
Abstract
The National Health Service (NHS) cardiac rehabilitation patient care pathway has remained largely unchanged for many years despite, on average, half of all eligible patients declining to engage. To investigate reasons for non-engagement, we explored the experiences of ten cardiac patients who participated in cardiac rehabilitation, dropped out, or declined, as well as experiences of seven people deemed significant others by participants. Our ethnographic study involved participant observations, repeat in-depth semi-structured interviews, and reflexive journaling. Reflexive thematic analysis was conducted, focusing on participants’ lived experiences. Utilising Bourdieusian concepts of habitus, capital, and field, this article highlights how personal biography, material conditions, and dispositional inclinations combine to make cardiac health care decision-making individual and complex. Despite this, health professionals were not always attuned to specific circumstances arising from differences in patients’ experiences and lifeworlds. By considering service improvement recommendations that acknowledge socio-cultural influences, cardiac rehabilitation can work towards providing patients and their significant others with more appropriate, personalised, and person-centred support.
Keywords
Introduction
Cardiac rehabilitation (CR) is one of the ways the UK’s National Health Service (NHS) tries to manage the thousands of cardiac events that happen in the UK every year (British Heart Foundation (BHF), 2023). A plethora of research evidence identifies the benefits of CR in reducing post-cardiac event mortality (Anderson et al., 2016; Aragam et al., 2015) and preventing further events (Anderson et al., 2016; Taylor et al., 2007). Additionally, CR is considered safe, with minimal risk of harm identified (Clark et al., 2013). Despite this, only 50% of eligible patients opt to participate in CR, and engagement varies when gender, social class, and ethnicity are considered (BHF, 2022a). The disparities in participation are not new, seeing little shift since the UK’s National Audit of CR (NACR) began some 15 years ago and against a backdrop of the NHS long-term plan targeting 85% participation (NHS, 2019). Stubborn levels of CR uptake are not only a UK issue, ranging from 10% to 60% uptake globally (Ades et al., 2017; Dalal et al., 2015). We were interested in investigating some of these disparities ‘on the ground’ in participants’ lived experiences of CR (non)participation. In doing so, we add to the research corpus by considering how Bourdieu’s interlinked concepts of habitus, capital, and field can assist in the appreciation of the complexities associated with health care decision-making, including the perspectives of cardiac patients and their significant others, whether the former attend, drop out of, or decline to attend CR.
CR operates as part of an NHS patient care pathway, during which each adult patient who has experienced a cardiac event will typically (sometimes automatically) be referred to a CR service. Whilst exercise-based CR continues to be the most prominent format, CR constitutes more than just exercise and also includes risk-factor management and behaviour change and education (British Association for Cardiovascular Prevention and Rehabilitation (BACPR), 2023). The effectiveness of medicalised and behaviour-change-focused interventions, such as CR, has faced considerable critique (Pavey et al., 2011), and yet such programmes continue to be delivered with this focus. With the proliferation of the ‘responsibilisation’ agenda, these interventions risk placing blame for poor uptake and adherence on individuals (Malcolm, 2014; Williams & Gibson, 2018), with little acknowledgement of the socio-cultural context within which decisions are made.
Person-centred (sometimes referred to as patient-centred) care is an approach woven into NHS health professional training, service planning, and delivery. Its focus is on providing care that supports patients’ preferences, needs, and values, rendering it personalised and empowering (NHS England, 2023). Person-centred care links to the organising principle of integrated care, argued to be an essential system-wide approach to more effective and efficient health and care (Greenfield et al., 2014). However, such approaches have faced scrutiny because they seemingly require people to fit within health care services, rather than ensuring services fit with the lifeworld of the individual (Greenfield et al., 2014; Hughes et al., 2022). Significantly, a study by Hughes et al. (2022) highlighted the complex personal and material contexts where resources may be drawn upon to manage one’s health, noting that current integrated care models, and thus person-centred care, fall short of meeting or supporting individualised needs.
Prior to the COVID-19 pandemic, models of CR programming remained largely unchanged for many years, with 75% of participants attending group-based, face-to-face programmes (BHF, 2020). The pandemic provided both a pause to consider and the necessity to try new approaches, giving opportunities to kick-start change in CR (Babu et al., 2020). However, in a recent BHF (2022b) report on CR participants’ perspectives, only half of participants reported receiving personalised support. Furthermore, a large void exists between the preference of the participant and mode of care received, for example, where the preference for face-to-face exercise delivery was replaced with virtual and home-based provision (BHF, 2022b). Indeed, the impacts of the pandemic, such as staffing availability, continue to be felt in CR (BHF, 2022a). Whilst changes to CR programming, such as offering different exercise modes, may make programmes more appealing to some, such changes can have limited impact on others, particularly if they fail to give due consideration to people’s needs or ability to navigate this care. Similarly, provision of online synchronous or asynchronous programmes may appeal to some, but not all. This is despite the pandemic having the potential to increase people’s willingness to access virtual sessions and appointments (referred to by the NHS as ‘telehealth’) more so than perhaps previously (Son et al., 2021). Thus, there continues to be an opportunity to consider how CR is planned and delivered in a more person-centred way, whilst appreciating that ‘more of the same’, even when tweaked, is unlikely to create the required fundamental change.
Alongside this, most studies investigating CR effectiveness sit within the biomedical field and/or have little theoretical framework. Sociological research provides a critical contribution to the often dismissed, ignored, or marginalised in-depth understandings relevant to health care (Fraser et al., 2019). Encouragingly, a growing number of sociological and ethnographic studies explore engagement in and with CR (e.g. Angus et al., 2018; Evans & Crust, 2015; Meredith et al., 2019). There remains, however, a dearth of research with participants who decline CR or drop out, or with significant others. This article seeks to address that gap and contribute to the body of qualitative literature on CR participation as well as to generate insights that could enhance person-centred service provision.
Having introduced the subject and relevance of this study, we next set out the theoretical perspective, followed by our methodological underpinnings and approach. The results and discussion are presented as a combined section to support the detailed exploration of the two themes relevant to the topic of person-centredness and the potential association with non(participation) in CR. A conclusion and further avenues for research complete the discussion.
Using a Bourdieusian Perspective
This qualitative study engages with the theoretical framework of Pierre Bourdieu whose ideas draw on the notion that there is no single reality that is objectively ‘knowable’; he labelled his approach as ‘structuralist constructivism’ (Bourdieu, 1989). Constructivism considers humans as social agents, generating knowledge and meaning from their own experiences. Bourdieu’s structuralist aspect, moreover, examines the structure of society and how this can influence experiences (Kauppi, 2002). Bringing both agency and structure into one theoretical perspective enables the putative dichotomy between the two to be bridged.
Bourdieu utilised the concepts of habitus, capital, and field. Habitus constitutes a system of durable dispositions (e.g. inclinations and tendencies) offering both a structure and structuring (Bourdieu, 1977), based on past social conditions and the shaping of present and future practices (Maton, 2014). Capital involves resources held by people or groups, which have social value that can be deployed, exchanged, and transformed within fields (Bourdieu, 2006). The main forms of capital discussed by Bourdieu comprise cultural, social, economic, and symbolic capital (Bourdieu, 1986). As a subset of cultural capital, physical capital (Bourdieu, 1978), pertaining to the body, is pertinent to the current analysis. Bourdieu (1994) described a field as a system of social positions structured by power relations. Field theory assists in understanding the interconnections between habitus and capital (Watson & Grenfell, 2016) and thus brings the discussion full circle in considering how agency and structure are bridged in Bourdieu’s theoretical framework.
Resulting from the interplay of these concepts, specific forms of practice emerge, each intertwined with several other concepts: doxa relates to an individual’s taken-for-granted beliefs about the social world, for example, their expectations of health care; illusio, the belief in the value and worth of the stakes in a particular field; nomos, the rules and laws of the field, either implicit or overt; and finally, hexis, the bodily display of the habitus (e.g. posture, demeanour, and accent). There are, however, likely to be instances where the field may feel incompatible with the habitus, termed hysteresis by Bourdieu (2000). Although rarely without challenges, hysteresis can be overcome through reflexivity and adaptation.
Bourdieusian theory was therefore considered highly relevant to the exploration of the person-centredness of cardiac rehabilitation. This framework provides a powerful means to examine and understand why some people make the health and health care decisions they do, and in particular identifies the specific structural and agentic influences that shape and guide people’s decision-making processes. Further, an appreciation of these influences enhances our understanding of different ways to approach personalisation in the context of CR.
The Research
Ethical approval was gained from the relevant Health Research Authority and Research Ethics Committee (reference: 19/YH/0183). The ethnographically inspired study aimed to generate rich, detailed, and potentially complex data, allowing the richness of participants’ experiences to shine through. As is typical in ethnography, the research utilised “multiple methods to gain a comprehensive understanding of the social environment and perceptions of the members of the social group” (Kraine & Baird, 2005, p. 87) being studied. Participant observations varied in length and number according to the participant (2 hours was the minimum observation time) and as permitted by COVID-19 restrictions in place. Observations were undertaken during CR attendance or in everyday environments such as at home. Repeated semi-structured interviews (n = 26 in total) and researcher reflexive journaling were also used. Here, we engaged in Bourdieusian reflexive practice, and journaling was engaged in such a way as to ‘work on oneself’. Bourdieu argued that one’s ability to do reflexive work is influenced partly by the structures within the habitus and partly by the objective conditions at the time the work took place (Bourdieu & Wacquant, 1992). In this case, the authors had differing positions in relation to the field: the primary researcher was a ‘cultural insider’ and held a BACPR-accredited exercise instructor’s qualification in cardiac rehabilitation. Another author also had specialist exercise instruction experience, whilst the other two members of the team held more ‘outsider’ positions to the cardiac rehabilitation field and provided more critical distance on the analysis. Bourdieu’s notion of doxa is apposite, as it can be used to describe a researcher’s ‘natural attitudes’ and taken-for-granted assumptions (Deer, 2014). Bourdieu described this as breaking with doxa, such that reflexivity aids the researcher in bending back on themselves, so as to rupture common-sense thinking (Bourdieu & Wacquant, 1992). Such participant objectivation (Bourdieu, 2003, p. 282) involved the application of Bourdieusian concepts (such as field, habitus, and capital) to the analysis of the researchers themselves (see Grenfell, 2018). Thus, the research team continually questioned the nature of the sociological analysis, their relationship with the world that is assumed, and the instruments of construction (Bourdieu & Wacquant, 1992) through recording daily processes, methodological decisions, and personal reflections and producing an audit trail.
Participant Recruitment
Participant Characteristics.
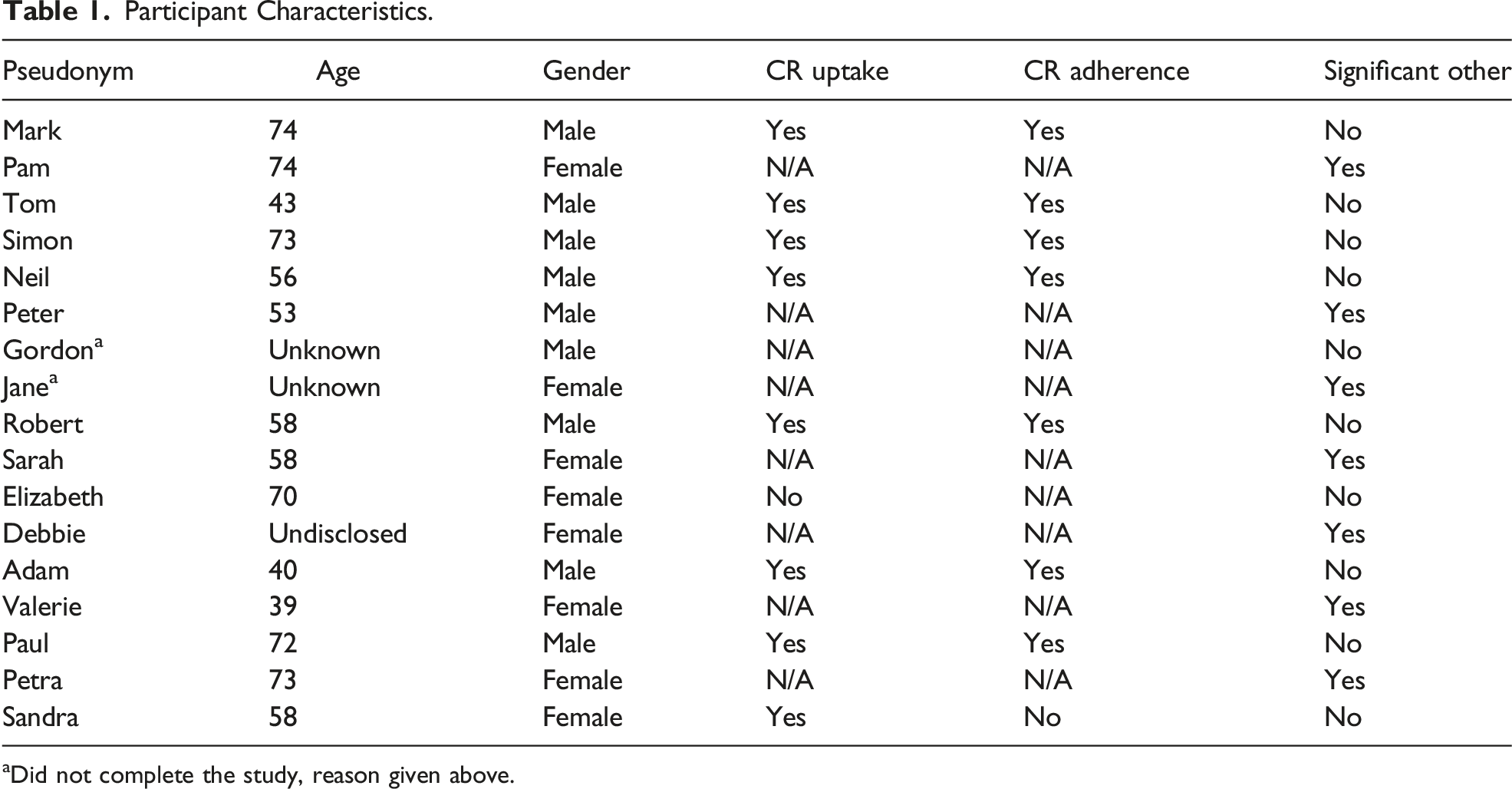
aDid not complete the study, reason given above.
Methods
A period of familiarisation took place prior to commencing participant observations, which aided rapport-building with participants and CR staff. Observations explored details such as where individuals positioned themselves within a CR session and sensory displays such as pleasure or pain. Observations continued for 6 months and helped inform interviews, the first of which were conducted between months 1 and 3. However, the restrictions created by the COVID-19 pandemic required a change in approach for the second phase of data collection. All second interviews were conducted online (Zoom or Teams platform) or via telephone, according to participant choice. Observations in these circumstances were understandably hampered and rendered impossible when the participant opted for telephone contact. Observation data and findings from the first-interview round informed the second interviews drawing on issues identified by the primary researcher as of interest, such as teasing out further detail about the influences on declining CR attendance. Brief field and voice notes were made in the field and written up in detail as soon as practicable afterwards. Three field diaries were used, one each for the two CR teams and one utilised as a reflexive journal (see below).
Interviews adopted a semi-structured approach, providing some structure but enabling the researcher to be responsive to the participant’s account. Participants were asked to reflect on the social and biographical context of their illness, to help ascertain how their experiences had been shaped by the structural aspects of social positioning vis-à-vis habitus, field, and capital positioning (Bourdieu, 1996). Second interviews provided an opportunity to revisit, revise, and refine accounts (see Bourdieu, 1999). Each interview was recorded and transcribed verbatim.
Commensurate with Bourdieu’s approach, ongoing reflexive practice was undertaken to acknowledge researcher influence and its potential to shape the topic of inquiry (Grenfell, 2018). Reflexive diary entries were made by the researcher and used to record daily processes, methodological decisions, and personal reflections (see McGrath, 2021). The biography and positionality of the first author/primary researcher was an important point of reflection. A background in CR exercise instruction provided partial insider status and shared cultural grounding, for example, in understanding CR exercise prescription. This aided rapport with CR staff and research participants, permitting access to interactions and conversations that might not have been available to a complete outsider (see Hammersley & Atkinson, 2007). Nevertheless, an awareness of the fluidity, mutability, and context dependence of researcher ‘insiderness’ (Allen-Collinson, 2013) was maintained through ongoing reflection, journalling, and dialogue with critical friends, who provided “a theoretical sounding board” to encourage reflexivity and constructively challenge interpretations (see Smith & McGannon, 2018, p. 113).
Data Analysis and Rigour
Reflexive thematic analysis was used to identify, analyse, and report themes within data and assist in the organisation and description of data (Braun & Clarke, 2019). Both inductive and deductive coding and theme construction were undertaken by the first author using a paper-based method, to enhance data immersion and familiarisation. Furthermore, reflexive diary entries were revisited alongside field notes and interview transcripts to provide context and enhance understanding (see McNarry et al., 2019). Codes and the eight broad themes were subsequently discussed with other research-team members as ‘critical friends’ who sought constructively to challenge initial interpretations and suggest alternatives (Smith & McGannon, 2018). Five themes were identified, and here, we focus upon data pertaining to ‘the influences on attendance at CR’. Other themes were also identified, including ‘the influence of others’, ‘material conditions and personal biography’, ‘the cardiac event’, and ‘relationships with health professionals’, and we present intersecting data from these themes, when relevant to our focus upon influences on attendance at CR.
Judgement criteria appropriate to the structural constructivist epistemological approach were employed to assess data quality and were selected to support the construction of a narrative that would invite transferability (Richardson, 2000; Sparkes & Smith, 2009; Tracy & Hinrichs, 2017). Criteria included worthy topic, analytic rigour, researcher sincerity through honesty and transparency, reflexivity, robust ethical considerations, expression of participants’ reality, and transferability (as relevant to naturalistic generalisability (see Smith, 2018)). These considerations for data quality followed through from data analysis into the results and discussion, to which we now turn.
Results and Discussion
In this section, key findings pertinent to CR non(participation) and the notion of person-centeredness in the context of CR are discussed, including the impact of, and on, the primary and secondary habitus, upon the deployment of existing and new capital, and navigation of the field. Pseudonyms are used throughout, and locations anonymised.
Shaking the Habitus – ‘The World’s Against Me’
The aim of the NHS pathway is to offer CR relatively rapidly post-cardiac event. The BHF (2020) identifies national waiting-time targets for CR commencement as 42 days for surgical and 28 days for non-surgical patients. However, early introduction does not always occur, or might be unacknowledged by the patient, sometimes due to immediate concerns following the cardiac event, as explored in detail below.
An NACR report stated that “the sooner patients engage with the CR process, the more likely they are to start, resulting in increased uptake” (BHF, 2020, p. 20). Data from this study do not necessarily support this assertion, however. Indeed, early discussions about CR were found to catch some patients ‘off guard’ coming too soon following their cardiac event and lacking clarity regarding CR itself, as captured in a fieldnote from a CR education session discussing uptake: Neil [patient-participant, aged 56] talked about his experience, his initial lack of understanding about CR, and mentioned a short introductory video would work well, showing people around, introducing people and just generally providing an insight into what to expect. He also talked about the stage at which the programme is introduced, who introduces it, and that this is timely for the person. This seemed to be supported by nods from others. Robert [patient-participant, aged 58] talked about the phone call he received, and the way CR was offered to him, including the information given, saying that in that moment it’s easy to say no, that you get so many phone calls where you’re just used to saying no and when you’re not completely sure who is on the phone. The CR nurse countered that, saying that they follow up with paperwork, but Robert [reported he] didn’t receive any paperwork.
Initial thoughts following the offer of CR were further discussed during a second interview with the patient-participant, Robert: Robert: I thought I’d be better off going back to work than going to a ‘keep fit’ exercise course, I couldn’t see the benefits. I suppose that I had the same thoughts when I was offered it again this time [after second cardiac event], you know I feel ok, let’s get back to work, let’s just crack on with it. So, I decided that I wasn’t going to participate. Interviewer: Why do you think people decide not to go? [to CR] Robert: … could be that initial rush after the operation makes you feel like: I don’t need that I feel like a new man, that’s possibly one reason. Er, and the fact that you just want to get back to a routine that you’re used to, get back to work, and suppose it could be different for someone that isn’t working. And it was also potentially in the early days not knowing how work would … or whether they would even allow me to do it without any kind of penalty or loss in earnings. So perhaps a little bit more time in the early days to give you a chance to look at all the ins and outs and then make a decision, rather than expecting a decision over just like that over the phone. I don’t know whether that call came too early after the procedure … I think I’m pretty sure it was within the first week … perhaps waiting a little bit longer before being offered it.
Analogously, patient-participant Mark (74) described his feelings about his cardiac event: “it wasn’t the crushing blow they say a heart attack is,” leaving him with an initial surge of positive feeling following surgical intervention. Mark considered that the problem had been ‘fixed’, and CR would not achieve further improvement. The sense of restoring order to one’s life emerged as important for participants, particularly in instances of protracted symptoms deleteriously affecting quality of life. Furthermore, unease was expressed about balancing the need to return to work and taking time off to attend CR, as demonstrated above by Robert’s concerns about the potential loss of income. Others talked about the need to maintain caring and/or domestic responsibilities. For example, Simon (73) was his wife’s main carer alongside looking after their home: I still did the housework … I had to do it at my pace I couldn’t exert myself.
Here, it can be seen how a cardiac event can shake or indeed reaffirm the primary habitus. When CR is offered soon after the cardiac event, participants’ decisions were sometimes made pre-reflexively, strongly shaped by primary habitus and dispositional schema, as well as by doxic assumptions about what might be involved in terms of leveraging economic, physical, and symbolic capital. When complex material conditions and personal biography are also involved (such as family history of ill health), the durability of the primary habitus, formed in early life, is often demonstrated through the pre-reflexive acts of the patient: I wouldn’t go on my own and join something [CR] … I never liked PE always found an excuse, never been a gym person, no nothing like that. … there must be people like me who just don’t want to talk about it [heart attack]. … I don’t want to be seen [as] I can’t do that, I just get on with it. I mean both of parents died at 60 and 63, so for me to make 70 has gobsmacked me. I never ever ever thought I would live this long, so I feel like I’m living on borrowed time anyway. (Elizabeth, patient-participant)
In their Bourdieusian CR study, Angus et al. (2018) similarly outlined how accessing CR can make one appear to others as incompetent and unable to self-manage, and this was particularly notable in those who felt undermined by their life circumstances. Indeed, the adjustment to or loss of a social position through employment uncertainty or lack of support from others, for example, can make behaviour change additionally challenging. When fearing that one’s social position could be negatively affected (Angus et al., 2018), CR can add another commitment to an already complex life and may be perceived as interference to the restoration of physical, symbolic, and economic capital (and thus social positioning), which might have already been adversely affected by illness (Angus et al., 2015). Maintenance of social position, restoration of social dignity (or symbolic capital), and concerns about loss of economic capital were notable concerns for many participants in the present study and can also relate to the requirements of other fields, such as caring responsibilities. This was observed in Debbie’s reasons for her significant other’s decision to decline to attend CR: [Her] finances were all in the air, so fuel in the car to get there and back doesn’t sound much but trying to do that on top of everything else was a bit of a concern for her. Erm parking, paying for parking, it was all the cost at the time because of what had been going on outside of all of this [relationship breakdown] was a bit of a concern for her. … I think she knew enough and had access to enough to not think that she needed anything. … [I think she thought] ‘the world’s against me going so I’m not going’ but I don’t know what benefit it [CR] would have had if I’m honest.
This observation aligns with extant literature in terms of social and economic barriers to CR (Angus et al., 2015; Clark et al., 2012), when acknowledging that living with a long-term illness can create existential uncertainty, as well as economic pressures.
In times of existential crisis, such as during recovery post-cardiac event, the ability to accumulate capital and/or exchange capital to sustain one’s social position in a field (economic and cultural capital via employment, for example) can be challenged. Consequently, the degree of change and level of risk were evaluated as part of the process of hysteresis and reflection caused by the cardiac event and based on what the patient-participant was prepared to accept. Patient-participant Elizabeth (aged 70), for instance, experienced a life patterned by ill health, both personally and amongst her family. She stated that “these last few years it’s just been one thing after another.” She was not the only participant to express such feelings following repeated episodes of ill health and mal events, and when asked about CR, Elizabeth tended to talk more about the wider context of her life. Some elements of practice she felt were within her ability to change, and others seemed incompatible with her primary habitus, including spatio-temporal restrictions on attending CR: It’s not like I’m in a town and I can get to places easy. It’s the drive out everywhere, it’s just the hassle of doing it, and I know it sounds stupid cause I’m retired, and I’ve got all day every day, but it’s the being tied to something like that ... so that doesn’t appeal to me at all. I suppose if I was a more sociable person, I’d go for the social side but that doesn’t interest me.
Relatedly, Bourdieu (1984; 2000) argued that people are inclined to live with what they know and understand, with relevance to the notion of belonging. Elizabeth is familiar with her surroundings, and she describes a place where she is able to ‘fit in’, whereas attending CR would require her to ‘step outside’ into social spaces where she might not feel comfortable and where her primary habitus would be less relevant. Importantly, rurality, alongside gender, ethnicity, and deprivation, was noted for the first time in reference to inequalities in the 2022 NACR report (BHF, 2022b). The report also highlights concerns about modes of CR potentially being determined by urban or rural location rather than according to the preference of the participant (e.g. rural residents provided with virtual CR and urban with in-person CR). Bourdieu’s conceptualisation of habitus incorporates past social conditions, therefore including material conditions and personal biography, as subjective structures, and portrays how these shape present and future practices as structuring (Bourdieu, 1977, 1990). Thus, whilst the impact of illness can create opportunities for the habitus to adapt and change, this is filtered by one’s lived, embodied experiences. ‘Biographical disruption’ describes the renegotiated embodiment that can occur when everyday life is disrupted by illness (Bury, 1982), akin to ‘shaking’ the primary habitus. Thus, the primary habitus may be restored or shifted in response to events, resulting in a habitus clivé or, eventually, a secondary habitus. The limits of the primary habitus are, however, expressed through thoughts, feelings, and actions. When these expressions do not align with contextualised expectations, however, such as the prevailing doxa within the field of health care, hysteresis occurs and produces the so-called ‘Don Quixote effect’ (Bourdieu, 1979, 1984), whereby there can be a delay in the development of strategies in response to a change of positioning (Mouzelis, 2007). In short, it takes time for a habitus clivé, or secondary habitus, to develop – and participants in the present study did not engage in CR for sufficient time for this to occur.
Specifically, in the quotes above, Debbie and Robert both remarked that they failed to see the benefits of attending CR. In Robert’s case, because his occupation was physically demanding, he considers such activity sufficient to benefit his cardiac recovery (see also Bäck et al., 2017; Dale et al., 2015 regarding occupational activity following a cardiac event). Robert did eventually change his mind following his second cardiac event, however, suggesting there is a limit to the extent to which the primary habitus determines behaviours. Indeed, he had previously expressed concerns about whether work commitments would allow him to attend, risking a potential loss of social position through reduced economic and cultural capital. However, upon raising his concerns, Robert’s employer agreed to flexible working to accommodate CR attendance. Without this employer support, it is unlikely Robert would have decided to attend. Relatedly, in their study of CR, Angus et al. (2018) noted how concealment of severity of illness could occur as a strategy to protect economic and physical capitals, particularly when discrimination in the workplace was a concern. Age and life stage were key variables here: where those eligible to attend CR are of working age, the opportunity costs of attending CR can involve different sources of capital than for retirees, for example, economic capital accrued through wage labour. Our findings add to the specific literature on CR uptake and adherence in working-age individuals (see, for example, Madden et al., 2011) and contribute to discussions regarding which activities can constitute effective CR (including whether occupational activity is considered beneficial) and about programmes undertaken outside of working hours and/or in asynchronous formats, such as via pre-recorded media.
A belief and/or “corporeal investment” in the significance of the ‘game’ (Pouliot & Mérand, 2013, p. 33), which in this case is CR, illustrates the applicability of the Bourdieusian concept of illusio. The presence of illusio reveals a connection between one’s habitus and the field, and without illusio, it can be difficult to rationalise potential benefits from engaging with CR. Thus, there may be a lack of motivation to attend, as highlighted in extracts from Debbie and Robert above. Reflexivity, such as that prompted by the engagement of Robert’s employer, enabled his consideration of CR as a ‘legitimate’ health-giving practice.
Dispositional Inclinations Towards an Active Secondary Habitus
Within the context of material conditions and personal biography, dispositions are important because they display beliefs, feelings, and perceptions and reflect the habitus, both primary and otherwise, indicating what might be deemed acceptable or not (Williams, 1995). In Bourdieusian terms, the interplay between habitus, capital, and field produces ‘game sense’ as part of the theory of practice (Bourdieu, 1977, 1984). Relatedly, Rowlands and Gale (2017, p. 8) described practice as “a window through which the habitus can be seen and understood.” The robustness of dispositions renders them useful in different social situations. As identified above, however, attending CR is likely to require a change to habitual practice and to doxa, and the often deeply embodied nature of this practice makes this challenging (Angus et al., 2018). Moreover, Bourdieu (2000) stated that dispositions may be difficult to hold together in trying situations such as in the face of ill health, which influences the ability to change and, possibly, to negotiate hysteresis and develop a secondary habitus.
Whilst physical activity challenges are not unique to CR, as a therapeutically mandated approach to ill health, influences on the decision to participate in CR have been highlighted as particularly varied amongst our participants. The perceived value of having dispositions that support physical activity engagement is recognised (Palmer et al., 2018). As a social ‘thing’, physical activity can be limited or supported by the social worlds one inhabits (Guell et al., 2016), with class (ergo capital distribution) and gender also key elements (Palmer et al., 2018). Early life experiences shape the primary habitus and therefore dispositions towards physical activity (Palmer et al., 2021), and, as Bourdieu (1984) argued, social class plays a role in both preference for specific activities and the level of engagement in physical activity. The relevance of being brought up in an environment where physical activity is supported was characterised by patient-participant Neil (aged 56), who described his middle-class childhood as being filled with outdoor activities. His continued enjoyment of outdoor activities he attributed to “just the way I was brought up.” Neil and several other participants described material conditions that involved both the opportunity and resources to engage with physical activity. Relatedly, research by Wiltshire et al. (2019) found a dispositional desire to seek opportunities for physical activity can persist into adulthood, despite the possibilities often being contingent on the limits of one’s social position.
Across the life course, disruptions to physical activity practice often occur (Palmer et al., 2021), for example, due to work, illness, or caring responsibilities. The “increased self-awareness of the body’s fragility” and the ephemerality of physical capital as one ages (Palmer et al., 2018, p. 950) can result in the ability to ‘move more’ being associated with many other factors that might disrupt routines, such as the effectiveness of medication, changes in the weather, and family needs (Phoenix & Bell, 2019). Indeed, several participants described how ‘life’ had influenced their dispositions regarding physical activity. Patient-participant Robert, for example, noted how his dispositions towards physical activity changed as his career progressed: I became a supervisor which made me more sedentary, more of an office-hours job, and I suppose really about that time I stopped exercising and concentrated on the career side of things.
Having taken on a sedentary job in early adulthood, patient-participant Neil explained how a game of football reignited his early dispositions towards an active habitus: I can remember I played five-a-side football for X [employer]. I was only in goal and it damn near killed me, I thought to me self, I’m knackered. I thought bloody hell, this ain’t right, so I just started getting fit from that day on.
Whilst for Robert his second cardiac event initiated his return to physical activity, for Neil his primary habitus and body schema were re-awakened by awareness of the decline in his physical capital in early adulthood. From then, and up to the time his cardiac symptoms became more severe, he had led an extremely active life, engaging mainly in outdoor activities, practices with which he was familiar due to his primary habitus.
Importantly, pain and fear post-cardiac event were highly salient to physical activity engagement; patient-participants had experienced significant traumatic health events, the ongoing consequences of which, particularly to their physical capital, were unknown. Fears about future adverse health events and the appropriateness of physical activity were often recounted, regardless of whether participants attended CR or not: I don’t take them [the dogs] out since I’ve had me heart attack because we’re on the hill, there’s a big dog walking field over there [points to the right]. Wherever I go I’ve got to come up this hill to get back home. I go with my granddaughter at weekends occasionally. I’ve done it once on my own, but I think it’s the fear that if anything was to happen, I’ve got this hill to come up. (Elizabeth/patient-participant/did not attend CR) [I would like to] go out for a bike ride, it’s not so much the getting out of breath at the time, ‘cause you get out of breath doing exercise, but it’s the time to take to recover afterwards. That’s the difficult part when you’re getting the chest pains and the little niggles ... you’ve got this constant reminder that you’ve had this incident happen. So now anytime I get the chest pain you’re like well why is that? (Tom/aged 43/patient-participant/attended CR)
These data indicate that despite the policy focus on behaviour change, factors other than motivation and the desire to lead a healthy lifestyle are required in negotiations regarding becoming and remaining physically active (Palmer et al., 2018; Phoenix & Orr, 2014). Accordingly, knowledge about the individual, their primary or secondary habitus, and existing capital resources in relation to CR are highly likely to be important considerations in person-centred approaches.
Secondary socialisation is also an important factor. For patient-participant Neil, his active secondary habitus was particularly characterised by his time in the military, where he was able to display symbolic capital (both to himself and others) through his determination and physical capabilities. The impact of military socialisation and discipline on physical capital was notable regarding four participants. As portrayed in Hockey’s (1986) ethnography of the UK military, the strict mind–body discipline regimes in military settings can result in feelings of greater control of bodily states and, in Bourdieusian terms, in influencing dispositions related to being physically active. This was characterised by patient-participants Mark and Neil, who explained: Mark: That’s the thing that was drummed into you in the forces, to stay fit and healthy. Neil: I don’t think it ever goes, there’s an old saying ‘once a Marine, always a Marine’ you don’t lose that ... it’s not so much the type of person that you are – whether you’re a decent, honest guy or girl sort of thing like, but it does affect your attitude to the way you do things.
An interest in being physically active was highlighted by all four ex-forces participants, who described opportunities to try different sports, physical requirements of the job, and a lived sense of needing to ‘look after oneself’. All had continued their physical activity into civilian life, although degrees of engagement varied. This like-mindedness is similar to the class habitus identified by Bourdieu (1984), where similar dispositions and lifestyles become ingrained. Secondary socialisation can be highly influential on subjectivity and the secondary habitus and can result in the development of new dispositions (secondary habitus) shaping engagement in physical activity. However, our research findings indicate that the durability of the primary habitus vis-à-vis physical activity was notably strong across the life course, evolving rather than being split. This evolution was noted particularly in participants with military backgrounds and shaped their experiences of physical activity, building on the primary habitus.
Contrastingly, where material conditions, possession of capital, and personal biography do not support the opportunity or resources to be physically active, the dispositions developed can lead to development of a primary habitus less inclined to physical activity. Patient-participant Elizabeth, for example, described her disdain for physical education at school, explaining that there was “nothing I stuck at” and nothing that interested her regarding extra-curricular physical activity. In adult life, she had “never been interested in attending gyms” but enjoyed walking around the shops and occasionally walking her dogs. However, her explanations immediately led into details surrounding her myocardial infarction recovery and how that not only limited her but made her fearful of doing things on her own, despite not being keen on group situations, reflecting both her habitus and lack of social and physical capital. Although dispositions towards physical activity can develop later in life (via secondary socialisation and development of a secondary habitus), in Elizabeth’s case this had not happened. Even when physical activity was suggested by health professionals as a health-promoting practice, for Elizabeth this was not considered sufficient incentive or ‘legitimacy’. Indeed, studies have shown how perceived legitimacy is an important part of both becoming and remaining physically active (Palmer et al., 2021; Tulle & Dorrer, 2012). As discussed throughout this section, dispositions towards physical activity initiated in early life often sow seeds that can then be developed in later life.
The above analysis of CR and physical activity dispositions, and how these might evolve, enhances understanding of participants’ habitus and how it is demonstrated through bodily hexis and practice, for example, the extent to which a participant is dispositionally inclined towards fields involving group situations and exercise, and whether these dispositions have been impaired by ill health. Personal biography and material conditions relate to the capital held by participants and the ability to accumulate and exchange capital, for example, in one’s perceived ability to enter and attend unfamiliar settings or the perceived competence to perform exercise techniques.
Conclusion
CR in its current format risks undue generalisation, by placing all patients on pathways with predefined options and timeframes, prioritising clinical outcomes above agentic and structural socio-cultural influences on the individual. This can strongly influence engagement with CR (remaining around 50% of those eligible, for at least the last 15 years). Particularly germane to this article, the CR approach taken can overlook how the fields of health care and CR are navigated, utilising (or not) primary habitus and capital, and thus fail to consider the relevance of personal biography and material conditions. Whilst participants’ preferences in relation to flexible and hybrid models of CR might be important in the evolution of services, preferences are constrained by what is currently offered and when/how it is offered.
Person-centred CR should be relational to the person and the socio-cultural contexts within which they are embedded. Decision-making and discussion associated with the introduction of CR is a good example of this, as identified in our data. Patients should be considered by health professionals in the context of their own life journey, habitus, and capital resources held, in addition to the field of CR and how this may be navigated. This includes how a patient could be best supported to adapt their bodily hexis and restore (or gain new) capital following the biographical disruption caused by a cardiac event.
Our research findings raise further questions around whether the medical model of illness actually serves the needs of the cardiac patient, or if patients could be more effectively supported to ‘self-rehabilitate’ in a manner commensurate with their material conditions and personal biography (as relevant to age, gender, and social class), based upon the capital at their disposal, or which they might be encouraged to develop within their already established fields (e.g. work and/or hobbies).
Nevertheless, it is important to emphasise the benefits and positive aspects of CR, alongside the challenges portrayed. What this study adds to the literature is an exploration of the ways in which socio-cultural influences on CR uptake are both important and complex, and the known benefits have the potential to serve only those who access the required fields. Our research contributes novel insights into the limited impact of current policies that are primarily focused on individual action and responsibilisation and utilise only a medicalised view of exercise and health. Whilst this research has begun to investigate the wider socio-cultural influences pertinent to cardiac patient journeys, it is hoped that health professionals and managers working in CR might draw comparisons with their own experiences and consider the transferability of the findings of this study to their own settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a dual PhD studentship funded by the University of Lincoln and the University of Copenhagen, and a Mildred Blaxter Post-Doctoral Fellowship from the Foundation for the Sociology of Health and Illness.