender-Based Violence (Image 4). Seven key codes were identified: Issues/Barriers, Trust, Gender, Body/Embodiment,Signifi cant Relationships, Employment, and Gender-Based Violence.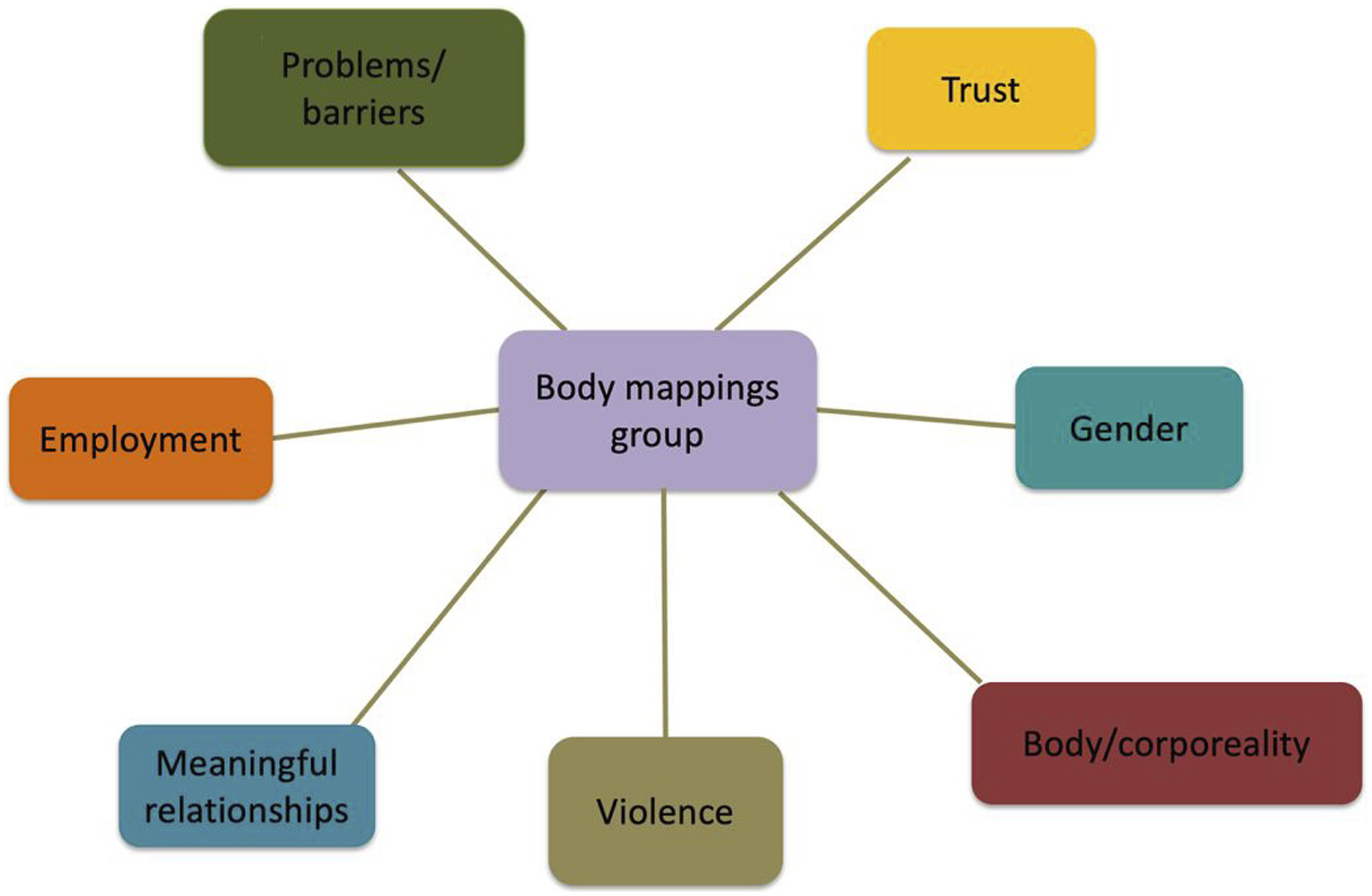
The next phase involved an in-depth examination of these relationships, visualized through a mind map that synthesized the data and a conceptual map that illustrated connections between codes and embodied units of corporeal registration. Data triangulation was then performed with additional information gathered from reflection groups and external sources such as WhatsApp groups. These supplementary sources provided cultural insights, clarifying names in their original languages and meanings. This material was integrated using NVivo software and treated as necessary for clarifying mapping elements.
Separate mind maps were created for each theme, providing a visual representation of key concepts, while the conceptual map emphasized hierarchical relationships and the primary points of connection. These tools supported the analysis of complex processes and helped translate knowledge. Additionally, the data were organized digitally, with each category of relationships assigned a Roman numeral and title. For example, under “Fertility and Body, Relationships and Kinship Bonds,” all related photos were organized, while an emerging code—such as “significant relationships”—was used to identify embodied units of corporeal registration, categorized as (a) Family, (b) Religion, (c) Romantic affection, etc.
Ethics
The project complies with Regulation (EU) No. 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons regarding the processing of personal data and the free movement of such data (General Data Protection Regulation), as well as Organic Law 3/2018 of 5 December on Personal Data Protection and the guarantee of digital rights. The materials have been stored in a cloud space provided by the university, with pseudonyms used and personal identifiers removed. The data were labeled with unique identifiers and securely stored. Personnel with access to this data (the researcher, research technician, and interns) are bound by professional secrecy and confidentiality, an obligation that remains in effect even after the project’s completion, prohibiting them from communicating or disclosing the information to third parties. In compliance with the aforementioned regulations, all processing activities related to personal data in this project ensure the principles of lawfulness, fairness, transparency, purpose limitation, data minimization, accuracy, storage limitation, integrity, and confidentiality.
Findings
The findings obtained through the analysis of the group body mapping technique identified six central aspects: Issues/Barriers, Trust, Gender, Body/Embodiment, Significant Relationships, Employment, and Gender-Based Violence. These elements help answer the research question and fulfill the study’s objectives (Image 4).
One of the most relevant findings was that trust emerged as a positive and central element in group interactions and the use of body mapping. Despite post-pandemic restrictions (such as masks and distancing), the participants and I were able to create a space of mutual safety and support. This allowed for the sharing of intimate experiences and helped break linguistic and cultural barriers. This was particularly evident among the Senegalese women in the final session on childbirth. The body mapping technique, in this case, created a conducive environment for collective well-being and protection. Unexpectedly, the dimension of pleasure in being together and mutual responsibility, that is, care, also surfaced (Image 5). Co-creation, co-participation, communal acts, and conviviality—cultivated through shared narratives, active listening, dialogue circles, food, and artistic activities—were reflected in the silhouettes, embodying the participants’ collective experiences. Each code highlights the different observed dimensions.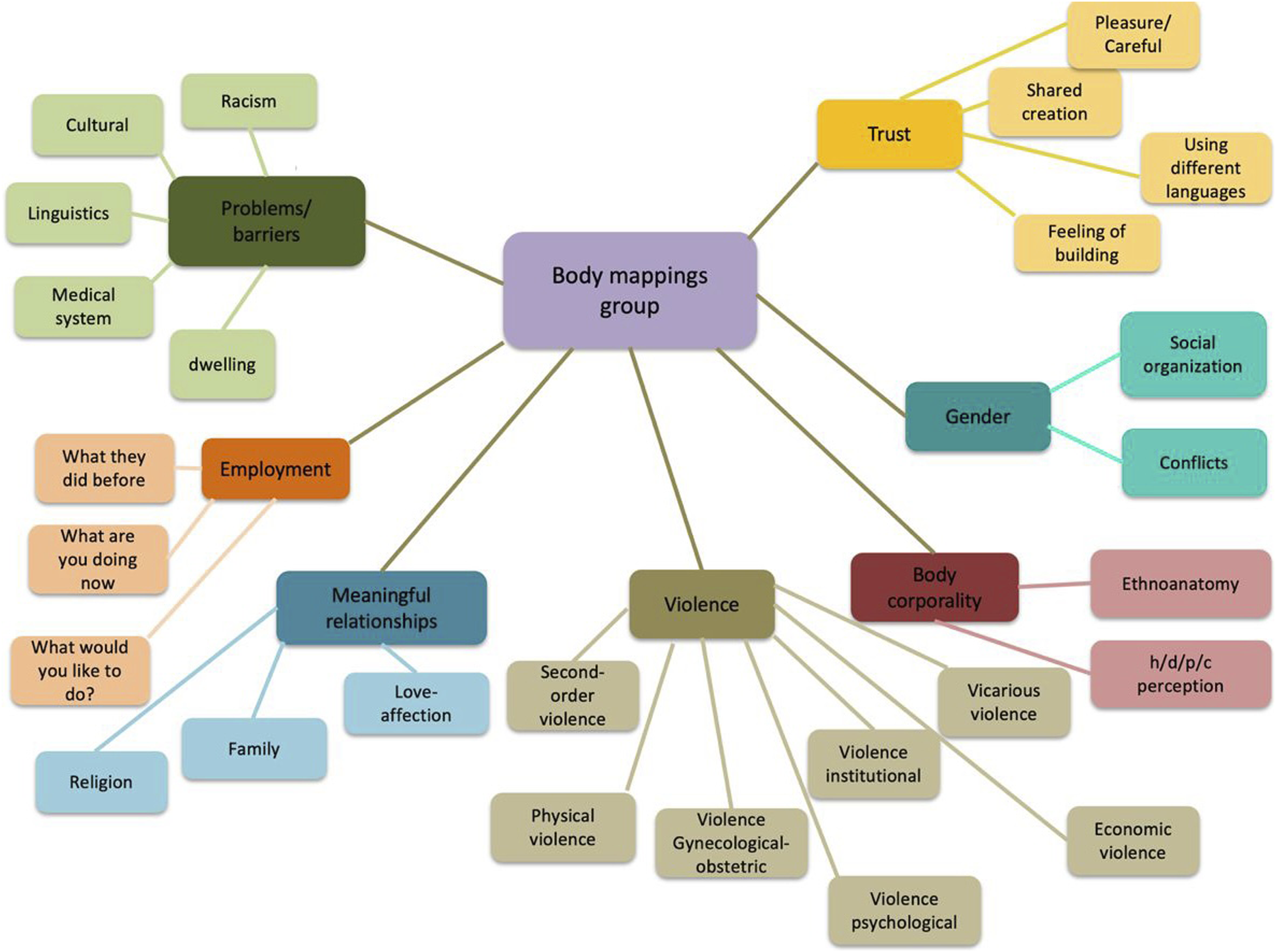
Gender was consolidated as a transversal axis in the mappings, offering a platform for women to reflect on the constructions of femininity and masculinity in both their countries of origin and their host countries (Image 4). The results reveal how sociocultural expectations impose subordinate roles on these women, particularly in relation to their husbands and families (significant relationships, Image 4), which are also reflected in sociocultural barriers (issues/barriers, Image 4). This aspect is closely tied to gender roles, employment, and the impact of migration status, which complicate and aggravate the experience in the SRH system. Topics related to sexuality, desire, and family planning—interacting with categories of age, gender, and religion—were recurrent themes in the body mappings, revealing the control exerted both by the family system (especially in-laws) and the biomedical system over women’s desires. This underscores body mapping’s ability to capture the intersectional and structural dimensions of violence while facilitating an interaction that transcends communication barriers and allows for the exploration of complex topics (Images 5 and 6). Representation of the intersection between the different dimensions and codes.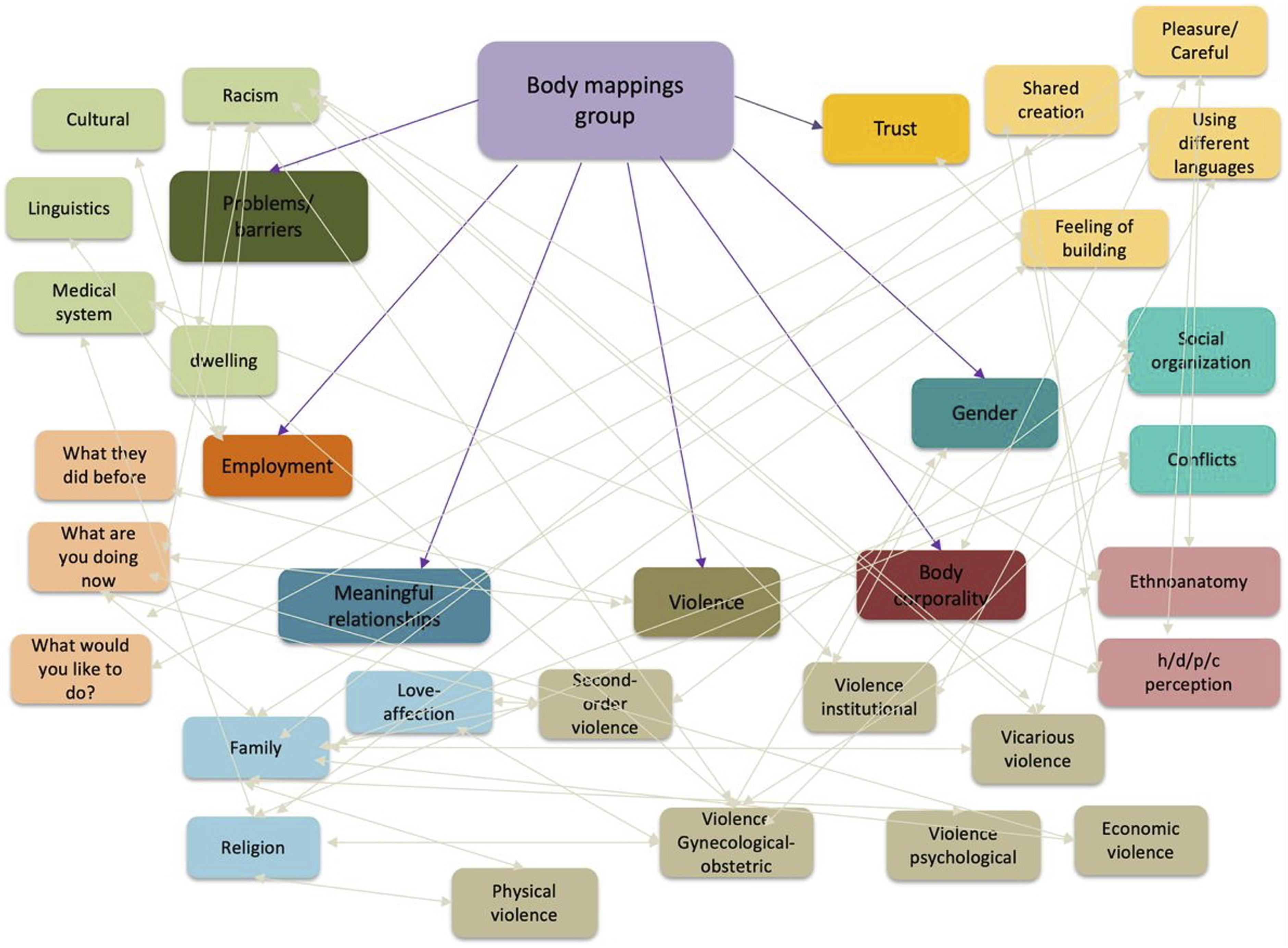
Another crucial and transversal aspect that emerges from the findings is the prevalence of GBV in the lives of the participants. This violence takes various forms—physical, psychological, economic, institutional, and obstetric—and is an almost universal and persistent experience of human rights violations among the migrant women in this study (Image 6). However, it was also observed that many remain in abusive relationships due to family pressure and fear of losing the support of their extended families.
The findings confirm the effectiveness of group mapping in the context of OV, providing a space for agency for migrant women. The relationship with OV becomes evident both in the narrative descriptions and the graphic representations of abusive practices, highlighting not only the exposure of the body but also the lack of informed consent. Additionally, there is a clear absence of explanations regarding treatments, timelines, and procedures, and an absence of mediators to facilitate reciprocal communication. There is also a recurring shortage of acceptance for cultural diversity. This is reflected in the conceptualization of the health, disease, prevention, and care processes (h/d/p/c, as illustrated in Image 6). In summary, both the physical and bodily dimensions of violence, as well as the emotional and spiritual aspects, are made visible. The system’s incapacity to provide a safe environment for these women is highlighted, and the mapping process functioned as a space for proposals, transformation, and advocacy, aiming to bring about improvements in the healthcare system.
The women described healthcare and social services as having significant limitations in identifying and addressing these complexities, revealing insufficient attention to cultural diversity and the specific needs of migrant women, as well as the professionals who, without proper tools, attempt to assist them. This only exacerbates the violence these women face, perpetuating their marginalization in both physical spaces and mental dimensions of oppression.
Discussion
The findings of this study reveal the complex web of often invisible barriers that migrant women face in accessing their fundamental rights. These barriers intertwine with instances of OV and other forms of GBV, generating processes of marginalization. Group body mapping allowed us to go beyond the simple observation of the multidimensionality of inequality in access to and care for SRH, providing evidence of the interconnections between these dimensions and uncovering the structural mechanisms that perpetuate these barriers.
From the fieldwork, the persistence of elements related to the perception of health, illness, prevention, and care (h/d/p/c perception, Image 6) emerged. Women tend to conceal certain traditional practices during childbirth or the immediate postpartum period from biomedical professionals, revealing a division they establish in addressing their SRH. This reflects a limited trust in the health system, exacerbated by experiences of racism and fear during medical visits, leading many to resort to silence as a survival mechanism (Barata, 2022; Brigidi, 2022), which in turn reinforces the structure of violence they endure.
Factors such as ineffective communication, their foreign appearance (i.e., the use of the hijab), misunderstandings with the healthcare system, and experiences of GBV create a landscape that deeply affects their SRH. Added to this are traditional views about the role of the mother and the family, as well as cultural perceptions of the body and risk (Quattrocchi, 2014), reinforcing a structure of control that exacerbates negative experiences during healthcare (Sadler et al., 2020; Schouler-Ocak, 2023). Being a woman, mother, migrant, and Muslim in a context of linguistic and cultural barriers magnifies these challenges. The study also highlights how healthcare systems, together with family and social dynamics, reinforce the vulnerability and perpetuate the marginalization of these women (Hacker et al., 2022; Candeias et al., 2021).
In his study on HIV and body mapping, Solomon (2007) notes that this technique can be potentially therapeutic, a concept also present in the referenced literature. However, it is crucial to clarify that while the findings may contribute to improving clinical practice, they are not intended to offer therapeutic treatment or relief per se. My approach does not focus on pathology or healing but rather on giving meaning and agency to individuals through listening and transfer. In this context, my role is that of a narrator (Brigidi, 2021). From this perspective, I interpret trust and group interactions as a space of care and co-creation, linking them to the concept of pleasure observed in the findings. Muelas de Ayala (2023) asserts that pleasure is a bodily emotional process, situated in time and space, involving the body, experience, and dimensions intertwined with claims. Thus, it transforms into a feminist practice that is situated, experienced, and transformative, both personally and collectively (Haraway, 1988; Muelas de Ayala, 2023). In her ethnography on equestrian experiences, DiGiacomo (2016) observes the distinction between therapeutic practice and the recovery of pleasure. The author highlights the challenges we face with pleasure: for it to be culturally legitimate, it cannot exist in isolation but must be discursively framed and experienced in medicalized terms as therapy. This can be extended, from a gender perspective to the experiences of the women who participated in this study. The group body mapping sessions generated experiences of empathy, laughter, and embodiment (DiGiacomo, 2016). These communal acts evoke the artificial kinship bond that Durkheim (1993) discussed, as these sessions created a meaningful commitment to the space, the research, and the individuals present.
In conclusion, it is essential to recognize the complexity of these experiences and their potential to create spaces of care and transformation, beyond traditional therapeutic frameworks.
Finally, it is crucial to acknowledge the study’s limitations. Cultural biases and methodological obstacles were encountered throughout the process. For example, the sessions with Senegalese participants did not flow as expected due to unforeseen cultural differences. These challenges underscore the importance of carefully curating the environment and dedicating more time to building trust to overcome resistance.
My active role as a researcher-facilitator also added complexity to the process. I made cultural mistakes, such as assuming that working on the floor would be comfortable for all participants and not adequately considering religious guidelines related to Islamic texts. These biases highlight the need for preliminary meetings with mediators to adjust these aspects in future research.
Conclusion
This study provides significant insights into the multidimensional barriers migrant women face in accessing SRH care, with a particular focus on OV and the experiences of marginalized migrant groups. By employing group body mapping, the research sheds light on the interplay between gender, age, migration status, and sociocultural factors that shape SRH care access and quality.
The findings reveal critical structural deficiencies in the public health and social care system, which often fails to address the specific and diverse needs of migrant women. These deficits manifest through invisible barriers, such as systemic discrimination, culturally insensitive practices, abusive behaviors, and control mechanisms, which compromise both access to and the quality of SRH care. Notably, the study highlights the prevalence of OV, encompassing physical, emotional, and systemic dimensions, as experienced by the participants. These forms of violence include neglect during labor, lack of informed consent, and the imposition of culturally inappropriate practices that deepen feelings of alienation and disempowerment among migrant women.
Through body mapping, the study effectively captured narratives that conventional tools often overlook, providing nuanced accounts of how intersecting vulnerabilities—such as migration status, limited language proficiency, and socioeconomic marginalization—exacerbate inequities in SRH care. For instance, participants reported mistrust in healthcare professionals stemming from discriminatory encounters, as well as intergenerational transmission of fear and disengagement from the healthcare system.
Beyond methodology, this research makes a substantial contribution to the field by offering practical recommendations for developing culturally competent, gender-sensitive policies and practices. It advocates for integrating intersectional approaches in public health strategies, with a focus on addressing structural inequities and fostering inclusive care models. Policymakers and healthcare providers can leverage these findings to design interventions that not only respond to the cultural and social realities of migrant women but also ensure their voices are meaningfully included in shaping healthcare delivery.
However, the study highlights the importance of having highly trained researcher-facilitators, which involves not only implementing body mapping in a careful and context-sensitive manner, avoiding oversimplifications or generalizations, but also creating a safe and supportive environment that encourages participants to openly share their experiences while being able to contain individual emotions and channel them into collective actions.
Future research should explore the broader applicability of body mapping across diverse sociocultural contexts, focusing on its potential to uncover systemic barriers and foster inclusive health interventions. Additionally, further investigation is needed into the social and psychological factors contributing to migrant women’s disengagement from healthcare services, particularly the role of intergenerational and peer narratives of negative experiences.
In conclusion, this study highlights both the systemic inequalities faced by migrant women in SRH and the potential of innovative methodologies, such as body mapping, to expose and address these challenges. The findings call for urgent action to develop healthcare systems that are equitable, culturally inclusive, and attuned to the specific needs of marginalized populations. Such initiatives are essential to improve not only the experience of care for these women but also the practice of providing care, ultimately fostering a more just and humane healthcare system.
Footnotes
Acknowledgments
First and foremost, I would like to express my profound gratitude to the women who participated in the study and their infants. Their generosity and willingness to share their experiences of sexual and reproductive life were crucial for the development of this research. I also want to acknowledge the work of the cultural mediators for their professionalism and patience throughout the process. Additionally, I am grateful to the associations that provided support and actively engaged in the administrative aspects of the study. I also want to highlight the invaluable contribution of the students and fellows involved in the project, whose dedication and commitment were essential in achieving the research objectives. I wish to express my deepest gratitude to the women who participated in the study and to their children for sharing their laughter, tears, and personal stories with me. I would also like to thank the manuscript reviewers for their valuable and meticulous work. This process has been an entirely horizontal dialogue aimed at improving the text and making it clearer. Their support has been an inspiring example of academic (Uncredited/Unknown) collaboration across distances.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Catalan Agency for Cooperation and Development.