
Abstract
Suicide capability is a multidimensional concept that facilitates the movement from suicidal ideation to suicide attempt. The three-step theory of suicide posits that three overarching contributors comprise suicide capability: acquired (fearlessness about death and high pain tolerance), dispositional (genetics), and practical (knowledge and access to lethal means) capability. Although extensive research has investigated relationships between individual contributors of capability and suicide attempts, little research has considered how an individual’s capability for suicide develops as a combination of contributors. Given suicide is multifaceted and complex, our understanding of capability development is relatively limited. This potentially negatively impacts prevention and capacity reduction–focused intervention efficacy. Therefore, this study aimed to explore how suicide capability develops. Fourteen community-based suicide attempt survivors were recruited using convenience sampling. Individual narratives were collected using open-ended interviews, and data were analysed using narrative analysis. Results indicated that participant narratives contained two elements. The first included how capability development and suicide attempt facilitation were often underpinned by the relational interplay between acquired and practical contributors. For example, participants without a high pain tolerance seeking attempt methods that were perceived to be painless. The second element contained a novel finding relating to the agentic role of participants when deciding and attempting suicide. Agency was revealed within and across narratives emphasising the active role the individual plays in their movement from ideation-to-action. The role of individual agency in coming to a decision to take one’s own life and then acting warrants further consideration within contemporary suicide theories.
The movement from thinking about suicide to attempting suicide is a complex process that is still not well understood in the suicide literature. Most research has focused on suicidal ideation despite most people who think about taking their own life not progressing to a suicide attempt (Franklin et al., 2017; Richardson et al., 2022). Recognising this, the ideation-to-action framework posits that different processes and explanations differentiate those who think about suicide from those who attempt (Klonsky & May, 2014). This framework has spurred a growing body of quantitative literature seeking to identify factors that differentiate suicide attempters from suicide ideators (Bayliss et al., 2024; Favril et al., 2020; Mars et al., 2019). A key feature of the framework, and the contemporary theoretical models of suicide that sit within the framework, are capabilities that facilitate movement from suicidal ideation to suicide attempt (Bayliss et al., 2021; Keefner & Stenvig, 2020; May & Victor, 2018).
These capabilities form the concept of suicide capability. Capability is argued to be a core mechanism the progression from ideation-to-action and have evolved from the interpersonal theory of suicide (ITS; Joiner, 2005; Van Orden et al., 2010), the integrated motivational–volitional model (IMV; O’Connor, 2011; O’Connor & Kirtley, 2018), and the three-step theory (3ST; Klonsky & May, 2015; Klonsky et al., 2021). The 3ST includes the broadest range of overarching contributors to capability (acquired, dispositional, and practical) and acknowledges that there is a complex interplay of factors contributing to an individual’s capability.
Acquired capability was first introduced in the ITS and comprises a fearlessness about death and elevated pain tolerance (Joiner, 2005; Van Orden et al., 2010). Given that humans are naturally aversive to injury, pain, and death, it is necessary to develop a fearlessness about death to attempt suicide (Joiner, 2005). An individual acquires this fearlessness from habituation to painful and provocative events (e.g. child abuse and non-suicidal self-injury; May & Victor, 2018), allowing them to overcome the innate aversion to injury and pain through an increase in pain tolerance to therefore act on their suicidal ideation. Dispositional capability includes genetic (e.g. phobias) and psychological contributors (e.g. personality traits) that may increase or decrease aversion to injury, pain, and death (Klonsky & May, 2015). For example, high sensitivity to pain or blood–injection–injury phobia may decrease suicide capability, whereas low sensitivity or low phobic reactions to blood, injection(s), and/or injury may increase capability (Klonsky et al., 2021). Practical capability comprises an individual’s knowledge of, and access to, lethal means (Klonsky & May, 2015). The more knowledge an individual has about killing themself and the more ready access to means, the greater the risk of a suicide attempt. Each capability on their own is often seen as insufficient to move someone from ideation-to-action; rather, it is more likely to be a combination of the three capabilities that is critical in enabling movement (Khazem & Anestis, 2016; Klonsky et al., 2021).
A recent scoping review (Bayliss et al., 2022) found partial support for suicide capability. Based on the empirical literature, various painful and provocative events (e.g. traumatic experiences), some genetic factors (e.g. single nucleotide polymorphisms), and access to, and knowledge of, lethal means (e.g. firearms) were found to be related to capability. Further, longitudinal research results have challenged acquired capability as a concept given the lack of prediction for suicide attempts (Ribeiro et al., 2021) and differentiation between attempters and ideators (Bayliss, Hughes et al., 2023). However, most of the studies included in the review were single contributor cross-sectional studies looking at how such contributors are related to suicide attempts rather than how suicide capability develops for an individual. Given that the pathway to suicide attempt is complex and likely to involve more than a single contributing factor (Lee & Pak, 2022; Tandon, 2021), cross-sectional single-factor studies limit our understanding of suicide capability (Bayliss et al., 2022; May & Victor, 2018). This is because a single factor can only capture a unidimensional understanding of capability with cross-sectional designs providing single-point-in-time understandings, both of which are unable to explain how suicide capability, as a multidimensional concept, develops over time. What this means is that critical questions about potential relationships between contributors and how individuals develop a capability for suicide remain unanswered (Ribeiro et al., 2020).
New knowledge about acting on suicidal ideation is needed and is more likely to come from inductive and idiographic approaches than from doing more of the same studies that have informed what we know now (Nock et al., 2019). While concerns about the generalisability of results are often associated with inductive and idiographic approaches, they are useful for theory refinement and grounding constructs in lived experiences (Smith et al., 2020). Given the argument that current suicide theories require additional research to better understand how individuals move to act on suicidal ideation (Millner et al., 2020), inductive and idiographic research approaches are well suited to address this. One starting point is suicide attempt survivors’ perspectives because they can provide insight into acting on suicidal ideation and how capability develops through first-person narratives (Galasinski & Ziólkowska, 2020; Robinson et al., 2022). Lived experience stories offer an opportunity to explicate the development of suicide capability as a multidimensional concept (Yunitasari et al., 2023).
One qualitative research analytic method that seeks to understand an individual’s experiences as told through stories is narrative analysis (Josselson & Hammack, 2021). Narrative analysis differs from other qualitative research methods (e.g. thematic analysis) in that the text is not broken down into themes but instead the whole text is considered a narrative (McAllum et al., 2019). It is the content of stories together with features such as story elements that helps explicate meaning of psychological experiences (Wong & Breheny, 2018). As a noted valuable method for individuals to explain behaviour that led to a suicide attempt (Fitzpatrick, 2016), narratives enable the unintelligible chronological development and action of a suicide attempt to become intelligible (Michel & Valach, 2011). Recent discussion about the value of narratives in suicide research has raised concerns about the influences of memory, perception, and attribution errors that may influence the stories told by participants (Bantjes & Swartz, 2019). However, as Hjelmeland and Knizek (2020) posit, the stories told are representative of the meaning and understanding that the lived experience has for the narrator. This is important in the context of this study because it is the meaning ascribed by the individual that is fundamental to understanding how they were able to develop their capability to act on their suicidal ideation.
As most capability research has focused on the identification or existence of contributors, how multiple contributors of capability develop through potential relationships and/or combinations to facilitate the movement from ideation-to-action has typically been overlooked. Unsurprisingly, little is known about how individuals develop their capability to act on suicidal ideation. Efforts to intervene and prevent the development of capability, and by extension suicide attempts and deaths by suicide, are likely to be misguided and potentially ineffective without understanding how an individual develops a capability for suicide. Thus, the aim of this study was to explore how suicide attempt survivors developed their suicide capability to move from ideation-to-action.
Method
Participants and Setting
The study was granted ethical approval by the University of Southern Queensland Human Research Ethics Committee (H21REA015). All participants volunteered and provided informed written consent to be interviewed for this study. Australian participants were recruited using convenience sampling from two sources: 1. A national lived experience organisation advertised the study via a recruitment flyer posted on social media and emailed to their lived experience collective. 2. The authors advertised the same flyer mentioned above via their social media accounts (e.g. Twitter and LinkedIn).
Individuals expressed interest in the study to the first author via email who then provided them with the participant information sheet and consent form. If an individual decided to participate (one individual did not participate), prior to the interview they were provided with a Readiness for Research© information sheet that was created and provided by Roses in the Ocean©. This sheet prompts individuals to consider whether they feel that sufficient time has elapsed since their lived experiences of suicide and motivations for participating in research. This was to ensure that participants were able to safely share their lived experiences.
Interviews were conducted via Zoom™ and lasted between 40 and 80 min. Before commencing each interview, the aim of the study was reiterated, and consent was re-confirmed. Participants were encouraged to speak without restriction or self-censorship. All participants completed their interview without stopping and continuing at another time. Participants were debriefed immediately after their interview and redirected to resources on the participant information sheet. Follow-up phone calls were made usually within 24 hours, but no later than 72 hours later, to check on participants’ welfare. Welfare was determined in relation to the participant stating that they were at potential risk of harming themselves. If this was stated, the interviewer would have contacted emergency services to request that a physical welfare check be carried out. A second welfare check would have been conducted at a later date. However, no concerns were raised by participants during these phone calls, but they were thankful for the opportunity to tell their story without interruption and without censorship. All interviews were audio-recorded and transcribed by the interviewer or a professional transcription company.
The sample comprised 14 Australian participants (identified as Australian through self-disclosure) aged between 29 and 74 years (M = 47.00 years, SD = 12.73). Most participants were female (n = 11), and each participant had at least one suicide attempt and/or interrupted suicide attempt (range: one to numerous attempts) with intent to die (De Leo et al., 2021). The most common suicide attempt method was overdose with prescription medication, followed by motor vehicle and cutting. Length of time since their last attempt ranged from 10 months to 24 years (M = 8.22 years, SD = 7.29).
Data Collection
Data were collected through open-ended narrative interviews using Michel and Valach’s (2011, p. 63) “the narrative interview with the suicidal patient.” As per the interview guide, participants were first asked: I would like you to tell me the story of what led to your suicidal crisis, please. Participants then told their story without interruption. After which the interviewer asked questions to clarify any aspects of the story that were unclear. Following this, the interviewer asked open-ended probing questions to elicit further information about other aspects of the participant’s life. Participants were then asked: Is there anything else you would like to tell me about your life? This approach allowed for flexibility regarding how the interview progressed. Moreover, this empowered the participant to talk about what they deemed meaningful and important, which is critical for narrative research (Mancini, 2019).
Data Analysis
An Overview of the Narrative Analysis Process.
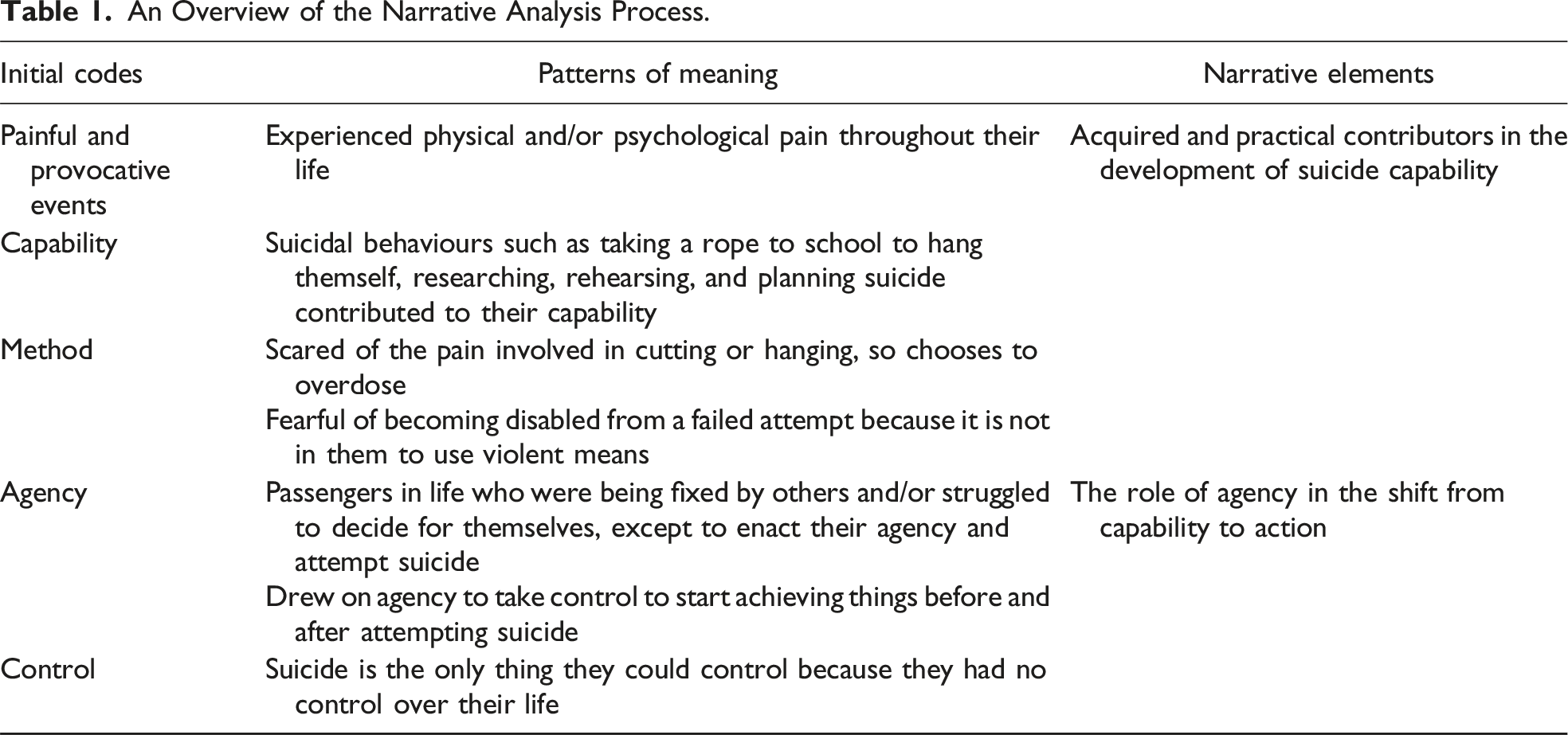
The first step comprised reading transcripts, generating initial thematic content, and identifying the Gestalt of the narrative. Interview transcripts were first reviewed for transcription accuracy by listening to the recording and reading the transcripts. During this review, a hermeneutics of faith that sought to identify and summarise meanings as explicitly conveyed by each participant was applied (Josselson, 2004; Josselson & Hammack, 2021). Coded excerpts were identified through Alexander’s (1990) markers of saliency, as adapted by Josselson and Hammack (2021). A general impression document that included a commentary of the interview, initial ideas, the Gestalt of the story, and reflexivity notes was created for each interview. While Josselson and Hammack suggest the participant create a life timeline drawing to highlight key life events, this was not adopted in this study. As interviews were conducted virtually during COVID-19 lockdowns and social distancing restrictions, it was difficult for the participant to create their timeline drawing during the interview. There was potential for participants to become unnecessarily frustrated if unfamiliar with Zoom (Archibald et al., 2019), and the additional time required to instruct participants to use the Zoom annotate function could have reduced the data collection process within the interview (Thunberg & Arnell, 2022). Instead, the researchers followed Hiller’s (2011) suggestion and created a timeline of the individual’s life as expressed throughout the interview to display key events, emotions, and other happenings (see Figure 1 for an example). Example of participant’s timeline created by the research team.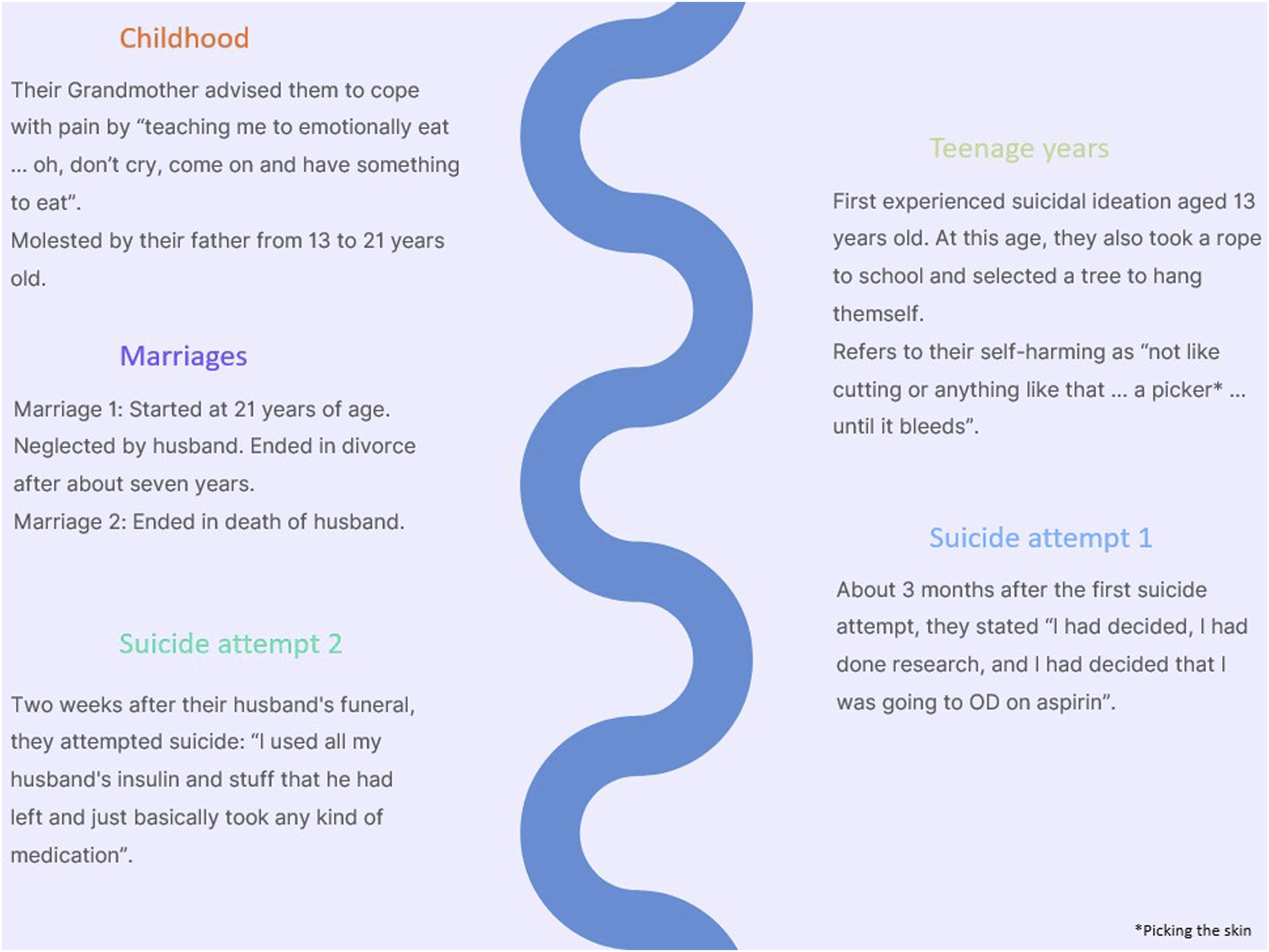
The second step involved reading the interview transcripts again. In this second reading, a hermeneutics of suspicion was applied to identify and code implicit voices and dialogues within narratives (Josselson, 2004; Josselson & Hammack, 2021). A table was created for the voices identified within each participant’s narrative and contained three columns with descriptive titles of codes: voices and dialogues (e.g. suicide prevention guidelines), clusters of implicit meanings derived from voices (e.g. ideologies restricting how suicide can be spoken about), and how these influenced the participants’ storytelling (e.g. asking if they can continue talking) or interpreted by the analyst (e.g. impact of painful and provocative events). After the completion of this second step, three documents were created for each participant – the general impression document, timeline, and a table of voices document.
At the start of the third step, each transcript was re-read again, and codes were reviewed to consolidate clusters of meaning into patterns of meaning. This involved moving beyond descriptive titles of codes (e.g. not listened to) to express what the patterns potentially mean in greater detail (e.g. previous suicide attempts were self-reported cries for help that no one listened to while they increased their capability for suicide). As a result of this third step, a fourth document was created for each participant – a two-column table that included one column for patterns and an empty column for theory connection.
The fourth step involved shifting from an inductive phase to a connection of data and theory phase (Josselson & Hammack, 2021). This step required linking patterns of meaning to ideation-to-action theories using the two-column table document created in the previous step. Given advancing theoretical understanding about the development of suicide capability through the lens of the ideation-to-action framework was a focus of this study, the ideation-to-action theories (i.e. ITS, IMV, and 3ST) were already embedded throughout the research process. Thus, an a priori selection of theories was deemed appropriate (Sperka, 2019). Data that did not align with existing theories were considered theoretical gaps.
The final step was cross-cases analyses. This involved identifying commonalities and differences between participants that were derived from the three aforementioned documents. This produced two shared experiences that contributed to the development of suicide capability (i.e. abuse and knowledge of lethal means). These differences enabled the comparison process that was conducted through grouping the two shared experiences. After which, cross-case analyses of these experiences through the lenses of the ideation-to-action theories were completed. Data considered theoretical gaps identified in the previous step were also cross-case analysed by identifying, grouping, and comparing particularities and differences. Analysis was conducted from an inductive position that sought to explicate how participants’ narratives could advance suicide capability theory through a focus on capability development.
Reflexivity Statement
A reflexivity statement from the first author is offered to contextualise and provide fidelity in the interpretations that underpin the results as is consistent with narrative analysis (Josselson & Hammack, 2021). I (LTB) do not have lived experience of suicidality; I believe this allows me to bring an open curiosity to the study of suicidality because I do not have a personal story to compare to other stories. This can help in reducing biasing or skewing interpretations based on my own story (Bukamal, 2022; Dwyer & Buckle, 2009). My assumptions and beliefs about suicide are that individuals choose suicide because dying is better than living and enduring the pain the individual is experiencing.
Being an outsider, looking in affected my reactions to the stories I heard, especially when attempting to understand the methods selected by participants when attempting suicide. At first, I felt disbelief that many individuals attempted suicide by overdosing given this can cause severe internal damage and is not as lethal as other means. While I was under the impression the suicide attempts were attempts to die, this choice of method challenged my impression as I pondered participants’ intent. However, after reading and re-reading transcripts, it was clear that the overdoses were attempts to die, but selecting this method was mainly a result of not wanting to use more violent methods because of the pain involved.
As analysis continued, I become cognisant of the voices expressed by participants when discussing their pathway to attempt suicide. That is, there was explicit and repeated first-person storytelling that alerted me to their active role when planning, preparing, and attempting suicide. Participants were explicitly telling me that they decided to attempt suicide and they made sure that decision would come to fruition through careful planning and preparation.
Results
While each of the 14 narratives presented a unique story of the journey towards a suicide attempt, two distinct narrative elements (i.e. features of stories; Boyd et al., 2020) that were present in all participant stories were identified through the analytic process. These two elements were, one, how capability for suicide developed and, two, accentuating a sense of agency when deciding and taking actions to attempt suicide. This first element illuminates how capability developed through acquired and practical contributors. The second element of the stories revealed agency in the movement from suicidal ideation to suicide attempt, agency being “the experiences of intending to act, of choosing to make one particular action rather than another and of initiating or triggering the action” (Haggard, 2017, p. 2).
The Development of Suicide Capability as a Multidimensional and Relational Concept
Both acquired and practical contributors of suicide capability were reflected in participants’ narratives. Acquired capability is theorised to develop from habituation to painful and provocative events and is characterised by a fearlessness about death and an increase in pain tolerance (Joiner, 2005; Van Orden et al., 2010). As part of telling their story, participants shared their experiences of painful and provocative events through having lived through various forms of abuse (e.g. childhood and sexual). Some participants spoke about their perpetrators and abuse vaguely, for example, “I had physical and verbal abuse from them [parents] and the relationship with dad was kind of weird because we were inseparable until I hit puberty.” However, other participants spoke about their experiences more specifically, such as being “sexually abused by an uncle of mine until I was 13” or their “brother would sneak into my room at night and touch me in private places and that’s something that has been uncomfortable to acknowledge, speak about, and reconcile with my whole life.” Another participant experienced sexual abuse from when they were 13 years old: Within the first week after I turned 13, I was in my bedroom and I was, I remember very clearly, I was cleaning my drawers out and I was sitting on the floor sorting some stuff out. And my dad came into my room … that was the day my dad started molesting me. And that went on and I’m very tempted to say, I’m very ashamed to say that it went on till I’m 21.
These participants expressed difficulties with intimate relationships that they attribute to being sexually assaulted as children and teenagers. Such difficulties include feeling like they have little or no control over their relationships, a lack of trust and fear of men that prevented disclosure of feelings, and marriages and relationships that ended in divorce or separation.
While increased pain tolerance is one characteristic of the acquired contributor, not all participants reported an increased pain tolerance despite having experiences of abuse and having a fearlessness about death. Instead, they focused on knowledge and access to lethal means precisely because of not having a high pain tolerance. To overcome this perceived lack of pain tolerance as conceptualised within the acquired contributor and to increase their overall suicide capability, participants then developed their practical capability through access to and knowledge of lethal means (Klonsky & May, 2015; Klonsky et al., 2021). Thus, the potentiality of suicide capability contributors functioned in relationship with and to each other. That is, acquired capability appeared to relate to practical capability through choice of means and methods. The following exchange illustrates this: One lady came in a couple of days after I did [following her own suicide attempt]. And she had bandages all up her arms. And a week later, she took the bandages off, was cut, cut, cut, cut, cut. She’d taken a bread knife and tried to kill herself by cutting her wrists. But she didn’t cut deeply enough. And she was found covered in blood on the bathroom floor. And the pain of cutting oneself, like that, which is indescribable, I wouldn’t have the guts to do it. … I would never have the guts to shoot myself, to slash my wrists, to throw myself into the river with pockets full of stones. I would never because I don’t fear death. I have no fear of death. Death to me is like, oh, thank fuck, it’s over … And it’s it seems to me, and I believe that doing it the way that I’ve chosen would be, it wouldn’t be, pleasant. But I do believe it to be painless, fairly quick and done right, it would be very successful.
The participant in this passage drew a clear demarcation between fearlessness about death and a lack of pain tolerance. This indicates that the link between the two as suggested by the acquired contributor in ideation-to-action theories appears to be different for this participant. While increased pain tolerance was not required, a minimising of pain was. In a sense, it is making practical choices to deal with pain through minimisation methods rather than tolerate the pain. Hence, a relationship between acquired and practical contributors was needed to facilitate a suicide attempt. This is also reflected in the following participant’s story: I’ve got all these pills. Suddenly for the first time in my life I’ve got an easy way to kill myself. I’d never had that before. I never wanted to hurt myself physically. I didn’t want to hang myself or slit my wrists or something because that would be painful. So I’m like, I’ve got all these pills so I’ll just take them … if somebody had handed me that bottle of pills or those two bottles of pills 10 or 15 years earlier, I would have taken them then. So I don’t think it was necessarily that I came to this decision at this point in my life, it was that I’d made the decision many, many years before and I suddenly had the opportunity.
These participants had access to a perceived painless method that enabled their suicide attempt despite an absence or lower level of pain tolerance. Thus, for some participants in this study, their capability for suicide seemed to develop from an interplay between acquired (i.e. fearlessness about death and pain minimisation) and practical contributors (i.e. knowledge and access to lethal means).
When Capability Shifts Into Action
This second identified element focuses on an internal factor that may form the basis of the aforementioned relationship and the movement from ideation-to-action; when participants narrated their suicide attempt(s), they emphasised agency in both the decision and actions taken to enact the attempt.
The following extracts taken from different participants highlight a sense of agency in the decision to attempt suicide, which was often expressed as control: “I can control this [death]. This is a decision I’m making for myself,” “I just think, fuck you. You don’t know what I – you don’t know how I think or what I feel like and it’s mine; it’s my only thing that I’ve got – that I’ve got control over,” and “I can control what is going to happen to me, how I’m going to die. They won’t kill me; I will die by my own hand.” Thus, the decision to attempt suicide was constructed as participants being an active agent in their attempt represented by them having control of that decision.
The shifting of capability into action included both agency in the decision and agency in the actions taken towards the suicidal act. As one participant stated, “the potentials there in me, but I’ve also come to recognise the signs. And I know now when I get to that point, I really, seriously need to reach out and get help.” This suggests that their potential increases and readies the individual for an attempt as they are aware they can draw on their agency. The following passage highlights the two aspects of agency: So one day, while I was in the second respite home, which was quite a nice place, it was nice people. I just thought that I’ve had enough. So I actually was at my car in the parking lot and I had a blow up mattress, which I had blown up in the back of my big old station wagon and I was getting ready with cylinder of helium and a bit of hosepipe. I was getting ready to actually do the deed … It was it was the most relaxing, relieving, comfortable feeling. I wasn’t. I wasn’t distressed. It was a conscious quiet decision that. Enough is enough. It’s like, I’m sorry, kids, I’d written suicide letters to all my children and to a whole bunch of friends. And I. I wasn’t upset or distressed. It was just a quiet, conscious decision to finish up because I’d had enough.
This participant uses the words “conscious” and “quiet” to narrate their decision to get ready for and attempt suicide suggesting that the participant was the agent of the (conscious) decision which was deliberated internally (i.e. quiet). The participant further demonstrated agency by writing suicide letters and preparing their death bed in the car ready for their suicide attempt. We do not know what they had “enough” of because it remains unspoken, but what we do know is that the participant explicitly communicated that they made the decision to attempt suicide and took deliberate actions to make the attempt happen. The following narrative from another participant articulates their agency and decision-making processes when moving from ideation-to-action: There’s [sic] people that I know who say to me, oh they think about suicide, but they would never do anything. I don’t personally get that because when I think about suicide, I do something, I don’t just think about it, I actually act on it. Because I noticed that when I act on it the sense of release that comes from making that decision helps me to do the act … When you make that decision, there’s a release that comes with that, it’s like wow I’ve made the decision, I don’t think about that anymore, I’ve made my decision I want to do this. When you go to the planning stage, and I also think about things like who will find me, I mean I still really think about this because I was afraid, I don’t want my kids to find me, I don’t want people that I knew to find me. There were thoughts at one stage of throwing myself in front of a truck, but I thought no it’s not fair to the driver. I actually once laid on train tracks then I thought no it’s not fair to the train driver, do you know what I mean, there’s always these things that come in your mind. What if somebody finds me, who’s going to find me, what condition will I be in, do I want to be found, do I want to go to the ocean where I won’t be found but then there’s going to be questions for the family what happened to them, you know what I mean. There’s [sic] always these things but all I know is there is a release that comes when you make the decision … Then when you do the act there’s another release that comes. There’s a release that comes when you make the decision, then when you pop the pills or cut yourself or set fire to yourself, there’s another release that comes with that. It’s like wow I don’t have to think about this anymore, I’m just going to close my eyes.
In this excerpt, we again see agency in both the decision and the act. However, this excerpt includes three progressive stages each told with an agentic voice. The first stage is deciding to die by suicide. The participant expresses that when this decision was made, they experienced a sense of release where the movement to attempt suicide was made easier. After this binary decision (i.e. to die or not to die by suicide) was made, the (second) planning stage was embedded with practical decisions to be made (e.g. how will I do it? Who will find me? Do I even want to be found?). Again, once this practical decision was made, another sense of release accompanied that decision, and thus movement continued to the attempt. As the participant refers to the various means they used to try to kill themself, their agency is further exemplified in the final stage through self-reported actions such as “cut yourself” and “set fire to yourself.” Agency in the decisions leading to a suicide attempt and actions taken to make decisions a reality for some participants appear to be indicative of a conscious enactment of their capability.
Discussion
This study aimed to understand how individuals developed their capability for suicide. Findings from this study reflect the acquired contributor of suicide capability (Joiner, 2005; Van Orden et al., 2010) in that abuse was prominent in narratives. But findings also indicate that some participants had one characteristic of acquired capability (i.e. fearlessness about death) along with a reduced and/or lack of the other characteristic (i.e. increased pain tolerance). For some individuals, pain minimisation rather than pain tolerance appeared critical in the development of capability. This is important because it indicates that the acquired contributor may contribute towards suicide capability in a more nuanced manner than what has previously been hypothesised (Bayliss et al., 2022; Ma et al., 2016).
This study also found that participants emphasised their active role in deciding and taking actions to attempt suicide. Despite an independent actor making decisions and acting on those decisions when attempting suicide, the concept of agency is not often present in suicidology discourse (Broz & Münster, 2015; Galasinski & Ziólkowska, 2020). Galasinski and Ziólkowska identified agency in suicidal actions (e.g. planning, preparing, and attempting) but not the decision to attempt suicide because that decision is ascribed as something external and outside of an individual’s control. Results from this study, however, indicated agency in both the decision and suicidal actions. Ascribing to Haggard’s (2017) definition of agency that includes intending, choosing, and initiating an action, we can see from the participants’ stories that agency appears to contribute to and may potentially underlie the shifting of suicidal ideation and suicide capability into action. Our findings indicate that taking control of one’s death through decisions and actions was paramount for participants.
Participants spoke about their potential for suicide and readying for their suicide attempt. Moreover, the stages (i.e. deciding, planning, and acting) that were progressed through to make an attempt highlight the gap between having a capability for suicide and attempting suicide. These current findings regarding the agency may be linked to a finding reported by Capron et al. (2022), which focused on the concept of a suicide readiness state. The authors suggested that an individual with suicidal ideation and a capability for suicide will attempt suicide when an unacceptable loss occurs (e.g. fight with their spouse and loss of job). While the concept of a suicide readiness state resonates with our findings, the unacceptable loss aspect does not. Further, Capron et al. indicate that the movement into a suicidal state once an unacceptable loss threshold is crossed is likely to be automatic. This suggests that individuals do not have control of moving into such a state and it is a fait accompli. As such, this may be interpreted as something that happens to individuals rather than being an agentic process. That is, individuals who have their negative threshold exceeded and experience suicidal ideation while having a capability for suicide will inevitably attempt suicide. On the contrary, the findings from this study suggest that the individual is conscious and the movement into a suicide readiness state is agentic, perhaps because it is the one thing they can control, thus challenging the notion that the movement into a suicide readiness state is automatic. Therefore agency appears to be critical for moving into both a suicide readiness state and attempting suicide.
We agree with Capron et al. (2022) that current theoretical models of suicide (e.g. ITS, IMV, and 3ST) appear to describe a state of readiness for suicide to occur but lack a missing aspect that shifts capability to action. O’Connor and Kirtley (2018) briefly touch on perceived control over suicidal behaviour, which may be seen as high capability within the IMV. However, this falls short of ascribing agency to the suicidal individual, and thus the missing aspect of shifting into action remains. This missing temporal aspect within current theories is imperative to explore and understand for timely and efficacious clinical intervention(s).
It may be that capability gets one to a state of suicide readiness, but agency is needed to move from this state to the final stages of action. The missing temporal aspect of theories, or when a suicide attempt happens from a suicide readiness state, may be initiated by the individual’s decision to choose suicide that fuels further practical decisions leading to the attempt. Our findings suggest a critical juncture in the temporal sequence from ideation-to-action is after the practical decisions (e.g. when, where, and how) have been decided. It may be at this moment that the practical contributor of capability is most important as the individual accesses means to attempt suicide. Capturing the moment an individual moves from the suicide readiness state (Capron et al., 2022) and when they decide to act may be where suicide prevention can be most effective. Further exploration of agency may help towards understanding the bridge that separates being ready for suicide and attempting suicide. Understanding this gap between readiness and attempt is essential for timely and effective interventions that can potentially interrupt the movement towards a suicide attempt and keep individuals safe at the very moment they need it.
As agency is yet to feature in contemporary theoretical models of suicide, and whether agency is a capability that itself needs to be developed warrants attention. The narratives from this group of suicide attempt survivors suggest the power of agency should be explored in more detail for greater understanding of the movement from ideation to action. Given this, we contend that agency could be considered within theoretical models of suicide regarding both the potentiality of a relationship between acquired and practical contributors and acting on their capability.
Limitations and Future Research
While this study had strengths such as including participants with experiences of various suicide attempt methods, differing lengths of time since last attempt, and a focus on allowing the participant to tell their own suicide capability development story, the study is not without limitations. First, the sample comprised suicide attempt survivors, which means that findings are of course indicative of non-lethal suicide attempts. This may account for the pain minimisation findings. Further, the sample mostly included participants who identified as female. While this sample reflects the Western-centric gender paradox whereby more females attempt suicide and more males die by suicide (Canetto & Sakinofsky, 1998), we were unable to ascertain if potential gender-related contributors influenced capability beyond this participant group. Second, the use of social media as a recruitment approach is not without its limitations. It is recognised that this has meant that not all elements of the sampling frame could be identified. A potential consequence of this is self-selection bias in that a non-representative sample may have overrepresented their experiences (Bayliss, Krishnamoorthy et al., 2023). However, given the target population, the use of social media as a recruitment tool was deemed appropriate as it did allow an increased probability of reaching a segment of the general population that may not easily be accessible or identifiable in any other way (Gelinas et al., 2017). Furthermore, clear participant inclusion criteria were also used to ensure that those who did participate in the study were members of the target population in an effort to minimise limitations associated with the recruitment approach adopted. Third, retrospective recall and the range of time since the last attempt may have introduced the fading affect bias (Walker & Skowronski, 2009). This bias can potentially increase a positive self-image – including overcoming adversity to foster hope – when individuals rehearse their story. As such, the role of agency may have been overemphasised as participants narrated their stories and implicitly reminded themselves of the adversity they have survived. Finally, the study did not incorporate cultural considerations regarding suicide. Like all behaviours, suicidal behaviours can be influenced by implicit cultural scripts that include beliefs, attitudes, values, and methods for suicide (Canetto, 2021). Therefore, findings and contributors to capability may have been influenced by unidentified cultural scripts. Despite these limitations, findings can be used as foundations upon which to develop other studies that extend and challenge, in this case, theoretical understandings of suicide capability and its development.
Based on the findings from this study, three recommendations are presented to advance understanding about the shift from suicide capability to attempt. First, the role of agency in the decisions about when and how an individual will attempt suicide requires greater elucidation. A starting point can be studies that deliberately focus on suicide attempt survivors’ agency (e.g. perceived capability for suicide (Rimkeviciene et al., 2016)) together with both acquired and practical contributors. Second, the final movement from a suicide readiness state to a suicide attempt remains unclear. For example, the question of exactly when ‘enough is enough’ continues to elude us. On one hand, longitudinal studies such as ecological momentary assessment that contain items which assess suicide capability as a multidimensional concept may be able to generate knowledge about the shift from a suicide readiness state to attempt (Spangenberg et al., 2019). On the other hand, a clearer sampling frame that includes more recent suicide attempt survivors could help clarify this shift while also helping reduce the impact of the fading affect bias. Finally, more diversity among participants is needed within suicide capability studies to reflect the disproportionate number of male suicide deaths. Fisher et al. (2022) argue that males’ gendered experiences must be considered regarding suicidal behaviour, and we complement this by questioning whether gender or sexual orientations could potentially influence differences in suicide capability, perhaps via cultural scripts.
Conclusion
Our findings suggest that the individuals in our study developed their capability for suicide through an interplay between acquired and practical contributors. Further, our findings bring forth for consideration the importance and place of agency in both the decision to attempt suicide and the suicidal act. Importantly, what our findings have shown is that if capability is something that is developed and that one has agency over the decision to exercise that capability, then there is potential to identify critical moments to help develop just-in-time interventions. These critical moments arise when capability has been developed sufficiently and when agency is about to be enacted for a suicide attempt.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Australian government.