
Abstract
Alberta is home to one of Canada’s fastest growing populations of Black people, driven by an influx of African immigrants to major metropolitan areas such as Edmonton and Calgary. As the Black population in Alberta continues to grow, it is crucial to the well-being of these communities that we understand their health service needs. Black women are a vulnerable group within the Black population due to inequities in social determinants of health such as access to healthcare. In Canada, little is known about the healthcare access experiences of Black women despite reported disparities in their health outcomes. As such, we undertook a qualitative study to examine access to health services for Black women in Alberta. Semi-structured interviews were completed with 30 Black women from Edmonton and Calgary. We applied intersectionality as an analytical framework to guide our understanding of how interconnected social processes shape Black women’s experiences of accessing healthcare. Following our thematic analysis, we identified two major barriers to healthcare access: patient–provider discordance and negative healthcare encounters. We identified two key facilitators: positive patient–provider dynamics and individual and social network strengths. Our findings suggest that Black women have distinct experiences of accessing the healthcare system which are best understood as a confluence of their race, gender, and other aspects of their personhood.
Introduction
As of 2021, Canada’s Black population surpassed 1.5 million, and now accounts for 4.3% of the general population and 16.1% of the racialized population (Statistics Canada, 2021a). The prairies have become home to the fastest growing Black population in Canada, which quadrupled between 1996 and 2016 (Statistics Canada, 2019). In Alberta, this growth was fivefold in 20 years, driven primarily by an influx of immigrants from African countries; as a result, about two-thirds of the Black population in Alberta are first-generation immigrants (Statistics Canada, 2019). Alberta’s Black Canadians tend to settle in Edmonton and Calgary, where they make up 5.8% and 5.2% of the population, respectively (Statistics Canada, 2021b). In Alberta, Black women make up 4.2% of the population of women (Statistics Canada, 2021b).
An analysis of the Canadian Community Health Survey (CCHS) revealed that despite Canada’s universal healthcare system, significant health inequities persist across racial groups (Veenstra & Patterson, 2016). After adjusting for socio-demographic characteristics (e.g., age, education, income level, residence, marital status, and immigrant status) and lifestyle factors (e.g., smoking, body mass index (BMI), and physical activity), Veenstra and Patterson (2016) found that compared to their White counterparts, Black women had greater self-reports of chronic conditions such as hypertension and diabetes. Previous studies have also described a high incidence of cardiovascular diseases in Black women and a greater likelihood of receiving inadequate treatment and management compared to White women (Chiu et al., 2015; Jha et al., 2003). Interpersonal factors at the patient and physician level such as differences in approach to care, poor cultural competence, and incidents of racism and discrimination negatively impact Black people’s experiences of healthcare access (Fante-Coleman et al., 2022). For instance, in their study on the relationship between race, discrimination, and chronic conditions in Canada, Siddiqi et al. (2017) found that Black people had the greatest likelihood of experiencing discrimination and poor treatment among those seeking care for chronic diseases.
Common experiences of both covert and overt interpersonal racism within the healthcare system have significant repercussions for Black people’s healthcare access and health outcomes (Fante-Coleman et al., 2022; Williams & Mohammed, 2013). Racism and acts of discrimination by healthcare personnel are detrimental to effective communication between patients and providers, patient satisfaction and adherence, and subsequent utilization of health services (Paradies et al., 2014). Moreover, acute and chronic experiences of racism serve as a significant source of psychosocial stress which negatively impact health and health behaviors (Williams & Mohammed, 2013). Racism experienced by Black people across Canada in navigating various systems is dynamic and multifold as it often occurs at intersections of other social locations. This is evident in Black women’s self-reports of their health being poorer than the general Black population (Public Health Agency of Canada, 2020). Patterns observed in Canada have also been reported in the United States, the United Kingdom, and other countries with significant numbers of Black populations (James-Conterelli et al., 2023; Silverio et al., 2023).
Black women are vulnerable to disparate health outcomes due to social factors which impede their ability to access timely care that effectively meets their needs. Previous studies have addressed the way inequities impact health and well-being outcomes for those with identities that have been marginalized (Anderson et al., 2009; Mahabir et al., 2021; Williams & Wyatt, 2015). There have also been reports and research undertaken to examine racial disparities in health service access (Ezeife et al., 2022; Fante-Coleman et al., 2022; Halwani, 2004); however, few have focused specifically on Black women’s experiences of accessing healthcare. As Alberta’s Black population experiences unprecedented growth, it is important to understand the health access needs of various groups within this population, especially those whose social locations may lend way to multiple coalescing forms of marginalization. Our study thus aimed to (1) understand the factors that impact Black women’s access to healthcare in Alberta and (2) identify tangible methods to support Black women’s healthcare access.
Theoretical Framework
Our approach to this study was guided by intersectionality, a Black feminist analytical framework. Though the concepts underpinning intersectionality predate the term (Bowleg, 2012), intersectionality became widely adopted after Crenshaw (1989) used the word “intersectionality” to describe Black women’s unacknowledged gendered-racialized social location which often led to their repeated dismissal in legal cases of workplace discrimination (Crenshaw, 1989). Intersectionality was positioned as a criticism of how Black women were omitted from feminist and antiracist discourse due to the “tendency to treat race and gender as mutually exclusive categories of experience and analysis” (Crenshaw, 1989, p. 139). In her landmark document, Crenshaw (1989) underscores how the convergence of multiple axes of disadvantage (i.e., race, gender, and class) contributes to multi-level marginalization and oppression. Intersectionality also serves as an analytical tool for understanding how social locations that intersect at the individual level are reflective of systemic privileges and oppressions occurring at a structural level (Bowleg, 2012).
In recent years, intersectionality has been used to examine women’s experiences within various contexts: identity development of Black women who are doctoral students and parents (Tucker, 2016), newcomer women’s experiences with perinatal care (Pimienta et al., 2022), Black female sexual health (Crooks et al., 2021), and the association between gendered racism and health for Black women (Lewis et al., 2017). The application of intersectionality theory is particularly useful in understanding Black women’s experiences of accessing healthcare as their health outcomes differ from both Black men and White women (Veenstra & Patterson, 2016), suggesting a distinct perspective that cannot be thoroughly examined through the lens of race or gender alone. Analyzing our data through an intersectional lens allowed us to understand how participants’ interconnected social locations shape their access to healthcare in Alberta. Though our study addresses various processes of privilege and oppression, our analysis was anchored on the axes of race, gender, and class as a means of recentering Black feminism in the application of intersectionality (Aguayo-Romero, 2021).
Methods
This manuscript reports on interpersonal-level barriers and facilitators to healthcare access as identified by a sample of Black women in Alberta. Focusing on this level of analysis allowed us to provide an in-depth exploration of how interpersonal processes such as Black women’s interactions and relationships with healthcare providers, family, and friends impact their experiences of healthcare access and affect health-related behavior and outcomes (McLeroy et al., 1988).
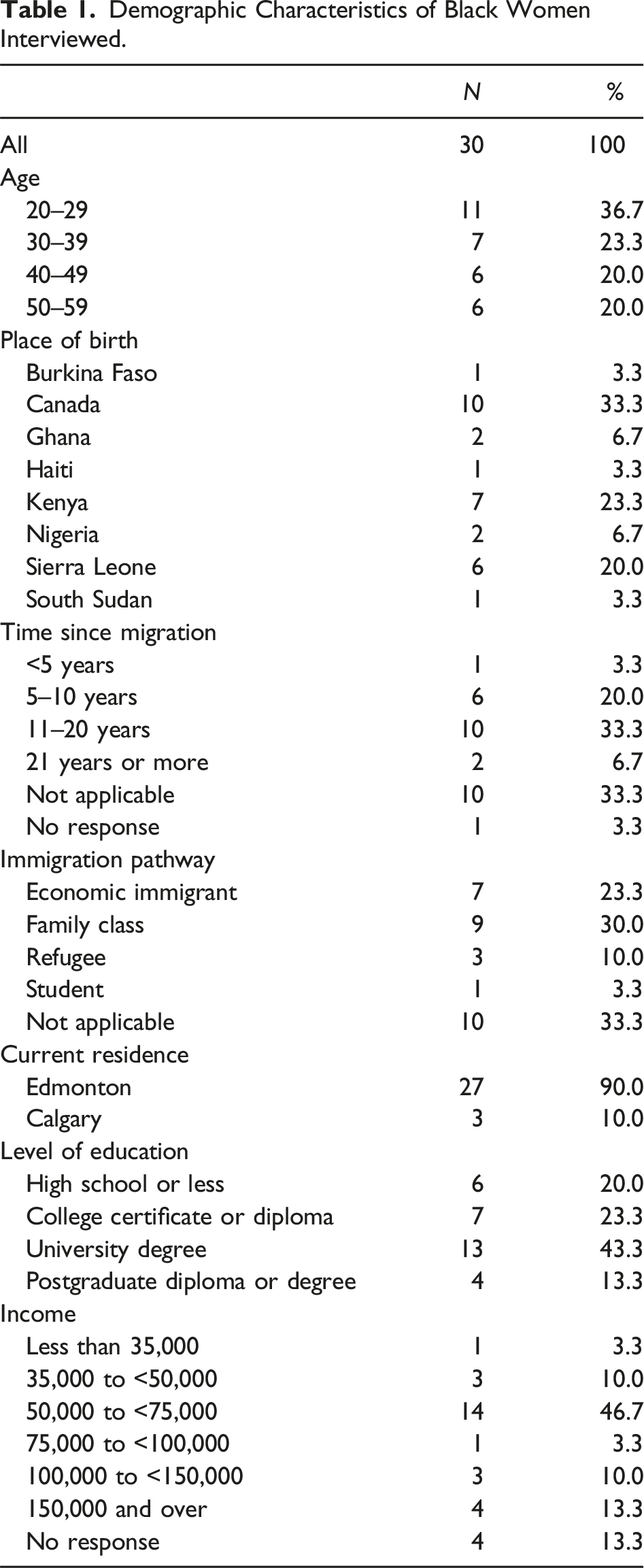
Ethics approval was granted by the University of Alberta Research Ethics Board (Pro00115790). We purposively recruited participants through established community relationships and snowball sampling. Participants had to meet the following criteria: identify as African, Black, or Caribbean; live in Alberta; and be over the age of 18. Interviews took place online by video call (Zoom) after participants read and signed the informed consent document provided by the research assistants. A few participants provided verbal consent at the beginning of the interview. Research assistants offered the opportunity for participants to ask questions before proceeding with interviews. Participants also completed a demographic questionnaire which included questions about age, gender, level of education, immigration pathway, and income. Interviews were semi-structured, lasting approximately 1 hour, and were recorded with consent from participants. Audio recordings of interviews were transcribed verbatim.
Data analysis was completed by a research assistant (MO) under the direct supervision of the principal investigator (BS) using NVivo qualitative analysis software. We adopted Braun and Clarke’s (2006) thematic analysis framework to facilitate the identification, analysis, and reporting of patterns of meaning within the data. Preliminary codes were generated based on our research questions; the research assistant also coded inductively, identifying additional codes that emerged from iterative engagement with the data. In addition to independent coding, rigor was ensured through the use of thick descriptions in sharing our findings, acknowledging our positionality, and engaging in reflexivity.
Positionality
The lead researcher (BS) and research assistants (MO and LK) for this study all self-identify as Black women; additionally, BS and MO are healthcare professionals, with MO having a recent history of employment within Alberta’s healthcare system. As part of the population of interest, we engaged in ongoing reflexivity to attend to tensions stemming from our positionality, acknowledging that there was potential for our insider and outsider status to affect various aspects of the study such as the design, data collection and the researcher–participant relationship, data analysis, and the reporting of our findings (Engward & Davis, 2015). We engaged in reflexivity through reflexive notes and bi-weekly discussions during research team meetings. Additionally, data analysis was iterative to allow the research assistant to critically engage with the data while accounting for their self-location with consideration for their proximity to the data (Olukotun et al., 2021). As Black women who have also accessed healthcare within Alberta, the researchers were careful to separate their personal experiences from that of participants to mitigate the risk of biases.
Findings
Demographic Characteristics of Black Women Interviewed.
Barriers to Healthcare Access for Black Women
Participants shared many barriers to accessing healthcare in Alberta. Interpersonal-level barriers to access were predominantly due to patient–provider discordance and negative encounters. Most participants experienced several barriers concurrently which affected their ability or desire to access needed services.
Patient–Provider Discordance
Participants identified several forms of discordance which posed barriers to their healthcare access. The various forms of discordance encountered hindered effective communication and the opportunity to establish a relationship with their provider which negatively impacted the ability to have their health concerns thoroughly addressed by the care provider.
Language
Several participants indicated that navigating the health system as newcomers with a non-English native language was challenging as care was typically delivered in English. They felt that their English proficiency was not at a level that allowed them to fully detail their concerns and would have been more comfortable communicating in their mother tongue. Language accommodations by healthcare providers were rare, and participants were left to navigate these situations on their own. One participant shared that the impact of language discordance on her care was bi-directional in that it limited expression and understanding for herself and the healthcare provider: … language can be a big—a big barrier for you to get what you want, to get your care, or to express, even to express if you have something going on with you, to express it to the person, so for the person to provide you what you need, or for you to get what you want. Language can be a big—a big—yeah, it can be a big red flag for you to get that—to get your—to get access. Like even over the phone, or in person, yeah, language can be, yeah, the biggest one. (EDM09)
This participant reported that despite ongoing language barriers to communication, she was never offered translation services; instead, she was typically asked, “When you’re coming for your next appointment, try to come with a translator, somebody who can translate, who can kind of communicate more clearly and make it easier” (EDM09). Another participant who worked as a healthcare provider also commented on this issue, stating that the lack of translators contributed to language barriers between patients and providers: And if they don’t bring somebody to interpret for them, then you don’t have anybody to interpret for you or work with you. That’s one big thing. We don’t have representation there at the hospital, so. (EDM21)
Participants described this issue as detrimental to their well-being, based on the limited ability to discuss their health concerns and care management with their providers. For some participants, limited English proficiency resulted in inadequate care; for others, there was also concern about inappropriate care. One participant shared an example of how miscommunication due to a language barrier can contribute to misdiagnosis or poor management of health: Just because, you know, like you don’t—say you don’t speak English, or the common language, and they’re having a hard time understanding you or just kind of, you know, getting a conversation through, they—again, you get treated like—or they just they would even give you the medication, or they would give you the care that they deem is the best fit. Maybe it’s not even for you, just because, you know, you cannot speak the language and let them know, “Okay, no. Like I don’t think I need that,” or, “I don’t consent to that,” you know? So language is a big, a big factor. (EDM02)
Culture
Cultural differences served as a barrier to a shared understanding of how participants experienced various health issues. Due to this disconnect, participants reported often feeling misunderstood by care providers. In one participant’s account of repeatedly seeking care for an acute concern, she shared that she was only finally understood by a physician with a similar cultural background, whereas previous physicians were unable to address her concern. She stated: I got a very, very bad rash, like a very crocodile looking rash on my skin, very embarrassing, even. And I went to the same clinic I was going to […] So every time I went, they’d give me something that wasn’t working, then I’d go again, it wasn’t working. Then I would go again, it wasn’t working. Until they eventually sent me to a specialist now, who did a biopsy on me, and it happened to be an African doctor, so I was able to explain how I was feeling, what was happening. And he gave me medication that dealt with the itch, you know? [Laughs] Oh, it was a nightmare. Yeah, so because I could really—there’s nothing different I was telling these other doctors, but they were not giving me anything that was helping and sending me home. And I would like—like itch, you know, to the point of bleeding, but nobody cared. (CAL01)
Another participant expressed a similar concern, elaborating that cultural and racial background impacted whether a provider understood an issue. This was partly due to unconscious biases which influenced if providers believed the experiences of a Black women seeking care: Then there has to do with actually getting heard and believed by the health practitioners. So if they’re of a different culture, or of a different race, they may not necessarily always understand the issue. They may not even—there might be an unconscious bias towards the individual, so that therefore, again, we’re kind of just kind of sitting there after an appointment like holding the ball, having to kind of figure out, “Okay, well, this person’s not going to hear me, so I have to now [Laughs] take more time out and find another person who might be able to hear me.” So it’s just a constant struggle. (EDM16)
Speaking to experiences of seeking primary care, a majority of participants shared that most of the physicians they had interacted with were White, with very few Black physicians accessible to them. For many, there was an overlap between race and culture, and in seeking care, not having a physician from the same cultural background made them feel out of place or hesitant about opening up: We are poorly represented when it comes to the medical field. We don’t have many Black doctors …. Well, I guess there is that kind of feeling, like you are out of place, and probably many people would feel the same, talking to somebody totally blinded to your cultural background and some of the issues that they may be dealing with health-wise. (CAL02)
Gender
Some participants valued family physicians who were both Black and a woman. In her search for a Black female physician, one participant criticized the Alberta Health Services search function which limited the ability to search by race, making it difficult to know how or where to look for a Black female family physician: I don’t think there’s a lot of Black female GPs in Alberta. And then for the way to find them, I’m having a tough time even knowing where to look. Like if I search that up, that’s not coming up with anything, or if I’m going through AHS, that’s not one of the criteria, for example, right? So it’s a little bit difficult for me knowing where to look, and even if I’m like talking to people in the community, they’re saying like the female GPs that they know are already fully booked. (EDM27)
While this participant believed that there was an overall lack of Black female family physicians, others argued that the issue wasn’t in their numbers. However, there was agreement in their lack of visibility. Participants expressed great difficulty in finding Black female physicians despite a high need from Black women in the community: I feel like there is a lot of Black doctors out there, but they’re just—in terms of that visibility, it’s very poor, especially when Black ladies, because I know a lot of Black ladies would like to have a Black doctor, if they can. (EDM22)
Negative Encounters
Participants described negative experiences in accessing healthcare in Alberta due to factors such as being dismissed or misunderstood, racism, and mistrust issues. These adverse encounters profoundly influenced their experiences accessing care.
Dehumanized and Dismissed
Participants shared instances of impersonal care which left them feeling dismissed—like physicians having no interest in them as a patient or a person. This was often coupled with the routine use of medical jargon in information-sharing, especially as it related to patient education: It is like I feel like my doctor doesn’t know—know me, doesn’t take enough time to get to—to know me as a patient, to know where I’m coming from, to know what kind of things he should explain to me maybe in a layman’s language, so I understand it better …. He just opens the door, and he just goes directly to his computer. So, “How are you? How can I do—what can I do for you today?” And he just starts to type. No eye contact. (EDM11)
For many participants, a lack of attentiveness to their medical history or current health concerns contributed to feelings of not being heard. Another participant detailed how the unique manifestation of certain conditions in Black people led to her concerns being ignored. She argued that in addition to being Black, being a woman also influenced whether a physician was willing to listen to her concerns: And so like when a White person is red, they are red, but if a Black person is red, like it’s really hard to see. [Laughs] And so you can imagine, you might have specific symptoms, but they can’t even see properly. Or like I’m allergic to like this specific adhesive, and it gives me like a rash, but like it takes a long time for the rash to be very visible to the naked eye, and I think like just things like that, because I’m Black, I’m sure can be under—and then on top of that, like being a woman, like you’re, you know, you’re intersectional now, so you—like maybe your interactions with like doctors, sometimes like there is like a—as a woman, maybe they might not even want to listen to you. (EDM07)
Racism
An overwhelming majority of participants reported experiences of prejudice, stereotyping, and discrimination based on their race. For our participants, incidences of racism typically coincided with other forms of bias related to gender, culture, or immigration and/or Canadian status. One woman reported being treated with less respect under an assumption that she was not knowledgeable about the care she should be receiving: But the way they are treating others versus they are treating me is not like—it’s like I’m coming—they are putting me like in the same bag like a bushman or something, someone who came, like [Laughs] who doesn’t know anything. So they have the—they say, “Okay, she doesn’t know anything, so we can do whatever we want. We can say whatever we want.” … Sometimes they say we don’t know anything, or we—I don’t know. The system, it’s like we are not deserving the treatment, or the respect, or they will treat you, but the way they behave, the way they talk to you is like, “Oh, okay. You are—you are lucky to be like in Canada.” (EDM26)
Incidences of racism were not limited to healthcare professionals alone but also took place in interactions with other healthcare personnel and auxiliary staff: The only thing, like if I go to the clinic, like the receptionist, because they are—they are White—White ladies there. Like people with colors, if that’s how I should say it [Laughs], so sometime they have this attitude like they don’t talk to you nicely. Like if you need something, like if I’m late, something like five minutes—because I don’t drive, so it would be like a couple times, like if I go there, even like ten minutes late, so they won’t allow me to see the doctor. They will ask me to rebook for the next one. And sometimes the tone of their voice—because, you know, like talking to somebody, you don’t need to—you can tell that oh, this person is like kind of racist, maybe because of my color, the way they talk to me. (EDM20)
Conversely, a few participants noted that while they had experienced some challenges in accessing healthcare, they did not believe these circumstances to be due to their race but broader issues experienced by most within the healthcare system: I’ve not really had like situations where I’ve been somewhere and somebody bluntly told me to my face, “I can’t treat you because you are Black.” I haven’t had those kind of straight situations. But I just know generally, like either Black or White, like there’s just a gap in access—like there’s a gap in accessing healthcare. (EDM23)
However, some participants reported that previous experiences of racism impacted how they now navigated the healthcare system. For instance, several women suggested that they had to be especially attentive to how they were dressed when seeking care in order to counter negative stereotypes about Black women: I know from going to my doctor’s office, I just I need to make sure I’m presentable, and I can’t pull up looking like, you know, a certain kind of way [Laughs], because I don’t want to be perceived in a certain type of way, right? So of course, you know, maybe we have to put a little bit more prep and care and mindfulness into those things, in comparison to people from other races, because we know the sort of stereotypes which can be attached to us, and unfortunately, there’s that. (EDM08)
Distrust and Mistrust
Distrust and mistrust were common threads among participants’ experiences of healthcare access. For the Black women in our study, their distrust was based on previous incidences or doubt about the intentions of healthcare professionals due to a lack of transparency, which led them to question the information shared with them. One participant was displeased at the casual manner in which her physician discussed a potential surgery. She was unconvinced of their decision-making, especially since she felt that their rationale was not clear: They kept on saying, “If things don’t change, you might have surgery.” Or what I’m thinking, “I’m not a guinea pig.” In my mind, I’m telling myself, “I’m not a guinea pig. I’m not going to go through this,” you know? [...] And that is why even for me to go to a doctor, and they tell me some things, I always ask, “Is it?” I mean, I don’t innocently just accept. (CAL01)
Relatedly, several participants reported looking online to cross-reference information provided by their physician. One participant asserted that it was important for individuals to ask questions during healthcare encounters and follow up with self-education: Like I know people say don’t go on Google and Google your symptoms, and stuff like that, but I also try to like read papers [Laughs], and read articles, read—go on, like try to search things up, just so that I have an idea. Or, for example, even if a doctor prescribes you medication, like you should probably Google what that is, to know [Laughs] like, “Okay, what am I ingesting?” Like I feel like a big thing that sometimes people don’t realize is you also need to have personal responsibility in your health. And so whilst maybe they might not have the medical background, or like I do, but taking personal responsibility means that when you—when a doctor gives you a diagnosis, or tells you to take this medication, you should ask questions. (EDM07)
Ultimately, due to their negative encounters in accessing care, some participants delayed care or avoided seeking care altogether for their health concern, unless it was an issue requiring urgent attention. One participant opened up about this matter, expressing the hesitation felt by other participants due to the potential of a negative interaction or being dismissed by healthcare providers: But yeah, like I know, for example, I need to even go get a physical done. I never had one, but like it’s just like what’s scaring me is just the talking down part, and so it’s not even—at this point, it’s not even fees. It’s more so like that human interaction with somebody that is scaring me from going to go get a physical done …. And it’s just that like human interaction, or the like, “I don’t know what I’m going to get. I don’t know what person is going to convince me that I’m okay when I know that I’m feeling something, or that something’s actually wrong with me.” (EDM10)
Facilitators to Healthcare Access for Black Women
Participants reported positive patient–provider dynamics and individual and social network strengths as supportive factors at the interpersonal level of accessing healthcare.
Positive Patient–Provider Dynamics
Among the Black women we interviewed, positive patient–provider dynamics were reported as vital to good quality care. Positive patient–provider dynamics were facilitated by patient–provider concordance and having a patient–provider relationship. These dynamics were associated with feeling respected and heard by healthcare providers. Effective communication and empathy were also cited by participants as aspects of care encounters that contributed to more positive experiences.
Patient–Provider Concordance
For many participants, there was comfort in having a Black physician oversee their care. Participants reported being more at ease with a Black physician due to being able to communicate their needs, feeling a sense of ease in that their concerns would likely be acknowledged. One participant expressed surprise after visiting a walk-in clinic that was staffed by a Black physician. She shared that she felt relaxed because she could speak freely without fear of being misunderstood: … the first time I saw a Black doctor was I went to a walk-in clinic at Northgate, and the Northgate, the mall, the mall at Northgate. And this guy was Black, and it was a walk-in clinic, so I was really surprised. I’m like, “Oh, wow, this is good, and I can actually relax, and come and talk to him, and [Laughs] without no fear that he will not understand what I’m saying.” Because [Laughs] although, yeah, I do speak clearly, but sometimes they still ask, “Oh, pardon me? What did you say?” (EDM17)
Participants also shared similar sentiments about being cared for by a physician who was a Black woman. One participant highlighted that it was especially helpful for her as it was easier to discuss certain topics with a woman. To her, having a care provider that looked like her and had a similar cultural background contributed to better care: And she was very understanding. I kind of felt that the fact that she was Black, she was African, it was—it was better. The other thing I can also say is that I feel more comfortable with women doctors, because we have something similar, rather than the men. The men doctors are quite good, but there are issues that I wouldn’t want to discuss with a male doctor, so that’s why I prefer a woman of color, unlike a White woman. (CAL02)
Having a Patient–Provider Relationship
Participants valued having a relationship with their healthcare providers. One participant shared a sense of safety with her non-Black physician, who she described as being able to relate to her because of their relationships with other African and Black people: He knows where I come from, so most of the time he—we talked about back home, and he explained. He said he has been there before, and he relates, I guess I could say. He relates so much, because he knows Black—he knows African people a lot, because he said he has an encounter with African people. So for me, I feel safe with him, and when we talked and he always like gave—like answered my questions correctly and gave all the necessary things that I should do, additional things that I should not do. So I think it’s a great experience for me. (EDM17)
Another participant agreed on the importance of the patient–provider relationship. Her relationship with her family physician was one of mutual respect, and she felt her concerns were always addressed. Additionally, she expressed feelings of trust which allowed her to openly share her concerns: It is important to have a good relationship with your doctor, because that trust, you know, that mutual trust, once it exists, it’s also easy for you to narrate your health issues, discuss openly, and the person is equally—or the doctor is equally open, and they will make suggestions. (CAL02)
Individual and Social Network Strengths
Participants built on their strengths and the skills of their social networks to facilitate their access to healthcare. The combination of individual and communal strengths empowered Black women to better navigate the barriers they encountered.
Advocacy for Self and Others
Many participants shared experiences of advocacy for themselves and from others. Advocacy was typically associated with persistence in ensuring that one’s concerns were taken seriously, especially after being dismissed by a number of healthcare providers. For some participants, family members who worked in healthcare became their advocates, helping them navigate situations where they were not receiving adequate care, or their needs were not being met: My mom is also a healthcare provider, so she has always over-advocated for me anytime I’ve been sick, so they usually know they have to take what I’m saying seriously if I’m in the hospital, when I had surgery once. They usually know that—like—whatever they could get away with, they probably can’t, because my mom knows the procedures on different types of things. So yeah, it’s probably—I probably get a little bit better healthcare, whether it’s her just taking over [Laughs] to take care of me, or—or she’s demanding certain things be done by the healthcare providers, so yeah. (EDM05)
Participants generally reported self-advocacy as something they routinely practiced when accessing healthcare. One participant remarked that she had engaged in a lot of self-advocacy in various situations over the years, facilitated by knowing her rights within the healthcare system. She shared that her self-advocacy allowed her to address barriers in accessing care as a Black woman: I’m in those situations where I can advocate for myself, and I’ve never really—it’s not something that I have—outside from those isolated incidents, in general, I feel because I am aware of my rights, I don’t let it—I don’t let the barriers—I break—I confront those barriers. I fight for my things, yeah. So [inaudible] for me, but I’ve had to do that because I’m a Black woman, right? (EDM01)
This participant also stressed that advocacy was important in accessing healthcare, not just for oneself but also for the next woman and one’s community as well: But I think for me, advocacy is key. I think whether it’s for yourself, or that it’s for your community, I think knowing your rights is really important, and knowing that it is your right to get healthcare, to access health, yeah. And so fighting for it is important because when you’re fighting for it, you’re not just fighting for yourself; you’re fighting for the next woman, right? (EDM01)
Health Literacy
Health literacy allowed participants to utilize healthcare from an informed perspective. Participants commented on knowledge as a tool to facilitate their access to healthcare and manage care encounters. For one participant, health literacy was fostered by her sister who was a practicing nurse. Her sister was a source of information about how to best navigate the healthcare system: My sister is a nurse and she like oftentimes—like we’re very fortunate to have her. At least that’s one person that’s in the healthcare system that kind of knows how it operates and kind of knows how to navigate it. So if I ever need help understanding on how to push for something, then like she’s there. (EDM04)
Another woman had the opposite perspective of the use of health literacy in healthcare access, sharing that her understanding allowed her to support others’ knowledge of their health and the healthcare system: And, you know, it’s good that maybe like I’m literate enough to really grasp that, but I do have friends that, you know, they don’t. Like and they’ll always like come up to me to ask questions, or, “What does this thing mean?” Because it not really—like they don’t really grasp it easily. So I guess it’s just for me, like understanding what is that thing, explaining what it is, why it’s important to have it, you know, things like that. (EDM23)
Social Network Supports
Overall, participants demonstrated that people in their social network played a supportive role in their ability to access healthcare. For some participants, a family member or friend was able to connect them to information or services they needed. In one instance, a participant’s sister referred her to a family physician, who eventually took on the participant’s husband and kids as patients as well: Um, actually, I just changed family doctor, because my previous one is going for retirement, and it wasn’t easy to find it, because he’s from my sister, so he doesn’t get—he doesn’t take new patients [inaudible] so somebody has to refer you to him, in order for him to accept you as a new patient. Because he’s my sister’s doctor, so my sister referred me to him, and I think it takes like one, between one to three months to get an appointment with him. And it is the same. Like I went into to get for my family, like my husband and my kids, so he said he’s very—he’s not taking new patients now, because he’s full, but because it’s my husband, he said he will take him next month. So like there is a wait. (EDM09)
Participants were open about the importance of being able to rely on others for support. There was an emphasis on reciprocity in this communal approach to care access, sharing that it was sometimes necessary to seek help from others who would later offer support as needed. One participant spoke passionately about this. She was willing to go above and beyond for anyone who sought her assistance: Sometime when you discuss things with your own fellow Black women and say, “I need help,” and women—women help. Then you don’t have to go into details. Then maybe that woman will also help you to direct you where you can go and get help. Me in particular, if you come to me and you ask me for help, my dear, I will go to … I will go to the maximum—I will go to the maximum level to help you. I will show you where you can get help. (EDM18)
Discussion
The stories shared by our participants suggest that Black women’s experiences of accessing healthcare in Alberta are influenced by interpersonal-level factors which interact in various ways depending on the social context and power dynamics at play. The barriers and facilitators we identified from our thematic analysis show how Black women’s positioning at the intersections of race, gender, class, and other social categories can be both a source of marginalization and empowerment. We elucidate the complex interplay between these social processes as they relate to our participants’ interactions with the healthcare system. We also acknowledge how the Black women in our study drew on their individual and social network strengths to mitigate barriers to their healthcare access.
Health equity, as defined by Braveman and Gruskin (2003), is “the absence of systematic disparities in health (or the major social determinants of health) between social groups who have different levels of underlying social advantage/disadvantage—that is, different positions in a social hierarchy” (p. 254). It is generally accepted that access to healthcare is a foundational aspect of health promotion and supports health equity within populations (Canadian Public Health Association, n.d.; Government of Canada, n.d.). However, in Canada, systemic discrimination and other injustices contribute to inequities in health service access and social determinants of health (Public Health Agency of Canada, 2020, 2022). For Black people and other racialized populations, racism taints their experiences of accessing healthcare and consequently is implicated in healthcare access disparities (Husbands et al., 2022; Mahabir et al., 2021). Black women, in particular, are subject to coalescing forms of discrimination within the healthcare system which contribute to their differential outcomes compared to the Black population and the general population (Veenstra & Patterson, 2016).
Data from across Canada exposes how multiple levels of racism and discrimination contribute to the health inequities experienced by Black communities (Public Health Agency of Canada, 2020). For Black Canadians, healthcare access at the patient–physician level is marked by challenges such as differences in approach to care, racism and discrimination, and poor cultural competence (Fante-Coleman et al., 2022). A significant barrier and common thread among our participants’ experiences was the perceived lack of racial, gender, and cultural concordance between themselves and their providers. For many, this was rooted in a desire to be respected and heard during their care encounters. Unfortunately, participants shared incidences of being dismissed or not taken seriously due to their race and gender. Such disregard for patients’ concerns due to prejudices or a lack of shared understanding are examples of the epistemic injustices faced by Black women in navigating the healthcare system (Paton et al., 2020). For our participants, their physician’s race, gender, and cultural background were perceived as factors that dictated the type of care they would receive. These perspectives are not unlike findings in the literature. For example, Weisse et al. (2001) identified variability in approaches to pain management for White and Black and male and female patients depending on physicians’ race and gender, which was suggestive of interactions between race and gender at the patient–physician level.
Our participants shared experiences of disrespect and mistreatment, discrimination, dehumanization, poor communication, and unequal access, similar to incidences shared by racialized patients within Toronto’s healthcare system (Mahabir et al., 2021). The Black women in our study criticized constantly rushed appointments and an unawareness of their personhood, which led to inattentive, impersonal, and dismissive care, echoing the findings from Fante-Coleman et al. (2022) focus groups with Black Canadians on their experiences with healthcare access. However, as both Black and woman, participants wondered if their negative experiences were due to their race, gender, or other social presentation or category considering “race and racism work with and through gender, ethnicity, class, sexuality, and/or nation as systems of power” (Collins, 2022, p. 85). Other participants reflected on their experiences of navigating the healthcare system as new immigrants to Canada, which for them was associated with unique challenges related to language barriers in accessing information and care. African immigrant women, for instance, face barriers to healthcare related to language, communication, access, and navigating the healthcare system (Matini, 2023). In particular, the lack of accommodation which our participants experienced related to language barriers directly contributed to their feelings of disregard and impersonal care. From some of our participants’ recounts, it seems that Black women are at risk of falling through the cracks of the healthcare system as ultimately, their negative experiences in accessing healthcare sometimes led to delaying or avoiding care.
For our participants, racial, gender, and cultural concordance fostered feelings of being “seen” and respected which contributed to positive patient–provider dynamics. Factors such as effective communication, empathy, and attention to patients’ cultural needs were cited by participants as important factors in establishing a genuine connection with healthcare providers and building authentic therapeutic relationships with their family physicians. Positive relationships with physicians and being cared for by physicians who were African, Caribbean, or Black have been previously documented as facilitators of healthcare access for Black Canadians (Fante-Coleman et al., 2022).
Relying on their skills in addition to leaning on their support networks is a reflection of Black women’s sense of caring as a communal practice (Etowa et al., 2017; Zinobia & Taylor, 2022). Participants deployed their health literacy skills in accessing healthcare for themselves as well as supporting the access of others within their social networks. Their understanding of their health and health information as well as how to access health resources and navigate the system fostered their empowerment and is a hallmark element of health literacy as a tool for health promotion (Canadian Public Health Association, n.d.). In some cases, health literacy facilitated advocacy and community care among our participants. Social well-being, especially as it relates to social inclusion, fosters access through the sharing of information, resources, and other forms of tangible support (Canadian Public Health Association, n.d.). In the face of the barriers experienced, our participants demonstrated resilience in their persistence of their right to access healthcare. The Black family, “Black Girl Magic,” and Black sisterhood serve as protective factors that facilitate resilience in Black women and girls, allowing them to thrive (Zinobia & Taylor, 2022). In particular, the support networks our participants relied on, which are typically built by Black women among their peers or elders, allowed them to “cultivate communities of support” and nurture collective coping from shared experiences, and empowered them to navigate inequities (Zinobia & Taylor, 2022, p. 223).
Black women experience racism in routine situations of everyday life and within various social contexts (Beagan & Etowa, 2009; Essed, 1991). Previous reports (Black Health Alliance et al., 2020; Veenstra, 2019) suggest a relationship between experiences of everyday racism, discrimination in healthcare utilization, and poorer health outcomes. Acute and chronic experiences of racism are implicated as a social determinant of health (Paradies et al., 2015) and are argued to be “the root cause of racial groups experiencing systematic differences in their everyday living conditions and lived experiences, and thus in their health status” (Siddiqi et al., 2017, p. 136). Racism within Canadian institutions such as healthcare contributes to undertreatment when seeking care; as such, Black Canadians are less likely to benefit from health services despite a universal healthcare system (Canadian Race Relations Foundations, 2015; United Nations Human Rights Council, 2017).
Though the two healthcare systems differ, our findings corroborate the results of recent studies in the United States examining healthcare access for African American women and African immigrant women (Ahad et al., 2019; Okoro et al., 2020; Tefera, 2024). Collectively, we underscore the pervasive nature of the mistreatment experienced by Black women when attempting to access health services. Though this paper focuses on the interpersonal-level factors of healthcare access for Black women, these barriers cannot be perceived as individual acts. These incidences of dismissal or discrimination should be acknowledged as enactments of deeply rooted biases within broader systems of injustices and inequities (Aguayo-Romero, 2021; Bowleg, 2012).
Strengths and Limitations
Though we attempted to recruit participants from across the province, our final sample only included women from Edmonton and Calgary, two major metropolitan areas with the highest population of Black people in Alberta (Statistics Canada, 2019). Additionally, a significant proportion of our sample lived in Edmonton at the time of the study. These sampling tendencies were, in part, due to our recruitment strategies, where we relied on our established community relationships and participant networks which were primarily in Edmonton. This limited our ability to recruit from smaller cities outside Edmonton or rural areas where Black women may have differential experiences due to the amount and type of resources available to them. Furthermore, contacting participants through online methods (email) and conducting interviews virtually may have limited those without or with limited internet access from participating.
Additionally, though a few of our participants shared previous experiences of language as a barrier to their healthcare access, all interviews were conducted in English. It is possible that this inclusion criterion restricted the contribution of some Black women who are not fluently English-speaking, and thus their perspectives and experiences are not fully represented in our study. Lastly, our demographic data did not account for other characteristics that may have supported further nuance in our analysis and understanding: the omission of gender orientation and primary language spoken at home. Acknowledgement of the diversity of the Black population should include consideration of how various social attributes may impact experiences of accessing healthcare. Considering these limitations, future research on access to healthcare for Black women should make intentional efforts to recruit participants from more underrepresented geographic areas and be intentional about the inclusion of non-native English speakers and gender-diverse women as their needs may be different from those reported in our study.
Conclusion
Despite the challenges outlined, the resilience and resourcefulness of Black women in seeking and advocating for quality healthcare are evident in the study. Their voices call for systemic changes, including improved cultural competency training for healthcare professionals, increased representation of Black healthcare providers, and enhanced patient-centered care approaches that prioritize trust, respect, and inclusivity. Overall, this study sheds light on the multifaceted experiences of Black women in healthcare access, highlighting both the barriers they face and the strengths they draw upon in navigating these challenges. It underscores the urgent need for targeted interventions and policy initiatives to address healthcare disparities and ensure equitable access to quality care for all individuals, regardless of their cultural or racial background.
Footnotes
Author Contributions
BS conceptualized the project and mentored research personnel. MO and LK conducted interviews and data analysis. MO and AM drafted the manuscript. AR, MO, SR, and BS provided critical feedback on the paper. All authors contributed to the finalization of the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Women and Children’s Health Research Institute (WCHRI) Innovation grant (No. RES0055457).