
Abstract
Adherence to the treatment of type 2 diabetes (T2D), which includes the use of prescribed drugs, following a healthy diet, and adopting a physically active lifestyle, is important to control the disease and improve the patients’ quality of life. The present study aimed to explain the determinants of adherence to treatment in patients with T2D based on Pender’s Health Promotion Model (HPM). The present research used a qualitative content analysis and was based on Pender’s HPM. The data were collected through in-depth semi-structured interviews with 20 T2D patients using a purposive sampling in Bandar Abbas, southern Iran. Maximum variation was considered in terms of gender, age, history of diabetes, type of drug used, education, and occupation. The data collection continued until data saturation. At the same time, the collected data were analyzed using the directed content analysis. MAXQDA 10 was used to manage codes and facilitate data analysis. The data analysis led to the extraction of 10 categories and 19 subcategories as the determinants of adherence to the treatment of T2D patients. The participants shared their experiences about personal characteristics and their ecological environment, specific cognition and emotions, and the behavioral results and experience as the determinants of adherence to T2D treatment. The categories extracted from this study in the form of HPM constructs provided a framework to explain treatment adherence. This information can help policy makers and planners in designing future programs.
Introduction
More than half a billion people worldwide live with diabetes, and this population is expected to increase to 783.2 million people by 2045 (Sun et al., 2022). Type 2 diabetes (T2D), as the most common type of diabetes, has become a global epidemic and is the major burden of healthcare worldwide (Reed et al., 2021). The highest relative prevalence of diabetes with 18.1% has been reported in the Middle East and North Africa (Sun et al., 2022). In Iran, a national study in 2021 showed that 15% of adults aged 35–70 have diabetes (Khamseh et al., 2021). Also, the prevalence of T2D in Hormozgan Province was reported to be 17.4% (Zoghi & Kheirandish, 2021).
T2D is caused by systemic disturbances in metabolic homeostasis. Genetic background and lifestyle are effective in the prevalence of the disease (Udler et al., 2019). T2D is associated with a significant morbidity and mortality (Sun et al., 2022). The behaviors recommended in the guidelines for T2D patients include the adoption of a healthy lifestyle, that is, improving dietary patterns, increasing physical activity (PA), and taking diabetes medication (Hallberg et al., 2019; Kaminski et al., 2022). Following these recommendations helps patients improve their quality of life (Majeed et al., 2021).
According to the World Health Organization (WHO), the definition of treatment adherence is “the extent to which a patient follows medical instructions” (Organization, 2003). Adherence to T2D treatment requires taking the prescribed medications, regular self-monitoring, following a healthy diet, and adopting a physically active lifestyle (Unni et al., 2022). Studies have shown that adherence to the treatment of T2D patients can lead to a reduction in emergency visits, the risk of hospitalization, and healthcare costs (Evans et al., 2022; Shani et al., 2022). However, adherence to treatment in T2D patients is less than optimal (Shimels et al., 2021; Weiss et al., 2020). In a review paper, the prevalence of non-adherence to treatment among T2D patients in the world is reported to range between 42% and 74.3% (Pourhabibi et al., 2022).
Considering the increasing rate of T2D, the problems caused by this disease, and insufficient adherence to treatment, the need to improve adherence to T2D treatment in all aspects of medication, diet, and physically active lifestyle seems essential. Identifying the determinants of T2D treatment adherence from the patients’ point of view can help design effective intervention measures. Previous studies mentioned the effective factors in adherence to T2D treatment included economic status, healthcare staff, family support, awareness, belief, health literacy, gender, complications, body mass index (BMI), and family history of diabetes (Hashimoto et al., 2019; Mannan et al., 2021; Pourhabibi et al., 2022). These factors include a wide range of individual, interpersonal, and external factors, and it is useful to use health promotion models that consider these factors. One insightful model with this respect is Pender’s Health Promotion Model (HPM), proposed in 1996. The HPM is highly comprehensive and helpful in understanding the factors that determine the behavior and interventions of adherence to the treatment of chronic patients including diabetes (Faroughi et al., 2021; Masoudi et al., 2020). Besides being effective in improving health promotion behaviors in patients, this model can improve awareness and psychological performance in diabetic patients, increase their self-efficacy, improve their understanding of the benefits of health promotion behaviors, minimize the perceived barriers, and increase interpersonal support and self-management (Lari, Noroozi et al., 2018; Lari, Tahmasebi et al., 2018; Ren & Li, 2022).
According to the HPM (Figure 1), factors influencing health behaviors includes three dimensions: personal characteristics and their ecological environment (consisting of microenvironment and meso-environment), specific cognition and emotions (with the core being self-efficacy), and behavioral results (Pender et al., 2015). Diagram of HPM.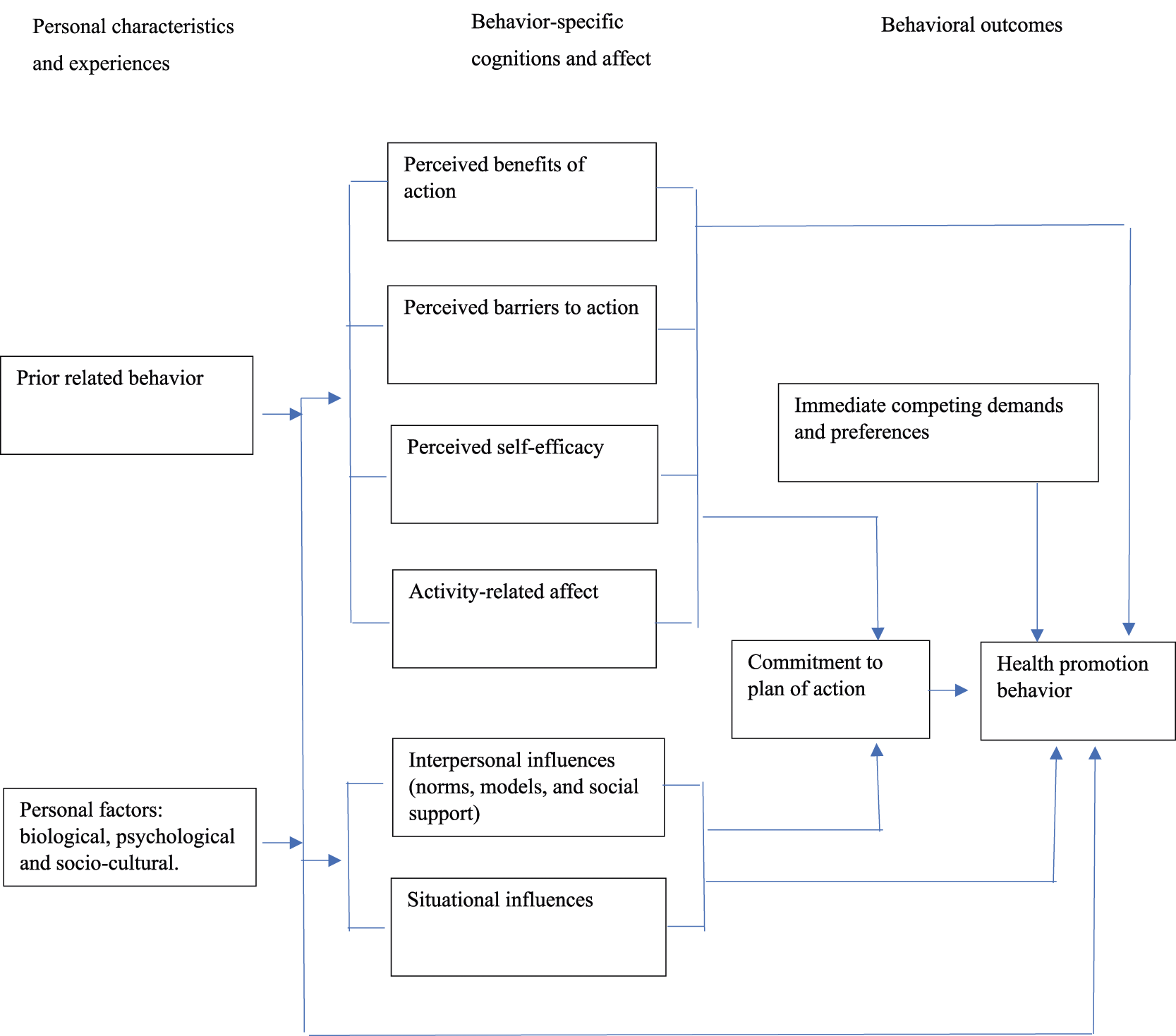
Considering that the determinants of treatment adherence can differ across different conditions, qualitative studies are required. In the related literature, most studies were cross-sectional. Most qualitative studies only dealt with pharmaceutical treatment (Bockwoldt et al., 2017; Rezaei et al., 2019), and were not based on the model, or did not address different individual, interpersonal, and external dimensions (Liu et al., 2018; Movahed et al., 2019). Therefore, it seems that conducting a qualitative study based on a suitable model that considers physical activity and diet in addition to pharmaceutical treatment is a fundamental step to strengthen the evidence for adherence to T2D treatment. Therefore, the present study was conducted to explain the determinants of adherence to treatment (medication, diet, and physical activity) of T2D patients based on the HPM.
Methods
Study Design
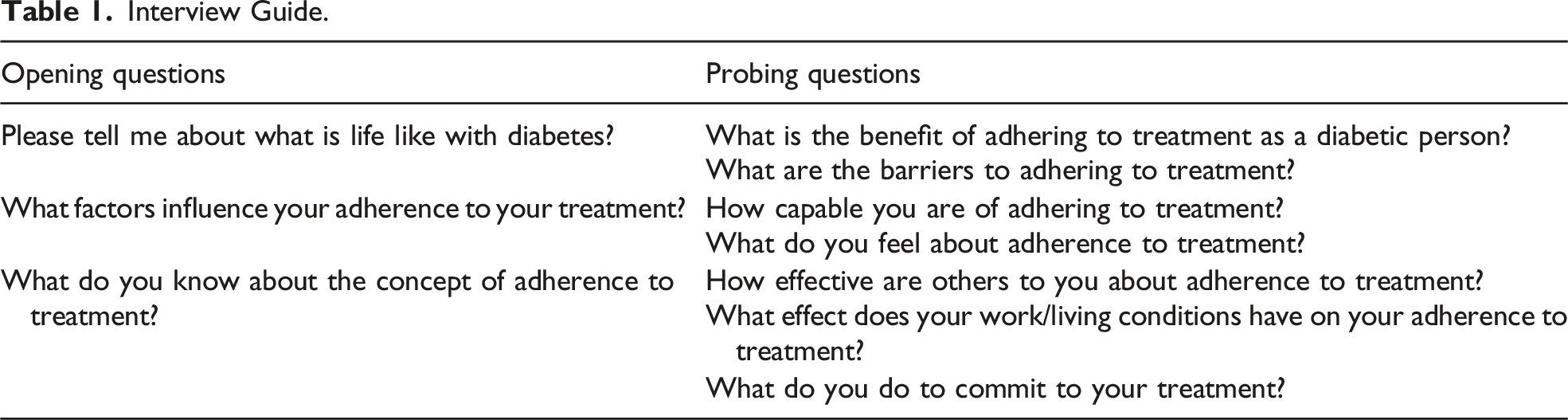
The present study used an in-depth semi-structured interview. A general interview guide was developed and used to facilitate the interview process. The reason for adopting a qualitative method was to provide deep insights into the individuals’ perceptions and experiences (Thomas et al., 2022), helping to gain a new perspective on issues that we have a little information about and also unraveling subtle details of phenomena that are difficult to express in a quantitative manner (Speziale et al., 2011).
We applied a directed qualitative content analysis to discover the determinants of treatment adherence in adult T2D patients. The directed content analysis is a common data analysis method in healthcare research in which the analysis begins with that theory as a guide for initial codes (Hsieh & Shannon, 2005). The theoretical framework of this study is Pender’s HPM (Pender et al., 2015).
Ethics Approval and Consent to Participate
The current research, which is part of a student PhD dissertation, was approved by the Ethics Committee of Hormozgan University of Medical Sciences (ethical code IR.HUMS.REC.1400.377). To ensure voluntary participation, informed consent forms were signed by the participants and permission was gained to record the voices. The interview files (typed files and recorded interviews) were kept confidential and saved in a separate folder encrypted. The interviewees were free to withdraw from the study upon request.
Setting
The present study was conducted among T2D patients living in Bandar Abbas in Hormozgan Province, southern Iran. Bandar Abbas has a population of 352,173, making it the largest city in Hormozgan. According to the data registry of Hormozgan University of medical sciences, 51,112 and 17,534 people have diabetes in Hormozgan and Bandar Abbas, respectively.
In Iran, in 2004, a comprehensive national diabetes program was initiated in both rural and urban phases, entitled as the National Program for Prevention and Control of Diabetes (NPPCD) (Delavari et al., 2004; Noshad et al., 2015). The NPPCD has three main levels for the prevention and control of diabetes. The primary level includes family physicians, urban healthcare centers, and private clinics. The secondary level includes public/private hospitals and specialty polyclinics. The third level addressed patients needing specialized care. This level includes specialty and subspecialty hospitals (Noshad et al., 2015). The primary level is free of charge in healthcare centers. However, services are not free in private centers and other levels, and T2D patients need to pay for services. The insurance coverage of T2D medical and pharmaceutical services may be different according to the type of insurance (e.g., social security insurance, medical service insurance, armed forces insurance, and supplementary insurances). In the present study, patients visiting the secondary and third levels were included in the study.
Participants
A total number of 20 T2D patients from Bandar Abbas city participated in the study and were selected through a purposive sampling method. These T2D patients had visited the medical centers of Bandar Abbas for their therapeutic measures, and in the meantime, an interview was held with them about their adherence to treatment (medication, diet, and physical activity).
In addition to the willingness to participate in the study, the other inclusion criteria in the present study were (1) definitive diagnosis of T2D and being under treatment for more than 1 year, (2) desire to share personal experiences about life with diabetes, and (3) being able to participate in interviews and share information and experiences. The data were collected from March 2022 to September 2022.
The participants entered the study through a purposive sampling. In this study, maximum variation was considered in terms of gender, age, history of diabetes, type of drug used, education, and occupation. The participants were told they could withdraw from the study whenever they wanted. The interviews were held after gaining the required permissions and setting an appointment with the patients. At the beginning of each interview, the researcher introduced himself and then explained the purpose and importance of the study. The informed consent form was completed by the participants who volunteered to take part in the interview.
Data Collection
Interview Guide.
Rigor
In this study, Lincoln and Guba’s criteria were used for data accuracy and to ensure trustworthiness (Lincoln & Guba, 1985).
It was attempted to ensure the validity of findings by reviewing the manuscripts and extracted codes, sending the data to colleagues, using their complementary comments, continuous review, and devoting enough time to collect the data. Also, member checking was done to increase the validity of findings. In a continuous review, researchers used data analysis concurrently with the data collection process. Also, enough time was devoted to the interview process (March–September 2022). In order to increase the transferability of findings, the samples were selected with maximum variety. Also, all the research processes and characteristics of the research population were recorded in detail by the researchers so that other researchers can replicate the study.
Data Analysis
At first, each recorded interview was transcribed verbatim, and immediately, the content of the interview was typed in Microsoft Word (2019 Professional Plus). Each interview was read several times for an in-depth understanding of the interview. In order to identify the primary codes or semantic units in the interview text, important phrases were highlighted and then divided into the smallest meaningful units (codes). The research data were analyzed using a guided qualitative content analysis approach based on Pender’s HPM (Hsieh & Shannon, 2005). The data were coded using predetermined codes (according to the model), and a new code was assigned to any text that could not be categorized with the initial coding plan. To facilitate the organization and analysis of qualitative data, MAXQDA 10 was used.
Results
Participants’ Demographics
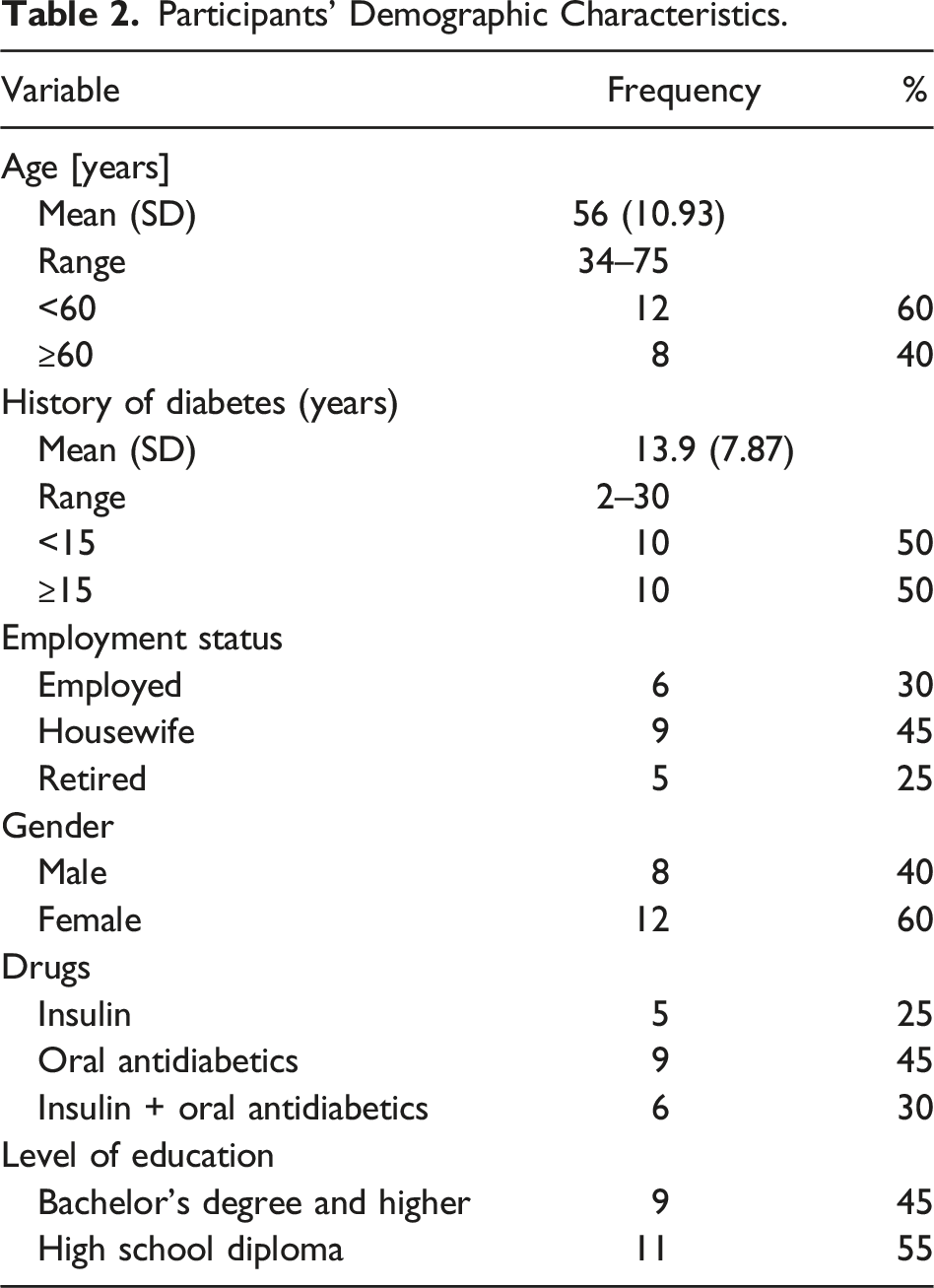
The participants’ age ranged between 34 and 75 years with an average of 56 ± 10.93 years. Their average history of diabetes was 7.87 ± 13.9 years. 60% of the participants were women and 45% were taking oral antidiabetics; 25% were using insulin and 30% were using insulin and oral antidiabetics.
Participants’ Demographic Characteristics.
Categories and Subcategories Extracted From the Analysis of T2D Patients’ Experiences.
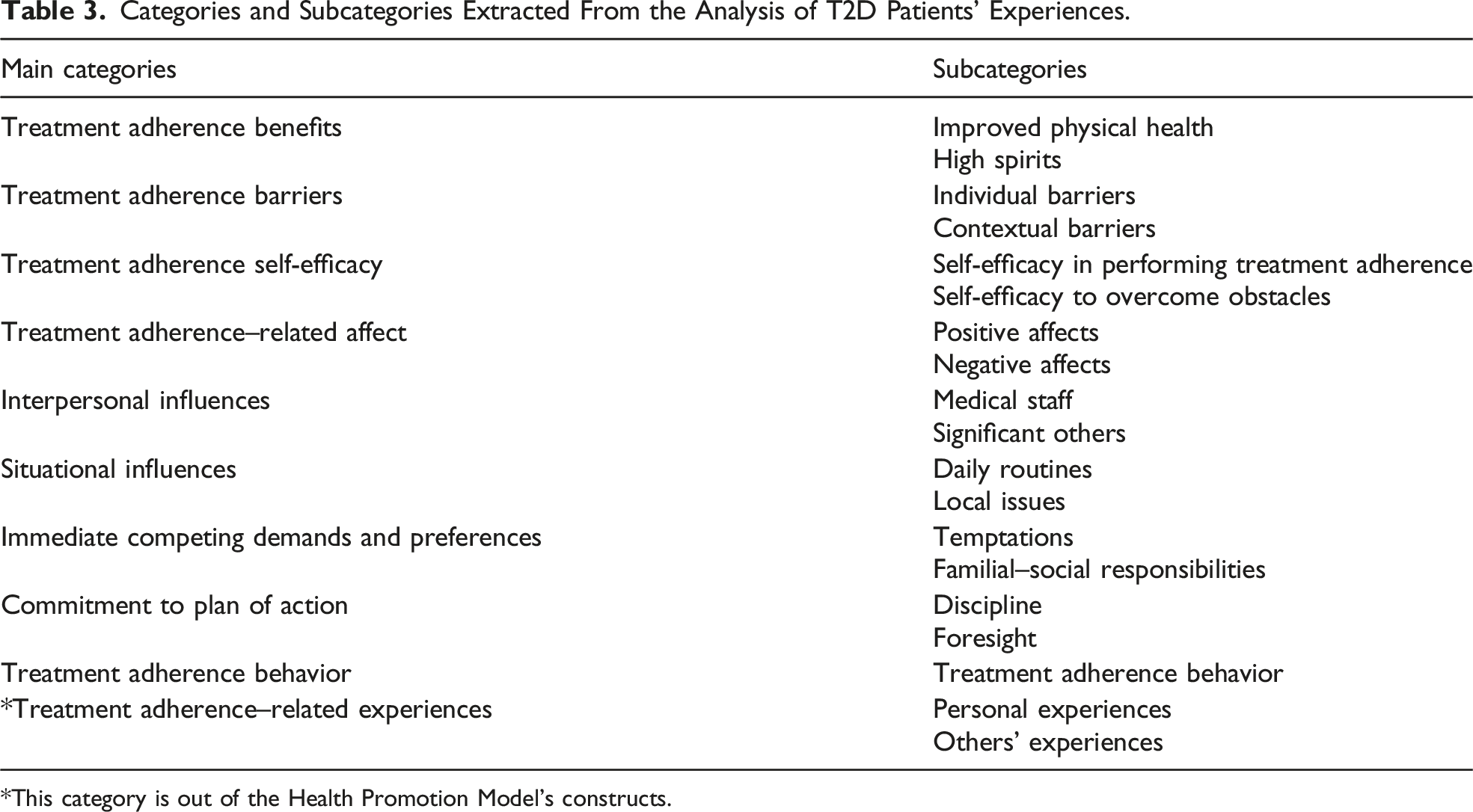
*This category is out of the Health Promotion Model’s constructs.
Treatment Adherence Benefits
The participants pinpointed the positive outcomes of adherence to treatment.
Improved Physical Health
Participants mentioned that adherence to treatment benefits their physical health. They mostly mentioned the benefit of adherence to treatment, reducing the complications of diabetes and improving their physical condition. The first benefit I gain from adhering to treatment is that it helps me to get physically fit and suffer from fewer side effects. (40-year-old man)
Sometimes, the stated benefits are not directly limited to their diabetic condition and affect them in appearance as well. By adhering to the treatment, I will lose weight and get fit. (48-year-old woman)
High Spirits
In the participants’ accounts, the benefits of adhering to the treatment for their mental state were mentioned too. Most participants talked about a better mood and the relief they experienced from adherence to treatment. When I am on a healthy diet, it helps control my disease and also positively affects my mood. (34-year-old woman)
Treatment Adherence Barriers
This category indicates the perceived barriers and the personal costs of showing T2D treatment adherence behavior. Barriers in this study are divided into two categories:
Individual Barriers
The barriers subsumed under this subcategory are those included in an individual’s private life, ranging from physical barriers to physical activities to the participants’ treatment costs and mental concerns. Economic status really matters to me and my adherence to treatment as a diabetic patient. For example, fruits are expensive and a diabetic patient must eat fruits and vegetables. (63-year-old man)
Contextual Barriers
Most participants mentioned contextual factors such as the low availability of healthcare services and insurance. Finding insulin and needle tip, which are often rare, is very annoying to me. (56-year-old man)
Treatment Adherence Self-Efficacy
The participants spoke of their belief in their ability to control diabetes by correctly showing treatment adherence behavior and coping with barriers.
Self-Efficacy in Performing Treatment Adherence
The participants’ personal belief in the correct T2D treatment adherence behavior was also raised. They talked about the ability to perform physical activity, live on a proper diet, the ability to recognize hypoglycemia based on symptoms, inject insulin, and interpret test results. It is easy for me to work with the new automatic pen-shaped insulin shots whose grade and unit are written on them. (34-year-old woman)
Self-Efficacy to Overcome Obstacles
The participants spoke of their belief in the ability to overcome many barriers that stand in the way of adherence to T2D treatment, including the ability to regularly take medication, keep physically active, and follow a proper diabetic diet in different conditions. I can resist eating cream even if I am at a party and no matter how the host insists on the guests eating. (63-year-old man)
Treatment Adherence–Related Affects
Mental positive or negative affects that arise before, during, and after the adherence to treatment behavior are subsumed under this category and are divided into two subcategories.
Positive Affects
The participants felt good when showing adherence behaviors, such as going for a walk and following a healthy diet. They expressed feeling healthy and lively. When I go for a walk, I feel much better, I get a better view of life, and I feel fresh. (43-year-old man)
Negative Affects
The participants talked about their negative feelings before, during, and after the treatment adherence behavior, such as the fear of the test, stress, feeling weak against the disease (diabetes), worry about the complications of the disease, and a negative view of diabetes. I keep thinking about whether I have to take medicine for the rest of my life. I am afraid I will get addicted to these pills if I always take them. (43-year-old woman)
Interpersonal Influences
The participants mentioned the effects of the family members’, friends’, and the health staff’s behaviors, beliefs, or attitudes concerning their adherence to treatment. These effects could improve or lower T2D treatment adherence behavior.
Medical Staff
The participants talked about the effect of physicians’, nurses’, and secretaries’ behavior on adherence to T2D treatment. These behaviors included sympathy for and encouragement of the patient to adhere to treatment or completely to the contrary to scare, insult, or mistreat him/her. I was excreting protein in the urine as I did not take my diet serious. My doctor scolded me and said I was to lose my kidney as I did not take insulin. So, I was scared and began to take a better care of myself. (56-year-old man)
Significant Others
The participants talked about the positive effect of relatives’ and family’s approval and encouragement on the adherence behavior. Also, sometimes feeling that nobody among the family cares enough about the patient creates a sense of disappointment and forces him/her to adhere to the treatment. To care for diabetes, the family, especially the spouse, plays a major role to support the patient and not get on his/her nerves. (48-year-old woman)
Sometimes, the family plays a negative role in adherence to treatment. My father-in-law is diabetic and is on pills for years. When the doctor told me you should take insulin, my husband’s family insisted that I do not do so and that I should not take insulin. (34-year-old woman)
Situational Influences
As most participants experienced, treatment adherence could be affected by special events such as job issues, living facilities, and religious occasions.
Daily Routines
During their daily life, most participants were faced with issues such as daily activities, family, work, and financial limitations, which had positive or negative effects on adherence to their treatment. I work at a dock in the sun and this is not good for my diseased condition. I have to drink water and adjust my insulin level so that my sugar does not drop. (56-year-old man)
Local Issues
As the participants commented, culture, religion, weather conditions, and facilities of the place of residence influence their adherence to treatment. During the month of Ramadan, breaking the fast with different sweet desserts and fried foods is harmful, and it’s hard for me as a diabetic patient to help eating those sweet things. (34-year-old woman) The high heat and humidity in Bandar Abbas make me nervous and tired. When I am tired, I can hardly walk, and worse, my blood sugar rises due to discomfort. (60-year-old woman)
Immediate Competing Demands and Preferences
The participants spoke of a competing demand that could not be avoided or a competing preference that could not be countered.
Temptations
Participants, on certain occasions such as a party, may not adhere to regular medication and healthy diet. They also have little control over the temptation of sugary substance. In popular social media, such as Instagram, there are attractive and tempting advertisements on desserts and high-carbohydrate fast foods that may tempt T2D patients to go for these kinds of food. Mental weakness and exhaustion make me prefer to sleep rather than any physical activity, and I haven’t gone for a walk for a week now. (59-year-old woman)
Familial–Social Responsibilities
Responsibilities that arise from the patient’s role in the family and society can be a competing priority or a competitive preference against the treatment adherence behavior. Such conditions can be not taking medicine or not going for a walk due to attending business meetings or helping family members. I remember going to work as usual. I had the morning dose of my drugs and left for work. Suddenly I was sent on a mission and had to leave for another city without any drugs to take. (45-year-old man)
Commitment to Plan of Action
The participants talked about the intention and knowledge of a planned strategy that could facilitate the adherence to treatment behavior of T2D.
Discipline
The most frequent points raised by the participants who successfully adhered to their treatment were a detailed plan for taking medication and doing regular physical activities. I take medicine at 5:00 AM every morning and I have a regular plan for that. (63-year-old man)
However, some participants did not keep to their predetermined schedule. As far as I can, I try to plan for everything, but I can’t follow things as planned. For example, I decide to go for a walk this evening but when the time comes, I won’t. (71-year-old man)
Foresight
The most frequent strategies the participants used to solve potential future problems were writing a medication plan and meal plan, categorizing drugs, buying more than the monthly consumption, and storing drugs in more frequently visited places such as the workplace, home, or relatives’ home. As there are higher chances of forgetting to take the medicine regularly, I set a reminder on my phone regularly, usually 10 days. (59-year-old man) I care a lot about my medicines. I have a special medicine bag that I take with me everywhere. (70-year-old woman)
Treatment Adherence Behavior
The participants talked about the behaviors they showed to adhere to treatment, physical activity, and adherence to the diet. I ride a bike every afternoon. (71-year-old man) I live on the diet as prescribed by the doctor. (75-year-old woman)
Treatment Adherence–Related Experiences
Part of the participants’ descriptions were not related to the HPM yet affected their adherence to treatment. These were the experiences they or others had gained from adherence to diabetes treatment.
Personal Experiences
The participants’ previous successful and unsuccessful experiences of the disease concerning their adherence to treatment are effective in their current behavior. I remember I stopped taking insulin without consulting a doctor and my left eye began to bleed. Now I take insulin on a regular basis. (43-year-old woman)
Others’ Experiences
It was important for the participants to know both the negative and positive experiences of the other diabetic patients. My mother’s heart problem and what happened to her due to diabetes made me take diabetes more serious. (56-year-old man)
Discussion
The present study aimed to unravel the determinants of adherence to treatment in T2D patients. The study was based on Pender’s HPM. Based on the concepts extracted from the participants’ interviews and the personal, interpersonal, cultural, and geographic determinants of T2D treatment adherence, it seems that the HPM is effective.
According to the participants’ experiences, the benefits of adhering to treatment not only improved their T2D condition but also contributed to their fitness and mood. Participants contended that the perceived positive affects could facilitate the adherence to treatment behavior. In this regard, Marinho contended that emotions are among the leading factors in good adherence to diabetes treatment (Marinho et al., 2018). This study found many barriers to successful treatment adherence. Individual and contextual barriers included the physical problems to do regular physical activity, complications of diabetes, forgetting to take medicines, high cost and low insurance coverage of medicines, doctor visits and lab tests, and low availability of drugs especially insulin, and this is consistent with international studies (Huang & Shiyanbola, 2021; Krishnamoorthy et al., 2022; Rezaei et al., 2019). In Iran, as suggested by the NPPCD and the NGOs, such as the Iranian Diabetes Society, there are different ways to promote the perceived benefits of treatment adherence and overcome the potential barriers. Examples are holding training sessions in health centers and diabetes clinics on adherence to medication, proper diets, and physical activities and instructions on how to control anger, stress, and anxiety. It is also possible to arrange for regular visits to psychological counselors in health centers for T2D patients for psychological checkups. Private clinics can also adopt similar methods with the assistance of NGOs. NGOs and public organizations can organize campaigns for treatment adherence in certain time frames.
More organized diabetes care services, such as determining the share of drugs and insulin for patients receiving services in each region and providing government and charitable financial facilities and special insurance for these patients to include laboratory, drug, and treatment services, can positively affect patient treatment adherence.
Participants’ mood, self-efficacy, belief in their ability to interpret the diabetes test results, doing physical activities in any weather type, following the diet, and taking medicine in unusual conditions such as on work missions or in parties can affect T2D treatment adherence and the barriers to adherence behavior. Studies have shown that T2D patients’ self-efficacy affects their adherence to treatment (Krzemińska et al., 2021; Çalli & Kartal, 2021). When faced with the barriers, individuals with a high coping self-efficacy recover faster and maintain their commitment to their goals (Ranjbaran et al., 2020). In this regard, the most common situational influences were the patient’s place of residence and job conditions. Some participants stated that their job restrictions often lead to the shortage of time to do physical activities, eat healthy food, and take medication regularly. The immediate competing demands and preferences mentioned included the preference of television and sleep to a stroll or the delayed insulin injection due to an important work meeting. A study in Japan showed that working more than 60 hours a week and skipping breakfast and meals routinely may affect the working population’s ability to control blood glucose level among T2D patients (Azami et al., 2019). Thus, organizations can take certain measures such as including the status of chronic diseases like diabetes in health records, considering job conditions and the health state, and offering emergency medicine pack at the workplace. In addition, considering the available features of Electronic Health Records (EHRs) in Iran, a smart ID card in Persian and English could be developed for all diabetic patients, including disease records, insurance, and emergency contact numbers, in case of any issue like changes in blood sugar while traveling.
As the participants pinpointed, besides significant others’ motivating role, support, and reminding, the sense of being important to others, especially the family, can create a strong motivation to adhere to treatment. Also, trust in the physician’s ability to control the disease and the health staff’s decent behavior all play a leading role in the regular visits paid to the physician and adherence to the treatment. Halepian found that trust in doctors was associated with an increased adherence to treatment, which also reduced the complications of diabetes (Halepian et al., 2018). Another factor underlying the adherence to treatment was one’s own or others’ previous experiences. These experiences could be influenced by the positive experience of sugar control through walking or the negative experience of amputating a diabetic friend’s leg.
Considering the experiences shared by patients and the traditional culture of Iran, especially in the south, where interpersonal factors matter most (Pourtorogh et al., 2022), it is suggested to involve significant others in patient’s life, including family members and friends in intervention programs. Also, with the development and growing number of clinics and improved appointment systems, the patient’s waiting time could decrease. The patient can access the health staff at the right time. Healthcare workers can help by introducing facilitators, such as drug reminder software, physical activity, and nutrition to plan and commit to patients’ treatment adherence. Many participants stated that the experience of using smartphone-based apps was useful. Studies also reported the effectiveness of using smartphone-based apps in improving the treatment adherence of chronic patients (Gross et al., 2021; Yu et al., 2021).
Limitations
The methodology used in this qualitative study was directed content analysis with maximum variation. It helped the present researchers achieve a deeper understanding of the determinants of treatment adherence and a better understanding of the patients and the challenges they face in the treatment adherence process. We included both visitors to public and private clinics because the approach in each may differently affect the patients’ knowledge and perception of treatment adherence (Drabble et al., 2019). One limitation in this study is that we only used the interview method. Thus, it is suggested to collect data through triangulation in future studies. We used the opinions of patients. Future researchers can explore the opinions of doctors, healthcare workers, and family about the determinants of adherence to diabetes treatment. As for the generalizability of findings, although these findings cannot be generalized to the wider population, the findings may be transferable to other similar cultural contexts.
Implications
The present study aimed to explore the determinants of adherence to type 2 diabetes treatment. Still, some determinants are left unexplored. Therefore, we can raise the following implications.
Typically, interventions use simple methods, such as medication reminders to improve adherence to chronic disease treatment (Drabble et al., 2019). Considering that a wide range of individual, interpersonal, and situational factors (Hashimoto et al., 2019; Mannan et al., 2021; Pourhabibi et al., 2022) influence adherence to T2D treatment, we suggest that interventions become more specialized and be designed in light of theoretical frameworks (Nili et al., 2020). Including the factors mentioned in the interventions can facilitate patients’ increased motivation to follow the treatment; low costs will be imposed on the treatment of the complications of diabetes for the individuals and the medical system.
It is also suggested that healthcare workers provide patients with the opportunity to express their concerns about adherence to treatment, medication, nutrition, and physical activity and introduce them to the right specialists if necessary.
Considering that adherence to treatment differs in different conditions and environments, it is suggested to improve self-efficacy and resilience in interventions aimed at developing individual skills.
Conclusions
Participants shared their experiences of personal characteristics and ecological environment, and specific cognitive, affective, and behavioral determinants of adherence to T2D treatment. The categories extracted from this study concerning HPM constructs and experiences shed light on the determinants of treatment adherence. Attention to the determinants of T2D patients’ treatment adherence will help program designers plan future programs to choose the most appropriate methods and applications to improve T2D treatment adherence and reduce the burden of this disease.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the participants for their sincere cooperation in this study.
Author Contributions
NSH contributed to the design and interview with participants, analysis, interpretation, and drafting of the research manuscript. ZH contributed to the inception, design, interpretation, and final approval of the manuscript for publication. SD and TA contributed to the data analysis, interpretation, and editing. AGH, AB, and NSH revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by a research grant from the Hormozgan University of Medical Sciences (grant no.: 4000362). The funding body (HUMS) didn’t have any role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.