
Abstract
The positive deviance approach seeks to identify and learn from those that perform exceptionally well. Positive deviance as an approach to quality improvement is gaining traction in general practice. This study aimed to explore and compare stakeholders’ perceptions of the factors that support the delivery of exceptional care in general practice and to refine a previously developed theoretical framework of factors associated with positively deviant care in general practice: the Identifying and Disseminating the Exceptional to Achieve Learning (IDEAL) framework. Semi-structured interviews were conducted with 33 purposively sampled patients, general practitioners, practice nurses, and practice managers in Irish general practice. Subsequently, a directed content analysis approach was employed to deductively analyse interview data using the IDEAL framework, and newly emerging factors were inductively analysed and abstracted into the framework. Several distinct strategies (e.g. patient activation and team collaboration), structures (e.g. facilities and staffing), and contextual factors (e.g. communication and rapport, and culture) were found to support the delivery of exceptional care, and differences in perceptions, values, and expectations emerged between patients and practice staff. Interview data largely supported the pre-determined factors posited by the IDEAL framework, and new factors were abstracted into the framework (e.g. facilities and infrastructure). Stakeholder engagement regarding the factors supporting exceptional care in general practice supported and extended the IDEAL framework, contributing to a more comprehensive understanding of how exceptional care is delivered in general practice. The refined framework will support researchers, policymakers, and teams looking to support, measure, and achieve exceptionally good patient care in general practice.
Keywords
Introduction
Achieving high-quality patient care is one of the most important, yet challenging, goals of healthcare (World Health Organization, 2018). Efforts to improve care thus far have emphasised learning from the absence of safety (Braithwaite et al., 2015). Unfortunately, interventions emerging from this approach (Safety-I) have not generated expected improvements (Shojania & Thomas, 2013; World Health Organization, 2018), and efforts have typically targeted acute care, while other healthcare domains such as primary care and pre-hospital care have received considerably less attention (O’Connor et al., 2021; Sheikh et al., 2013).
Recently, more proactive approaches to quality and safety have been advocated such as the ‘Safety-II’ approach. This approach recognises that patient care ‘goes well’ far more often than it ‘goes wrong’ (Braithwaite et al., 2015; Lawton et al., 2014), thus appreciating the complexity and innate variability of healthcare systems (Hollnagel et al., 2015). Safety-II is consistent with the broader idea of positive deviance (PD) (Kelly et al., 2016). Having emerged from international public health settings to address childhood malnutrition (Marsh et al., 2004), PD investigations focus on identifying and learning from individuals whose unusual behaviour allows them to succeed where others in the community fail, termed ‘positive deviants’ (Marsh et al., 2004; Sternin, 2002). In healthcare, PD relates to learning derived from individuals, teams, or organisations who perform exceptionally well in an area of interest, despite facing similar resource constraints and challenges as others within the community (Bradley et al., 2009; Lawton et al., 2014). Patient and staff involvement is core to the ‘bottom-up’ ethos of PD, and so solutions to problems are formulated from within the community (Baxter et al., 2015). Strategies developed at the ‘sharp-end’ tend to be more acceptable and feasible within existing resources and thus are more likely sustainable and adoptable elsewhere (Marsh et al., 2004; Walker et al., 2007).
Recently, PD has been gaining traction in primary care settings as a way of improving care quality (O’Malley et al., 2022). Research fostering a PD approach in general practice has been promising, generating improvements in various healthcare (e.g. cost effectiveness; Curry et al., 2013), clinical (e.g. blood pressure; Bolen et al., 2021), and behavioural (e.g. smoking cessation; Awofeso et al., 2008) outcomes. Previous applications have predominantly targeted specific care processes or outcomes (e.g. prescribing behaviour; O'Malley et al., 2022). However, while this work has value, factors that contribute to safety and quality often affect multiple outcomes and function at various system levels (Baxter et al., 2018; Reason, 1995; Vincent et al., 1998). As applications of PD typically focus on exceptional individuals and/or healthcare organisations, factors at other system levels such as the practice team (Nelson et al., 2002) are often neglected. A failure to address issues across the system limits the impact as it does not consider the interactions between the different levels of a healthcare system (Ferlie & Shortell, 2001). Latent and abstract factors (e.g. organisational culture and team relations) often underpin a range of outcomes and have directly impacted patient care (Baxter et al., 2018; Reason, 1995; Vincent et al., 1998). As such, identifying and sharing associated strategies may stimulate more far-reaching improvements in quality (Baxter et al., 2018). Understanding these behaviours also provides crucial contextual information around how exceptional care is delivered (Bradley et al., 2009; Lau et al., 2015). Importantly, PD addresses this enduring implementation issue by integrating organisational context into the understanding of best practices (Bradley et al., 2009). This elucidates both the ‘what’, specific practices that positive deviants use to succeed, and the ‘how’, the contextual factors that enable this (Baxter, 2016).
A recent review (O'Malley et al., 2022) synthesised previous applications of the PD approach in primary care to develop a theoretical framework of factors associated with positively deviant care outcomes in primary care: the Identifying and Disseminating the Exceptional to Achieve Learning (IDEAL) framework. The IDEAL framework comprises factors that enable positive deviants to achieve ‘exceptionally good care’ delivery (O'Malley et al., 2022), which can be conceptualised as the capacity of individuals, teams, and practices to deliver an outstandingly high-quality of care across various different outcomes. Theory building is essential for understanding potential causal links between different factors and the context within which a phenomenon occurs and for guiding research (Bradley et al., 2007) and developing evidence-based interventions (Craig et al., 2008).
While the IDEAL framework provides a robust overview of factors associated with PD in primary care, there is a need to refine this theory further to ensure all factors are comprehensively assessed and to examine the applicability of the identified factors in a novel context (Baxter, 2016; Maxwell, 2021). Furthermore, meaningfully incorporating a stakeholder perspective gives theory the greatest potential to both advance knowledge and guide practice (Storberg-Walker, 2003). As much of the PD research synthesised within the IDEAL framework lacked the patient’s voice (Baxter, 2016), integrating the lived experiences of both patients and practice staff will allow a more rich understanding of exceptional care delivery (Creswell & Creswell, 2017) and ensure that findings are relevant, valid, and transferable (Boaz et al., 2018; Terwee et al., 2018). Accordingly, this study aims to extend our understanding of the factors associated with exceptionally good care delivery (O’Malley et al., 2022) in general practice using semi-structured interviews with patients and practice staff. Specifically, we sought to explore and compare stakeholders’ perceptions of the factors that support exceptional care delivery and to test and refine the IDEAL framework pertaining to excellence in general practice care delivery.
Materials and Methods
Theoretical Frameworks
While many PD frameworks have been developed for public health and other settings (e.g. Marsh et al., 2004; Sternin, 2002), guidance by Bradley et al. (2009) was used as it was specifically designed for applying PD principles in healthcare settings. According to the approach, positive deviants are identified (Stage 1) and studied using qualitative methods to identify strategies that help them succeed (Stage 2), the efficacy of which are then tested statistically in more representative samples (Stage 3), and finally, the most effective strategies are disseminated to others (Stage 4). The study’s methods aligned with Stage 2 of the PD framework (Bradley et al., 2009) by using qualitative methods to generate hypotheses about factors that support the delivery of exceptional general practice care. While the use of routine data is recommended to identify positive deviants, our study took a modified approach to studying exceptional care delivery aligned with principles of PD. In addition, a Safety-II approach informed the study. This encompassed a focus on ‘work as done’ to consider everyday performance variability and identify adaptations that allow staff to respond to varying conditions; a concern with understanding the whole system and explicating how the system achieves success; and a focus on helping staff build adaptive capacities and capabilities for working successfully in unpredictable complex systems (Hollnagel et al., 2015; Plunkett & Plunkett, 2022). This approach to studying exceptional care delivery was undertaken due to the study’s recruitment period coinciding with disruptions to Irish general practice caused by the COVID-19 pandemic (Homeniuk & Collins, 2021) and a lack of publicly available data for general practice in Ireland (Moran, 2016). A qualitative approach was also chosen as the analysis of organisations requires open-ended, qualitative methods to explore both the specific strategies these organisations use and the broader context in which they function (Patton, 2002).
In addition, interview data were analysed in accordance with the IDEAL framework (O'Malley et al., 2022) of factors associated with positively deviant care in primary care. This framework consists of 37 categories distributed across seven system levels and was derived from a systematic review by the authors (O'Malley et al., 2022) of previous applications of PD. The 3 system levels of this framework (macrosystem, network, and national levels) were combined to ensure feasibility of the interview guide and due to the similar degree of control practices have over factors at these levels. Accordingly, factors supporting exceptional care were explored across five levels of the general practice system: 1. the patient level, the individual receiving care in general practice; 2. the provider level, the individual directly providing patient care in general practice; 3. the microsystem (team) level, the group of professionals working together to provide care to discrete populations of patients in general practice; 4. the mesosystem (practice) level, the general practice, including its physical environment and how it is managed; and 5. the macrosystem, network, and national levels, the organisation of general practice services within the community and its interface with secondary care, along with policies, supports, and external organisations impacting general practice at a national level.
The design of our study was informed by Clinical Microsystems Theory (CMT) (Nelson et al., 2002), a systems approach to change that appreciates the complexity of healthcare. Accordingly, care was evaluated across multiple levels of the primary care system, including the clinical microsystem (i.e. practice team), a level often omitted from PD research (Baxter, 2016). CMT thinking has been valuable in developing staff-led improvement programs (Janamian et al., 2014), including applications of PD in primary care (e.g. Kirsh et al., 2012).
Setting
General practice is the first point of contact within the Republic of Ireland’s healthcare system, providing approximately 29.1 million consultations annually (Collins & Homeniuk, 2021). General practices in Ireland are operated independently of the state healthcare system, the Health Service Executive (HSE). The HSE was established in 2005 as the single body with statutory responsibility for the management and delivery of health and personal social services in the Republic of Ireland, accountable directly to the Minister of Health (Health Service Executive, 2011). While 90% of practices are privately operated (O'Kelly et al., 2016), around 89% of practices are contracted by the HSE to provide free healthcare access to 43% of patients with public coverage (Homeniuk & Collins, 2021; Health Service Executive, 2019). Increasing workload and a looming shortfall in general practitioners (GPs) (Irish College of General Practitioners, 2022) has worsened since the COVID-19 pandemic, causing significant disruptions to operations in general practice (Homeniuk & Collins, 2021). Despite the increasing use of IT, publicly available quality data for general practice is not widely available (Shi, 2012). In the Republic of Ireland, there is little agreed data generated by GPs themselves (O’Dowd et al., 2017), and obtaining access is challenging due to patient safeguarding (Moran, 2016).
Participants and Recruitment
Opportunistic and maximum variation purposive sampling techniques were employed to ensure a heterogeneous sample with regard to age, gender, and healthcare profession/role of participants (Suri, 2011). Participants were recruited from two main stakeholder groups in general practice (patients and practice staff) and so included any adult with experience in receiving, providing, or managing general practice care in the Republic of Ireland (i.e. patients, GPs, practice nurses, and practice managers). In August 2021, advertisement materials were posted on social media and shared by email with relevant university departments, research networks, and professional bodies. As financial reimbursement addresses barriers against participation (VanGeest et al., 2007), participants were entered into a €50 voucher raffle.
Data Collection
Data were collected using semi-structured interviews, as they are frequently used in a healthcare context to collect new data (DeJonckheere & Vaughn, 2019) and allow the exploration of participants’ unique perspectives without imposing assumptions (Baxter, 2016). An interview guide was developed (see Supplementary Item 1) and piloted with a patient and a GP and modified as necessary. Open-ended questions and probes, loosely informed by other PD investigations (Baxter, 2016; Goff et al., 2020), explored what exceptional care looks like at the five different levels of the general practice system (e.g. ‘If we think about an exceptional practice team, how do they work together?’). For the purpose of this study, ‘exceptional care’ is framed and explicated as the delivery of an outstandingly high quality of care that is perceived as effective, safe, efficient, patient-centred, timely, and equitable to an exceedingly high standard. At the beginning of each interview, participants were introduced to the concept of ‘exceptional care’ and were asked to discuss the factors they believe support exceptional care delivery from their experience of receiving or providing care in general practice. Identifying factors actually used in practice to support exceptional performance is core to PD and Safety-II, and so factors that were deemed unattainable (e.g. personal physician available within 24 hours) were not discussed further or coded during the analysis. Interviews were conducted by video call (i.e. Zoom) at a time convenient for the participant between August 2021 and November 2021 until data saturation (Kuzel, 1992) was achieved within the two main stakeholder subgroups: patients and practice staff. Data saturation was considered in accordance with principles proposed by Francis et al., (2010) for determining saturation in theory-based interview studies with pre-established conceptual categories. Accordingly, data saturation was achieved when no new categories shared by at least two participants were identified in two consecutive interviews.
Reflexivity
The interviewer (i.e. the first author: female PhD-level health services researcher) had an ‘insider’ status with practice staff due to their shared understanding of care delivery but was an ‘outsider’ to the direct provision of care (Gair, 2012), which may have allowed participants to speak as experts in their field (Elliott & Ragsdale, 2020). Similarly, having experience mostly as a patient, the interviewer shared an ‘insider’ status with patients, who may have felt more comfortable discussing care experiences with someone working outside of general practice. Having both an insider and outsider status with participants created a more balanced perspective in the analyses. Moreover, the COVID-19 pandemic likely impacted the interviewing experience. For example, video conferencing software may dull communication and rapport (Humphries et al., 2022); however, talking with participants before the interview helped build rapport. Further, given concerns of virus transmission (Verhoeven et al., 2020), participants may have preferred the privacy and flexibility of online interviews. Due to the sampling strategies, the interviewer was previously acquainted with some of the participants.
Data Analysis
Interviews were digitally recorded and transcribed verbatim and imported into NVivo software for data management and coding (Noble & Smith, 2015). Pragmatism was adopted as the study’s epistemological position (Dures et al., 2011), as it recognises the importance of identifying solutions to problems and understanding the context within which a phenomenon occurs (Creswell & Creswell, 2017; Dures et al., 2011) and allows for the exploration of both the ‘what’ and ‘how’, using combined qualitative and quantitative assumptions (Creswell & Creswell, 2017). In addition, as the current analysis sought to apply the framework of PD factors (O'Malley et al., 2022) to understand stakeholders’ perceptions of the factors supporting exceptional care delivery in general practice, a directed content analysis approach was adopted (Assarroudi et al., 2018; Elo & Kyngas, 2008; Hsieh & Shannon, 2005). This analytic approach was selected as it is commonly used in healthcare research (Elo & Kyngas, 2008) to test if/how data fits into existing theories (Assarroudi et al., 2018; Mayring, 2004). Moreover, theory building requires both deductive and inductive reasoning (Storberg-Walker, 2003), and this approach supplements the deductive analysis of data using pre-determined categories (Hsieh & Shannon, 2005) with the inductive analysis of newly established categories (Assarroudi et al., 2018), allowing factors to be supported, refined, and extended in a new context (Hsieh & Shannon, 2005).
The full data analysis process is explicated in Supplementary Table 1. In essence, a formative categorisation matrix based on the IDEAL framework (O'Malley et al., 2022) was developed, along with a codebook outlining coding rules (Assarroudi et al., 2018). Once familiarised with the transcripts, two researchers (a PhD candidate and a PhD-level human factors psychologist) independently coded ten transcripts to test the categorisation matrix. Codes and categories were continuously refined regularly throughout the analysis by the authors, and discrepancies were discussed until achieving consensus (Mayring, 2004). The lead author analysed the remaining transcripts with a concurrent rechecking and reworking of factors to increase reliability (Mayring, 2014). Following the main data analysis, categories and subcategories were inductively analysed, whereby similar or dissimilar categories were combined appropriately (Dey, 1993) as far as was reasonable (Elo & Kyngas, 2008). An example of this process is presented in Figure 1. While typically calculated within summative content analyses (Hsieh & Shannon, 2005), frequency analyses have also been used within a DCA (Akdemir & Yenal., 2021; Brown et al., 2021). Frequencies were collated here to address the study’s second research aim and compare salient factors between groups (Schilling, 2006). Definitions and illustrative quotes were also provided, and figures were created using Edraw Max software. Example of inductive abstraction process for Leadership category.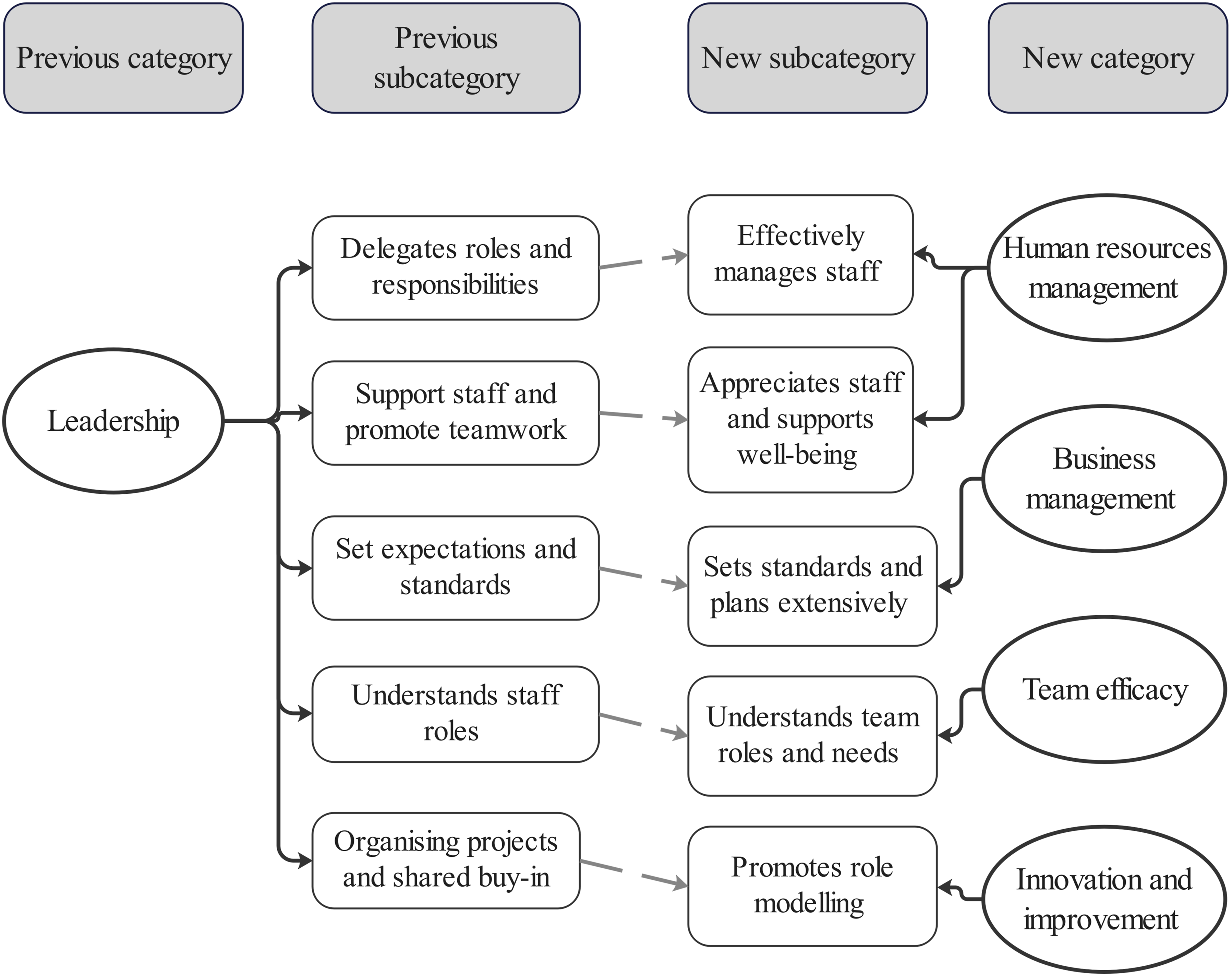
To ensure trustworthiness, the study followed procedures by Lincoln and Guba (Lincoln & Guba, 1985). To enhance the study’s confirmability and dependability, a reflective journal and audit trail were maintained (Houghton et al., 2013; Toffoli & Rudge, 2006). Furthermore, transcripts were read several times and category choices were discussed until reaching consensus (Graneheim & Lundman, 2004). Credibility was ensured through member checking of both the initial transcripts to confirm accuracy and a summary of the study’s findings to ensure agreement with interpretation of the data, and minor changes were made to the transcripts and data interpretation where necessary. Incorporating a variety of unique perspectives and providing detailed research descriptions enhanced transferability (Houghton et al., 2013). Moreover, the use of coding stripes within NVivo supported inter-researcher agreement (Jackson & Bazeley, 2019), and annotations facilitated transparent decision-making and provided an audit trail (Houghton et al., 2013). In addition, NVivo allowed coding to be located, checked, and compared (Houghton et al., 2013), and matrix-coding queries provided a comparison of salient categories (Bassett, 2010).
Ethical Approval
Ethical approval for the study was obtained from the Institutional Review Board at the university of the lead author. Participants were sent study information and subsequently received an electronic consent form to complete prior to the commencement of each interview. To protect participants’ psychological wellbeing when sharing their experiences, an ‘ethics of care’ was developed and practiced with participants to map out how and by who care would be provided to participants (Milligan & Wiles, 2010) and to ensure contextual sensitivity, responsiveness, and attentiveness during the interview (Hankivsky, 2004).
Results
Participants
Demographics of Participants.
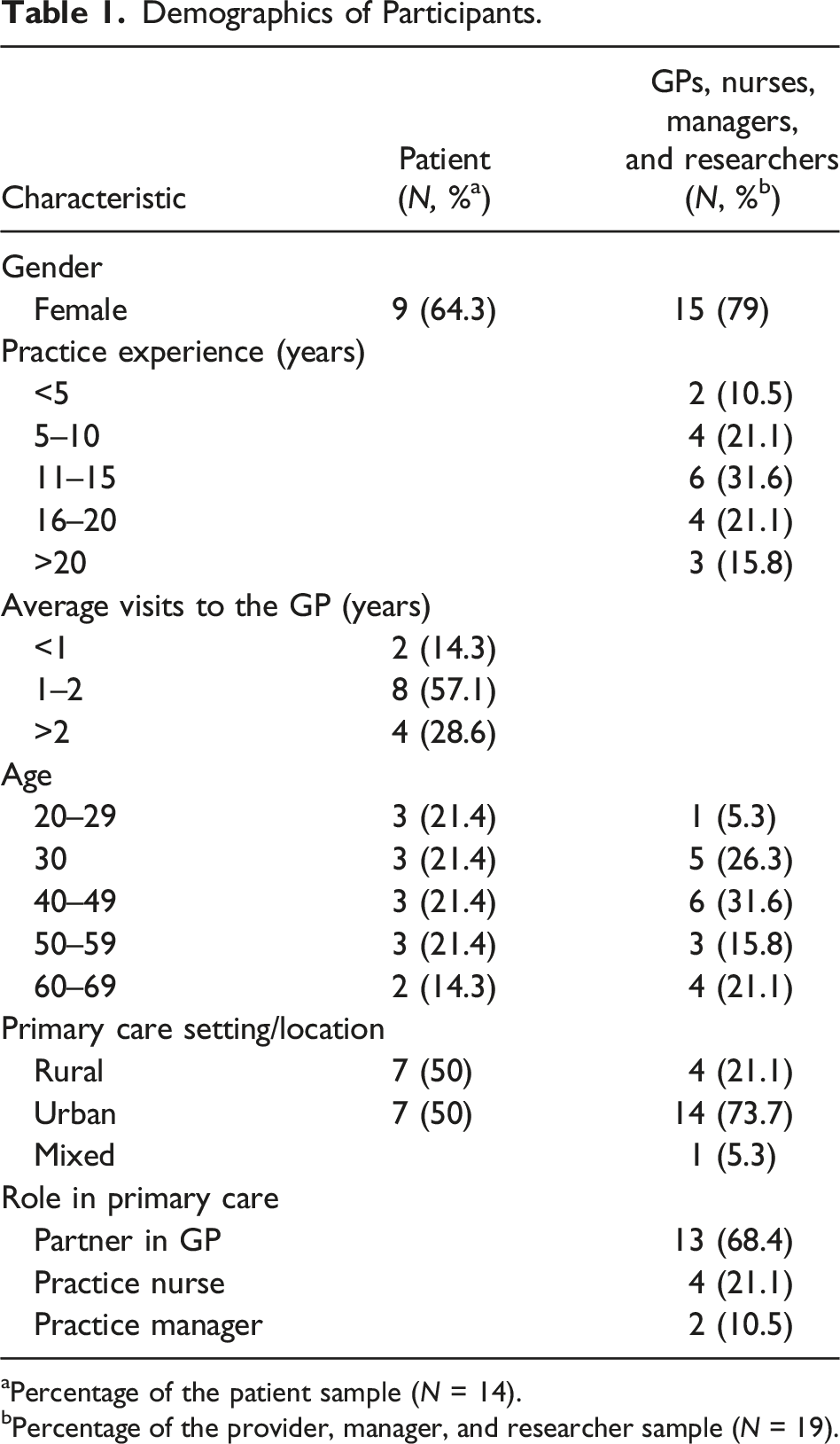
aPercentage of the patient sample (N = 14).
bPercentage of the provider, manager, and researcher sample (N = 19).
Refined Framework
In total, 1,912 meaning units representing unique factors supporting exceptional care were coded across all interviews. This resulted in the refinement of the IDEAL framework into 28 categories and 104 subcategories across five system levels (i.e. from a previous 37 categories across seven system levels; see Figure 2 for revised framework). The following sections chart and illustrate each level of the refined IDEAL framework. IDEAL framework of factors that support the delivery of exceptional care in general practice.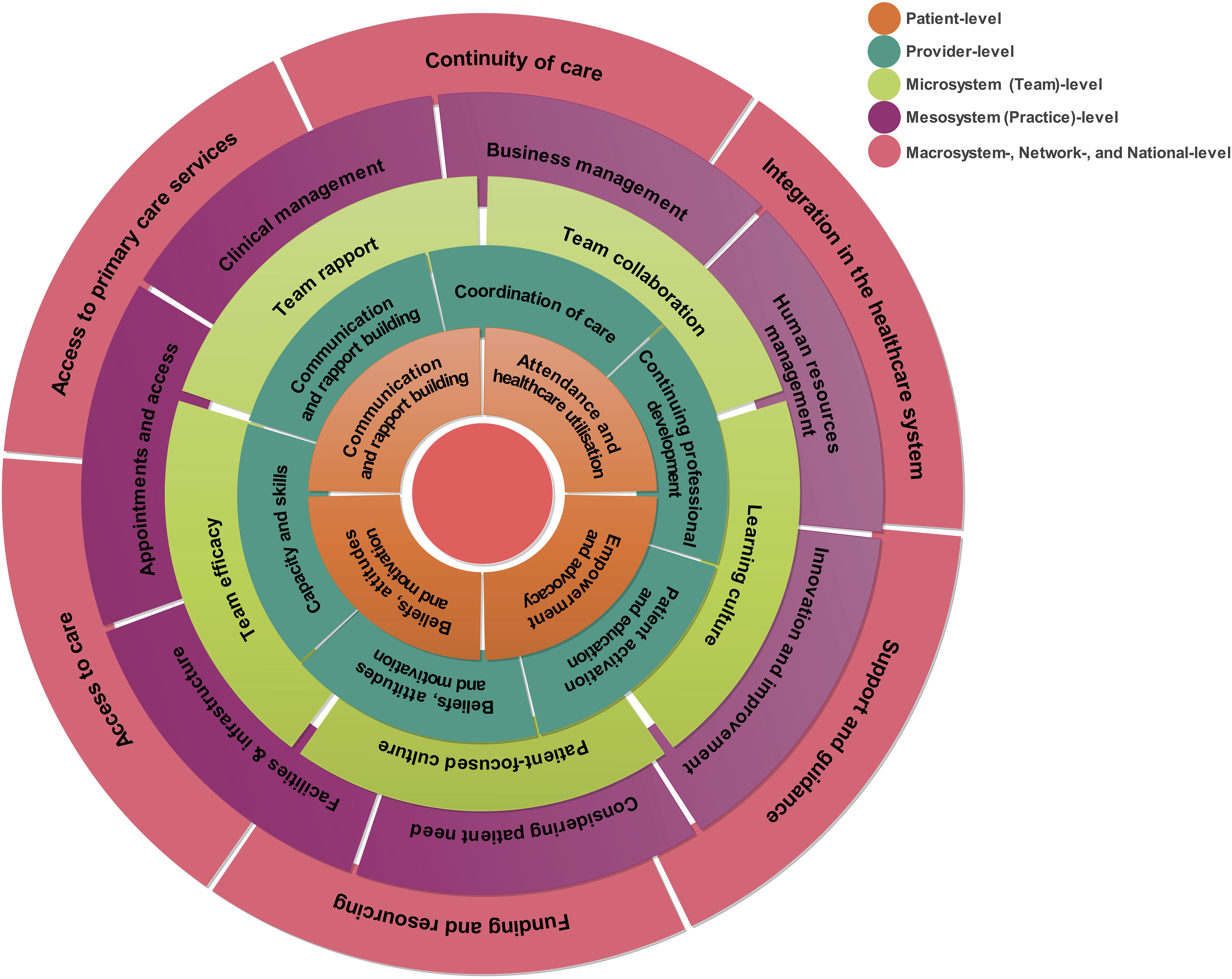
Patient Level
A comprehensive list of categories and subcategories with supporting quotations are provided in Supplementary Table 2. Participants described how patients with a sense of empowerment and the ability to self-advocate can help support the delivery of exceptional care by, for example, engaging in shared decision-making. Participants also valued patients’ efforts to communicate and build rapport with the provider, such as treating the provider with kindness and respect. Moreover, the patient’s beliefs, attitudes, and motivation around healthcare play a role in supporting care, such as having realistic expectations, as well as a patient’s attendance and healthcare utilisation behaviours at the practice.
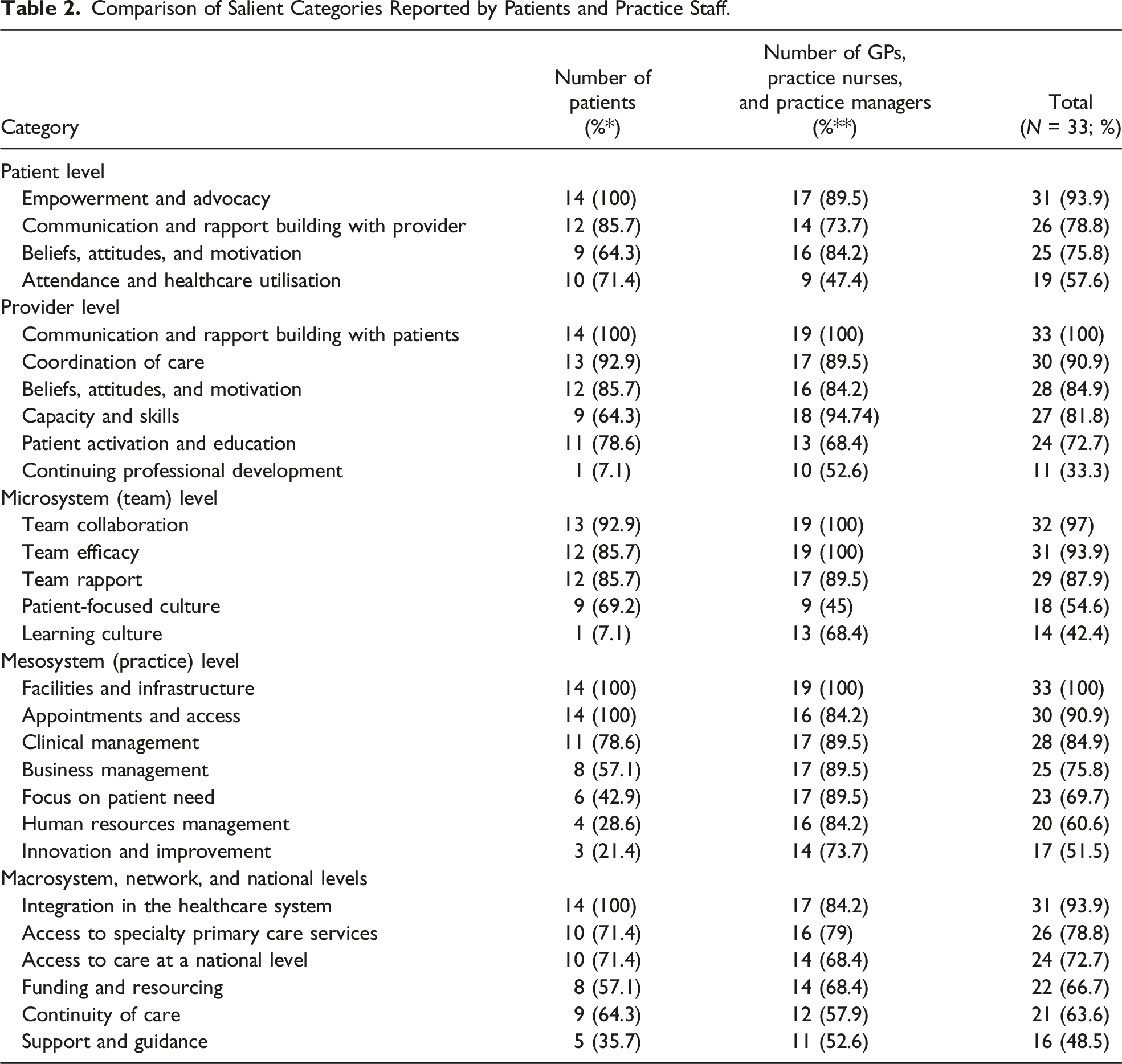
Comparison of Salient Categories Reported by Patients and Practice Staff.
Provider Level
All participants expressed the importance of communication and rapport building with the patient, supported by listening to patients, for example. Efforts by the provider to ensure seamless coordination of care were also important, such as organising good follow-up care. Moreover, the internal beliefs, attitudes, and motivation of the provider can help support the delivery of a higher quality of care, such as having a holistic approach to healthcare. The provider’s capacity and skills are also important, including, for example, having extensive time management and organisational skills. Participants also described activating and educating patients as an important factor enabling exceptionally patient-centred care, and it was noted that nurses often have a more pivotal role in supporting chronic disease management, health promotion, and preventative care. Finally, continuing professional development is important for providers looking to deliver care in line with best practice.
Patients emphasised patient activation and education more often than GPs, practice nurses, and managers. However, while patients typically discussed the provider’s efforts to support behaviour change, providers described educating patients and shared decision-making more often. Unsurprisingly, healthcare and administrative staff discussed the provider’s capacity and skills more often, along with the importance of continuing professional development. Modifications were made to categories at the provider level, which was refined from seven categories to six categories (see Supplementary Table 3).
Microsystem (Team) Level
The vast majority of participants expressed the importance of effective team collaboration in supporting the delivery of exceptional care, facilitated by regular practice meetings, for example. The team’s efficacy beliefs were also an important enabling factor, such as valuing team members and having a multidisciplinary team structure. Furthermore, rapport between team members was discussed frequently, whereby team members support one another and have good relationships. Having a patient-focused culture centred on valuing and respecting the patient was also essential, as well as fostering a learning culture where teams embrace change and have dedicated learning time.
At the team level, patients were more likely to identify factors related to the team’s patient-focused culture. Conversely, GPs, practice nurses, and managers reported more factors related to the team’s efficacy, such as having a multidisciplinary structure, and the team’s learning culture, such as being willing to learn when things go wrong. Categories at the team level were refined from six categories into five categories (see Supplementary Table 3).
Mesosystem (Practice) Level
All participants discussed the role of the practice’s facilities and infrastructure in providing exceptional care to patients and valued, for example, having a pleasant environment with good accessibility. Appointments and access was considered a key factor by most participants, who valued having different ways to book appointments, for example. Moreover, the management of clinical processes enabled exceptional care delivery, such as utilising robust systems for clinical management, as well as having a business management orientation, supported by highly organised practice management. Considering patient need within the practice set-up was also essential in providing exceptionally good patient-centred care. Finally, how the practice manages its human resources was important, as well as efforts by the practice to continuously innovate and improve care.
Patients placed a greater emphasis on appointments and access compared with GPs, practice nurses, and managers; however, while patients valued different ways to book appointments and efforts to facilitate access, providers and practice managers described having systems for appointment scheduling more often. In contrast, providers and practice managers were more likely to discuss the practice’s clinical, business, and human resources management. Practice staff also mentioned the importance of innovation and improvement more frequently, along with efforts to consider patient need in practice operations. Following framework modifications, the 11 original categories were refined to seven categories (see Supplementary Table 3).
Macrosystem, Network, and National Levels
Most participants considered access to specialty primary care services and continuity of primary care as two essential factors enabling exceptional care as patients seek further services in the community. Almost all participants valued integration of primary care in the wider healthcare system, with timely access to specialists and diagnostics, for example. Most participants also valued access to care at a national level, including timely general practice care for both public and privately insured patients. Moreover, funding and resourcing was key in supporting the delivery of exceptional care, as well as national support and guidance for staff in general practice.
Providers and practice managers mentioned access to specialty primary care services, including proximally located general practice services, more frequently than patients, as well as support and guidance from the health system, including the engagement of general practice stakeholders in policymaking. The nine categories at this level were refined to six categories (see Supplementary Table 3).
Discussion
This article applied the framework of factors associated with PD (O'Malley et al., 2022) to explore stakeholders’ perceptions of the key factors needed to support the delivery of exceptional care in general practice. Several distinct strategies (e.g. patient activation and team collaboration), structures (e.g. facilities and infrastructure), and contextual factors (e.g. communication and rapport, and team cultures) required to achieve exceptionally good general practice care were identified across five system levels, and differences were observed in the perceptions, values, and expectations of stakeholders. In addition, refinements were made to the IDEAL framework by incorporating the perspectives of key stakeholders, as to ensure that all potential factors were identified and that previously identified categories were transferable to a novel context and relevant to those directly involved in delivering and receiving general practice care.
Similar to previous applications of PD, cultural and social contextual factors were found to be essential to delivering exceptional care (Baxter et al., 2019). Maintaining long-term collaborative relationships (Razouki et al., 2016) was believed to be core to delivering exceptional care in general practice, and there was a clear symmetry in personal aspects of the patient–provider relationship valued by interviewees, suggesting a true partnership (e.g. listening, trust, friendliness, and respect (Lings et al., 2003)). Likewise, supportive relationships among team members were pivotal in creating a caring environment for both patients and staff (Wei & Watson, 2019). Given its relationship with quality (Wei et al., 2018), creating a caring culture may generate more positive patient, provider, and organisational outcomes (Durant et al., 2015; Johnson et al., 2016; Sánchez-Hernández et al., 2009; Wei et al., 2018). One potential strategy for fostering more effective supportive working cultures might involve targeting and developing the positive cultural factors identified by this study and similar research (Baxter et al., 2019).
In addition to contextual factors, many strategies well-established as supporting exceptional care were identified (e.g. coordinating future care (McAllister et al., 2013)). Interestingly, some studies have found no difference in what strategies exceptional performers use; instead, contextual characteristics influenced how they were implemented (Baxter et al., 2019). Similar to Baxter et al. (2019), our study found that having multidisciplinary staff did not necessarily mean better collaboration (Liberati et al., 2016); rather, having good team efficacy beliefs and fostering a patient-centred learning culture facilitated effective collaboration. As the context within which teams perform is just as important as what they do (Robert & Fulop, 2014), improving the behaviours and cultures underpinning the delivery of specific strategies may result in greater improvements than developing new ways of working (Baxter, 2016).
Consistent with the literature, most practice-level factors constituted infrastructure, organisational structures, and processes used to deliver care (Goff et al., 2020; Rand et al., 2020). Strengthening these factors, referred to as the practice’s core (Miller et al., 2010), can benefit the patient. For example, Jamshidi et al. (2020) linked several aspects of the practice environment to patient outcomes (e.g. music and lighting). However, it is important to note that outcomes influenced by the physical environment are mutually contingent upon the social environment (Ruga, 2008). Furthermore, identifying modifiable factors that teams can learn from and change may be more useful (Lawton et al., 2014). The contextual elements, or ‘adaptive reserves’ (Miller et al., 2010), previously discussed impact care quality (Goff et al., 2020) and can be modified effectively (Weaver et al., 2013). Thus, similar to the patient, provider, and team levels, improving practice-level performance requires a strengthening of the practice’s adaptive reserves in addition to building the practice’s core (Miller et al., 2010).
External to the practice, many of the system attributes identified are well-documented as impacting patient outcomes, including access, continuity, and integration (Andres et al., 2016; Kringos et al., 2010; McMurchy, 2009). Notably, many system-level factors identified by participants were prescriptive as opposed to descriptive of the current system. While timely and equitable (Wolfe, 2001) access to care is essential, it was commonly noted that patients without private insurance face considerable difficulties in accessing timely care (Goldrick-Kelly, 2018). However, despite severe system constraints, many providers still manage to deliver exceptional care, oftentimes ‘exceeding patient expectations’ (Levine et al., 2012) (e.g. offering to see certain patients more often). Given the additional workload and time required to deliver exceptional care, without appropriate system supports it will inevitably come at a cost to the provider (e.g. burnout (Pérez-Francisco et al., 2020)). Again, the presence of these barriers reinforce that it is how exceptional performers work together and overcome challenges that distinguishes them (Razouki et al., 2016). Moreover, research indicates when staff have the tools, they are intrinsically motivated by improving the care of patients (Rand et al., 2020; Ryan & Deci, 2000). As such, efforts to strengthen the internal capability of general practice should be supplemented with a tackling of system-level barriers (Kim et al., 2008).
Consistent with extant literature, patients, providers, and practice managers largely agreed upon the core aspects of high-quality general practice care (Levine et al., 2012); however, some notable differences were observed (Campbell et al., 2002). Interestingly, many factors assumed a distinct reality contingent on the perspective (Lings et al., 2003). When discussing collaboration at the team level, for example, staff discussed having regular meetings while patients perceived the ease at which they received care between staff (e.g. administrative staff dealing with repeat prescriptions). It is unsurprising that patients also perceived more latent factors, given that they are astute observers of their care (Donaldson, 2015) and evaluate service quality experientially (Johnson et al., 2016). Accordingly, patients also frequently mentioned availability, accessibility, and communication (Campbell et al., 2002; Levine et al., 2012). Conversely, providers and practice managers report more aspects of care that go on behind the scenes (Levine et al., 2012). GPs commonly mentioned professional standards and visit coordination (Campbell et al., 2002; Frankel et al., 2005), practice managers elucidated factors required to run the organisation, and practice nurses frequently discussed activating and engaging patients (Baxter, 2016).
One explanation for the observed discrepancies between patients and practice staff is differences in values or perceived expectations between stakeholders (Levine et al., 2012). This was particularly evident at the patient level; while patients in particular felt it was important to attend appointments on time, providers valued when patients work to the best of their abilities and understand the constraints of general practice. This highlights the extent to which providers value the patient–provider partnership (Levine et al., 2012). As alluded to by participants, exceptional general practice care transcends the achievement of clinical targets, characterised instead by sustained partnerships with patients and providing long-term holistic family and community-oriented care (Starfield et al., 2005). This finding also highlights the impact a patient’s expectations have on their perceived role and conceptualisations of high-quality care (Andres et al., 2016). As noted in the interviews, providers have a pivotal role in nurturing the ‘exceptional patient’ (Collins & Rochfort, 2016). Working with patients to develop their role expectations (Yeh et al., 2018) may help them achieve empowerment (Salord et al., 2021), which research has linked with improved satisfaction (Yeh et al., 2018), healthcare utilisation, and clinical outcomes (Wong et al., 2014). As engaging different stakeholders provided more complete and contextualised information, future research exploring perceptions of care needs to engage the whole team, including the often overlooked patient (Baxter, 2016).
Engaging with key stakeholders in general practice informed the refinement of the IDEAL framework into 28 categories and 104 subcategories across five system levels. Incorporating the perspectives of different participants facilitated the exploration of whether perceptions of key factors converge, complement one another, or diverge (Vogl et al., 2018). While most modifications were minor, such as merging categories due to similar content (e.g. beliefs and attitudes and motivation) or renaming categories to reflect newly emerging subcategories (e.g. self-efficacy renamed to empowerment and advocacy), engaging with the perspectives of patients and staff also supported the identification of newly emerging categories. For example, facilities and infrastructure, which has not been identified by previous PD primary care investigations, was added as a new category, as all participants described aspects of the practice environment that they felt supported the delivery of exceptional care (e.g. wheelchair friendly). As the practice environment can potentially affect patient outcomes (Jamshidi et al., 2020) and many environmental features are relatively low cost to improve (e.g. paint and music) (Ruga, 2008), the addition of this category to the framework is practicable.
Strengths and Limitations
The diversity of the sample in terms of gender, age, and location of practice is a methodological strength and was important as patients’ satisfaction varies according to these characteristics (Johnson et al., 2016). In addition, gathering multiple perspectives increases the applicability of findings (Sabzmakan et al., 2014) and provides a more ‘complete picture’ (Baxter, 2016). While interviewees were predominantly women, this was expected as most patients (Wang et al., 2013), GPs under 55 years old (O'Kelly et al., 2016), nurses (Health Service Executive, 2019), and managers (Health Service Executive, 2019) are women. Furthermore, engaging interviewees from across Ireland and those with broad oversight of general practice (e.g. GPs involved in education) supported the validity of findings (Baxter, 2016). In addition, the multidisciplinary composition of the research team (a PhD candidate with background in health psychology, a human factors psychologist, a behavioural psychologist, and a GP and clinical lecturer) enhanced rigour (Hall et al., 2018).
The study’s primary limitation is that positive deviants were not identified using routine quality data (O'Malley et al., 2022) due to COVID-19 and data accessibility issues. However, simply using a PD lens to explore exceptional care inspired discourse (Toscos et al., 2018), and this modified approach allowed us to contextualise the previously developed framework (O'Malley et al., 2022). Second, practice nurses and practice managers were relatively underrepresented in the sample compared with GPs. Recruiting these groups may have been more challenging as there are fewer practice nurses and managers within Irish general practice, and GPs typically have more established professional bodies. Given their invaluable perspective, future research exploring general practice care delivery needs to ensure these stakeholders are meaningfully involved. This would also allow for data saturation to be achieved within each stakeholder group rather across all practice staff, which in turn would ensure that the perceptions and values of each stakeholder had been comprehensively assessed (Hennink et al., 2017). Third, while the generalisability of findings may be questioned, the framework aligned well with interview data and findings are in broad agreement with other studies. Future research based on representative national samples would examine generalisability further (Lings et al., 2003). Finally, while data collection was negatively impacted, disruptions caused by COVID-19 (Homeniuk & Collins, 2021) elucidated important factors allowing teams to respond effectively to these unforeseeable circumstances. As resilience in response to system variabilities is core to PD and Safety-II (Bradley et al., 2009), the factors identified here likely reflect key enablers of resilience.
Implications for Policy, Practice, and Research
Larger policy is needed to strengthen the system-level factors identified (McAllister et al., 2013), particularly as workload (Crosbie et al., 2020) and staffing (Teljeur et al., 2010) are forecast to worsen further in the coming years. A notable finding was the variety of innovative strategies participants both suggested and reported using to counteract system-level challenges (e.g. nurse substitution to increase workforce capacity (Teljeur et al., 2010)). This provides further evidence that meaningfully engaging practice staff in policy development may produce more effective guidance (Gabbay et al., 2013).
In practice, teams should apply the IDEAL framework to understand care within their practice and should implement relevant factors locally (Kirsh et al., 2012). Furthermore, given the importance of contextual factors in supporting the delivery of exceptional care, the measurement of clinical outcomes (e.g. audits) within the practice should be supplemented with measures of cultural factors (e.g. safety culture assessments) (Baxter, 2016) for a more complete assessment of quality.
Finally, consistent links with existing literature indicate that these factors show promise for enabling positively deviant success (Baxter, 2016). However, further research is warranted to determine which factors are associated with clinical performance (O'Malley et al., 2022) and whether an amalgamation of best practices achieves more robust improvement (Taliani et al., 2013). Moreover, the alignment of the framework with interview data contributes to the trustworthiness of the theory (Lynham, 2002), and novel factors (e.g. facilities and infrastructure) and sub-factors/subcategories (e.g. providing holistic care, valuing a patient’s perspective, and exceeding expectations) identified by this investigation enhance its comprehensiveness and relevance to practice. As this framework is still in its infancy, this study sought to purposefully inform and intentionally confirm/disprove the theoretical framework through the participation of patients and practice staff, as recommended in theory building (Lynham, 2002). The refined IDEAL framework has great potential to inform the development of quality improvement tools that support general practice teams in identifying both areas of exceptional performance and those requiring improvement within their practice. One form of improvement tool that supports capacity building are reflection- or discussion-based tools (e.g. MaPSaF (Parker, 2009)). Accordingly, further work to develop the IDEAL framework into a discussion-based assessment tool, to facilitate teams to measure their capacity for delivering exceptional care, and, subsequently, to promote discussion around strategies for achieving improvement (Nancarrow et al., 2015) is recommended. The development of such a tool would need to be supported by robust investigation of its practicability, comprehensibility, feasibility, and relevance to practice (Terwee et al., 2018) to give the resulting tool the greatest potential to both advance theory and guide practice.
Conclusion
As the drive for high-quality general practice gains momentum, we took a modified approach aligned with PD and Safety-II to identify key factors needed to deliver exceptional care. Exceptional general practice is an extraordinarily unique paradigm of caring, characterised by long-term collaborative relationships and teamwork, coordination, and continuity, a propensity for learning, and a holistic focus on the patient. The framework provided herein should be used by researchers, policymakers, and practice teams looking to understand, measure, and achieve exceptionally good care delivery in general practice.
Supplemental Material
Supplemental Material - Identifying Factors that Support the Delivery of Exceptional Care in General Practice and Development of the IDEAL Framework: A Qualitative Study
Supplemental Material for Identifying Factors that Support the Delivery of Exceptional Care in General Practice and Development of the IDEAL Framework: A Qualitative Study by Roisin O’Malley, Sinéad Lydon, Aileen Faherty, and Paul O’Connor in Qualitative Health Research
Ethical Statement
Ethics approval
Ethical approval was obtained from the Research Ethics Committee at the University of Galway on December 1st 2021 (ref. no. 2021.01.012). Participants gave informed consent to participate in the study before taking part.
Footnotes
Acknowledgments
We gratefully thank the patients, GPs, practice nurses, and practice managers who took part in this study and for generously sharing their time, thoughts, and experiences with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Irish Research Council, as part of the Government of Ireland Postgraduate Scholarship Programme [GOIPG/2020/977]. The funder had no active role in the research process or article preparation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.