
Abstract
Cancer of the head and neck is a confronting condition, as the disease and its treatments alter the appearance and function of body organs associated with physical appearance and identity. Many of the risk factors for head and neck cancers, including tobacco, alcohol, and human papilloma virus, can also have significant negative social and moral permutations. Language and action (discourse) plays an important role in constructing disease and illness and shape the way it is managed, both institutionally and socially. This research used a critical constructionist lens to investigate how the common discourses surrounding head and neck cancer are constructed within the healthcare context and how this influences patients and healthcare professionals’ responses to the illness. Data were collected through semi-structured interviews, field noting, journaling and literature reviews. Analysis was guided by a three-dimensional approach to critical discourse analysis that investigated text, discursive practices, and social context. The overarching finding was that deviance dominates the common discourse and shapes head and neck cancer and responses to it. Deviance is channelled through metaphors, adjectives, descriptors, and collective nouns and is made overt through labelling, avoidance, blaming, shame, and categorization. Discourse is contextualized by a sociocultural understanding that when someone deviates from what is perceived as normal, they are devalued. Open dialogue and reflection on head and neck cancer discourse could enable better understanding of how people experience their condition and inform more supportive responses.
Background
Cancer of the head and neck, particularly of the mouth and throat, is a confronting condition. The disease and its treatments often alter the appearance and function of body organs associated with physical appearance and identity. It also profoundly affects a person’s ability to engage with important social rituals associated with communicating, eating, and drinking. This is because cancers of this region require challenging multimodal treatment. The particular stressors associated with both the principal diagnosis and the side effects of treatment include body image concerns (Bennion & Molassiotis, 2013; Costa et al., 2014; Ellis et al., 2019; Qualizza et al., 2018) impaired taste (McLaughlin & Mahon, 2014) loss of speech, and respiratory and nutritional alterations (Bressan et al., 2017; Ehrsson et al., 2015). All these changes can challenge self-esteem and self-identity, percolating into many aspects of everyday life long after the initial cancer has been treated (Fillion et al., 2009; Fitchett et al., 2018; Threader & McCormack, 2016). Furthermore, it can lead to anxiety, depression (Suzuki et al., 2016), and feelings of disgust and embarrassment (Azlan et al., 2017a, 2017b; Powell et al., 2016; Reynolds et al., 2014).
Studies exploring the effects of other cancers with obvious physical changes (e.g., breast cancer) indicate that physical alterations such as a mastectomy and hair loss from chemotherapy are confronting changes that influence women’s quality of life (QoL) (Bu et al., 2023) and sense of self and are leveraged by the media to create fear (Lantz & Booth, 1998; Thorne & Murray, 2000). Further to this, people with cancer and their carers can experience a disgust response in relation to many cancer-related phenomena including surgical disfigurement, in cancers such as head and neck cancer (HNC) and sarcoma, the presence of a stoma in bowel cancer, and artificial feeding techniques (Azlan et al., 2017a; Powell et al., 2015). These physical changes, along with the responses of other people, can lead to embarrassment and ultimately social exclusion, delayed health-seeking behaviours (Reynolds et al., 2016), and mental health issues (Azlan et al., 2017a; Powell et al., 2015, 2016).
A person’s sense of self is linked to appearance, and is vital to their function in society, with beauty, symmetry, and effective facial function considered desirable (Turner, 2008). Disfigurement in the form of distorted facial features that can occur in HNC can dramatically affect how attractive or unattractive someone appears to others, leading to a repellent reaction and social disqualification or exclusion (Jones et al., 1984). An attribute that discredits an individual and devalues their social identity has historically been defined as ‘stigma’ (Goffman, 1963). Stigma is an umbrella term embracing numerous negative constructs such as labelling, stereotyping, cognitive separation and discrimination (Link & Phelan, 2001). The social construction of stigma can be seen as a collective reaction to a person’s physical, behavioural, or genetic deviance from an accepted norm (Goffman, 1963; Jones et al., 1984). Society’s view of normality is objective and homogenised and reflects someone or something that is socially, morally, and biologically desirable (Canguilhem, 1989; Rose, 2009; Tengelin et al., 2020). Health is often constructed as the normal state and diseases such as cancer are seen as a deviation of this norm (Conrad & Barker, 2010), which are therefore susceptible to stigma.
Previous studies indicate that HNC is susceptible to both felt and enacted stigma (Bonanno & Esmaeli, 2012; Costa et al., 2014; Daley et al., 2010; Dodd et al., 2016, 2019; Graboyes et al., 2019; Lebel & Devins, 2008; Lebel et al., 2013; Threader & McCormack, 2016; Yang & Pittman, 2017). Scrambler and Hopkins (1990) distinguished between “felt” and “enacted” stigma by defining felt stigma as the fear of being singled out or rejected for a physical or behavioural attribute related to the stereotypes that surround the mark in society. In contrast, enacted stigma is the act of prejudice or discrimination that people experience solely based on their attribute’s social and cultural unacceptability (Scambler, 2004).
In the case of HNC, stigma is also influenced by its perceived deviant origin. A notable feature of HNC is its relationship to mostly modifiable lifestyle risk factors such as ingesting tobacco, drinking alcohol, and sexual practice (Cohen et al., 2018; Sivasithamparam et al., 2013). Risk and responsibility in relation to these behaviours are increasingly dominant discursive constructions of cancer in general (Gibson et al., 2017; Kerr et al., 2018; Willig, 2011) and there are often detrimental implications for any person diagnosed with a lifestyle-associated cancer (Bell, 2014; Chapple et al., 2004; Lebel & Devins, 2008; Lebel et al., 2013; Threader & McCormack, 2016). Individuals with these types of cancers can experience multifactorial levels of blame, guilt and shame if it is perceived that they have control over their illness or diagnosis (Chapple et al., 2004; Gibson et al., 2017; Threader & McCormack, 2016). These responses can be attributed to the violation of social expectations which govern and define desirable and responsible behaviours (Jagannathan & Juvva, 2016).
Despite significant social and cultural implications associated with HNC, there is little understanding of how HNC is constructed within a social and cultural context. The pervasive nature of language and other speech acts (known as discourse) play an important role in constructing disease and illness and shapes the way it is managed, both institutionally and socially (Penson et al., 2004; Sontag, 1989; Stolberg, 2014). The analysis of discourse is a way to operationalise the social constructionist paradigm by helping to interpret text in context and by examining and challenging the events that shape and are shaped by culture, knowledge, and power (Fairclough, 2003; Grbich, 1999). Studying discourse in a critical way also illuminates power structures that are embedded in the social, institutional, and political context of the treatment and experience of disease and illness and encourages new ways to think and speak about them.
The aims of this research were to critically explore how the social discourses surrounding HNC are constructed and how these discourses influence patients’ and healthcare professionals’ responses to the illness. It also aims to identify different ways to think, speak and act about HNC. This paper presents the first finding of a larger study.
Methods
This study used a critical constructionist approach to guide its data collection and analysis. Fairclough’s (1989, 1995) critical discourse analysis (CDA) methodology guided the exploration of the social constructions of HNC. Discourse analysis often relies on Social Constructionism’s theoretical premise that social reality is created by people under the constraints of pre-existing sociocultural beliefs and structures. This approach focuses on the dialectical relationship between humans and society (Berger & Luckmann, 1966; Bryde Christensen et al., 2023). CDA operationalised and expanded on the social constructionist underpinnings of this study of discourse using a critical lens to contest the ‘common stock of knowledge’ and to encourage social change. Specifically, CDA enabled a deeper understanding of how prevailing ideologies influence the experience of HNC from the perspective of both the patient and the healthcare professional. CDA also facilitated investigation of the way that language shapes health-related issues and, more broadly, examines how language shapes professionals’ and lay-persons’ perceptions of health issues such as cancer and the practises that surround them (Smith, 2007).
Study Site
Australia’s healthcare system is a multifaceted mix of public and private providers. This study was conducted with participants from a major publicly funded tertiary referral hospital and its network in Queensland, Australia. This clinic saw approximately 600 people with HNC a year at the time of this study (Queensland Head and Neck Cancer Centre, 2015).
Participants and Recruitment
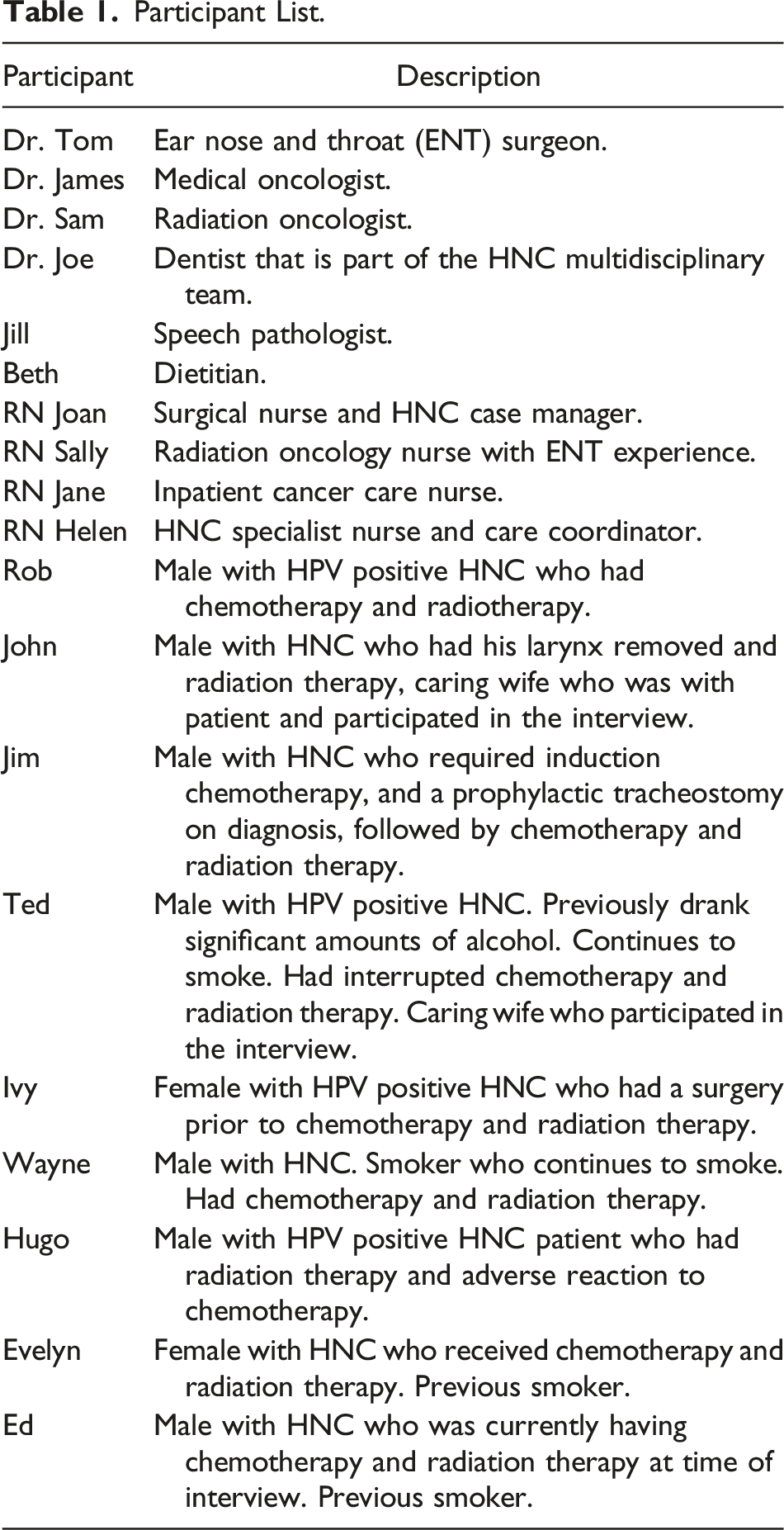
Participants included nine individuals with a diagnosis of non-metastatic mucosal squamous cell carcinoma (SCC) of the head and neck within the last two years. This ensured participants’ recollections of their cancer experience were current. Two participants living with HNC chose to have their partner present during the interview to assist with communication and recollection of events. Ten health care professionals, including medical, nursing, and allied health professionals who had more than two years’ experience working with people experiencing HNC also participated. Both participant groups were used to give different perspectives of HNC.
Participant List.
Ethical Considerations
Human research ethics approval was granted by the local health service and university ethics committees (no. HREC/12/QPAH/602 and 1300000181). Interviews were conducted by an experienced cancer nurse, who was able to deal with any emotional distress if it arose. For all interviews, participants were required to sign a consent form and were informed that all information would be de-identified using pseudonyms. They were also assured they would not be disadvantaged if they chose not to participate in the research. All raw data were stored, and password protected as per ethical guidelines.
Data Collection
Both written and spoken text were used as data in this study. Data included participant interviews, observational journaling, fieldnotes and historical and contemporary literature. The semi-structured interviews were conducted by CT. For critical constructionist studies such as this, observational field-noting and journaling directly post interviews applied another lens to data collection as a way to observe and record naturalistic structures that may not be captured through interviews alone (Chambers, 2003). Further to this, multiple literature reviews were performed iteratively throughout the study, these data sources added not only depth to the interview data but also gave context to social practices and norms and the dialectal relationship between discourses and society.
Undertaking this research as the Cancer Care Coordinator for people with HNC afforded CT an insider’s status when interacting with the participants. It also positioned her as a co-creator of knowledge in both the data collection and analysis phases of this research. For this reason, there was no presumption that the methods of data generation used, and the participants’ voices were a complete reflection of day-to-day practices but were rather a co-construction of both the participants’ and the researcher’s conceptualisation of HNC.
Analysis
Fairclough’s (1985, 1989, 1992a) three-dimensional model to was used to guide analysis and to show the complex and variable relationship between discourse and social practices. These dimensions include: text (written or oral); discursive practices (production and consumption of text); and, sociocultural practices (contextualisation of text and discursive practice) (Fairclough, 1989). Fairclough argues that if all three dimensions are addressed then there is no set formula as to how to present this study findings.
Interrogation of the interview data was commenced with in-depth reading and re-reading of the participant transcripts by CT. Interviews were listened to for nuances and summarised to help make early and ongoing conclusions. These early codes were supported by both contemporary and historical literature reviews to help develop themes and align with social practices and norms. Themes continued to be refined as interrogation continued by both CT and ALM through investigating dominant and resistant discourses and contradictory statements and their connections to, and influence over, HNC (Fairclough, 2009; Liamputtong & Ezzy, 2009; Wodak & Meyer, 2009). At this point, themes were aligned with the three dimensions of Fairclough’s CDA and concept maps were made and refined until the three interrelated themes were identified. Ongoing discussions with all authors throughout this process clarified thoughts and finalised the overarching findings, including deviance, institutional power structures and the agency of survivorship.
Findings
This first key finding in a larger study is that deviance dominates the discourse and shapes HNC and responses to it. Various sub-themes are also explored including the way that physical changes cause fear, disgust and embarrassment, but is a trade-off for being alive; felt and enacted stigma in relation to smoking, leads to blame; conflicting discourses about HPV leads to shame; and, assumptions and categorisation of people with HNC creates and is created by stigma.
‘A Human Monstrosity’: Physical Changes Cause Fear, Disgust and Embarrassment
Appearance is vital to our function in society, with beauty, symmetry, and effective facial function considered the desirable norm (Turner, 2008). Historically, the discourse relating to caring for people with HNC was that of fear and stigma mostly because of its poor prognosis, the fearsome reputation of tracheotomy, the often “stormy” recovery, and the debilitating and mutilating physical effects of surgery (Folz et al., 2008). These changes could not be hidden behind a waistcoat or corset, as in the case of other surgeries, such as that of the abdomen (Folz et al., 2008). The visual aspect of HNC was highlighted by the wife of a person living with a laryngectomy: I think, as they say … it’s one of the worst cancers you can get because it’s so life changing and it’s out there. It’s not something that you can have an operation and nobody else would know or the side effects. (John’s wife)
The aggressive, often brutal, nature of treatment for HNC is well documented. Early surgery consisted of a COMbined MANDibulectomy and Neck Dissection Operation, known as the “commando” or “military” surgery, and also named as the surgery reflects the manoeuvres of commandos during military operations, which address the opposition from two directions (McGurk & Goodger, 2000). Early radiation therapy was also referred to by one famous patient as “torture” and “crucifixion,” like “bayonets in his throat” (Folz et al., 2007). The confronting nature of contemporary treatment for HNC and its effects were well described by one of the nurses: Some of the surgeries I find horrific … a mandibulectomy where they take the whole jaw and they put a swinging jaw in. Sometimes they could get the bone out of the leg and reconstruct the jaw … I find glossectomies where they take a tongue is horrible, and I’ve had patients that have actually had hairy tongues because they didn’t bother to shave the area … Rhinectomies where they lose a nose … I remember when I first dressed one … “oh my God,” because you’re just looking into a person’s nose and there’s nothing there. You’re looking at their snot … and you can see them breathing. (RN Joan)
The side effects relating to these treatments can be life-changing and devastating. Both people with HNC and healthcare professionals described the responses to acute symptoms like pain, lethargy, sunburn, desquamation and feeding through a tube. … the external toxicities are wet desquamation of the neck skin which can be pretty awful … They’ve got pain on swallowing, and they’ve got this thick, mucus-y membrane they just want to cough up. I think it’s what turns off a lot of people is the constantly coughing, hacking, sick-looking patient ... (Dr. Bill)
From a chronic perspective, obvious disfigurements, and transmutation of anatomical structures for example … transposing duodenum [bowel] back into the pharynx to produce a conduit for swallowing (Dr. James), give organs new meaning, not only functionally but also to the senses and can contribute to an image that elicits negative responses from others and can cause embarrassment: I get more looks now. Just before at the nurse’s station they were looking at a photo of me with all my hair, like a bit of a Elvis comb back happening, and goatee, packing 102 pounds … they’re looking at me and I’m looking at them and the nurse is pointing and saying, “I’m sure that’s him,” … and they asked me “are you [name]?” and I’m like “yeah, I am.” … I don’t recognise myself sometimes. I think I look a bit like Gollum out of Lord of the Rings. (Ed)
Furthermore, changes to social rituals related to eating and drinking may also induce disgust responses. Disgust is a sociocultural-determined human emotion in reaction to a stimulus. However, in a social context, it is expected that the same condition or stimulus would similarly cause disgust in many people (Powell et al., 2016): They pulled all me teeth out [to do the radiation] … Going from chewing food, chewing food to baby food, and now anything that’ll go through a straw … And the swelling around my mouth … I used to get a lot of different reactions from people … [they] tend to look at me a few times and have a bit of a stare … (Ed)
Studies of disgust and embarrassment in cancer identify a strong relationship between these responses and mental health issues (Azlan et al., 2017a; Powell et al., 2015, 2016). Becker (1973) argued that social responses to deviance were created by social groups making rules about what is aesthetically pleasing and then labelling people as deviant when they do not conform. The disfigurement of facial appearance and function are confronting to both people with HNC and healthcare professionals and can impact responses by healthcare workers, leading to both enacted stigma: I didn’t like looking after them … you think about what it looks like, what it smells like, the nasogastric tube and just all that … it doesn’t really look nice. (RN Helen)
And felt stigma which was exemplified by the knowledge that they were now different from ‘the normal’: I felt that some of the [nurses] were struggling with it [tracheostomy]... As I said, you’ve got all your normal and then you got someone with a trachie and it’s different … (Jim)
Both felt and enacted stigma occur because of “otherness” or deviation from normal (Bonanno & Esmaeli, 2012). The inability of the person with HNC, to conceal their physical ‘deviances’ perpetuate these stigma responses. These reactions from others even included family, as described by one participant’s experience with their grandchild: She was frightened of it because I had that thing there and the tube in the nose … they’ve got a pool, so I hopped in and had a swim, and she got out of the pool and said to her mother, “Should Granddad be swimming in our pool because he’s sick? He won’t pass anything on that we could catch, will he?” Yet my daughter had sat down with her and tried to explain and yet that was one of her fears, that she was frightened that she would catch what sickness I had. (Rob)
Furthermore, the wife of John, who lives with a laryngectomy, identified how they experienced both felt and enacted stigma through avoidance by others: He had that problem the whole time we were away, and you do get people when you go and sit at a table with people, and you’d find the next night they’d be somewhere else because they couldn’t handle it or what have you. (John’s wife)
Physical Changes are a Trade-off for Being Alive
Further to the images of a human monstrosity and its impact on patients, there was a competing discourse within the healthcare team that focused on the power of medicine: This is the best anatomy, this is anatomy for the connoisseur, there’s no smelly bowels or leaking urine and you can restore people’s function and save their lives … (Dr. Tom) Our main thing is to keep them on this side of the grass, isn’t it? … Because we don’t know what’s on the other side of the grass … I said, “mate, you’re still on this side of the grass so this is a small price to pay, no teeth, small price to pay”. (Dr. Joe)
This discourse is ostensibly biomedically driven. Biomedicine views disease and illness from a mechanical causality perspective and treatment from a biomedical, surgical, and pharmacological viewpoint (Filc, 2004): a reductionist philosophy that has underpinned its success. Yet it has also challenged the way society conceives health and illness: culturally, socially, and politically. Biomedicine is by far the dominant paradigm in western healthcare and healthcare professionals’ practices are influenced by biomedical institutional structures and practices that contribute to knowledge and power. Foucault (2008) claimed that one of the critical things that biomedicine had done to society was take away the sovereign power of death. He argued that the normality of death as a part of life was replaced with the power of medicine to improve and prolong life: a term he called biopower (Foucault, 2008). Therefore, the impact of the physical and social changes, were counteracted by an understanding that this was ‘trade off’ for being alive: People come in here … and I said, “you’d probably need an operation and a neck dissection, and you’ll have a scar,” … you’ll have a big scar all around … and they say, “I’ll have a scar.” I say, “yeah, but you’ll be alive and the other option is to be dead, and as you’re better alive with a scar than to be dead,” (Dr. Tom)
It’s All Your Fault: Felt and Enacted Stigma in Relation to Smoking, Lead to Blame
In addition to a physical mark, the origin of a disease or attribute is also a dimension of deviance that can contribute to ensuing stigma (Jones et al., 1984). Importantly for a condition like HNC, it highlights whether a person can be blamed for their condition. Smoking and other forms of ingesting tobacco have oscillated between acceptance as a cultural norm and repudiation as a cultural taboo throughout history (Corti & England, 2007). The perceived social deviance of smoking is a relatively modern concept, intensified since the link was made between lung cancer and tobacco smoke in the mid-20th century and has been pathologized further with graphic smoking cessation campaigns. There are often implications for people with cancer related to lifestyle factors such as smoking (Bell, 2014; Chapple et al., 2004; Lebel & Devins, 2008; Lebel et al., 2013; Threader & McCormack, 2016). This can include influencing impartiality of care as articulated by one of the nurse participants: When they come back [from smoking] and the other nurses say, “that’s disgusting, how can they have been out for a smoke?” and then they’ve asked for pain relief. “They can frigging wait for their pain relief, if they’re well enough to go out for a cigarette.” (RN Joan)
The experience of stigma related to smoking by the patients was multifactorial. One person who did not smoke identified how they felt healthcare professionals’ made assumptions about them: They’d ask me, “do you smoke?” I said, “no.” “Have you ever smoked?” “No.” And they go … that’s not right ... It was like … you can see in their heads … you must be lying,” (Jim)
Another participant who smoked described a perceived feeling of inevitability: No, I didn’t think they made me feel guilty, but … I think as soon as it’s anything like throat, lungs … They're probably just cagey enough to say, “are you a smoker?” first, and then you say, “yeah,” and they go, “well there you go”. (Wayne)
Risk and responsibility has previously been described as a dominant discursive construction of cancer. Willig (2011) identified that there is a strong moral tone that focuses on an examination of lifestyle after a diagnosis of cancer, including questions around sun safety, smoking, and diet. This is perpetuated by the media and other public forums who often make discussions about health and, importantly, ill health as one of individual responsibility (Gibson et al., 2017; Miele & Clarke, 2014). Furthermore, those who resist lifestyle modifications even when armed with knowledge of the risk of cancer are often deemed to inevitably develop cancer at some point in their lives (Bell, 2012). Such discourse was identified in this study: I would get to their level and speak their kind of language, “mate … you’ve been chuffing on dhurries [smoking cigarettes] all your life, what do you expect?” (Dr. Joe)
The social reception of cancers ‘caused’ by the individuals lifestyle choices not only feeds into stigma and blame. It can also lead to shame and affect identity and relationships (Chapple et al., 2004; Gibson et al., 2017).
Conflicting Discourses About HPV Leads to Shame
HPV is one of the most common sexually transmissible diseases and so highly contagious that it is suspected that almost all sexually active adults will be exposed to this virus at some point (Boffetta & Hashibe, 2006). The social discourse around HPV and cancer pathologizes what would be a typical or normal life experience—that of having sexual relations—and links this normal human social and sexual practice directly to the spread of HPV, which may then lead to cancer (Polzer & Knabe, 2012). Unlike cervical cancer, where conversation has long been about its link to HPV and the social implications related to this, one medical officer recognised that this conversation is yet to be seriously had in the HNC community: …it hasn’t been as prevalent as it is now and we’ve only really recognised it as a distinct entity in the last decade … Why haven’t we discussed it? I think we haven’t discussed it properly in the community because we’ve been a bit slow at it, but also head and neck cancers only account for about 4% of all cancers, so we tend to get dwarfed by … the big ones (Dr. Sam).
People living with HNC identified that the link to HPV and questions about transmission were uncomfortable for their teams to discuss with them and often avoided: It was hinted that it was a sexually transmitted disease in the conversation I had with [the doctor]. I remember it was [the doctor] who said, “we just assume most of the population have been exposed to it, they’ve got it,” … [the] number of partners and oral sex, so that wasn’t explained to me … My sense was there was no-one that could really talk about that … It has impacted on my sexual life. (Hugo)
The association between HPV and HNC can cause major embarrassment, relationship stress, and fear for the patient (Mehanna et al., 2013), particularly with absence of honest dialogue. It led to an uncomfortable reaction from one partner due to fear and stigma and caused shame and relationship changes: I think she slapped me in the balls when we got to the lift outside [the doctor’s] office. I did explain, “hold on, this is actually from before I even met you, it’s got nothing to do with you” … [it’s] potentially linked to oral sex and that’s something we’ve stopped doing … Even if it was safe or not safe, it like, “fucking hell, we’re not going to do that.” (Hugo)
However, in contrast to avoiding conversations with patients, a conference at the hospital where the research took place featured a section on HNC titled “Oral Sex and Cancer.” This section of the conference had in fact no talks on the relationship of sexual practices to HPV in the context of HNC, yet the link was used to catch attention and garner interest in the session. The visual link through the text on the posters had the potential to subconsciously lead to stigmatization by connecting a person’s HNC to sexual behaviours.
For other people with HNC the relationship between their cancer and HPV was not embarrassing or stigmatising, but a way to deflect from smoking as a causality factor, specifically for two patients it gave them permission to continue to smoke after diagnosis and treatment: … all he said to me was, “we found out what the cause of the cancer was,” and he said it was a virus [HPV] … All I said to people after that was, “it was a viral cancer” … Other people didn’t all assume that “that’s okay, you can go back to smoking,” but I made that decision myself. (Ted)
This indicates that peoples’ constructions of their cancer are often enmeshed with cultural understandings and moral framings that are prioritized individually.
Labelling Through Assumptions and Categorisation Creates and is Created by Stigma
HNC discourse emphasises the association with behaviours such as smoking, drinking, and sexual activity. Drawing on these images can lead to assumptions about the person with HNC, for example, these activities have often been constructed as masculine or more socially acceptable among men (Corti & England, 2007). While not all these behaviours are, by definition, masculine characteristics, society continues to make assumptions about what behaviours reflect male and female gender roles. A historical review of HNC in only male celebrities depicted the cancer of the chain-smoking president Cleveland, the womanising Emperor Fredrich III, the drug-taking Sigmund Freud, and the party animal Sammy Davis Jr. among others (Folz et al., 2007). Healthcare professionals in this study perpetuated these assumptions, by generally describing patients as ‘he’ and as illustrated by “blokey” tones and class-based assumptions: You explain it to them in the setting that they understand. Like a builder or if they’re a mechanic you can talk about it, “you got to take this out before you can blah-blah-blah” so you try to relate … (Dr. Joe)
Even people with HNC made assumptions about other patients who were presenting to the clinic: It was really confronting [coming to the clinic] because most of the blokes [men] there were a lot older than me, smokers, alcoholics. (Hugo)
Categorisation, particularly related to causative factors, is also a common discursive practice in HNC. Although categorisation is often used to describe the diagnostic and prognostic factors related to the disease characteristics, it removes the person with HNC from the picture and leads to assumptions that can contribute to both enacted and felt stigma. This was done for two reasons: first, it was used to describe the people with HNC from a sociodemographic perspective; and second, to give information about biomedical features such as epidemiology, tumour response, and prognosis. From a textual perspective, collective nouns were used by healthcare professional participants and even myself (before I became sensitised to these issues) such as “old school” head and neck patients versus HPV-positive head and neck patients: I really love the different types of patients that you get in head and neck cancer, so such a variety from the classic old school smokers/drinkers, rough-as-guts group, to the HPV-positive group, which tend to be younger and professionals. (Jill, Speech pathologist)
Each group was also described differently from a sociodemographic perspective. These assumptions were then linked to social perceptions of causative factors. They were in their 60s and 70s, heavy drinkers, heavy smokers, lots of comorbidities, very often lower socioeconomic, which of course that goes with heavy drinking and heavy smoking … These days … they’re younger, much more physically fit, often working, which is an issue for many of them because they often can’t work for four to five months … they’re often breadwinners … (Dr. Bill)
In summary, the interviews clearly indicate the social construction of HNC is embodied in social and political discourses that emphasise aesthetics and disease origin or responsibility.
Discussion
The overarching finding presented in this paper is that deviance dominates the common discourse and shapes HNC and the responses to it. This is revealed through various discursive practices, such as disgust, fear, avoidance, blaming, labelling, and categorizing. All of these are socially constructed. These practices are manifested at a textual level using metaphors, adjectives, descriptors, and collective nouns. Then contextualised by a sociocultural understanding that when someone deviates from what is perceived as normal, they are often devalued and stigmatised. While this is an analysis within a healthcare institution, it could also reflect the wider societal perspective.
The broad historical reality that cancer is deviant filters through the discourse of HNC; this historical reality in itself leads to a certain level of stigmatisation, frequently causing people to be rejected or removed from their pre-cancer beings or social locations (Capasso, 2005; Clarke & Everest, 2006; Sontag, 1989). Crocker et al. (1998) placed stigma firmly in context, arguing that stigma was not always linked to an attribute of the stigmatised person but rather to the social predicament in which they are enmeshed (such as cancer), and the sociocultural stereotypes surrounding this condition. Therefore, people who are stigmatised can be devalued from a social rather than a personal perspective. This study investigated stigma in HNC from a sociological and, more importantly, social constructionist perspective, exploring how discriminatory praxis, however it is enacted, is constructed and perpetuated by micro level interactions between healthcare professionals and patients, discursive strategies and macro level structures including biomedicine as the western healthcare paradigm and societal understanding of what is normal (Fairclough, 1989; Link & Phelan, 2001).
Our findings indicate stigma in HNC arises from multiple discursive practices. Textually this was evident by the graphic depictions of treatment effects that consume the participants’ interviews similarly to what has been previously described (Argiris et al., 2008; Folz et al., 2007, 2008; Logan, 2009; McLaughlin & Mahon, 2014) and was further evident in the close discursive links of HNC to smoking, drinking, and sexually transmissible disease (Bell, 2014; Chapple et al., 2004; Lebel & Devins, 2008; Lebel et al., 2013; Threader & McCormack, 2016). Similar to a previous study of prisoners, this study identified that stigmatised identities are the effect of some form of disciplinary process, such as normalisation and categorisation, and are only understood as deviant when they are interpreted and distributed through discursive practices such as fear, embarrassment, multi-dimensional disgust, blame, categorisation, and labelling (Toyoki & Brown, 2014).
Historically surgery has claimed authority in treating HNC (McGurk & Goodger, 2000; Oldhoff, 1967). In this study removing tumours and manoeuvring body parts so that the person “can swallow and speak” and “be cured” was seen as a triumph over the alternative which was death. These positions of power afforded to different healthcare professionals is directly reflective of the socio-political positioning of those practitioners in their ability to treat HNC (Saks, 2012). This is measured through tangible outcomes and outcome measures including survival (Haddara & Lingard, 2013). Yet this authority over life becomes a discursive struggle particularly for those with long term and permanent changes related to their cancer.
This struggle is also identified in relation to how HPV is discussed in the HNC community. We identified that the absence of conversation can lead to shame for some HNC patients, yet for others the having a ‘virus’ was a way to deflect from their history of smoking and the implications of this for their cancer diagnosis. Similar to other studies, we found that the social discourse around HPV pathologizes what would be a typical life experiences and links this normal human social and sexual practice directly to the spread of HPV (Polzer & Knabe, 2012). HPV needs to be normalised through open discussion by healthcare professionals so that people receive the right information even if the conversation proves to be uncomfortable (Dodd et al., 2016, 2019). Furthermore, information needs to be clear and consistent to help diminish stigma, shame and blame (Daley et al., 2010).
Implications for Change
One important element of critical inquiry is that it aims to encourage people to reflect on their own practice. The findings of how language perpetuates certain historical images of cancer, and how it elicits responses from both healthcare professionals and people living with HNC can encourage practitioners to reflect on how these discourses and discursive practices affect the person’s experience. Importantly, we hope this research can open dialogue about cancers (such as HNC) that historically have been associated with perceived morally and socially questionable causes and encourage reflection on the way the discourses relating to these factors are presented, contextualised, and consumed. This is a challenging but important objective. This open dialogue could also extend to the stigmatisation and social reconstruction of identity related to the long-term toxicities and disabilities associated with HNC and its treatment. By considering how the social concept of normality is fluid and socially constructed by the person living with ongoing toxicities and disabilities at any given time and in any given space, health care professionals could be more responsive to the person’s experience of their cancer. Through listening and witnessing healthcare professionals play an important role in supporting people with cancer to make sense of the fragmented world of cancer treatment and its ongoing side effects.
Furthermore, studying cancer through a social constructionist lens can shape practice as a clinician and as a researcher by encouraging thought beyond the positivist biomedical model and investing in a more balanced approach to education and care. A recent study from Sweden noted that the ability to critique what is presented as normal should be the political nursing education agenda (Tengelin et al., 2020). We identified that critical discussions about norms could support conversations on power and privilege and impact future nurses’ roles as authorities on discourse surrounding what is constructed as normal, pathological, or blameworthy (Tengelin et al., 2020).
Conclusion
HNC is a complex illness. It requires complex research strategies to understand how assumptions about it are made. It also requires an in-depth understanding of deviance, stigma, and other social responses surrounding diagnosis and treatment effects of the illness. The common discourse relating to deviance influences the construction of the illness and the way people experience it. Open dialogue and reflection of the discourse presented can support changes in the way we inherently think, speak, and act in relation to people with HNC.
Footnotes
Author Contributions
All authors contributed to the study conception and design. This study was conceived by CT. Preparation, data collection and analysis were performed by CT and ALM with support from PY. The first draft was the manuscript was written by CT. All authors read, reviewed, and approved various versions and the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.