
Abstract
Chronic illness can disrupt many aspects of life, including identity, social relationships, and anticipated life trajectories. Despite significant scholarship on chronic illness, we know less about the ways in which chronic illness impacts feelings of loneliness and how people with chronic illness deal with loneliness. Drawing on concepts of biographical disruption and liminality and data from walking and photo-elicitation interviews with 14 people, we aimed to explore how people with chronic illness experience loneliness in their everyday lives. Tracing how past and present illness experiences are implicated in the lived experience of loneliness and the strategies people use to manage loneliness, our findings illustrated that being caught in a liminal state where participants struggled to maintain and adapt to a new normality in life with chronic illness was a central thread woven throughout their experience of loneliness. Although participants drew on their personal agency and adopted strategies to account for, manage, and limit disruptions from chronic illness and loneliness, they found that their strategies were not completely effective or satisfactory. Chronic illness and loneliness continue to be largely considered as an individual’s problem, limiting opportunities for people with chronic illness who experience loneliness to seek support and social connection. Our research highlighted that chronic illness and loneliness need to be acknowledged as both a personal and collective problem, with multi-level responses that involve individuals, communities, and society.
Keywords
Introduction
Loneliness is a pressing and rapidly growing social challenge (Surkalim et al., 2022), defined as the negative emotional response to a discrepancy between a person’s desired and actual level of social relationships (Peplau & Perlman, 1982). As a subjective experience, it is often framed as an individual’s problem and even a personal failing (Hawkley, 2022). This over-endorsement of independence and individual responsibility is problematic because it contributes to the stigma of loneliness, limiting opportunities for people to seek support and social connection (Barreto et al., 2022). Interventions to address loneliness have tended to focus on equipping individuals with the skills to become more socially connected or cope with lonely feelings better. Such interventions have included social skills training, social cognitive training, and mindfulness (Cacioppo et al., 2015; Masi et al., 2011; Veronese et al., 2021). When used on their own, the effectiveness of these interventions is equivocal, in part because, it is claimed, they have insufficiently addressed the socio-structural factors that contribute to loneliness (e.g., disadvantage and discrimination) (Akhter-Khan & Au, 2020), and meso-level interventions focusing on creating opportunities for increased social connection and cohesion are required (e.g., increasing social interaction networks through community activities or social media (Barbosa Neves et al., 2019)).
Research shows that there is a relationship between loneliness and chronic ill-health. People with chronic illness are found to be more likely to experience loneliness compared to those without (Lim et al., 2023; Petitte et al., 2015). There is also growing evidence that the relationship between loneliness and chronic illness is cyclical, with loneliness reported to negatively impact health and well-being, and vice versa (see, e.g., Birken et al. (2023) and Shi et al. (2023)). There is, however, still relatively limited research on how living with chronic illness intersects with feelings of loneliness. Understanding how people with chronic illness make sense of loneliness in their daily lives is needed to inform effective responses that support this “at-risk” group. In this article, we draw on data from walking and photo-elicitation interviews to explore how people with chronic illness experience loneliness in their everyday lives. Specifically, drawing on concepts of biographical disruption and liminality, we trace how past and present illness experiences are implicated in the lived experience of loneliness and the strategies people use to manage loneliness.
Methodology: Understanding Loneliness and Chronic Illness
There is a considerable body of sociological literature on chronic illness and its impacts on social connectedness. Bury’s (1982) work on biographical disruption provides insights into how a diagnosis of chronic illness can markedly disrupt people’s way of being, their sense of self, their social roles and relationships, and their access to social and material resources. Similarly, Charmaz (1983) argued that the demands of chronic illness diminish social relationships and can erode valued self and social identities. Researchers have applied and developed Bury’s “biographical disruption” and Charmaz”s “loss of self” to examine how socially contextualized situations shape and are shaped by chronic illness. Relevant work includes (but is not limited to) studies showing that chronic illness contributes to the fluctuation, contraction, and straining of social connections when people need to navigate disrupted identities, life trajectories, and functionality (Morris & Sanders, 2018; Perry & Pescosolido, 2012; Potter, 2023). Other researchers have sought to understand how people diagnosed with chronic illness seek to adapt to and manage “chronically ill” identities and disrupted social resources, for example, Locock et al. (2009), Sanders et al. (2015), Sanderson et al. (2011), and Cluley et al. (2023). Disruptions to social relationships and identities associated with chronic illness are not always experienced as one-off adjustments. Instead, continual and changing problem solving is required to negotiate disruption and reestablish a sense of normality. Some people maintain (often taxing) social connections and roles linked with pre-illness identities, some attempt to construct new social connections and roles to align with post-illness identities, and others adopt a combination of both. However, generally such strategies are reported to be insufficient in satisfactorily adapting to the disruption they are trying to manage (Cluley et al., 2023; Trusson et al., 2016).
The fluid and relational conceptualization of the response to disruption aligns with the concept of liminality. Liminality occurs when individuals are suspended “betwixt and between”—an ambiguous, often transitory state of being neither here nor there, neither one thing nor the other (Turner et al., 1969). The notion of liminality illuminates the straddling of boundaries between illness and wellness (Brown et al., 2017), tensions between pre- and post-illness identities (Saunders et al., 2018), and the inability to return to “normal” (Trusson et al., 2016). Being stuck between pre- and post-illness identities and normalities is arguably a key underlying factor driving social disconnectedness and thus loneliness. Researchers have shown that people describe the experience of loneliness as liminal during major life changes where there is adjustment to altered social identities, roles, and relationships, such as becoming a parent (Nowland et al., 2023), transitioning to university (Rutherford & Pickup, 2015), retirement (Bischoff et al., 2021), and moving into residential care (Cook et al., 2021). However, there is a paucity of research using liminality to understand the interplay between chronic illness and loneliness.
Although the above-mentioned studies provide rich insights into the disruptive impact of chronic illness on a person’s social identity, social connectivity, and sense of place in the social world, as well as the strategies that people use to (re)establish social connection, there have been few studies that have specifically focused on loneliness and how those with chronic illness deal with feelings of loneliness.
Methods
In our study, we took a qualitative, descriptive, participant-led approach, well suited to examining the perspectives and worldviews of those most involved in a phenomenon (Bradshaw et al., 2017). Our approach was informed by the interpretivist and constructivist paradigm of qualitative research as we aimed to examine the various ways in which people experience and make sense of their social world (Creswell & Poth, 2016; Denzin & Lincoln, 2018). We drew on a combination of walking and photo-elicitation interviews to explore how people with chronic illness experience loneliness in their everyday lives. Our study was approved by the University of Sydney Human Research Ethics Committee (2021/909) and University of New South Wales Human Research Ethics Committee (HC200333). All participants provided written or verbal informed consent prior to their interview. We offered participants a gift card to thank and compensate them for their time.
Sampling and Recruitment
We recruited participants who were aged at least 18 years, were residing in Australia, were conversant in spoken English, had a diagnosis of chronic illness, and expressed that they felt lonely. We purposively sampled to include participants with diverse sociodemographic characteristics (e.g., age, relationship status, and living arrangements), from a range of geographic locations (e.g., metropolitan and regional), and who had been living with chronic illness for different lengths of time. Participant recruitment materials were distributed through not-for-profit organization newsletters, websites and mailing lists, medical centers, and health and community care professionals.
The sample consisted of 14 participants (11 women and three men) aged between 22 and 68 years. Eight participants lived with family and six lived alone. Ten participants resided in metropolitan areas, while four resided in a regional area. Participants had lived with one or more chronic illnesses for 5–40 years. Their chronic illnesses included human immunodeficiency virus, post-traumatic stress disorder, depression, anxiety disorder, bipolar disorder, arthritis, multiple sclerosis, sleep apnea, fibromyalgia, epilepsy, cancer, lupus, and irritable bowel syndrome.
Data Collection
Walking and photo-elicitation interviews were conducted between November 2020 and April 2022 to facilitate a participant-led approach to data collection. We recognized that some participants would not be able to participate in a walking interview due to their geographical location, the severity of their chronic illness, or COVID-19 lockdown restrictions. Therefore, we invited such participants to take part in a photo-elicitation interview.
Nine walking interviews were conducted in person at the participant’s preferred location, and they decided the walking route. The interviewer walked alongside the participant while interviewing them (Kinney, 2017). Participants were asked to point out aspects that were important to them and their sense of health, loneliness, and connection so that the interviewer could take a photograph of these. These aspects were used as prompts to facilitate the interview. Advantages of walking interviews include helping to reduce power imbalances, encouraging spontaneous conversation, and offering an opportunity to observe the participant’s everyday life (Bartlett et al., 2023; Kinney, 2017). Walking interviews have provided insights into how people engage with their social and physical environment (Carpiano, 2009), the connections between participants and their community (Kinney, 2021), and people’s relationships with others and their sense of loneliness (Butler & Derrett, 2014).
Five photo-elicitation interviews were conducted in person at a mutually convenient location or through online video conferencing. Participants were asked to provide photographs of aspects that were important to them and their sense of health, loneliness, and connection. These photographs were used as prompts to facilitate the interview. Photo-elicitation is the use of photographs within research interviews (Harper, 2002). This approach encourages a different kind of reflection on lived experiences and produces a different kind of information by evoking feelings, thoughts, memories, and information that traditional words-alone methodologies cannot (Cleland & MacLeod, 2021). Researchers have highlighted the value of photo-elicitation in revealing detailed and insightful accounts of experiences in a range of health contexts, for example, social isolation, quality of life, and meaning of life (Burton et al., 2017; Glaw et al., 2017; Oliffe et al., 2019).
An interview guide was used to guide discussion during the walking and photo-elicitation interviews and included open-ended questions and prompts about participants’ description of the aspects they pointed out or their photographs, the reasons they chose those aspects or photographs, and what they meant to their experience of chronic illness, loneliness, and social connectedness. Interviews were audio recorded with participants’ permission and then later transcribed using a professional transcription service. Transcripts were checked for accuracy and de-identified to protect participant anonymity. Participants were allocated pseudonyms to protect their confidentiality. Following each interview, the interviewer wrote detailed field notes for each participant to provide contextualizing information.
Data Analysis
NVivo was used to organize the data (Lumivero, 2017). Interview transcripts were read repeatedly and coded for recurrent ideas. Sections of text from the interview transcripts were examined alongside the relevant photographs. As photographs can have personal meanings and be interpreted subjectively in various ways, our analysis was grounded in the participants’ own explanations for their photographs. We examined how each photograph was described by the participant to explore why participants made visible certain places, activities, relationships, and items, providing an additional layer to their accounts. As such, we analyzed the participants’ photographs through their verbal explanations. Thematic analysis techniques (both inductive and deductive) were used to identify substantive and conceptual patterns in the data (Pope et al., 2006). Initial codes were further explored within the context of existing theories of illness experience to make sense of the patterns that emerged from the data and resulted in the three themes discussed below.
Reflexivity
Our research team consisted of a broad and diverse range of expertise, including qualitative methodologies, health sociology, social sciences, psychology, anthropology, pharmacy, and health sciences. All members of our research team were female. Interviews were conducted by two members who were experienced social scientists with expertise in qualitative research. Interview coding and initial thematic analysis were conducted by two members: a postdoctoral researcher with expertise in qualitative research and a health sciences honors student. As data collection and analysis progressed, the research team met monthly to refine the interview guide and discuss the themes identified. Our combined experience and expertise facilitated rich data collection and analysis through the use of probing techniques and close attention to emerging and recurrent themes and allowed us to develop a refined understanding of the interplay of chronic illness and loneliness, leading to insights about how people with chronic illness experience loneliness in their everyday lives.
Results
We found that participants were caught in a liminal state where they had lost the old normality from pre-illness life and were struggling to find a new normality in living a life with chronic illness. All participants drew on their personal agency and adopted strategies to account for, manage, and limit disruptions from their chronic illness and loneliness. However, they found that their strategies were not completely effective or satisfactory. Three themes emerged from the analysis: (1) tensions between old and new normalities, (2) relational disruption, and (3) improvising and making do. We use quotations from participants’ interview transcripts and photographs taken during walking interviews and provided by participants to illustrate these themes.
Theme 1: Tensions Between Old and New Normalities
Participants shared that the limiting and debilitating effects of chronic illness disrupted their life trajectories, forcing them to abandon their pre-illness identity and previous normality. They described how repeated or prolonged disruptions due to chronic illness contributed to the loss of established and familiar routines, identities, and social relationships. Being deprived of their former valued ways of being was a key factor to their sense of displacement in their social worlds and thus their experience of loneliness. They described how their attempts to relieve the tensions between their old and new normalities were often only partly effective or sometimes not effective at all.
Feelings of loneliness associated with nostalgia and longing for participants’ pre-illness life, and their struggles to transition across the “old” and “new” divide were captured in the following excerpts and photographs provided by Eloise, in her sixties and living with an autoimmune neurological condition causing debilitating chronic pain. Eloise provided juxtaposed photographs to highlight the contrast between her life before chronic illness and her new normality (Figures 1 and 2). Eloise’s condition disrupted her old normality by stopping her from riding her motorbike to freely meet other people, walking long distances to paint with her friends from art class, and travel overseas. Her inability to care for a large house and garden necessitated the sale of the family home (a home that had been in the family for generations). Eloise was a subject in the photographs of her pre-illness life (these photographs have not been included to protect participant confidentiality) but not in photographs of her life with chronic illness. The contrast between having other people available to take photographs of her and needing to take her own photographs further emphasized her sense of loss, displacement, and loneliness. Prior to learning to live with chronic pain I would ride my motorbike everywhere (Figure 1(a)). It gave me the freedom and opportunity to meet other people. I can no longer ride. I no longer meet up with friends. Life is lonely. Now I am trying to find that feeling again on an e-trike (Figure 1(b)). It’s not the same. However, it helps me get out of the house occasionally, but it doesn’t help find friends. I used to spend hours walking or riding to find the perfect place to relax, sketch and paint with my friends from art class (Figure 2(a)). However, I can no longer do this and I long to be there with them. However, I created a quiet place on my own and I depend on thousands of memories and family photos of our travels to paint now (Figure 2(b)). This brings me peace, but still very lonely, really lonely, but I’m trying. My passion was travelling the world with my family and taking photos. I am unable to do this now. I will have to learn to be creative in other ways. How do I ever accomplish anything again? How do I make my life worthwhile? How do I find meaning in life again when pain is controlling me and my life? This was our family home we build together 30 years ago. I could no longer manage the home or the property, so we made the difficult decision to sell and move to a small townhouse. Chronic pain is about loss and grief and loneliness and rejection. (a) Eloise’s photograph of her previous motorbike and (b) Eloise’s photograph of her current electric trike bike. (a) Eloise’s photograph of how she previously painted in nature with her friends from art class and (b) Eloise’s photograph of how she currently paints alone in her painting studio.
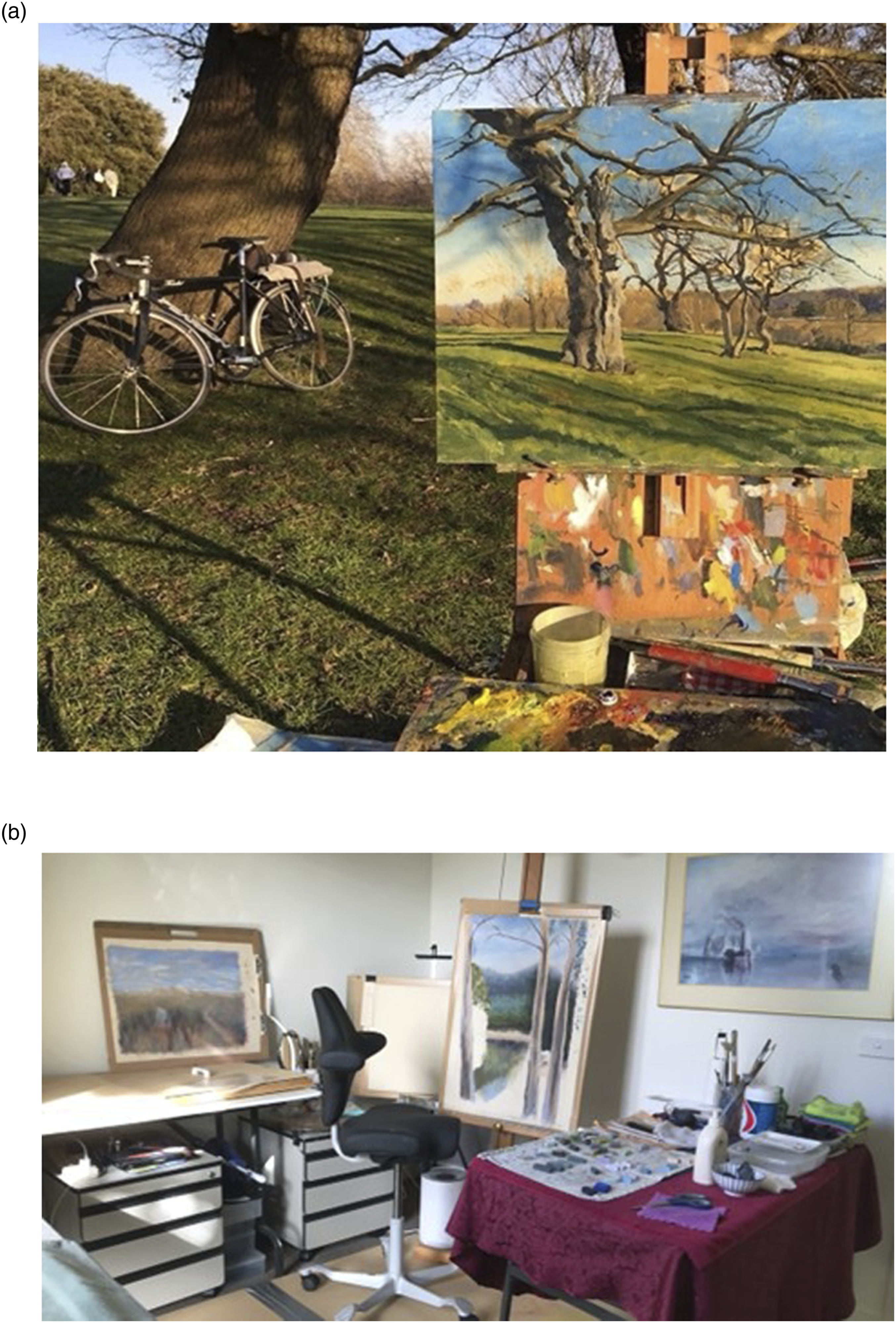
Eloise’s excerpts highlighted her attempts to recreate aspects of her old normality to manage her feelings of loneliness. She was partially successful in rescuing the satisfaction she associated with prior valued activities. The affordances of technology (her electric trike bike) enabled her to leave her house and gave her back some of the freedom that had been taken from her by chronic illness, but it did not help her find or reconnect with friends. Establishing a painting studio in her home enabled her to resume painting, but the experience was not the same when she cannot walk or cycle to paint in nature with other people. Now she draws on memories and past photographs as proxies for social interaction and painting inspiration. The absence of friends to share her new normality with meant that loneliness was ever-present and existing in the disconnect between her pre- and post-illness life.
Rosemary, in her sixties and living with a neurological condition, similarly shared a longing to return to her pre-illness life during her photo-elicitation interview. Her chronic illness disrupted her old normality physically by limiting her mobility and mentally by introducing uncertainty and anxiety about the future. Yet, unlike Eloise, who sought to find ways to adjust to her new normality, Rosemary’s excerpt highlighted the internal struggle she experienced: her desire to return to the familiarity of her former, pre-illness self and her resistance toward her current, chronically ill self. She also struggled to navigate her new normality without a vision of what this might look like. She described the loneliness that stems from her feeling of being stuck in the liminal space between old/past and new/present normalities. There’s a real grief process involved with when you lose capacity. And that goes right back to what we’re talking about, it’s the loneliness in that … Sometimes it’s almost impossible to find that new normal because one part of you is sort of saying, “Well, I just don’t want the new normal, I just want the old one, I just want to go back.” And maybe there’s that fight thing where you just want the old normal back, and you just can’t find what the new normal is … People like me are kind of still stuck in that with one foot in the other camp.
Theme 2: Relational Disruption
Participants also described the disruptive impact of chronic illness on interpersonal relationships and the strategies that they used to maintain social bonds with other people. Sustaining connections with friends and family members, while extremely important to participants, required them to hide parts of their chronically ill identities and present a pre-illness self and a socially desirable identity. However, presenting a socially acceptable identity and concealing the adverse physical, emotional, and social consequences of their chronic illnesses was a lonely experience. This loneliness was not only an outcome of the need to face the struggles of living with chronic ill-health on their own with little social support but also because hiding their lived reality left many participants feeling invalidated or misunderstood by others.
Laura, in her fifties and living with musculoskeletal and mental health conditions, described how her relationship with family members negatively impacted her sense of connectedness during her walking interview. Her excerpt below highlighted the feelings of disconnection which can arise through having relationships which are emotionally draining and invalidating. When she reached out for help, either people did not know how to react or they denied her request for support. I never be myself around my family. I can be myself a little bit, but no, they never really know what’s going on underneath. They never know, so I just put on this whatever … I spent my whole life being invalidated and not listened to, not believed by my whole family … You want to totally be able to be yourself, and I can’t be myself. There’s been times where I’ve reached out for help and then not got it because people don’t know how to respond or don’t know what to do. So I just keep it to myself. I just stay quiet. I just don’t tell people what’s going on … I think just when I tell people I’m not coping and then they just come back at you and go, “Don’t you have coping skills?” or, “Can’t you do this?” I’m like, “If I could remember what the coping skills were, do you think I’d be asking?” This is what a lot of them do to you now, “You’ve got the skills. You should know what to do.”
During her walking interview, Tina too, in her thirties with multiple physical and mental chronic conditions, explained that people around her did not acknowledge the ever-present nature of chronic illness and expected her “to just somehow get on with it or just get over it.” For Tina, loneliness is being given the message—directly or indirectly—to conceal her chronic illnesses, though when she does so, she is ironically dismissed as “not that sick”: I’ve had people say, “Are you still sick with that?” I’m like, “Yes, it’s a chronic illness, it’s never going away.” … You can’t win. You can’t win. If you show your disability, I’ve had people say, “No one wants to hear about your pain. It’s so boring.” Oh, I’ve had people say that. Like, “It’s tedious and you’re always going to have it, so we don’t want to hear it. Just hide it. No one wants to see it.” So I get told that and then I hide it and they go, “Well, you’re clearly not that sick, what do you want from me?”
The challenge of disclosing the personal struggles of living with chronic illness was also illustrated by Michella, in her fifties and living with an autoimmune condition. Her photographs showed that her main social connections were her work colleagues. While managing symptom flare-ups was a central part of her lived experience, she kept these struggles hidden from her work colleagues and shouldered lone responsibility for her chronic illness. As she explained, her secrecy was due to a fear that she would be socially ostracized or discriminated in the workplace (Figure 3). Concealment was part of her strategy to protect herself against social rejection and contributed to her feelings of loneliness. There’s a lot of anxiety attached to inviting somebody into your safe space, and people thinking, “Oh god, she wants something again.” I have a lot of trouble asking people for help or saying to people, “I’m not doing well” … That’s when my illness was flaring quite badly and very, very swollen feet, and that’s called vasculitis (Figure 3). But I never ever told anyone, the workplace. I always keep anything to do with my health very private and very secret because you worry about being discriminated against. Michella’s photograph of her chronic illness flare-up.
Furthermore, Michella shared a collage of photographs of rainbows to represent past moments of social connection and her current experience of loneliness. Her excerpt below demonstrated the struggle of losing social relationships and the critical importance of support networks and social bonds for participants. As Michella described, her memories of the past connection she felt with her work colleague highlighted the importance of past social relationships, but also amplified her present experience of loneliness: she describes it as a reminder of the loss of someone to share beautiful or “light” moments with (Figure 4). Rainbows. This is travelling back and forth from that old workplace. I used to carpool with another guy who became incredibly important to me, because you’re in a car for two hours a day so we would talk a lot. When he left, prior to that workplace closing down, I was devastated. I didn’t realise how much having somebody there for that concentrated period each day, I didn’t realise how much that meant for me. Rainbows, we used to, not chase them, but they were there, they were a prominent feature. It means lightness, they generally come out as the sun is coming out, so it just makes things lighter. But also, a lot of them [photographs] were taken when I was travelling on my own, and that represents loneliness as well. Michella’s collage of photographs she took of rainbows.
While these examples help us to understand the increased feelings of loneliness which can develop because of strained relationships when living with chronic illness, participants also talked about the people within their network that were important for feeling socially connected and supported. Participants valued having someone who could listen to their experiences, connections which helped them feel supported, and individuals who empathized with them and who showed them they cared. Most of these networks consisted of close friends and family members. The following quote from Betty’s photo-elicitation interview illustrated the importance of the support she received from her friend while living with long-term mental and physical health complications after being involved in a car accident: She supports me, not just professionally, but emotionally. She checks in, how am I doing, how’s life? And then we discuss the technical things and then she checks in again, “How are you with all of that?” It’s just I’m so blessed.
This quote shed light on how Betty, in her forties, appreciated that her friend could holistically support her; her friend simultaneously supported her practically with her career and emotionally through regularly checking in with her. Betty shared a photograph of the flowers and coloring book gifted by a friend she met through a volunteering initiative group after her car accident (Figure 5). The kindness her friend displayed provided her with a sense of connectedness. The gifts were significant for Betty as they reminded her that someone thought about her in times of difficulty. Betty’s photograph of the gifts she received from her friend after her car accident.
It was common for some participants to not only talk about close friends but also include acquaintances and people they had incidental contact with, highlighting the immense value they placed on the experiences created by these positive connections. Betty described how she both contributed to and received support from an online Facebook group during COVID-19 lockdown restrictions. She explained how sharing evidence-based self-care techniques on the group chats helped her encourage herself as well as others to engage in better health and well-being practices. Betty described the significance of her photograph of the online Facebook group as “Beautiful connections occur in the space as well, usually between me and my friends, sometimes between them” (Figure 6). Her experience also places emphasis on the importance of digital experiences and technology in increasing feelings of connectedness. Betty’s photograph of an online Facebook group that she contributed to and received support from.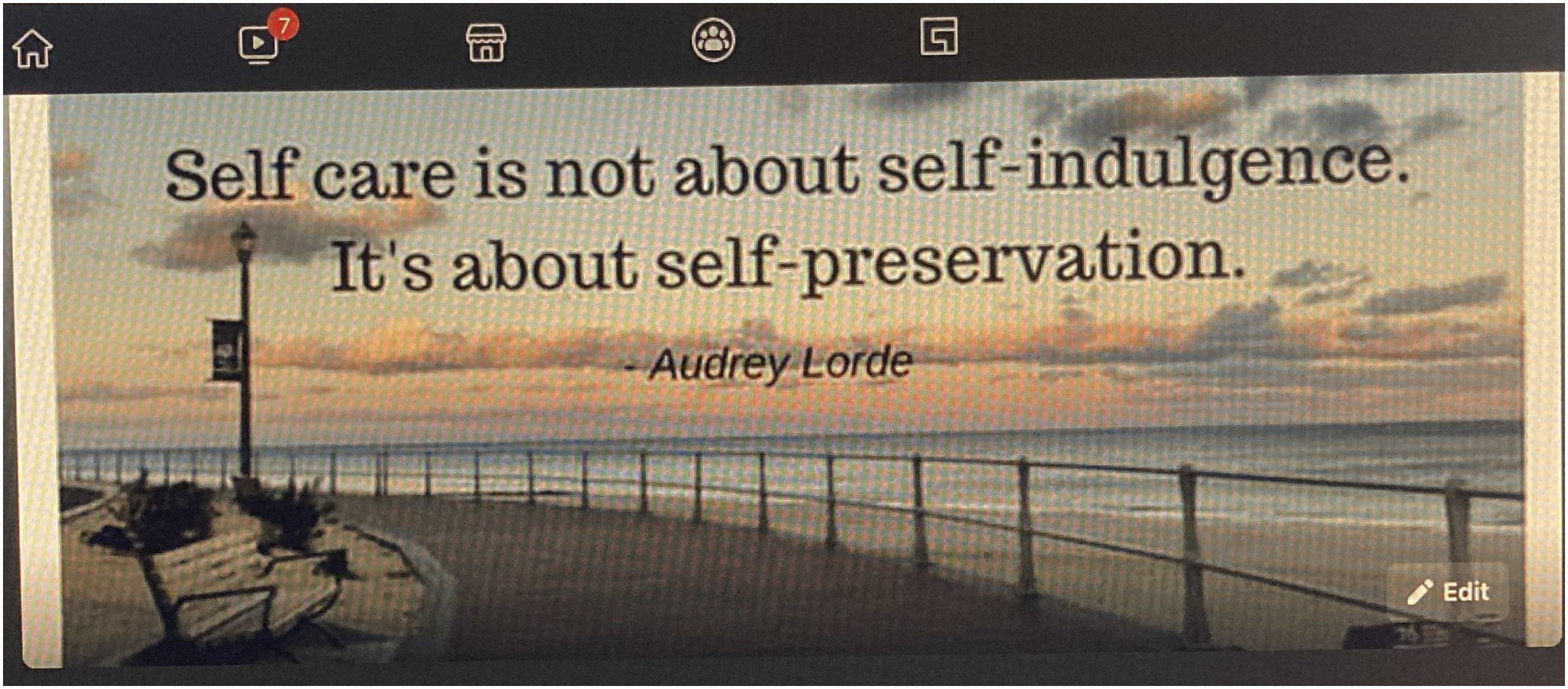
Similarly, Elisabeth, in her thirties and living with gastrointestinal conditions, talked about the importance of online community groups in tackling loneliness during her walking interview. She highlighted the value of online communities in overcoming geographical barriers and facilitating feelings of connectedness through shared experiences. Elisabeth explained that although she openly shared her feelings with her family and friends, communicating with people with similar experiences increased the depth of her conversations and her feelings of connectedness. On Instagram, there’s a whole bunch of people that have this community and all have their Instagram page and they share about chronic illness and stuff like that. And is that the community for me? Do I want to share about what’s going on with me? Do I just want to observe? Do I want to have people I can talk to? For me, where is that sweet spot? I think I’m still in that place of finding that, but I have started to explore more what that might look like for me, and I think that’s been really important … I think it’d be really nice to talk to somebody that has the same experience as I do, even though they’re slightly different.
Theme 3: Improvising and Making Do
In response to the inadequacy in participants’ desired level of social relationships and their ongoing search for a new normality in their life with chronic illness, participants shared different ways of staying “connected.” Some participants connected with themselves through solitary activities, some connected with acquaintances, while others connected with neighborhood spaces and places and nature.
What was striking and perhaps unsurprising from participants’ accounts was that managing loneliness often involved finding solitary activities. These included growing and caring for a lemon tree (Figure 7), writing song lyrics, writing a memoir, learning about the history of the buildings in the local neighborhood, and assembling flat pack furniture. During her walking interview in the local bushland, Jessica, in her sixties and living with an autoimmune neurological condition, explained that reading books provided her with a distraction from loneliness: I buried myself in a set of books by [name of author]. They were pure airport reading trash. But there were about five or six of them in a series about a family and I just read those and, I don’t know, snapped out of it. There was nothing really in there that made an impact on me, but I just enjoyed them so much. And I thought, “Well, you’re never lonely if you’ve got a good book” … Distracted myself with something that I enjoy doing, I think that’s probably the best way of putting it. Rosemary’s photograph of her lemon tree.
Participants also talked about the importance of neighborhood spaces and places in fostering connectedness and managing loneliness. As an example, Verna, in her sixties with an autoimmune neurological condition, described the significance of being part of a close-knit community and the sense of familiarity she has by being known to most people in her town (police officers, café owners, and other local community members): “It is my place and look, I love that. But also, I participate in that to make it happen.” Accentuating her own agency, she finds social interaction and manages loneliness by going to her local café and park (Figure 8). During her walking interview, several people greeted Verna and talked with her briefly. She explained that these micro connections, albeit with acquaintances, reinforced her sense of belonging by reminding her that she is known in the neighborhood. The importance of agency, intention, and effort was highlighted by Verna when she commented that people do not seek her out spontaneously: “You have to participate, you can’t expect it to happen to you.” Some days I feel like shit, but I make myself come out and drive around in my mobility scooter so that I actually see people, so that you don’t feel isolated … This community here and where I live and the people I know from all around here, it makes my life infinitely better … When people see you, a familiar face, again and again, even if you just nod to each other, it makes you feel part of something … See, I have lots of encounters like that, for which I am extremely grateful. Oh, I love it. I do belong to that. There is a community of that. But they wouldn’t search me out. Photograph of Verna’s local park taken during her walking interview.
Like Verna, Nick visited routine locations in his neighborhood’s spaces and places to feel connected. During his walking interview, Nick, in his fifties with a number of chronic illnesses, passed the local café, library, neighborhood center, main traffic intersection, garden, medical practice, supermarket, church, and hospital. Nick also exchanged greetings with a few people during his walking interview. He rhetorically questioned whether his micro connections with acquaintances were a temporary and superficial remedy to his feelings of loneliness. See, these little spots where I say hello to people along the way, is it a Band-Aid? Maybe, but it keeps me from feeling totally alone and totally isolated.
In the absence of social relationships, participants also talked about the importance of green spaces in fostering a sense of connectedness. A number of participants spoke about the value they placed on being outdoors in a natural environment, for example, the bush, greenery around the home, and the lake, as part of their strategy to manage loneliness. Ross, in his sixties with a musculoskeletal condition, described his life-long connectedness with the local beach during his walking interview (Figure 9). Whenever he felt lonely, he would visit this setting. I’ve grown up living on this beach and surfing on this beach … I’ve just got psychological connectedness with it … So, if I can’t come down here and walk along the beach and sit here, I drive past the point. Photograph of Ross’s local beach taken during his walking interview.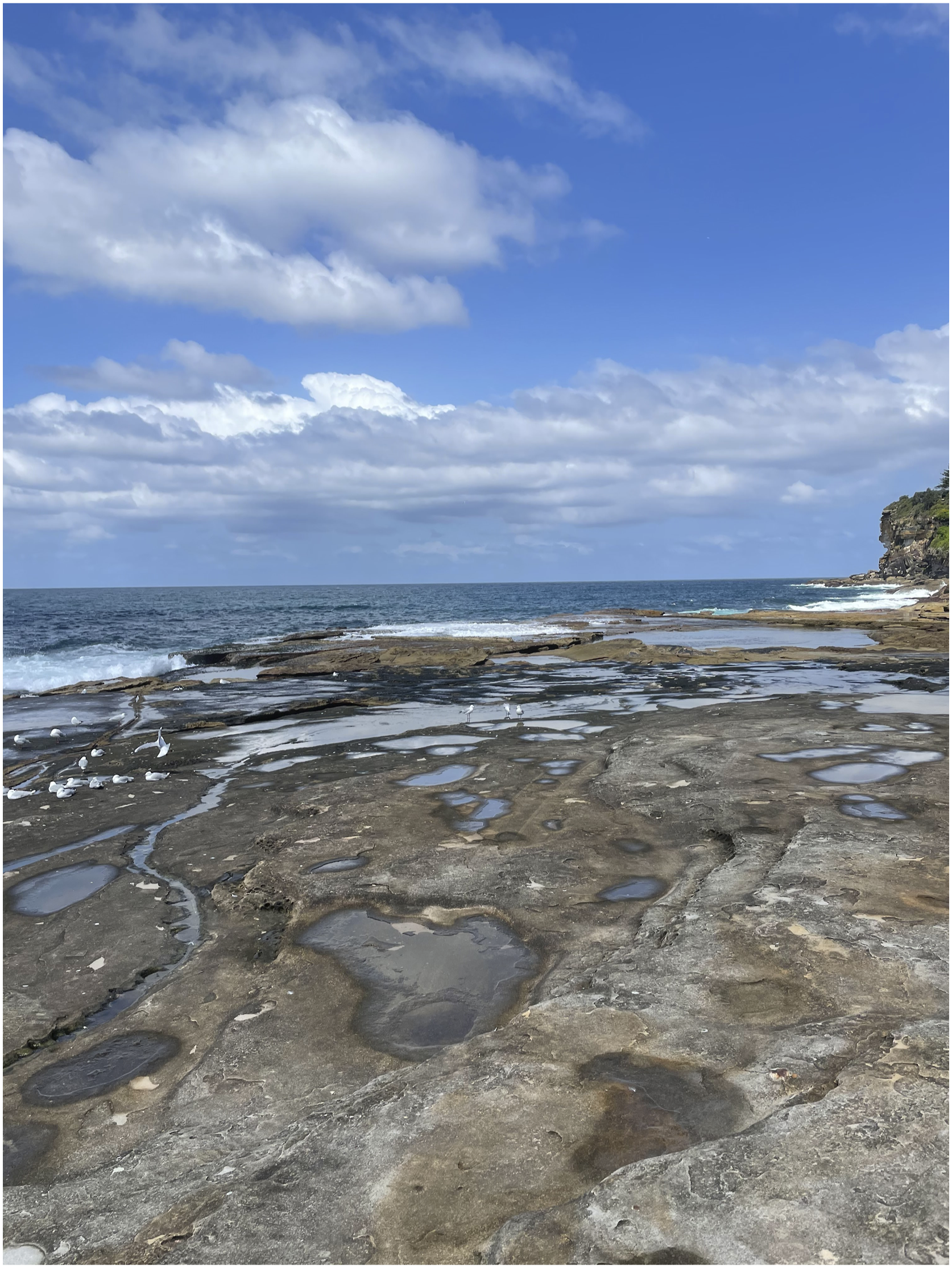
Discussion
Our research shows that while the concept of biographical disruption encompasses the search for a new normality, the liminality in how people with chronic illness experience loneliness is important. We revealed that the liminal struggle to maintain and adapt to a new normality in life with chronic illness was a central thread woven throughout the experience of loneliness for our participants. The loss of established and familiar routines, identities, and social relationships permeated their experiences. The upheaval of their old normality forced participants to abandon their former ways of being and knowing. In response, the participants drew on their personal agency to improvise and make do with the material and social resources available to them to manage some, but not all, of their feelings of loneliness.
This article builds on a body of work which highlights that being on the liminal threshold of the old and new can be a disconcerting experience for people with chronic illness (Blows et al., 2012; Bruce et al., 2014; Dauphin et al., 2020; Little et al., 2022; Strickland et al., 2017; Trusson et al., 2016). Our findings illuminate how biographical disruption, the struggle for normality, and the liminality of living with chronic illness contribute to feelings of loneliness. Our themes illustrate that living with chronic illness is a fluid, temporal, and dynamic journey where participants have departed from their old normality but have not arrived at a satisfactory new normality in their life with chronic illness—they were caught in a “neither here nor there” phase. Participants’ struggles to reestablish a new normality were prolonged as their strategies for coping with chronic illness and loneliness were only effective to a certain extent. Therefore, they appeared to be “stuck” en route to an ambiguous destination, potentially positioning them in a state of sustained liminality and loneliness. This experience resonates with sociological literature showing that liminal phases can be protracted over a lengthy period or even indefinite (Balmer et al., 2015; Brown et al., 2017; García-Santesmases & Sanmiquel-Molinero, 2022; Saunders et al., 2018). As such, participants were often not progressing through Sanderson et al.’s (2011) proposed process of normalization, and instead their accounts remained at the “disrupted normality” and “struggling for normality” taxonomies. We suggest that sustained liminality may be a common experience for people with chronic illness given their long-term nature and patterns of recurrence and deterioration, and a potential result is loneliness.
We call attention to how chronic illness and loneliness continue to be largely considered as an individual’s problem, with insufficient regard for the intersecting socio-structural and meso-level forces that contribute to loneliness. Similar to the findings from other, albeit few, published studies which have explored the experience of loneliness for people with chronic illness (Bay et al., 2020; Brighton et al., 2022; Molzahn et al., 2008), our participants’ accounts emphasized the relational aspects of their experience of loneliness—it involved others or the absence of others. Their singular efforts were not completely effective in moving them out of a liminal state of loneliness. Therefore, the management of loneliness is both a personal and collective endeavor. Our findings also echo Peacock et al.’s (2014) “no legitimate dependency” discourse in which almost everything about people’s lives is deemed to be the responsibility of the individual and the legitimacy of seeking support is denied. This discourse is stigmatizing; it can worsen the experience of loneliness and hinder people from reaching out for support and connection (Barreto et al., 2022). Chronic illness and loneliness need to be acknowledged as both a personal and collective problem, with multi-level responses that involve individuals, communities, and society.
In our study, photographs taken during participants’ walking interviews and provided by participants added a poignancy and “visibility” to the data and led to a more detailed understanding of the experience of loneliness while living with chronic illness. The photographs made visible and highlighted the invisibility of participants’ struggles for normality, capturing their creative strategies in response to disruption, and the elevated significance of solitary activities, micro connections, spaces, and places. We could see that participants often shouldered sole responsibility for their chronic illness and feelings of loneliness. Their photographs offered a window into the authentic, insider view of the interplay between chronic illness and loneliness. Such photographs can be used to engage individuals, communities, and society and promote dialogue regarding the experience of loneliness for people with chronic illness. Presenting patient narratives of their experiences to other people through visual methods, such as research-based drama (Dupuis et al., 2016), graphic novels (Czerwiec & Huang, 2017), and drawings (Cheung et al., 2019), has been useful in shifting perceptions, fostering insight, and stimulating critical reflection. Future work should explore the application and utility of photographs in bringing people closer to the lived experience of chronic illness and loneliness.
Our study was subject to methodological considerations. We interviewed participants who spanned most of the adult age range and lived with a variety of chronic illnesses for a range of years. Despite our efforts to invite people with diverse genders and from wider geographical locations, participants were predominately female and from metropolitan areas. Future research should seek to involve individuals with diverse genders and from wider geographical locations and culturally and linguistically diverse backgrounds. Additionally, we recognize that COVID-19 restrictions and precautions which were in place at the time of the interviews may have influenced participants’ perceptions and experiences of loneliness.
Conclusion
This article illuminates that our participants experienced a pervasive liminal state where they were displaced from the old normality from their life before chronic illness and struggled to find a new, satisfactory normality in their life with chronic illness. Drawing on the concepts of biographical disruption and liminality, we have examined how normality, relational disruption, and improvisation are implicated in participants’ lived experience of loneliness. The current societal discourse around chronic illness and loneliness favors independence and individual responsibility. This discourse, however, limits opportunities for people with chronic illness who experience loneliness to seek support and social connection. The management of loneliness is both a personal and collective endeavor, which needs multi-level responses that involve individuals, communities, and society.
Footnotes
Author Contributions
M.M.Y.C.: formal analysis, writing—original draft, and writing—review and editing. S.L.: conceptualization, funding acquisition, investigation, and writing—review and editing. R.R.: formal analysis and writing—original draft. K.W.: conceptualization, funding acquisition, and writing—review and editing. L.D.: conceptualization, funding acquisition, and writing—review and editing. A.R.: conceptualization, funding acquisition, and writing—review and editing. M.L.M.: investigation, and writing—review and editing. L.S.: conceptualization, funding acquisition, and writing—review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Australian Research Council (DP200101872) for funding this research.