
Abstract
There is an urgent need to generate deeper understandings of how suicidality manifests and evolves during pregnancy and the following year. Several perinatal studies have examined the incidence of suicidal thoughts and behaviours and associated social and obstetric risk factors; however, there is very limited research offering insights into women’s experiences of suicidality at this time in their lives. This study aimed to generate a theory to explain how suicidality evolves in the perinatal period. A grounded theory design was used with data generated using anonymous online surveys (119 participants) and in-depth interviews (20 participants) with women who received pregnancy care in the past 5 years in Australia. The developed theory holds shame as a core concept. Origins and contexts of shame reflect current epidemiological understandings of risk for perinatal suicide, including experiences of gender-based violence, adverse childhood experiences, and a history of mental health difficulties. When women feel that they are defective, are unworthy of love and belonging, and do not possess what it takes to be a good mother, they can conclude that their family is better off without them. Pathways beyond shame were facilitated by compassionate and rehumanising care from family, friends, and care providers. Findings demonstrate that perinatal suicidality is a complex multidimensional phenomenon, influenced by socio-cultural expectations of motherhood and interpersonal, systemic, and intergenerational experiences of trauma. Increasing the prominence of perinatal suicide prevention within health professional education and practice, and addressing systemic barriers to compassionate health care are critical first steps to addressing perinatal suicide.
Keywords
Introduction
There is an urgent need to address limitations in our understanding of maternal suicide. Although most women are in frequent contact with health professionals during pregnancy and the early years of their children’s lives, suicide is a leading cause of maternal death in Australia and other high-income countries (Australian Institute of Health and Welfare, 2021a; Knight et al., 2021; Meurk et al., 2021). Both Australian and international literature has identified unique characteristics of suicide at this time in women’s lives. For example, women appear more likely to use violent means of suicide in the perinatal period (Khalifeh et al., 2016; Knight et al., 2021; Meurk et al., 2021; Modini et al., 2021), generally considered uncharacteristic of female suicide. However, there are stark gaps in our knowledge about underlying causes of perinatal suicide.
Existing literature identifies several risk factors for maternal suicide, including exposure to intimate partner violence and a history of mental health disorder (Giallo et al., 2018; Orsolini et al., 2016). Several perinatal studies have examined the incidence of suicidal thoughts and behaviours and associated social and obstetric risk factors (Giallo et al., 2018; Orsolini et al., 2016; Palladino et al., 2020); however, there is very limited research offering insights into women’s experiences of suicidality at this time in their lives.
Available qualitative research has produced descriptions of symptoms, help-seeking, or approaches to coping (Praetorius et al., 2020; Tabb et al., 2013), some of which are limited by exclusive focus on the experience of suicidality in the context of postnatal depression (Praetorius et al., 2020). A recently published grounded theory study which sought to understand what makes perinatal women suicidal offers some theoretical insights; however, these are limited by a number of factors (Reid et al., 2022). Firstly, broad conclusions were drawn from the relatively small number of women who participated in the study. Of these, all but one participant reported suicidality in the context of a first pregnancy or postnatal period, with women who had experienced suicidality following miscarriage, termination, or stillbirth excluded from participating.
This literature has so far failed to deliver an adequate understanding of how recognised risk factors for suicide influence experiences in the perinatal period. There is an urgent need to generate deeper understandings of how suicidality manifests and evolves during pregnancy and the following year, and how these recognised risk factors operate within women’s lives and within health care interactions. The importance of addressing this gap in our knowledge is echoed by broader calls to ensure mental health practices are informed by qualitative research (Braun & Clarke, 2019; Galasiński, 2021).
Drawing on anonymous online surveys and interviews with women who experienced perinatal suicidality, the aim of this qualitative study was to generate a theory to explain how suicidality evolves during pregnancy and the following year. Our overall goal was to produce knowledge to support communities, health professionals, and health services and systems to improve perinatal suicide prevention initiatives. More broadly, we also aspired to bring attention to perinatal suicide prevention as a core responsibility of quality maternity care.
Study Design
Methodology
This study employed grounded theory methodology, adopting the methods proposed by Birks and Mills (2023). Grounded theory is particularly useful when very little is known about a topic of inquiry. First described by Glaser and Strauss (1967), the methodology utilises an inductive process to generate a theory grounded in data. Used within a qualitative paradigm, grounded theory facilitates the construction of meaning with participants, allowing their experiences to drive the analytical processes. The research team assumed a constructivist position (Birks & Mills, 2023; Charmaz, 2014, 2017), and the study was informed by critical traditions, including feminist and trauma-informed critical commentary on the over-medicalisation of human experience, distress, and suicide (Bentall, 1992; Herman, 1992; Miller & Striver, 1997). Professional and personal experiences within the research team were proactively utilised, including mental health professional (authors 2–7), mental health peer support volunteer (authors 1, 3, and 4), midwifery (author 1), and nursing (author 8) expertise, along with personal experiences of perinatal distress (authors 2–4) and loss of a mother to perinatal suicide (author 2). The research team undertook a whole-day training together prior to the commencement of recruitment led by authors 1 and 8, focusing on grounded theory methodology, methodological rigour and reflexivity, and study protocols.
Data Generation
Following approval by the Royal Children's Hospital Human Research Ethics Committee (HREC 61635), data were generated via anonymous online testimonials (surveys) and in-depth telephone and video interviews. Women 18 years or older at the time of recruitment who had been pregnant in the preceding 5 years in Australia, who had experienced thoughts of suicide in pregnancy and/or the year following, irrespective of pregnancy outcome, were eligible to participate.
Recruitment occurred via social media in two rounds. Potential participants were invited to complete the survey (first round of recruitment) or register their interest in an interview (second round of recruitment). Information sheets were provided. Survey submission was considered consent to participate, and interview consent was obtained via REDCap (Harris et al., 2009, 2019). Qualitative surveys have the potential to generate rich and complex accounts of participant’s experiences (Braun et al., 2021). Used successfully in past grounded theory research (Birks & Mills, 2023; Chun Tie et al., 2019), surveys offered women an opportunity to share their experiences of perinatal suicidality anonymously, an important consideration when researching sensitive topics like perinatal mental health and where women may hold concerns regarding the involvement of child protection services. The survey consisted of eligibility questions, and five broad questions encouraging women to narrate their experiences of perinatal suicidality (supplementary file), including what they thought contributed to how they were feeling, and experiences of seeking mental health support. Basic demographic data were also collected.
Interviews were conducted by mental health professionals working on the PANDA National Perinatal Mental Health Helpline. Interviewers were provided training in undertaking research interviews and were professionally prepared to respond to distress in participants should it occur. Interviews commenced with the question ‘what would you like to share about your experiences of suicidality during pregnancy and/or the following year?’. Consistent with theoretical sampling techniques characteristic of grounded theory, follow-up questions were designed to inform the developing theory.
There were no incidents of participant distress during the study period that required crisis assessment and management or referral, although processes were established prior to recruitment to facilitate this if necessary. Participant safety processes were modelled on PANDAs existing helpline practices as an accredited national mental health service, and options for 24/7 support were reinforced throughout for survey and interview participants. Safety of the research team was also a priority; a number of strategies were implemented to support researcher welfare, including reflective supervision practices and a researcher wellbeing plan.
Analysis
Data were generated in two rounds; survey data was used to generate a draft theory (June–September 2020), which was then further developed and tested during interviews (November 2020–January 2021). The principal researcher (author 1) led the analysis, writing memos throughout – a reflective process which interrogated and accounted for the role of the researcher in the analytical process, including the researcher’s history and pre-conceived ideas. The entire dataset of interview transcripts, surveys, field notes recorded by interviewers, and memos was uploaded to NVivo (QRS International Pty Ltd, 2020) to facilitate analysis. Grounded theory adopts an iterative and increasingly abstract process of data generation and analysis (Birks & Mills, 2023): 1. Initial coding: labels applied to segments of data that reflect concepts relevant to the research question; categories start to form. 2. Intermediate coding: categories elaborated and relationships between concepts identified; a core category, or process, begins to develop. 3. Advanced coding: integration of theory through the development of a storyline and use of theoretical codes.
Regular meetings were held between the principal researcher and members of the team undertaking data generation. These meetings sought to support researcher wellbeing, seek iterative feedback on all stages of data analysis, and capitalise on opportunities for theoretical sampling (lines of enquiry) in future interviews.
Findings
Participants
Participant Characteristics. a
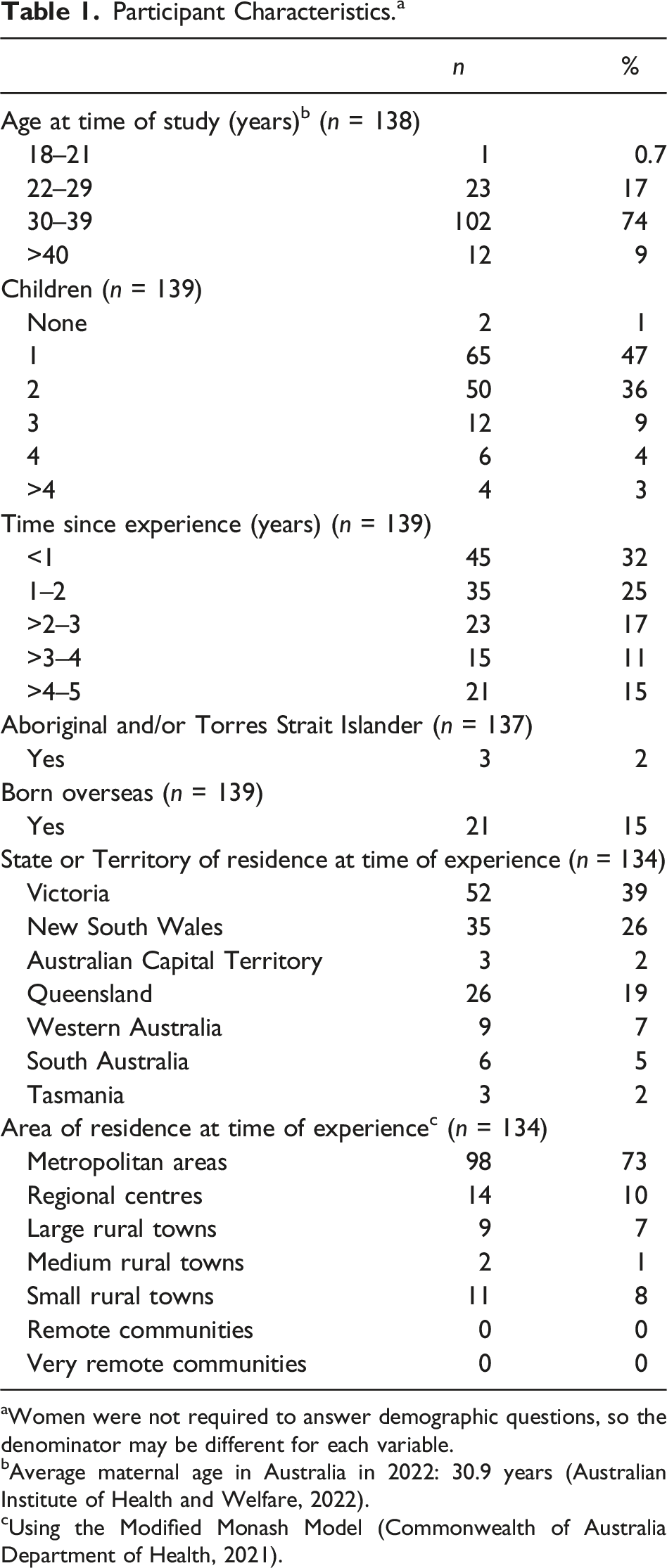
aWomen were not required to answer demographic questions, so the denominator may be different for each variable.
bAverage maternal age in Australia in 2022: 30.9 years (Australian Institute of Health and Welfare, 2022).
cUsing the Modified Monash Model (Commonwealth of Australia Department of Health, 2021).
Participants’ reported diverse mental health experiences. Some women had long-standing mental health challenges before pregnancy, while others considered their mental health to be very good prior to their experience of perinatal suicidality. A number of women had attempted suicide during their lives, both during and outside the perinatal period. As grounded theory strives to generate a theory which is grounded in the data, we were sensitive to different or unique pathways women with diverse experiences of mental health may describe relative to perinatal suicidality. However, it became clear during analysis that regardless of specific mental health context or whether someone had been provided with a formal mental health diagnosis (or what that diagnosis was), there was a striking, core human experience within women’s stories of perinatal suicidality.
The Theory: Pathway Through Shame
Birks and Mills propose the use of storyline as both an analytical tool and a mechanism for articulating the final theory (2023). Findings are therefore presented in the form of a storyline. It is not necessary for raw data to be provided when presenting theory in storyline (Birks et al., 2009; Birks & Mills, 2023; Strauss, 1987); however, participant quotations have been provided in a supplementary file to support individual reader preference.
Although not all elements of the theory describe specific aspects of every woman’s experience of perinatal suicidality, it is an abstract explanation of this process, as described by those who participated in this study. This process is presented as Figure 1 and unpacked in the dialogue that follows. An additional pictorial diagram that was generated following theory completion to support dissemination and implementation of study findings with diverse academic and non-academic audiences is available as a supplementary file. Pathway through shame.
The developed theory contains three components: shame talk (capturing the way women express themselves relating to their perinatal experiences); contexts of shame (reflecting the contexts in which women experience shame or exacerbate feelings of shame); and pathway through shame (the core pathway that characterises the process of perinatal suicidality). These processes all hold shame as a core concept. Our definition of shame is based on Brown’s Shame Resilience Theory: an intensely painful feeling or experience of believing that we are defective and have failed, and are therefore unworthy of love and belonging (Brown, 2006). This clear understanding of what shame is (and therefore is not) was instrumental in the eventual identification of shame and its influence as the core category in this theory.
Origins of Shame
Many participants shared common origins of shame, including adverse childhood experiences such as abuse or neglect, gender-based violence, and intergenerational trauma. Women often reported a range of compounding difficult or traumatic experiences. These experiences, often occurring early in women’s lives, changed the way they viewed themselves and the world. We understand the adaptations women made to help them cope with these experiences as normal responses developed within very challenging contexts that, if not modified, understandably present difficulties within the context of pregnancy and the transition to parenthood.
Violated Expectations
Women’s experiences of pregnancy and early parenthood, including their experiences of health care at this time, violated their expectations of themselves as mothers and humans. They expressed this as feeling like abject failures; that their bodies had failed them, and that they had in turn failed their children and families. This pathway of shame is influenced by the context of socio-cultural constructs of motherhood and complex pregnancy experiences, such as perinatal loss, hyperemesis, or premature birth. Harmful socio-cultural constructs and expectations of motherhood could be promoted and upheld by health professionals and friends and family. For example, women may have negative or traumatic experiences of labour and birth dismissed as they had a healthy baby; the role of the ‘good’ mother was to sacrifice herself for the sake of her children. Experiences of disrespectful or de-humanising care, a sense of having failed at pregnancy and birth, breastfeeding, or early parenting, could all be experienced (felt) as clear evidence that they were in fact defective mothers.
Disappearing Self
A pregnancy, new baby, and/or loss of a job/career heralded the disappearing of self (identity). This loss of self was also influenced by the way women felt they needed to parent in order to be a ‘good’ mother; for example, feeling that they needed to be able to keep their toddler happy while also preventing their newborn from crying. Women reflected that there was no longer space for ‘self’ distinct from ‘mother’. These feelings can be exacerbated by sleep deprivation and the physical toll of pregnancy and early parenthood, as well as care providers and systems, friends, and family who enquire about or prioritise the baby’s wellbeing without showing the same care for the woman beyond her role in growing, birthing, and feeding her baby. This loss of self was perceived as permanent; they did not hold hope that the ‘self’ would return.
Psychological Isolation
Different from being physically alone, psychological isolation is a deep feeling of being disconnected and apart (Miller & Striver, 1997). This relates strongly to, and may be considered an outcome of, shame; the knowledge that your defectiveness means you are not worthy or able to experience love, safety, and belonging, and that the love you have to offer your family is not worth a lot. As this shame (defectiveness) is sensed as permanent, feeling alone and disconnected is also understood as permanent – leading to desperation and intolerable feelings of being trapped and needing to escape. Current exposure to intimate partner violence, characterised by coercion and control, can create further urgency for escape.
The Only Option
This concept represents the ‘logical’ equation women shared. If you ‘know’ (feel at the time) you are defective, are unworthy of love and belonging, and do not possess (and will not possess) what it takes to be a good mother, your family is therefore better off without you. This ‘logical’ understanding of the situation led women to feel that the only option available to them, and the one that best expressed their love and care for their family, was to die by suicide.
Re-defining the Good Mother and Re-imagining Self
Stories of the pathway beyond shame commonly featured experiences of compassionate rehumanising care from friends or family, or mental health, primary, and perinatal professionals. These experiences of connection and safety demonstrated to women their worth as people, and that they were in fact deserving of love and belonging. Over time, this supported women to re-define what a good mother was to them, and to re-imagine self. The process of re-defining the good mother commonly included dismantling socio-cultural expectations of motherhood and defining the kind of parent they wanted to be for themselves. In direct opposition to the disappearing self, women can re-gain and re-imagine self as well as/distinct from mother, which could include a return to work or study. Within compassionate and safe relationships, women were able to generate more flexible understandings of the kind of mother they wanted to be (and person more broadly); they were able to feel that they were ‘enough’ – for their children, families, and themselves. Women were able to feel that their families were better off with them.
Discussion
Early in the analysis process, shame was identified as a central element of perinatal suicidality. The use of a theoretical code in grounded theory is not determined prior to analysis, but driven by the developing theory (Glaser, 1978) which is grounded in the data itself. In our case, Brown’s Shame Resilience Theory (SRT) was used as a theoretical code to understand pathways through shame, add explanatory power, and further develop Brown’s theory in the process. The SRT is a grounded theory generated through interviews with 215 women which sought to explain why and how women experience shame, how shame impacts women, and the processes and strategies they utilise to address concerns regarding the impact and consequences of shame. The following discussion is structured using the SRT as a theoretical code to position our work in the context of this earlier theory and other literature.
What, Who, and How to Be
The SRT presents the idea of a ‘shame web’; ‘participants most often experienced shame as a web of layered, conflicting, and competing expectations that are, at the core, products of rigid socio-cultural expectations’ (Brown, 2006). The web encompasses expectations regarding who, what, and how women are expected to be based on factors such as class, age, sexuality, and roles such as ‘mother’. Expressed by individuals and upheld by media (Brown, 2006), rigid expectations regarding what, who, and how women are meant to be as mothers are evident in our theory. The potentially harmful impacts of our socio-cultural constructions of ‘the good mother’ have been established (Brown, 2006; Brown et al., 1994; Sonnenburg & Miller, 2021; Staneva et al., 2015), although rarely applied within the context of perinatal suicide (Praetorius et al., 2020; Reid et al., 2022).
Women expressed feeling like profound failures and ultimately defective mothers when they were unable to live up to these expectations. Shame is understood to be activated not solely when there is a sense of failure, but when the person feels that they are close to an ‘undesired self’ (Ogilvie, 1987) or ‘unwanted identity’ (Brown, 2006). In this way, women experienced intense shame not simply because they felt they were failing as a mother but because they felt they were ‘defective’ mothers (the undesired self). This understanding of an undesired self as it relates to perinatal suicide is unique.
Whether to Be
The SRT does not extend to the relationship between shame and suicide. In addition to questions of who, what, and how to be, women in our study grappled with the question of ‘whether to be’.
The origins and contexts of shame identified in this theory reflect current epidemiological understandings of risk for perinatal suicide, including experiences of gender-based violence, adverse early childhood experiences, challenging perinatal experiences, and a history of mental health difficulties (Giallo et al., 2018; Khalifeh et al., 2016; Meurk et al., 2021; Modini et al., 2021; Orsolini et al., 2016; Palladino et al., 2020). Concerns regarding escalating rates of poor mental health, including self-harm behaviours, among young girls and women add further urgency to our efforts to understand and prevent perinatal suicide (Australian Institute of Health and Welfare, 2021b). Our theory provides novel insights into the ways these factors inform women’s ‘internal worlds’ and decision-making in the perinatal period.
As complex multifactorial and social processes, it is important to understand shame and suicide in the contexts in which they manifest and evolve. The relationship between shame and suicide has been identified in non-perinatal contexts (Bryant & Garnham, 2015; Cover, 2012; Taylor, 2020) and is included as a relevant though not central concept in a recently published perinatal study (Reid et al., 2022). Shame however does not feature prominently in the widely adopted Interpersonal Theory of Suicide (IPTS) (Van Orden et al., 2010). We do not consider the experience of perinatal suicidality to be sufficiently captured by the concepts of perceived burdensomeness or thwarted belonging offered by the IPTS, and support the assertion that the theory’s lack of sensitivity to individual social, political, cultural, and structural circumstances and contexts significantly diminishes its explanatory power (Hjelmeland & Knizek, 2021; Hjelmeland & Loa Knizek, 2020). The understanding of shame offered by our theory, including psychological isolation as a central feature of perinatal suicidality, is unique and has important practice implications.
Although diverse suicide behaviours were reported by participants, our analysis was not able to generate clear theoretical explanations for why some women progress to suicide behaviours and others do not. Factors which could be perceived as protective against suicide behaviours in some contexts could later and quite suddenly be understood by women as contributing to suicide behaviours, such as their profound love and care for their child/ren and families. Women who shared experiences of suicide behaviours reflected that in those moments, they were no longer able to endure; however, there was no clear pattern or process identified to explain this loss of capacity to go on. As a result, while other authors have attempted to draw conclusions about suicidal action based on minimal data (Reid et al., 2022), we felt that it was not appropriate to do so in spite of our significantly larger dataset.
The Pathway Beyond Shame – Implications for Compassionate Care
Experiences of compassion were central to pathways beyond shame and perinatal suicidality. A similar process was identified in a study with women seeking help for suicidality in the context of intimate partner violence (Taylor, 2020). Women described hunting to feel human, ‘fighting for a sense of belonging and personal value by perceiving validation from health care providers’ (Taylor, 2020). The SRT supports this process; women seek connection in order to develop shame resilience, with connection allowing women to move away from socio-cultural ‘trappings’ of the shame web to experience empathy (understood in Brown’s theory as the experience opposite to shame) (Brown, 2006).
Gilbert’s contributions to the compassion literature help to explain this process. Adopting principles of courage, empathy, and ethics as a foundation, he defines compassion as ‘a sensitivity to suffering in self and others with a commitment to try to alleviate and prevent it’ (Gilbert, 2017). While shame encourages disengagement and disconnection (as seen in the common origins of shame and experiences of psychological isolation in our theory), compassion fosters integration, reconnection, and support. Qualities such as validation, connection, and kindness function as an antidote to shame (Gilbert, 2017), reflected in our participants’ experiences of feeling seen and valued, often by care providers who demonstrated these values in their practice. Gilbert proposes that compassion is enacted in health practice in two ways: ‘the ability to be sensitive and engage with suffering, to turn toward rather than away from it, […] and the preparedness and dedication to acquire the wisdom to work out what best to do’ (Gilbert, 2017).
Experiences of de-humanising and disrespectful health care were common amongst participants; they functioned as powerful reminders of their (perceived) worthlessness and created profound barriers to women accessing the care and support they needed. Fragmented, under resourced, and stressed health systems foster compassion fatigue and burnout in providers, contributing to disconnection, poor quality, and in some cases traumatic experiences of care for women and families (Lokugamage & Pathberiya, 2017; Rydon-Grange, 2018). The stories shared with us demonstrate that compassionate care which seeks to foster connection and safety while remaining sensitive and responsive to common origins and contexts of shame is crucial to perinatal suicide prevention. Increasing the prominence of perinatal suicide prevention within health professional education and clinical practice guidance, including the central roles of shame and compassion, and addressing systemic barriers which make it difficult for providers to practice with compassion (Rydon-Grange, 2018), are critical first steps to addressing perinatal suicide.
Strengths and Limitations
This is one of the first qualitative studies to explore perinatal suicidality. Offering both in-depth (interview) and anonymous (survey) ways of engaging with the study allowed women to participate in ways that felt safe for them. The research team encompassed important personal and professional expertise relevant to the topic, allowing us to adopt both insider and outsider perspectives. By utilising grounded theory as our methodology, we have generated explanatory understandings that would not have been possible with more descriptive approaches.
As a social process, shame is highly sensitive to contexts, including culture (Gilbert, 2007). Although our sample could be considered large for a qualitative study and included significant diversity of perinatal and mental health experiences, there are some important contexts our theory may not adequately reflect. Maternal death encompasses deaths occurring during pregnancy and the following 365 days regardless of pregnancy outcome; therefore, we did not limit participation based on specific pregnancy outcomes. However, only two participants did not identify as having children. As both participated via survey, we were not able to establish an in-depth understanding of their experiences as may have been possible in an interview context. As such, our theory may not adequately capture how women who do not identify as having children experience shame and suicidality, for example, following miscarriage or termination. Diverse pregnancy experiences and outcomes (planned and unplanned pregnancy, termination, miscarriage, stillbirth, and neonatal death) were all otherwise represented in our sample, and it is therefore likely that our theory reflects the way shame is experienced in these contexts. Our study specifically sought to engage women with experiences of perinatal suicidality and therefore will not necessarily reflect experiences of non-binary or transgender people. Similarly, our study was not specifically designed to reach Aboriginal and Torres Strait Islander women or women of refugee backgrounds; undertaking research about perinatal suicidality with these important communities would likely require a different approach with a focus on co-design and culturally safe, community-led methods. Finally, this study was not able to include experiences of women who have died by suicide; these women may have differences in their experiences of shame and perinatal suicidality.
Conclusion
This study addresses urgent calls for us to expand our understanding of maternal suicide. We have identified that the evolution of perinatal suicidality is driven by experiences of shame and feelings of disconnection and defectiveness. Pathways beyond shame and perinatal suicidality can be facilitated by compassionate and rehumanising relationships and care experiences that enable women to feel worthy, deserving of love and belonging, and that their families are better off with them. Despite the clear importance of compassion in perinatal suicide prevention, health professionals and systems face numerous barriers to providing compassionate care. Improved identification and response to common origins and contexts of shame and removing interpersonal and systemic barriers to compassionate care are critical first steps to addressing perinatal suicide.
Supplemental Material
Supplemental Material - Pathways, Contexts, and Voices of Shame and Compassion: A Grounded Theory of the Evolution of Perinatal Suicidality
Supplemental Material for Pathways, Contexts, and Voices of Shame and Compassion: A Grounded Theory of the Evolution of Perinatal Suicidality by Laura J. Biggs, Bonnie Jephcott, Kim Vanderwiel, Imogen Melgaard, Shannon Bott, Mitzi Paderes, Julie Borninkhof, and Melanie Birks in Qualitative Health Research
Supplemental Material
Supplemental Material - Pathways, Contexts, and Voices of Shame and Compassion: A Grounded Theory of the Evolution of Perinatal Suicidality
Supplemental Material for Pathways, Contexts, and Voices of Shame and Compassion: A Grounded Theory of the Evolution of Perinatal Suicidality by Laura J. Biggs, Bonnie Jephcott, Kim Vanderwiel, Imogen Melgaard, Shannon Bott, Mitzi Paderes, Julie Borninkhof, and Melanie Birks in Qualitative Health Research
Supplemental Material
Supplemental Material - Pathways, Contexts, and Voices of Shame and Compassion: A Grounded Theory of the Evolution of Perinatal Suicidality
Supplemental Material for Pathways, Contexts, and Voices of Shame and Compassion: A Grounded Theory of the Evolution of Perinatal Suicidality by Laura J. Biggs, Bonnie Jephcott, Kim Vanderwiel, Imogen Melgaard, Shannon Bott, Mitzi Paderes, Julie Borninkhof, and Melanie Birks in Qualitative Health Research
Footnotes
Acknowledgements
We would like to sincerely thank the women who generously shared their stories with us, without whom this study would not have been possible. Thank you, Christielee Plumridge, for sharing your experiences, passions, and humour with us as Peer Investigator. A special thank you to Professor Stephanie Brown, who has kindly shared her wisdom throughout the course of this study, including offering comments on an early version of this manuscript. And finally, thank you to the talented and patient Rowena Coe who designed the graphic (![]() ) to help us share our findings visually.
) to help us share our findings visually.
Contributor Statement
LB and MB conceived of and designed the study. Data generation was carried out by BJ, KV, IM, and SB, with supervision and mentoring by LB, MB, MP, and JB. LB led data analysis with methodological expertise from MB. BJ, KV, IM, SB, MP, JB, and MB provided iterative feedback on the developing theory. LB wrote the manuscript in consultation with MB, BJ, KV, IM, SB, MP, and JB. Data visualisation was developed by Rowena Coe in collaboration with the study team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Suicide Prevention Australia Innovation Grant. The funder did not adopt an active role in the study, including design, data generation, or analysis.
Correction (March 2023):
This article has been updated with minor textual and style corrections since its original publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.