
Abstract
Little is known about the experience and impact of intersectional stigma experienced by rural young people (15–25 years) who have a parent with mental health challenges. The StigmaBeat project employed a co-design approach to create short films to identify and challenge mental health stigma from the perspective of young people who have experienced this phenomenon. The aim of this paper is to describe the co-design methodological approach used in StigmaBeat, as an example of a novel participatory project. We describe one way that co-design can be employed by researchers in collaboration with marginalised young people to produce films aimed at reducing mental health stigma in the community. Through describing the processes undertaken in this project, the opportunities, challenges, and tensions of combining community development methods with research methods will be explored. Co-design with young people is a dynamic and engaging method of collaborative research practice capable of harnessing lived experience expertise to intervene in social issues and redesign or redevelop health services and policies. The participatory approach involved trusting and implementing the suggestions of young people in designing and developing the films and involved creating the physical and social environment to enable this, including embedding creativity, a critical element to the project’s methodological success. Intensive time and resource investment are needed to engage a population that is often marginalised in relation to stigma discourse.
Keywords
Introduction
Co-designing research and interventions with young people in the mental health field is a common participatory method (Boydell et al., 2017) to co-create interventions that appeal to and impact positively on the intended population (Thabrew et al., 2018). Inequalities between young people and adults can be redressed through recognition of different kinds of expertise (Goodyear-Smith, 2015). However, the term co-design is often used erroneously, where a process of consultation or engagement has been undertaken to gather stakeholder views in a limited manner without commitment to integrating these views into designing better healthcare responses (Thabrew et al., 2018). Remedying tokenistic practices in participatory research requires precision in articulating and implementing co-design methods to prevent conceptual slippage and mislabelling (Smith et al., 2022). Describing co-design projects can provide concrete examples drawn directly from research practice.
This project undertook the challenging aim of employing co-design with a population of young people marginalised on multiple axes and focussed not on specific healthcare goals but on understanding their experiences of marginalisation, inviting them to generate resources to challenge it. We define our co-design approach as applying a set of participatory methods for bringing together those with technical expertise and lived experience in an inclusive space, to creatively explore and generate responses to address a complex social problem (intersectional stigma) (VicHealth, 2019). There remains insufficient work with young people who experience parental mental health challenges (PMHCs) and indeed with multiple populations who are marginalised by social structures, especially in community settings. Moll et al. (2020) note a lack of clarity as to how to meaningfully employ co-design with populations with intersecting vulnerabilities.
This paper describes the co-design methodology and methods employed in the StigmaBeat project, undertaken in rural Australia. The context of the project is outlined, introducing the topic of intersectional stigma for young people who experience PMHCs. We then clarify what is meant when we refer to co-creation and co-design. We describe the StigmaBeat project and how it was developed, using descriptive text with photographic images. The key learnings garnered from our implementation of the participatory process will be described before we present recommendations for other researchers and practitioners wishing to undertake similar projects.
We employ Hinshaw’s (2007) definition of stigma, which builds on the seminal work of Goffman (1963) as a pervasive devaluation of an individual on the basis of a characteristic that is disfavoured or disgraced. Link and Phelan (2001) operationalised the concept through identifying the components of stigma as labelling, stereotyping, separation, status loss, and discrimination, recognising the role of power differentials in stigmatising behaviour. In relation to mental illness, stigma arises from public perceptions (public stigma), from one’s internalised stereotypes or conditioning (self-stigma), and from association with a stigmatised person or group, such as a family member (associative stigma) (Reupert & Maybery, 2015).
Co-design projects in mental health have been described previously (e.g. Goodyear et al., 2022; Larkin et al., 2015). However, our project is distinct in that it was situated in the community rather than a healthcare setting with a cohort of young people with experience of PMHCs. Our goal was to understand the lived experience of intersectional stigma and to identify where, when, and how it impacted on a cohort of rural young people, in order to develop a targeted intervention (short films).
Focus of This Article
The aim of this paper is to describe the co-design approach and parallel research and intervention processes used in this novel participatory project. We describe ways that co-design can be employed by researchers to collaborate with young people who are marginalised by social structures, to strengthen understanding of their lived experiences. To our knowledge, no prior studies have documented co-design projects with young people who experience PMHCs, although a recent Austrian project engaged in a co-design model with various adult stakeholders, to develop a program for children (Goodyear et al., 2022; Zechmeister-Koss et al., 2023). Working with this cohort addresses a gap in research practice, considering the increasing body of work on this population (e.g. Riebschleger, 2004; Van Loon et al., 2014). This project sought to instead collaborate with young people, to deepen shared understandings of stigma, and provide a platform for participants to articulate their experiences of mental health stigma through the creation of a series of short films. The project envisioned a range of potential outputs, including creative and multi-media productions, to promote and spread the key messages that young people produced. On reflection, following a reviewer’s comments, the research team (which included a young person with lived experience of PMHCs who was an employee at Satellite Foundation) had made an implicit assumption that the young people would not wish to contribute to co-authorship of the research elements of the project. This was based on our concern that this would be an extra burden on the time and commitment of the young people, when they were already contributing significant effort into other forms of output generation (the films). Furthermore, we may have risked the disengagement of some young people from the project, for whom academic activities had been fraught with difficulty, as is detailed in the data from this study (Yates et al., in press). While research was not perceived to be a major motivator for young people to be involved in this project, on reflection including them as authors is another opportunity to reduce power imbalances in this kind of work. The team will consider how to offer such opportunities in future in non-threatening ways, around the StigmaBeat project.
Aims of the StigmaBeat Project
The overall aims of StigmaBeat were to (a) generate new knowledge about intersectional stigma, identified and defined by young people living in rural Australia, (b) use data produced through a co-design process to create audio-visual resources focussed on reducing stigmatising attitudes in the environments young people frequent, and (c) identify ways that co-design could be employed to provide young people with opportunities to name and describe their lived experiences of stigma.
To accomplish these aims, the young peer co-facilitators in collaboration with the research team (and informed by the lived experience of young people who were part of earlier consultations) developed a creative, inclusive, and non-judgemental environment in which trust could flourish and young people would feel safe to engage in brave conversations about stigma, their families, and mental health. This led to employing co-design principles to co-create audio-visual resources that could be used to promote important and difficult conversations about mental health stigma.
Intersectional Stigma Experienced by Young People and Families Experiencing PMHCs
The adolescent and emerging adulthood years (aged between 15 and 25) are a time of dynamic physiological, cognitive, and psychosocial change and growth (Viner et al., 2015; Özdemir et al., 2016). Young people grapple with issues around identity (Özdemir et al., 2016), connectedness and belonging (Jose et al., 2012), sexuality and relationships (Tolman & McClelland, 2011), and tumultuous social and legal processes associated with transitioning to adulthood (Roberts, 2018). When young people experience PMHCs, additional issues such as isolation and discrimination (Reupert et al., 2021), socio-economic disadvantage (Reupert et al., 2013), and caring responsibilities (Gladstone et al., 2011; Maybery et al., 2005) may be relevant.
Many young people who experience PMHCs have positive health outcomes and describe opportunities for development of empathy, maturity, and independence (Drost et al., 2016). Simultaneously, some young people report compounding stressors emerging from being exposed to, and responding to, their parents’ symptoms and treatment (Reupert & Maybery, 2007). A lack of family-focussed health and social support contributes to family life dominated by persistent and unpredictable change and disruption (Foster et al., 2016; Gladstone et al., 2011). Socio-economic disadvantages often accompany psychiatric disability in unequal social systems (Reupert et al., 2013), and public and self-stigma may adversely impact young people’s identities and relationships (Dam et al., 2018; Davidson & Scott, 2018).
A recent review found that mental health stigma interacts with and exacerbates other forms of stigma and discrimination, such as poverty stigma, sexism, racism, and homophobia (Reupert et al., 2021). Intersectional stigma refers to the compounding nature of a familial experience of prejudice, discrimination, and exclusion arising from being ‘marked’ as different for multiple intersecting reasons (Reupert et al., 2021). Yates and Gatsou (2020) found the self-identity of parents aspiring to the cultural norm of a ‘good parent’ was influenced and inhibited by self-stigma, as defined by Watson (2007). Negative self-appraisals emanated from assumptions about a psychiatric diagnosis precluding an identity as a capable parent. This could be compounded by self-stigmatisation associated with unemployment, being reliant on income support, experiencing teenage parenthood, and/or bodyweight issues. We are not aware of similar research exploring intersectional stigma with young people who experience PMHCs. However, sexual identity, disability, poverty, and rurality are all characteristics that may be subject to stigmatising attitudes, and for many, these intersect.
Co-Design and Participatory Research Methodology
Participatory methods represent an orientation to inquiry that recognises the value in constructing knowledge through the convergence of experiential and theoretical perspectives (Kemmis & McTaggart, 2005). Acknowledgement that research is grounded in power relations is evident in participatory approaches that seek to redress power disparities through establishing equalising collaborative structures (Corrigan & Oppenheim, 2023). While power differentials cannot be eliminated, by recognising that they exist and enacting strategies to mitigate their effects we can reduce their impact in data production and analysis (Gladstone & Stasiulis, 2017; Swadener, 2005). Participatory methods can effectively engage young people in collaborative relationships with adult researchers to produce research outputs (Boydell et al., 2021); however, careful consideration of how stories are represented and how the ‘voice’ of participants is shaped through the research process is required (Gladstone & Stasiulis, 2017).
Co-design approaches utilise participatory methodology and methods (Cornwall & Jewkes, 1995) to design solutions to identified problems and can be conducted with or without a research component. In this project, we had both. Examples include development of information resources (brochures and films) or community arts initiatives for education or awareness-raising purposes. Co-design is defined as collective creativity that takes place across an entire design process, with the explicit intent of developing an output or intervention (Thabrew et al., 2018). In this project, the intervention is the films, while research outputs are publications and presentations and the development of each were distinct but interwoven processes. Our co-design process generated the knowledge that was the basis of the short films on stigma; the young people led the design and had creative control over the film narratives and the animated characters. They took the photographs used in the photo-stories, and voice recordings captured participants’ stories in their own words. This knowledge, synthesised through qualitative data collection and analysis processes, was also used to generate the academic publications. Whilst the authoring of this output included a young person with lived experience, predominantly, young participants demonstrated enthusiasm and desire for involvement in the film outputs. There was not similar interest in the data analysis and academic writing. Reflecting back on this, we wonder if it may have been possible to describe and make accessible the academic writing in ways that would similarly engage young people being mindful of the time and effort involved in the other outputs. In relation to dissemination of the films as an output, six of the young people have gone on to co-design an education/advocacy package featuring the films, and two participants co-facilitated a 90-minute workshop at a national conference.
Benefits of youth participation in research projects have been found for both research outcomes and for the young people involved. Research quality can be enhanced through the richness of multiple perspectives and via the in-depth discourse that such an approach necessitates (Clark, 2010). Young people and researchers may gain important knowledge and skills. Young people may gain communication, planning, organisation, problem solving, and critical thinking skills (McDonagh & Bateman, 2012) while researchers and communities also gain through the benefits of lived experience knowledge from those who bring a different perspective (Boydell et al., 2017). These benefits can emerge from both participatory research and co-design. Pride and accomplishment in the completed research and non-research ‘outputs’ may be an additional outcome (Di Lorito et al., 2018).
Boydell et al. (2017) recognise young people “as socially competent and engaged actors who have much to contribute to the creation and dissemination of new knowledge” (p. 300) which applies broadly to co-design and/or participatory research and their respective outputs. We share their socio-political worldview that through listening to and amplifying the accounts of young people from population groups who are largely marginalised in the public domain, we can build connectedness, combat isolation and alienation, and emphasise and understand the nature of interpersonal relationships within which stigma occurs. We share with Prebeg et al. (2022) an ethical imperative to enable young people to contribute to shaping how their experiences and needs are framed and met in a field (i.e. mental health) from which they are often excluded (Yates et al., in press). We wanted to challenge and invert knowledge hierarchies that elevate adult academic and medical perspectives and often exclude or silence the voices of young lived experience experts (Gladstone et al., 2006). The complex, intersecting operations of stigma across various facets of people’s identities and statuses tend to undermine the capability of those stigmatised, to name and narrate their experiences, and to have these recognised in interactions with relatively powerful others (Chapman & Carel, 2022). For this reason, we sought to accommodate different perspectives and to identify and name epistemic injustices (Yates et al., in press) in the processes of co-constructing new knowledge that was used for developing the audio-visual resources and for the academic outputs. This stance allowed us to move beyond a priori academic or clinical framings of stigma to undertake the important but challenging process of working alongside young people, enabling them to talk about and visualise their experiences of stigma.
The StigmaBeat Project
StigmaBeat grew from a partnership between an international research team and an Australian child, youth, and family mental health service, Satellite Foundation. The project evolved from a desire to identify and address the structural drivers of mental illness stigma, as experienced by young people, in families experiencing PMHCs. An interlinked parallel research process included collection of data on the project processes and outcomes including satisfaction surveys, focus group recordings, and observational field notes.
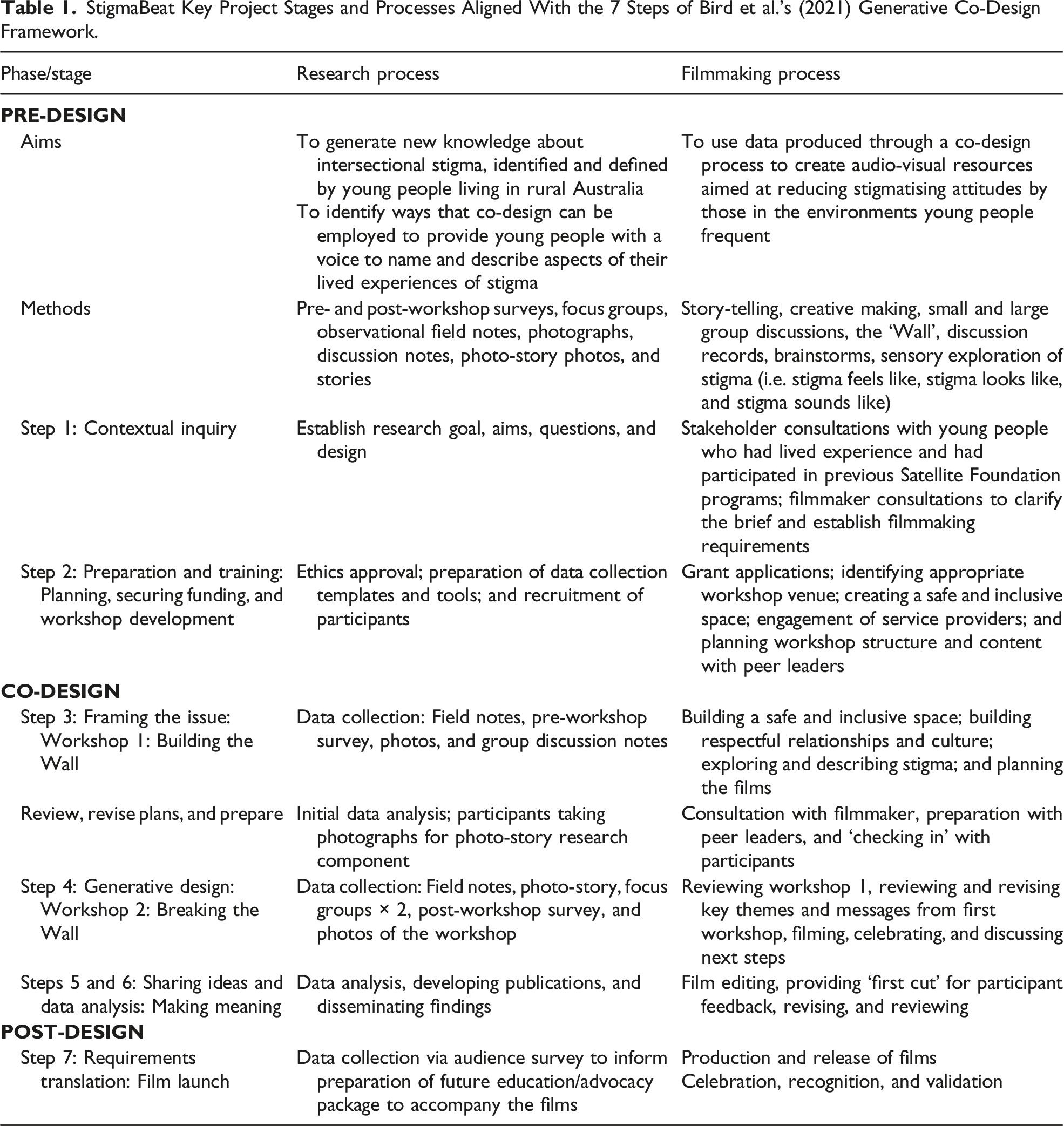
StigmaBeat Key Project Stages and Processes Aligned With the 7 Steps of Bird et al.’s (2021) Generative Co-Design Framework.
Participants
Eighteen young people aged 15–25 years from a rural location in Victoria, Australia, participated in one or both of two workshops (18 attended workshop 1 and 16 of those participants attended workshop 2), co-facilitated by peer leaders who also had lived experience of PMHCs. Participants were aged between 15 and 24 years, with an average age of 18.4 years. Eleven participants identified as women, four as men, and two as non-binary. Two young people attended as a couple to workshop 1 and brought their young baby. Another participant was accompanied by her therapy dog. Participants listed their hopes and aspirations for the project as learning about the importance of mental health, sharing challenges with others who may have similar experiences, improving personal social skills, and contributing to an intervention aimed at reducing mental health stigma.
The Co-Design Processes
The project team comprised researchers, practitioners with expertise in mental health, and young people, and one young person who had experience of PMHCs. All co-authors had prior knowledge and experience in participatory and co-design methodologies, half had lived experience of PMHCs (although are no longer young people) and qualifications included nursing, psychology, occupational therapy, sociology, and social work. This collaboration enabled diverse knowledge, experience, and perspectives to influence and shape the structure, methods, and content of the project with potential barriers and challenges (such as transport difficulties or emotional support needs) foreseen and proactively addressed. The researchers and practitioners primarily informed the conception of the project along with data collection and analysis. The young people and Satellite Foundation primarily informed the conception, design, and conduct of workshops and the development of films.
There were seven phases of the bespoke StigmaBeat co-design process (Table 1) with each phase building on the previous one so that information gained in one phase iteratively informed subsequent phases. The process was informed by Bird et al.’s (2021) generative co-design framework. This seven-step methodological framework was developed to address deficits in the adoption, scale, and spread of health innovations, through defining a rigorous process for embedding the views of end users (Bird et al., 2021). It was applied to the StigmaBeat project as a robust process to privilege the perspectives of participants within our co-design methodology. It commenced with contextual inquiry involving consultations with young people who have lived experience of PMHCs to gain insights into their perspectives on stigma and culminated in a public launch of the short films that young people co-produced. A further translation piece – developing and delivering an education/advocacy package to reduce stigma in the priority settings identified by the young people – is currently underway.
Pre-Design
Stakeholder Consultations
The project commenced with a group consultation with 12 young people aged 18–25 years, known as ‘Orbiters’, who had previously attended programs facilitated by Satellite and had remained engaged with the organisation. The initial consultation privileged the voices of young people from a socially marginalised group (Halvorsrud et al., 2021), to ascertain if a project on stigma resonated and to propose the idea of a film-making project. Producing short films was suggested by the research team as an engaging and creative activity, with the possibility of developing powerful and evocative products that could be accessible to a broad range of audiences (Davis et al., 2019). This was enthusiastically endorsed by the young people.
Developing ‘Courageous Conversations’: Two Co-Design Workshops
After funding was confirmed, a second consultation was conducted with the same group of Satellite ‘Orbiters’, to provide specific guidance on the ‘how’, ‘who’, and ‘what’ aspects of the project. Young people provided suggestions on how to maximise safety and inclusivity to promote engagement and participation. Strategies were brainstormed for recruiting participants and developing the workshop structures and processes (Table 1). Ideas for indicating to young people from diverse backgrounds that the workshops would be welcoming and inclusive included diversity symbols displayed on flyers and linking recruitment information to a short video depicting young people from Satellite talking about what to expect, based on their previous experiences of undertaking Satellite Foundation programs. We also ensured the space was physically accessible and that transport support and food were available.
Recruitment
Young people with experience of PMHCs were recruited through social media posts and flyers designed by young people with lived experience to ensure inclusive age-appropriate language and graphics were used. Flyers were posted in public places (e.g. libraries and train stations) and disseminated through mental health and social services. Youth mental health practitioners working within youth, education, and mental health sectors proved integral to promotional efforts, sharing the flyer and project information with young people who were their clients.
Co-Design
The Workshops
The highly interactive workshops were designed by Satellite peer facilitators in conjunction with the research team to create a space for deep and ‘courageous’ conversations where vulnerability was embraced. The peer facilitators were themselves young people with lived experience of PMHCs who had undertaken peer leadership training and were engaged professionally in paid positions to undertake this role. They drove epistemic processes through shaping the workshop structures and content and in their interpretations of discussions as recorded in notes and lists that were used to develop the films and for the academic outputs. Young people addressed key questions through discussion, games, and creative exploration. Questions included: What is stigma? How does it impact you? What would your life look like if there was no stigma? Where do you experience stigma? What would make a change to your experiences of stigma?
The two full day workshops were held at a purpose designed youth facility in a rural town. Participants were paid 100 AUD for each workshop, in recognition of their time and expertise. The workshops were held two weeks apart to enable time in between for young people to reflect on the conversations they had engaged in and undertake a photo-story activity. As most participants attended school or work, the workshops were held on weekends. They were facilitated by two young peer leaders, with the support of a Satellite Foundation programs manager (also a young person with lived experience of parental mental health challenges) and a researcher who both had extensive experience in group facilitation with young people. The first session was called ‘Building the Wall’, and the second, ‘Breaking the Wall’. The Wall was a metaphor for stigma. As one peer leader commented, stigma “holds important conversations hostage” and so like a wall creates a barrier between people that prevents social connectedness and empathy.
Workshop 1: ‘Building the Wall’
Building trust and connection between participants and between participants and facilitators was a focus of the first workshop, to allow for open and respectful sharing of thoughts and experiences. This was accomplished through application of trauma-informed principles (Bendall et al., 2021) such as gentle, playful warm up activities, a focus on relationship building, strength-based discussions, sensory modulation (e.g. provision of fidget spinners, drawing materials, and different seating options), trigger warnings, and easy access to food, drinks, and toilets at all times and games during break times. Participants were also encouraged to bring a support person to the workshop if needed, and this option resulted in five youth practitioners being present for the first workshop and three during workshop 2.
After providing informed consent, participants completed a survey which gathered demographic information and data about their expectations and reasons for taking part. Participants were advised of areas within the building they could move to if they wanted to step out of the observational space (Gladstone et al., 2014).
The concept of stigma was explored in a multitude of ways, and the young people identified experiences of stigma within a range of settings. Semi-structured discussions led by the peer facilitators asked participants questions such as “What does stigma look like? Feel like? Sound like?” and “What has stigma stopped you from doing?” Story-telling and making activities promoted accumulating awareness and understanding about the ways that stigma is embedded in social structures and the impact it has on individuals, families, and communities.
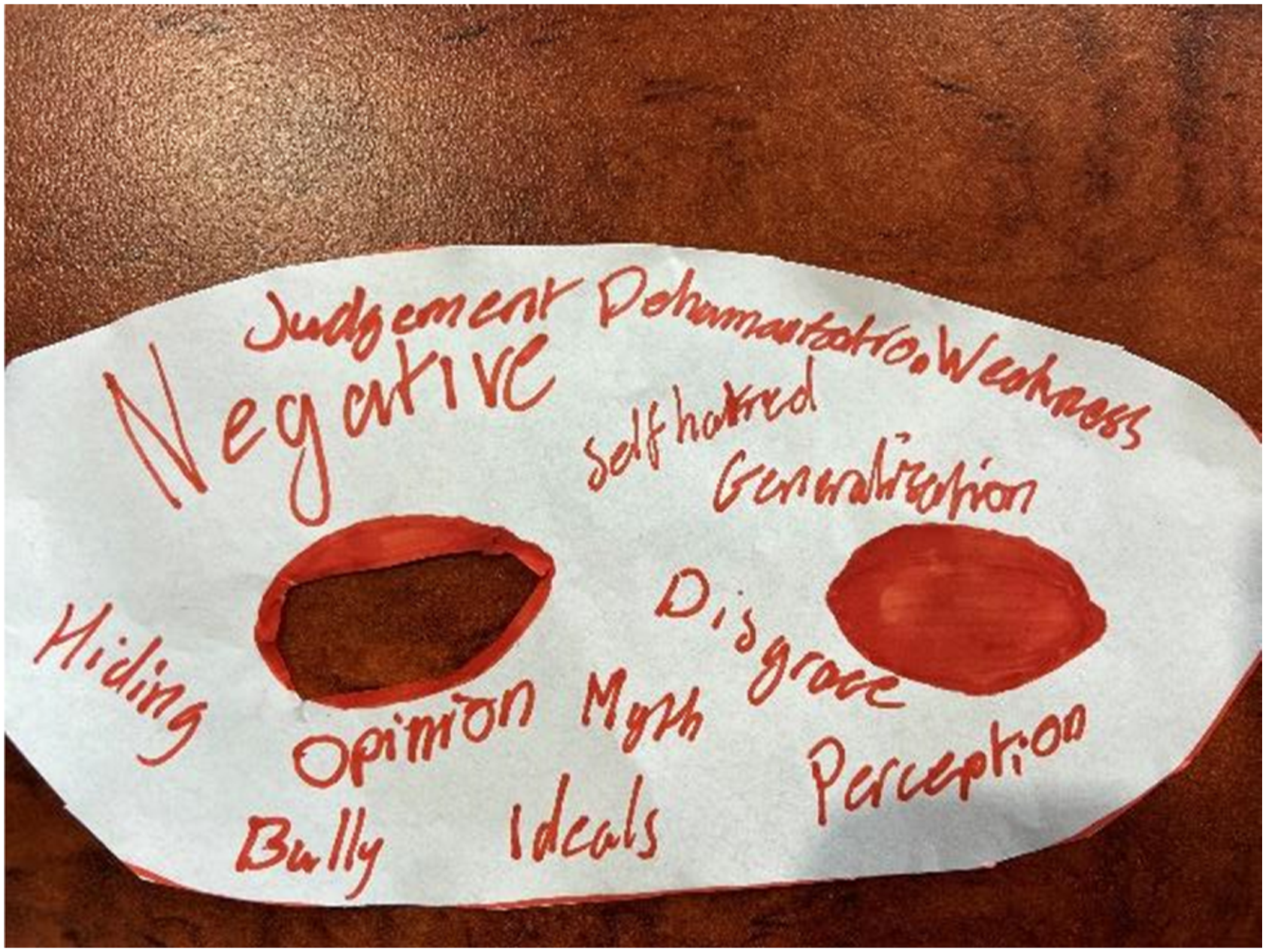
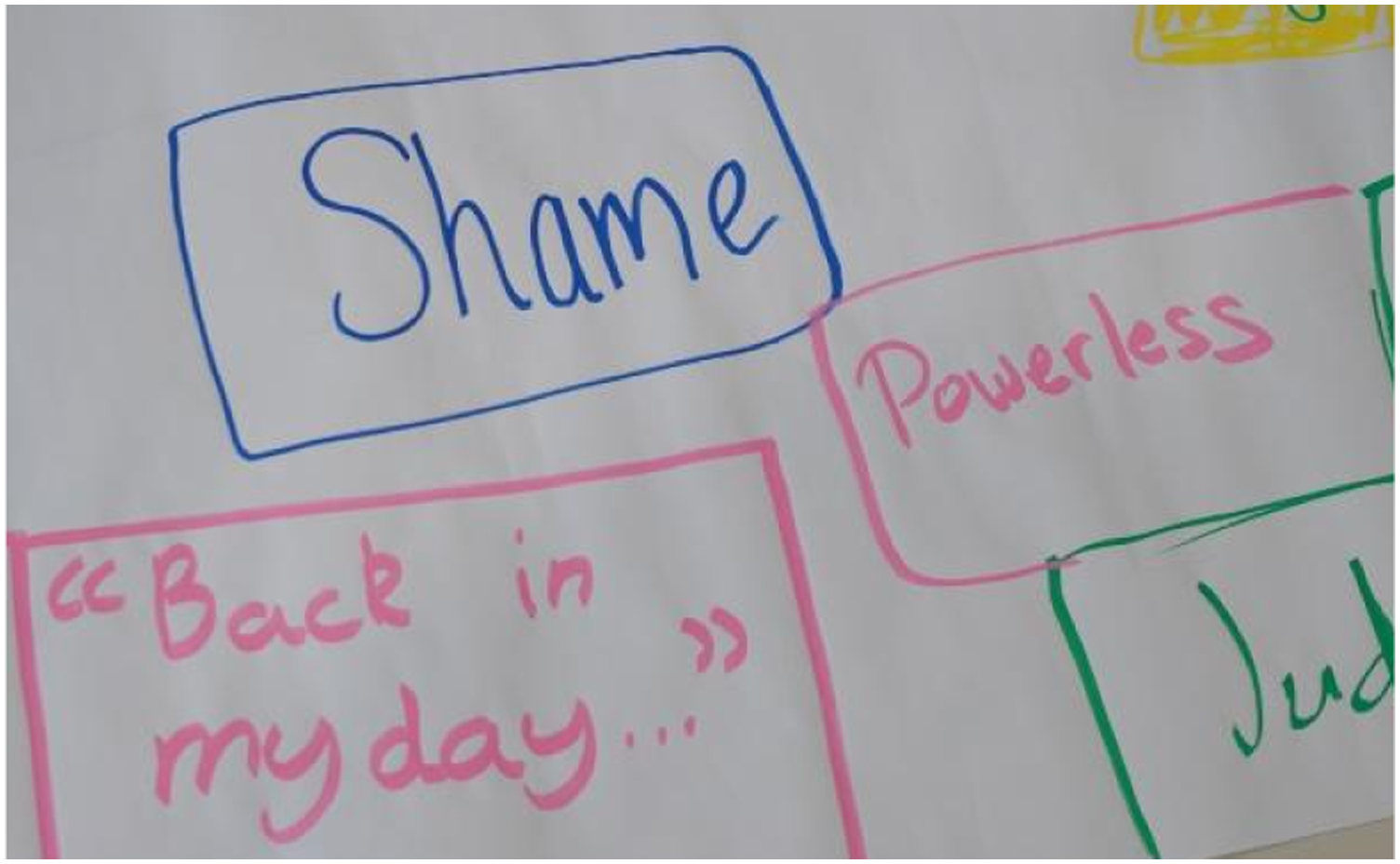
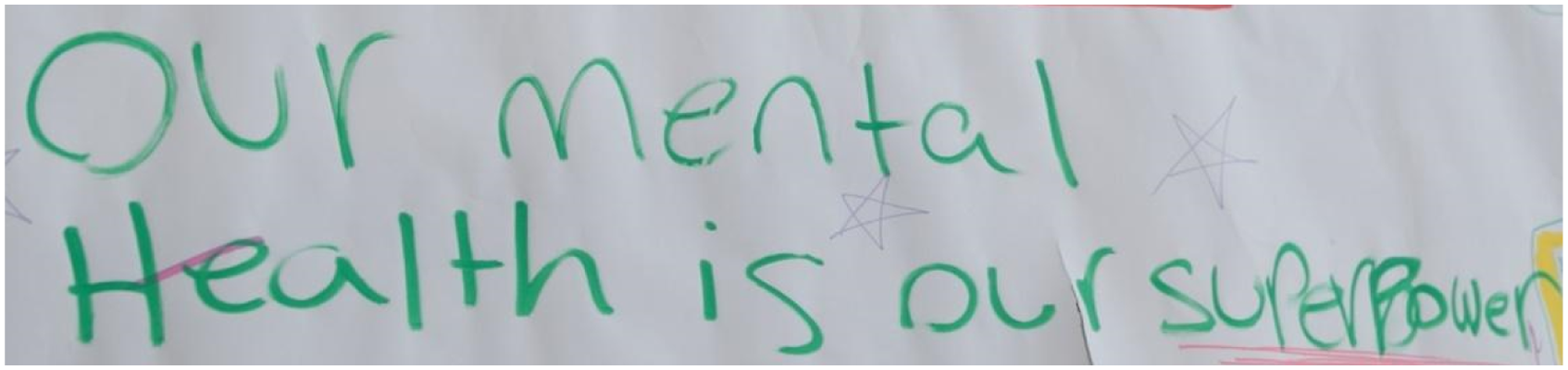
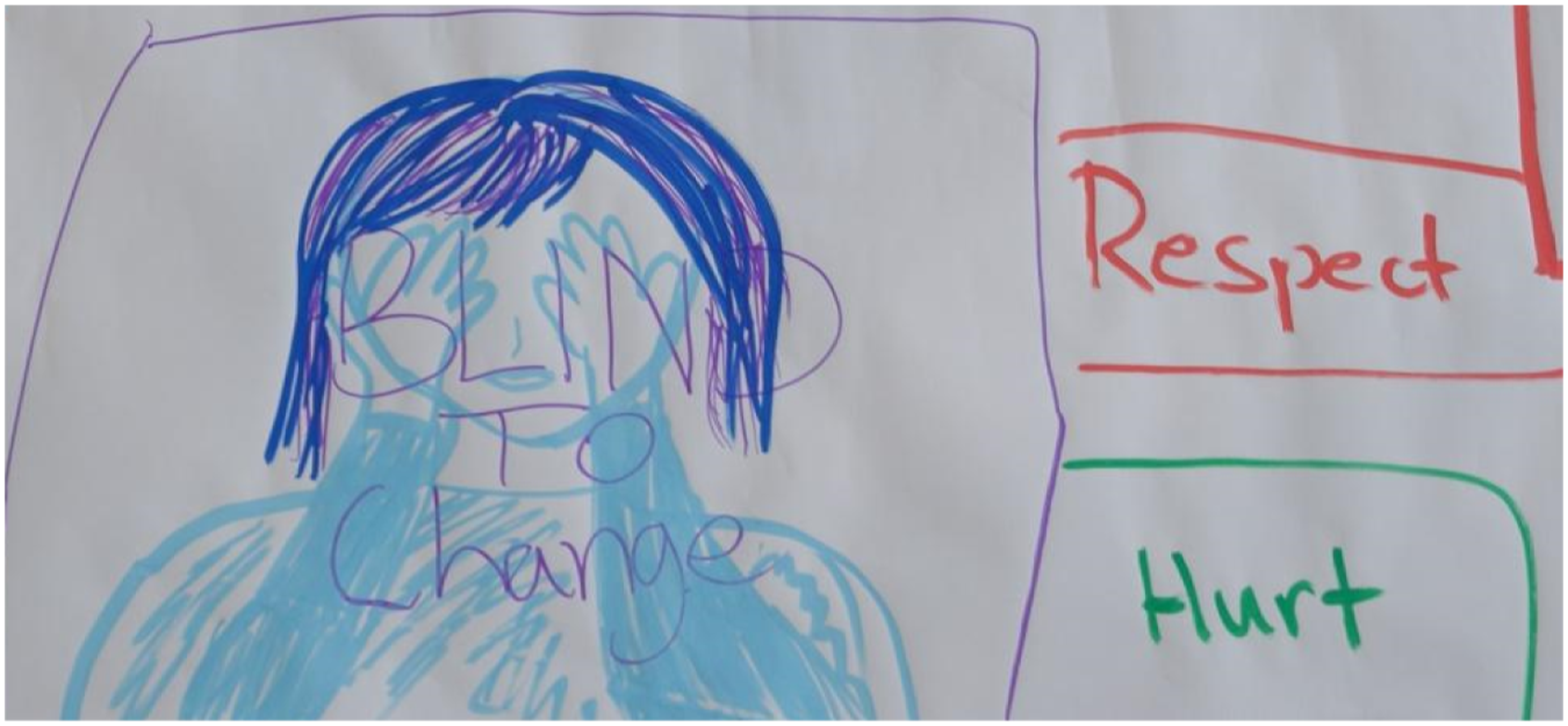
Embedding creativity meant using craft materials and games to explore difficult topics. In one activity, a game using stacked wooden blocks was modified by adding questions to each block so that as each young person moved a block, they read out a question that the group could respond to. Questions included: What defines you? How do other people see you? What do you wish we talked about more in society? In another activity, the young people were asked to form groups of three, and while one person shared an experience of stigma, the other two group members made an object for the person, using A3 paper, tape, and coloured textas. Completed objects included a mask, gloves, a pleated cape, and a shield (see Figures 1–5). Creating a safe space. Made objects. Wearing a mask. Stigma group brainstorm. Games were used to stimulate deep conversations about stigma.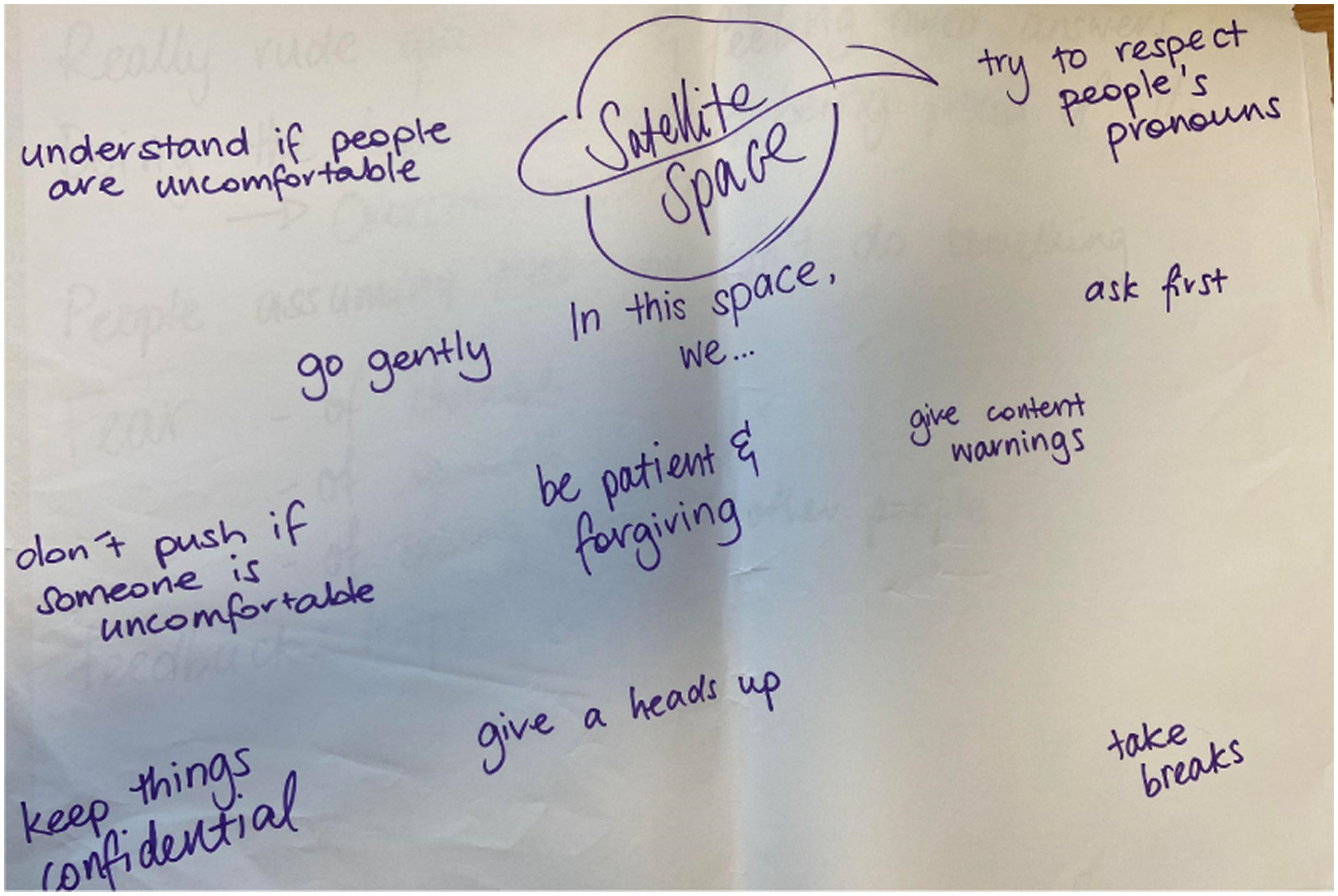

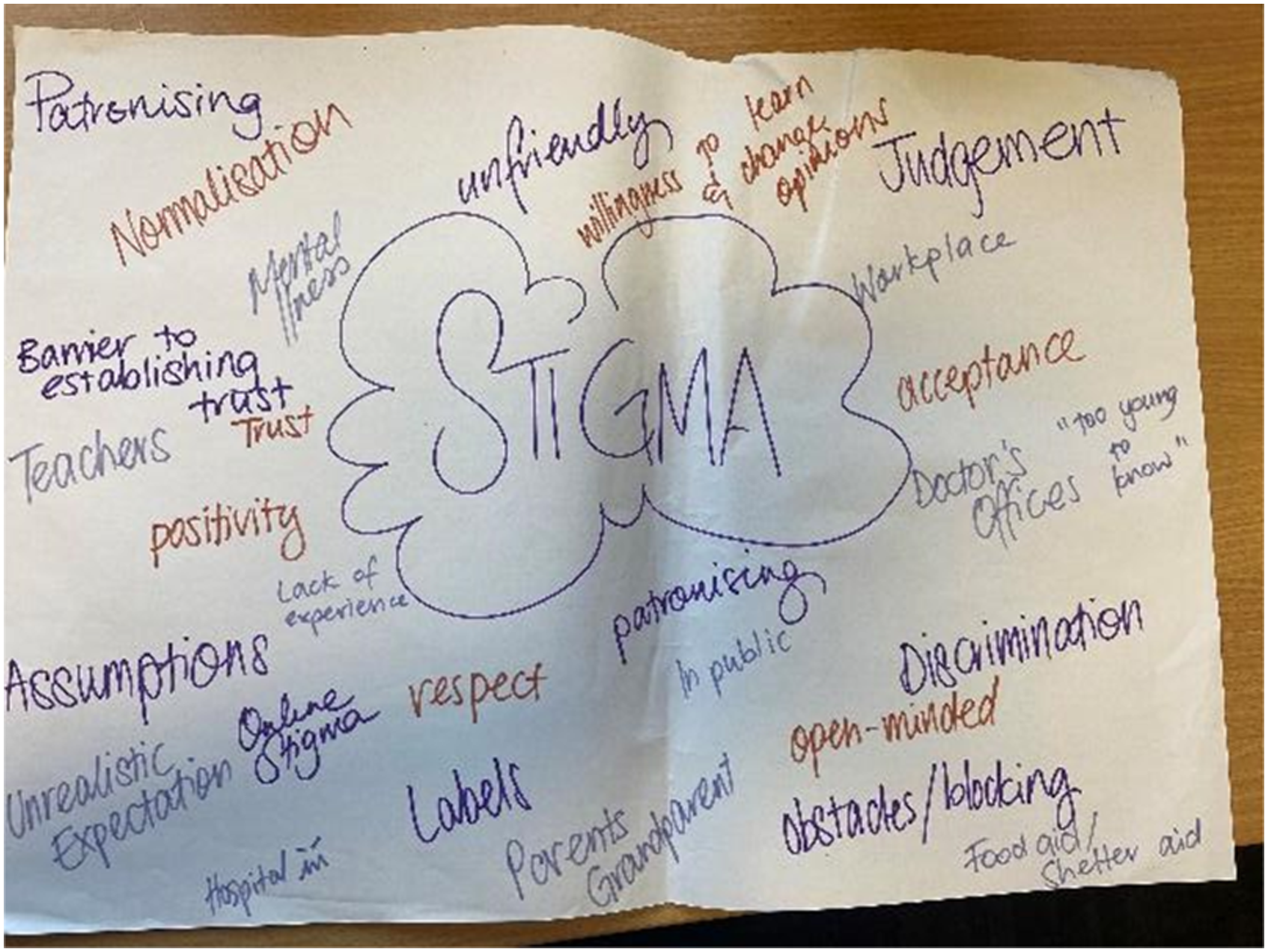

Ten metres of paper was rolled out across the floor towards the end of the session with participants invited to write or draw what stigma is and what it does, creating a stigma ‘wall’ (Figures 1–3).
Photo-Story
Towards the end of workshop 1, participants were invited to engage in a photo-story project. This method was incorporated at the suggestion of the research team as a creative, engaging, and accessible way for young people to express their thoughts, feelings, and experiences around the complex and evocative topic of stigma (Varvantakis & Nolas, 2021). The young people consulted in the pre-design phase endorsed this. In the 2-week interval between workshops, participants were invited to take up to five photographs that encapsulated their response to the prompt: ‘Where can you find stigma-free spaces? Take a photo of something that makes you feel the way you think a stigma-free world would feel’. Photos were then emailed to the workshop facilitators, printed in colour, and brought to the second workshop.
Between the two workshops, the research team met to review the data, using it to inform the second workshop activities and methods. A preliminary analysis of the data from workshop 1 identified key themes, gaps, and areas requiring additional exploration or clarification during workshop 2. This enabled the structure and content of the second workshop to be strongly informed by the data.
The research team engaged a filmmaker experienced in digital story-telling and working with children and young people around social and health issues. Robust discussions between the research team and filmmaker helped shape the workshop 2 outline, with participant ideas being sorted analytically and developed into three short film concepts that were subsequently presented to the young people. Workshop activities were structured to allow participants to share their photo-stories with the filmmakers, participate in a focus group to reflect on the workshops and share their experiences of participating, to continue the exploration of stigma, and to provide opportunities for ongoing connection through informing them of Satellite programs and supports.
Workshop 2: ‘Breaking the Wall’
The second workshop was held in the same location as the first with the same peer facilitators. The filmmakers were introduced, and the process for collecting footage explained, with participants having the opportunity to opt in or out of different aspects; for example, they could choose if they wanted to take part in a focus group and whether they wanted to share their photo-story with the filmmakers. The main themes from the previous workshop were reviewed with opportunities for participants to express agreement, dissent, clarification, and/or expansion. Further creative activities, such as a ‘shout and share’ activity where participants were asked to identify the word associated with stigma that they most wanted to change and shouting it out into the wind together, consolidated and clarified researchers’ and facilitators’ understanding of young people’s conceptualisation and experiences of stigma. At this workshop, the paper ‘stigma wall’, constructed in workshop 1, was broken as it was held up as a banner and participants ran through (Figures 6–9). ‘The Wall’. ‘The Wall’. ‘The Wall’. ‘The Wall’.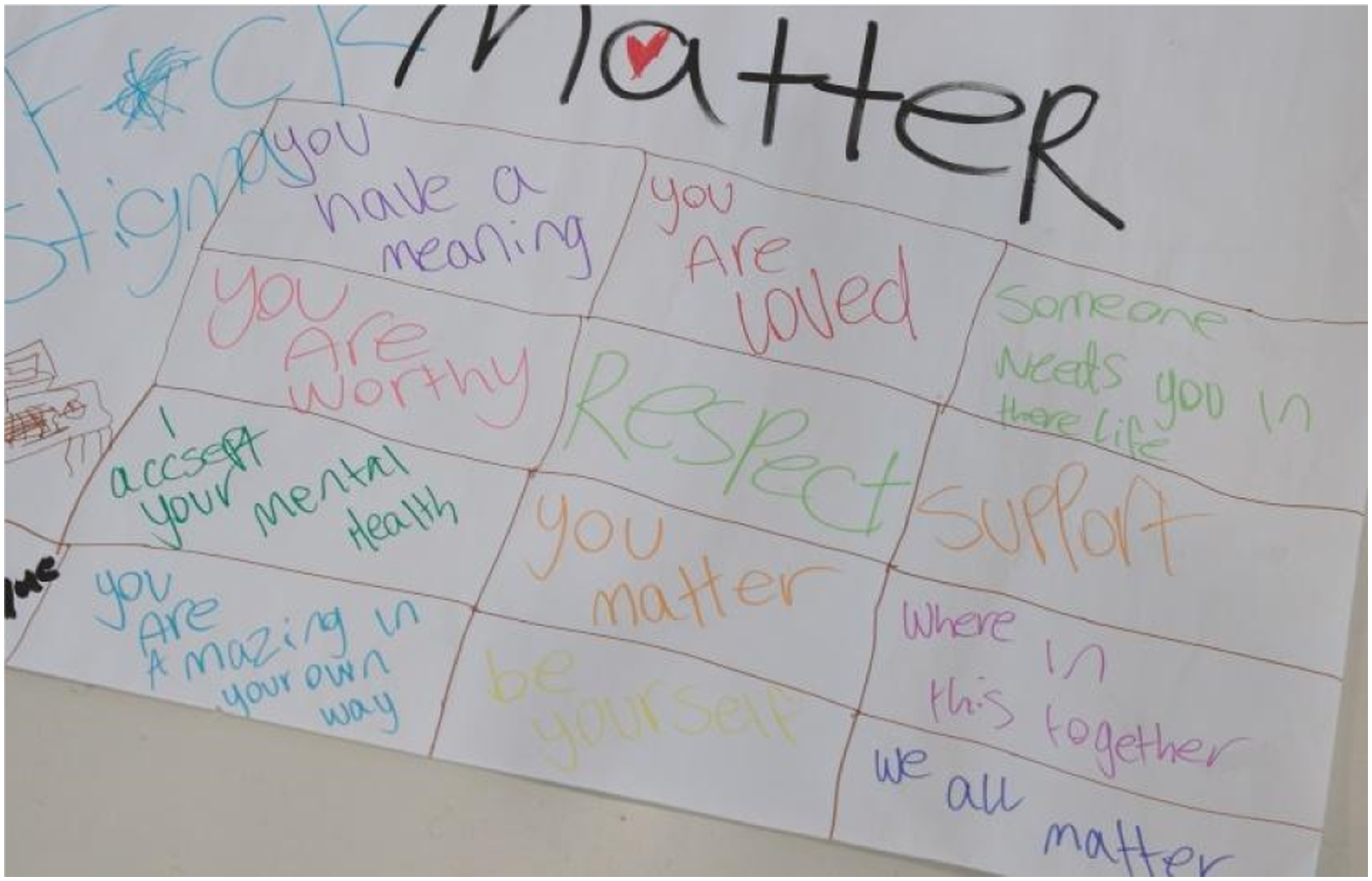
Participants were asked to choose one of the photos they had taken and to describe (in writing or verbally) the meaning behind their image. The images were displayed on a wall without their ‘stories’ to allow participants to derive their own interpretation of the meaning (Figure 10). Participants were then invited to share in group discussion their reflections on or responses to photographs that others had taken. This discussion informed development of the photo-story films and also constituted data in the research process. Photo-story gallery.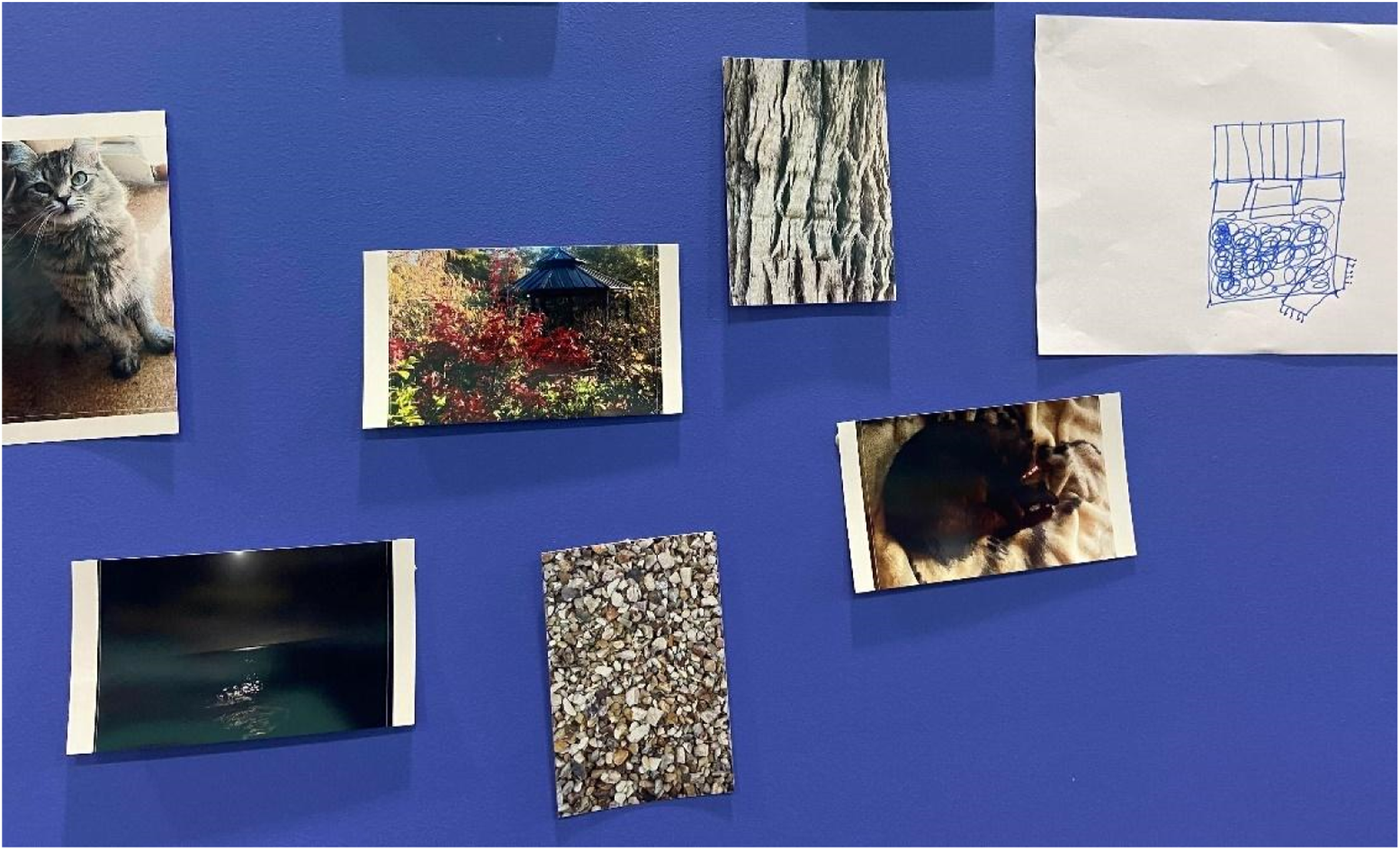
Filming
During the second workshop, young people aged over 18 years were invited to be filmed to provide footage for the audio-visual resources. Footage of some of the workshop activities was unobtrusively recorded, with only those young people who were over 18 and had consented, identifiable in the film. All participants were invited to meet individually with the filmmakers to film their photo-stories. In this part of the project, the camera focussed on the photo, and only the participants’ voices were recorded.
Additionally, the filmmakers conducted individual interviews with consenting participants who were aged over 18. This was an adaptation to the original project plan. The initial intention had been to avoid any identifiable people in the final films due to ethical considerations around anonymity and confidentiality. However, in response to young people stating that they wanted to be seen as they were proud to be role models breaking down stigma, this additional opportunity to contribute was created and used to enhance the audio-visual package with an introductory film. In addition, a series of 12 photo-stories depicting young people’s representations of a stigma-free world were created, and an animation. The animation depicted how stigma manifests in different settings, the fatigue created by constantly combating stigma, and the idea that all and any of us can be both subjects and perpetrators of stigma. This latter film features a participant’s voice.
During the editing process, participants were invited to provide feedback on the storyline and character sketches used for the animation. They could vote for their preferred characters from eight possible options. The young people approved their anonymous photo-stories after minor edits were made in response to their feedback. It was important that each participant was completely comfortable with their content before it was shared.
Post-Design
Launch
At a public launch, participants in attendance were invited to speak about their experiences of participating and their responses to the final products. Participants, their families, the recruitment and support agencies involved, funding bodies, and interested community members were invited to attend the event. One young person subsequently participated in an interview on local radio about the project.
The next steps are to co-design with the same group of young people, an education/advocacy workshop featuring the films, and evaluate the outcomes of delivering this to various settings such as healthcare, housing and homelessness services, and educational institutions. These are some of the places the young people identified experiencing stigma.
Reflections on Using a Co-Design Approach
In the StigmaBeat project, we employed co-design methodology to co-create short films that illuminate the experience of stigma for young rural people from families with PMHCs. The process resulted in audio-visual resources that the young people recognised and endorsed as being accurate reflections of their experiences and understanding of stigma. To our knowledge, this project is unique in its focus on combining co-designed research (knowledge production) with development of an intervention (the films) with this population. To balance discrepancies in power, the research team prioritised the knowledge and experiences of young people, a group who are marginalised in public discourse.
The films could be seen both as counter-narratives that challenge stigmatising discourses (e.g. regarding age, mental health, sexuality, gender, and socio-economic conditions) and also shed light on alternative perspectives that challenge dominant understandings of stigmatisation. Young people as a population are often stigmatised. Stereotypes portray them as being lazy, immature, disorganised, moody, disruptive, ignorant, and lacking in knowledge and experience (Kelly, 2018). However, researchers have also recognised young people to be socially competent and engaged, capable of contributing to new knowledge production and dissemination (Boydell et al., 2017; Gladstone et al., 2006, 2011, 2014; Gladstone & Stasiulis, 2017), and our experience aligns with this latter description. We made it clear that the researchers wanted to learn from the young people in our co-design project. We were not there to teach them about stigma. This was a novel approach that fostered trust, reduced power discrepancies, and grounded the workshops in a collaborative framework that valued the knowledge of each person. A significant body of work in the research field of parent, child, and family mental health has demonstrated the valuable contributions of young people experiencing PMHCs to the generation of new knowledge (e.g. Drost et al., 2016; Gladstone et al., 2011; Riebschleger, 2004).
We intentionally set out to redress the social inequities young people experience in their everyday lives by prioritising what they had to say and safeguarding their autonomy during the knowledge production process. This was operationalised through consultations, providing a choice of activities and the choice to opt out, creative control over what was filmed, and an opportunity to contribute to editing and approval of the final films. There are no guarantees that co-creation will lead to improved research outcomes or that devolution of power will occur (Rose & Kalathil, 2019). Outcomes are dependent on the unique project culture, structures, and processes. However, we believe that the StigmaBeat processes and outcomes (both research outputs and films) were enriched by a commitment to reduce power differentials (Moll et al., 2020) and to create the cultural environment necessary to optimise engagement. The dynamic and adaptive climate co-design necessitates can be both a challenge and advantage and must be factored into ethical considerations, planning, and resourcing (Goodyear-Smith et al., 2015).
Strengths of the Co-Design Process
Arts-based research methods are a dynamic and creative way to engage multiple perspectives in contributing to knowledge production and challenging the status quo (Boydell et al., 2012; Gladstone et al., 2012). We combined filmmaking tasks with ambitious research goals of collectively co-creating knowledge on the experience and understanding of stigma for young people. We embraced principles of an equitable and experientially informed research model, according to Smith et al.’s typology (2022) along with a generative co-design framework (Bird et al., 2021) to guide the process. Although a guiding framework grounds the project within an evidence-based method, in the midst of the process it often feels messy. A degree of comfort with the chaos of co-creating, collecting, interpreting, reviewing, and revising data is a prerequisite for undertaking participatory work.
The key components of the workshops included peer leadership, embedding creativity, and operationalising a trauma-informed approach. Having peer facilitators lead the workshops enhanced trust. Commencing the first workshop with young peer facilitators sharing their own stigma experiences made the content relatable and provided role modelling and a common language that opened up space for difficult conversations. It demonstrated the commitment of the ‘older’ members of the research team to relinquish space, to listen, and to be present in supporting roles. Evidence on the value and efficacy of peer leadership in research is scant. Where young peer leaders are employed, the model most often applied is that peer leaders are recruited, trained, and supervised to convey information or education to their peers that has been developed by adults (Cowie & Olafsson, 2000; King & Fazel, 2021). However, in our project, the young people were experts, with the researchers communicating what was needed in terms of data collection and the young people deciding how to structure the workshops to prioritise engagement, connectedness, and choice. Trusting the knowledge of the young people about what would work shifted the power dynamics and invited innovation.
While the process of making films in itself was a creative endeavour, layers of creativity were embedded throughout the workshops, from introductory activities like badge making to playing music in the breaks and opportunities for drawing, writing, and photography, a strategy endorsed by Moll et al. (2020) to illuminate stakeholder experience and to inspire the co-design process. A variety of mediums for participation offers multiple opportunities for self-expression (Lee et al., 2020) and enables participants to respond in their preferred mode. The meaning of individual and collective narratives could be constructed, deconstructed, and reconstructed through creative exploration alternating with group discussion. The ‘Wall’, for example, was created as a representation of the accumulated knowledge about stigma as a barrier from workshop 1. It was brightly coloured and included text, symbols, and drawings. In workshop 2, a focus on what needed to change led to the literal breaking of the ‘Wall’ as participants crashed through the paper. The use of creativity enhanced safety and inclusion. Creating a welcoming and inclusive space was paramount to engaging the target population, a group we knew faced multiple barriers to participation. From an ethical standpoint, it was also critical to ensure that these activities and brave conversations did not cause harm. Trauma-informed principles focussed on relationship building and attended to sensory needs, choice, autonomy, and validation (Bendall et al., 2021). A focus on building relationships between the young people was an intentional strategy to promote social connectedness in the group. The majority of the participants attended both workshops, speaking to the success of these strategies and the sense of belonging that was cultivated.
The Limitations of Co-Design Process: Opportunities Missed
There were challenges and limitations in our implementation of the co-design method. The research team arrived with a pre-determined idea that the output would be audio-visual resources. Had we initiated the project with only the goal that we wanted to reduce stigma, the young people may have suggested alternative ideas that may or may not have included an output; however, the filmmaking goal appeared to have strong endorsement that didn’t waver during the project. Time and resources dictated that we could only hold two workshops. Had more funding been available, the young participants could have been involved in conversations with the filmmaker between workshops – presenting their ideas directly rather than having them interpreted through the research team. Similarly, the young people could have been involved in the filming and editing processes themselves. This would have enhanced the skill development outcomes that are often cited as an advantage of co-design (McDonagh & Bateman, 2012).
The research aims, questions, and methods were largely determined by the research team, which included one young person with lived experience of PMHCs, in collaboration with the peer co-facilitators; however, there was scope for affirmation and adaptation. This is consistent with most co-design health research where “foundational co-design activities were typically taken by the researchers prior to any contribution activities” (Slattery et al., 2020, p. 6). In a meta-review of research co-design in health, the authors found no co-design approaches that focussed on the research planning phase. Instead, the co-design elements were relegated to particular parts of the process such as interpretation and dissemination of results and implementing practice change (Slattery et al., 2020). Participation of young people is always dependent on being ‘invited in’ to the research space, a foreign and potentially intimidating place with its own customs, language, and expectations which are known only to those who are insiders, and is exclusionary by design (Harding et al., 2021).
Implications for Future Co-Design Projects
McDonagh and Bateman (2012) have detailed the factors that need to be considered prior to embarking on co-creation projects with young people. Resourcing, building activities that align with the cognitive and psychosocial development of participants, confidentiality and ethics, training, recruitment and retention, and the potential role of parents, including their gatekeeping role, all require thoughtful planning. We highlight the importance of interrogation of power in relation to roles, responsibilities, and decision-making, including transparency about how and when power over decision-making will be shared. This aligns with Moll and colleagues’ (2020) reflexivity tool which asks “How will you interrogate power and privilege?” (p. 4). Embedding creativity and operationalising trauma-informed principles helps cultivate (although cannot guarantee) a culture of psychological safety.
There was apprehension from the research team about whether young people would want to be involved in such an endeavour and a recognition that the rationale and motivations for their participation might vary. We wondered if they would (a) show up, (b) take the project seriously and participate fully, (c) come back for the second workshop, and (d) provide feedback on the films. Questions around who determines measures of success and how these are pertinent. Balancing the needs and preferences of different perspectives including academic rigour can bring power dynamics to the fore. All of this needs to be addressed at the outset and throughout the process.
Some of the young people have been actively involved in disseminating the films through co-designing and co-presenting a 90-minute workshop which has been piloted at a conference and will continue to be delivered in presentations led by the young people to diverse healthcare, education, and community sector audiences. However, the young people have not yet been involved in the development of peer-reviewed papers and have not expressed an interest to do so. We cannot assume that these are activities young people want to be part of, while at the same time we can make them accessible and achievable to those who do. As this project moves into evaluating the impact of the films on changing attitudes and behaviour, the young people who continue to take part will be invited to engage in collecting and analysing the data and preparing publications.
Finally, this project was made possible through the collective extensive knowledge and experience of the research and project team along with well-established collaborative relationships built over years of work in this field. Co-design projects are complex and require substantial capacity for constant critical reflection. The composition of the research team requires careful forethought.
Conclusion
Co-design is often used in health but rarely described or evaluated (Slattery et al., 2020). Utilising a co-design approach in mental health research necessitates thoughtful planning, substantial resourcing, robust relationship building, and proactive planning for a plethora of potential challenges. Issues of power are salient in populations where power differentials are marked, including when conducting research with young people. Vigilance is needed to anticipate, detect, and prevent exclusion and those in positions of authority using power over participants of any age, especially when they are young people.
The positive outcomes from well-executed co-design projects can be vast and produce knowledge to drive innovation in health interventions. Developing co-design projects with young people can have reciprocal benefits through sharing diverse knowledge, skills, perspectives, and experiences. Through fostering innovation and harnessing rich lived experience, they can be used to identify and address many complex social challenges that adults have not been able to remedy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Foundation for Rural and Regional Renewal (ABC Heywire Youth Innovations Grant) and Latrobe Health Assembly.