
Abstract
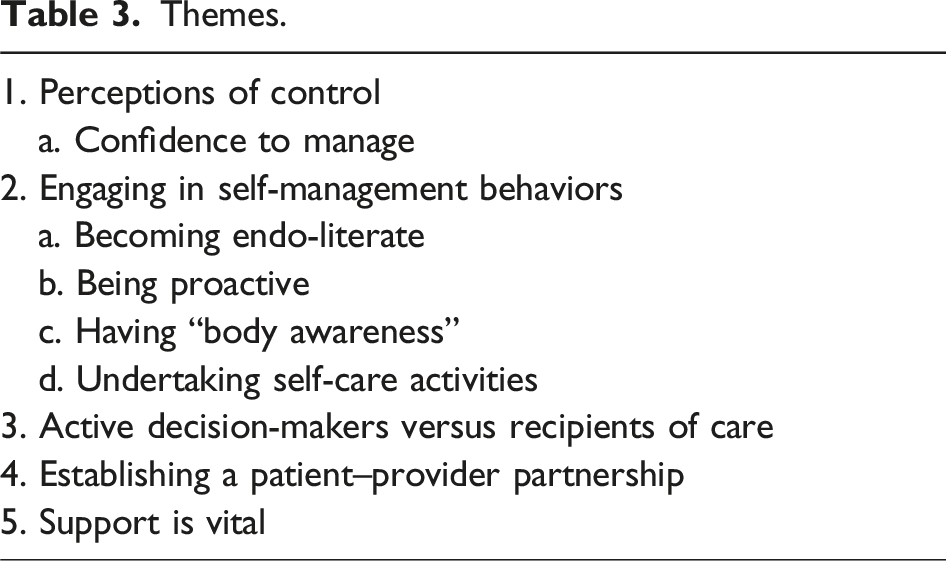
Self-management is pivotal for effective chronic disease management. However, this concept remains unexplored among people with endometriosis, who often experience chronic pain and significant impacts on their quality of life. This research explored participants’ experience managing endometriosis and their understanding and integration of self-management into their lives. Inductive reflexive thematic analysis was used to analyze transcripts from 15 semi-structured interviews among people with endometriosis. The themes captured many aspects of self-management and included (1) perceptions of control, (2) engaging in self-management behaviors, (3) active decision-makers versus recipients of care, (4) establishing a patient–provider partnership, and (5) support is vital. The extent to which participants engaged in self-management varied, however, is consistent with self-management literature for other chronic conditions suggesting that there is a role for self-management among people living with endometriosis.
Introduction
Endometriosis is a common inflammatory condition in which endometrial-like tissue grows outside the uterus leading to pain and adhesions. People with endometriosis can experience a diverse range of symptoms including pain with menstruation, heavy bleeding, gastrointestinal symptoms, pain with intercourse, and chronic pelvic pain (Zondervan et al., 2018). On average, it takes 5.5 years to be diagnosed (De Graaff et al., 2013), indicating a significant amount of time that individuals are dealing with symptoms without a diagnosis. Despite the significant burden, it can impose on people’s health and lives, endometriosis is rarely referred to as a chronic disease, yet an Australian policy review indicated endometriosis meets five of the six criteria of a chronic disease related to causation, duration, treatment, disease course, and impact (O’Hara et al., 2018).
Self-management is central to the management of chronic disease, and the World Health Organization recognizes the importance of people with a chronic disease being active participants in their own care (World Health Organization, 2002). Self-management is a multifaceted construct for which there is no agreed definition in the literature (Barlow et al., 2002; Van de Velde et al., 2019). Van de Velde et al. (2019) proposed the following definition of self-management: “the intrinsically controlled ability of an active, responsible, informed and autonomous individual to live with the medical, role and emotional consequences of his [sic] chronic condition(s) in partnership with his [sic] social network and the healthcare provider(s)” (p. 10).
Self-Management Attributes.
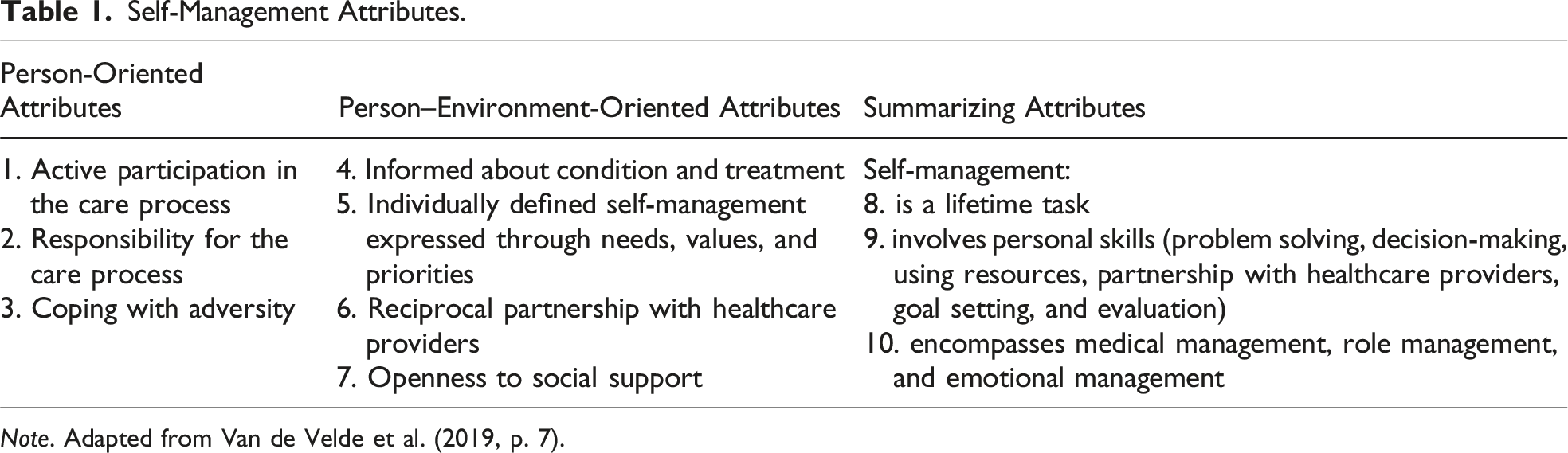
Note. Adapted from Van de Velde et al. (2019, p. 7).
It is important to note that while the terms self-care and self-management are often used interchangeably in the literature, self-care forms part of self-management and relates to the tasks that an individual performs at home to manage the symptoms of the condition and its impact on their daily life (Clark et al., 1991). In contrast, self-management is a broader concept that extends beyond self-care per the 10 attributes and definition provided by Van de Velde et al. (2019).
Self-management has been associated with improved health outcomes, quality of life, health behaviors and skills, self-efficacy, adherence, decreased mortality, and reduced health service usage/costs (Brady et al., 2011; Panagioti et al., 2014; Van de Velde et al., 2019). A systematic review determined that the concept of self-management remains relatively unexplored in the endometriosis literature (O’Hara et al., 2019). This research aimed to explore the participants’ experience of managing endometriosis and their understanding and integration of self-management into their own lives.
Methods
This article presents the results from the qualitative component of the Endometriosis Management in Australia study (a large mixed-methods community study). The large study explored women’s experiences of managing endometriosis in Australia and included a survey that enquired about participants’ medical history, treatment use, quality of life, and some aspects of self-management (e.g., self-care activities, self-efficacy, and engagement in healthcare) (O’Hara et al., 2021, 2022). While many of these aspects of experiencing endometriosis were suitable for study using quantitative methods, a qualitative approach was necessary to elicit participant-led, rich data to understand women’s lived experiences with managing the disease and the role, if any, of self-management in this process. Semi-structured interviews were used to collect this data. Ethics approval for the research was granted by the Monash University Human Research Ethics Committee (approval number 2017-1166).
Participants
Participants who completed the Endometriosis Management in Australia survey were invited to participate in an interview by providing contact details at the end of the survey. Women were eligible to participate in the survey and interviews if they were aged 18 or older, self-reported a surgical diagnosis of endometriosis, were able to communicate in English, and were living in Australia. A large number of survey respondents volunteered for an interview (n = 468). Therefore, purposive sampling (Gibbs et al., 2007) was used to ensure that the sample selected for interviews reflected a breadth of experience among women of different ages, education, time since diagnosis, and regional locations. An email invitation with the explanatory statement and consent form was sent to participants, and interested participants were asked to select a time, date, and their preferred method of interview (face to face, videoconference, or telephone). All participants provided written consent.
A total of 15 interviews were conducted between March and August 2018. Participants were aged between 19 and 58 years, resided in different geographical regions (major city, inner regional, and remote), had varying levels of education (“high school education or less” to “university education”), and included women who were at varying stages of their endometriosis journey (from those who were newly diagnosed to those who had lived with the diagnosis for 37 years).
Procedure
All interviews were conducted by the first author with one interview conducted face to face on campus, six via Zoom, and eight telephone interviews. Interviews lasted between 40 minutes to 1 hour and 45 minutes. The interview opened with the following question: “Can you tell me about your experiences of endometriosis?” and an interview guide provided prompts relating to managing symptoms, facilitators and barriers, self-management, and participants’ perspectives of endometriosis (Supplemental File 1). However, the conversation was directed by the participants’ responses.
Interviews were audio recorded (with permission) and transcribed. During the transcription process, transcripts were checked by the first author against the original audio recording for completeness and accuracy and any amendments were made. Transcriptions were de-identified by removing names, locations, health clinics, and names of health professionals before analysis. Interview transcripts were labelled by participant number.
The framework proposed by Malterud et al. (2016) was used to estimate the appropriate number of interview participants in this study. This is in line with Braun and Clarke’s (2022b) recommendation to use “information power” rather than saturation to determine the appropriate number of participants to include in reflexive thematic analysis studies. Malterud et al.’s (2016) framework includes considering the aim, specificity of participants, whether there is an established theory related to the study, quality of dialogue, and analysis strategy. At the beginning of the study, it was estimated that approximately 12–15 women would need to be interviewed; however, this was reviewed continuously throughout the study and discussed with the research team.
Data Analysis
Application of Reflexive Thematic Analysis.
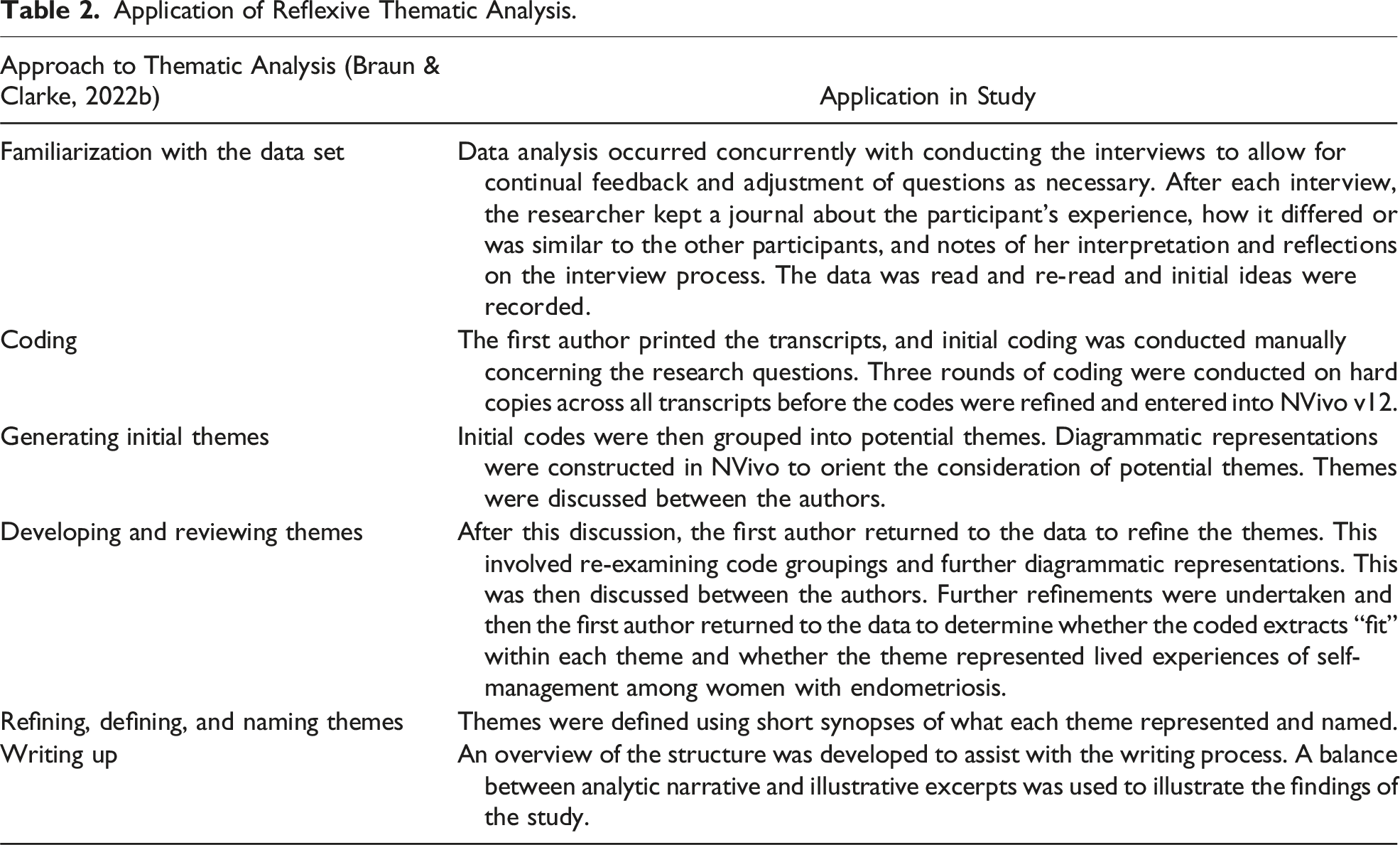
Regular meetings were held between the authors to discuss the interview and analysis process. Reflexivity was integrated into this project through the first author keeping a research journal to document their position as a researcher, perspective on methods employed, data generated and reflections on the research process, interviews, and analysis (Grbich, 2013). Discussions were held between the two authors after each interview to reflect on the process and data from the interviews. The first author undertook the preliminary analysis of the data; however, all themes were reviewed and finalized for publication by all the authors.
Results
Themes.
Theme 1: Perceptions of Control
The notion of control was central to participants’ experiences of endometriosis, including their experiences with managing and self-managing the condition. At different points in time, participants varied in the extent to which they believed they had control over their health and the symptoms of the disease, and this variability manifested in their decisions about treatment and engagement with self-management.
Participants reported that at times, they felt like there was only so much they could personally do to exert control over their symptoms and disease: Well, because I think some things aren’t in my control; I mean, you know, I can only do so much to, to um, to manage it, but um, my body has its own mind.
Perceptions of control seemed to affect participants’ willingness to engage in and perceived utility of self-management: I mean, I always tried to manage it myself, but it depends on how badly you’ve got it. Of course, you know, there are various degrees of endometriosis. I had it very severely, unfortunately. But I have heard of other women who just had it, you know, they had just had it, ah, a little bit of it. Ah, so as I say, it depends on how badly you’ve got it as to whether you can manage it yourself or not, I believe.
Control also seemed to affect treatment decisions. A few women had opted for a hysterectomy in an attempt to manage the disease. One participant felt the severity of the disease was such that she could not manage it and asked her doctor: … could you give me a full hysterectomy? I’m sick of going through all this pain, the bleeding each month, which really, as soon as one period ended the next one seemed to come on, started coming on. It was just continuous …
Others felt that there were actions that they could take to help feel like they had at least some control over the disease. Self-care tasks were seen as helpful for regaining a degree of control over the disease: If I follow that diet, I don’t seem to experience pain as much. But it’s also, um, I think, around a mental benefit because it kind of gives you the power back, in a way. Like, I previously never had any idea when a flare-up was going to come. When it happened, I didn’t know what to do, whereas now, when I follow that diet, I feel like I have it under control a lot more and it feels like I have a—a bit of control back over my body and the way that it’s reacting to things.
The extent to which participants felt that they had some control over the disease varied over time, depending on their circumstances, symptoms, and experiences. The perceived efficacy of the different treatment options in controlling their symptoms or disease often strongly influenced how women felt about their illness. For example, one woman had recently had surgery during which the surgeon confirmed that the current hormonal treatment was working and the disease had not progressed. She reflected that at that moment she felt that she was now in control of the disease; however, she also recognized that if she had been asked before the surgery, she would have felt that she had little control or confidence to manage the condition because “it just seemed like everything was going wrong.”
Confidence to Manage
Linked to perceptions of control was the confidence that participants felt in managing their condition. Some felt they were in control of their symptoms, knew what to do if they were experiencing symptoms, felt their management approach was working, were engaged in self-care activities, could advocate for themselves, and had connected with others with the disease so they felt like they were not “the lone ranger out there.”
Others reported that they did not feel like they were in control, treatments were not working, symptoms remained variable, they had some knowledge but would like to know more, or they were restricted by their circumstances, which compromised their ability to pursue additional management approaches. A participant reported that a lack of confidence influenced her emotional well-being: Not very confident, like trying all these things that I’ve tried and everything failing to, to help. It brings me down, it just sort of makes you feel useless or like, you’re, I’m giving up.
Levels of confidence seemed to be influenced by whether they had the strategies they needed to deal with symptoms, whether they felt they weren’t the only ones going through the experience, whether they could talk about their experience with others, and whether they had the necessary information to understand the condition and treatment options and could advocate for themselves. The outcome of various treatments and engagement in self-management behaviors appeared to influence both perceptions of control and the resulting confidence that participants had to manage their endometriosis symptoms, such that if the combination of treatments and self-management activities they were undertaking “were working,” they felt more in control and confident to manage the condition.
Theme 2: Engaging in Self-Management Behaviors
Participants spoke about several things they have done to manage their endometriosis, including becoming endo-literate, being proactive, having body awareness, and undertaking self-care activities.
Becoming Endo-Literate
Participants spoke of having limited knowledge about endometriosis before their diagnosis, with half of the participants indicating that they had not heard of the term “endometriosis” before their diagnosis. Among those participants who had heard of the term, some described their knowledge as limited or having heard about the disease from their friends or family members. A few had wondered before their diagnosis whether endometriosis could be the cause of their symptoms after reading information about the disease.
Nearly all of the participants spoke about educating themselves about the condition after their diagnosis. This education was self-directed, as a few participants noted that they were not provided with information at diagnosis. Some participants investigated how they could manage their condition better: I think once you go through it, you sort of, I guess, you do research a little bit to try and find anything, um, else that you can do. Any changes you can make to try and, um, make yourself a bit more aware and also to try and, you know, to make it easier for you.
Participants reported that their knowledge about the condition and its management had improved substantially with time post-diagnosis, although a few commented that they would still like to know more about the disease. Reported sources of information included research or medical articles, books, media articles, “Dr Google” and the internet, endometriosis associations, online support groups, and discussions with health professionals. Some women preferred experiential knowledge, seeking advice and information from other women with the disease through online support groups. So I tend to turn to other women now who have endometriosis to get advice and to get support, just because I feel like it—it works a lot better coming from people who understand it and have been through it themselves.
Being Proactive
Some participants spoke of being proactive when managing their disease. For some, such proactivity meant researching different treatment approaches before trying them; for others, it meant taking their pain medications pre-emptively to manage the pain, particularly before their period.
When participants were managing the disease outside of the home (e.g., work and social situations), they were proactive in their approach to managing the symptoms. They spoke about making sure they had their pain medications, a heat pack, being careful where they sat (as some chairs made them uncomfortable), using a transcutaneous electrical nerve stimulation (TENS) machine, wearing comfortable clothes, taking water, and frequent breaks (e.g., walking around and stretching). Some participants scheduled activities around their “worst time of the month”: I always had to manage it I had to manage my painkillers I had to make sure I had a heat pack with me and I had to make sure we weren’t you know where if we went out for lunch or something where we sat, how what the chairs were like how long we were there for.
The experiences of the women suggest that they implemented actions based on their symptoms. However, some women were proactive in the sense of being able to predict circumstances that may amplify their symptoms (e.g., symptoms being more severe around menstruation) and taking pre-emptive mitigating measures.
Having “Body Awareness”
Participants spoke about being in tune with their bodies and having “body awareness” rather than formally monitoring their symptoms (e.g., keeping a record of symptoms or using period tracker apps). For some participants, this body awareness prompted them to seek medical advice to obtain a diagnosis; for others, it enabled them to evaluate whether a particular medical treatment was working or prompted them to undertake self-care tasks to manage their symptoms. This sense of body awareness motivated some participants to respond to changes in symptoms or to the side effects of treatment, whether it be by following up with their medical providers or by discontinuing treatment because it affected the way they felt: Last April I had a Mirena inserted. I went for a follow-up earlier this year and I said to her, to the gynae, “I’ve been constantly bleeding and I have been constantly bleeding for probably 18 months.” A very, very precise pinpoint pain which I just felt, oh, this is different, and it wasn’t during a period, it was at some other time. And I just felt this is—this is abnormal, what’s going on here? And, um, er, it was discovered I had a, er, a rather large cyst on my left ovary and that turned out to be due to endometriosis.
Undertaking Self-Care Activities
Self-care was the most widely discussed aspect of self-management, with all participants reporting that they undertook some self-care activities. These activities included changing their diet, using essential oils, undertaking exercise, taking supplements, using TENS and using heat, and undertaking relaxation exercises.
The extent to which participants engaged in these activities varied: some undertook self-care activities during or in the lead-up to their period, others in response to their symptoms, and still others undertook these activities every day. One participant reported spending up to three hours a day on various self-care activities (e.g., physical stretches, relaxation exercises, meditation, and walking) to rehabilitate from surgery and “improve my physical and mental wellbeing in order to strengthen my capacity.” The perceived efficacy of these self-care activities varied: some participants reported that these activities were beneficial; others reported deriving little benefit.
Dietary changes varied between women. Some participants noted certain food triggers associated with their symptoms (e.g., gluten, dairy, caffeine, alcohol, some types of meat, and some vegetables), while others spoke of trying to “eat healthier” to improve their overall diet and general health (e.g., reducing intake of processed or packaged foods or sugar). A few participants adopted particular diets, such as paleo or vegetarian diets, and one participant reported trying to avoid chemicals (e.g., purchasing organic fruit and vegetables). One participant explained her attempts at dietary change: Um, I don’t strictly follow it seven days a week but I have cut back largely on red meat and wheat and dairy, um, and alcohol and all of that sort of thing, and I find that that does really help.
A few participants reported changing their diet based on information from health practitioners, while others changed diets on their own and self-assessed whether it improved their symptoms.
The self-reported efficacy of undertaking these dietary changes varied across participants: some reported that it improved their symptoms (e.g., reduced bowel disturbances and bloating, increased energy levels, or general improvement in overall health), as one participant noted after eating a trigger food: “I start to, it sort of starts to hurt again, so I understand a bit better now, that if I’m already feeling unwell, eating those things isn’t going to help me.” However, other participants reported no consistent improvement in symptoms associated with dietary change.
Some participants spoke of undertaking exercises to help with their symptoms, including walking, doing physical stretches, pelvic exercises, strengthening exercises, swimming, jogging, or yoga. Some reported benefits from undertaking exercises, in terms of reduced symptoms or improved overall physical and emotional health. However, others found that pain or fatigue either prevented or increased after, undertaking exercise: Like even now, when I walk, you know, at the shops for I don’t know, sometimes I can last 15 minutes, sometimes I can last half an hour, and then the pain comes on and then I feel like I’m going to pass out. So, it’s just extremely hard exercise-wise.
A few participants mentioned that it was difficult to stay motivated to exercise: Um yeah, I noticed that it was a struggle to push myself, um, because you’re just, you know, lying on the couch in pain with a heat pack, it’s kind of like the last thing you want to do. But once I did it, I would always feel better after it and a lot more positive. And, um, I think it’s also knowing that, you know, you are achieving even if it’s something small; you’re still achieving something and you’re still getting out of the house and, and doing something as opposed to just sitting there all day.
Some participants used heat to help manage the pain (e.g., warm baths, heat packs, hot water bottles, or heat patches). For some, the use of heat was associated with their periods while for others, such use was daily. Participants reported that the heat eased their pain “somewhat” and provided comfort and “warmth and you can—it’s an excuse to cuddle up, go to bed, and if you’ve got a hot pack wrapped around your belly, nobody asks you a question.”
Rest was used by some women to help manage their endometriosis symptoms. Some participants reported such extreme fatigue at the end of the day that they would “collapse straight into bed.” Others modified their behavior to ensure they weren’t over-exerting themselves, for example, by taking regular rest breaks at work or having an “afternoon nap.” For some, the intensity of the pain was such that there was no other choice but to rest, while others have found that pushing through the pain made it worse: Usually the first day of, of a period, I would get that colicky pain, really very severely to the point where I couldn’t do anything else except, um, be with the pain, as it were. So I would have to go and lie down and just sort of, um, tough it out. So if I’m feeling like I have a bad day, I will, I will rest and I will just wait it out until it goes rather than pushing myself, because I’ve found that, if I push myself through it, it just gets worse.
Theme 3: Active Decision-Makers Versus Recipients of Care
The degree to which participants actively engaged in decision-making around managing their endometriosis symptoms varied depending on their circumstances. Some participants spoke of times when they became active decision-makers taking ownership of their health decisions in comparison to times when they became recipients of care allowing these decisions to be made by others: Well, it was actually again my gynaecologist [who] pressured me into it. He said that if I didn’t try this medication [the Mirena] there was nothing else he can do and he’d have to take me off as a patient.
For some participants, being recipients of care, rather than active participants in care, occurred when they were younger, when they felt they could not question medical advice, or when they were first diagnosed and knew little about endometriosis.
Negative experiences with medications or surgery prompted some participants to take a more active decision-making role, which involved researching the potential treatment, asking other women with the disease for advice, and listening to their bodies. A few participants spoke about regretting some of their decisions when managing the disease, particularly about early decisions about the choice of health practitioner, surgery, medical, and fertility treatments: So, you know, quite happily went into surgery trusting that this doctor knew what he was doing, um, but, you know, he was not trained in excision or, you know, anything like that. So, in hindsight now [with] what I know, I wouldn’t have gone with surgery with him, but I just trusted him because he was a doctor and that’s what we’re supposed to do, so just went with it. Um, but I felt really unprepared for what I was about to go into, um but, I sort of felt like, well, this is a specialist. I assumed he knows what’s best and I trust that, you know, whatever he’s giving me is the best thing for me. So um, I sort of went into it [Zoladex injections] a bit blindly, um, and sort of definitely learned from that, that um you know, even if it takes a couple of days, go away and think about it; don’t just sort of, on a whim, accept that that’s probably the best answer.
Decisions about medical treatments, surgery, and complementary approaches were influenced by several factors at different times. In terms of medical and surgical treatments, some participants felt they were “out of options” or their symptoms were so severe that they accepted what was offered. For example, one participant decided to have a hysterectomy and oophorectomy because “the problem was getting worse and I had to do something and it felt like the only something I could do.”
In addition to health practitioners, participants reported that their decisions about the management of the symptoms and disease were influenced by several people. Some participants consulted family members and friends when evaluating options for treatment. A few also consulted other women with endometriosis through online support groups about particular treatments or asked for recommended practitioners to consult.
Theme 4: Establishing a Patient–Provider Partnership
Having a positive patient–provider partnership is necessary for the effective management of chronic conditions. Participants’ experiences with finding a supportive healthcare practitioner were mixed. Nearly all of the women interviewed for this study reported negative experiences at some time associated with seeking care for their endometriosis. A few participants reported struggling to find a doctor that they could work with, and a few had stopped consulting with some medical practitioners, with whom they had negative experiences (e.g., not consulting with GPs or specific specialists). Participants reported being dismissed in the lead-up to their diagnosis and after diagnosis when they presented with ongoing symptoms or side effects from treatments. I still have the same symptoms I had with the injections but now I’m getting others you know I like I said my hair’s falling out, I’ve put on weight and all this sort of stuff. And yeah then when he was like really dismissive about it um he said oh you know I don’t I don’t think those some of those symptoms are caused by that I’m sure it’s just stress and all that.
Some participants reported that they did not feel health professionals took the time to understand their experience, their priorities, and what their quality of life was like with the symptoms they were presenting with and experiencing. A few felt that they were “thrown in the too-hard basket” or were “shuffled out” of the specialist’s office.
Despite needing to try multiple health professionals until they could find one they felt they could work with, nearly all of the participants reported a positive relationship with at least one health professional (e.g., GPs, specialists, nurses, physiotherapists, complementary providers, and mental health professionals). Participants reported that the providers they had a positive relationship with had good communication skills and described that their chosen health professional listened to them and was empathetic and “easy to talk to.” Participants felt that they could ask the GP or specialist questions and were comfortable discussing concerns with them. They indicated that questions from their health professional tended to be accompanied by an explanation of why the information was needed.
Participants spoke about these positive interactions fondly and indicated that they felt there was a “genuine interaction”; some explained that this experience made them feel validated, while others valued the fact that their questions were answered (via a phone call or email) without needing to book another appointment: It was nice to walk in and have someone who listened. I think that’s the biggest thing. The hardest thing about this is that, for so long, you’re sort of treated like you’re a little bit crazy and you, you feel like no one’s listening and that no one cares and it, it’s refreshing to walk into a specialist who not only just spends, like, he spent the first, probably 10, 15 minutes just listening to me explain everything from the beginning to the end, and then didn’t dismiss anything, which was amazing. Um, so it definitely makes you feel validated and, and makes you feel like you’re not going crazy.
Participants viewed the patient–provider relationship positively when practitioners took the time to listen and understand their experience with the condition or symptoms. These practitioners focused on their well-being and worked with them to identify the best treatment option for their circumstances. In addition to presenting options like medication and surgery, participants reported that a few practitioners suggested that they engage with allied health practitioners (e.g., psychologists), self-care activities, and complementary therapies.
Theme 5: Support Is Vital
Having a support network was vital for nearly all of the women to help them manage and cope with their endometriosis. A few participants spoke about being vocal about their condition which helped them not only to debrief about the disease but also to connect with others who also have the condition. Online support groups through social media were pivotal for many of the participants, including endometriosis-specific groups as well as groups concerned with particular treatments (e.g., hormonal IUD groups). The groups provided information, support, and opportunities for women to share stories of their journey or learn from other’s stories. These groups were a source of experiential knowledge and information about different treatments, recommended health professionals, and tips and tricks for managing symptoms. It is also a space within which women could connect with others, which helped to alleviate feelings of isolation. It just makes you feel that you’re not alone and you know the whole world’s problems aren’t on your shoulders you can actually share them around because you’ve all gone through the same thing.
Two participants indicated they didn’t join online support groups as they perceived their symptoms to be “mild” in comparison to others or they didn’t think it would be helpful. Others reported negative experiences with joining support groups noting, “it’s just stories of trauma and all sorts of things that I’m not sure if that’s particularly healthy or it’s not particularly healthy for me.”
Participants indicated that their workplaces, family, and friends supported them with managing endometriosis. A few participants mentioned that their workplaces were supportive, demonstrated by colleague(s) with whom they could talk about their condition, who were understanding when they needed to take time off for surgery or because of the symptoms, who called to check on them when they had been unwell and offered amended hours or work practices to suit their circumstances. Family members often provided practical support by assisting with daily activities (e.g., showering, helping them get dressed, and preparing meals), providing suggestions to help manage the condition, inviting them to live with them on an ongoing basis, or offering them a place to stay while they recovered from procedures. They accompanied them to appointments, advocated on their behalf, and visited when they were in the hospital. Many of the participants highlighted how important it was for them to have family members who understand the physical and emotional impacts of the condition, and that having such support made it just that much easier to manage and cope with the condition: Yep, um, she [mum] takes me to specialists, um [for] all, basically all my appointments, she drives me too because I can’t drive at the moment. Um, just the emotional support when, when I’m in pain. You know, getting me a heat pack or rubbing my back, um, when I can’t wash my hair; as I said, she helps me in that way. Um yeah, it’s just that love from her and support, just makes it that little more bearable.
Friends provided participants with opportunities to debrief about the condition, as well as practical support when their symptoms “flared” (e.g., driving them to a hospital) and checking in on them when they were unwell. Participants who had partners reported that they were instrumental in providing support to manage endometriosis, providing understanding, and providing emotional and practical support. While participants generally discussed the supportive people in their lives, some did note that at times colleagues, partners, and friends were not always supportive due to a lack of understanding of the condition and the symptoms they were experiencing.
Discussion
This study explored the lived experiences of self-management among participants with endometriosis. The experience with self-management varied between people and was often influenced by symptomatology, their experiences, knowledge base, confidence, and the degree of control that they perceived they could exert over their symptoms/condition. The extent they engaged with self-management also varied over time and was influenced by the factors presented above.
There were consistencies in the accounts of self-management presented by the participants with endometriosis in this study and the 10 attributes of self-management proposed by Van de Velde et al. (2019). The participants’ accounts highlighted person-oriented attributes (Table 1, Van de Velde et al., 2019) such as taking an active role and responsibility for the care process (e.g., becoming active decision-makers, undertaking self-care tasks, and being proactive) and coping with adversity (e.g., taking ownership, control, feelings of self-efficacy, and self-care tasks). Person–environment-oriented attributes were also discussed such as being informed about the condition (becoming endo-literate), developing a partnership with healthcare providers (establishing a patient–provider partnership), and being open to support (support is vital). With reference to the summarizing attributes of Van de Velde et al. (2019) model, participants spoke of the development of personal skills such as problem solving, decision-making, and patient–provider partnerships. Discussions around self-management domains tended to focus predominantly on medical management (e.g., self-care tasks, “body awareness,” symptom management exercised through perceptions of control, and self-efficacy). To a lesser extent, role management was discussed in terms of needing to be proactive, planning, and altering behaviors. In contrast, emotional management was not typically discussed by participants and warrants further investigation given the substantial impact on both physical and mental quality of life (Nnoaham et al., 2011; O’Hara et al., 2021). Participants’ experiences are discussed with reference to the broader literature below.
In defining and discussing self-management, participants spoke of implementing self-care activities to manage the symptoms of endometriosis. The popular use of heat, rest, diet, and exercise is consistent with findings of other research on women with endometriosis (Armour et al., 2019; Ballweg, 2003). In their surveys, Armour et al. (2019) and Ballweg (2003) found that the reported efficacy of self-care activities varied, which suggests that the effectiveness of these activities may be specific to the individual or linked with different symptom profiles. In contrast, Mardon et al. (2023) in their systematic review reported no significant effect on endometriosis symptoms when diet supplements, diet modifications, yoga, and the use of pain medications (NSAIDS) were compared to placebo or hormonal therapies. This may indicate that there is a need to move beyond looking at individual self-care activities and examine self-management as a whole (Table 1) within this cohort.
Becoming knowledgeable about the health condition is a key attribute of self-management (Attribute 4) and is closely linked to decision-making skills (Attribute 9.2) (Van de Velde et al., 2019). If knowledge is limited, then self-management efforts are likely to be impeded as sufficient knowledge is required to make informed decisions about one’s care (Clark et al., 1991; Schulman-Green et al., 2016). Participants’ descriptions of their experience with acquiring information about the disease and its management suggest that there is a need for more patient education at the time of diagnosis and for ongoing management of the condition.
Being an active participant and taking responsibility for the care process are core aspects of self-management (Attributes 1 and 2; Van de Velde et al., 2019). However, the interviews indicated that there appears to be a learning curve associated with the disease as most participants tended to move from being passive recipients of care to being actively involved in the decision-making process. This finding is in line with Holman and Lorig’s (2004) assertion that individuals with a chronic disease are initially inexperienced at filling the role of “active participant” but need to learn how to be an effective participant, which requires the support of healthcare professionals and programs.
Participants demonstrated that they took action by being proactive and engaging in self-care tasks aspects associated with the medical management domain of self-management (Attribute 10.1). In the broader self-management literature, this domain is also associated with monitoring symptoms (Van de Velde et al., 2019). In contrast, participants in this study did not seem to formally monitor their symptoms; rather, they spoke of a “body awareness.” The concept of “body awareness” appears consistent with the term “body literacy”—credited to Laura Wershler—defined as a woman’s understanding of “how her health and wellness is connected to her menstrual cycle” (Justisse International 2005, p. 6). However, participants’ descriptions extend beyond this original concept of body literacy and incorporate an awareness of symptoms and an evaluation of treatments and self-care efforts on one’s health and well-being. Wershler suggests that body literacy enables a woman to engage in “meaningful discourse with care providers and be a full participant in decisions made about her health” (Justisse International, 2005), which is consistent with the findings of this study as participants reported symptoms and side effects to healthcare providers and were engaged in treatment decisions.
Perceptions about the ability to and utility of self-management appeared to be influenced by the extent to which participants felt confident to self-manage and that they had control over their condition. Perceived self-efficacy is a foundational concept in chronic disease management (Grey et al., 2015; Holman & Lorig, 2004; Schulman-Green et al., 2016) and has been the target of self-management interventions for chronic disease (Lorig et al., 2009). According to Bandura (1989, 2004), greater self-efficacy is associated with a greater commitment to achieving goals, with the belief that one can perform tasks to achieve these goals and confidence that one can overcome any challenges. Bandura’s theory suggests that supporting women to feel confident in managing their disease may lead to a greater sense of agency and positive health outcomes.
The participants’ perceptions of control over their illness and symptoms appear in line with the construct of internal–external health locus of control (Strudler Wallston & Wallston, 1978; Wallston et al., 1978). Locus of control in its simplest form refers to the degree to which an individual believes they have control over their health (Norman & Bennett, 1995). Health locus of control has also been studied in various chronic illnesses such as arthritis (Cross et al., 2006), diabetes (Trento et al., 2006), and chronic pain (Baker et al., 2008). Strickland (1978) reviewed the evidence on locus of control and health behaviors and found that those with an internal locus of control tended to seek information about their disease, assume responsibility for their health, and take action to improve their health. Participants’ experiences in this study suggest that their engagement with different treatment approaches and self-care behaviors, improving their knowledge about the disease and how they related to health professionals and ultimately how they experienced the disease, may, in part, be related to their perceptions of control over their health.
Seeking support was integral to a participant’s journey with endometriosis, whether that support was finding a healthcare professional they could work with or finding support through family, friends, colleagues, or online communities. Seeking support through healthcare providers and having an openness to social support is consistent with self-management attributes 6 and 7 (Table 1—Van de Velde et al., 2019). Holman and Lorig (2004) also contend that the formation of a positive patient–provider partnership is necessary for the effective management of chronic diseases and is associated with improved patient health outcomes (Kaplan et al., 1989). While most participants seemed to be able to find a source of support, some accounts highlighted negative experiences, including difficulty finding a healthcare practitioner they could work with, needing to try multiple providers, or difficulties with online support groups. The impact of having social support among people managing chronic conditions is mixed with a systematic review highlighting positive health outcomes (including improved clinical, emotional, and behavioral outcomes) (Strom & Egede, 2012), while other studies have highlighted negative impacts (including social isolation, anxiety, and deteriorating health) (Palant & Himmel, 2019).
Limitations
A strength of this study was the inclusion of women of diverse ages, from different geographic locations (e.g., major cities and rural and remote areas), and with varied experiences of endometriosis. However, despite taking measures to recruit women from culturally and linguistically diverse backgrounds, only a small minority of women who participated in this research speak a language other than English at home. Therefore, the experiences of culturally and linguistically diverse groups are limited and need to be further explored.
It is important to acknowledge that this study was exploratory in nature and cannot be generalized beyond the sample. Furthermore, the qualitative study design cannot explore important questions such as causal relationships (i.e., did self-management improve outcomes for people with endometriosis). This was never the intention for this study and is an opportunity for further research using a longitudinal quantitative approach to assess outcomes after engaging in self-management.
Implications for Research and Practice
While many of the attributes of self-management were discussed in this study, the emotional management domain warrants further investigation given that previous research indicates that quality of life is impacted among those that live with endometriosis (Nnoaham et al., 2011; O’Hara et al., 2021). Further research is required to translate the findings from this study and the broader chronic disease literature to develop tailored self-management interventions for people with endometriosis. This work can be guided by a review of general self-management programs and their applicability to this cohort. Further, the design and evaluation of these endometriosis-specific self-management programs could be guided by the Self-Management Analysis in Chronic Conditions (SMACC) checklist (Moreels et al., 2023) which was developed through a Delphi study and was based on Van de Velde et al.’s (2019) self-management conceptual analysis study.
To conclude, this research provides unique insight into the experiences of self-management among people with endometriosis. Participants described undertaking many of the components of self-management presented in the chronic disease literature, indicating a role for self-management among people with endometriosis. Interventions have been designed for other chronic conditions to improve self-management skills with results indicating some moderate improvements in self-efficacy, psychological health, and health behaviors (Brady et al., 2013). Given the results of this study, there may be potential to develop interventions to assist patients with endometriosis to develop self-management skills. Further research is needed to design and evaluate self-management interventions for this cohort.
Supplemental Material
Supplemental Material - Self-Management Among People Living With Endometriosis: A Qualitative Study
Supplemental Material for Self-Management Among People Living With Endometriosis: A Qualitative Study by Rebecca O’Hara and Louise Roufeil in Qualitative Health Research
Footnotes
Acknowledgments
This research was conducted as part of Rebecca O’Hara’s PhD which was conducted at Monash University and supervised by Prof. Jane Fisher, Dr Heather Rowe, and Adjunct Associate Professor Louise Roufeil.
Author Contributions
RO contributed to the conceptual design of the project, conducted the interviews, performed the analysis, and drafted and reviewed the manuscript. LR contributed to the conceptual design of the project, reviewed the analysis, and reviewed the manuscript. All authors approved the final version of the manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Rebecca O’Hara’s PhD was supported by an Australian Government Research Training Program Stipend.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.