
Abstract
Refugees and immigrants have experienced heightened health inequities related to COVID-19. As community-embedded frontline health personnel, refugee and immigrant community health workers (riCHWs) played essential roles in the provision of informational, instrumental, and emotional support during the unprecedented first year of the pandemic. Despite the importance of this workforce, riCHWs are at high risk for burnout due to low recognition and demanding workloads. This was exacerbated as riCHWs navigated a new and uncertain health delivery landscape. We sought to glean insight into riCHWs’ stressors, coping strategies and resources, and self-efficacy to identify ways to support their work and wellbeing. Using a narrative inquiry approach, we conducted semi-structured, in-depth interviews with 11 riCHWs working in a midsized city in the midwestern United States. We generated three distinct yet interrelated themes: (1) Rapid and trustworthy information is key, (2) Creativity and perseverance are good … structural support is better, and (3) Integrating riCHW expertise into health promotion programming and decision-making. Although riCHWs were deeply committed to enhancing community wellbeing, quickly shifting responsibilities in tandem with structural-level health inequities diminished their self-efficacy and mental health. riCHWs relied on work-based friends/colleagues for informational and emotional support to enhance their capacity to deliver services. Findings suggest increasing opportunities for peer support and idea-exchange, professional development, and integration of riCHW expertise in health promotion decision-making are effective strategies to enhance riCHWs’ professional self-efficacy and personal wellbeing.
Introduction
The novel SARS-CoV-2 (COVID-19) pandemic shone a stark light on existing health inequities experienced by immigrant and refugee populations in the United States (Hopman et al., 2020; Matlin et al., 2021; Saifee et al., 2021). Unequal access to healthcare, information, and health-promoting resources; lack of employment protections in sites with large numbers of immigrant and refugee workers (e.g., employer failure to provide adequate personal protective equipment [PPE] and physical distancing standards in meatpacking plants); and cultural emphases on social connectedness among some communities posed unique challenges to COVID-19 prevention and mitigation (Kluge et al., 2020; Tippens & Springer, 2021). During the pandemic, community health workers (CHWs)—frontline public health workers who use their status as community members/allies to facilitate access to health/wellbeing-promoting resources and improve service delivery (American Public Health Association [APHA], n. d.)—played vital roles communicating health information, navigating health systems, and connecting community members to health and social services, especially during the unknown of the early stages of COVID-19 (Peretz et al., 2020; Rahman et al., 2021; Recto et al., 2022). Examples of CHW roles include hospital staff, case managers, community and faith-based organization staff, health education and outreach personnel, and health promotors and advocates (Love et al., 1997; Malcarney et al., 2017; World Health Organization, 2021).
CHWs with immigrant and refugee backgrounds have been uniquely positioned to provide health-related services to migration-affected communities during COVID-19. CHWs are often physically and culturally embedded in the communities in which they work and are viewed as trusted, invaluable members of health teams given their capacity to understand unique community needs and strengths and to deliver culturally responsive health information and programming (Chaidez et al., 2018; Palmer-Wackerly et al., 2020; Sabo et al., 2017; Spencer et al., 2010; Toney et al., 2022; Torres et al., 2014). However, as frontline health workers, CHWs were extremely vulnerable to experiences of burnout, compassion fatigue, and moral distress. The U.S. Centers for Disease Control and Prevention (CDC, 2020) described the onset of COVID-19 as a “fast-moving public health crisis.” Frontline health personnel operating during public health crises are at disproportionate risk for experiencing poor mental health, including emotional distress and burnout (Deng & Naslund, 2020; Harrell et al., 2020). Burnout is characterized by emotional exhaustion, cynicism or depersonalization, and poor professional efficacy (Harrell et al., 2020; Maslach et al., 2001). In a review of the mental health effects of COVID-19 among frontline health workers in low- and middle-income countries, Deng and Naslund (2020) noted CHWs were at increased risk of suffering extreme psychological effects of COVID due to systemic health inequities (e.g., gender inequality, lower salaries, and membership in historically marginalized social or cultural groups).
Although there is limited research regarding stress and burnout among refugee and immigrant CHWs specifically, several factors could place them at additional risk for decreased psychosocial wellbeing, particularly in the context of a pandemic. Many CHWs do not work in the formal healthcare sector; therefore, at times, their legitimacy and roles have been undervalued in biomedicine (Humphrey & Kiernan, 2019; Kane et al., 2016; Torres et al., 2014). This low recognition in tandem with demanding workloads, resource constraints, and blurred boundaries as community-embedded personnel places CHWs at risk for burnout (Chaidez et al., 2018; Dugani et al., 2018; Leo et al., 2021; Sabo et al., 2017). Although such challenges were highlighted prior to COVID-19, these risks were exacerbated during the pandemic as CHWs’ roles extended beyond their original scope of work to include additional tangible, emotional, and social support to their communities (Rahman et al., 2021; Recto et al., 2022). Moreover, CHWs who hold minoritized or marginalized positionalities share experiences of stereotyping, racism, and discrimination—in both workplace and community settings—with the community members they serve (APHA, 2022; Hunte et al., 2023).
Purpose of the Study
There have been recent calls to center the perspectives, experiences, and expertise of minoritized health workers in health-related research, practice, and policy decision-making (e.g., APHA, 2022; Hunte et al., 2023). Despite their importance in health promotion, research on CHW-led programming often focuses on the perspectives of health organizations, rarely bringing CHWs’ voices to the forefront (Palmer-Wackerly et al., 2020). Additionally, recent attention has been paid to the need to support frontline health workers in emergencies, both to ensure their personal wellbeing and to sustain an essential workforce during global health crises (Harrell et al., 2020; Søvold et al., 2021). Thus, this study sought to co-create the meaning of experiences of immigrant and refugee CHWs providing essential COVID-19 services and information in a midsized midwestern U.S. city. To enhance focus and readability, we hereafter refer to refugee and immigrant CHW participants in this study as riCHWs when described in the aggregate. Three questions guided this project: 1. What were the primary work-related stressors riCHWs experienced during COVID-19? 2. How did riCHWs cope with COVID-19 and work-related stress? (Sub-question: What were their preferred supportive resources?) 3. How did riCHWs describe feelings of self-efficacy providing health services in an unfamiliar and emergency health context?
Theoretical Frameworks
Dunn and colleagues (2008) coined the term “coping reservoir” as a metaphor to describe how one’s ability to respond to stress is influenced by the interplay of internal resources (e.g., personality traits, temperament, and coping style) and depleting and replenishing factors. In the example of medical students’ coping by Dunn et al. (2008), negative (depleting) inputs included factors such as stress and energy demands, while positive (replenishing) inputs included psychosocial support, mentorship, and intellectual stimulation (p. 45). Similarly, although not explicitly applying the coping reserve model, Aryal and D’mello (2020) found that occupational stress related to low status and powerlessness (depleting factors) among CHWs in Karnataka, India, was affected by coping style (e.g., positive reappraisal, humor, and avoidance). In a study of French health workers during COVID-19, Vancappel et al. (2021) found associations between lower job status, fewer years of experience, and a higher number of post-traumatic symptoms as well as a mediating effect of coping strategies, supporting the coping reserve model.
As riCHWs navigate multiple communities of belonging and hold different statuses and relationships within each of these, we used the sense of community theory to add greater nuance to the coping reserve model. McMillan and Chavis’ (1986) posited sense of community is comprised of four elements: membership (sense of belonging), influence (sense of mattering or making a difference to a group), integration and fulfillment of needs (feeling that needs will be met via group membership), and shared emotional connection (perception of shared history and experiences). These pillars are relevant to riCHWs who are members of the groups with whom they work and have a strong investment in promoting community wellbeing through their work (Lohr et al., 2018; Torres et al., 2014). Applications of sense of community theory to health research have become more prominent in studies examining the roles of social capital, social networks, and social cohesion on health and healthcare delivery (e.g., Carpiano & Hystad, 2011; Hystad & Carpiano, 2010; Mahmoudi Farahani, 2016). Sense of community theory has also been used by researchers exploring immigrant and refugee postmigration adjustment (Badali et al., 2017; Keel & Drew, 2004; Modesti & Talamo, 2021; Weng & Lee, 2016). Weng and Lee (2016) noted the importance of ethnic community in cultural maintenance and in extending familial and fictive kin networks. Additionally, organizational-level structures such as refugee resettlement agencies and ethnic community-based organizations (ECBOs) play a critical role in enhancing sense of community via social support or peer groups, activity nights, cultural celebrations, and resource-sharing events (Badali et al., 2017; Dubus, 2017; Keel & Drew, 2004; Tippens et al., 2021). Our application of the “coping reservoir” in tandem with the sense of community theory enabled us to explore macro-, meso-, and micro-inputs related to burnout and resilience as well as unpack how riCHWs navigated resources from multiple communities of belonging to enhance their self-efficacy and capacity to support their communities during the first year of COVID-19.
Method
Study Setting and Context
This study was conducted in a midsized Midwest U.S. city in a top refugee-receiving state per capita. The city is one of two primary resettlement locations in the state and is home to two refugee resettlement agencies. Additionally, there is strong coordination among ECBOs, human service agencies, the school district, etc., to provide services to immigrants and refugees via a welcoming coalition. To this end, the principal investigator (PI; JAT) had participated as a member of the local immigrant and refugee health coalition for approximately 5 years at the time of study inception and data collection. The community-academic research team represents multiple ongoing partnerships and consists of three women based at ECBOs, including two riCHWs (SDV, LES, and NC); six university faculty members with diverse training in health equity and social sciences, including two with immigrant backgrounds (VC, APW, EM, KC, YX, and JAT); and two graduate and two undergraduate students, including one with an immigrant background (BB, AM, EEG, and MC). Power relations are a principal concern in narrative and community research (Clandinin & Connelly, 2000; Minkler & Wallerstein, 2012; Muhammad et al., 2015). Interviewers (AM and JAT) were a PhD student and a faculty member with experience conducting qualitative research. Both were known to some riCHW participants through their participation on the citywide coalition, which may have influenced responses (e.g., participants eliminating information that is assumed to be shared or known by the interviewer; see Corbin Dwyer & Buckle, 2009). To mitigate this potential challenge, we reminded participants they were selected for their expertise and that researchers did not have day-to-day experiences within their communities. We also included probing questions in the interview guide (developed by the entire team) to elicit specific information that may have been assumed to be known by interviewers. To ensure interview quality, we conducted practice interviews with coalition members and regularly reviewed interviews during scheduled team meetings. To enhance rapport with interviewees, AM and JAT used strategies proposed by Bergen and Labonté (2020), including asking individuals to participate in a place they felt was private, clearly explaining why riCHWs’ expertise was necessary and why individuals were selected, showing respect throughout the interview, and using humor and self-disclosure during conversations.
Study Design and Procedures
We interwove the coping reserve and sense of community theoretical underpinnings with participatory and narrative research approaches to create a rich tapestry elucidating how riCHWs negotiated community health promotion in a new, unfamiliar context. Specifically, we used a community-based participatory research (CBPR) approach to ensure research questions, procedures, and findings were relevant to and shared with community stakeholders during the first year of COVID-19. CBPR emphasizes equal partnerships between community and academic collaborators who are working toward a common goal (Holkup et al., 2004; Minkler et al., 2012); connecting CBPR with coping reserve/sense of community acknowledges that communities themselves are best equipped to identify their needs and resources. Within the CBPR approach, the team decided to use narrative inquiry (Clandinin & Connelly, 2000) to privilege riCHWs’ experiences and expertise as workers whose perceptions are traditionally excluded in health promotion research (Palmer-Wackerly et al., 2020). Narrative inquiry enabled us to interrogate interview data beyond the “what” (i.e., direct representation of experiences) and into the “how” (e.g., language and emphasis used to describe certain experiences), for “whom” (e.g., what stories were told and how might interviewer positionality have influenced story selection and sharing?), and the “why” (e.g., possible desired outcome from story sharing) (see Lal et al., 2012 for review of integration of narrative inquiry into combined qualitative mixed-methods research). This was important to our team for two reasons. First, we wanted to have a deep understanding of how riCHWs made sense of their experiences, particularly in an ever-shifting and unpredictable work and life context. Second, we wanted to identify what stories were emphasized to better support riCHWs. Lindsay and Schwind (2016) noted that researchers become co-participants in narrative inquiry through listening, observing, and co-existing with participants to glean deeper insight into and co-construct knowledge. This form of inquiry has an important role in highlighting diverse perspectives and positionalities related to community intervention (Riley & Hawe, 2005), especially in an unprecedented health landscape such as that created by COVID-19. Moreover, when employed as a participatory strategy and coupled with coping reserve and sense of community frameworks, narrative inquiry enabled us to explore how riCHWs identified and used their coping reserves in a broader community context as well as to use this information to better support riCHWs via local coalition/organizational stakeholders.
Overview of Research Alignment With CBPR Principles.
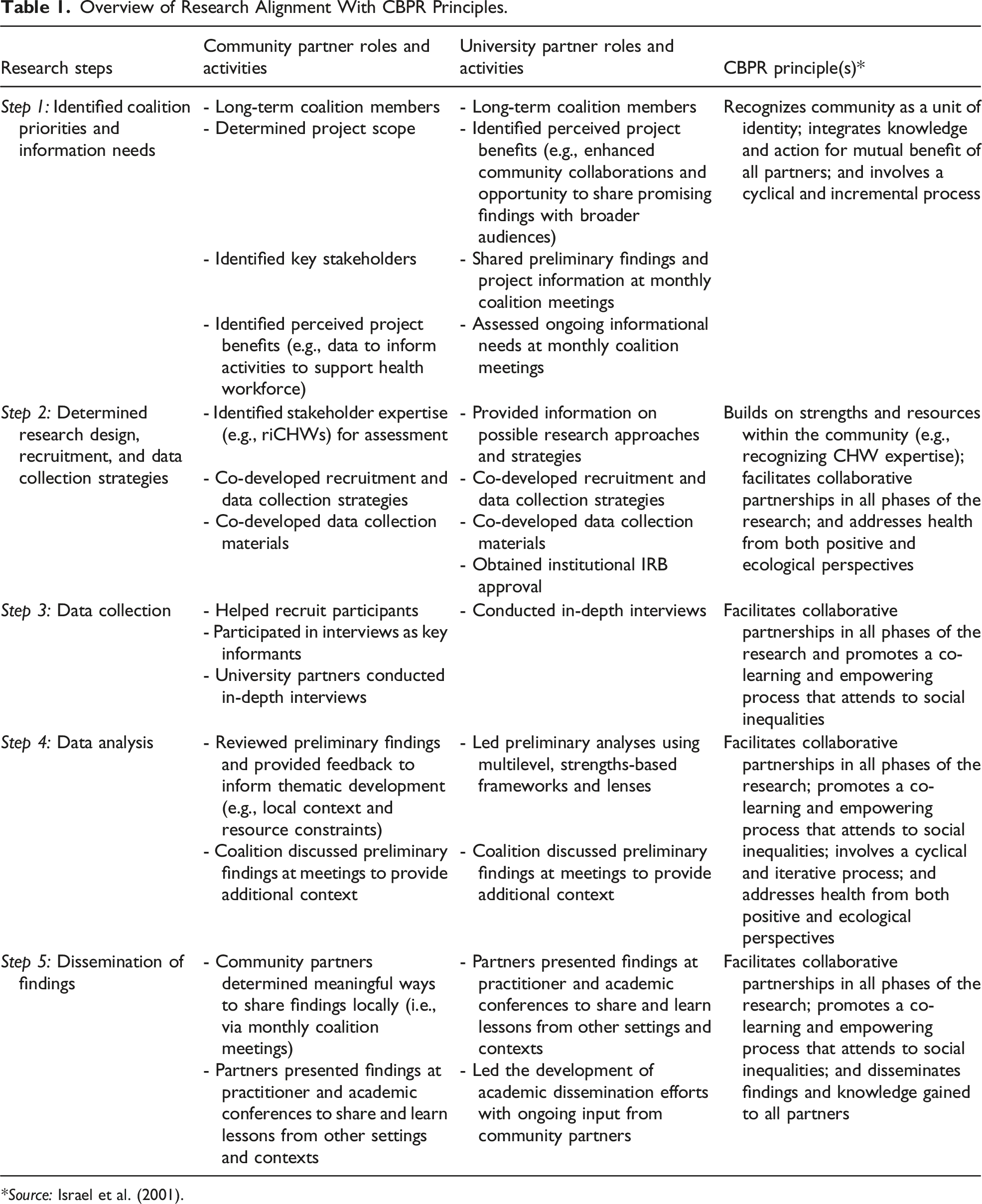
*Source: Israel et al. (2001).
Ethical approval was granted by the Human Participants Protection Program at the University of Nebraska-Lincoln Human Participants Protection Program (approval no. 20200920608EX). We recruited riCHWs through member organizations of the citywide immigrant and refugee health coalition via purposive and snowball sampling (i.e., email listservs, word-of-mouth, and asking if others should participate post-interview). Individuals who were 19 years of age or older, born outside of the United States, were providing direct services to immigrant and refugee communities, and self-identified as belonging to one or more of these communities were eligible to participate in the study. Individuals who agreed to participate were sent a copy of the informed consent form via email. AM and JAT also reviewed each section of the informed consent form with participants prior to interviews, pausing to address any questions after each section. Participants were reminded that they could choose not to answer specific questions or withdraw from the study at any time. Participant consent for interviews and video and audio recording was taken via verbal agreement directly prior to the onset of each interview.
We used semi-structured, in-depth interviews as our data collection procedure, which AM and JAT conducted via end-to-end encrypted remote videoconferencing between December 2020 and March 2021. By this time, riCHWs had been relying on videoconferencing software for many of their daily work activities, and the interview was mostly viewed as “another meeting or appointment”; therefore, we did not face logistical challenges we had anticipated (e.g., participants who may be unfamiliar with videoconferencing technologies). However, some riCHWs noted that some of their clients—particularly older adults—had continued to struggle with the transition to videoconferencing, which is an important consideration for researchers and practitioners wishing to engage with communities during unique circumstances such as COVID-19. In cases where employer-based videoconferencing software was unfamiliar, riCHWs said they used Facebook Messenger, WhatsApp, or similar apps that individuals were already using; however, connecting with community members via social media apps further blurred already fuzzy professional and personal boundaries. Having a remote interview location was a potential challenge for two reasons. First, in offices with open floorplans or where offices may be in close proximity, there is an increased potential for social desirability bias—not merely between the participant and researcher but also between the participant and coworkers (similar to focus group settings). Second, participants who were interviewed from shared office spaces were wearing masks, which made it somewhat challenging to hear some responses as well as detect nonverbal communication cues. We attempted to mitigate some of these challenges by asking riCHWs to participate in a place they felt was private and asking clarifying questions if we thought we misheard or misunderstood a response.
The interview guide was designed to glean insight into riCHWs’ experiences supporting their communities during the pandemic and to gather recommendations to improve resources and supports for frontline health workers. Questions focused on perceptions of how the pandemic affected specific communities and community members (e.g., older adults compared to youth), scope of work and core tasks before and related to COVID-19, self-efficacy (e.g., challenges and resources/supports used to overcome identified challenges, successes and favorite work activities, and key skills and attributes needed to support communities during COVID-19), and any additional information riCHWs wished to share with investigators. All interviews were conducted in English. The average length of interviews was approximately 90 minutes (range: 35–180 minutes). Participants received $40 virtual gift cards upon completion of the interview to acknowledge their time and expertise.
Data Analysis and Dissemination
Interviews were transcribed verbatim by BB and AM and reviewed by the research team. BB and JAT conducted independent narrative analyses of transcripts first using inductive coding to privilege participants’ stories and how they made sense of their experiences through sharing stories with interviewers (Langellier, 1989, 2001). In later rounds, we used deductive coding for actionable areas (e.g., riCHWs’ suggestions for supportive resources) to share immediately with the local coalition as well as to integrate into overall theme generation. Preliminary codes and themes were shared with the wider team and refined based on community and academic partner input. BB and JAT condensed and finalized themes, which were agreed upon by the research team. Coding was completed manually; however, we used MAXQDA to supplement data analysis and ensure data accuracy and quality (e.g., term searches to ensure our coding was complete and showed variations within final themes). Findings were shared with the refugee and immigrant health coalition at monthly meetings.
Findings
Participant Sociodemographic Characteristics
Participant Characteristics and Communities Served.
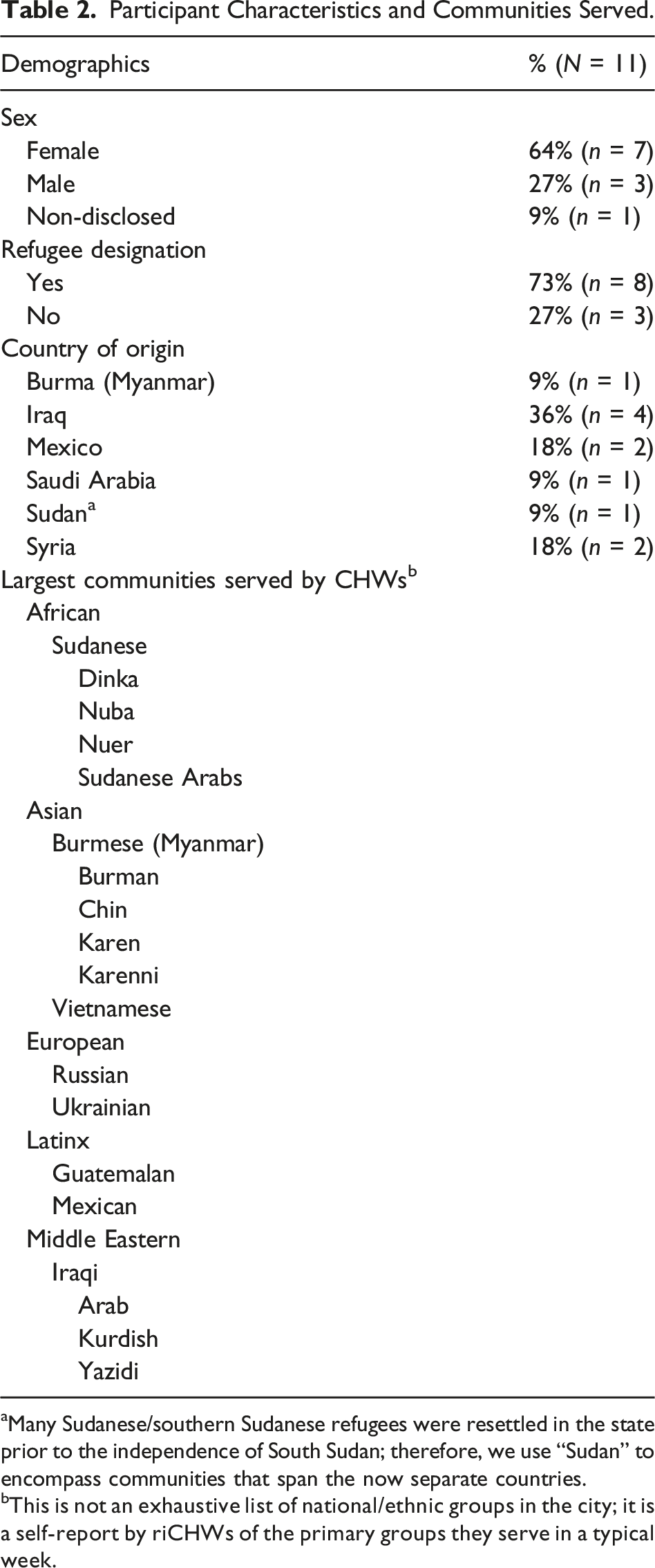
aMany Sudanese/southern Sudanese refugees were resettled in the state prior to the independence of South Sudan; therefore, we use “Sudan” to encompass communities that span the now separate countries.
bThis is not an exhaustive list of national/ethnic groups in the city; it is a self-report by riCHWs of the primary groups they serve in a typical week.
Overview of Themes
Participants almost unanimously reported an increase in work/case load and exhaustion related to the provision of services and resources during the first year of COVID-19. Despite this, most riCHWs expressed gratitude to be in roles that enabled them to provide instrumental, informational, and emotional support to their communities. Within this context, we paid careful attention to depleting and replenishing inputs, generating the following themes pertaining to CHW burnout, resilience, wellbeing, and supports: (1) Rapid and trustworthy information is key, (2) Creativity and perseverance are good … structural support is better, and (3) Integrating CHW expertise into health promotion programming and decision-making. The following sections explore these themes in greater depth.
Theme 1: Rapid and Trustworthy Communication Is Key
Communicating Rapidly Changing Health Information and Guidelines
All participants referenced challenges related to communicating ever-changing health information and recommendations during the early stages of COVID-19. Two riCHWs specifically noted how changing guidance from the Centers for Disease Control and Prevention (CDC) and county health departments created fear among community members who stopped trusting information: “Elders are isolated. They stay in the house. They used to walk to the community center [but] now they are afraid because they say [COVID] is in the air” (Sudanese CHW). The same Sudanese CHW continued, “there were so many diseases [in refugee camps in Kenya and Ethiopia] that many do not see COVID as a big deal.” Although such a contradiction highlights the importance of considering variations in within-group risk perception in health promotion efforts, riCHWs mainly reported such health behaviors as an annoyance because it meant (to them) that community members were not following their advice. Similarly, an Iraqi CHW shook their head in disbelief when talking about adolescents in their community: “Some teens don’t even have masks … or they hang below their noses!” A different riCHW from Iraq said that people in their community wanted to comply with health guidelines but found it difficult: “With meatpacking jobs and large families, how can [Iraqi refugees] possibly physically distance?” They continued: They are at a higher risk of contracting COVID and at their jobs they cannot easily call out sick, you know? They are on a point system and, so, if they miss work, they lose points. And if you add up so many points, then you lose your job. Then that, of course, creates this whole cascade of potential problems.
Other riCHWs shared similar challenges within the communities they served, expressing frustration in the incongruence between the health guidance they were meant to convey and the on-the-ground realities. Indeed, many participants themselves reported contracting COVID-19 and still caring for family and community out of both necessity and feelings of obligation.
Most participants were unaware of existing COVID-19 informational resources developed in multiple languages (e.g., infographics, pamphlets, and videos) by institutions such as the CDC and the National Resource Center for Immigrants, Refugees, and Migrants. Several riCHWs were asked to develop resources for local agencies and clinics, revealing a lack of local capacity to disseminate rapid health information, including to frontline health workers responsible for communicating health information and debunking myths. However, it is also important to note here that lack of trust in official sources of health information (e.g., government media releases or websites) is a documented barrier to health information-seeking among immigrant and refugee populations (e.g., Healey et al., 2022; Kubisa, 2021; Longanga Diese et al., 2022). Moreover, guidelines that seek to change health behaviors are meaningless in contexts wherein such guidance is not only not enforced but actively discouraged by employers (e.g., lack of employer protections; Tippens & Springer, 2021).
Organizational (Mis)Communication and Referrals
riCHWs described feeling frustrated by decisions that were made at the organizational level without their involvement but that had grave impacts on their communities. This frustration was nearly always noted when participants described feelings of burnout, specifically related to navigating systems they felt were working against them and against the best interests of their communities. This is best illustrated by an Iraqi CHW’s frustration with widespread interpreter lay-offs at one organization (a decision made at the organization’s headquarters in a different state): It was either February or March [2020], when me and some other [hourly] interpreters got emails from [agency headquarters in different city] saying that they were not going to use our services anymore. Honestly, I thought in a pandemic they would use interpreters on staff, but they did not. They got rid of us and then all these clients, these patients … they should not have been abandoned. […] Clients and their therapists at the clinic would ask me, “How can we get a hold of [agency]?” and I tell them how [agency] got rid of all of their interpreters. So now I am helping them [without pay]. But the problem is that, even me, I cannot get a hold of the agency. So how would anyone expect somebody who does not speak the language to get a hold of them? (Iraqi CHW).
Several riCHWs echoed the severe ripple effects of widespread interpreter lay-offs in the city (beyond the aforementioned headquarters) in their communities. Some volunteered as interpreter liaisons in addition to their formal roles but struggled to fill voids left by budget cuts. A Burmese CHW lamented that phone-based interpretation in clinical settings was insufficient as interpreters did not have the capacity to follow-up with patients in the same way as riCHWs. For example, they noted diabetes as a risk factor for additional complications from COVID-19 when discussing challenges faced by a newly diagnosed community member: This older man who did not speak English … did not understand that you must take the medication every single day and, you know, how they give only 30 days at a time at the pharmacy? He thought after the 30 days that he was done taking it. He did not know that he had to continue taking the medication. He did not know that there was such a thing as medications that you need to take every single day and when it is done, you need to go back to the pharmacy and get more medication. (Burmese CHW).
Despite increased resource and service requests by community members, riCHWs found themselves navigating systems that diminished their value (e.g., cultural expertise and language skills), revealing ways in which the very system within which riCHWs were functioning was a depleting input. Many participants reported a sense of helplessness filling service gaps as leading to despair, worsening mental and emotional health, and burnout.
Theme 2: Creativity and Perseverance Are Good … Structural Support Is Better
The lay-offs driven by a culmination of COVID-specific budget reductions and massive funding cuts to federal refugee resettlement during the Trump Administration (Tippens & Springer, 2021) created service gaps felt by riCHWs at the local level. Guidelines for physical distancing also created new challenges for riCHWs, many who described spending most of their time on the phone or teaching community members how to use videoconferencing programs when in-person services became remote. Most participants referenced “creativity” and “perseverance” as necessary attributes to work successfully during the first year of COVID-19. For example, a Burmese CHW said of helping older adults: “We have to be creative. We drop off [arts and crafts] packages to clients and do exercise on [videoconferencing program] so they do not get bored.”
Although a few participants said staff and funding shortages drove them to work harder for their communities, many admitted the realities made them feel helpless and want to give up at times, describing a situation where there were simply “too many jobs and not enough hands.” Due to their status as both community members and formal service providers, many riCHWs felt a sense of obligation to use personal resources to help their communities (e.g., buying groceries and toiletries, translating health information during “off” time, and contributing to funeral expenses). Participants described contradictory feelings of gratitude for having resources to help communities and overwhelm related to the heightened demand for instrumental, informational, and emotional support. Illustratively, an Iraqi CHW noted feeling helpless regarding increasing COVID-related deaths in their community: Funerals are incredibly expensive for all people, especially those that did not plan for a loss to occur. Not like a senior, this is a younger, healthier person who [recently] passed away. The family cannot easily pay for the ceremony and additional arrangements they need to make. It is hard when we cannot connect families to support for that sort of thing.
In addition to feeling overwhelmed by the high demand for resources, riCHWs struggled to provide emotional support in the context of widespread grief and what many described as a community mental health crisis. When asked what would help them better cope with their roles, one Sudanese CHW responded, “I want to learn to talk to the grieving [due to COVID deaths] … you know, to show you care for them. I want that training” (emphasis theirs). They continued: There is a lot of stress in the community [because of COVID-19], whether from losing family members or losing a job, losing things that you value and in life. So, we need to be having that training. [How] to be able to talk to someone that is grieving, you know how to do that without upsetting them or how to be able to connect with them.
Other riCHW participants reinforced this idea, stating a strong desire for additional mental health and psychosocial support training. Only one CHW from Saudi Arabia described a level of comfort providing emotional support, stating, “I love connecting with my community on a human level, doing whatever it takes to help … crying with them, sharing personal stories … whatever it takes.”
A Mexican CHW described the additional challenges providing health crisis services and support to a community that included undocumented and mixed-status families: I had a conversation with somebody who was worried that COVID testing would be used by ICE [U.S. Immigration and Customs Enforcement] as a mechanism of immigration enforcement. They were worried about engaging in the testing process because they were afraid of documentation status issues. And we can all say, “Oh, that wouldn’t happen, that can’t happen, or that doesn’t happen.” But we also know that [the U.S. Department of Homeland Security] has exploited other data collection mechanisms to do their bidding, so it is not out of the realm of possibilities. So then undocumented individuals are afraid to be tested [and] they may not know that they could be transmitting it to family and friends. That is a huge vulnerability and systemic issue.
Community members often sought COVID-related advice from riCHWs for situations that seemed impossible or had no “good” outcome. This include supporting individuals and families who were making decisions that could result in severe illness/death or deportation, which made participants working in these contexts feel helpless and emotionally distraught. [We have] seen families dealing with the risk of death for a family member and asking is [healthcare seeking] worth the risk of deportation? So, [another health worker] has just been telling people “Yeah, I know it feels risky, but do it anyway.” I do not know that that is a great work around. I think it is a terrible place for somebody to be in. (Mexican CHW)
Two riCHWs based at the same ECBO both stated one of the most helpful forms of support they received was from the director who carved out weekly time for staff to debrief and share both personal and work-related experiences, challenges, and successes. An Iraqi CHW noted this organizational support provided critical time and opportunities for learning and social support: “[I learn from] my peers, my work friends. We all know how [the experience working during COVID] is and we help each other.” Participants representing all nationalities echoed this sentiment, listing peer riCHWs across community and institutions among their most important resources for friendships and informational and emotional support during a challenging time.
Theme 3: Integrating CHW Expertise Into Health Promotion Programming and Decision-Making
In addition to wanting professional development training, especially related to mental health and psychosocial support (MHPSS), many riCHWs wanted opportunities to share their specific expertise with other professionals in the field. This was also most associated with MHPSS programming; specifically, participants described the importance of mental health provider training in human rights violations, refugee and immigrant migration processes, and culturally tailored MHPSS services and resources. Participants discussed challenges of having a predominantly white, monolingual health and human services workforce in the city. (Acknowledging many refugees in the state are also considered White by U.S. Census standards, when used by participants, “white” was typically used to refer to a health and social service workforce composed of predominantly white, U.S.-born women.) riCHWs expressed a need for health and MHPSS providers who speak languages other than English; who are educated about the human rights violations and discrimination endured by immigrants and refugees in premigration, transit, and postmigration contexts; and who deliver culturally sensitive services. Prior to the onset of COVID-19, staff from multiple organizations collaborated to host a professional development series wherein riCHWs and other community members provided culturally specific education and training to MHPSS and social service providers. Many riCHWs missed such opportunities to share valuable expertise. In an example reported by a CHW from Saudi Arabia, they stated their knowledge was dismissed by colleagues because of their immigrant background: “You know how this white [work] culture is [in city]. Immigrants and refugees know things. I know things. But our ideas always get dismissed, you know?”
An Iraqi CHW expanded on how institutional racism affected their overall scope of work, particularly regarding the importance of trust in service referrals: [Providers need] more on cultural services. Not for us [riCHWs] but for the people we work with in the community. If I need to refer them, I need to know if the organization is okay, if it is safe, if [patient/client] could go to this organization.
In addition to training and education, riCHWs wanted to work in institutions and systems where their expertise was valuable in all areas of decision-making, not just as an “add-on” (e.g., one-time trainings). When prompted about what this would look like, participants mostly discussed wanting increased recruitment of more riCHWs to expand and diversify the frontline workforce as well as see more ethnoracial and language diversity among allied health and social service personnel. They also wanted to be included in decision-making spaces to provide invaluable insight into “what is really happening on the ground.” Some riCHWs wanted additional capacity building related to health and mental health skills, U.S. health system navigation, and U.S. cultural norms and history to enhance their service provision skills.
Discussion
In this study, we simultaneously sought to identify riCHWs’ stressors and resources and to center their voices in health equity research, addressing calls from Palmer-Wackerly et al. (2020) and Rosenthal et al. (2021). riCHWs hold pivotal positions in their communities as both trusted members and as health sector professionals; they act as cultural liaisons and are often praised for their vital role in keeping healthcare organizations running smoothly (Brandenberger et al., 2019; Chaidez et al., 2018; Palmer-Wackerly et al., 2020; Sabo et al., 2017; Toney et al., 2022); yet, they are underrepresented in political and decision-making spheres, despite being frontline personnel directly impacted by the decisions being made (Bhatia et al., 2021; Dugani et al., 2018; Toney et al., 2022). Including riCHWs at the table allows them to advocate for their needs directly with multilevel stakeholders while providing opportunities to enhance health equity (Palmer-Wackerly et al., 2020; Wallerstein et al., 2018).
Our study yielded comparable results as Toney et al. (2022) wherein CHWs described challenges delivering health information and resources. Our participants emphasized the specific challenges of community-based health promotion and disease prevention efforts during a pandemic and provided systems-level recommendations to support frontline health workers’ efforts and overall wellbeing. These included the need for rapid and trustworthy communication, increasing provider and allied health workforce capacity to deliver culturally responsive health information and resources, ongoing professional development, training to build capacity and improve riCHWs’ self-efficacy, and integrating riCHWs’ expertise into organizational structures and decision-making spaces. Collaborative decision-making is important during public health crises public health crises; however, it is important to be aware of potential multiagency collaboration and communication challenges, particularly during emergencies. For example, Kapucu (2006) noted that emergencies create uncertainty and that bureaucratic systems that tend to operate smoothly in contexts of simple information cease to function when information is more complex and multidirectional (e.g., crisis information sharing from bottom-up vs. top-down, rapid information spreading across networks), suggesting the critical importance of pre-emergency communication, collaboration, and trust. In the context of our study, COVID-era fiscal constraints (e.g., real and anticipated budget cuts) negatively affected inter-agency collaboration and communication (Rahman et al., 2021), which participants described as the negative consequences of interpreter lay-offs. Abbas and Norris (2018) identified five areas that affect health collaboration and communication in emergency and disaster contexts: leadership culture and attitudes, (mis)trust among diverse disciplines/sectors, situational awareness (“knowing and recognizing what is going on around us”), technology/information-sharing channels, and legislation (e.g., prohibitions regarding sharing identifiable health information) (p. 3). Importantly, riCHWs can serve as cultural liaisons to enhance community-organization trust and provide critical insight into on-the-ground realities (situational awareness). This expertise is often undervalued but is critical to information-sharing and multisector collaboration in health emergencies (Abbas & Norris, 2018; Humphrey & Kiernan, 2019; Warmington et al., 2004).
Finally, this research supports and expands both Dunn et al.’s coping reserve model and McMillan and Chavis’ (1986) sense of community theory as well as the application of this theory with immigrants and refugees. We believe pairing frameworks enabled us to unpack community, including how communities of belonging can serve as both depleting and replenishing inputs in specific contexts. For example, replenishing inputs included emotional and informational support from riCHW peers while a distinct depleting input was unacknowledged expertise by members of the city’s social services community. Prior research demonstrated the importance of ethnic communities and community organizations in enhancing belonging for immigrants and refugees in postmigration settings (e.g., Badali et al., 2017; Keel & Drew, 2004; Weng & Lee, 2016). As previously stated, participants in our study navigated and negotiated multiple communities of belonging. Their insights highlight the importance of mutual assistance—such as exchanging ideas and providing emotional support—in enhancing riCHWs’ sense of community. This is seen in riCHW group membership (e.g., the habitual use of “we” among participants to describe collective challenges and successes), integration and fulfillment of needs (e.g., within-CHW group informational and social support), and shared emotional connection (e.g., perception of shared challenges during unprecedented times). Moreover, this study shows how the fulfillment of these three elements reinforces the fourth and final element: influence, described by McMillan and Chavis (1986) as a “sense of mattering or making a difference to a group.” Mutual assistance, therefore, can be viewed as the “oil” that makes the machine work: peer support and debriefing helped offset diminishing self-efficacy via brainstorming ideas as well as simply normalizing that everyone else was struggling, too. With this critical buttress, riCHWs were able to continue to provide vital services in their communities.
Implications for Practice and Research
Resource constraints and a lack of standard operating procedures necessitated riCHWs to expand their scope of work during the early stages of COVID-19 (see also Maciel et al., 2020; Peretz et al., 2020). Such rapid shifting of responsibilities in tandem with structural-level health inequities (e.g., social service sector budget cuts and immigration policies) diminished riCHWs’ self-efficacy in supporting their communities. Prioritizing debriefing sessions (such as those discussed by two riCHW participants in our study), bidirectional learning, and continuing professional development and training is critical to workforce self-efficacy and retention (Palmer-Wackerly et al., 2020). Additionally, riCHWs in this study emphasized the importance of opportunities to debrief and provide/receive emotional support from work colleagues and friends in time exclusively reserved for such exchanges. Although not explicitly mentioned by riCHWs in this study, training on boundary setting may be beneficial in preventing burnout and compassion fatigue for health workers negotiating multiple community roles and community expectations (Alvarez-Hernandez et al., 2021). Further research is needed to glean insight into how employers can create supportive structures that are effective in enhancing a sense of belonging and self-efficacy.
Importantly, riCHWs have been viewed as critical to improving population health equity. For example, the American Public Health Association (APHA) released a November 2022 policy statement, “A Strategy to Address Systemic Racism and Violence as Public Health Priorities: Training and Supporting Community Health Workers to Advance Equity and Violence Prevention.” Yet, their own experiences of structural, institutional, and interpersonal racism pose significant barriers to their ability to provide essential services (APHA, 2022), as described by participants who shared experiences of having their expertise diminished within their institutions. Recent scholarship has highlighted the personal and professional impacts of racism on CHWs, describing the importance of institutional and policy recognition of their expertise as decision-makers (e.g., Hunte et al., 2023; Kissinger et al., 2022). Indeed, although we showed the creativity, perseverance, and resilience of riCHWs in this study, there was broad recognition of the necessity of structural supports to enable them to serve their communities to the best of their abilities.
Study Limitations
Although this study contributes important information regarding riCHWs’ experiences during the early stages of COVID-19, it is not without limitations. riCHWs’ perceptions of white women in positions as researchers could have influenced responses, and some individuals may have felt pressure to participate given the partnership between their organizations and the university on this study. Additionally, although purposive and snowball sampling are appropriate recruitment strategies, we may have inadvertently missed riCHWs experiencing severe burnout and mental health challenges and who were, therefore, unable to deal with the stressor of an additional engagement (i.e., the interview). As such, this may paint an incomplete picture of riCHWs’ diverse experiences during COVID-19.
Conclusion
Eleven riCHWs described their experiences of COVID-19 as the pandemic reached the one-year mark. Using narrative inquiry and analysis, we generated the following themes: (1) Rapid and trustworthy information is key, (2) Creativity and perseverance are good … structural support is better, and (3) Integrating CHW expertise into health promotion programming and decision-making. Despite an unwavering commitment to their communities’ wellbeing, riCHWs experienced diminishing self-efficacy related to shifting responsibilities in an unprecedented health terrain. Collaborating with riCHW peers from diverse immigrant and refugee groups helped counter reduced efficacy via informational and emotional support. Although riCHWs are uniquely positioned to provide critical health information and services, it is imperative we remember that these are human beings managing their own emotions and responses to a pandemic while simultaneously trying to help their larger communities. Based on their work in South Africa, Schneider and Lehmann (2016) argued for the need to move from community health workers to community health systems, the latter defined as a “set of local actors, relationships, and processes engaged in producing, advocating for, and supporting health in communities and households outside of, but existing in relationship to, formal health structures” (p. 114). This call parallels an increased focus on addressing the structural determinants of health among public health scholars, practitioners, and policymakers. riCHWs have filled service gaps, and it is time to respond by supporting their unparalleled contributions to health promotion and disease prevention by listening to their expertise and ideas as well as developing compassionate structures to support their work and wellbeing.
Footnotes
Acknowledgments
We are grateful to the members of the Lincoln, Nebraska New Americans Task Force for their direction and guidance in this research. Many thanks to the incredible health workers who lent their perspectives and expertise to this research during the height of an unprecedented community health crisis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible through a grant received by JAT under the University of Nebraska-Lincoln Rapid Response Grants mechanism, funded by tobacco settlement funds.
Ethical Statement
Informed Consent
All participants provided verbal informed consent prior to enrollment in the study.