
Abstract
The demand for patient-centred care and patient engagement in their healthcare has driven patient portal introduction. The widespread adoption and use of patient portals, however, has been a rather slow process in the United Kingdom. Hence, a limited number of studies have explored patient perceptions and experiences of general portal use, which forms a foundation for successful implementation of a portal. This study, therefore, focuses on the experiences and attitudes of patients regarding use of patient portals and access to their health information. It further explores various factors perceived by patients that may influence portal use and uptake. The overall findings from this study highlight positive patient perceptions of portal use. Nevertheless, it demonstrates various areas of improvement essential to ensure future success of portal implementation and acceptance.
Introduction
Prioritising patient engagement in their care process has gained growing attention due to its potential to allow patients to make informed decisions and increase patient satisfaction with their healthcare outcomes (NHS England, n.d.; World Health Organization, 2016; Irizarry et al., 2015; Laurance et al., 2014). This has therefore increased the demand for patient-centred care in the healthcare sector, resulting in a demand by both providers and patients to increase the role of consumers in their healthcare and decision making (Zarcadoolas et al., 2013). This and several other social and human factors like healthcare expenditure, demand for home-based care, and lack of an adequate number of medical workers have led to the active implementation of patient portals, as they allow remote access, disease self-management, minimised hospital visits, and treatment adherence, thus reducing unnecessary burden on the healthcare staff and resources (Kruse, Argueta et al., 2015).
Patient portals are online or electronic tools that allow patients to access their health information and medical records (Hoogenbosch et al., 2018; Lee et al., 2020; Nøst et al., 2021). These are services that are managed by the healthcare provider and are linked to a patient’s electronic health record (Irizarry et al., 2015; Kruse, Bolton et al., 2015). It allows patients to enter or retrieve their health information, therefore increasing patient participation (Ryan et al., 2016).
Patient Access and myGP are patient portals used by surgery, inpatient, or outpatient services in the United Kingdom (UK), which provide patients with features like appointment booking, ordering repeat prescriptions, secure messaging with healthcare professionals, and viewing medical records (iPLATO Healthcare Ltd, 2021; Mohammed et al., 2020). The NHS App is a more recent service in the country and has functions similar to the Patient Access portal while supporting additional features like the mandatory COVID-19 vaccination proof and checking symptoms against possible health issues (Best, 2019; Nelson and Allkins, 2020). However, implementation, uptake, and use of patient portal services and access to medical records and linked services in the UK are limited, and their widespread incorporation has been a slower process compared to many first-world countries (Mohammed et al., 2020).
Many studies associated with patient portals have included both portals and personal health records interchangeably in their study, although they vary in terms of their ownership and features (Kruse et al., 2015a, 2015b). This variation in ownership refers to the control patients have over their health information in each of these tools. Patient portals are controlled by the patients’ healthcare provider and tethered to the hospital electronic health record system while giving patients access to their health information. Personal health records on the other hand are untethered and give patients greater ownership over their health information and more options for them to input data (Zhao et al., 2018). Despite these variations, existing studies have failed to draw clear differentiation between patient portals and personal health records (Kruse, Bolton et al., 2015). Additionally, although patient portals are developed to increase patient engagement in their healthcare, there is a lack of importance given to understanding their experiences and expectations of using a portal (Ryan et al., 2016). The majority of studies have either focused on practitioners’ or providers’ perspectives of the impact of patient portal implementation (Kooij et al., 2018) or have evaluated the impact of disease-specific portals used solely by patients with a certain health condition such as diabetes or cancer or evaluated the acceptance of certain vendor-specific portals, thereby benefiting the private vendor alone (Mohammed et al., 2020; Sääskilahti et al., 2021). The successful implementation of a patient portal however requires that experiences of all stakeholders including those of patients using varying portal services be evaluated (Kooij et al., 2018). This study, therefore, aims to assess the experiences and attitudes of patients in the UK towards patient portal–enabled engagement, access to medical records and linked information, and its contribution to their involvement in their healthcare process.
Methods
Methodology
A qualitative grounded theory (GT) study was conducted. A qualitative method was used as it aids in generating in-depth information of patient experiences by allowing patients to explain their perceptions in their own words rather than subjecting them to provide limited answers through a survey or structured questionnaire (LaVela and Gallan, 2014).
Study Design
Participants and Recruitment
Adult (≥ 18 years old), UK resident, and English-speaking users of either ‘myGP’, ‘Patient Access’, or ‘NHS App’, with access to their health information or records, were targeted. Recruitment was initiated by posting an advert containing details of the study on various social media platforms and discussion forums including but not limited to LinkedIn, Facebook, Reddit survey subs, and Healthcare Forums accessed via Google searches. Interested participants were asked to contact the researcher by either emailing or filling out an interest form. An email containing the participant information sheet and the consent form was sent to the registered individuals who met the inclusion criteria (n = 24). Individuals who consented (n = 15) were invited for a Zoom interview. Recruitment was carried out over a period of 2 months (September 2021–October 2021), and interviews were conducted until data saturation was achieved, that is, no new concepts emerged. Fifteen participants were interviewed at their convenience, and thirteen were included in the study (two were excluded as it was revealed during the interview that they did not have access to any of their health information or solely used the portal to access the COVID-19 vaccination proof).
Data Collection
Interview Guide.
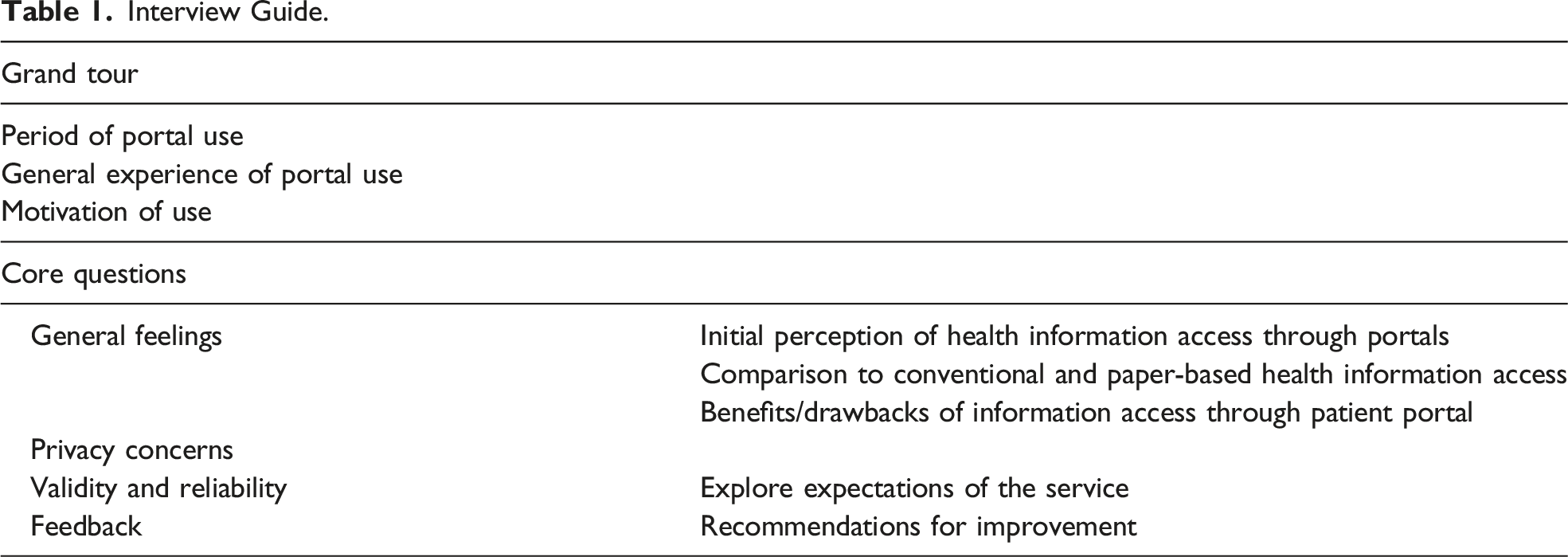
Data Analysis
The interviews were transcribed, and the data were analysed using grounded theory, as it has an inductive and exploratory nature that allows for greater interpretation of patients’ healthcare experiences (Sbaraini et al., 2011). An iterative process of simultaneous data collection and analysis was involved, thus allowing researchers to explore emerging concepts or theories in subsequent interview and allowed testing of emerging themes and understanding any relations or patterns in depth, thus enabling the generation of core theory and concepts grounded in our data.
The constructivist grounded theory approach was employed as it allows the researcher to engage in the creation of theories and therefore strikes a balance between participants’ and the researchers’ views in the findings (Alemu et al., 2017). Additionally, it provides the researcher with the ability to generate novel and comprehensive theories while maintaining the originality of the data collected (Alemu et al., 2017; Chong and Yeo, 2015).
This method comprises initial coding followed by focused coding and theoretical coding, respectively (Chun Tie et al., 2019). Line-by-line coding was employed for the initial coding of data as it provides more scope for critical evaluation of data and therefore aids in the generation of many questions to explore new concepts (Charmaz, 2006). This was then followed by focused coding where codes from the initial coding and memos were compared, frequently occurring codes were noted, and relationships between initial codes were explored to develop more concise codes and categories. In the theoretical coding, these categories were compared, and themes were developed. During the coding process, in-vivo codes comprising specific terms used by participants were used to preserve the meaning conveyed by participants and prevent incorporation of researcher bias (Charmaz, 2006; Chiovitti and Piran, 2003).
During the data collection and analysis, the first author conducted the interviews and transcribed them. Both the authors were actively and independently involved in each of the coding stages, with the first author conducting first-hand coding by reading through all of the transcripts and field notes to get a sense of the data as a whole. The codes developed were then discussed between the two authors to ensure reliability.
Additionally, throughout the coding process, the authors used memos to document thoughts and ideas about the data. Regular meetings were set up to discuss our coding decisions, ensuring that we agreed about the emerging categories and themes.
Results
A core GT identified was that ‘patient portal–enabled access to health information or records alone does not drive patient-centred care and patient engagement’. Five interrelated themes were extracted from coding. Overall, these themes demonstrate that patient portal access to health information drove excitement among its users, and in some cases it enhanced patient activation with their care process and was viewed as a useful step up from the conventional mode of health information access. Nevertheless, the themes have revealed that the portal service used, its features, and patients’ awareness and their perceived necessity of each feature within their portal influence their experience and appreciation of the service. The portal use experience is not only limited to portal design and features but also extends to be influenced by several personal, external, and environmental factors as detailed in themes 2 and 4. Furthermore, patient expectations and responses were analysed to devise a theme highlighting patient portals’ vision for the future.
Theme 1: Patient Portal and Patient Interaction
Portal Service and Its Features
A considerably equal number of participants used Patient Access (n = 7) and the NHS App (n = 10). Some (n = 4) had access to both the services. None of the participants mentioned using the myGP portal, although one participant mentioned having a myGP account, and they found it less useful. Participants who used Patient Access had the service for more than a year, whereas the majority had registered to the NHS portal only in the past 6 months. The use of the NHS App was mostly driven by the need to retrieve the COVID-19 vaccination proof. For example, patients stated, ‘The NHS app, [used] only recently since I heard about its introduction for the travel pass primarily’.
A broad range of features were available to participants via patient portals. These features included ordering repeat prescriptions, booking appointments, and accessing medical information like health records, test reports, consultations, immunisation, and medical history. The features available were different for participants using different portal services and varied depending on the surgery. Participants highlighted this variation, and one stated, ‘In this [NHS App] also you can see consultation, but I did not see much detail’. Another added, ‘I think I’m supposed to be able to book appointments with my GP but I actually can’t ... I think our GP just doesn’t use that function’.
Additionally, the commonly used features varied among participants. A participant stated, ‘For patient access, the main things I used for were appointment booking at my GP’, whereas another said, ‘The patient access I use it mainly for the repeat prescription and for sending requests [medication]’.
Participants displayed poor awareness of all the features available to them through the portal, and some highlighted this by stating ‘I can’t remember which all features it has but the main reason I use it is to order my prescription every few months due to a medical condition’.
Patients’ Portal Experience
Most perceptions of the participants regarding patient portals were positive, expressing that portals made health services and information access easy, efficient, and immediate. Additionally, they described patient portals minimised elaborate conversations with healthcare staff. One stated, ‘It’s [patient portal] brilliant, because If I can get away with not having to ring my doctor surgery, then that is an absolute bonus for me’. Another reported, ‘It was the best experience I’ve had of trying to deal with the GP and manage medicine and stuff like that’.
Theme 2: Factors Influencing Patient Portal Use
GP Recommendation and Patient Choice
In most cases, patient portals were recommended to participants by their GP for use of specific functionalities. One stated, ‘It was then suggested [by the surgery] to make appointments’. Although participants became aware of the service from recommendation by the GP surgery, the majority voiced that ultimately it was their independent choice to register to the service, by expressing, ‘I was happy to like use apps all the time so I was familiar so I would have probably chosen that even though my GP hadn’t suggested it’ and ‘it was my independent choice and no one forced me to use’. Additionally, participants added that the use of the service did not feel obligatory as the conventional mode of access was still available, and one stated, ‘It didn’t seem like I was being forced to [use the service] by my surgery or anything like that. So, I am still aware that there are telephone services available for people who may not have a smartphone or not want to use the app for whatever reason’. However, some participants explained that they had no choice or limited choice of services to choose from, and one stated, ‘My GP surgery only used the Patient Access app ... so there was no choice, and the NHS app is the only app that gives you access to your results and the COVID pass so there was no choice. I had to get both’.
Perceived Benefits and Information Need
Participants’ realisation of the potential benefits of the service aided their portal uptake and use. They recognised the ability of patient portals to enhance the speed and efficiency of their healthcare processes. They identified that portals enabled having all the services presented to them at their fingertips, thereby making access available to them at their convenience and out of GP working hours. One mentioned, ‘It’s [portal] a good deal, better than holding on for an hour or more trying to get through to the receptionist’.
Additionally, increased healthcare and information needs motivated use, and this was evident from participants’ statements like, ‘I was very much like wanting to know as soon as possible when the results came in, so that was sort of what spurred it [use] initially … I would say, I don’t use it often but if something is wrong with me at a particular time then I’ll be using it again’.
Pandemic and Digital Shift
With the COVID-19 pandemic and several healthcare services moving online, portal use, specifically use of the NHS App, among participants increased. One participant emphasised that ‘it is partly to do with the pandemic … was trying to get all the information because in a pandemic it makes you realise that I need to sort out and make sure that all my healthcare is okay’. Another added, ‘The NHS App gives you the option to have a vaccine passport, so that’s automatically a reason to use something like that’.
Theme 3: Patient Portal–Enabled Health Information Access and Its Impact
Patient Emotions
Participants had a positive experience of accessing their health records, test reports, and other health information via portal services. They were pleased to have this service available through their portal. Initial access to their health information spurred feelings of keen interest and curiosity among the participants. These emotions further developed to feeling informed, reassured, in control, less dependent, and more confident. A participant stated, ‘I think it is more interesting really. There was nothing, in particular, I wanted to look up’, and another added, ‘I suppose it was quite freeing in a way or like it gives you a degree of independence from the doctors’. Alternatively, there were also feelings of shock and surprise among some participants after viewing old and forgotten health information, and one expressed, ‘I really liked it, it was quite interesting and it’s quite surprising, it’s a bit strange seeing everything you’ve had wrong with you in the list and it’s quite daunting’.
Healthcare Process
The majority of participants expressed that portal-enabled access to health information had a positive impact on their healthcare process, while some stated that it made little or no significant difference to their care. One explained that ‘It’s not that just because you can see your health information, disease or whatever condition, it doesn’t mean that you then become aware of your health … I would say it hasn’t made any difference by having access’. Many participants highlighted that access to their health information made them aware of their medical history or allowed them to recall forgotten health information, with one mentioning ‘long time ago, I had an allergy to penicillin, that was recorded which I myself had forgotten’. Additionally, access to health records allowed patients to easily compare and identify previous treatments that have worked. It further helped by bridging any communication gaps and language barriers and enabled patients to be more proactive, involve in shared decision making, and make informed healthcare choices. One participant stated, ‘Some of the things the doctors said I didn’t fully understand. But with the app, I can look at it myself’, and a second added, ‘I find that really reassuring I’ve got the level same access level as they [doctors] do’. A patient also highlighted how the patient portal had supported their medical needs during travelling and highlighted its benefit in a situation of potential emergency and stated, ‘As a patient if I am aware of my medication as well, then if I am travelling abroad and all that I am more in control of my own health …. I can have that access in case of an emergency’.
Conventional Versus Portal-Supported Health Information Access
While expressing how portal access made a difference from the conventional method of receiving and accessing health information, participants emphasised that portal access is comparatively faster and serves immediate information needs. They highlighted that it makes information access easier and meaningful with all health information available at one place, thus preventing scattering of health records and aiding the generation of longitudinal health data. Additionally, participants appreciated the ability of the service to allow them to access and interact with their health data at a time and place of their convenience. These views are evident from participants stating, ‘It’s much more efficient, it’s much easier, it’s quicker, it’s done in my time and in my speed at my convenience’, ‘“It’s more convenient rather than getting updates from different places like mail messages or whatever’, and ‘“Through the app, you can just access it on your own terms, no one is trying to prompt you’.
Perceived Drawbacks
Participants identified varying threats of having access to health information and records via their patient portal. Key concerns included an obsession of viewing records and the potential risk of self-diagnosis. One pointed out that ‘I think having access to your own records will lead to people jumping to wrong conclusions about their records, whereas on the other hand, it might require them to see a GP but because you have access to your records you might be less inclined’.
Additionally, participants acknowledged data security and privacy issues. The majority, however, had little or no privacy concerns. This was due to their confidence in either the service provided by the NHS, their device security system, or both. Many believed that a strong password was key to ensuring data security. This was evident with participants stating, ‘I have no concerns because … I think National Health is being quiet, the data protection and all that, they take that, you know seriously’, and ‘it’s just a case of being able to make a good password’. On the other hand, a few were apprehensive of potential hacking but were willing to make trade-offs, either due to the absence of confidential information present within their records or due to their perceived benefits of patient portals. A participant expressed, ‘I am not worried because I don’t think there is anything on there that I am worried about anyone seeing or using it’.
Theme 4: Patient Portal Adaptability and Ease of Use
Information Interpretation
Most of the participants reported that the health information presented to them via their portal was comprehensible and provided detailed information of their diagnosis or treatment. Some believed that the interpretability of the information depended on the type of report and level of an individual’s medical knowledge. This was further reflected among participants as they expressed that although they managed to understand the information presented, they experienced some level of difficulty in interpreting the medical terms and stated that they relied on colloquial and supported explanations to interpret the data. For example, a participant stated, ‘I obviously don’t understand the medical term but if the word normal is used that I will think that is okay’. Many also mentioned relying on Google and other resources to research and understand complex information.
Technological Literacy
None of the participants expressed having trouble in navigating through the given patient portal; however, they voiced their concern regarding the limited accessibility of portals for the disabled and the older population with poor technological literacy. One participant stated, ‘To me, I would say there are no downsides, but I can see that as a problem for people who have no help, no knowledge of how to use the system’, and another added, ‘I think this [patient portal] is more towards the younger generation than the older ones’.
Theme 5: Expectations and Future Developments
Patient Expectation
Several participants had no initial expectations from patient portals and accessing health records, as they registered to the service out of curiosity or to use it specifically for repeat prescriptions or appointment booking. A participant expressed, ‘I had no expectation, to begin with, I didn’t know what to expect so I think it has met my expectation’, and another stated, ‘At first, I was curious, and I’ve accessed some fairly old documents going back to 1993 … It was an interesting read, and I am glad I saw those letters’. They were fascinated to see various features, their health information, and medical history in their patient portal. All participants considered the service reliable in general, but this perception varied for different features. Additionally, one pointed out that ‘it is still dependent on human input, so it is as reliable as you consider a human’, and another added that the service reliability depended on the GP surgery providing it. Furthermore, some had suggestions for future improvement. A participant emphasised this by stating, ‘So far it has met my expectations. Obviously, going forward there is a lot of room for improvement’.
Future Developments
Some of the key suggestions for portal improvements among participants included obtaining more information access via patient portals and incorporating additional features such as accessing various test request forms, inbuilt resource links to better interpret test reports, and results or flagging any potential errors within the records, which can improve their overall experience of portal use. Many voiced the need for establishing consistency of service and portal features offered across GP surgeries and increasing promotion of portal services to enhance portal use and adoption. These were explicitly stated by participants as ‘I don’t understand why all GPs don’t use it. I think if all surgeries used it, it would be a lot easier for people to understand because it would just be one process for everyone’, and ‘I did speak to a few of my friends and not many people seem to be using it [patient portal], I don’t think it is heavily promoted. So, I think marketing a bit more’.
Discussion
The participants in this study used the NHS App, Patient Access service, or both. None of them stated using the myGP service; this could be due to poor promotion of the service in the participants' practice as highlighted in a study by Ryan et al. (2020) or due to promotion of alternative services. A broad range of features were available to participants through the NHS and Patient Access portals, including ordering repeat prescriptions, booking appointments, viewing medical records and test results, and accessing consultation documents. However, the features available and used by each participant varied depending on the portal service used and their registered General Practitioner (GP) surgery. The variation of features within the same portal service is due to the surgery being responsible for deciding what portal services are accessible to their patients (EMIS, 2021; NHS website, 2022). Additionally, most of the participants displayed poor awareness of various features within their patient portal, therefore leading to non-use. This results when there is a lack of communication and guidance provided to patients by the providers regarding portal features and their use (Powell et al., 2018; Walker et al., 2020). Patients are usually provided with details of setting up an account and logging in, whereas information on features is not elaborate (Lee et al., 2020). Portal introduction must, therefore, be accompanied by adequate patient training and guidance to enable effective use of the service (Lee et al., 2020).
The majority of the participants in this study revealed that their GP recommended the respective portal service, which is known to play a significant role in patient portal adoption and use (Ryan et al., 2016). Although portal services were recommended, participants expressed having an open choice to register for the service. Hence, their continued portal use was influenced by their voluntary interest and perceived benefits of the service, which are considered key factors essential for long-term use of a portal (Wildenbos et al., 2017; Mishuris et al., 2015; Elers et al., 2018). Additionally, the use of the NHS App among participants was strongly influenced by its feature which allowed them to access their COVID-19 vaccination proof. This outcome is in accordance with a study (Powell et al., 2018), which highlights that in many cases patient portal use is a result of a reactive process to either a policy or a process.
Overall, among the participants, booking appointments and ordering repeat prescriptions were the most widely used features within a portal, whereas accessing health records and test results was a result of curiosity or response to the availability of the service. This is consistent with previous research findings (Alpert et al., 2019; Mohammed et al., 2020). Alternatively, studies by Rodriguez (2018) and Moll et al. (2018) reported that accessing medical records and viewing test results were the most used features of the portal. This difference in findings could be a result of varying medical and health information needs among portal users. For example, in this study, the appreciation of the ability to access health records and information via a portal was directly proportional to the healthcare needs of the participants. This finding is consistent with previous studies which have noted that individuals’ health, discharge, and medication status influence portal use (Ancker et al., 2015; Fisher et al., 2009; Hannan, 2010; Moll et al., 2018; Ordaz et al., 2021; Powell et al., 2018).
Irrespective of their health status, participants had positive experiences of viewing their health information, medical records, or test results. They reported feeling confident, in control, aware, and informed of their health and care processes. This response is consistent with previous studies (Alpert et al., 2019; Mold et al., 2015; Moll et al., 2018). Furthermore, participants expressed feeling reassured by being able to access information which earlier only their healthcare practitioners had access to. Some also cited that portal access helped bridge language and communication barriers with the providers. This equivalent access and enhanced information communication prevent patients from feeling powerless and ignored (Rathert et al., 2017), which in turn can aid in safeguarding their emotional well-being which can otherwise be negatively influenced by caring neglect (Reader and Gillespie, 2013).
In addition to expressing these emotions, participants noted several benefits of accessing their health information and records. They expressed becoming aware of their medical history and allergies which they previously had no knowledge of or had forgotten. This awareness aids in ensuring patient safety by minimising the risk of patient allergies and history being ignored during treatments (Ordaz et al., 2021). Access to medical history further allowed participants to compare different treatments, identify progress and patterns, and make informed choices in their ongoing or upcoming care. A similar benefit was voiced in a study by Fisher et al. (2009).
Furthermore, accessing health information and records via a portal was deemed easy, quick, and efficient by the participants. They valued the ability of portals to make seeking emergency medical assistance easier, with all necessary health information and history easily accessible. Individuals travelling frequently considered this as one of the most beneficial aspects of electronic access, since it allowed them to easily share health information with different care providers and healthcare services. This in turn can enhance care coordination and save time and resources otherwise spent on conducting repetitive consultations and tests (Baudendistel et al., 2017). Additionally, participants reported that electronic access to their health information helped to keep them on track of their healthcare timeline by keeping them up to date regarding their treatments, immunisation, and medication and therefore ensured receiving medical attention when necessary. This outcome is useful as, in most cases, there is a lack of clarity regarding who is responsible for test result dissemination, thereby resulting in serious safety implications for patients due to the potential failure to follow up (Thomas et al., 2021).
Participants in this study identified patient portals as more beneficial compared to the conventional modes of accessing health information as they not only catered for their health information needs but also provided multiple services. This could be one of the drivers to portal use as a study (Hannan, 2010) suggested that access to records alone is not viewed as a useful service by patients but this feature supported by options like appointment booking, messaging, and ordering prescription intrigued patients. Additionally, it allowed having all resources and data in one place and prevented scattering of information. Participants further emphasised their appreciation regarding the possibility of accessing information at a time and pace suitable to them. Similar admiration is reflected among patients in a study by Zanaboni et al. (2020). Furthermore, participants were not very concerned regarding their ability to interpret the health data presented to them. Although many reported difficulties in understanding medical terminologies, which is considered essential for interpreting medical information (Freise et al., 2021), the ability to view their health information in accordance with their convenience aided their data interpretation. Some reported looking up the internet and researching as methods used to aid their interpretation. On the other hand, some responses reflected that they did not make an effort to understand the information in depth and instead referred to informal and simple terms to ensure the reports are normal.
The majority of the participants displayed awareness regarding data privacy, but it was one of the least expressed concerns. Among users of the NHS App, this response was majorly due to trust in services provided by the NHS, therefore suggesting the influence of product branding, which was demonstrated as one of the strengths of the NHS App by Beaney et al. (2019). The lack of concern was also influenced by participants’ perception of the level of sensitivity of their medical information within their portal. On the other hand, some participants were willing to make trade-offs. This aligns with findings of a study (Vodicka et al., 2013) which noted that irrespective of their privacy concerns, patients are keen to use patient portals and access their health information as they believe that the benefits of the service outweigh any potential harm or drawbacks.
No participants in this study exhibited personal negative experiences of portal use. Nevertheless, they expressed their concerns about how a portal could negatively impact a certain set of people. The most expressed concern was patient portals’ potential to stem disparity by limiting access to old, disabled, and individuals with poor health and technological literacy. This risk holds true in a study (Wildenbos et al., 2017) that reported lower portal acceptance among the older and vulnerable groups as a result of poor health literacy or resistance to change. Alternatively, another study (Lockwood et al., 2018) identified that older adults registered to one or more portals irrespective of their technological literacy, therefore highlighting their interest in using a portal. This suggests that increased provider encouragement, support, and training can prevent these individuals from being alienated from the service (Lyles et al., 2013; Mishuris et al., 2015). Furthermore, there were concerns that access to health information and medical history via patient portals might result in paranoia and obsession among some individuals. Similarly, physicians in a study (Witry et al., 2010) expressed concern that access to health information could fuel hypochondria among users.
Despite these general concerns, the services offered by these portals met the majority of the participants’ expectations. The access to health information feature was beyond the initial expectation of most of the participants. Nevertheless, many expressed keen interest in obtaining more health information and details of their medical records. This demand is persistent among patients across various studies (Dendere et al., 2019; Sulieman et al., 2020; Van den Bulck et al., 2018), therefore promising future success of portal implementation and adoption.
Limitations
This study has some limitations. Firstly, the process used to recruit participants through social media adverts could have limited participation of individuals inactive on these platforms or those with minimal access to the internet. This could have also influenced the lack of participants using the myGP patient portal. Secondly, some Zoom interviews were interrupted by the individuals’ video conferencing set-up which could have restricted them from providing elaborate answers. The impact of these on the study results however are minimal as 13 participants, which is considered the minimum number required to achieve saturation in an interview-based study, were included (Vasileiou et al., 2018). Thirdly, this study did not collect patient demographics; this thus limits the study’s ability to explore influence of age, gender, or health status on the use of patient portals. However, the concepts emerging in this study can be used as a foundation to explore the influence of various patient characteristics on the use of patient portals.
Conclusion
The core category and the themes in this study contribute towards understanding patients’ experiences of accessing health information through patient portals and represent that patient portal is well accepted among patients; however, leveraging its potential to contribute towards greater patient engagement and enabling patient-centred care require greater efforts than solely providing patients access to their health information or records. It was evident from the findings that portal use among patients is influenced by personal preferences, the service provider, and portal features, whereas their perceptions of accessing health information are influenced by their health situation and information needs. There is also a scope for future development. A key area of improvement is the need for establishing consistency of portal service offered across surgeries. This can aid familiarity and usability of the service, therefore avoiding confusion among patients. Additionally, there is a need for increasing awareness of the service and its available features and providing patients with the necessary support in the form of training and encouragement to enable uniform access and use. Overall, the study’s findings can be leveraged by policymakers, portal service providers, and healthcare providers to improve the interventions to enable patient-centred care.
Footnotes
Acknowledgments
The authors were the only contributors to the article, and therefore, they have no additional acknowledgements to state.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study has been approved by the Swansea University Medical School Research Ethics and Governance Committee (SUMS RESC project ref. no.: 2021-0065). All participants provided digitally signed informed consent prior to participation in the study.
Guarantor
Preksha Machaiya Kuppanda will be the guarantor for this article.
Contributorship
All authors included have made substantial contribution to the design of work, analysis, and draft of the article. The version of the article being submitted has been approved by both the listed authors.