
Abstract
Medical guidelines recommend actively addressing patients’ information needs regarding complementary and integrative healthcare (CIH). Within the CCC-Integrativ study, an interprofessional counseling program on CIH was developed and implemented at four comprehensive cancer centers (CCCs) in Germany. As part of the process evaluation, this study examines cancer patients’ experiences with interprofessional CIH counseling sessions conducted by a physician and a nurse. Forty problem-centered interviews were conducted using a semi-structured interview guide. All interviews were audio-recorded, transcribed verbatim, and analyzed using deductive–inductive content analysis based on Kuckartz and Rädiker’s approach. Findings revealed that most participants had prior experience with CIH approaches and were burdened by physiological and psychological symptoms. Counseling sessions focused on cancer- and treatment-related symptoms and appropriate CIH recommendations (e.g., herbal poultice against anxieties and acupressure against nausea). Participants appreciated the mutual exchange and integration of perspectives from different healthcare professions within the interprofessional approach. They noted that the counseling team comprehensively addressed their healthcare and CIH information needs. Suggestions for improvement included the specificity of the CIH recommendations. As the participants only received counseling and no CIH treatments, information about reputable CIH providers was particularly important to many seeking advice. Patients with cancer receiving tailored CIH counseling from two healthcare professionals experienced benefits in CIH counseling for symptom management. The interprofessional teams offered a comprehensive perspective on patients’ needs, proposing personalized recommendations for symptom control. These insights may foster collaboration between healthcare professionals interested in CIH counseling, enabling them to expand and consolidate their counseling services.
Keywords
Introduction
Due to cancer patients’ high demand for complementary and integrative healthcare (CIH) approaches (Horneber et al., 2012; Keene et al., 2019) and its growing evidence base (Deng, 2019; Guerra-Martín et al., 2021), clinical guidelines recommend actively asking cancer patients about their information needs on CIH (German Guideline Program in Oncology, 2021; Schofield et al., 2010). Counseling interventions on evidence-based CIH applications have been shown to meet cancer patients’ information needs (Horneber et al., 2018), improve their satisfaction and quality of life (Klafke et al., 2019; Stie et al., 2020), and increase patient activation (Foley & Steel, 2017). Patient activation is a concept that refers to knowledge, attitudes, and behaviors that help individuals to successfully cope with their health or chronic conditions (Hibbard et al., 2004). Enhanced levels of patient activation are associated with improved symptom management and health outcomes (Hibbard & Greene, 2013).
However, previous patient-centered interventions integrating CIH into oncology focused only on one professional group (either medical or nursing staff) (Klafke et al., 2019; Witt et al., 2020), which does not reflect the multidimensional, interprofessional approach of integrative oncology (Deng et al., 2009). Within the CCC-Integrativ study, a complex interprofessional intervention was developed and implemented at the four university cancer centers in Baden-Wuerttemberg, Southern Germany, to improve the integration of CIH into oncology care. The intervention includes elements at the patient, provider, and system levels. Patients diagnosed with cancer received three individual counseling sessions and additional informational materials about CIH (intervention on the patient level). At least one of the three consultations was conducted interprofessionally, and the healthcare staff of the counseling teams underwent a 13-day blended learning training program before the intervention. The participating physicians had diverse medical backgrounds, including specialties such as internal medicine, oncology, general medicine, general surgery, and visceral surgery. Some had additional qualifications in palliative medicine, intensive care medicine, acupuncture, pain therapy, mindfulness-based treatments, and anthroposophical medicine. The nursing experts had backgrounds in intensive care, anesthesia, oncology, pain management, and palliative care. Some also had special qualifications in aromatherapy, wraps, compresses, and anthroposophical nursing. Provider-level interventions included supervised training and team-building activities, while intervention on the system level incorporated training on CIH in the outpatient setting (Valentini et al., 2022).
In parallel to the main study, a process evaluation was conducted, since in complex, multicenter interventions, the factors that influence the adoption of the clinical intervention differ from those that determine whether the intervention is successful (Bauer & Kirchner, 2020). Examining intervention fidelity, quality, and context of implementation can inform the development of strategies to optimize the intervention (Skivington et al., 2021). The mixed-methods process evaluation aimed to identify barriers and facilitating factors at the different context levels (Bossert, Mahler et al., 2022). To address these research objectives, three distinct yet interconnected studies were designed and conducted in consideration of the Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2009), a recognized framework for the evaluation of complex interventions (Kirk et al., 2016). The CFIR provides a comprehensive structure for describing the processes and factors that explain intervention effects. It integrates key concepts from various implementation and evaluation research models specifying five core domains (Intervention characteristics, Outer setting, Inner setting, Characteristics of individuals, and Implementation process) for the analysis of the intervention process. As such, the CFIR enables valuable insights and guidance for analyzing healthcare change processes (Klafke et al., 2017).
The present study examines the perspective of patients voluntarily participating in interprofessional counseling sessions on CIH (study 3 of the process evaluation) (Bossert, Mahler et al., 2022). The current analysis focuses on: patients’ experiences with the interprofessional counseling program; which factors they perceived as beneficial or hindering in the counseling context; and to what extent the interprofessional approach to counseling influences patient-centered communication and information transfer about CIH. The patients’ personal benefits and experiences when integrating the CIH recommendations into their daily lives will be reported in another publication.
Method
Study Design
In patient-centered interventions such as CCC-Integrativ, a qualitative research approach allows an in-depth exploration of patients’ needs, feedback, and satisfaction regarding each implementation aspect (Patton, 2015; Safaeinili et al., 2020). We decided to conduct problem-centered interviews, characterized by a deductive–inductive approach to data collection and analysis. This interview type is well-suited when prior assumptions exist about the phenomenon under investigation. By incorporating subjective statements from the interviewees, this approach expands and enriches prior knowledge. Researchers use their prior knowledge to structure interviews and formulate questions (deductive reasoning) that guide respondents’ statements toward the research problem. Additionally, researchers actively engage with interviewees and their narratives, allowing them to contribute individual perspectives and insights (inductive reasoning). Consequently, this interview method is valuable to supplement or correct prior knowledge about implementing CIH counseling programs (Witzel, 2000).
Data Collection
Participants were recruited at the four participating CCCs (Freiburg, Heidelberg, Tuebingen-Stuttgart, and Ulm) in Southern Germany between July 2021 and April 2022. We selected 40 patients (10 per CCC) from the intervention group based on a purposive sampling strategy to maximize variance in specific demographic data (age, gender, cancer diagnosis, and treatment approach) (Palinkas et al., 2013). The aim was to obtain a comprehensive picture of patients’ perceptions in this way. Please refer to the main study protocol for specific information regarding patients’ inclusion and exclusion criteria (Valentini et al., 2022).
The study assistant in charge or a counseling team member at the respective CCC invited the patients and informed them (orally and in writing) about the aims and proceedings of the interview study. Patients had ample time (several days) to consider participation. Written informed consent and a data protection agreement were obtained.
The first author (HD), with a psychological and medical background, conducted all interviews. The first 20 interviews (five per CCC) took place after the participants had received their initial consultation (IC). In a second wave of the data collection, an additional 20 patients (five per CCC) who had received one or two follow-up consultations (FCs) were interviewed. Depending on patients’ mobility or preference, interviews were conducted on site at the CCCs (5%), by telephone (55%) or videoconference (40%). In two cases, the participants’ spouses attended the interview due to the participants’ hearing loss or speech problems.
Before each interview, the research objectives and the interview process were explained, and oral consent for the audio-recording was obtained. Participants had the opportunity to ask questions and were encouraged to share both positive and negative experiences with the CIH counseling intervention. The problem-centered interviews were conducted using a semi-structured interview guide with the option to adjust the questions’ sequence flexibly to avoid interrupting the participants’ narrative flow. The interview guide encompassed several key topics, including participants’ prior experience with CIH approaches, their reasons for participating in the counseling program, their experiences during the counseling sessions, and their perspectives on the interprofessional counseling approach. Furthermore, participants were asked about the implementation of the CIH recommendations in their daily lives, the supplementary information materials they received, their level of health literacy, and patient activation. The guide also aimed to identify personal benefits participants derived from the counseling intervention, any suggestions they had for improvement of the counseling, and whether there were any unmet expectations regarding the counseling program.
The interviews lasted between 25 and 60 min, averaging 44 min. Following each interview, the researcher (HD) took field notes documenting the interview process, including the atmosphere, the main topics discussed, and any notable observations made. After 35 interviews, no new categories emerged, signifying data saturation. All interviews were audio-recorded and transcribed verbatim. Transcripts were pseudonymized by removing all identifying content. The transcripts and findings were not presented to participants for comment or correction for logistical reasons.
Ethical Considerations
The study was planned and carried out following the principles of the Declaration of Helsinki and the European Data Protection Law. Ethical approval for the process evaluation was granted by the Medical Faculty of Heidelberg Ethics Committee, No. S-307/2020, on November 24, 2020. Considering the potentially emotional nature of the interviews, participants were assured that their information would be treated confidentially and that consent could be withdrawn at any time without compromising medical care. The interviewer’s psychological background proved beneficial in assessing the participants’ psychological distress. It was possible to immediately refer to the counseling teams and initiate appropriate psychological support if necessary.
Analysis
MAXQDA Analytics Pro 2022 was used to prepare the pseudonymized transcripts and conduct the computer-based analysis (VERBI Software, 2021). MAXQDA is a software that supports transcription and analysis of audio- and video-recordings, interviews, literature reviews, content analyses, and mixed-methods analyses and can be used to create notes, case summaries, concept maps, and reports of scientific projects and studies. A deductive–inductive content analysis was carried out, adhering to the methodology outlined by Kuckartz and Rädiker (2019). In the initial phase (initiating text work), the first author familiarized herself with the material by writing memos and case summaries, incorporating the field notes into this process. Based on the interview guide’s topics, the domains of the CFIR (Damschroder et al., 2009), and the initiating text work, a preliminary deductive–inductive category system was developed. HD and UB first consensually coded 10% (four interviews) of the material. The MAXQDA function intercoder-agreement was used to check whether the encodings of the two authors matched at the segment level. The codings were considered to match if the overlapping range of two codings reached 95%. After adjusting the segment boundaries (co-coding of speaker labels and nonverbal aspects), the intercoder-agreement exceeded 70%—the intercoder-agreement analysis aimed to uncover ambiguities in the coding instructions and improve the coding system. Figure 1 depicts a schematic representation of the final coding system, which includes the main categories and their corresponding subcategories. Category system: patients’ perception of the interprofessional counseling program on complementary and integrative healthcare.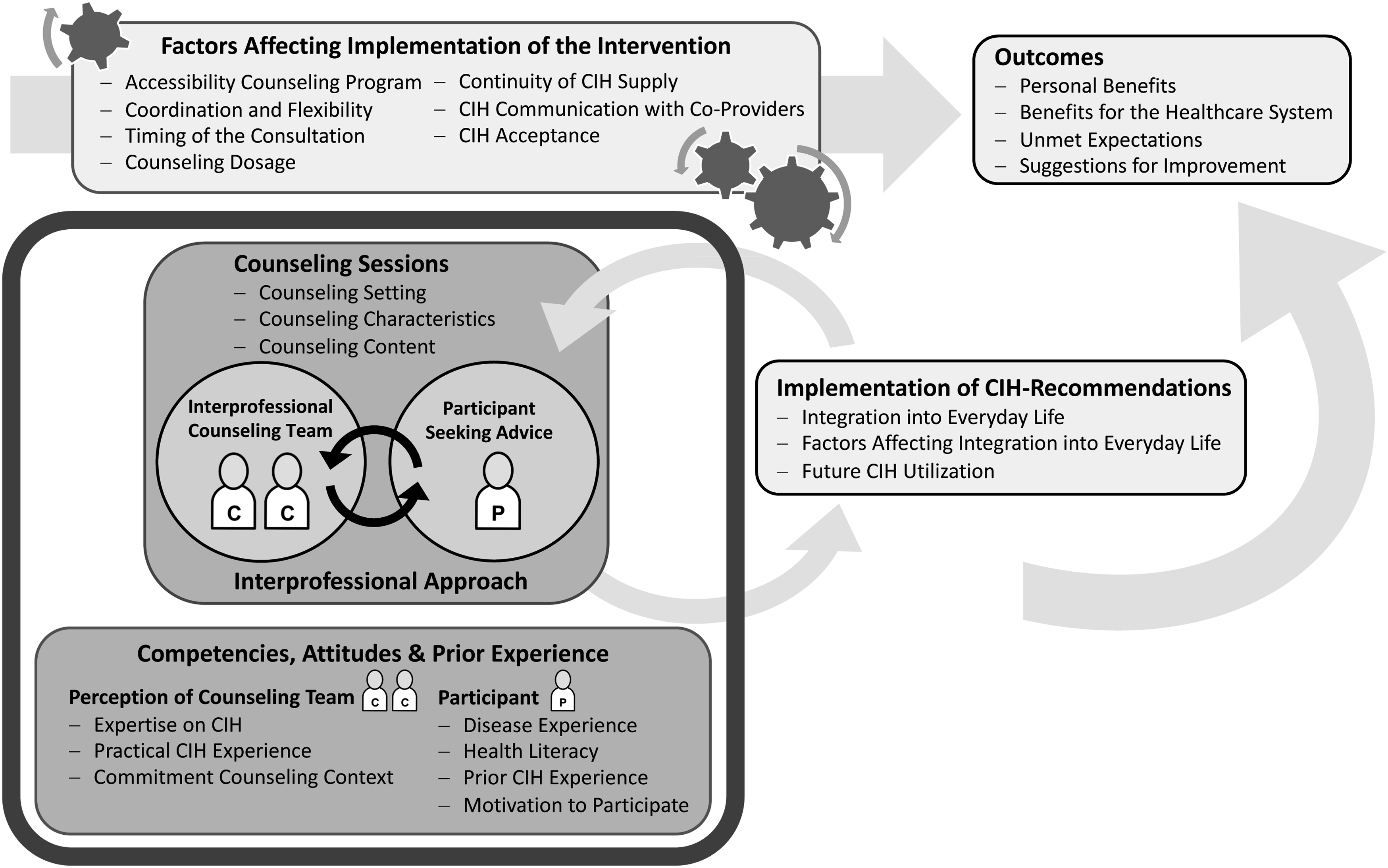
Patients’ quotes were translated from German into English and are presented along with participants’ pseudonyms to highlight the findings in this article.
Reflexivity and Trustworthiness
Reflexivity incorporates the personal, interpersonal, methodological, and contextual factors of the research process, facilitating the delineation of one’s subjectivity and specific measures to address the potential influence of the researcher’s position and perspective (Olmos-Vega et al., 2023). The process evaluation team comprised researchers with diverse backgrounds in health services research, implementation science, psychology, medicine, and nursing science. They have extensive experience conducting mixed-methods process evaluations within the context of CIH and utilizing the CFIR framework (Klafke et al., 2017). None of these researchers were directly involved in delivering the counseling intervention, which facilitated the reduction of potential bias and an impartial perspective (Holmes, 2020).
The first author (HD), who played a crucial role in data collection, processing, and analysis, is a medical doctoral student with a bachelor’s degree in psychology. Her psychology background provided her with experience conducting interviews and engaging empathetically with patients. The second author (UB) has a background in nursing science, possesses experience with qualitative patient interviews, and was involved in designing and evaluating the blended learning training program for the counselors; she had no connection to the participating patients. The other researchers involved in the process evaluation were not involved in conducting the patient interviews either. Interpretation of the results was guided by the researchers’ prior knowledge and theoretical assumptions, emphasizing openness to new aspects in the spirit of inductive analysis. In addition, all team members reflected on the findings from their own professional angles; the multidisciplinarity thus allowed for a differentiated view of the data from various perspectives, including healthcare providers, the healthcare system, and the psychological aspects of healthcare. Furthermore, the researchers reflected on their own positions and considered how these might influence the findings.
Attention was paid to the criteria of credibility, transferability, reliability, and confirmability to ensure the high quality of the study, and a detailed description of the study objectives, study context, recruitment process, and data analysis was provided. The transcription of the interviews was primarily conducted by the same author (HD) who conducted the interviews, enhancing reliability, particularly for statements that were challenging to understand on the audio-recordings. Illustrating the results with quotes from the interviews contributes to increasing trustworthiness (Cope, 2014). All aspects of the research process were discussed in regular interdisciplinary meetings. The interprofessional collaboration and mutual exchange allowed for a critical review of the research findings and the generation of new insights. This ensured a valid and reliable understanding of the research findings. After several rounds of discussion of the data, the authors concluded that the present interpretation is the most trustworthy understanding of the data, although alternative interpretations were considered. Nevertheless, it must be acknowledged that combining different data sources (e.g., focus groups and quantitative data from questionnaires) from the other process evaluation studies could contribute to a more comprehensive exploration of the study’s purpose, and thus, the conclusions might be further extended (Cope, 2014). All research team members commented and accepted the following draft of the report.
Findings
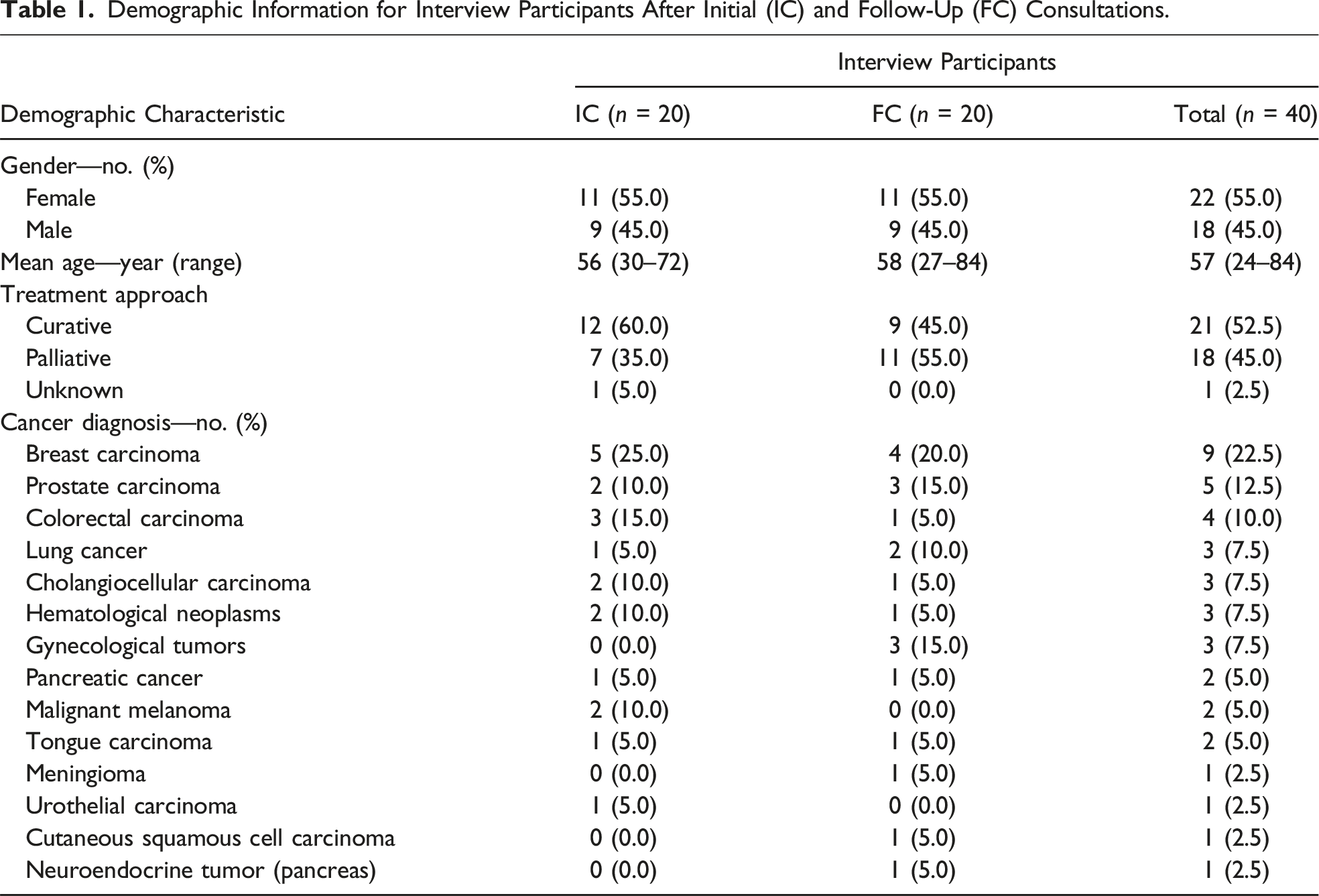
Demographic Information for Interview Participants After Initial (IC) and Follow-Up (FC) Consultations.
Participants’ Prior Experience With Healthcare Utilization and Complementary and Integrative Healthcare (CIH) Approaches.
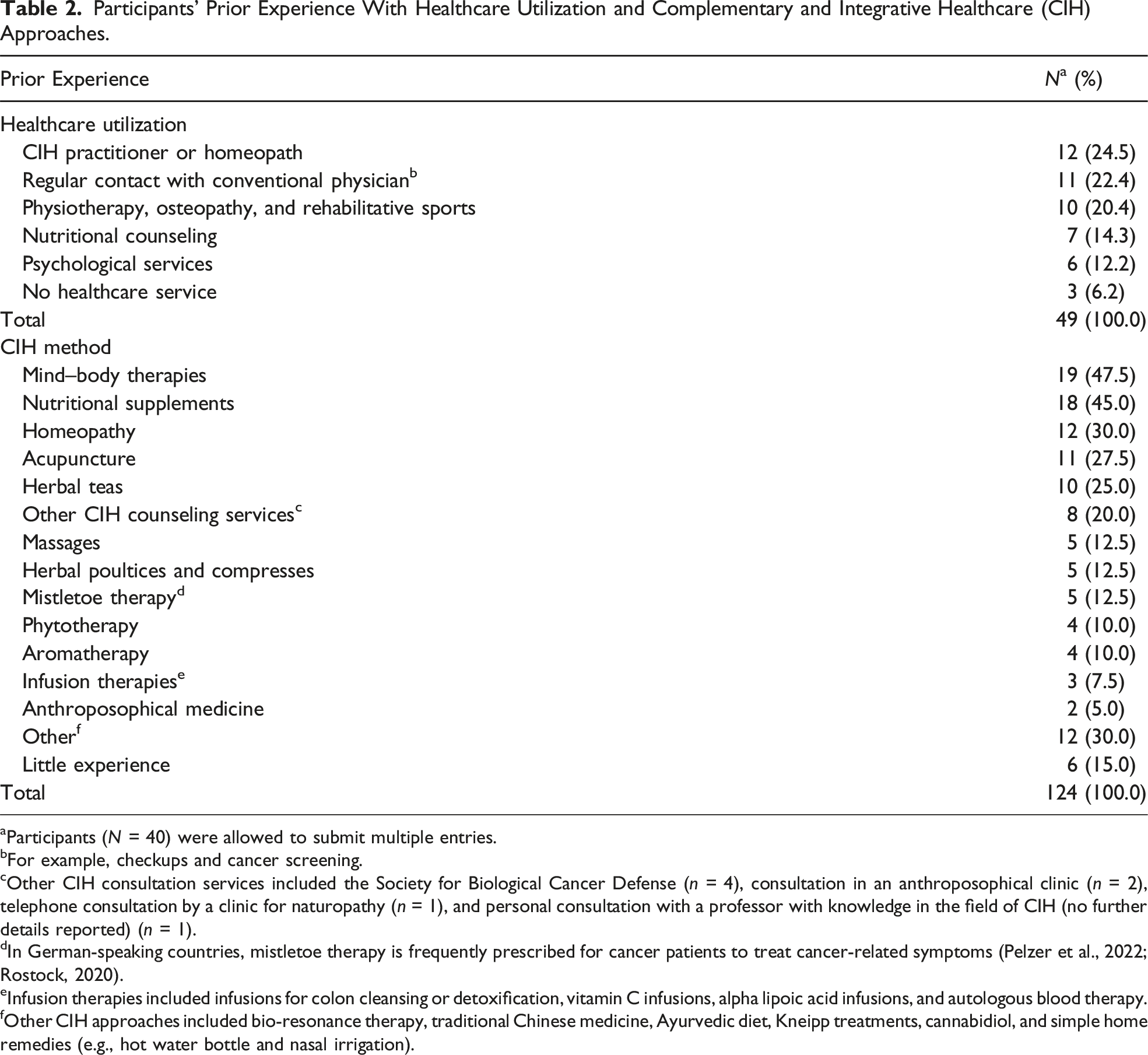
aParticipants (N = 40) were allowed to submit multiple entries.
bFor example, checkups and cancer screening.
cOther CIH consultation services included the Society for Biological Cancer Defense (n = 4), consultation in an anthroposophical clinic (n = 2), telephone consultation by a clinic for naturopathy (n = 1), and personal consultation with a professor with knowledge in the field of CIH (no further details reported) (n = 1).
dIn German-speaking countries, mistletoe therapy is frequently prescribed for cancer patients to treat cancer-related symptoms (Pelzer et al., 2022; Rostock, 2020).
eInfusion therapies included infusions for colon cleansing or detoxification, vitamin C infusions, alpha lipoic acid infusions, and autologous blood therapy.
fOther CIH approaches included bio-resonance therapy, traditional Chinese medicine, Ayurvedic diet, Kneipp treatments, cannabidiol, and simple home remedies (e.g., hot water bottle and nasal irrigation).
Counseling Setting of Initial (IC) and Follow-Up (FC) Consultations.
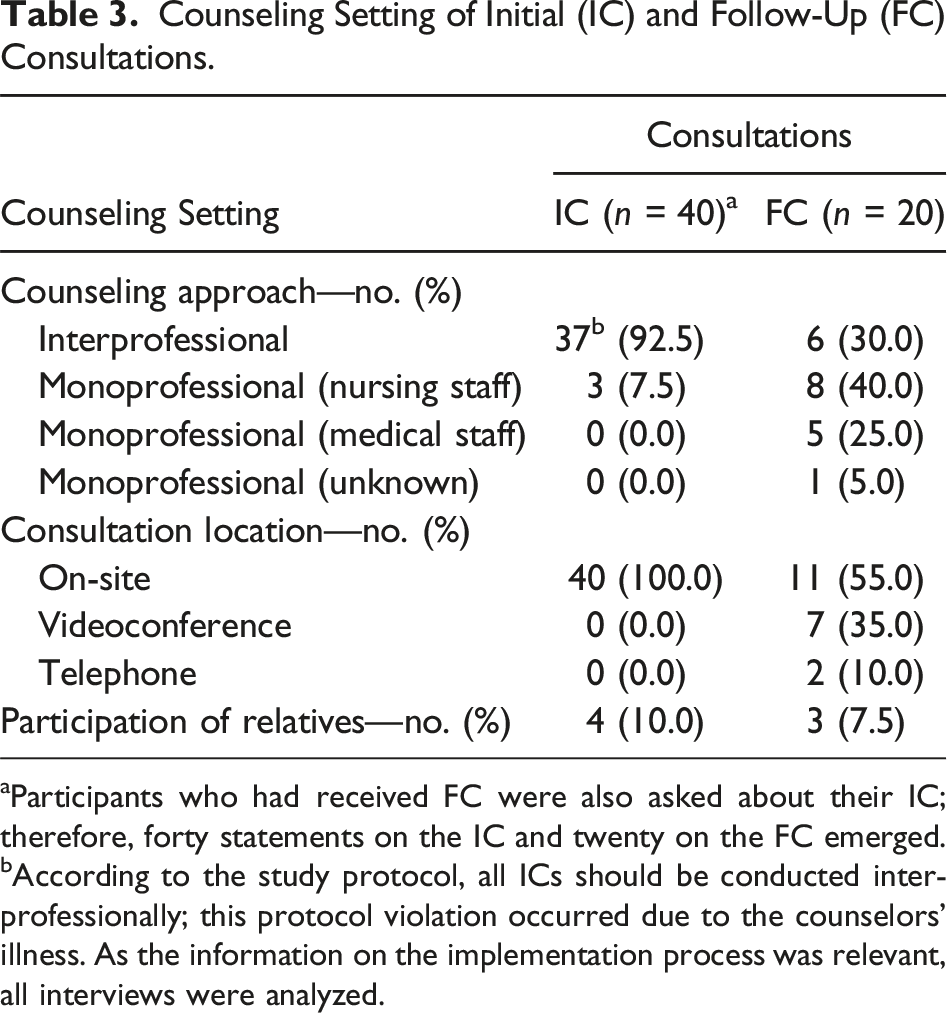
aParticipants who had received FC were also asked about their IC; therefore, forty statements on the IC and twenty on the FC emerged.
bAccording to the study protocol, all ICs should be conducted interprofessionally; this protocol violation occurred due to the counselors’ illness. As the information on the implementation process was relevant, all interviews were analyzed.
Qualitative data analysis resulted in six main categories: (1) Competencies, attitudes, and prior experience of individuals; (2) Counseling sessions; (3) Interprofessional approach; (4) Factors affecting the implementation of the intervention; (5) Implementation of the CIH recommendations; and (6) Outcomes. This article reports on the results of categories 1–3 (for improved clarity, the defined category system with anchor citations can be found in Appendix 2).
Competencies, Attitudes, and Prior Experience
Participants’ attitudes and prior experience relevant to the counseling context included their disease experience, health literacy, prior experience with CIH approaches, and motivation to participate in the study. Related to the disease experience, some participants described a significant psychological burden, particularly in the case of advanced disease, extended disease history, or young age, although not exclusively limited to these conditions. Furthermore, some participants described unfavorable encounters with the healthcare system, such as their concerns not being earnestly considered or insufficient time allocated to address their supportive needs as part of their overall disease history. One patient (female, 57 years) expressed the expectation of receiving thorough medical care, encompassing the management of side effects, during chemotherapy. Nonetheless, she conveyed a sense of having to “constantly actively approach the doctor and ask for an appointment” to ensure her concerns were acknowledged, which she perceived as frustrating (R 20).
Regarding health literacy, defined as an individual’s access to health information and the ability to understand and use it effectively (Institute of Medicine, 2004), participants indicated a strong interest in health-related topics. Their main sources of health-related information were relatives, friends, colleagues, the Internet, and physician consultations. Half of the participants reported using these sources of information to focus on a healthy lifestyle, such as following a nutritious diet or exercising regularly, to maintain good health.
Furthermore, most participants reported prior experience with CIH applications, often in alignment with this objective, and many indicated that they had tried several complementary treatments. As an example, one participant (male, 54 years) recounted favorable experiences with acupuncture in managing “stressful situations or instances of physical tension or tightness, […] or for addressing back pain” (R 7). Another participant (female, 57 years) shared her practice of using liver compresses or cabbage compresses to “relax the abdomen a little,” a method she found to be “very helpful” (R 20). Only a few participants stated that they had no prior experience with CIH applications, although many of them also indicated to follow a health-conscious lifestyle.
The most frequently cited motivation for participants to enroll in the counseling program was their desire for more information on CIH. They hoped to receive information on symptom management and tumor control. However, more nonspecific concerns were also mentioned, such as learning about options beyond conventional medicine, as the following quote demonstrates: “I was just interested to know what other options they [the counselors] know—what else can be done outside of traditional conventional medicine” (R 15; female, 36 years).
Additionally, some participants stated that they had enrolled in the counseling program to receive feedback from conventional healthcare professionals regarding the impact of the previously employed CIH methods, diet, and lifestyle on their health, considering the cancer diagnosis. Furthermore, apart from their CIH information needs, participants cited a desire to support research and emotional needs as motivation to participate. Emotional needs included the need for control, the desire to have someone to talk to about problems associated with the disease and therapy, and support in dealing with the diagnosis. Four participants indicated a general interest but no concrete expectations of the consultation.
Many participants regarded the counselors’ professional competence in CIH as high. One participant (female, 61 years) described her experience in comparison with another consultation on CIH, in which she received recommendations from which she suffered side effects. She perceived that the counselors of the CCC-Integrativ study “have much more knowledge, and […] could point out the error […], they have a more profound knowledge than many who call themselves naturopaths” (R 22).
In addition to theoretical expertise, participants cited practical experiences with CIH applications as an essential characteristic of the counselors. One participant (male, 68 years) expressed concerns that the professional training of the counseling teams may not be sufficient for the intervention’s purpose, pointing out that CIH is sometimes referred to as “experience medicine” and, therefore, counseling on CIH requires “a lot of experience to grasp everything—and […] to be able to pass it on” (R 4).
In contrast, another participant (female, 52 years) welcomed the practical recommendations and the counselors’ assessment of what frequency was realistic in applying the CIH recommendations: That was actually a good hint from the nurse because, with the yarrow poultice, she said that I should first make sure I can do it twice a week before I overwhelm myself. And that was a very realistic assessment. Twice a week, even though I am still at home. (R 25)
Another characteristic of the counseling team frequently cited was their commitment to the counseling process and willingness to provide support beyond the counseling session. Participants indicated that some counselors invested significant effort in conducting the counseling sessions and creating a pleasant atmosphere. Furthermore, participants provided positive feedback when the counseling team conducted further research on specific CIH applications and shared this information through email, in the counseling letter, or in FC sessions. Additionally, participants recognized the counselors’ thorough examination of their medical histories and efforts to collaborate with their treating physicians regarding symptom management.
Counseling Sessions
This category incorporates the counseling content and characteristics as described by the participants. The counseling characteristics consist of three subthemes: the interaction between participants and counselors, the specification of CIH recommendations, and the scope of the counseling sessions.
According to participants, the counseling content focused on discussing treatment- and disease-related symptoms and appropriate CIH applications for symptom control (e.g., herbal poultice application in the heart area to alleviate anxieties and agitation, and acupressure against nausea). In addition, general information was provided on CIH principles, nutritional and lifestyle recommendations, and psychosocial support. Participants indicated that in some consultations, conventional healthcare also played a role. For example, conventional healthcare treatment options or the dosage of medications was discussed in the context of pain. The participants reported that the consultants sought feedback on implementing the recommended CIH applications during FCs. Based on this feedback, the applications were adapted, deepened, or expanded if necessary. Some participants indicated that they received direct points of contact for CIH treatments. They were referred to university services such as psycho-oncology or given information about external providers of yoga courses or mistletoe therapy. Nevertheless, as shown in the following quote, certain participants noted that they would have liked more information about trustworthy and competent CIH providers. The how and who is indeed an issue. I notice it with mistletoe therapy: I have asked here in my environment, also my physiotherapist, if anyone knows someone who could guide and support me now with mistletoe therapy, but no one has come up who has a medical background. There are alternative practitioners, of course, but that’s not what I want. (R 25; female, 52 years)
In six cases, participants’ relatives attended the counseling sessions. These participants often mentioned that their relatives were already knowledgeable about naturopathy and claimed to have benefited from their support. As a result, the participants’ relatives played an active role in the counseling context by asking questions and taking notes. A female participant (30 years) stated that the attendance of relatives could increase acceptance of CIH recommendations: Maybe you can also recommend other people to take their relatives with them because, especially regarding nutrition, it usually affects the entire household and not just the patient alone. My boyfriend just happened to accompany me [...] However, upon reflection, I found it [his presence] very helpful so that [...] the other person also understands the background [...]. And with my boyfriend, it also helped that there was a doctor and a nurse, and they told him and not me because I googled it. (R 17)
Regarding the counseling characteristics, participants described the interaction with the counseling team as patient-centered. They felt understood, appreciated, and attentively heard, with ample opportunity to express their needs and concerns. Apparently, this type of interaction is not always present in medical encounters, as demonstrated by the following quote: What I found very positive was that the two of them first listened, took a proper medical history, really questioned me in detail, and first got a general impression of how I am doing; what therapies I have had; what I already know. And this helped to build up my confidence. […] Not one doctor over the whole years has taken as much time for me as these two did… (R 25; female, 52 years)
In the context of specifying CIH recommendations, participants expressed positive feedback when the counselors demonstrated or practiced treatments together with them, such as preparing wraps or breathing exercises. A female participant (27 years) stated that she “really liked that, when it came to relaxation, [she] was not only recommended a relaxation method but that [they] also practiced it briefly, i.e., applied it practically” (R 24).
In most cases, participants perceived the framework and content of the consultation to be sufficient and that all their issues were addressed. However, in some cases, there was a need for additional information, such as specific, practical guidelines, details on how the treatments work, or assistance in obtaining the necessary materials. This is evident from the following quote: I would have liked more explanation, although I don’t know if that would be beyond the scope of the consultation. For aromatherapy, for example, I did not get much of a scientific explanation, but I was very convinced about it afterward when I used it. The explanation was obviously enough to try it. However, with the overlay, I was a little frustrated, lying [there] thinking, “What is that all about?” >laugh< Because I did not understand it. (R 17; female, 30 years)
Interprofessional Approach
Most participants perceived the interprofessional counseling approach as beneficial. Some participants reported that the counseling team was divided thematically, with the nursing staff often providing practical advice on CIH applications such as aromatherapy or compress preparation. In contrast, medical staff focused on theoretical content and pointed out potential benefits and risks of CIH approaches, including interactions and side effects of dietary supplements with cancer therapy. Collaboration between physicians and nurses was perceived to be “harmonious,” with one participant (male, 74 years) even describing that he “almost did not notice who was the doctor and who was the nurse.” He stated that “the two harmonized very well with each other.” He perceived it as a “togetherness, a conversation between all three of us, where you did not notice any hierarchical order,” which was “very positive” (R 36).
Mutual exchange and complementing of different perspectives were identified as the main advantages of interprofessional counseling, enabling a holistic approach. The presence and expertise of medical staff provided a sense of security, while the nursing staff could communicate and deal with participants more efficiently: For me, it was okay—an even more secure feeling because there was someone there who knew about the complementary approach and then also a doctor who confirmed from a conventional medical point of view that this is good or could help. That is not a matter of course for every doctor […] Sometimes it is also smiled at ... this complementary approach. (R 28; female, 64 years)
Moreover, participants indicated that interprofessional counseling could promote mutual understanding between the different disciplines. A 54-year-old participant described the approach as “very complementary.” He believes that “it ultimately also develops a mutual understanding—from nurses to doctors and doctors to nurses,” which he perceived to be “a good thing” (R 7).
However, when participants were asked about their preference for the FC, some noted that an interprofessional approach might be critical, particularly for complex problems or serious illnesses. In contrast, a monoprofessional FC might suffice for simple issues. Therefore, one participant (female, 52 years) suggested discussing with patients beforehand whether they would prefer an interprofessional or monoprofessional consultation: I think it would be a good idea—to consider when this interprofessional approach makes sense. Before the consultations, it should be discussed again […] It does not have to be that it is necessary, as you can see in my case. However, it can also be the other way around that someone comes with a severe medical history, and it would be good if both [nursing and medical staff] were present. And you might clarify in advance whether the interprofessional approach is necessary. (R 25)
Discussion
This study examined cancer patients’ perceptions of a newly implemented interprofessional CIH intervention focused on patient-centeredness and patient activation. Content analysis of the interviews revealed that participants perceived the interprofessional counseling team to address their health and CIH information needs. They highly valued the collaborative exchange and integration of perspectives from various health professions. However, a few participants desired more specific information regarding recommended CIH measures and reliable CIH providers. They expressed an interest in the practical implementation of applications such as mind–body practices, wraps, and compresses as part of the program rather than just receiving counseling.
Participants’ Attitude and Motivation to Participate in CIH Counseling
In line with pre-existing literature (Lopez et al., 2017), our findings indicate that many patients in the CIH counseling program had prior experience with CIH approaches, such as consulting homeopaths and emphasizing a healthy lifestyle. Hence, their primary incentive for enrolling in the counseling program was expanding their knowledge of CIH, developing an integrative approach to their treatment, and receiving personalized information tailored to their individual needs and preferences. Interestingly, participants with limited CIH experience demonstrated similar concerns and motivation as those with extensive prior knowledge. However, these participants appeared unable to articulate specific issues related to CIH; instead, they expressed a general interest in the emerging field of health and self-care, suggesting an even greater need for further guidance. CIH counseling teams might consider the different prior experience of patients diagnosed with cancer when counseling about CIH and, accordingly, provide more general information about the principles of CIH. For patients with considerable prior experience, feedback on previously used CIH applications could be more relevant.
A study of the association between CIH use and unmet needs among cancer patients discovered that patients consult CIH practitioners to address unmet needs related to information and communication with physicians, symptom control, and psycho-emotional support (Bonacchi et al., 2015). Compared to conventional healthcare providers, CIH practitioners often devote more time and attention to communication, allowing patients to ask questions, express their concerns, and be emotionally understood (Bonacchi et al., 2015). Similarly, in the present study, participants expressed the desire for more information on CIH and emotional needs as a driving motivation for their participation in the counseling program. The participants valued the patient-centered communication with the counselors, their commitment, and the generous time frame of the counseling sessions, especially since some patients reported contrasting experiences within the healthcare system in their previous disease history. These findings are consistent with a systematic review that indicates patients perceive interactions with healthcare professionals positively when the approach is person-centered and healthcare professionals possess good interpersonal skills (Collet et al., 2022).
Individually Tailored Counseling Sessions
Participants in the current study perceived the specially trained counseling teams as competent and knowledgeable about CIH and evidence-based databases related to CIH applications. As participants’ information needs were sometimes specific and other times more general, counseling sessions focused on cancer- and treatment-related symptoms and CIH recommendations for symptom control. However, other topics were also discussed, as inquiries about CIH treatment methods are often associated with needs related to the broader disease experience (Horneber et al., 2018). Accordingly, professional counseling on CIH treatment should be tailored to patients’ individual needs, include balanced information about risks and benefits, and consider conventional treatment options. Additionally, it is advisable to provide nutrition and exercise recommendations and consider psychosocial aspects (Blödt et al., 2016; Horneber et al., 2018).
Furthermore, participants highly valued the exceptional dedication and engagement of the counselors in the counseling context. The counselors’ practical experience with the application of CIH measures was also considered a crucial aspect. Nevertheless, participants in our study expressed a desire for even more information or references to credible providers of CIH applications. Consequently, it is important to consider how this concern can be addressed more effectively in the future. In Germany, the medical professional code of conduct allows referrals to colleagues, and accordingly to reliable CIH providers, only in sufficiently justified cases to maintain professional neutrality (German Medical Association (Bundesärztekammer), 2021). Therefore, addressing the participants’ desire for more information or references would require a suitable compromise.
Some participants noted that they perceived their relatives’ participation in counseling as supportive. Klafke et al. (2014) have shown that men experience active support from their partners when using and maintaining CIH measures. Therefore, some researchers recommend involving relatives in counseling on CIH to achieve realistic patient expectations of risks and benefits and to avoid potential adverse effects (Horneber et al., 2018; Klafke et al., 2014). Our findings supplement these recommendations, indicating that involving family members may enhance the acceptability of CIH approaches and facilitate their application at home.
Interprofessional Counseling Approach
Given the patient-centered approach and increasing complexity of cancer care, interprofessional teams are necessary for optimal care coordination and patient communication (Knoop et al., 2017; Kurniasih et al., 2022; Prades et al., 2015). Nevertheless, a review of physician–patient consultations in oncology (Bossert, Korus et al., 2022) has shown that, to date, consultations have predominantly been monoprofessional. The CCC-Integrativ study is the first intervention project with an interprofessional counseling approach, offering CIH care and treatment for all patients with a cancer diagnosis. Participants in our study reported benefiting from the interprofessional approach and noted the considerable advantage of healthcare professions working together. They stated that the presence of medical staff gave them confidence in the safety of CIH recommendations, as they received reliable information about the risks and benefits of CIH applications in the context of conventional cancer therapy. Previous studies have shown that patients are more willing to share their opinions and talk openly with physicians about CIH when they receive evidence-based information about CIH treatments from trained oncologists (Bozza et al., 2018). In addition, participants in our study reported feeling understood by the nursing staff, who possessed a more profound comprehension of their personal needs. These results support findings that trained nurses play a critical role as members of an interprofessional team since they may possess the ability to comprehend patients’ needs better, effectively assess symptoms, and identify appropriate CIH interventions (Cook et al., 2015; Rojas-Cooley & Grant, 2006).
Through joint consultations involving medical and nursing staff, patients receive trustworthy and comprehensive information regarding CIH, resulting in a sense that their personal needs are being addressed, which may ultimately enhance their overall well-being (Ben-Arye et al., 2015). In our study, participants perceived the interprofessional approach as beneficial during an IC. Especially if concerns are complex or the disease process is severe, patients tend to have higher counseling needs. Incorporating the perspectives of different professional groups and targeting their expertise may minimize suffering.
Limitations and Strengths
To our knowledge, this study is the first exploration of cancer patients’ encounters with an interprofessional CIH counseling program. To prevent confirmation bias, researchers accountable for the process evaluation were not involved in implementing the counseling intervention. By examining patients with diverse profiles from four CCCs, we acquired valuable insights regarding patients’ experiences and the factors that impact the counseling context. Nonetheless, it is crucial to recognize the constraints of this study. Firstly, it should be noted that patients with considerable prior experience in CIH and those with higher levels of health literacy and activation may have been more inclined to participate in the counseling program (Bravo et al., 2015), introducing a potential bias. In addition, there is a possibility that participants could not remember all aspects and details of the counseling program (recall bias). However, qualitative research is about subjectivity, that is, presenting subjective experiences in a way that not only reflects consistencies and parallels but also preserves the nuanced character of the data (Broom, 2005). Nevertheless, it is important to acknowledge that the experiences of the 18 patients who declined to participate due to reasons outlined in the Results section could not be investigated, raising the possibility of selection bias. However, patients with similar characteristics, such as poor health status and high symptom burden, also participated in the study.
Another limitation of the study is associated with the participants’ awareness of the distinctiveness of the interprofessional counseling approach employed. Such awareness may have introduced response bias, compromising the validity of the study results. In addition, the favorable perception of the interprofessional approach may have been influenced by the heightened attention generated through the presence of two health professionals simultaneously. However, the participants’ diverse perceptions regarding the benefits and necessity of the interprofessional approach in different situations indicate that factors beyond the study design influenced their views. This highlights the significance of considering multiple factors when evaluating interprofessional counseling programs and underscores the necessity for further research.
During data analysis and development of the category system, it became evident that adherence to the constructs of the CFIR was not always feasible due to its limited applicability to the patients’ perspective. According to Safaeinili et al. (2020), the CFIR does not encompass all pertinent dimensions necessary for examining patient-centered interventions, specifically in assessing patient needs, feedback, and satisfaction. In our study, we identified patient statements pertaining to the CFIR construct Outer setting and Characteristics of individuals. However, to comprehensively capture various dimensions of patients’ perceptions of the implementation of the counseling intervention, we classified these statements under a broader category named Competencies, Attitudes, and Prior Experience. In this regard, we used the CFIR primarily as a heuristic tool for developing the interview guide and facilitating the deductive–inductive data analysis. Nonetheless, when these findings are combined with those of the other process evaluation studies, it can be inferred that all domains of the CFIR will be addressed, leading to a comprehensive understanding of the implementation process of the counseling intervention.
Future Research and Clinical Implications
Future research on the implementation of CIH counseling approaches in standard clinical care should take an interdisciplinary approach to reap the benefits of patient-centered communication about CIH for holistic treatment. The findings of this study highlight the need to explore further the indicated and possibly additional factors that impact the implementation of innovative CIH counseling approaches to optimize patient care. In this regard, attention should be paid to individual patient-related factors and special patients’ unmet needs when counseling on CIH for symptom management. The present study has shown the potential influence of the interpersonal context on the implementation process of CIH counseling interventions. Therefore, future efforts to implement CIH counseling services should build on these findings and consider interprofessional counseling, early integration of family members, and the implementation of supportive structures such as patient education programs to maximize the effectiveness of these approaches.
Conclusions
As part of the process evaluation, insights into patients’ perceptions can contribute to a better understanding of barriers and facilitators to implementation and help to tailor the intervention to patients’ health needs. In addition, the results of this study may inform the implementation of future interventions of this type. Based on our results, we recommend considering the following when conducting CIH counseling interventions for cancer patients: counseling on CIH approaches needs to be patient-centered, include concrete information on the practical application of CIH treatments, and provide recommendations for trustworthy CIH providers. The participation of relatives in the consultation may increase the acceptance of CIH and support patients in integrating CIH applications into everyday life. Interprofessional counseling teams trained in utilizing CIH treatments and employing patient-centered communication techniques facilitate discussion and acceptance of CIH. The main advantage of this approach is that the professions complement each other, resulting in a more comprehensive and holistic treatment approach. If there are multiple consultations, discussing with patients whether an interprofessional approach is appropriate in a follow-up consultation should be considered. This may be indicated in cases of high symptom burden or psychological distress.
Supplemental Material
Supplemental Material - A Qualitative Analysis of Cancer Patients’ Perceptions of an Interprofessional Counseling Service on Complementary and Integrative Healthcare
Supplemental Material for A Qualitative Analysis of Cancer Patients’ Perceptions of an Interprofessional Counseling Service on Complementary and Integrative Healthcare by Helena Dürsch, Ursula Boltenhagen, Cornelia Mahler, Stephanie Joos, Joachim Szecsenyi, and Nadja Klafke in Qualitative Health Research
Footnotes
Acknowledgments
The authors would like to thank all staff members, patients who participated in the CCC-Integrativ study, and those who participated in the process evaluation. Furthermore, the authors want to thank Lea Gölz and Leonie Horn for their support in developing the category system.
Author Contributions
NK and HD conceived and designed the study. HD collected and processed the data, and HD and UB coded the data. HD analyzed the data in terms of thematic interpretation and wrote the first draft of this paper, and NK critically revised it. CM, SJ, HD, NK, and UB discussed the data, coding system, and thematic interpretation. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study is part of the process evaluation of the project CCC-Integrativ, which is supported by the Innovationsfonds of the Federal Joint Committee Berlin 2019–2022 (funding years: October 2019–March 2023)—grant number: 01NVF18004. The study’s funder does not influence the study design, data collection, analysis, interpretation, or manuscript writing. Since this is a government grant, there is no commercial interest.
Ethical Statement
Data Availability Statement
The data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.