
Abstract
There is a scarcity of qualitative research focusing on the implementation of infection prevention and control (IPC) guidance in low-income countries. This study aimed to address this gap by exploring the perspectives of healthcare workers (HCWs) regarding the implementation of IPC guidance at the healthcare facility level in Uganda. The study also sought to generate a theoretical understanding of the processes involved in implementing IPC guidance in these settings. This robust qualitative research employed a design based on constructivist grounded theory methodology, conducting individual interviews with 13 frontline health workers such as doctors, nurses, nurse interns, and laboratory staff. The key findings of the study revealed that HCWs undergo a process of ‘striving for improved practice’ in their efforts to implement IPC guidance. This process involved four phases: recognising the importance of IPC, playing a role, encountering challenges, and overcoming challenges. However, achieving full implementation proved difficult due to various individual and organisational barriers presented by the low-income setting. HCWs employed improvisation as a means to overcome these obstacles. Additionally, the study identified enabling factors that facilitated the implementation of IPC guidance within these settings. This study is significant as it applies robust qualitative research methods to provide valuable evidence of HCWs’ perspectives on an important topic in an under-researched context, with findings transferable to similar settings.
Keywords
Introduction and Background
Healthcare-associated infections (HAIs) are infections that occur during the course of receiving healthcare, typically within 48 hours of hospital admission (WHO, 2018). These also include infections that manifest after discharge and those acquired by HCWs due to their occupation exposure (Monegro et al., 2021). In the United States, approximately 3.2% of hospital patients are estimated to have at least one HAI on any given day, while in Europe, the estimated prevalence is 6.7% (CDC, 2018; ECDC, 2016). In low-income countries, the estimated prevalence is higher and ranges from 5% to 19% (The World Health Organization [WHO], 2015). Although limited data is available for low- and middle-income countries, a systematic review and meta-analysis focusing on Southeast Asia revealed a pooled prevalence of 9% based on 41 studies (Ling et al., 2015). While in Ethiopia, a meta-analysis by Alemu et al. (2020) reported a pooled prevalence of 16.96% for HAI burden nationwide. These figures indicate a higher burden of HAIs in comparison to the United States and Europe, highlighting the disproportionate impact in low-income countries. HAIs often lead to significant patient morbidity, mortality, prolonged hospital stays, and additional costs for diagnostic and therapeutic interventions, which are incurred in addition to the patient’s underlying disease (CDC, 2018; WHO, 2018).
Additionally, these infections contribute to an increase in antimicrobial resistance (AMR) further exacerbated by the use of antibiotics for HAIs. A comprehensive analysis by Henriksen et al. (2019) revealed a strong association between the prevalence of Acinetobacter spp. and resistance rates against third-generation Enterobacteriaceae. The rise in AMR poses a significant challenge to the effectiveness of antibiotics, compounded by the emergence of resistant strains of pathogens. Therefore, it is crucial to develop effective infection control interventions that can prevent the further development and spread of multidrug-resistant organisms, reduce patient mortality, and mitigate the financial burden on patients and healthcare services. Implementing robust IPC practices, including the prevention of HAIs, is one such strategy that can address these concerns.
It is estimated that up to a third of HAIs could be prevented by implementing essential infection control measures (WHO, 2016). These measures include effective hand hygiene, IPC practices such as safe management of care equipment and environment, management of blood and body fluid spillages and waste management, proper diagnostics, and appropriate antibiotic use (WHO, 2016). However, there is considerable variability in the implementation of IPC programmes across countries and hospitals, leading to inconsistent patient protection against HAIs (Hale et al., 2015). To address this, guidelines such as the Core Infection Prevention and Control Practices and the WHO IPC core components have been published to minimise variability (CDC, 2015; WHO, 2016). Despite these efforts, challenges remain in raising awareness and effectively implementing IPC guidelines, resulting in rising HAI rates and multidrug-resistant organisms (Wushouer et al., 2017). Given the growing reliance on IPC guidelines for patient safety, research on their use in practice is crucial.
A systematic literature review (unpublished) was conducted to inform this study, focusing on the evidence available up to March 2018. The main aim was to identify existing research related to the implementation of international IPC guidance and the methodologies employed in such studies. This review demonstrated a dearth of qualitative research on the implementation of IPC guidance at the health facility level in low-income countries, highlighting the need to gain a deeper understanding of IPC guidance implementation in low-income countries through qualitative methods.
To fill this knowledge gap, this paper presents the findings of a qualitative study that sought to explore HCWs’ perspectives on the implementation of IPC guidance at the health facility level in Uganda, a low-income country. The study also aimed to generate a theoretical explanation for the processes involved.
Methods
This study employed a qualitative research design based on the constructivist grounded theory research methodology (Charmaz, 2014). This approach brings attention to the role of subjectivity and proposes that researchers and participants play an active role in shaping the realities in which they participate. Constructivist grounded theorists aim to achieve a conceptual understanding of the phenomena they investigate, taking into account the temporal, spatial, and contextual dimensions of the research (Charmaz, 2014). As a result, the findings of the study are, at all times, provisional and specific to the contexts in which they are developed. Constructivist grounded theory was chosen for this study as it aims to develop a detailed “understanding of the underlying social processes within a certain context” (Charmaz, 2014, p. 13). Context is paramount for understanding the implementation of IPC guidelines as contextual cues can promote certain behaviours and subsequently foster or hinder implementation interventions (Nilsen, 2015). Using a constructivist grounded theory approach allowed the researcher to focus on the underlying social processes that might affect the implementation of IPC guidance in the Ugandan context. These processes were not immediately apparent but emerged over time as the data were analysed and theorised (Charmaz, 2006). Additionally, by applying a theoretical coding process during analysis, constructivist grounded theory provided a rich theoretical understanding of the realities of IPC guideline implementation as perceived by healthcare professionals in Uganda. In accordance with this approach, a decision was made not to apply pre-determined theoretical perspectives but to allow a theoretical explanation to emerge.
Ethical Considerations
Information about the study was shared with potential participants through a participant information sheet, and written consent was obtained from those who willingly chose to take part. To protect participant anonymity, names were removed from the transcripts, and pseudonyms were used when reporting the findings. Confidentiality measures were implemented by clarifying to each participant, at the commencement of every interview, that only the researcher and supervisory team would have access to the interview recordings and transcripts. Ethical approval for the study was granted by the appropriate ethical committees in both the United Kingdom (HLS/NCH/18/031) and Uganda (MRRH-REC IN-COM 047/2019).
Participants and Data Collection
The study was conducted at a government-funded tertiary hospital with 450 beds, situated approximately 250 km from the capital city. This hospital serves a population of around 4.6 million people across six districts and boasts a variety of specialised departments, such as surgery, obstetrics and gynaecology, outpatient and community health, internal medicine, diagnostics, and paediatrics.
The data collection process involved face-to-face individual interviews with 13 frontline healthcare workers actively involved in implementing infection prevention and control (IPC) guidance at the facility. This diverse group included a senior infection control nurse (n = 1), doctors (n = 2), staff nurses (n = 3), student nurses and interns (n = 2), a laboratory technician (n = 1), IPC committee members (n = 3), and a midwife (n = 1). The interviews took place between October 2019 and November 2019.
A semi-structured broad interview guide (Appendix I) was utilised flexibly. While not exhaustive, the guide covered general issues related to understanding the meaning of IPC guidance, decision-making processes, and the factors influencing these decisions.
In order to determine the initial sample, purposeful sampling was employed, allowing for the identification and selection of individuals who possessed abundant and relevant information pertaining to the implementation of IPC guidelines in practice (Patton, 2014). The researcher closely examined the organisational structures and responsibilities of staff members involved in IPC within healthcare facilities in Uganda, and it was decided to conduct interviews with as many individuals serving on the hospital IPC committee as feasible, given their expertise and familiarity with the research domain.
After the initial interviews, the approach shifted from purposive sampling to theoretical sampling, which directed the researcher towards specific areas for further data collection, as guided by the constructivist grounded theory methodology (Charmaz, 2014) (Appendix II). The researcher followed the principles of Glaser and Strauss (1967), asking questions such as ‘Which group of potential participants should be included in the next phase of data collection, and for what theoretical purpose?’. For instance, upon initial analysis, it became evident that the implementation of IPC guidance involved various individuals beyond senior nurses. Subsequently, the next stage of theoretical sampling aimed to gather insights and perspectives on IPC implementation from other staff members, including staff nurses and junior clinical care providers.
At the beginning of each interview, participants were provided with an assurance of confidentiality and the choice to refrain from answering any specific question or to conclude the interview at any time if they wished. The interviews varied in duration from 15 min to 1 hour, and they were digitally recorded and transcribed in full by the researcher. Throughout the interviews, emphasis was placed on avoiding any imposition of limitations on the participants and, instead, allowing them the necessary time to freely express themselves. As a result, the researcher’s involvement was restricted to asking open questions, actively listening, and seeking clarification when necessary. The questions were designed to be non-directive and focused on general issues that covered understanding the meaning of IPC guidance, decision-making, and factors influencing these decisions, aligning with the primary objective of the study, which was to gather insights into the interviewees’ perspectives. In this way, and in line with the constructivist method (Charmaz, 2014), data was co-constructed between the researcher and the participant during the conversational interview. The initial questions served as broad guidelines, subject to modifications following the methodology’s theoretical sampling procedures (Charmaz, 2014). As the analysis progressed and concepts and categories emerged, the questions became more focused. Additional questions, such as ‘How does your experience impact adherence to IPC guidelines?’, ‘What are the sources of the guidelines?’, ‘How does hospital management support influence your decisions?’, and ‘How does external organisational support impact IPC guidance implementation?’, were incorporated. Throughout the analysis, memos were written immediately after each interview and during the process, facilitating reflection and contributing to theoretical development, while also maintaining an audit trail.
Data Analysis
Analysis was conducted by one researcher and discussed with study supervisors to enhance rigour. The analysis was initially conducted inductively, without any pre-determined theoretical perspective, in order to let the concerns of participants emerge; however, later Glaser’s theoretical codes were used to conceptualise the relationships between the emerging sub-categories. The analysis began after the first interview and continued concurrently with data collection (Charmaz, 2014). In the initial coding stage, transcripts were read line by line, sentence by sentence, or paragraph by paragraph to make sense of the data and facilitate the emergence of preliminary codes (Appendix III). The preliminary codes were re-visited when each subsequent transcript was coded. Focused coding was used to move across interviews and compare participants’ experiences, actions, and interpretations. This process determined the adequacy of the earlier codes, and some codes were subsequently renamed to improve their fit. However, in the early stages of analysis, grouping codes together was avoided in an effort not to force any interpretation of meaning too early. Similarities and differences between codes were identified, and finally codes were condensed into categories with sub-categories (Appendix IV). By going back and forth comparing data, these were revised as evidenced in the analytical memo in Appendix IV. Making decisions was revised to ‘recognising the importance of IPC’, manoeuvring was revised to ‘overcoming challenges’, and facilitating was turned into a new category, ‘enabling conditions’ while a new category, ‘encountering challenges’, was created. Categories were conceptualised through theoretical coding, an advanced level of coding that builds upon codes selected during focused coding and establishes connections between them using a theoretical model developed to illustrate the process (Figures 1 and 2). Findings were exemplified by quotes from participants. This entire process was done using NVivo 12 to organise, sort, and store the data, while mind maps, diagram sketches, and sticky notes were used to assist in visual conceptualisation. Illustrations of the various stages in this process are provided in Appendices II, III, and IV, demonstrating how an auditable trail of analytical decision-making was used to enhance rigour in analysis (Baillie, 2015). Asymptote of IPC implementation. Basic social process of striving.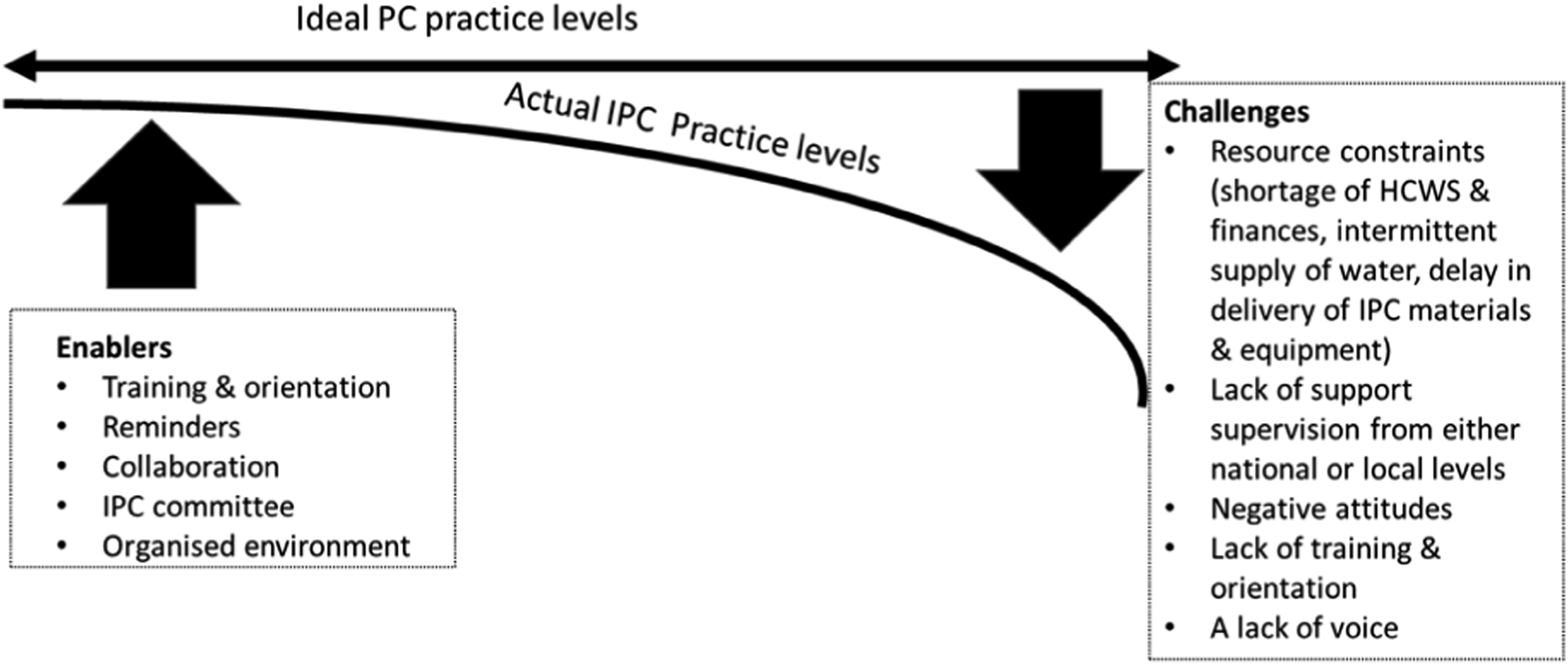
Findings
‘Striving for Improved Infection Prevention and Control Practice’
There are always challenges or complexities in these contexts, such that an ideal state of full IPC implementation is never achieved in reality. This constant striving but not quite getting there describes the concept or theoretical code of ‘asymptote’. This theoretical code illuminates a key point: the ‘ideal state’, or its construction, is not attainable by anybody. In this study, the ideal state was the required level of IPC practices for fully implemented IPC guidance.
However, this ideal state of IPC practices operates akin to asymptotes. In this context, the curving trajectories of IPC practices and the ideal state converge but never actually intersect (Gipson, 2006). As illustrated in Figure 1, enabling conditions and strategies from healthcare workers (HCWs) push IPC practices towards the ideal levels. However, challenges pull IPC levels away from the ideal levels, meaning these two never meet, as in an asymptote.
The basic process through which this is achieved is ‘striving’. This explains the continuous struggles in trying to implement IPC guidance by HCWs in these contexts. Therefore, this grounded theory speaks to the primary challenges HCWs faced in trying to achieve ideal IPC implementation in Uganda and how these challenges were overcome. It explains the patterns of meaning and actions that reflect participants’ experiences and elucidates the central social process in the Ugandan healthcare setting that HCWs go through to mitigate challenges faced when implementing this guidance.
The participants’ primary concern revolved around the implementation of IPC guidance amidst numerous challenges. While HCWs acknowledged the significance and necessity of IPC, they encountered obstacles in fully incorporating the guidelines into their daily practice due to various factors. These challenges included limited resources, a shortage of healthcare workers, inadequate funding, intermittent water supply, delays in the delivery of IPC materials and equipment, lack of support supervision at both national and local levels, a lack of representation and voice, negative attitudes among HCWs, and insufficient training and orientation.
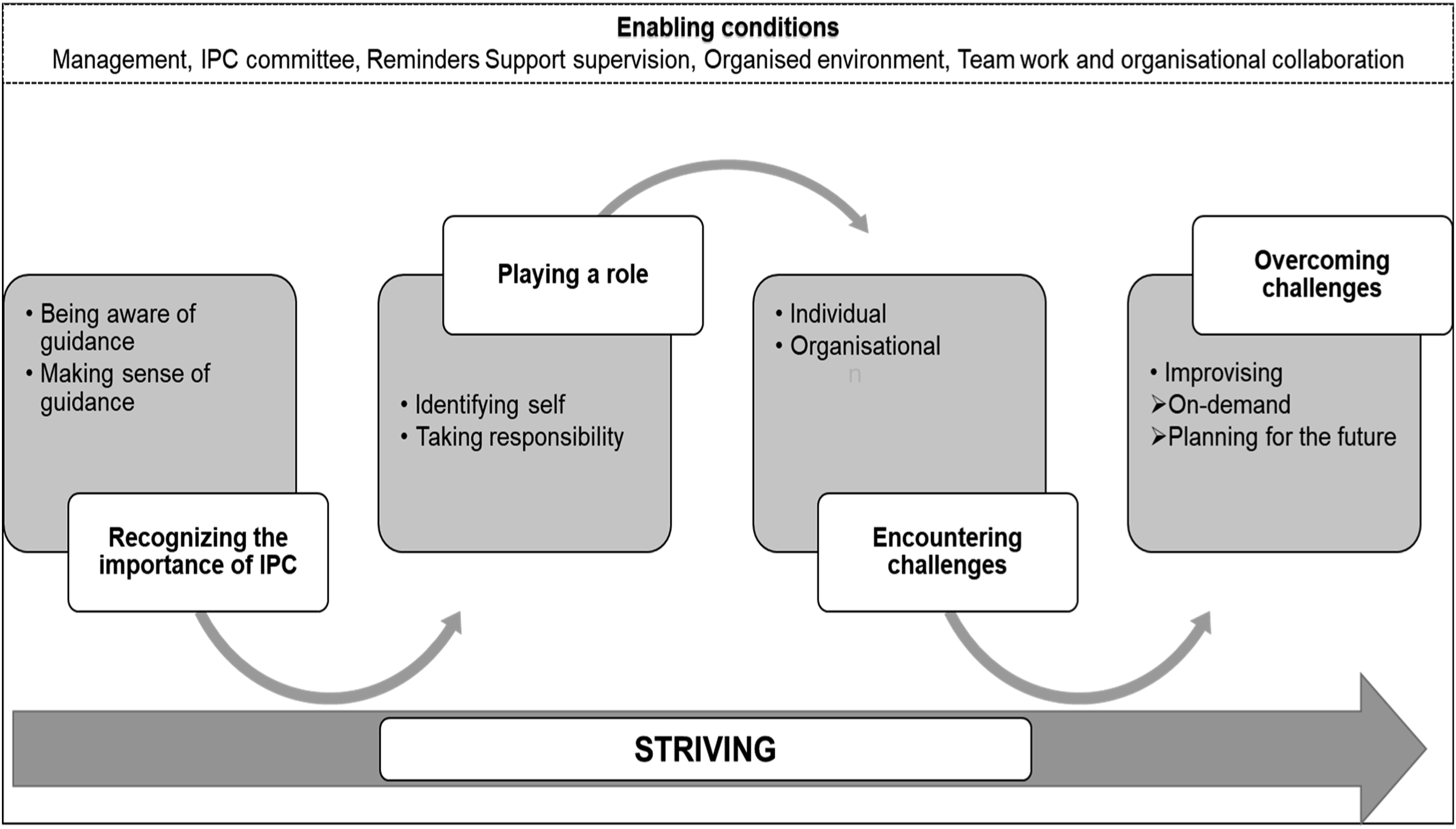
In order to address the impact of these challenges on IPC practices, HCWs engaged in a process of ‘striving’ (as depicted in Figure 2) as they attempted to implement IPC guidance and enhance healthcare safety within a resource-limited context. This concept of striving encapsulates the fundamental social process involved, with key categories describing the distinct phases of this process. These phases include recognising the importance of IPC, playing a role, encountering challenges, and overcoming those challenges (as shown in Figure 2). Each of these main categories is associated with several concepts, which can be sub-categories or theoretical properties within the category. These sub-categories or properties highlight the contextual factors and social interactions that influence the implementation of IPC guidance. It is important to note that while these phases or stages are presented in a linear manner, they do not necessarily occur sequentially. They represent interconnected facets of the broader struggle for achieving ideal IPC practices within a healthcare facility operating in a low-resource setting. The subsequent section provides a detailed presentation of each main category, using anonymised participant codes for identification purposes.
Recognising the Importance of IPC
The findings within this category elucidate participants’ perspectives on the benefits of IPC and how these perspectives influenced their motivation to integrate IPC guidelines into their daily responsibilities. A crucial prerequisite for implementing IPC guidance was the participants’ recognition of its significance. This recognition was fostered through various means, including training sessions such as continuous medical education (CME), and information disseminated by external organisations like the World Health Organization, Infectious Diseases Institute (IDI), and government sources. Participants acknowledged the importance of IPC in safeguarding both themselves and their patients from infections, as reflected in the following participant quotes: ... infection control is key because I may be having my infection, and I don’t have to transfer it to the patient. (Participant 11, Nursing Officer) To me, IPC means a patient should come to hospital, be treated for what they come and not get any other infection from the hospital and likewise, we, the health workers, shouldn’t be picking infections from the hospital or from the patient. (Participant 10, Nurse Intern)
Playing a Role
Once HCWs recognised the importance of IPC in safeguarding themselves and their patients from infections, they became more motivated to implement IPC guidance. This implementation process involved participants taking on distinct roles based on their professional identities, such as being a doctor, an in-charge nurse, an IPC member, or a student intern. These role identities influenced how participants assumed responsibility throughout the process. For instance, the nurse in charge of the wards felt an additional sense of responsibility in ensuring the safety of both patients and staff. One participant likened their role to that of a mother, underscoring their commitment to keeping everyone under their care safe from infections. I am like the mother, the housemaid of the home. Hmm, I guard them. I guard the community against the infections, I guard the students against infections to them, and then I protect the patients, I prevent nosocomial infections from the students to the patients and attendants and also the community which we look after. (Participant 3, Nurse in Charge)
Doctors felt that in executing their roles, they had a particular function of advocating for IPC. The role of the doctor, for example, me, I keep reminding myself and others the benefits of infection control and prevention. (Participant 4, Doctor/Medical Officer)
Additionally, nursing officers or staff nurses felt that they were responsible for supervising students or student interns, as the following quote illustrates. When the students come, they don’t know, they can mix up things unless you take [supervise] that student step by step that’s when you will ensure they do the right thing, but very few are interested. You have to follow their every step, for example, if they are doing this and that you have to follow them and even [show them] where and how to dispose wastes whether it’s in highly infectious bin or non-infectious bins. (Participant 13, Midwife)
Encountering Challenges
As healthcare workers assumed various roles, they faced challenges specific to their context within a Ugandan tertiary hospital. These barriers were conceptualised within a typology of either individual challenges, such as negative attitudes by some staff, or organisational-level challenges such as resource constraints (shortage of HCWs and finances, intermittent supply of water, infrastructural challenges, and delay in delivery of IPC supplies), lack of training and orientation, lack of support supervision from either the national or local levels, and lack of a voice for staff to make suggestions. These are illustrated by the quotes below: Then another challenge is also having no resources, as I said. We don’t really get enough resources, materials especially because of financial resources, the finances are not enough, so we are constrained there. (Participant 1, Nurse in Charge) For example … recently we had no running water in the maternity ward, how will we then make sure that people (HCWs) wash their hands after touching patients, after palpating mothers. (Participant 13, Midwife) What I am trying to [say] is there is no funding. There are no funds allocated for IPC activities. (Participant 6, Lab Technologist)
Enabling Conditions
Within the same context, there were enabling conditions that facilitated the implementation process, for example, management support, the presence of an IPC committee, having visual reminders, having support supervision, having CMEs, an organised environment, teamwork, and cross-organisational collaboration. For example, participants frequently discussed management as having an impact on the success of IPC implementation, especially because they were responsible for overall planning for hospital requirements; the following quotes illustrate: We try to maintain a good relationship with the hospital management. We have regular meetings and discuss together what we need. When it comes to administration [Management], there are the ones that drive this entity, so if I am lacking this, like I have mentioned water, there is no way I can look for water, so they come up as the administration, they know how they talk to the police to see to it that water is delivered, that’s how administration comes in and when we talk of this waste, …. they make sure that they contract someone to carry away that waste to someplace. (Participant 7, Nurse in Charge)
In addition to the good relationship and the support from management, participants felt that an effective IPC governance structure was also critical to successful IPC implementation. Participants placed great value on having an IPC committee. They felt that an IPC committee offered direction, made decisions, conducted audits of IPC in the hospital, and made sure all the IPC supplies were available by making requests to management, as highlighted in the quote below. They [the IPC committee] request materials on our behalf like detergents which we use in disinfection. They decide on what we use and what’s purchased in the hospital. (Participant 7, Nurse in Charge) The committee is basically an overseer of safety practices in the lab and in the hospital and also overseeing the planning, budgeting and then also makes sure that people are implementing what you want them to do. (Participant 6, Lab Technologist)
Having reminders acted as an enabling condition for implementation as it served as an effective memory jogger for people who might otherwise forget, as this participant revealed: Being a human being, we really need to be reminded on what we are supposed to do, much as we know we can be busy and forget to implement or do it the way it supposed to be done. (Participant 8, Nursing Officer)
In addition to having reminders, most participants referred to the benefits of having support supervision as part of their working practices. The benefits that participants recounted as a result of this supervision provided an opportunity to fill in gaps in information, particularly regarding IPC guidance. We have supervisors in the hospital who keep moving around, help us solve problems and also encourage us to improve on infection control. (Participant 13, Midwife)
Overcoming Challenges
Due to the presence of various obstacles, accompanied by certain facilitating conditions, HCWs were compelled to devise strategies to overcome these challenges. These strategies manifested in the form of improvisation, either in response to immediate needs (on-demand improvisation) or as part of future planning (planning for the future improvisation). On-demand improvisation occurred spontaneously when individuals encountered pressing situations that required them to find timely solutions to overcome obstacles. For instance, the shortage of consistent water supply was addressed by providing alcohol-based hand rub (ABHR) to specific areas or departments that experienced water scarcity issues or high patient volumes. Some HCWs took it upon themselves to purchase their own ABHR to mitigate this problem. Additionally, mobile water trolleys were used to ensure the availability of water for proper hand hygiene during such circumstances as exemplified in the following quote. I mean at times when we have no running water, so they brought this alcohol hand rub and usually some water in trolleys in some areas. (Participant 7, Nurse in Charge)
However, if there was a shortage of ABHR, this was prepared locally at the hospital. In the following excerpt, a participant highlights how they used the technique of preparing alcohol locally at the health facility to overcome the challenge of a shortage of ABHR. ... and when it’s not there [ABHR], or when the government has not supplied us, then our hospital prepares it locally. And this locally made alcohol hand rub was approved by IDI, because it’s them that trained us. (Participant 2, Infection Control Nurse)
Furthermore, although not an ideal resolution, participants had to resort to asking patients for assistance during periods of scarcity. Patients or their families were often requested to procure their own essential IPC materials, as captured in the following quote: You tell the patient or their relatives to buy since you don’t have gloves and you want to help somebody. (Participant 11, Nursing Officer) … so I would run around either to borrow something to use or to look around or to send a patient to go and buy for themselves. (Participant 8, Nursing Officer)
Planning for the future involved anticipating future challenges and devising proactive solutions prior to their occurrence. This involved recognising the inevitability of resource demands and shortages in these contexts, prompting senior leadership, particularly IPC committee members, to adopt a strategy known as ‘planning for a rainy day’. For instance, these participants frequently stocked up on IPC supplies during periods of abundance. These stockpiles served as a buffer during times of scarcity and shortages, as illustrated in the following quote. We have our small office for IPC where we keep at least some things for an emergency like detergents and gloves. (Participant 5, Nurse in Charge)
Further, although the health facility provided an opportunity to train students as part of a broader collaboration between the hospital and the schools, by having students, the hospital filled gaps arising from a shortage of HCWs. As the following quote illustrates, these students played a significant role in ensuring the implementation of IPC measures and delivering care. Although they [students] are here to practice and to learn the hands-on practice, they also help us cover in some cases when the nurse is so busy. (Participant 11, Nursing Officer) There is nothing we can do about that [staff shortage], so students are part of that [solution]. We train them, and they work with us. (Participant 3, Nurse in Charge)
The above strategies allowed the implementation of IPC guidance to come closer to ideal levels.
Discussion
The objective of this qualitative grounded theory study was to explore the implementation of IPC guidance at the healthcare facility level in the context of a low-income setting of Uganda. The study also aimed to develop a theoretical understanding of the processes involved in implementing IPC guidance based on the experiences of HCWs. This process was conceptualised as ‘striving for improved IPC practice’ and involved four phases: recognising the importance of IPC, playing a role, encountering challenges, and overcoming challenges. Through the analysis of these phases, the study shed light on how HCWs implemented IPC guidance in these contexts. The study identified specific barriers faced by HCWs and underscored the crucial role of improvisation in overcoming these barriers during the implementation of IPC guidance. Additionally, the study identified enablers that facilitated the implementation process. The concept of striving for improved IPC practices through improvisation may serve as a valuable model for addressing barriers, leveraging enablers, and enhancing the implementation of IPC guidance in low-income contexts.
Striving
In the modern world, striving is always part of our lives, as individuals are constantly bombarded by barriers that they have to navigate to reach goals. However, common assumptions around the use of striving tend to mask differing and complex understandings. Several definitions of the term ‘striving’ exist. For example, the Oxford Dictionary defines it as “to try very hard to achieve something” (Oxford Dictionary, 2015), while the Cambridge Dictionary (2020) expands on this and defines striving as “to try very hard to do something or to make something happen, especially for a long time or against difficulties.” In line with these definitions, within the current study striving meant giving one’s best to implement IPC guidance even when weighed down by challenges. This is echoed by Nilsson et al. (2019) in their phenomenological study aiming to understand how women with osteoporosis in Sweden strive to maintain their daily lives. Participants reported that striving to maintain their daily lives meant believing in themselves and their capabilities and not giving up. In comparing these definitions with the concepts emerging in this grounded theory study, issues of ‘action’ and ‘challenges’ are highlighted by Nilsson et al. (2019), possibly hinting at a sense of responsibility similar to the current study in which participants took responsibility for keeping patients safe, particularly when overcoming the challenges they faced. Although this was a phenomenological study in a different context exploring a different topic to the current study, it has similarities which add understanding to the theoretical concept of striving, as noted by the current study findings.
Further, the concept of ‘striving’ in this study could be said to align with theoretical concepts of altruism, which is the performance of cooperative unselfish acts beneficial to others and a general willingness to go the extra mile in professional activities (Feldman, 2017). Although there is a wide variation in the definition of altruism within the literature, common fundamental concepts are giving, sharing, cooperating, helping, and different forms of other-directed behaviour (Monroe, 1994). According to MacAskill (2015, pp. 14–15), altruism is about asking, “How can I make the biggest difference I can?” and using evidence and careful reasoning to find an answer. By striving to implement IPC, we see HCWs displaying altruistic behaviour, such as buying their alcohol hand rub sanitisers to make a difference in the uptake and utilisation of IPC guidance for safer healthcare.
However, critics have argued against altruism, pointing out that all human action is ultimately motivated by self-interest. Human beings often seek to benefit others, but when they do so, it is because they regard helping others as a mere means to their good (Elgat, 2015; Krauss, 2005; Monroe, 1994). For example, in the current study, it could be argued that, by buying their ABHR, HCWs were acting in their own interests, ensuring that infections are not transmitted to them and, in turn, to their families. Nietzsche states that because of this self-interest, altruism does not exist (Elgat, 2015). However, within the current study, altruism was demonstrated, for example, not only by going the extra mile to purchase their ABHR and improvising but in the repeated participant accounts of concern for patients, other staff, and students. HCWs showed absolute resolve in observing and practising the required IPC measures. Additionally, ‘striving for improved IPC practice’ developed from this study has some similarities with extracts from Alfred Alder’s theory of striving for perfection or superiority (Adler et al., 1956). In his early theory, Alder used the term striving for superiority to describe psychologically unhealthy people who strive for personal superiority over others. However, over time, Adler’s understanding of ‘striving’ evolved as noted through the various words he used like completion, mastery, perfection, and superiority to describe how humans seek to move from “the present situation, as observed and interpreted, to a better one, one that was superior to the present status” (Manaster & Corsini, 1982, p. 41). Thus, striving for perfection or superiority is the natural human desire to move from a perceived negative position to a perceived positive one (Watts, 2015). In relation to this study, it could be argued that some participants were striving to create a positive situation that would reduce HAIs through the successful implementation of IPC guidance. For example, nurses in charge are seen to act as ‘mothers’, with a duty of protecting their patients and staff against infections regardless of the circumstances through training, meetings, supervision of other staff, and practising recommended measures.
Improvisation
Uncertainty is inherent in healthcare, particularly in the context of low-income countries as evidenced in the current study, for example, resource constraints, the intermittent water supply, and the delay in delivery of IPC supplies. It is important to note that the Ugandan Ministry of Health plays a pivotal role in ensuring the implementation of IPC guidance within healthcare facilities through a series of established structures, such as the National IPC Guidance Committee which is responsible for developing the guidance and providing oversight at a national level, and the Local IPC Committee which is responsible for providing oversight and ensuring implementation at a health facility level. The resource limitations highlighted in the current study do not imply the state evades its responsibility. Instead, they are indicative of broader challenges and uncertainties inherent in such contexts. One strategy adopted by individuals for acting in the face of uncertainty is to improvise. As noted in the current study, participants’ ability to navigate these challenges through improvisation positively impacted the implementation of IPC guidelines. Through improvisation, HCWs demonstrated high motivation and commitment to adhere to IPC practices.
Within the literature, improvisation has long been considered a function of music, dance, and the theatre arts and is generally defined as the flexible treatment of pre-planned material (Weick, 1998). More specifically, in jazz, improvising has been described as “reworking pre-composed material and designs in relation to unanticipated ideas conceived, shaped, and transformed under the special conditions of performance, thereby adding unique features to every creation” (Berliner, 1994, p. 241). An exploration of these definitions and characteristics of this concept in relation to the art and practice of nursing provides an opportunity to illuminate related qualities within healthcare. While exploring improvisation in nursing, Hanley and Fenton (2013) noted that healthcare, particularly nursing, has always demonstrated improvisation because it is often required to meet the needs of patients in a rapidly changing environment usually littered with challenges. This is supported by findings from a qualitative descriptive study that analysed the subjectivity of nursing workers in the practice of adapting and improvising materials in Brazil, where participants revealed that the improvisations always occurred because, in addition to the typical way of dealing with problems, they were numerous that it was impossible to enumerate them (Lima et al., 2016). The authors noted that there was an observation of numerous scenarios in which, through the scarcity or inadequacy of material resources, nursing professionals performed various improvisations and adaptations.
Against this background, as applied in this study, improvisation served as a means to address resource limitations and overcome challenges encountered. By improvising, participants were able to vary their actions based on context or situation. Rather than being a mandated course of action within the study, it was an iterative process that allowed HCWs to creatively solve the problems at hand. This strategy also has similarities to a study on the palliative care movement in Kerala (Santhosh, 2016); Santhosh argued that resources from within the community need to be utilised to address its problems rather than wait for the state to step in and resolve them which is evident through the different improvisation techniques applied by participants in the current study. One theory that may put the role of improvising into the context of what is often considered a medical decision-making process is the dual process theory of clinical reasoning, as identified by Pelaccia et al. (2011). In this theory, Pelaccia et al. (2011) suggested that doctors rely on two processes to determine a course of action for a patient. The first is an intuitive process that is based on experience and pattern recognition. We see this in this study’s findings through what was conceptualised as on-demand improvisation where individuals were faced with the need to identify just in time resources and other strategies to overcome challenges as they were encountered. The second is an analytical and rational process that comes from a rational and deliberate judgement based on additional information collected actively by the individual in their environment and the conscious application of rules that have been acquired through learning. This was observed in this study through what was conceptualised as planning for the future improvisation where participants developed an enhanced awareness of their context and the challenges presented and were able to come up with strategies or solution through thought planning and action. Therefore, in improvising, information about a situation is collected and integrated in a social process, through interactions with other practitioners, the patient, and other staff members. McKenna et al. (2013) pointed out that this social nature of improvisation enables HCWs to extend their knowledge base beyond their individual funds of knowledge, capitalising on the knowledge of the other colleagues on their team or within their network, and thereby act more effectively in situations with high levels of uncertainty and challenges. This combination and reorganisation of knowledge and information allow HCWs to arrive at unique and creative solutions, as noted in this study.
Strengths and Limitations
The constructivist grounded theory method facilitated the exploration of an area of high complexity in a low-income context. The exploratory and constructivist nature of the study allowed the identification of aspects of practice through the first-hand experiences of HCWs as guideline users in the co-construction of the data through face-to-face interviews. The codes and categories developed in this grounded theory offered insights into the implementation of IPC guidance in a low-income country. Adopting this approach promoted the development of a theoretical explanation of the component parts of the process of ‘striving’ to implement IPC guidance; what the specific contextual barriers and enablers are; and how HCWs strategize through improvisation to get as close as possible to effective IPC implementation. Therefore, this study applied robust qualitative research methods to provide valuable evidence of HCWs’ perspectives on an important topic in an under-researched context.
One limitation of the study is the constrained time frame while collecting data and the busy schedules of HCWs, which meant that the researcher had to take advantage of the best available time for the participants, sometimes conducting more than one interview in a day. Therefore, the researcher could not always comprehensively analyse data from one interview before going into another. Corbin and Holton (2011) advised that it might be necessary to proceed with fieldwork as the opportunity to gather data presents itself, regardless of whether this allows for ample time to engage in analysis. Furthermore, data collection was hampered by the onset of the COVID-19 pandemic meaning that there was a lack of variety in the sample as interviews involved a narrow range of IPC practices at a single tertiary healthcare centre. The onset of lockdowns and travel restrictions meant that the study was not able to recruit from lower-level healthcare facilities and actors at the national level as initially planned. These limitations could be overcome by future studies with fewer time constraints.
Conclusion and Recommendations
Despite facing various challenges in low-resource contexts, HCWs made significant efforts to implement IPC guidance, although they never fully achieved it, akin to the theoretical construct of ‘asymptote’. This ongoing process was conceptualised as ‘striving for improved IPC practice’, offering valuable insights into the implementation of IPC guidance in resource-constrained settings. The substantive theory of this study was derived through inductive data analysis, providing a unique perspective in terms of the theory generated and methodology used in this area. The theory not only sheds light on the challenges and enabling factors that influence the implementation process but also highlights how HCWs overcome the diverse challenges they encounter. It demonstrates the remarkable degree of improvisation employed by HCWs to ensure the effective implementation and practice of IPC measures in low-income settings. Therefore, health managers should pro-actively demonstrate through staff meetings, clinical supervision, and supervisor support arrangements the value it places on the roles and responsibilities fulfilled by all its HCWs in delivering safe healthcare.
Future research could explore this topic on a wider scale involving actors at all levels of IPC implementation within a specific context, to identify the different experiences among all these participants. For example, involving hospital administrators and Ministry of Health officials who are not directly involved in delivering healthcare will add to the findings of the present study and complement this research. Given that this study was designed and conducted before the COVID-19 pandemic, the context of which likely changed after the pandemic, further research could explore the current contemporary context in Uganda. This would allow for exploration of the situation following the Ebola and COVID-19 outbreaks. These findings could be compared to findings from the current study to ascertain the impact of the pandemic on IPC practices within the country.
Supplemental Material
Supplemental Material - Striving for Improved Infection Prevention and Control Practice: A Grounded Theory of Healthcare Workers’ Struggles in Implementing Infection Prevention and Control Guidance in Uganda
Supplemental Material for Striving for Improved Infection Prevention and Control Practice: A Grounded Theory of Healthcare Workers’ Struggles in Implementing Infection Prevention and Control Guidance in Uganda by Andrew O. Kalule, Kay Currie, and Lesley Price in Qualitative Health Research
Footnotes
Acknowledgments
The authors would like to thank the Infection Control Africa Network (ICAN) for their support and guidance.
Author Contributions
AOK, KC, and LP conceptualised the study. AOK oversaw data collection and local IRB approvals. AOK conducted data analysis with advice from KC and LP. All authors contributed to the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data collection for this study was supported by the Glasgow Caledonian University Global Challenges Fund.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.