
Abstract
Contemporary practices of long-term antipsychotic maintenance treatment for schizophrenia are being challenged, and clinicians must consider the possibilities of reducing long-term maintenance use. However, research indicates that people with schizophrenia receive little support from mental health staff to reduce antipsychotic medication. This article reports a study which aimed to investigate interdisciplinary mental health staff’s accounts of tapering of antipsychotic medication and to explore different positions that mental health staff assign to themselves and others. Six focus groups were conducted with 39 mental health staff from outpatient clinics, inpatient units, forensic mental health units, and community mental health services. The data analysis combined analyses of the interactions during focus groups and the thematic content. Results were considered from a discourse analytic perspective considering the function and consequence of accounts applied by the mental health staff. The mental health staff accounted for their perspectives on tapering from the following three distinctive positions: 1) No, patients will eventually realize that they need the medication, 2) Yes, but tapering means running a big risk of relapse in symptoms, and 3) Yes, we need to welcome risks to support personal recovery. Our findings indicated that there was reluctance among interdisciplinary mental health staff to let service users make decisions and limited possibilities for people with schizophrenia to have their request for tapering of their antipsychotic medication met by mental health staff.
Introduction
Long-term treatment with antipsychotic medication for people with schizophrenia is common practice in mental healthcare (Harrow et al., 2012; Murray et al., 2016). While antipsychotic medication is effective in overall symptom reduction in schizophrenia (Jibson, 2022; National Institute for Health and Care Excellence (NICE), 2014), the efficacy of long-term maintenance treatment beyond 2 years is less certain (Harrow et al., 2012; Murray et al., 2016). Leading experts have raised a debate as to whether the benefits of long-term antipsychotic maintenance treatment are in fact balanced out against treatment-related adverse effects (Morrison et al., 2012; Murray et al., 2016; NICE, 2014) including cardiac arrhythmias (Frommeyer & Eckardt, 2016), obesity, insulin resistance, type 2 diabetes, metabolic syndrome (De Hert et al., 2012; Henderson et al., 2015), sedation, movement disorders (Leucht et al., 2012), and dopamine dysfunction (Howes et al., 2012). Thus, clinicians are advised to consider the possibility of reducing long-term maintenance use of antipsychotic drugs for people in remission of psychotic symptoms (Leucht et al., 2012; Morrison et al., 2012; Murray et al., 2016). International clinical guidelines for the treatment and management of schizophrenia recommend a 5-year stabilization period after 1–2 psychotic relapses and continuous treatment for people with three or more psychotic relapses (NICE 2014; Sundhedsstyrelsen, 2014). However, these guidelines do not provide procedures on how to reduce or discontinue antipsychotic medication past stabilization phases (Horowitz et al., 2021). A recently published method for tapering of antipsychotic medication (Horowitz et al., 2021) recommends a gradual tapering process concurrent with continuous screening of symptoms that may minimize the risk of relapse and antipsychotic withdrawal syndrome.
People with schizophrenia often have a desire to reduce or discontinue antipsychotic treatment (Bülow et al., 2016; Geyt et al., 2017; Morant et al., 2018). However, studies indicate that people with schizophrenia receive little support from mental health professionals to reduce or discontinue antipsychotic medication and often see no other way than to self-initiate and conceal adjustments or discontinuation (Bülow et al., 2016; Geyt et al., 2017; Morant et al., 2018) at the risk of recurrence of psychotic symptoms and antipsychotic withdrawal syndrome (Horowitz et al., 2021). Contemporary mental health services are being increasingly criticized from within for being dominated by the medical model (Bracken & Thomas, 2001; Moncrieff, 2009), implying that biomedical knowledge presides over social, cultural, and political factors in the understanding of mental issues (Bracken & Thomas, 2001). Also, default drug treatment dominates services, and drugs are initiated and maintained due to alleged risk (Moncrieff, 2009). Risk adverseness seems especially pronounced in relation to treatment of people with schizophrenia whose antipsychotic drugs are rarely deprescribed without prescribing a new antipsychotic drug (Moncrieff, 2009). Research shows that healthcare professionals attribute what they perceive as “non-compliance” in taking medications as prescribed as a consequence of “lack of illness insight” in people with schizophrenia (Martínez-Hernáez et al., 2020; Seale et al., 2006). “Lack of illness insight” is thereby equated with irrationality and inability to make rational decisions regarding one’s own treatment (Roe et al., 2009), implying that people with schizophrenia are unable to participate in decisions regarding their treatment. Additionally, concepts such as “risk avoidance,” “dignity of risk,” and “duty of care” may also play a role in health professionals’ perspectives on tapering. Cooper et al. (2019) found that British community-based mental health professionals are reluctant to support reductions or discontinuation of antipsychotic medication due to a perceived risk of relapse. In 1972, “dignity of risk” was first described in relation to the indignity of overprotecting people with intellectual disabilities (Perske, 1972). Later, the notion has been used in relation to risk avoidance by mental health professionals who are encouraged to support personal choice and growth for people with mental illness by offering them the dignity to take risks (Burns-Lynch et al., 2010; Marsh & Kelly, 2018). However, a review on dignity of risk shows that health professionals struggle to balance dignity of risk with their duty of care requirement to protect service users from harm and failure (Marsh & Kelly, 2018).
People with schizophrenia may be in contact with a variety of different healthcare services and mental health staff who work within and across multidisciplinary teams to provide treatment. However, there is a paucity of research on interdisciplinary mental health staff’s perspectives on tapering of antipsychotic medication for people with schizophrenia, which may constitute barriers to effective and safe tapering. In this article, we approach this by exploring mental health staff’s language use when they share their perspectives on tapering.
Theoretical Perspective
We took a social constructionist approach to discourse analyses, which asserts that discourse is constructed, constructive, situated, and action-oriented (Wiggins & Potter, 2017; 96), arguing that social reality is mediated by language and that language is constitutive of the social as it makes certain enunciative positions available for speakers (M. Jørgensen & Phillips, 2002; Potter & Wetherell, 1987). This action-oriented nature of discourse directs focus toward how speakers can position themselves by accomplishing different discursive acts (Edwards & Potter, 2001). Accounts are a distinct form of discursive acts that follow standard forms (Potter & Wetherell, 1987). Accounts are produced in situations in which people act or risk being accused of acting in unexpected or inappropriate manners requiring them to account for their actions (Potter & Wetherell, 1987). In these situations, people may draw on a typology of accounts such as excuses and justifications employed to explain actions, or requests and disclaimers that function as pre-accounts for actions in situations where people expect that their actions might reflect negatively on themselves (Potter & Wetherell, 1987).
In applying discourse analytic theory, it is possible to show how speakers position themselves and others through situated language use (Harré & Lagenhove, 1999). Positions are a set of rights and duties designated to people to act in specific ways in specific social interactions (Harré & Lagenhove, 1999) (e.g., a medical doctor will have the duty to help the ill and the right to define illnesses, while a patient will have the right to seek medical treatment and the duty to respect the medical institution). Speakers’ actions are both enabled and limited by the perceived positions of other speakers in concrete conversational contexts (Harre & Slocum, 2003). That is, some people are more advantageously positioned than others in specific social interactions, and while some positions are negotiable, others are not (Harre & Slocum, 2003). The aim of the analysis reported in this article was to investigate mental health staff’s accounts of tapering of antipsychotic medication and to explore different positions that mental health staff assign to themselves and others, as they discuss tapering in focus group discussions.
Methods
Participants
Six audio-recorded focus groups were conducted between May and June 2022. We aimed to include a purposive sample of diverse and “information-rich” (Patton, 2015) mental health staff employed in adult hospitals and community mental healthcare services with a minimum of 1 year employment and experience in working with people with schizophrenia. Participants were recruited in mental healthcare services of two Danish regions. Key individuals (i.e., development managers or head nurses) at each recruitment site informed unit managers about the study and asked them to recruit among their employees according to the sampling criteria. We recruited 39 mental health staff. Participants included two psychiatrists, two medical doctors specializing in psychiatry, one medical student, 13 registered nurses (one held an MSc in nursing and five held a graduate certificate in mental health nursing), 15 nurse assistants, two psychologists, one occupational therapist, one pedagogue, one physiotherapist, and one social worker. A total of 13 participants worked in inpatient services, 10 worked in outpatient services, while 16 worked in community services. Participants had worked in mental health services for .5–40 years (average: 13.2 years). Participants were between 25 and 65 years of age (average: 45 years of age), and 29 were female while 10 were male. Three focus groups were conducted in each of the two regions including one focus group with staff from inpatient settings (Region A), one focus group with staff from forensic settings (Region B), two focus groups with staff predominantly from outpatient settings (one in each region), and two focus groups with staff from community mental health services (one in each region).
Data Generation
Claims discussed in focus groups.
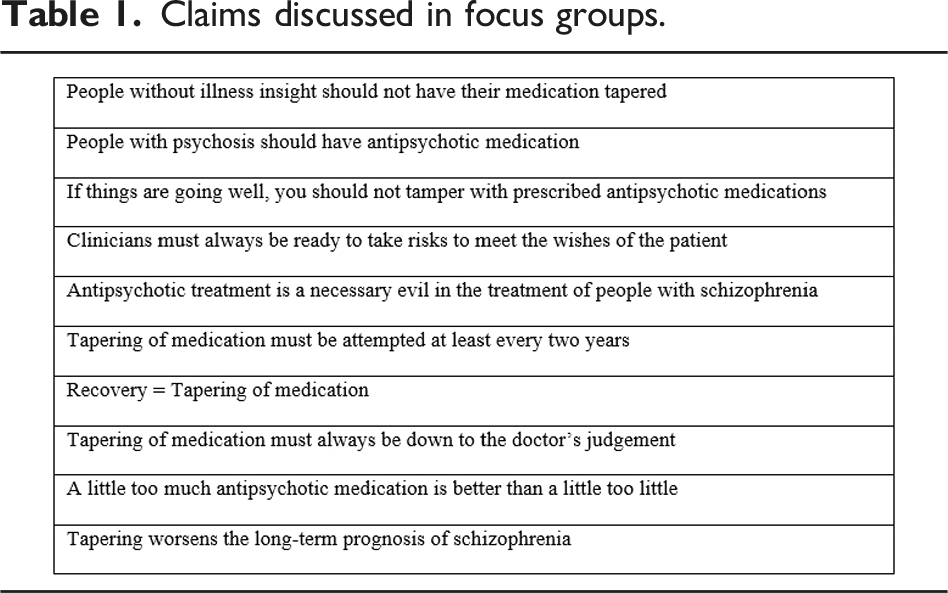
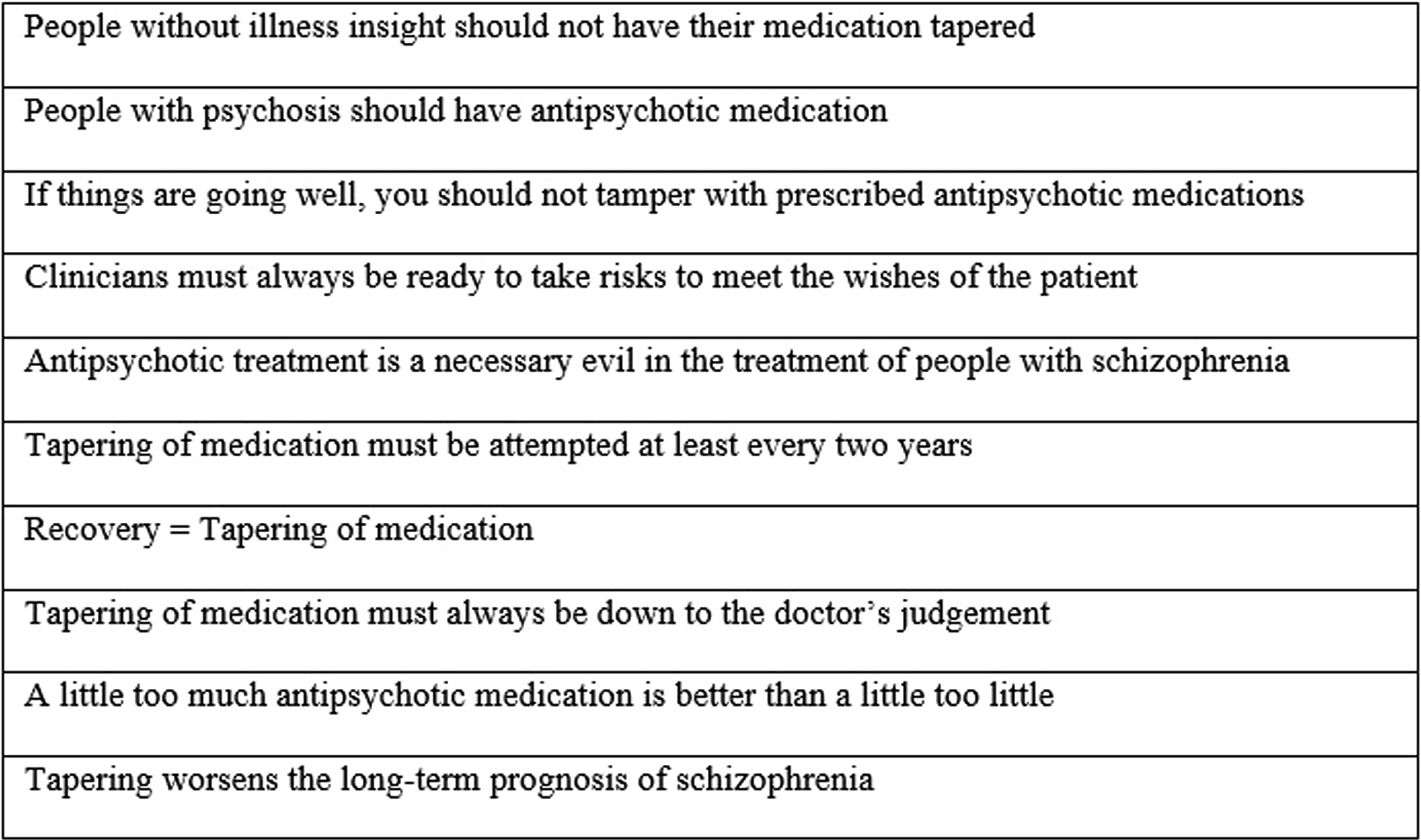
The focus groups were moderated by KR with PSC as an observer. The moderator introduced the topic and the focus groups as an open exchange of opinions and experiences with no right or wrong answers or need to reach agreement. The moderator read the claims aloud, handed them to the participants, and asked them to self-facilitate the discussion of the claims throughout the next hour. Both the moderator and observer wrote field notes about how the participants interacted. Focus groups lasted between 45 and 77 minutes with a total of 6 hours and 44 minutes. Recordings were transcribed verbatim by a secretary. The transcription followed Bloor et al.’s guidelines (Bloor, 2001) including verbatim transcription of all talk. Non-linguistic sounds such as emotional aspects of conversation were marked with asterisks. KR checked transcriptions for accuracy against the audio-recordings and linked the transcripts to the field notes by adding a symbol indicating conversational interactions.
Ethics
The study was conducted in accordance with the Declaration of Helsinki. In accordance with Danish legislation, formal ethics committee approval was not required due to the qualitative nature of the study. The study and data management plan were approved by the Capital Region’s data protection agency, Pactius (P-2022-169). All participants were provided information about the aims and methods of the study, their rights for anonymity, and that they could withdraw from the focus group at any time without any consequences. All participants provided written consent to participate.
Data Analysis
The data analysis combined an analysis of interactions between participants during focus groups with an analysis of the thematic content (Halkier, 2010; Morgan, 1997). As described above, the thematic content was considered from a discursive perspective with regard to the functions and consequences of accounting (Potter & Wetherell, 1987) and positioning (Harré & Lagenhove, 1999). Memo-writing was conducted throughout the research process to investigate, compare, and analyze the full data material, to develop ideas, and to systematically reflect on assumptions and actions taken during the analysis (Järvinen & Mik-Meyer, 2020). The analysis started with a review of the audio-recordings and repeated readings of the transcripts and field notes to obtain an overall understanding of the data set (Coffey & Atkinson, 1996). This was followed by a process of inductive coding of the thematic content of the full data set (Coffey & Atkinson, 1996), in which initial codes, themes, and memos were discussed among KR, NB, and JM. In this provisional analysis, three positions were identified that reflected three distinctive functions and consequences of typical accounts created as the participants discussed tapering. These positions were further developed and elaborated on through memo-writing to gain insight into how the participants discussed and negotiated different aspects of the thematic content. This led to a process of re-coding the full data set in accordance with the three tentative positions including openness toward identifying additional positions. Sequences of interaction were selected for further investigation and detailed transcription (Potter & Wetherell, 1987), and this process included an investigation of what was rhetorically achieved in the interactions. This step resulted in the formulation of the three final distinctive positions of typical accounts applied by the mental health staff. KR wrote up the results providing extracts of conversations from the focus groups. This included a final process of listening to the audio-recordings and rereading of the original transcripts and field notes to corroborate the findings.
Analysis
In the sections below, we present the general interaction patterns identified in the focus groups followed by a presentation of the identified three positions.
Interactions
While some focus group participants were day-to-day colleagues, most participants came from different units within the same hospital or different community centers within the same municipality. All focus groups easily adapted to collaboratively facilitating the discussions and decided among themselves how they wanted to discuss the claims. Therefore, the moderator used no probes during the discussions. Interactions were to a large extent informal with lengthy turn-takes with occasional interruptions and questions directed at one another or the wider group. The participants continually challenged apparent consensus, each other’s arguments, and stated when they disagreed with other participants. Challenging statements and disagreements were accepted and would often lead to modifications, negotiations, or further elaborations of the claim discussed.
The mental health staff accounted for their perspectives on tapering of antipsychotic medication for people with schizophrenia spectrum disorders from the following three distinctive positions: 1) No, patients will eventually realize that they need the medication; 2) Yes, but tapering means running a big risk of relapse in symptoms; and 3) Yes, we need to welcome risks to support personal recovery. During focus group discussions, individual staff members tried to account from different positions, but the general pattern was that each staff member spoke from one position. Thus, they mainly challenged themselves and each other to strengthen and defend their position. Further, the three identified positions were employed within and across mental healthcare settings, professional backgrounds, length of employment in mental healthcare services, age, and gender, which indicated that tapering of antipsychotic medication was discussed in a multifaceted fashion within and across focus groups.
Positions
No, Patients Will Eventually Realize That They Need the Medication
When accounting for tapering in terms of “No, patients will eventually realize that they needed the medication,” antipsychotics were generally described as effective in reducing symptomatology and to have revolutionized the treatment of psychotic illnesses. In this vein, antipsychotics were equated to medication for physical diseases such as insulin used in the treatment of diabetes to describe the importance of antipsychotics in minimizing the risk of relapse. Schizophrenia was depicted as a chronic illness, and stable phases were not described as a predictor for tapering, rather as a sign that medications are effective and should be maintained. Comments or concerns raised about adverse effects were closed down, and antipsychotics were described as not always causing adverse effects.
Concepts such as “compliance” and “illness insight” were continually discussed and described as a prerequisite if tapering was to be justified. Non-compliance with medications was stated to be caused by patients’ lack of illness insight, as not perceiving oneself as ill, and thus in no need of antipsychotics. Accordingly, mental health staff were portrayed as having a societal responsibility to safeguard society against people who are psychotic. However, non-compliance was also presented as a situation in which tapering could be justified to ensure compliance and alliances with patients. Referred to as “a negotiation technique,” tapering was presented as offering small dose reductions or switching to other antipsychotic drugs. Such reductions were to be withdrawn as soon as patients were willing to agree to the dose initially prescribed.
Accounting in this way included undermining patients’ preferences regarding their medical treatment. Participants portrayed themselves as being pressured by patients and patients’ relatives to taper medications but justified that “medications are needed as prescribed” by referring to clinical experiences of patients and their relatives sooner or later realizing that the prescribed antipsychotics were needed. Further, it was described that patients in recent years wanted more information, stated clearer opinions, and demanded clearer answers regarding their medical treatment. This was initially narrated as positive, but patients were described as using “Dr. Google” to malinger treatment-related adverse effects to put pressure on psychiatrists to change or cease medications. Additionally, it was contested whether patients truthfully wanted tapering when they requested it, as it was stated that patients would want full discontinuation of their medications, which was used as an argument to legitimize refraining from talking with patients about tapering.
In the extract in Figure 1, these aspects regarding truthfulness were discussed in relation to the claim “Clinicians must always be ready to take risks to meet the wishes of the patient.” James, Patricia, and Linda were from inpatient mental healthcare services in Region A. Leading up to the extract, James cautioned against blindly following patients’ wishes. Extract 1.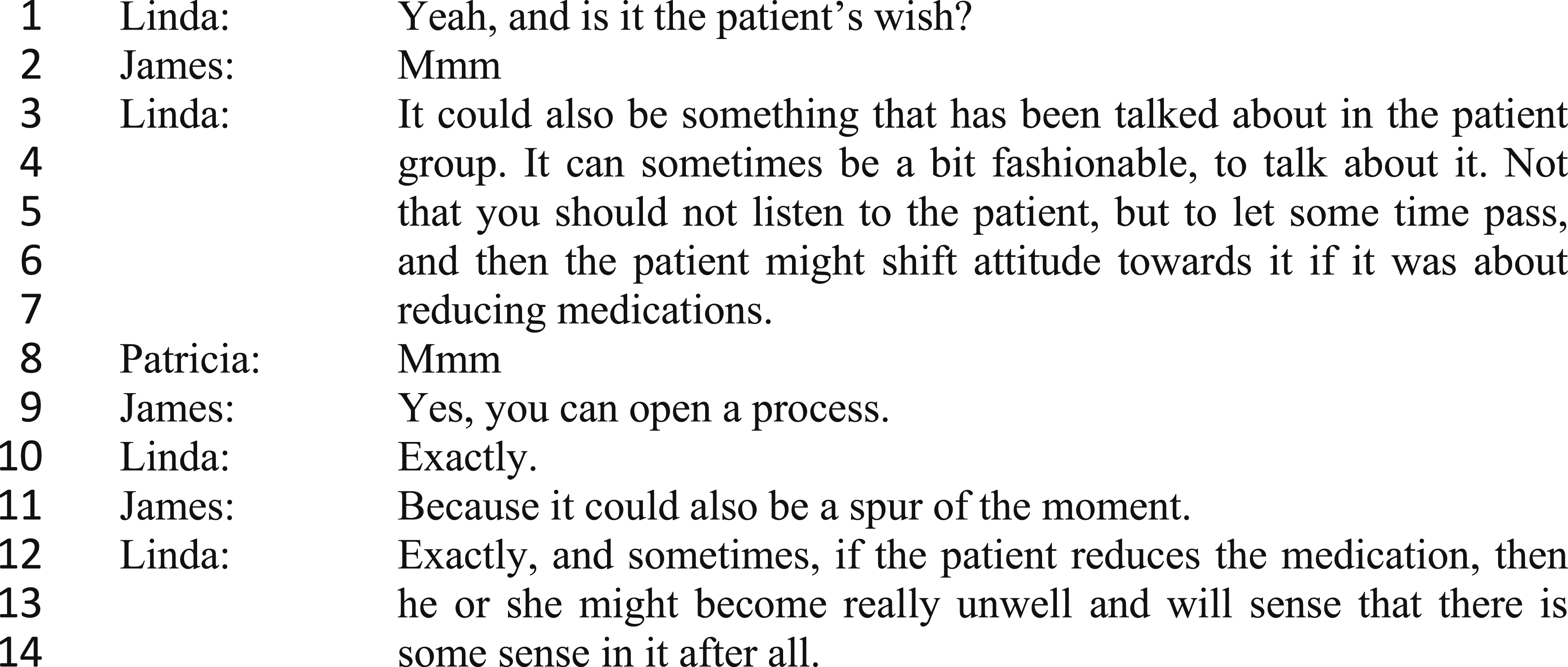
In the beginning of the extract, Linda questions the authenticity of an individual patient’s wishes, suggesting that patients might be influenced by a general attitude among patients in which tapering has become trendy. This argument leads Linda to legitimize that staff may circumvent patients’ requests for tapering, seen in lines 4–7, where she employs a disclaimer: first stating that staff should listen to patients but then, that if staff let time pass, patients might change their opinion. By accounting in this fashion, Linda avoids explicitly stating that staff should not listen to patients to avert possible negative interpretations of her argument. Accounting in the same fashion, James argues that it is best not to engage with patients in conversations on tapering, stipulating that tapering might be based on sudden impulses (lines 9 and 11). At the end of the extract, Linda further justifies abstaining from tapering grounded in an anticipation that patients might relapse and will realize that the staff acted with good reason.
The extract indicates that there is no problem associated with patients sharing their treatment-related preferences, but that conversations about tapering should be avoided and patients’ perspectives rejected. Mental health staff position themselves as having the duty and right to authorize patients’ wishes and thus define what counts as valuable factors to be included in treatment-related decision-making by putting patients in their care in passive positions where they passively receive the healthcare services offered.
Yes, but Tapering Means Running a Big Risk of Relapse in Symptoms
In accounting for tapering in terms of “Yes, but tapering means running a big risk of relapse in symptoms,” antipsychotic treatment was generally positioned as a crucial part of keeping illnesses under control and to achieve recovery, explained as living a meaningful life despite mental illness. However, antipsychotics were also depicted as a cheaper treatment than non-pharmacological approaches and as a means to secure rapid discharge of patients. Further, treatment with antipsychotics was portrayed as a practice in which overmedication and polypharmacy were not adequately managed. Tapering was regarded good clinical practice during stable phases of illnesses to hinder overmedication and treatment-related adverse effects: not primarily legitimized out of consideration of patients’ preferences. Yet, various reservations were described that could lead to patients being discouraged from tapering.
A typical reservation toward tapering was linked to conflicting research evidence regarding risk of relapse and excess mortality due to metabolic side-effects. Ascribing only few metabolic side-effects to antipsychotics was used as a rhetorical strategy to legitimize that staff did not consider tapering. A second typical reservation toward tapering was an anticipated risk of drug abuse. This was contested by psychiatrists arguing that drug abuse is best targeted using the lowest effective dose of antipsychotics as high doses may lead to abuse of stimulants. A third typical reservation toward tapering concerned the duration of stable phases. Refraining from tapering until patients have been stable for long (yet unspecified) periods of time was described as favorable to minimize the risk of relapse. So, having certain predetermined intervals for tapering was warned against. A fourth typical reservation regarded the individual’s medical history. Despite stable phases, tapering was presented as indefensible for patients with multiple psychotic episodes, involuntary admissions, or long illness durations. Accounting in this way included appealing to a duty of care, that is, requirement to apply clinical knowledge and to inform patients about risks of tapering including relapse, readmissions, as well as losing employment and relationships. However, younger patients with single or few psychotic episodes were portrayed as more likely to be assessed suitable for tapering.
These reservations were discussed in one focus group in relation to the claim “Tapering of medication must be attempted at least every two years.” Rebecca and Ryan were from in- and outpatient mental healthcare services in Region B. Leading up to the extract presented in Figure 2, Rebecca argued that tapering should be evaluated according to the individual patient’s medical history. Extract 2.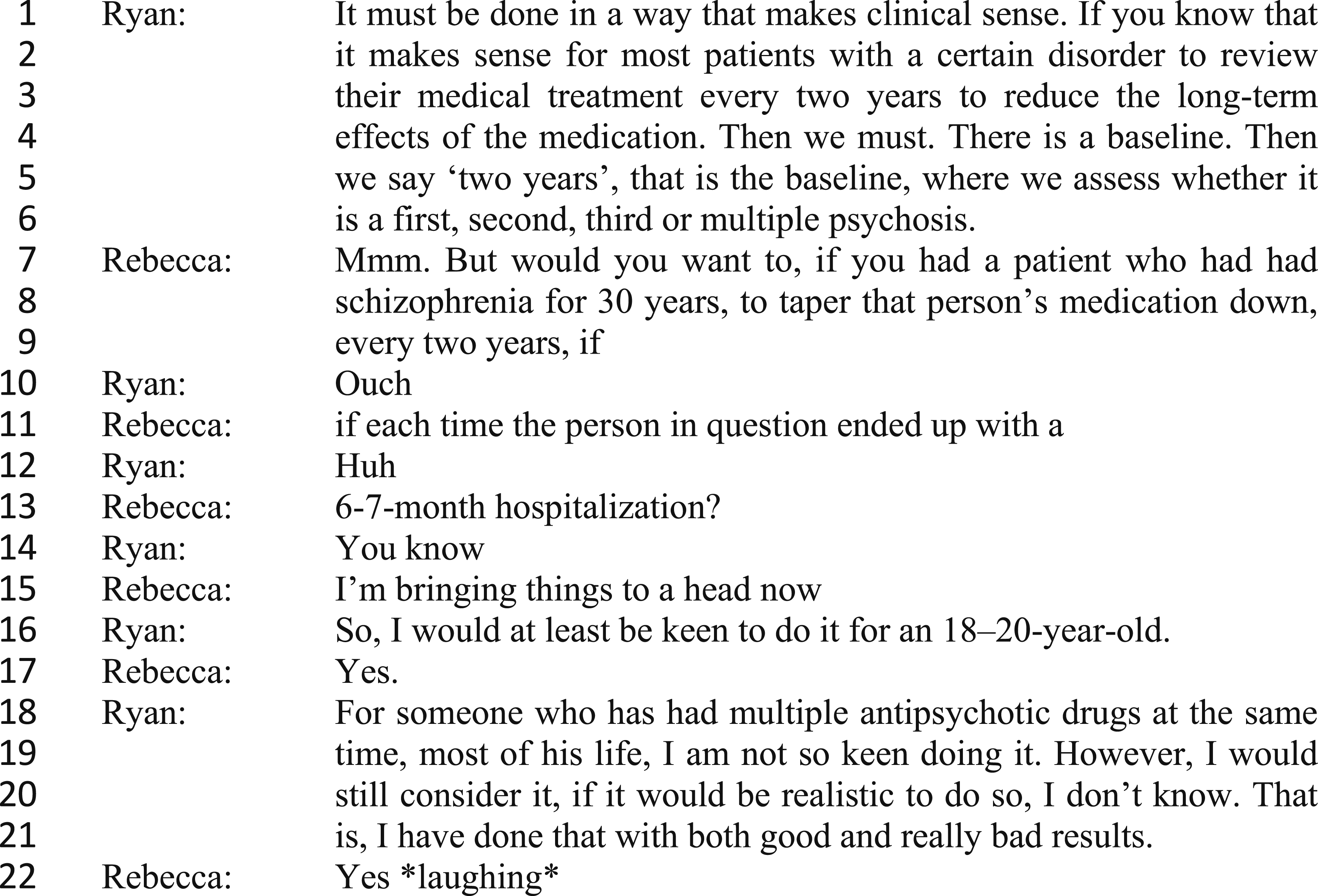
In the extract, Ryan sets out to argue that he will taper medications if evidence justifies it. Rebecca is employing—what she acknowledges to be—an extreme example (lines 7–9, 11, and 13) to problematize Ryan’s position. Ryan responds by moderating his initial statement (line 16), to which Rebecca says “yes,” supporting this response. However, Ryan resumes his initial argument in lines 18–21, insisting that he would consider tapering for patients with various medical histories justified by his clinical experience of having done so with both desirable and undesirable outcomes. In line 22, Rebecca reacts with laughter to Ryan’s response, once again indicating that Ryan should be more reluctant to taper. With the use of “we” (line 4), “you” (line 7), and “I” (lines 16 and 19), the extract further indicates that treatment-related decision-making is dominated by staff’s perspectives without active involvement of patients’ preferences.
In this position, mental health staff position themselves as knowledgeable professionals who have the right to act in manners that protect patients and conversely position patients as vulnerable people who have the right to be protected against harm.
Yes, We Need to Welcome Risks to Support Personal Recovery
When accounting for tapering in terms of “Yes, we need to welcome risks to support personal recovery,” the main argument for tapering revolved around securing patients’ right to self-determination by supporting and accommodating patients’ preferences regarding treatment. In this way of accounting, schizophrenia spectrum disorders were outlined as fluctuating illnesses in which the severity of symptoms varies over time. Patients were described as developing and learning throughout the course of illness leading to strengthened coping strategies to overcome challenges and illness fluctuations. These arguments were used to justify that medications should be reviewed continuously and tailored according to current needs with the aim of identifying the least effective dose or establishing remission.
Accounting in this way entailed reporting descriptions of having good experiences in conducting and supporting patients through tapering processes. Offering tapering was recounted as a result of engagement in continuous conversations with patients about their satisfaction with prescribed medications. To minimize the risk of relapse, it was stressed that tapering must be supported by helping patients to be attentive toward warning signs and known stressors, as well as identifying useful coping strategies. Tapering medications to the lowest effective dose was depicted as conducive to pedagogical and relational work. Once patients come out of the sedated state, they become more active and begin to feel emotions providing fruitful conditions for rehabilitative and recovery-oriented approaches. Descriptions of such experiences were used to legitimize patients being potentially undermedicated in relation to what might be needed medically to suppress all psychotic symptoms.
Although mental healthcare services were portrayed as having changed within the last decade with the implementation of recovery-orientated practices, a concern was raised that not all mental health staff embrace a recovery-oriented paradigm. Staff were described as leaning too heavily on the efficacy of antipsychotics to achieve clinical recovery and being unresponsive toward patients' complains of adverse effects. Striving and hoping for a life with a job, family, friendships, and leisure activities was narrated as understandable, and tapering was portrayed as an intervention supporting functional and social recovery. Thus, it was reported necessary to weigh antipsychotic doses up against quality of life and preservation of functional level including daring to take risks to accommodate patients’ preferences for treatment. Opposed to taking chances, taking risks was presented as using clinical expertise to take well-considered risks to support patients in their strive for personal recovery. Recovery-oriented practice was discussed in one focus group in relation to the claim “Recovery = tapering of medication.” Helen, Debra, Emma, and Melissa worked in community mental healthcare services in Region B. Leading up to the conversation presented in Figure 3, the focus group participants had concluded that recovery does not equal tapering. Extract 3.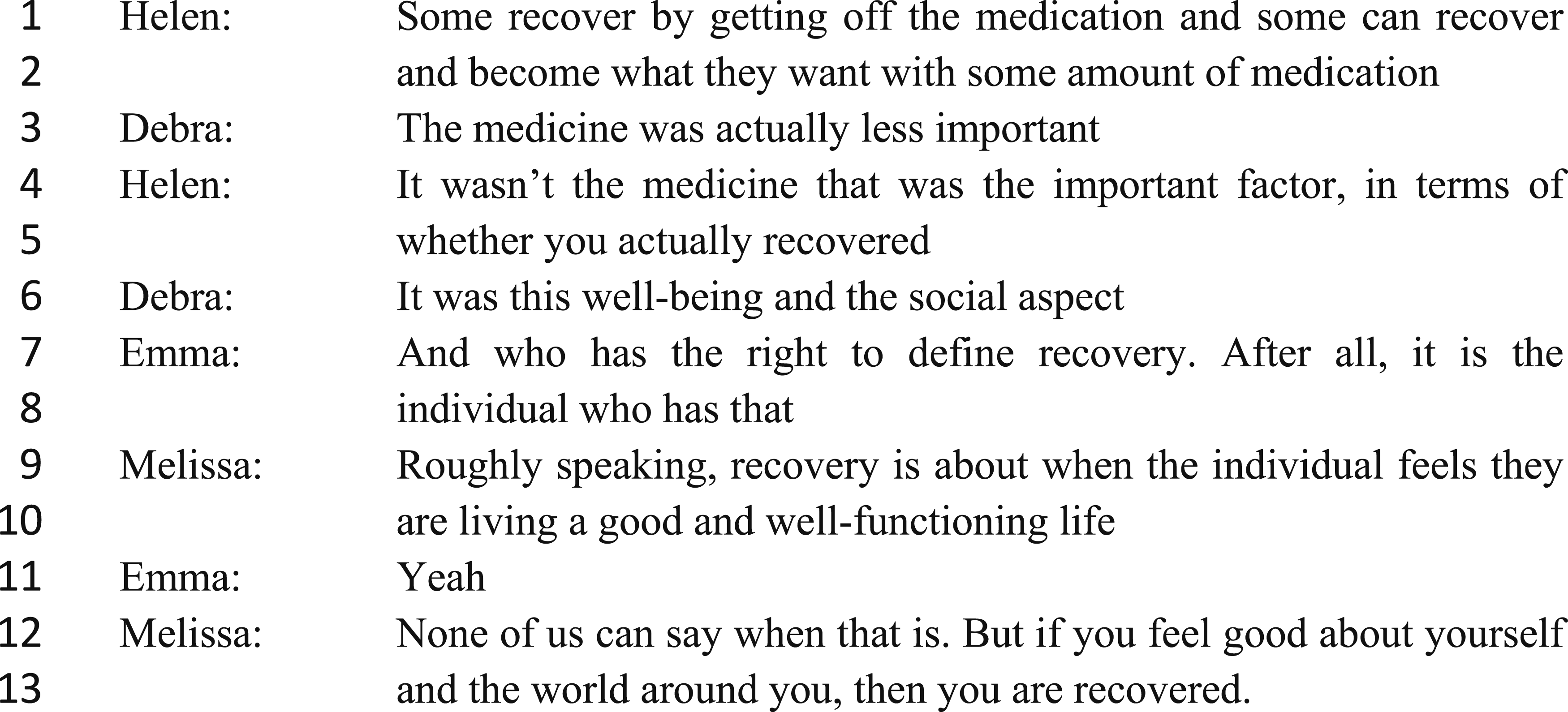
In the beginning of the extract, Helen argues that recovery does not equal clinical recovery. Debra argues that the earlier dominant focus on medication has been minimized with the implementation of recovery-oriented practices (line 3). In lines 4–5, Helen ascertains that in contemporary recovery-oriented practice, medical treatment is no longer considered central to secure recovery from mental illness, to which Debra adds that the central determinants for recovery have been occupied by quality of life and social functioning (line 6). Appealing to principles of patients’ right to self-determination, Emma employs a rhetorical question to justify the viewpoint that it is up to each patient to define recovery (lines 7–8). In the same vein, Melissa appeals to the principle of patients as experts in their own health (lines 9–10 and 12–13) to justify that staff have no right to define what recovery entails for individual patients. Their arguments therefore indicate that practicing according to contemporary recovery-oriented practices requires staff to view patients as equal experts and include patients’ preferences in treatment-related decision-making.
Thus, in this position, the mental health staff positioned themselves as having limited expertise and a duty to acknowledge and include experiential knowledge in decision-making. However, within this way of accounting, staff such as nurses and nurse assistants described how they, because of their positions close to patients, got to know patients better than doctors or even patients themselves. “Knowing patients” was applied to justify that they had the right to speak on behalf of patients in decisions regarding medication and tapering.
Discussion
This study is the first to examine how interdisciplinary mental health staff talk about tapering of antipsychotics for people with schizophrenia. The analysis emphasized the value of exposing discourses on tapering because it clearly revealed different positions and ways of legitimizing action. The positions “No, patients will eventually realize that they needed the medication” and “Yes, but tapering means running a big risk of relapse in symptoms” showed how staff’s discourse was founded in the biomedical model in which the mental health staff foreground medical knowledge and clinical experience, which was in accordance with previous studies on mental health services (K. Jørgensen et al., 2020; Turton et al., 2010; Waldemar et al., 2019) as well as the critique of the dominance of the medical model presented in the introduction. In the position “No, patients will eventually realize that they needed the medication,” little or no reference is given to the fact that tapering could be clinically warranted without being stated as a request by service users. Instead, most of the discourse pointed to mental health staff being pressured to conduct tapering, whereas mental health staff recounted schizophrenia as chronic diseases for which antipsychotic maintenance treatment is needed. Contrary to this, the position “Yes, but tapering means running a big risk of relapse in symptoms” reflected rhetoric in which the mental health staff described tapering as warranted by factors decided on by clinicians, such as signs of adverse effects. However, in neither of these positions, tapering was legitimized primarily out of consideration of service users’ preferences for treatment.
The discourse inherent to the position “Yes, we need to welcome risks to support personal recovery” reflected strong affiliations to the recovery-oriented paradigm, which highlights patients as experts in their own health and patients’ right to self-determination, implying continuous engagement in conversations with service users about effect and satisfaction with treatment. Within this position, service users’ treatment preferences are integrated in decision-making without compromising the mental health staff’s sense of duty of care. This suggests that, contrary to previous findings (Marsh and Kelly, 2018), it can be possible for mental health staff to balance dignity of risk with their duty of care requirement to protect service users from harm. Now, claiming, as in this third position, that the focus of mental health services has changed from a dominating focus on medicine to a focus on personal recovery might be questioned. When comparing the three positions, biomedicine remains the dominant discourse in our findings. Thus, medical knowledge is foregrounded at the expense of integration of clinical expertise and users’ preferences. Despite increasing attention toward and implementation of recovery-oriented practice in mental health services, research shows that the delivery of recovery-oriented practice is challenged (Boutillier et al., 2011) and that recovery orientation does not limit the dominance of the biomedical model (K. Jørgensen et al., 2020; Waldemar et al., 2019).
We argue that the three positions reflect three degrees of paternalism in mental healthcare provision. Paternalism may be defined as actions that restrict autonomous choice, such as coercion, deception, and manipulation or nondisclosure of information (Beauchamp and Childress, 2001). In the position “No, patients will eventually realize that they needed the medication,” known preferences for treatment are ignored and overridden. Authority and legitimacy are given to the course of action already agreed upon by mental health staff, and divergences are only made to secure compliance with medications. The disregard of service users’ preferences are not justified based on temporary loss of capacity to participate in decision-making but out of stipulating to know best what will benefit the person, thus reflecting hard paternalism (Beauchamp and Childress, 2001) of unjustified use of paternalistic decision-making in healthcare (Di Nucci, 2018). In the position “Yes, but tapering means running a big risk of relapse in symptoms,” the mental health staff are bounded by duty of care, which is stated to require them to apply their biomedical and clinical knowledge to protect service users against what they perceive as harmful decisions. Referencing worst-case scenarios and high-stake consequences are used to reject service users’ preferences and to persuade them from tapering reflecting use of soft paternalism in which it can be stipulated that service users are not adequately informed (Beauchamp and Childress, 2001) and not afforded genuine options on how to fully participate in treatment-related decision-making. In this position, duty of care prevails over any risk-taking to accommodate service users’ preferences, which was in accordance with the findings of the review on dignity of risk (Marsh and Kelly, 2018) and the qualitative study on community mental health staff’s views and experiences of antipsychotic reduction and discontinuation by Cooper et al. (2019).
The position “Yes, we need to welcome risks to support personal recovery” revealed a more subtle form of paternalism, in which nurses and nurse assistants justify representing service users as patient-advocates in decision-making regarding medication based on “knowing” patients. This illustrates a blind and uncritical stance toward how they, like other health professionals, represent a paternalistic position. Advocating for and “knowing” patients have been criticized by Lupton (1995) as an idealized version of nursing introduced as nursing practice moved from a task-centered to a person-centered model with the aim of excluding power differences in the nurse–patient relationship. However, Lupton argued that, as part of the nursing practice, nurses are expected to surveille their patients and collect data regarding their health status, and thus, they exert a “medical gaze” (Lupton, 1995). Paternalistic approaches are identified in various contemporary studies of mental health practice (K. Jørgensen et al., 2020; Seale et al., 2006; Valenti et al., 2015). Similar to the findings of our study, a study by Seale et al. (2006) investigating shared decisions in consultations about antipsychotic treatment found that psychiatrists may apply “strategic dishonesty” to ensure treatment adherence at what was perceived as being in the best interest of service users (Seale et al., 2006). However, if decision-making is to challenge the dominance of paternalistic approaches in mental healthcare, it is not sufficient to inform service users or for clinical staff to speak on behalf of service users. In shared decision-making, service users must be actively involved in the process, and decisions must be reached jointly in a manner that includes service users’ preferences (Charles et al., 1997).
Methodological Considerations
Focus group discussions were a fruitful approach to generate data on mental health staff’s perspectives on tapering of antipsychotic medication for people with schizophrenia. The interventionistic and confrontative nature of the activity-oriented focus group discussions combined with a low degree of moderator involvement added to create informal and relatively free-flowing responses compared to answers given during a structured interview. This, in turn, created valuable variation in the accounts applied by the participants. Based on the findings of our study, we cannot know how health staff might act in practice. Thus, this study would be usefully extended by ethnographic studies on mental health staff’s actions in mental healthcare practice to determine whether the identified positions reflect observable actions. The application of theoretical perspectives made it possible for us to take a reflexive stance toward our taken-for-granted assumptions and provide a focus for analysis beyond an everyday perspective (M. Jørgensen & Phillips, 2002). However, we acknowledge that combining a variety of sources (e.g., focus groups, field notes from observations, and journal documents) may have contributed to a fuller exploration of the study objective and that our conclusions will therefore be preliminary.
Conclusion
The three distinctive positions identified in this article predominantly reflected biomedical discourse and, to a lesser extent, recovery-oriented discourse. Notably, all three positions reflected degrees of paternalism with a restricted stance toward mental health service users’ autonomous choice and active involvement in treatment-related decision-making. Thus, the findings indicated that the medical model dominates interdisciplinary mental health staff’s accounts on tapering, including a lack of readiness to letting service users make decisions and a limited possibility for people with schizophrenia to have their requests for tapering of their antipsychotic medication met by mental health staff.
Footnotes
Acknowledgments
The authors would like to thank all participants of the study as well as the development managers and head nurses that helped them with recruitment.
Author’s Contribution
KR, NB, and JM came up with the study idea and the study design, and planned the data generation. KR was responsible for the data generation and initial analysis. KR, NB, JM, and PSC contributed to the data analysis process. KR wrote the first draft of the study, while NB, JM, JN, and PSC critically revised the draft. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Novo Nordisk Foundation (Grant No.: NNF21OC0072644).
Ethical Approval
In accordance with Danish legislation, formal ethics committee approval was not required due to the qualitative nature of the study. All participants provided informed written consent prior to study participation.