
Abstract
Medical assistance in dying (MAiD) was introduced into Canadian federal legislation in 2016. Mental illness as the sole underlying medical condition (MI-SUMC) is currently excluded from eligibility; such exclusion is scheduled to expire on March 17, 2024. Irremediability, capacity, quality of life, autonomy, family involvement, and healthcare system constraints have been debated intensively. Recent studies have not explored the views of family members of persons with mental illness on MAiD MI-SUMC. This study aimed to fill this knowledge gap. Twenty-five Ontario residents who had a loved one with mental illness participated. A persona–scenario exercise was designed to explore participants’ views on MAiD MI-SUMC in hypothetical situations. Reflexive thematic analysis was used to analyze the data. A lived experience-advisory panel was engaged throughout the study. Seven themes were developed: Witnessing suffering; A road with barriers and limitations; Societal barriers; The unknowns of mental illness; Individual choices: the life or death that a person wants; MAiD MI-SUMC as an acceptable choice when suffering cannot be relieved with available treatments and supports; and The emotional outcome. Participants constructed their views based on their experience of supporting a loved one with mental illness. MAiD MI-SUMC was perceived as a multifaceted issue, whose acceptability and potential introduction required a concurrent exploration and discussion of the challenges arising due to limitations of the healthcare system, the opportunities and limits to family involvement, and the value of patient autonomy.
Keywords
Introduction
Canadian federal legislation was adopted in 2016 to legalize medical assistance in dying (MAiD) for capable adults with a “grievous and irremediable medical condition” whose natural death was “reasonably foreseeable” (Government of Canada, 2016). Initial legislation included multiple eligibility criteria and safeguards; some of the most relevant were related to voluntariness of the request, capacity, informed consent, two independent assessments, a minimum waiting period between the request and the administration of MAiD, being informed of means available to relieve the requester’s suffering, and securing final express consent immediately before MAiD was provided. The requester can withdraw their consent at any moment. In 2019, the Superior Court of Québec supported a challenge to the reasonably foreseeable natural death criterion on the grounds of a Charter violation (Superior Court of Québec (QCSC), 2019). Hence, in 2021, another eligibility track—commonly known as track 2—was established for persons without a foreseeable natural death. New safeguards for this additional track included, among others, ensuring that the requester, provider, and assessor agree that the means available to relieve suffering have been seriously considered by the requester; consultation with a practitioner with expertise on the requester’s medical condition (if none of the assessors has such expertise); and a minimum 90-day period between the start of the assessment and the moment in which MAiD is administered (Government of Canada, 2021). Persons with mental illness as the sole underlying medical condition (MI-SUMC) were excluded from making a request until March 2023; this exclusion was extended through to March 17, 2024 (Government of Canada, 2023). Other extensive MAiD eligibility criteria and safeguards are in place and described in detail in previous and current assented bills.
In the Netherlands and Belgium, country-wide legislation allowing MAiD was introduced in the early 2000s, and mental illness was not considered differently from other medical conditions for eligibility purposes. In the Netherlands, documented cases of MAiD MI-SUMC precede legislation on MAiD introduced in 2001 (Staatsblad van het Koninkrijk der Nederlanden, 2001; van Veen et al., 2022). In 2021, less than 2% of 7,666 MAiD procedures were performed for mental disorders (Regional Euthanasia Review Committees – RTE., 2022). In Belgium, MAiD was legalized in 2002 (Moniteur Belge, 2002). Figures for the year 2022 indicate that under 1% of 2,966 procedures were for mental disorders (Commission fédérale de contrôle et d'évaluation de l'euthanasie – CFCEE, 2023). The absolute number of total MAiD procedures for all medical conditions, including mental illness, is rising in both countries. The overall prevalence of mental disorders among high-income countries (English-speaking and European) has been reported as comparable (Steel et al., 2014). Other estimates, segregated by global region, point to a 15.15% overall prevalence of mental disorders for the Americas (including Latin America and the Caribbean) and 13.66% for Europe (Castaldelli-Maia & Bhugra, 2022).
Irremediability (Simpson, 2018) and intolerability of suffering (Simmons et al., 2022; van Veen et al., 2022), the impact of mental illness on the requester’s capacity (Dembo et al., 2018; Freeland et al., 2022), the role of suicidality in a MAiD request, and the influence of social determinants of health (Freeland et al., 2022; Health Canada, 2022; Simpson, 2018) are some frequently raised issues in connection with MAiD MI-SUMC. The role of decisional autonomy has also been discussed (Dembo et al., 2018) in relation to pursuing or refusing healthcare and also in relation to MAiD (Health Canada, 2022).
As with many conditions, the views of family members of individuals living with mental illness require careful exploration, as they are frequently tasked with providing care to their loved ones (Smolej et al., 2022) and are emotionally (Goldberg et al., 2021) and relationally (Shankar & Muthuswamy, 2007) impacted by their loved ones’ illness. Family members who are primary caregivers often act as advocates and help navigate the healthcare system to secure care for their loved ones (Pope et al., 2019). Previous studies on MAiD in Canada, for conditions other than mental illness, have explored the support needs of family caregivers of MAiD requesters (Hales et al., 2019; Smolej et al., 2022; Thangarasa et al., 2021) and the psychosocial impact of supporting a loved one who is going through MAiD (Goldberg et al., 2021; Thangarasa et al., 2021), including bereavement (Hashemi et al., 2021; Thangarasa et al., 2021). Nonetheless, the views of family members of persons living with mental illness on the introduction and use of MAiD MI-SUMC have yet to be explored, and this study aimed to do so.
Methodology
Lived Experience Engagement
We worked with two family members of persons with mental illness and two persons with lived experience of mental illness as part of a lived experience-advisory panel. The panel contributed throughout all stages of this study. Two of its members—one family member and a person with lived experience—joined the data analysis team (VC and MRvK), and three supported the report writing (VC, MRvK, and MD). Engagement was guided by the Strategy for Patient-Oriented Research (SPOR) (Canadian Institutes of Health Research – CIHR, 2014). Following our panel’s recommendation, we have adopted the term “mental illness” to present our study procedures and findings. We acknowledge that the term “mental disorder” is employed by major diagnostic classification systems, and different stakeholders can ascribe different connotations or meanings to each term or use them interchangeably.
Theoretical Grounds
We adopted a critical realist ontology (Braun & Clarke, 2021a; Fletcher, 2017); this is an approach that highlights the multiple facets of certain issues—such as MAiD MI-SUMC—that cannot be fully isolated, observed, or measured as they are permeated by social phenomena. Additionally, we embraced a contextualist epistemology (Braun & Clarke, 2021a; Madill et al., 2000), whereby knowledge production is shaped by the context of researchers and participants alike. We strived to identify a diversity of experiences and perspectives, including divergent voices. Our ontological and epistemological positioning allowed us to approach and explore our participants’ views on MAiD MI-SUMC in recognition of the interactions, contexts, and social processes present throughout their lives. We also wanted to remain mindful of how different types of knowledge (i.e., experiential and disciplinary) can be included or excluded depending on the context in which it is produced and disseminated. Highlighting the experiential knowledge of family members who have walked alongside their loved ones with mental illness was paramount. Informational saturation has not been pursued; its epistemological assumption of achieving a completeness of understanding (Braun & Clarke, 2021b) was not commensurate with our aim to explore the uniqueness of the lived experiences of the participants.
We also adopted a reflexive stance (Halverson & Halley, 2023) about our individual experiences and identity attributes that we have brought to the analyses and interpretations presented here. This research team comprised members with varying degrees of mental health expertise, including persons with lived experience, trainees, scientists, and clinicians, and intersections between them. Among our members, there were different levels of lived experience of chronic illnesses, as well as different experiences of healthcare access permeated by sociocultural elements of power, privilege, and vulnerabilities. This team also included members of diverse ethnicities, genders, and immigration histories.
Participants and Recruitment Procedures
We included 25 participants, aged 18+, residing across Ontario, Canada, who self-identified as family caregivers, relatives, or closely connected to a loved one with mental illness. Recruitment occurred between April and December 2022. Our lived experience-advisory panel helped co-design recruitment materials, including e-flyers shared among mental health and caregiver organizations. The Centre for Addiction and Mental Health’s (CAMH) Facebook official account was used to display ads linked to an institutional webpage with contact details. CAMH’s research registry was also used; this is an institutional platform to share participation opportunities with individuals who have expressed previous interest in research. Our lived experience-advisory panel facilitated connections with community organizations and potential participants. Each potential participant completed a screening phone/video call to establish eligibility. Eligible participants had an informed consent discussion with research staff, provided consent, and answered demographic questions about themselves and their loved ones. Data were captured using Research Electronic Data Capture (REDCap) (Harris et al., 2019). A phone/video call was scheduled to complete a semi-structured interview of approximately 1-hour duration. A post-doctoral research fellow, HB, administered all study procedures, including interviews. This study was approved by CAMH’s Research Ethics Board, study number: 158-2021.
Interview
Our interdisciplinary study team, including our lived experience-advisory panel, co-developed a semi-structured interview guide based on a persona–scenario exercise (PSE) (Valaitis et al., 2014): a strategy whereby participants imagine a persona and add details based on prompts. The PSE gives participants the flexibility to imagine a fictitious persona and to introduce details that would make it authentic and representative of their experiences and views. Persona–scenario methods have been used as part of healthcare service-design initiatives (Lokker et al., 2021), as well as a tool for facilitating patient engagement (Chang et al., 2021). Given the sensitive nature of a topic such as MAiD MI-SUMC for family members of persons living with mental illness, PSE provided an emotionally safe opportunity to discuss this topic, in contrast to re-telling their experiences, and those of their loved ones, in response to a direct inquiry.
In this study, the interviewer read a preamble with information about MAiD—definition, eligibility, procedures, and legal status of MI-SUMC—and then conducted the interview. The interview comprised three sections. The first section explored overall views on MAiD MI-SUMC and prompted participants to imagine a person with a mental illness who, in the participants’ opinion, might be inclined to seek MAiD. The second section focused on the imaginary persona’s MAiD MI-SUMC request and assessment, and fictional scenarios in which this could be acceptable, or unacceptable, to the participant. The interview ended with questions about MAiD MI-SUMC and suicidality. The interview was piloted and a lived experience panel member provided feedback. Participants completed the interview by phone, or via video or computer-to-phone calls using Cisco Webex. Only the participant and the interviewer took part in the call, which was audio recorded. Each participant received a CAD $30.00 physical or digital gift card upon completion of the interview. Audio recordings were transcribed by a professional agency, or by research staff/trainee, and proofed for accuracy by a second research team member. Some representative quotes have been lightly edited for clarity.
Analysis
Data were analyzed using an inductive approach to reflexive thematic analysis (RTA) (Braun & Clarke, 2006; 2021a), to ensure that codes and themes were developed directly from the dataset. Transcripts were managed and coded using NVivo 12. Data analysis was led by HB. During familiarization, the lead analyst explored each transcript to gain an initial understanding and panoramic view of the participants’ experiences and opinions. Open coding was then used to identify and label experiences or views related to the research question. Lastly, patterns across the dataset were proposed, and divergent perspectives were identified. Themes were developed and articulated into a narrative. Codes and themes were tracked in Microsoft Excel 2016 for auditing purposes.
The analysis was conducted between December 2022 and January 2023 and supported by a data analysis team (Braun & Clarke, 2021a) that included the lead analyst (HB), two members of our lived experience-advisory panel (VC and MRvK), three psychiatrists (VS, DES, and MG)—two of them with experience as MAiD assessors—and the principal investigator (LDH). This group provided advice on analysis planning, codes/themes delimitation, and narrative structuring. The principal investigator and the lead analyst worked with the entire dataset, while the data analysis team worked with codes, themes, and thematic maps. Procedures, resonance with lived experience, and theoretical issues were discussed in regular meetings.
Results
Demographic Characteristics
Participant characteristics.
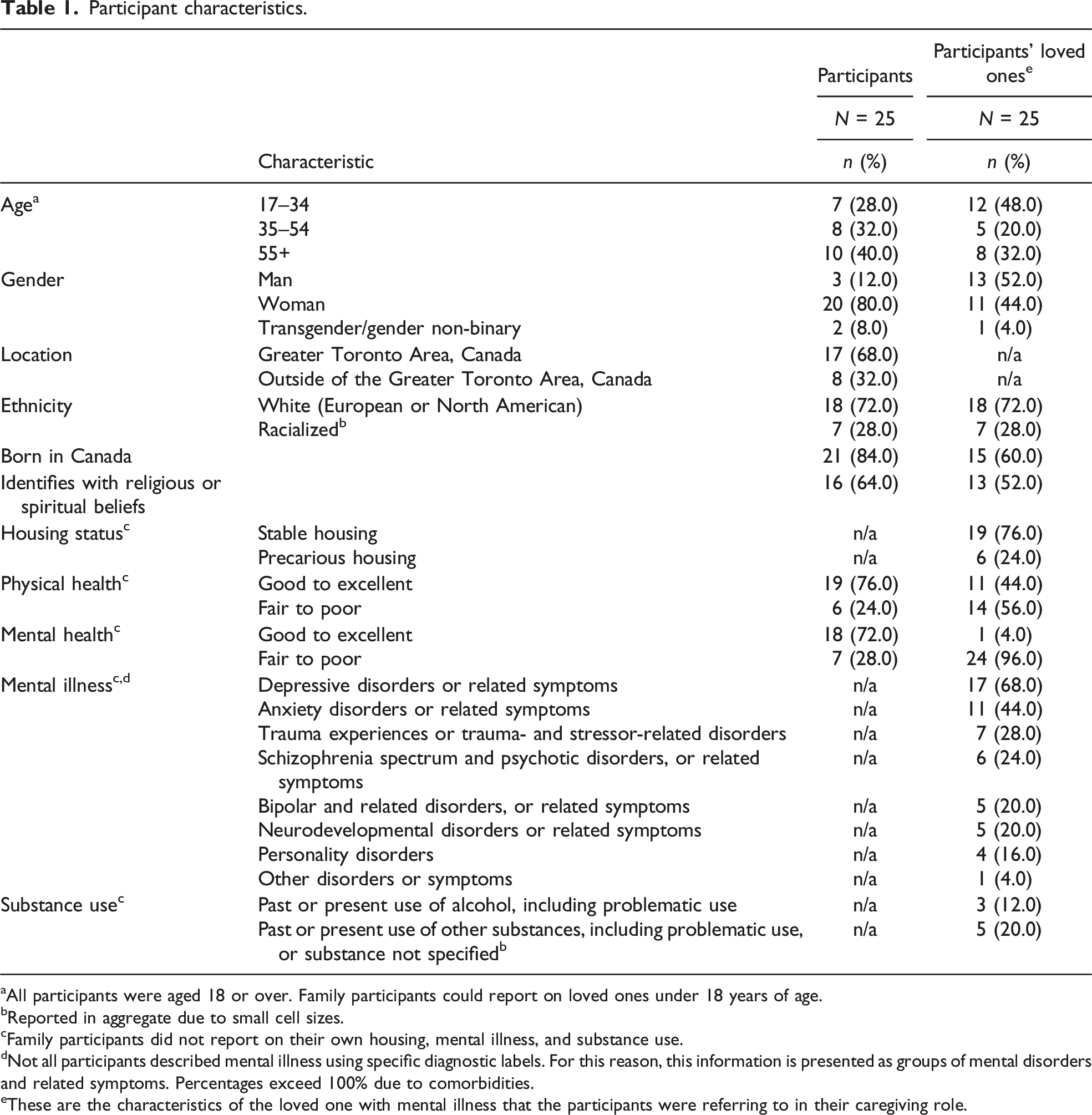
aAll participants were aged 18 or over. Family participants could report on loved ones under 18 years of age.
bReported in aggregate due to small cell sizes.
cFamily participants did not report on their own housing, mental illness, and substance use.
dNot all participants described mental illness using specific diagnostic labels. For this reason, this information is presented as groups of mental disorders and related symptoms. Percentages exceed 100% due to comorbidities.
eThese are the characteristics of the loved one with mental illness that the participants were referring to in their caregiving role.
We identified seven themes, presented in Figure 1. The first three, Witnessing suffering, A road with barriers and limitations, and Societal barriers, depict experiences, challenges, and limitations encountered when supporting a loved one with mental illness. Next, under The unknowns of mental illness and Individual choices: the life or death that a person wants, we discuss individual and contextual elements that helped participants make sense of the trajectories that mental illness can follow and its impact on their loved ones’ lives. These individual and contextual elements inform the individual choices that persons living with mental illness could contemplate in relation to their healthcare. Then, in MAiD MI-SUMC as an acceptable choice when suffering cannot be relieved with available treatments and supports, we discuss how multiple—but not all—views pointed to MAiD as an acceptable choice for some people with a mental illness. Finally, in The emotional outcome, we describe how family members imagined the emotional experience that would be faced by an imaginary person who learns of the outcome of their MAiD MI-SUMC request. The quotes presented herein were derived from 23 out of 25 participant transcripts. Thematic map of participants’ views on MAiD MI-SUMC. Note: A dotted line represents conditional links between elements; the participants’ individual views on each preceding theme might result—or not—in a subsequent connection.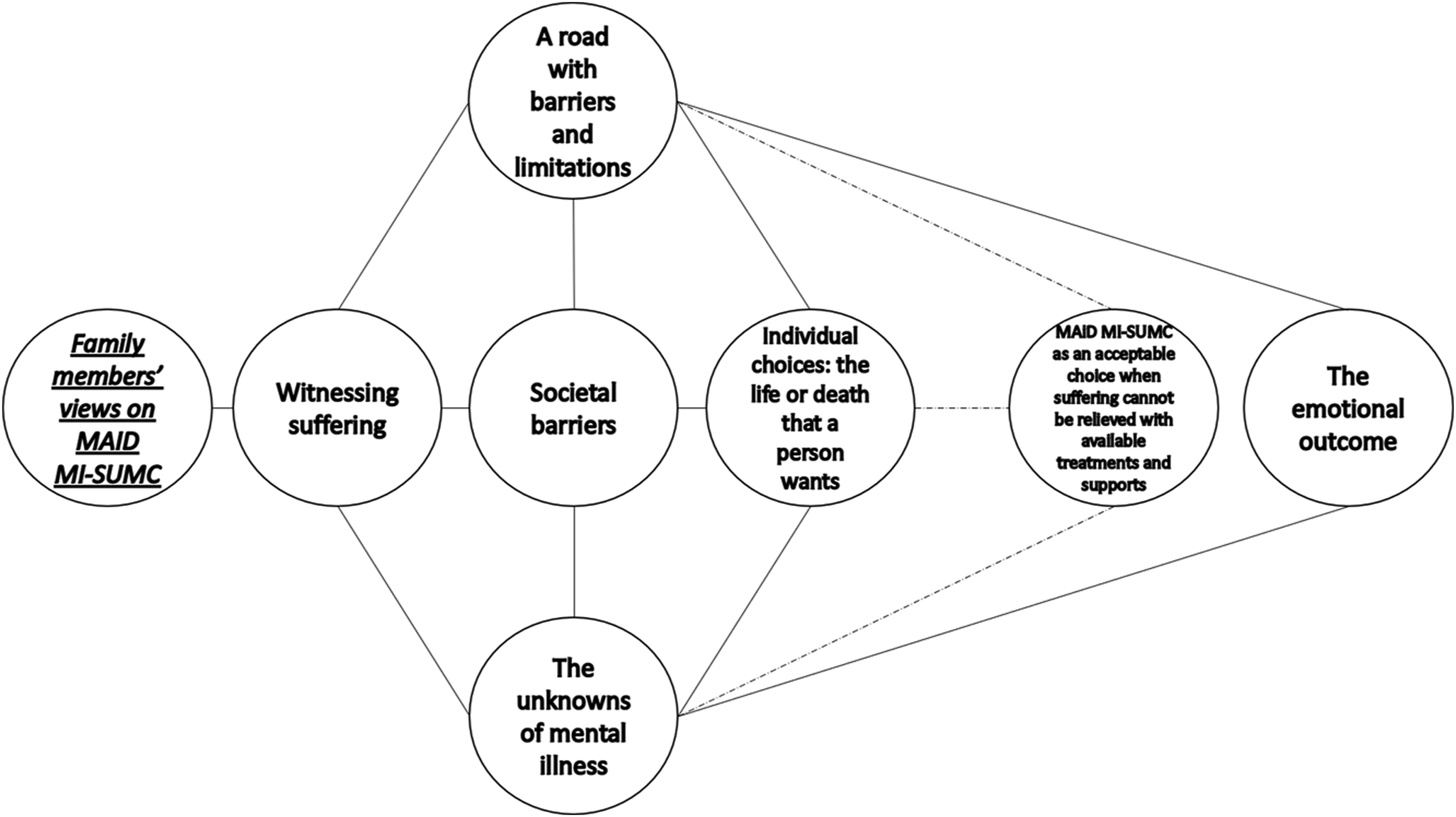
Witnessing Suffering
Caregiving for a loved one with mental illness is a challenging endeavor. Participants witnessed the trajectory of the illness and the negative long-term impacts their loved ones experience on a daily basis. They acknowledged the suffering that has been present during extensive periods of their loved ones’ lives. I see the aftermath of psychoses; I see a beautiful woman curled up in the corner. And then you give her more meds and she comes to be, but she’s still very reserved and not really content. So, it would be unfair for me to make a comment when I’m not living and walking in her shoes, and living in that brain. So, it’s difficult for me to speak on somebody else’s behalf when I’m not walking in their shoes. But I do respect the woman that she is and the challenges that she’s tried to overcome most of her life. I had the concept of mental illness before I had seen what my sister has been through, and now I can see [that], sometimes, there’s so much suffering and pain that she’s not able to manage, you know?
A Road with Barriers and Limitations
Participants generally highlighted difficulties in navigating the healthcare system and finding timely, appropriate mental health supports that met their loved ones’ needs. The healthcare system was described as having limited capacity, as demand exceeds service availability. When a person living with mental illness encounters access barriers, the opportunity to start their recovery journey does not materialize and their well-being is further impacted. So, if you don’t understand how to navigate systems, you don’t know what’s wrong with your mental health. And, I know there are telephone lines where people can call, etc., but I don’t think everybody has that wherewithal. And, unless they have an advocate, which a lot of them don’t, I can see how they would become desperate and in despair, and feeling hopeless. I personally had to help with my children getting the right behavior therapy that they needed. And that was fighting the powers that be to get them that help. So, imagine a parent of typical kids trying to get help and not having anyone listen back. So, never mind an adult, you know, a grown man who was probably one of, you know, thousands that required severe help and didn’t think it was there for him.
Participants also recounted the particular challenges faced by a loved one living with addiction or problematic substance use. Support programs appear to be designed in ways that are not commensurate with the long-term needs associated with addictions. Until we, as a society and a health care system, can find a better way to respond to people in the long term—like, 28-day programs aren’t going to cut it for people that are that entrenched. And we have to get past that nonsense of “you fix people in 28 days”; you don’t. It’s a longitudinal journey that we need to walk alongside with people. And the healthcare system just isn’t set up to do that. And, if we’re not prepared to help people to do that, then I think we need to give them some dignity to make some choices.
We also heard how, in times of crisis, participants wished to protect and help their loved ones to a greater extent, but they were constrained by the limited resources and supports available. Those resources and supports targeted immediate safety needs without any additional provisions for continued care. And the second-last time, when we looked up and said, “there is absolutely no one that can help us with her—no one that can come in and save her. We cannot save her. No one is there. Police aren’t going to help us.” Emergency doctors just released her to us with nothing. Nothing. Right? No plan. No additional trauma help or—you know. Now, you try to take your life. And this has been the case the whole time, right? You [try to] take your life and they just release you to nobody. Right? So, nobody is there to sort of catch you and help you work through this traumatic thing that you’ve just tried to take your own life. There is nobody there to support you.
Lastly, participants described an additional limitation of the healthcare system which, in their experience, does not offer meaningful opportunities for the involvement of families. I think, actually, in all mental health, I think families get shoved aside. Well, family members aren’t involved in very much for mental health now, so why should we decide—when it’s MAiD—that, all of a sudden, family members get the opportunity to be involved in mental health? That’s pretty much been stripped away from family members as it is.
Societal Barriers
In addition to the access barriers and limitations of the healthcare system, participants recognized the intertwined relationship between mental illness and negative social determinants, such as poverty, which further limits the psychosocial support options their loved ones could access. Our social safety net is so broken that I think a lot of people who are disabled with mental illness are living in a lot of despair and don’t have good supports. And I think they might not choose that option [MAiD] if they had a better support, better mental health support and better—you know, that they weren’t living in poverty and so on. So, there’s lots of sort of systemic issues that get in the way of why people aren’t getting what it is that they need.
A person with mental illness must also confront stigma. Participants acknowledged how stigma has been witnessed throughout the lives of their loved ones. Living with mental illness carries with it the burden of stigmatizing notions that often trivialize these health conditions and, unlike other health conditions typically considered “physical,” portray them as something that can be modified at will. And, like, mostly, people’s reactions are, “well, you should just—why don’t you just think positive thoughts? Why don’t you just—you know—shake that off?” I think that, unfortunately, conversations around [MAiD] for mental health maybe are colored by that implicit or explicit bias about people with mental health disorders specifically, as opposed to people with [a] physical disorder.
The Unknowns of Mental Illness
Family members had entertained questions and reflections about the nature of mental illness, the way in which it could impact a person’s capacity, and how treatable mental illness could be. We heard how mental illness could have a biological origin, particularly in the brain, and result in clinical manifestations that cannot be accurately operationalized or measured. And the problem is, because all the things we can suffer from, not only from the physical, but also from an organ that’s so important like the brain—it can give us things that cannot be measured, but people are feeling things, and having symptoms, real symptoms.
Other participants suggested that mental illness could impact the individual’s capacity to make decisions about healthcare, engage in healthy behaviors, or pursue treatment. These views on mental illness highlight the difficulty in establishing which domains of cognition and behavior are affected by the illness and how recovery could be facilitated or impeded. So, my first thing is, if you’re mentally ill, right, my question is “what kind of judgment do you really have?” Right? No, I think that it might be harder to treat the intractable symptoms with somebody with mental illness—just because their mental health issues make the treatment difficult. You know they are in denial that they have mental health issues. They don’t take their medications as prescribed—that type of thing.
The diversity of views on the nature and impacts of mental illness also resulted in divergent opinions about its potential treatability. I think it’s different because a lot of people think if you have a mental illness, it can be fixed. Or, like there should be a cure for it or you can fix it with therapy but, you know, I have two uncles who have schizophrenia, or who have like mental illnesses; I have been with them for almost half their lives, and you see no improvement, honestly. I believe this person [with mental illness] can still live a very happy and productive life if they are given the right treatment, and to evolve past the traumatic events of their life.
Individual Choices: The Life or Death that a Person Wants
Participants described the value they saw in ensuring that their loved ones have the opportunity to steer their own lives in a personally meaningful way. This requires taking into account the quality of life that a loved one could perceive, their ability to enjoy it in their life, and the stigma they might experience. The experience of suffering, the particular living circumstances, and the uniqueness of each recovery journey are all elements that the person with mental illness uses to inform their own assessment of their quality of life, in the participants’ views. Does the client themselves feel that the pain and the suffering that they are currently in is beyond their ability to handle and they would like to terminate? That should take precedence over how many years of therapy they’ve had, over what kind of support systems, whether they have family members that are against [MAiD], none of that should matter. It always should come down to “does this person want [MAiD]?” and “does the person requesting identify their own suffering and anguish as intolerable enough they don’t want to continue on?”, right? I don’t particularly see any benefit to that person continuing to live if they don’t want to, right? I think I’m still of the firm belief that we should give people the real choice to decide for themselves if [MAiD] is right given their circumstances. And people would know better than—like, individual people would know better than anybody else what their circumstances are and if they can honestly see the quality of their life improving or continuing to decline.
Family members were mindful of the diversity of views that emerge when discussing MAiD MI-SUMC. They acknowledged that reducing the level of debate to a confrontation between supporting and opposing voices is problematic. Participants highlighted that the experience of mental illness can only be fully appraised by the person living with it. I would personally hope that someone can get through [mental illness] and have hope—to push through. But, I can’t judge anyone for it. And, I know there are many strong feelings around it and I really think, I don’t believe [MAiD] is a totally yes/no answer, at least for me.
We heard how preserving life and relieving suffering caused by illness are both choices that a person with mental illness could decide to pursue. Some people fall on the side where suffering is just, you know, that kind of suffering no one can ask another human being to endure that—and it’s humane to allow people a more kind and compassionate way to end their suffering. But, then, there are other people who value life so greatly that they say it would be terrible for anyone to end their life when there’s a possibility things could turn around for them.
MAiD MI-SUMC as an Acceptable Choice when Suffering Cannot Be Relieved with Available Treatments and Supports
Across the dataset, there were instances in which participants suggested that MAiD MI-SUMC could be considered acceptable in cases of suffering that cannot be relieved after having tried available treatments, interventions, and supports. Participants discussed and reflected upon the individual caregiving experiences and views on mental illness that informed their particular stance. I don’t believe in suicide, so I don’t think that that is really the option. But I think that you want to assist yourself in dying. When you’ve tried all the other options, then I think that [MAiD] is a good option. If it’s an autonomous person who’s able to make their own decisions, and they’ve tried everything, and they don’t want to go on, I think that they should have the right to have [MAiD]—you know, it’s their life. It’s their path. And it’s their choice.
MAiD MI-SUMC was seen as an acceptable choice after having reflected on the journey of living with mental illness experienced by a loved one, including the treatments and supports tried along the way. Family members underscored that it is important that their loved ones assess the quality and the circumstances in which their lives take place, and make informed choices about the path they wish to follow. Understanding MAiD MI-SUMC as acceptable in certain instances required acknowledging a spectrum of varying circumstances surrounding the person with mental illness and any potential individual decision. It also required recognizing that the suffering experienced by a loved one with mental illness cannot be fully appreciated by external observers. Throughout these themes, MAiD MI-SUMC was described by participants as an issue in which complex individual and contextual factors converge over time, on a case-by-case basis, and in a way that cannot be generalized.
The Emotional Outcome
Participants were asked to imagine the journey of a person with mental illness pursuing MAiD MI-SUMC. This included a search for information, the formalization of a request, an assessment, and the moment in which an outcome is communicated to the applicant. Family members acknowledged that, although a MAiD MI-SUMC request could result in either an approval or rejection of the request, the emotional outcome experienced by the person living with mental illness could manifest itself in multiple and nuanced ways.
Across the dataset, it was generally viewed that an individual with mental illness whose MAiD MI-SUMC request is rejected would experience negative emotions. These emotions could be internalized or externalized, resulting in additional suffering. I think [the imaginary person] will feel disappointed. I think he will feel that he’s not even good enough to die, to get help to do that. I’m sure there’ll be anger and frustration, and depression, and sadness, and despondency and, you know, desperation.
A contrasting view described situations in which a rejected MAiD MI-SUMC request could elicit relief in the requester, who might also second-guess their initial decision to pursue MAiD MI-SUMC, and perceive the situation as an opportunity to embark on a new recovery journey. [The imaginary person] might feel relief, very much so, like, “Oh my God, I’m glad I didn’t do that. What was I ...,” like she did after her first jump. “What was I thinking, how could I—I’m going to get the help I need,” like she could feel that relief. “Somebody said no, so now I’m going to get help, I’m going to work hard to get well and reach out,” and so on.
An approved request was generally visualized as eliciting relief, nested in the individual’s realization that the suffering that has been present throughout their life will finally come to an end. I think that [the imaginary person would] probably [feel] some relief. Like he doesn’t have to deal with whatever has been bothering him for most of his life anymore. I would think that if [the imaginary person] got herself involved in all of this in the first place, and had all the facts, because this is a very serious decision, I would imagine that she’d probably feel relieved.
Participants also described that, even if a MAiD MI-SUMC request was granted, the person living with mental illness could experience a mixture of anxiety and relief. This highlights the multiplicity of emotions that could arise throughout the experience of a MAiD MI-SUMC process. I think [the imaginary person] would be relieved and maybe a little bit scared. There might be some fear there.
Discussion
In this study, we explored the perspectives of individuals who have a loved one living with mental illness, on the introduction and use of MAiD MI-SUMC. They identified issues related to barriers and limitations of the mental healthcare system; their desire for formal involvement opportunities in their loved ones’ healthcare; the role of the social determinants of health in eliciting or maintaining health disparities directly impacting their loved ones; and the autonomy of the patient to assess their own suffering and individual circumstances in order to inform their individual choices regarding healthcare. We discuss how these issues could have implications for research, policy, and health services in connection with MAiD MI-SUMC. An in-depth exploration of the perspectives on MAiD MI-SUMC held by persons living with mental illness is available elsewhere (Bastidas-Bilbao et al., 2023).
Firstly, participants consistently identified challenges they have witnessed when their loved ones tried to access mental health support and emphasized a demand for services that exceeds capacity. When services are finally accessed, these might not properly target the patient’s needs—for example, addiction and rehabilitation services—or might only be provided as short-term emergency services without further continuity. The literature recognizes that only a fraction of Canadians perceive that the help received has fully met their mental health needs; difficulties in navigating the system, shortage of professionals, lack of integration between community and specialized services, and financial burden are some of the most frequently acknowledged barriers to timely and appropriate care (Moroz et al., 2020). The experiences described by participants are consistent with some of the limitations of the current mental healthcare system evidenced in research. The role of substance use disorders merits particular attention in the discussion of MAiD MI-SUMC, given their overall prevalence and high rates of comorbidity with mental illness, alongside the stigma, social determinants, siloed treatments, and clinical impacts for individuals and families (Lai et al., 2015; Yang et al., 2017).
Participants also expressed a desire for opportunities to be involved in the mental healthcare provided to their loved ones. In that regard, the literature has reported that, for family caregivers, certain care settings (i.e., hospitals) are identified as contexts in which collaborative and trusting relationships with healthcare professionals are difficult to establish (Dirik et al., 2017; Doody et al., 2017). The challenges for the involvement of family caregivers in care planning and decision-making have been discussed in empirical studies and literature reviews, with family caregivers’ voices being frequently critical of the lack of opportunities for active and meaningful involvement (Stuart et al., 2020; Vestphal et al., 2023; Wilkinson & McAndrew, 2008). Gaps have also been identified between caregivers’ and clinicians’ views on the involvement of family (Sharon et al., 2020). Moreover, although patients are legally entitled to autonomously determine the degree of family involvement they wish to have, family caregivers perceive confidentiality as a barrier that can result in less or no access to information, less involvement, and even exclusion (Doody et al., 2017). The experiences of participants in our study suggest a need for developing practices, as part of any potential implementation of MAiD MI-SUMC, aimed at responding to expectations regarding patient-led decision-making and the involvement of families during assessments, including setting limits and achieving a shared understanding of the implications of confidentiality among families, patients, and providers.
The influence of contextual factors in the suffering experienced by their loved ones with mental illness was consistently acknowledged by participants. These included negative social determinants of health—such as disparities in resources, lack of a social safety net, or other unfavorable contextual characteristics—and stigma, all of which exerted a detrimental impact on their loved ones’ well-being and resulted in further disparities in health outcomes (Jenkins et al., 2021). Along with recognizing social factors that could elicit or exacerbate their loved ones’ suffering, participants also discussed the role of the persons with mental illness as the ones with privileged knowledge to appraise the quality of their own lives and make healthcare decisions best suited for their particular circumstances, including MAiD MI-SUMC. These elements illustrate that MAiD MI-SUMC decision-making can be complex and strongly related to autonomy. The role of patient autonomy in regard to MAiD MI-SUMC has also been reported by persons with mental illness seeking MAiD MI-SUMC in international jurisdictions where the procedure is legally available (Pronk et al., 2022).
The individual experience of suffering and the role of social factors, as it was discussed by our participants, are themes that converge with some conceptualizations found on the literature on suffering. The literature describes suffering as entailing an interaction between social and individual elements that shape subjective cognitions and meanings that cannot necessarily be appraised by external witnesses (Carnevale, 2009). Additionally, suffering can occur due to illness, to the way in which illness is experienced, or, even, in absence of illness (Cassell, 1982; Frank, 2001). The idea that unfavorable social determinants of health could create circumstances that would compel people to pursue MAiD MI-SUMC has been debated from multiple perspectives (Bahji & Delva, 2022; Simpson, 2018). However, the influence of social determinants is not exclusive to mental illness. Furthermore, the identification of specific social determinants that would consistently result in an improved mental health remains elusive and challenging (Alegría et al., 2018).
Participants also discussed the role of autonomy, which also converges with a conceptualization of treatment futility—known as qualitative futility—that aims to determine the quality of the medical treatment outcomes based on the treatment and life goals autonomously set by the individual (Levitt & Buchman, 2021; Xu & Sisti, 2021). The implications of patient autonomy also underscore the challenges of shared decision-making—a process whereby the patient provides expertise about their own views, resources, goals, and preferences, while the healthcare provider contributes with their expertise in medical conditions, treatments, and potential outcomes (Drake et al., 2009)—in a context of uncertainty, such as that posed by mental illness in light of its nature, implications, and potential trajectories. However, shared decision-making could play a meaningful role in MAiD MI-SUMC in order to ensure that decisions are aligned with the patient’s best interest, the most pertinent information, and a collaborative exploration of the patient’s values (Parascandola et al., 2002).
Across the dataset, the acceptability of MAiD MI-SUMC seemed intricately related to individual suffering and available treatments and supports that did not result in relief. However, additional factors could be identified within this relationship, as reported by the participants. Firstly, the availability of treatments and supports would depend on the capacity and functioning of the healthcare system. Secondly, the social determinants of health would permeate the patient’s suffering, introduce facilitators or barriers to healthcare, and influence the overall illness trajectory. These factors could lead to a wide variety of individual circumstances that each patient would take into account, along with some corresponding uncertainties, to inform their own decisions, including potentially pursuing MAiD MI-SUMC.
In addition to the knowledge shared by family participants, our lived experience panel also contributed to this study as advisors and decision-makers (Canadian Institutes of Health Research – CIHR, 2014). Open communication with the study leads facilitated the exchange of ideas and informed the nature and scope of the study itself. Newsletters and frequent meetings were useful in keeping our panel updated on study progress and being able to debrief with them about research progress. The researchers encountered minor challenges related to language usage, which led us to adjust some written materials and identify creative ways of communicating important concepts. Debrief sessions were essential to handle occasional instances of disagreement, especially when they evidenced tensions between scientific and lived experience perspectives. Preserving rapport with our lived experience panel was paramount. Financial considerations resulted in some limits to the frequency and intensity of lived experience advisory engagement. The emotional impact of having conversations about the difficulties and despair experienced by families and their loved ones was a significant challenge.
This study contributes to the literature by highlighting the value of the lived experience of our participants as a form of knowledge and by showcasing the importance of using responsive and reflexive methodological approaches grounded on a compatible ontology and epistemology. This study also exemplifies steps and methods that facilitate the inclusion of family members in discussions about MAiD MI-SUMC, which is paramount in future debates on this very topic. However, this study has some limitations related to demographic and ethnic diversity, with women accounting for the vast proportion of participants; this is nonetheless consistent with the literature on caregiving for persons living with mental illness, where women frequently constitute a sizable majority and also experience higher levels of burden (Treichel et al., 2020). Given these disparities, future research should hear the voices of Indigenous and racialized women—intersected with a wider range of social determinants of health—along with other communities, such as LGBT2SQ+ persons, caregiving men, and families of persons with addictions. We did not include a discussion of MAiD in cases of dementia, which has many important implications as a neurodegenerative condition, distinct from the conditions typically known as mental illness, and therefore outside of the scope of the current project.
Other limitations are related to the fact that some persons living with mental illness might not have support from their families, or a family network at all. Less family support and increased family conflict are reported as predictors of symptom severity, substance use, and increased use of emergency services (Haverfield et al., 2019; Young et al., 2005). By virtue of wanting to participate in this study, our family participants might differ from others who, for varying reasons, might not be able to engage with their loved ones’ care and experience of mental illness. Future studies should address this engagement gap. It should also be noted that substance use disorders were limited in our sample; the implications of MAiD in the case of severe substance use disorders merit further research. Given the scarcity of studies on MAiD MI-SUMC involving family members, this research represents an initial step to ensure that families are not excluded from this social debate. We underscore the value of constructing scientific knowledge about MAiD MI-SUMC with epistemic justice (Bradley & Wasserman, 2023) and in recognition of the epistemic authority (Zhang et al., 2023) of those with lived experience of the different facets and roles that are permeated and transformed by mental illness.
In sum, in this study we identified how family members viewed MAiD MI-SUMC in ways that were informed by their own experiences and challenges throughout their journey supporting and, sometimes, providing care to their loved ones. Participants recognized that those living with mental illness are in a crucial position to appraise their own suffering and quality of life in order to inform and make healthcare decisions autonomously. Contextual factors were also identified as having a role on the facilitation—or prevention—of family involvement, access to care, and the exacerbation of suffering. A systematic and sustained exploration of these individuals and social factors is necessary to achieve a broader understanding of how mental illness impacts individuals and their families alike, and shape possible healthcare decisions to follow, including MAiD MI-SUMC.
Footnotes
Declaration of Conflicts Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hamer Bastidas-Bilbao, Vicky Stergiopoulos, Vivien Cappe, Mary Rose van Kesteren, Alexander I. F. Simpson, Michael Dawthorne, and Lisa D. Hawke declare that there is no conflict of interest. Donna Eileen Stewart declares that she has served in the Expert Panel on MAiD and Mental Illness, the Canadian Psychiatric Association Working Group on MAiD, and as a reviewer of the Canadian Association of MAiD Assessors and Providers (CAMAP) curriculum on MAiD. Mona Gupta declares that she has received funding related to this subject from CIHR; she was Chair of Health Canada’s Task Group on MAiD Practice Standards, the Chair of the Federal Expert Panel on MAiD and Mental Illness, and the Chair of the AMPQ ad hoc committee on MAiD. Tarek K. Rajji has received research support from Brain Canada, Brain and Behavior Research Foundation, BrightFocus Foundation, Canada Foundation for Innovation, Canada Research Chair, Canadian Institutes of Health Research, Centre for Aging and Brain Health Innovation, National Institutes of Health, Ontario Ministry of Health and Long-Term Care, Ontario Ministry of Research and Innovation, and the Weston Brain Institute; he has also received for an investigator-initiated study in-kind equipment support from Newronika, and in-kind research online accounts from Scientific Brain Training Pro, and participated in 2021 and 2022 in an advisory activity for Biogen Canada Inc; he is also an inventor on the United States Provisional Patent No. 17/396,030 that describes cell-based assays and kits for assessing serum cholinergic receptor activity; he served on the MAiD Practice Standards Task Group as CAMH representative. David Castle has received grant monies for research from NHMRC (Australia), Barbara Dicker Research Fund, Milken Institute, Canadian Institutes of Health Research, and Psyche Foundation; consulting fees from Seqirus; honoraria for talks from Seqirus, Servier, and Mindcafe Forum; and honoraria as advisory board member from Seqirus and Lundbeck; he is a founder of the Optimal Health Program (OHP) and holds 50% of the IP for OHP; is part owner and board member of Clarity Healthcare; and is unpaid board chair of the Psyche Institute; he does not knowingly have stocks or shares in any pharmaceutical company.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by a grant (332964) awarded to Dr. V. Stergiopoulos by the Canadian Institutes of Health Research and a grant awarded to Dr. L. D. Hawke by the University of Toronto’s Department of Psychiatry Suicide Studies Fund.
Ethical Statement
This study was approved by the Centre for Addiction and Mental Health (CAMH) Research Ethics Board (158-2021). All participants provided written informed consent prior to enrollment in the study.