
Abstract
Behavioral and psychological symptoms of dementia (BPSD) pose great challenges for the caregivers during the evolution of the disease with impacts on patients, caregivers, and healthcare providers. Caregivers often remain very present and involved once the difficult decision has been made to relocate the person to a residential and long-term care center (centre d’hébergement de soins de longue durée [CHSLD] in Quebec). The experience of caregivers about BPSD management in CHSLDs remains poorly understood. The aim of this study is to explore the needs and experience of caregivers of patients with BPSD living in CHSLDs, as well as the solutions they suggest to better manage BPSD in CHSLDs. We carried out this qualitative interpretive descriptive study with six focus groups, including 32 caregivers, in Quebec, Canada. Data analysis identified six themes: (1) the transition period between home and the CHSLD; (2) the lack of knowledge about BPSD; (3) the approach to BPSD by healthcare professionals; (4) the lack of communication; (5) defining the caregiver’s role in the healthcare team; and (6) the caregiver’s need for respite. These results offer relevant avenues to improve collaborative practices with caregivers in CHSLDs involved in the care of people with BPSD.
Keywords
Introduction
More than 55 million people worldwide are affected by major neurocognitive disorders (MNCDs), one of the leading causes of disability and loss of autonomy among elders (World Health Organization, 2021). Up to 80% of individuals diagnosed with MNCD will experience neuropsychiatric symptoms, also known as behavioral and psychological symptoms of dementia (BPSD) (Van der Linde et al., 2016). These symptoms include agitation, anxiety, psychotic symptoms, disinhibition, aberrant behavior, and aggression. They are a major burden and distress factor for the person with MNCD as well as their caregivers, and strongly contribute to the decision for institutionalization (Bozgeyik et al., 2019; Chapman et al., 2020; Chiao et al., 2015; Toot et al., 2017). We define “caregiver” as any relative, partner, friend, or neighbor who has a significant personal relationship with, and provides a broad range of assistance for, an older person or an adult with a chronic or disabling condition (Family Caregiver Alliance, n.d.).
In Quebec, Canada, the residential resources for people with evolving MNCD are mainly centres d’hébergement de soins de longue durée (CHSLDs), translated as residential and long-term care centers. People admitted to a CHSLD usually have a great loss of autonomy and can no longer be safe at home despite the resources and support in place (FADOQ, 2020, Gouvernement du Québec, 2019). As of March 31, 2020, 38,886 people lived in a public or private CHSLD. Of this number, 92% were aged 65 and over and 48% were aged 85 and over (Ministère de la Santé et des Services sociaux du Québec [MSSS], 2021a). In 2018, patients with MNCD represented up to 80% of the residents living in CHSLDs (MSSS, 2018). CHSLDs offer a 24-hour staff presence, mainly beneficiary attendants, auxiliary nurses, and licensed practical nurses. These institutions are facing problems regarding care, staff shortage, and facilities falling into decrepitude for more than 15 years (Archambault, 2017; FADOQ, 2017; Protecteur du citoyen du Québec, 2019). The median survival following admission in CHSLDs was 649 days (21 months) between 2016 and 2019 (Nguyen, 2022).
In 2018 in Quebec, approximately 20% of people declared being caregivers, which represented approximately 1,489,000 people (MSSS, 2021b). Even after placement in residential long-term care facilities, caregivers remain involved in the personal care of their loved ones (Gaugler, 2005). A recent expert report estimates that caregivers provide nearly 85% of the care for the elderly, regardless of living environment (Centre de recherche et d’expertise en gérontologie sociale du CIUSSS du Centre-Ouest-de-l’Ile-de-Montréal, 2020).
Background
Caregivers are an invaluable resource for the quality of life of patients with MNCD and for ensuring good management of BPSD. They have a deep understanding of the patient, stemming from their knowledge of the individual, their tastes, values, biographical history, fears, and worries, which is essential to the implementation of an adapted approach to BPSD (Graneheim et al., 2014; Kolanowski et al., 2005; Powell et al., 2018; Robertson et al., 2019). However, being a caregiver often comes with experiencing high levels of burden through physical, financial, and psychological consequences. Indeed, their role directly impacts their social and their personal life. It also brings emotional burden such as tenseness, strain, anger, and the guilt of insufficient caring (Ankri, 2005; Chiao et al., 2015). Furthermore, a systematic review (Sury et al., 2013) showed that admission to a care home did not relieve the caregiver’s burden and could even generate a feeling of guilt and failure. Graneheim et al. (2014) studied the experience of caregivers who had to relinquish the care of a person with dementia to a nursing home and found that they were going through a crisis process.
Meleis’ theory of transitions (Meleis, 2019; Meleis et al., 2010) allows us to better understand the experience of people living an event that leads them to move from one state or condition to another and how they adapt to it. According to Meleis’ theory of transitions (Meleis, 2019; Meleis et al., 2010), a situational transition such as placing a loved one in a CHSLD involves changes in their needs that affect several facets of their life and lead them to redefine themselves (Davies, 2010; Davies & Nolan, 2003). Thus, a healthy transition, which means that the person has found a new state of well-being, a new self, requires the identification and response to these needs by the healthcare team (Davies, 2010). Some of these needs have already been identified in previous studies. Graneheim et al. (2014) identified that transition could be facilitated with support to maintain a significant relationship with the patient, and by being formally recognized as partners in care, with their experience being valued. Another study suggests the caregiver’s quality of life could improve with adequate support and communication from existing staff (Barken & Lowndes, 2018). Even though there is a growing literature about the general needs of caregivers whose loved one is placed in a nursing home, we know little about their experience in regard to better BPSD management after placement. Therefore, in order to better support caregivers of patients with BPSD living in residential and long-term care facilities, it becomes essential to increase knowledge about their needs in this specific context. Our research question was: what are the needs of caregivers of people with BPSD housed in CHSLDs, and the best way to meet them, from their point of view?
In the article, we use the term “patients” to refer to the people living with MNCD and BPSD; we must keep in mind that patients are loved ones, with relationships, unique stories, and once fulfilled lives.
Methods
Design
This study is based on the methodology of the interpretive description of Thorne (2016). The interpretive nature of the description helps to understand the meaning people give to their experience, as well as the links between the components of this description. Thus, the interpretive description allows a better understanding of the way in which the experiences, the needs, and the solutions envisaged by the caregivers are articulated. The results obtained can then serve as a relevant basis for concrete applications in clinical practice (Thorne, 2016). In psychiatry, interpretive description is useful to better understand lesser-known, complex, and sometimes even chaotic phenomena (Ng et al., 2020). Our diversified research team included a geriatric psychiatrist working in a variety of contexts including in CHSLDs; three postgraduate students who are also clinician researchers who have practiced in CHSLDs; and a researcher in nursing sciences with expertise in mental health and qualitative research. From the start of the study, the members of the research team wrote a collective methodological and reflexive electronic journal. This journal served to detail methodological decisions and the reflective component served to help researchers reflect on their own influence on the research process, as well as to work collectively during data analysis.
Participant Recruitment
Recruitment extended from May 2018 to December 2018, and took place in 10 CHSLDs affiliated to 2 local health districts. We recruited participants using the purposive sampling method. They were solicited by paper advertisements, such as posters and pamphlets that were posted in CHSLDs, or directly by nurses and doctors working in the CHSLDs. Once they communicated their interest, researchers called them to briefly explain the project and discuss their availability to participate in a focus group. Any caregiver of a patient living in a CHSLD and suffering from BPSD could be included in this study. Participants had to be 18 years old or older and speak French or English. There were no exclusion criteria. We sent the consent form by email to each participant before the focus group. At the beginning of the focus group, we verbally explained the project, and the participants signed an informed consent. At any time during the study, participants could withdraw their consent. We obtained ethical approval from the Research Ethics Board of two health centers located in two different regions of the province of Quebec, with the final approval given by the Comité d’éthique de la recherche du CIUSSS de l’Estrie—CHUS (approval no. MP-31-2018-2584). There was no financial compensation or reimbursement for research participants.
Data Collection
Data consisted of focus group interviews and field notes. At the beginning of the focus group interview, we explained the main concepts (e.g., BPSD or MNCD) pertaining to the study to the participants, to ensure a common understanding of the topic. Focus group questions were built after meetings with professionals and physicians working with our population, mainly from geriatrics and geriatric psychiatry teams. We favored this method because it stimulates the discussion on a shared lived experience, and thus obtains a rich portrait of the experience of informal caregivers through verbal interaction (Krueger & Casey, 2015). We conducted focus groups using an open interview guide to explore, first, the experience and needs of caregivers, and second, to find solutions for the difficulties that were identified by the participants. Here are few examples of questions from the interview guide: - How moving to CHSLD redefined your role as a caregiver? - What is your role in managing BPSD? - What are your needs regarding management of BPSD?
The focus groups were conducted in CHSLDs and lasted on average 1.5 hours. There were a total of six groups ranging from three to seven participants. We met the participants at the CHSLD where the person in their care lived, or in a CHSLD in the same region. The focus groups were led by two researchers at a time, where one mainly conducted the interview while the second overlooked the technical aspects, such as ensuring anonymization and time checking, as well as taking field notes. At the end of each focus group, time was taken to provide feedback on the group experience and discuss the participants’ experience, as well as to answer any questions, to best ensure the well-being of the participants. Ten of the participants were caregivers of patients whose psychiatrist in charge was a member of the research team; eight were met by her during the focus group. The interviews were audio-recorded and then transcribed in verbatim reports, where each participant was assigned a numeric code to ensure anonymity. Field notes were also taken immediately after interviews with both researchers during debriefing sessions.
Data Analysis
Data analysis began with the the first focus group interview. The focus groups interviews were conducted until the researchers reached consensus on the formulation of the categories and when a rich description of the phenomenon that takes variation into account was obtained (Thorne, 2020). The analysis was carried out with the method of Miles et al. (2014) which includes three levels of coding: (1) the condensation of data, by a first level coding and the development of themes; (2) the presentation of data: making connections between emerging themes in order to make them larger themes, by building a thematic tree structure; and (3) the elaboration of conclusions and their verification through an iterative process in the form of tables (matrices) to find the best way to group the themes in order to obtain the best possible representation of the phenomenon studied. To do so, each verbatim was coded line by line, mostly by teams of two researchers at a time. Throughout the coding process, we consulted our field notes, wrote analytic notes in our collective journal, and met to gain depth and consensus in our understanding of the data. As we acquired a good sense of the data with the analysis process, there formed a consensus-based understanding of caregivers’ experience, needs, and related solutions in six categories presented in the result section.
Results
Participants
In total, we interviewed 32 participants: 22 women and 10 men, aged between 47 and 82 years old. They had been acting as caregivers for between 7 months and 20 years. They had various relationships with the patient: spouse (n = 13), child (n = 14), sibling (n = 2), ex-partner (n = 1), cousin (n = 1), and sister-in-law (n = 1). Five people declined to participate; one did not consider himself a caregiver, three had difficulties attending the focus group, and one did not call back.
Needs, Experiences, and Solutions of Caregivers
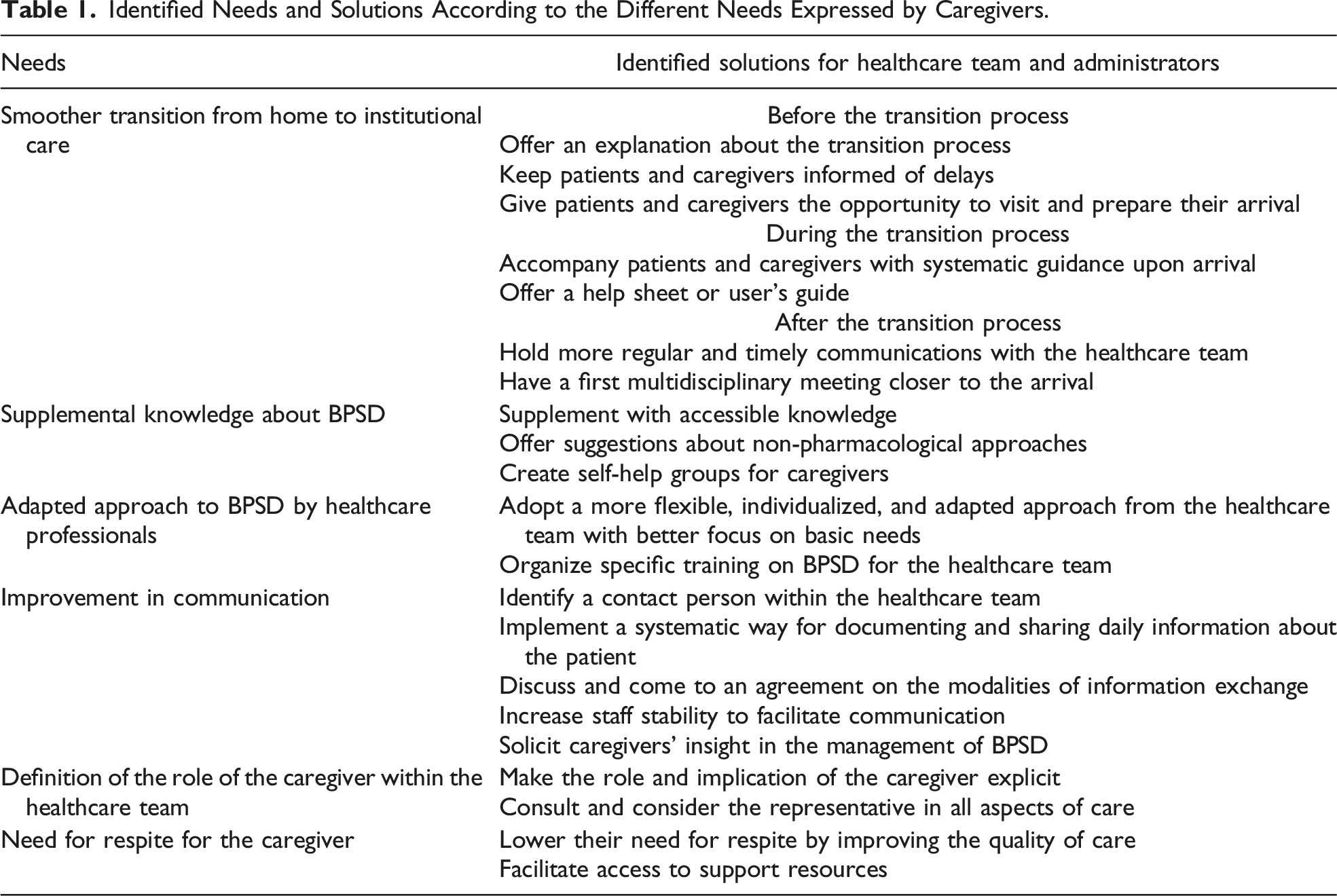
Identified Needs and Solutions According to the Different Needs Expressed by Caregivers.
Need for a Smoother Transition From Home to Institutional Care
Most caregivers expressed several difficulties with the transition process when the patient moves from their home or a seniors’ residence. Participants describe that the transition would be smoother if they could have a timeline and explicit tasks to prepare and better accompany the patient. In their experience, they are often not consulted when choosing the CHSLD and think they have to fight to express their disagreement. They report that the selection process for the suitable facility is long and primarily based on administrative aspects that are not very close to clinical reality: I didn’t get much support. I’ll put it that way, and leave it at that. The waiting times were very long. My mother’s assessment … we could say… They did an assessment, and it took forever, it never seemed to end. And on top of that, it was bad, she was not oriented properly.
They say that this process results in the patient having to move, and that moving numerous times results in a deterioration of the patient’s condition, which causes the caregiver great stress and distress: “In fact, on my end, I didn’t find much support. My mother, in thirteen months, had to move six times.”
Despite long delays for placement in a new institution, caregivers find they are not updated regarding the waiting times, often notified at the last minute, with little time to prepare for moving. But now, it’s for the next morning, not in three days, the next morning. So we prepared the bags, packed, and announced the news. It was quite a big process, and it seems that when we get there, we take care of the administrative stuff: the petty cash, the hairdresser. Then, everybody arrives. Anyway, I find, and yet I work in the field, I think they take for granted that we all know how things work. But it’s not like that at all in real life. And even me, who knows a bit about it, felt helpless. So, I tell myself that someone who doesn’t know about it at all is really going to have a hard time. Anyway, that’s how I experienced it.
On the day of admission, many caregivers feel overwhelmed by administrative procedures without appropriate support. They express that this process makes a very emotionally hard day even more difficult. In comparison, caregivers who were met by the staff upon arrival note that this made the transition easier. Others describe that having a say in the relocation, or being able to visit the CHSLD beforehand, facilitated the overall process.
Overall, caregivers feel that adaptation to this change is also hard emotionally: “To get her into [the CHSLD], it was the worst moment of my life. I’ll remember that for the rest of my life. I cried about it for two days. It’s terrible to arrive home alone. It’s frightening.” Many are left isolated at home and alone to face their role change. They feel guilty for the relocation of their loved one.
Although many expressed they could initially be relieved to rely on someone else to look after their relative, caregivers reported they could become more concerned and stressed after the transition. They described different causes: the patient displaying more BPSD following the change of environment and the decreased quality of care. A participant said: When, after a week there, you realize that it’s not working at all. They say, ‘Well, she has behavioural problems, and this and that.’ Then you say to yourself, ‘Whoa, where did that come from, she didn’t have that before.
With the long waits to see the physician or attend multidisciplinary meetings, they are worried that the CHSLD team will not be able to meet the patient’s basic needs. Furthermore, they become wary of the incidents that occur in CHSLDs, such as falls.
On the other hand, other caregivers report that the initial relief is maintained in environments they trust. Consequently, they observe improvements in their quality of life, reductions in their distress, and they feel more secure: “But in a way, I was relieved to know that my mother would be taken care of in an environment where there would be people to look after her.”
Solutions
To address their needs regarding a smoother transition process to CHSLDs, caregivers made the following suggestions: (1) update them on delays before the patient moves to a CHSLD; (2) provide more information about the process; (3) put them in contact with a contact person within the CHSLD if questions arise; (4) allow them to visit the CHSLD before the transition and to prepare the patient’s room before their admission; (5) provide systematic guidance upon arrival and initially offer regular communications to update them on the patient’s condition; and (6) schedule the first multidisciplinary meetings closer to the arrival. They think that written information would be helpful, such as a guide with factual information (e.g., contact details, to-do list for the admission day, and practical as well as support resources for caregivers).
Need for Basic Training on Knowledge About BPSD
Overall, participants reported they could confidently manage BPSD at the time of admission to a CHSLD because of their involvement with and knowledge about the patient themself, their experience with the illness, their intuition in the best approach to use, and their ongoing creativity. They often help the CHSLD team find the triggers and look for concrete solutions to reduce BPSD. With their approach, caregivers feel they have better outcomes than the healthcare team because they invest more time and are more emotionally involved: She loved choirs. I understood that, and I knew that. And it’s also something we have in common. I love music of all kinds. I seem to have a very special connection with my mother in terms of music. When I use that, it works. And there’s even a nurse who asked me to give her the titles of songs that I make her listen to. I’m working on that, I’m going to give her some. And that’s it, it works!
However, most still feel insecure and think they could benefit from more knowledge on the subject. For some, this feeling is exacerbated by invalidating comments made by CHSLD staff. They would appreciate more reassurance about the measures they have already implemented or shared with the staff, and education about MNCD and BPSD.
Within their process of learning and caring for the person suffering from MNCD and BPSD, many express having a sense of personal growth as they learn new skills and fulfill themselves as a caregiver: “Anyways, as for me, I’ve developed more compassion for human beings, more love for people in general. I’ve seen myself change through these years because I was a caregiver.”
Solutions
To improve their knowledge about BPSD, caregivers ask the healthcare team to help them by teaching them strategies to de-escalate BPSD (e.g., non-pharmacological approaches). They also suggest self-help groups for caregivers to share and benefit from others’ experiences.
Need for an Adapted Approach to BPSD by Healthcare Professionals
Many caregivers report that they had to adapt their approach to patients and would like healthcare workers to do the same. They raise the concern that personalized non-pharmacological interventions are not always used as the first-line treatment for BPSD. They observe that basic strategies, such as meeting a person’s needs (e.g., ensuring that patients wear their glasses and hearing aids) or individualizing the approach, are not routinely implemented. They also feel that CHSLDs are clinical and unwelcoming, and should instead be a warm and living environment. Some even compare them to a prison, as people cannot get out and the rules are rigid. Oftentimes, caregivers observe that there are less BPSD manifested by patients when staff members give more attention and time to them, and when they adopt a more humane and caring approach. Furthermore, caregivers highlight that greater stability of staff members allows for the development of a bond with patients. On the other hand, caregivers describe that staff often do not know the patient’s life story, characteristics, and sometimes even their name.
Unfortunately, most caregivers observe that the difficulty in managing BPSD is compounded by the staff’s lack of knowledge about MNCD, resulting in incomprehension about the different BPSD and the best approach. However, they noticed a significantly better approach implemented in the Special Care Units, where the mission is specifically to offer specialized care for BPSD. This brings great relief to the caregivers whose relatives have benefited from this specialized care. Caregivers note that staff members that do not adopt the right approach are a minority, but this makes a large difference for patients with BPSD. They observe that unskilled staff members are more prone to use medication, often not helpful, or more inclined to use methods that appear timesaving but do not maintain autonomy (e.g., diapers or restraints). While some caregivers agree to give medication because they are eager to see the patient relieved quickly, many would like an approach that involves less medication and more attention to the person’s life story and basic needs. They also note resistance to change in the practice that perpetuates difficulties in adopting a good approach to BPSD: I had a document. In terms of behavioral approach, there’s this, this, this… But it didn’t change a thing. And we came back with an intervention that was done here. There are certain elements that have changed, but hardly, hardly.
Indeed, many observe that if a doctor, a health professional specializing in BPSD, or themselves make a suggestion for better care for the patient, this suggestion is not always implemented, and if it is, it is often only for a short period of time: “When the clinical nurse specialist wasn’t there, it was sure to come back to natural. And I saw things that didn’t make sense that came back to how things were before her recommendations.”
Thus, caregivers often notice that these practices diminish the quality of care and as a consequence BPSD are maintained or, worse, exacerbated. Sometimes, these shortcomings in basic care go as far as negligence and deprivation of care: You know, my mother, because she was aggressive, they kept her in the same incontinence underwear from noon to 8 o’clock at night. Because she was aggressive, they didn’t reposition her in bed overnight. Because she was aggressive, and she pushed her tray away, well she didn’t eat, and too bad for her. Because she was aggressive, that was always the question for … she could stay in bed in the afternoon because she had been aggressive in care.
To compensate for the lack of individualized approach to BPSD and basic needs not being met, some caregivers get more involved or hire a care attendant. Overall, they think the difficult work conditions (e.g., work overload, understaffing, and staff instability) strongly contribute to their observations that healthcare professionals cannot manage BPSD properly.
Solutions
Caregivers would like the healthcare team to be more flexible in its approach to BPSD. They suggest focusing more on responding to patients’ basic needs, such as comfort, hunger, thirst, and toileting. They would like to be solicited to find solutions and adapt approaches in this regard. They advocate for the healthcare team to take greater interest in the patient’s life story and use this information as support in their care: There are two things she doesn’t have: she doesn’t have vision loss and she doesn’t have hearing loss. It’s written in her life story, by the way. Nobody reads it. My mother is not deaf, my mother understands everything, everything, everything… If you yell at her, she gets aggressive.
Caregivers would like the healthcare team to treat the patients as they would like their relatives to be treated. Many also believe that the healthcare professionals would benefit from more specific training regarding BPSD, and that skilled staff have better outcomes with BPSD management: The key is the staff, then the information, the education about this disease. That’s the only way to manage it. It’s not with medication and strength, it’s knowing how to deal with it… coax the person, how to talk to him or her.
Most believe that a better organization of care would be beneficial. For instance, CHSLDs could put in place a more generalized implementation of the Special Care Unit approach and better allocate patients on different floors based on their MNCD.
Need for Improvement of Communication
Many caregivers feel that better communication is needed with the healthcare team to ensure proper care of the patient on a daily basis and in a continuous way, specifically regarding BPSD. They would like the nursing staff to be more proactive and to update them more regularly regarding daily events. They want to be aware if the patient’s condition is deteriorating and to be informed about their relative’s eating habits, sleeping patterns, and daily activities and how they are doing on a given day. Finally, some caregivers express that greater exchange of information can help identify triggers to address BPSD. While some want to meet the treatment team on a regular basis, others feel that they must fight to make sure that the treatment team attends the meetings already scheduled. Others feel that these meetings are not very useful as they are often held without the regular staff, making it difficult to write a good intervention plan. They would like for this plan to be applied and respected by all. Many caregivers express that they must repeatedly ask for information from staff and they often feel like they are bothering them when doing so. They encounter long delays to obtain requested information, and often that information is lost or unavailable. The whole process takes up a lot of their energy: That I don’t feel bad and say: ‘Oh, I should go … ah, I’ll wait a bit.’ I’m always walking on eggshells, I don’t want to bother them because I can see that there are some good things … and, at the same time, I want to have the information because I feel that my mother is not doing so well today. Especially since right now her condition is going down. Everything is changing. I’d like some kind of automaticity.
For caregivers, this lack of communication sometimes manifests as an absence of communication or perceived avoidance from the healthcare professionals. Furthermore, some suspect that information is purposely hidden from them. As a result, they feel disrespected and do not trust the healthcare team: “So I don’t understand this lack of communication. But not only the lack of communication, this sort of reluctance to share information. It’s like they’re saying, ‘We know what we’re doing, don’t bother us!’” Consequently, some caregivers will document gaps in care with notes, photos, or videos. Some caregivers brought to light that the lack of communication may have a legal impact when decisions are made regarding medication changes or other important health situations without consulting the patient’s representative: When I go to the doctor, my doctor talks to me. I am my mother’s representative, so I expect that when my mother sees her doctor, that he’ll talk to me, that there will be a discussion, that there will be a sharing of information.
In circumstances where there is a lack of communication, caregivers are worried about the quality of care in CHSLDs and it drives them to advocate for a better system, conditions, and care. Some will even hire lawyers. Even though many would like to complain and take action, they are afraid this will generate negative feelings from the staff and they are worried this might have negative repercussions on the patient in their absence. However, when communication is good, most caregivers feel reassured and relieved, and it gives them confidence in the healthcare team.
Many caregivers would also like to communicate with staff to share their knowledge of the patient and contribute to the care with their expertise. However, they feel that their input is often disregarded and that the staff learn from their own mistakes and experiences with the patient, instead of being guided by the caregivers. Also, several caregivers observe a lack of communication, and sometimes even conflicts, between staff members. They are worried this may affect the quality of care and the information transmitted from one to another. They would appreciate it if the staff developed trust and confidence among all parties, as a team with a common goal should do: “The reality is that they don’t listen to us, and they listen even less to the patient!”. Some caregivers highlight problems with communication between staff and patients, such as disrespectful interactions with patients, as well as a lack of dignity and interest manifested by the healthcare team: The other thing I want to say about disorders … about people with cognitive disorders. When the nurse comes or the attendant talks in front of… I’ll call him x, my husband. They talk in front of x as if he wasn’t there.
Solutions
To improve communication, caregivers suggest that the healthcare team could identify a reference person who has regular contact with the patient within the CHSLD to relay pertinent information to the caregiver. Some suggest that the beneficiary attendant acts as the resource person and be given more access to sensitive information, such as the patient’s file. Others suggest appointing a case manager: A hub… someone…a case manager. Why doesn’t it exist in this system someone who’d make links between hospitals, institutions and even in-house. The case manager can have many patients. And it’s that person who organizes the team meetings, and these matters. I think it would be very helpful for us. To me, it would be helpful to have someone who knows about that.
They recommend that the CHSLD team ensure a systematic pathway to share information with caregivers about the patient’s daily life (e.g., information about care, diet, mobility, sleep, changes in condition, BPSD, or medication) and that both should agree on the best way to communicate: When you bring your child to daycare… you want to know how the day went. They will tell you. Why is it we can’t get this information here ? I don’t understand. I feel like I don’t actually hear about much, unless it’s going badly. I don’t know if there’s any way to systematize a follow-up for us, you know in the routine. I don’t know, we meet once a month.
For caregivers, staff stability is also a solution to improve communication. They suggest that establishing regular staff stability would decrease the loss of information and facilitate communication as the caregivers and staff would better know each other.
Need to Define the Role of the Caregiver in Partnership With the Healthcare Team
Most caregivers would appreciate it if their role was better defined when the patient moved to a CHSLD. They want to ensure they can act as a real partner of care within the CHSLD healthcare team: “It took several months before we met a doctor, before we knew… you know, what are the expectations? You know, because basically it would be nice to know “okay, we expect this from the family or the caregivers.””
Because of gaps in care, several caregivers feel the need to take on a lot of responsibilities in the CHSLD: providing primary care, managing and finding proactive solutions for BPSD, monitoring medication, and even helping staff with other patients. Some want to relieve the team, overwhelmed by a lack of staff members: We are there to do certain things too. They have to see us as an asset. Say, ‘We’re going to work as a team.’ If the families are involved, it’s just better for them, the staff. So, to see that as positive. And that we’re going to work together. We’re going to have the same vision. And we’re going to be equal. And not, ‘Oh no, she [the caregiver] is going to come and bother us.’; ‘Oh no, we don’t have time to talk about it.’ No, we’ll take a few minutes, not hours. We know all that very well!
However, compensating for and supporting the staff often leads to stress and exhaustion, but many caregivers are more satisfied with the living conditions of the patient. While some caregivers think the healthcare team appreciates their help, others feel their input is unwanted and unwelcome. That being said, ultimately, the majority would rather spend quality time with their loved ones than have to spend their energy advocating and compensating for better care.
Solutions
Caregivers want to know what is expected of them by the staff. They also would like to be more involved and consulted with respect to their role in the patient’s care and respected as legal representatives: There is only one thing in life… By speaking to one another we can understand one another. And if it’s difficult, then they have to explain it to us. And we will explain to them the story of our husband, our parent, with pleasure.
Need for Respite for the Caregiver
Many caregivers want some rest and relief from their responsibilities to be able to attend to their other obligations, to save their energy and be able to care for themselves.
These responsibilities may impact their quality of life as they continue to invest heavily in the care of the patients at the cost of their leisure time, other relationships, and work: I’m in a new relationship with someone. And to be able to share time with my new relationship and to go take care of my mother, that annoys me. I say to myself, ‘Well, look, I’ll go during the week instead of on Sunday. But I’m also bothered by the fact that I usually go on Sundays, before she has lunch, I make her listen to her music’.
These responsibilities come with a significant emotional toll, such as exhaustion, guilt, helplessness, shame, worry, irritability, anger, sadness, and ambiguous loss, which greatly affects their mental health. Some need to go on sick leave or premature retirement. Others even say these difficulties have led to depression, needing medication or seeing a psychologist. Many say they have a savior temperament that contributes to their outstanding commitment: “You don’t let down someone that you loved all your life.” They often feel very isolated in their role, and misunderstood. Consequently, some lose their support network: “I have no one to talk to. Not even him [the patient] because he can’t hear me. I find it hard.” Those who do have support say this lightens the workload and reduces exhaustion. They express that their energy is modulated by the kindness and human approach of the staff.
Solutions
Caregivers wish CHSLDs would implement efficient strategies to improve the quality of care, thus diminishing their need for respite. Many feel that they would not be exhausted if the care focused more on primary needs of the patients. They also suggest facilitating the access to support resources by making their contact details more readily available. They believe talking to support groups or having access to a helpline could be beneficial.
Discussion
This study explored the experiences, needs, and solutions of caregivers of patients with MNCD and BPSD living in a CHSLD. As demonstrated in previous studies (Centre de recherche et d’expertise en gérontologie sociale du CIUSSS du Centre-Ouest-de-l’Ile-de-Montréal, 2020; Gaugler, 2005), our study showed that caregivers remain involved in the care of their loved one even after placement in long-term residential facilities. We found that caregivers’ needs are not well understood by healthcare professionals during and after this transition. This study highlights that CHSLD teams, including beneficiary attendants, nurses, and physicians, could benefit from stepping back from a position of expertise and being open to consider an active role for caregivers in CHSLD.
Significant shortcomings in the administration and quality of basic care were raised, consistent with reports from media and different organizations (Archambault, 2017; FADOQ, 2017; Protecteur du citoyen du Québec, 2019) regarding the situation in CHSLDs in Quebec. This problem is unfortunately no different in the United States and Europe (Scientific American, 2021; Spasova et al., 2018). Similar concerns were raised during the pandemic, questioning whether the problems in care were due to that unprecedented context or whether the pandemic was simply exposing the ongoing problem in an acute manner (Protecteur du citoyen du Québec, 2020a).
Even though caregivers made numerous suggestions that could be implemented to improve BPSD management, the scope of the results was compelling because they addressed much broader issues than help regarding BPSD, which was our initial hypothesis. Caregivers expressed themselves on six main areas that must be translated into objectives for healthcare teams and administrators: 1. Aiming for a smoother transition to the CHSLD; 2. Implementing basic training on knowledge of BPSD for caregivers; 3. Fostering a human and evidence-based approach to BPSD by members of the healthcare team; 4. Improving communication with caregivers; 5. Defining the role of the caregiver in the CHSLD proactively; 6. Promoting practices that reduce the need for respite for caregivers.
This study shed light on precise needs that are not easily expressed by caregivers while they are busy with their evolving role and adapting to a new environment. We also heard how complex it is with active BPSD, with these patients needing more clinical attention and adapted care. Previous authors emphasized that the transition in a long-term care facility is an emotionally charged step for caregivers (Crawford et al., 2015; Fitzpatrick & Tzouvara, 2019; Gaugler et al., 2009; Graneheim et al., 2014; Pritty et al., 2020). Our findings highlighted that the first impression and the uncertainty of what is coming next may impact what caregivers are going through and the communication and their relationships with healthcare professionals in the following months, which was described similarly in the literature (Barken & Lowndes, 2018). Because caregivers report that patients often move numerous times within a short period, staff should ensure a thorough handover to the next team.
As reported by previous researchers, caregivers clearly expressed that partnership of care is crucial to value caregivers’ expertise and share the responsibilities between caregivers and healthcare staff (Davies & Nolan, 2003; Ryan & McKenna, 2015; Tible et al., 2017). They referred to the small attentions to the patients that were coherent with their biographical history and made to preserve their dignity. We also found that caregivers could lose their confidence that CHSLD facilities can look after patients because they observed that patients’ individualities are sometimes ignored, with basic needs unmet. Caregivers were significantly distressed by the lack of personalized care. On that matter, with their theory of “becoming a person again,” Hunter and colleagues (2016) provided an understanding on how we can offer person-centered care with psychosocial interventions, notably by maintaining personhood in both patients with dementia and staff in long-term care.
Moreover, participants reported many examples of institutional neglect and decried the serial moving of patients, resulting in clinical deterioration. Therefore, caregivers ask more specifically to increase the capacity for units with a specialized approach to BPSD, including Special Care Units. Following the transitions theory of Meleis (2019), we see here a transition in the role of caregiver which seems to be perceived differently by the care team. This one sees the caregiver as a loved one who is freed from a burden, when in fact the caregiver would rather need to move from the role of the sole caregiver of the person living with BPSD to the one of a “caregiver partner.” This observation is important for health professionals who want to better collaborate and better support caregivers in this context. Given the emotional charge of the topics addressed by the participants, we found that many caregivers were reluctant to communicate their observations, needs, and solutions and this study is a strong voice for them.
Caregivers and CHSLD staff would benefit from regular advice and training about the preferred non-pharmacological approaches for BPSD (Tible et al., 2017). For instance, the PIECES model is well-recognized and accessible to better understand the contributing factors and triggers for BPSD (Hamilton et al., 2020). In our study, caregivers described disparities in the approach to BPSD by the CHSLD staff, as the Protecteur du Citoyen recommended to offer them training to better meet patients’ needs (Protecteur du citoyen du Québec, 2020b). Caregivers also emphasized that maintenance of a non-pharmacological intervention plan should also be put forward, with a leader promoting its application and adjustment over time. This leader, either a beneficiary attendant, a nurse, a social worker, or a case manager, could also take the responsibility of communicating regularly with caregivers, often also the patient’s representative.
Even if we cannot cure patients with MNCD and BPSD, caregivers remind us that we can accompany them and the patient with dignity, by being available and listening to the needs of all parties. Because caring for patients with BPSD is difficult, trust, openness, and honesty are invaluable in this overwhelming context. Better communication on a patient’s progress and prognosis could also be profitable to set realistic objectives in care, reframing the expectations of the healthcare team and caregivers in a manner that respects the patient and is coherent with the stage of the disease. Previous authors also suggested that better support to caregivers could help to address their expectations in the long-term care setting and prepare for end-of-life care and bereavement (Barken & Lowndes, 2018; Lewis, 2014). Exploring the type of caregivers we are working with as a healthcare team could be beneficial, described as adapters, strugglers, and case managers profiles by Davies and colleagues (2014). In our study, the healthcare worker’s perspective was not directly taken into account, and this would certainly be interesting to bring other solutions. Nevertheless, caregivers were clear that they were realistic about work overload and truly wanted to help.
Regarding the limitations of our findings, we underline that data collection was done by focus groups interviews, which may induce a social-desirability bias. This is also true with some participants who had one of the researchers as a geriatric psychiatrist who had cared for their loved one. However, many strategies were used to minimize bias. These participants were advised at the beginning that the study was led by this physician. Also, at the time of the focus group interviews, all medical follow-ups involving the caregivers' relative were over, so research would not influence ongoing care. Finally, the physician was not given a primary role in the single focus group interview in which she took part, mostly taking notes and facilitating expression. Another researcher was given the responsibility to lead and ask the questions to minimize bias during the interactions.
We were aware that data analysis in qualitative research can lead to personal biases. To minimize these biases, we used an open “reflexive journal,” and field notes and each focus group interview transcript were analyzed by two different research members with discussions to reach consensus. The interview guide evolved with the preliminary data analysis to a second version as suggested in qualitative research to further explore the preliminary data. Finally, the preliminary results were presented to the last focus group to collect their comments and ideas about the answers obtained from previous focus groups interviews. They validated that the preliminary results represented well their reality and experience.
In addition, only caregivers that were able to make themselves available and with a desire to share their experience participated in the project. These were therefore more often participants who were very greatly involved or who had a more meaningful experience that they wanted to share. Next, the interviews were conducted in a CHSLD; although the participants were assured of confidentiality, it is possible that the choice of setting had an inhibiting effect on them, for fear that the healthcare staff would be aware of the information they shared.
Nonetheless, one of this study’s strengths was the focus on the specific needs of caregivers of patients with MNCD and BPSD living in CHSLDs. To our knowledge, it is the first study to address this specific issue. The researchers used a constructive approach that allowed the participants to describe both positive and negative aspects of their reality, but also to suggest solutions. As a result of this methodology, the solutions provided by caregivers are concrete, applicable, and based on their experience. Furthermore, the participants are from different CHSLDs with generalizable results. This study gives invaluable insight for healthcare providers, CHSLD executive boards, and politicians to improve care and prevent caregivers’ distress and burden. Because the study was completed before the COVID-19 pandemic, some answers could be different due to the lockdowns, new restrictions, rapidly changing rules, and other ways to communicate (Protecteur du citoyen du Québec, 2020b). However, we think the results are still accurate and that the solutions suggested by the participants could have helped during the COVID-19 crisis in CHSLDs. With all the mediatization of CHSLD setbacks, we must also consider that repeating this study after the beginning of the pandemic could have brought more explicit expression of needs and solutions.
Conclusion
In conclusion, this study brought a new perspective for the management of BPSD for patients living in CHSLDs. Caregivers can be allies to the medical and nursing team in CHSLDs. Instead of needing educational tools about BPSD management, as we primarily thought, caregivers named that reducing stress for healthcare professionals, caregivers, and patients is a priority for a better management of BPSD in CHSLDs. They remind us that placement is worrying and CHSLDs are often described as undesirable environments to live in. Even though restructuring CHSLDs to increase staff capacity and improve stability for patients can appear a daunting task, caregivers have suggested numerous solutions. Further research could focus on the impact of these solutions on BPSD (e.g., holistic transition to CHSLDs or communication skills training for healthcare professionals in this specific setting and population).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.