
Abstract
As speech and language therapists, we explored theories of communication and voice that are familiar to our profession and found them an inadequate basis on which to generate deep and rich analysis of the qualitative data from people who have communication difficulties and who use augmentative and alternative communication. Expanding our conceptual toolkit to include the work of John Shotter allowed us to reconceptualise voice and where it is emergent in dialogue. Reimaging voice will inform clinical and research praxis with people who have communication difficulties as it allows practitioners to attend more closely to the complexity and nuance inherent in interactions with this population. Our proposition is exemplified with excerpts from a single participant who has communication difficulties to illustrate the value of dialogic theory in praxis. This article presents a provocation for the wider academy of qualitative health research; do we have the concepts and tools to develop meaning with people whose lived experiences may also be hard to voice in monologues?
Keywords
Visual and creative methods are becoming more widely used in qualitative health research (Baumann et al., 2020; Fraser & al Sayah, 2011; Wilson et al., 2015), however, language, spoken or written, is the main modality through which research is conducted. This excludes many people who have difficulties understanding and using language (Nind, 2008). This is problematic because understanding people’s experiences is a keystone for improvements in health service design and delivery. The Unspoken Voices Project is concerned with learning about the experiences of people who use augmentative and alternative communication (AAC). People participating in this research project cannot speak clearly or speak at all, but their voices are needed to inform the development of their services. This context impelled the search for conceptual tools for meaning making that did not rely on interpretation of spoken monologues. Three authors on this paper are speech and language therapists (SLTs) with experience of using creative and visual methods in practice. Despite having these practical skills, we found ourselves seeking new concepts and theories to make sense of the meaning that emerged in the dialogues between therapist and participant and between dyads of participants and carers. This paper demonstrates how applying John Shotter’s dialogic theory of interaction (Shotter, 2009, 2010, 2011, 2015, 2016) helped us attend to the pith of meaning making with people who have communication difficulties. We selected moments from the data to elucidate an application of Shotter’s theory, to show how and why the enlivened writing of Shotter is relevant to the field of communication difficulties. Other qualitative health researchers seeking to listen beyond messages in spoken accounts may also find our application of dialogic theory useful in their endeavour to understand more about the lived experience of others.
People can experience communication difficulties at any stage across the lifespan because of congenital and/or acquired health conditions. Some people who have communication difficulties use AAC – a set of strategies often deployed by SLTs to support people to communicate when they are unable to speak clearly. Augmentative and alternative communication strategies encompass gestural signs, such as Makaton™, and paper-based resources containing pictures of words that people can point to. Augmentative and alternative communication also includes computer-based systems that produce synthetic speech to express messages entered into, or pre-programmed within them (Hall et al., 2023). Augmentative and alternative communication systems that produce synthetic speech are called voice output communication aids (VOCAs); voice output is activated by the user either typing in their message or selecting text or symbols that have been programmed to represent specific words or phrases. People who use AAC are a heterogenous group who may experience physical and cognitive as well as communication difficulties. People who use AAC employ a wide range of multimodal communication strategies including disordered speech or vocalisations, gesture, physical movement, and eye pointing alongside external AAC systems to enable them to communicate (Hall et al., 2023). They also depend on an active and responsive communication partner to engage in interactions, supporting and interpreting these multimodal signals to co-create shared meaning (Beukelman & Light, 2020). It is our observations of the intimate and nuanced interactions between people who use AAC and their communication partners that led us to wonder at the nature of proximity and social closeness achieved between people beyond words.
Speech and language therapy (SLT) is a profession that supports people who experience communication difficulties. Clinical practice is influenced by the International Classification of Functioning, Disability and Health (ICF) (World Health Organisation, 2001) within which the impact of communication disability is categorised into areas of impairments of body function, activity or execution of a task, and participation in a life situation. Speech and language therapy services tend towards an expert clinical model whereby professionals’ control clinical interactions, selecting the assessments used, and the pace of therapeutic activities conducted (Korvarsky, 2014). Clinical assessments of speech and language focus on evaluating the nature of the impairment, rather than the impact of communication difficulties on activity or participation of the individual (Barnes & Bloch, 2018). Service users can be characterised as passive recipients of therapy intervention (Ferguson, 2009) with little opportunity for co-participation. This impairment-focussed approach might work in some clinical contexts, but in many circumstances the identification of deficit does not give rise to a good solution for the outcomes that are important to service users. This is the case in AAC services. Augmentative and alternative communication can have a significant impact on aspects of activity and participation which improve their quality of life through greater access to social, educational, and occupational opportunities (Smith & Murray, 2011). Augmentative and alternative communication interventions need to be oriented towards the interactional and contextual factors that influence an individuals’ communication rather than speech or language deficits (Light & Mcnaughton, 2015). Models of clinical practice focussing more on the activity and participation aspects of communicative function are better suited towards serving the needs of this population. Such models would benefit from conceptual tools that help to explore the nature of communication in action; allowing SLTs to attend to what is important to people about the experience of communicating, rather than the process of communication.
Speech and language therapy training is dominated by biological, neuropsychological, and linguistic theories of speech and language. Theories include linear, transactional models of communication, for example, the ‘communication chain’ (Denes & Pinson, 1993). In this model messages are physical (speech, writing, sign) consisting of semiotic signals in which meaning is inherently contained (words in language). This transactional basis for communication has informed SLT through the development of the cognitive-neurological model for language processing in adults (Coltheart et al., 2015) and the psycholinguistic model of speech development in children (Stackhouse et al., 2010). Communication, in these models is conceived as the process of interacting physical messages: the back-and-forth transmission of communicative signals between speaker and listener or recipient. Linear models of communication direct us towards the monologistic, unidirectional transmission of physical messages (Linell, 2009) that are understood based on the assumption of a language processing model, universally shared by neurotypical people. These models also situate responsibility for communication within the realm of the individual. They serve to foreground the physical and cognitive skills and abilities required to transmit and receive these messages as being fundamental to successful communication. Furthermore, linear models of communication when applied in clinical practice focus on phenomena that are explicit. They fail to fully represent the interactive and dynamic nature of communication between people, nor do they enable recognition of the influence of social processes on human interactions (Korvarsky 2014). Linear, transactional models of communication lack strong epistemological and conceptual depth and consequently can undermine qualitative inquiry into the experiences of people who have communication difficulties (Guendouzi, 2014).
The Unspoken Voice Project seeks to support a shift to more socially rooted, activity- and participation-focussed models of clinical practice. The research team engaged with relevant theory to deepen our analysis of experience. A recent qualitative evidence synthesis of the experience of communicating using AAC identified that the nature of co-constructed meaning making was not well represented in existing studies concerning this population (Broomfield et al., 2022). Qualitative analysis in research with people who use AAC tends to be descriptive rather than analytic resulting in lack of conceptual depth in the results (Broomfield et al., 2022). Attending to the nature of the interaction as well as the messages used to communicate may connect researchers to a deeper understanding of the evolution of shared meaning making. Sociological theorists have worked with the linguistic philosophies of Wittgenstein and Saussure and extended the conceptualisation of communication to incorporate aspects of social processes and human interaction. Goffman’s communication theories (1981) attend to paralinguistic features that indicate what is meant rather than what is said during talk-in-interactions, and to the multidimensional facets of ‘speaker’ and ‘hearer’ in an interaction. Attention to the nature of the interaction rather than the linguistic skills and/or deficits of individuals can help to actualise communication difficulties as being socially constructed (Korvarsky 2014), rather than solely being in the realm of the individual. Conversation analysis (CA) is a distinct interaction focussed approach (Wilkinson, 2010). Conversation analysis has been used in research concerning people who use AAC to understand how impaired speech and AAC work together in conversations, and how the nature of the interaction results in shared meaning making (Bloch & Wilkinson, 2004). Conversation analysis can provide insight into the nature of multimodality and uncover some of the less explicit communicative mechanisms through which meaning is negotiated between people with communication difficulties and their communication partners. Conversation analysis is an instrument suited to the micro-analysis of conversational data (Simmons-Mackie, 2014) rather than a conceptual or philosophical tool; CA is helpful in analysing the nature of the interactive process of talk-in-interaction but has perhaps been less used, in the context of people with communication difficulties, to foray between the macro and micro levels necessary to explain as well as explore phenomena in context. The intention of the Unspoken Voices Project was to delve deeper into the essence of experience and the nature of the lifeworld of people who use AAC.
Lifeworld is a concept routed in phenomenology (Husserl et al., 1984) and developed in sociology by theorists who establish the interdependency between society, social order, and an appreciation for intersubjectivity which underpins co-operation and shared meaning making (Habermas, 1981). Contextualising interactions within a personal history, alongside recognition of the systemic influences that may have informed the development of a persons’ lifeworld, are important elements of mutuality in communication. Ethnography, routed in sociological and anthropological understandings of communication and its impact on individual experience and their lifeworld, has been used to explore identity, voice, and representation with young people who use AAC (Wickenden, 2011). Wickenden (2011) explicates the challenges posed by observing and transcribing aspects of AAC users’ messages as opposed to recognising the intended meaning of the individual as realised via the ethnographers’ interpretation. Herein lies a tension between the literal (physical or synthetic) voice of the person who uses AAC – one that transmits a message – and the metaphorical one generated through a mediated translation of a range of contextual, relational, and interpretated signals. Wickenden’s engagement with sociological communication theory enabled them to identify a more metaphorical conceptualisation of voice; something which is co-constructed between people, informed by context, and influenced by relational aspects of those involved in an interaction.
Teachman et al., (2018) also use this notion of voice in their study with young people who use AAC, based on the philosophical work of Mikhail Bakhtin and his writings on dialogism (Bakhtin et al., 1986). Teachman at al., (2018) suggest that ‘that voice only exists in the relation between two or more speakers’ (p. 38). By considering the idea of multiple messages interacting with one another to construct voice dialogue is imagined as a mediated and co-produced interaction resulting in meaning which is ‘dynamic, relational and always uncertain’ (Teachman et al., 2018, p 38). We considered these conceptualisations of voice in the context of our experience of research and clinical practice and whether they could help us to further elucidate the nature of interactions with people who use AAC in our study. We recognised that a broader conceptualisation of voice was helpful when consider data collected to the Unspoken Voices Project, but we noticed something more subtle than a co-creation between actors in an interaction. We wanted to explore our data using a concept of voice that was more mystic, transcendent and perhaps philosophical.
Shotter veers away from conceptualising voice per se; for Shotter, predefined or generalisable concepts risk channelling our thinking inwards, to what is already known (Shotter, 2016). He prefers the idea of difference-making distinctions, or signals that indicate features to attend to, ones that rouse our anticipations to notice similarities and differences (Shotter, 2016). Through Shotter’s dialogic lens, voice can be reimagined as something much more fluid, and formless that surfaces as and when there is a confluence of ideas. This conceptualisation of voice allowed us to at attend to ‘poetic moments’ in the data: those that ‘create the complexly intertwined influences at work in dialogical spaces’ (Shotter, 2016, p114). This allusion to the creativity at work in interaction – the fusing of multiple core elements which direct us towards meaning making – is an idea that resonated with us from our clinical experiences of working with people who use AAC. There exists living, dynamic moments in the ‘landscape of now’ (Shotter, 2016, p75) which we are drawn towards when the unique contours of the dialogue generate something striking, arresting or poetic (Shotter, 2011); that is, moments that make us feel a certain way. Shotter’s work allowed us to attend to these embodied reactions during dialogue in interview interactions, but also afterwards when in dialogue with the data. We noticed the ‘spontaneous occurrence of unique openings’ (Shotter, 2016, p151) during interactions with people who use AAC when the actors involved in the interview respond and react to what is not, as much as to what is spoken. Shotter describes these embodied and instinctive actions and reactions in dialogue as ‘withness-thinking – the relationally responsive kind of thinking we do in our everyday interaction’ (Shotter, 2016, p71). Shotter’s depictions of human interaction and relationships provided us with a lens to see different possibilities within the shapes created by dialogue, those which are driven by the micro-mechanics of behaviours in conversation. It was these ideas that inspired us to apply Shotter’s dialogic theory to guide and mould our interactions with the data in the Unspoken Voices project and to reconceptualise voice.
Our engagement with Shotter’s work provided a theoretical frame from which we were able to reflect on interactions with people have communication difficulties and identify where voice is emergent in dialogue. We will use data excerpts from the Unspoken Voices Project to demonstrate how an expanded version of a critical dialogic theory can advance our conceptual position. Our intention is to encourage greater consideration of and critical engagement with sociologically derived philosophies that can advance clinical and research practice.
The Unspoken Voices Project
Background: The Unspoken Voices Project is concerned with understanding more about the expectations and experiences of AAC from people with communication difficulties. The project includes two qualitative research phases: phase one, the focus of this paper, is a longitudinal cohort study which follows people from pre-assessment for AAC, to 6 months post-receipt of an AAC device. The aims of phase one of the project were to (a) to find out whether expectations from AAC change over time, (b) to add depth to our understanding of what outcomes are important to people from AAC and (c) to identify barriers and facilitators to engaging with AAC.
Ethics and data collection: The project received ethical approval from the Health Research Authority in the UK (IRAS ID: 227722/ REC reference 18/YH/0001). People were recruited to phase one of the project if they were over 12 years old, had a communication difficulty, and had been referred to a regional centre for AAC assessment in the southwest of the UK. A series of 4 semi-structured interviews were conducted with each participant: (1) prior to assessment for AAC, (2) after the initial assessment, (3) following receipt of an AAC device and (4) 6 months after the AAC device was issued. A total of seven participants were recruited to phase 1 of the project. Communication partners (parents, family members, carers and professionals) were included in interviews where that was the preference of the participant.
Patient and public involvement (PPI): A PPI group consisting of people who use AAC and their family or carers supported the development and implementation of The Unspoken Voices Project. The group provided practical support, producing accessible materials during recruitment, and offered invaluable insights to the academic team as data were being collected and interpreted. The activity and impact of this group in the project have been reported in detail elsewhere (Broomfield et al., 2022).
Data: The authors used conceptual tools from Shotter’s dialogic theory to appraise and interact with qualitative data collected in this phase of the project, attending to poetic moments within the data which we felt reflected a significant unit of meaning (Sullivan, 2012). We familiarised ourselves with the data during transcription, data preparation and during analysis, and attended specifically to aspects of data that were remarkable to us and which sparked a feeling of needing to respond or dialogue with these moments. The concepts and ideas represented by these key moments were used to inform further thematic analysis, conducted in consultation with the PPI group. The PPI group checked and challenged the observations and commentary made about these moments and the subsequent analytic process.
Examples used within this paper have been drawn from interviews 1 and 3, conducted with a single participant to The Unspoken Voices Project who has been given the pseudonym Dave. The excerpts presented have been chosen to exemplify poetic moments which shaped our interaction, interpretation and further analysis of the data set. They enabled us to see where and how meaning making constituted more than basic semantic decoding of the language signals but was extended through dialogue and in the emergence of voice. This learning informed our analytic approach to the data set across the cohort study to allow for the generation of a richer, conceptual interpretation. We will use these excerpts to demonstrate how Shotter’s dialogic theory helped us to explicate the nuanced nature of interactions with people who have communication difficulties.
Participant: Dave is a 50-year-old man with Downs Syndrome. Dave’s speech is severely dysarthric, meaning that he is very difficult to understand, and he does not read or write. Dave uses some Makaton™ (a sign-based language programme used to support communication) as well as a VOCA AAC device to communicate (synthetic speech is transcribed in capitals in the excerpt). Dave works at a local café, in a warehouse, and attends a local day centre for 4 days each week. He lives at home with his father Steve (pseudonym). Steve participated in interviews with Dave, along with Dave’s SLT, Jane (pseudonym). Dave, Steve and Jane all provided written consent to be involved in the project; an accessible participant information sheet, explanatory film, and consent form were made available to Dave. Author KB, also an SLT, carried out the interview from which examples have been drawn.
Dialoguing with the data
The following excerpts have been selected from the data collected and transcribed following interview 1 (prior to assessment for AAC) and interview 3 (after receipt of a new AAC device).
In excerpt A (Figure 1), Steve highlights the need to attend to paralinguistic signals during interactions with Dave. He recognises that there may be contrasting information between Dave’s words and his intention: ‘you’ll notice some of the things he’s sounding more enthusiastic about … even though he, you know, he didn’t actually give any different answers’ (Figure 1, lines 1–3). Steve is also aware of the challenges of communication with Dave and encourages KB to ‘use all the clues’ (Figure 1, line 5–6), suggesting that he knows meaning making requires detective work and synthesis of multiple sources of information. This excerpt was noteworthy because it describes the nature of dialogue with people who have communication difficulties. It resonated with our experiences as clinicians as we regularly draw the attention of conversation partners towards non-verbal features of communication with people who have communication difficulties. Steve is apologetic: ‘I’m sorry, it’s a bit difficult to interpret …’, which we felt was remarkable because it was juxtapose to our noticing with awe the natural and instinctive way the actors in the interaction worked synchronously to scaffold the meaning making process during the interview. Excerpt A, from interview 1.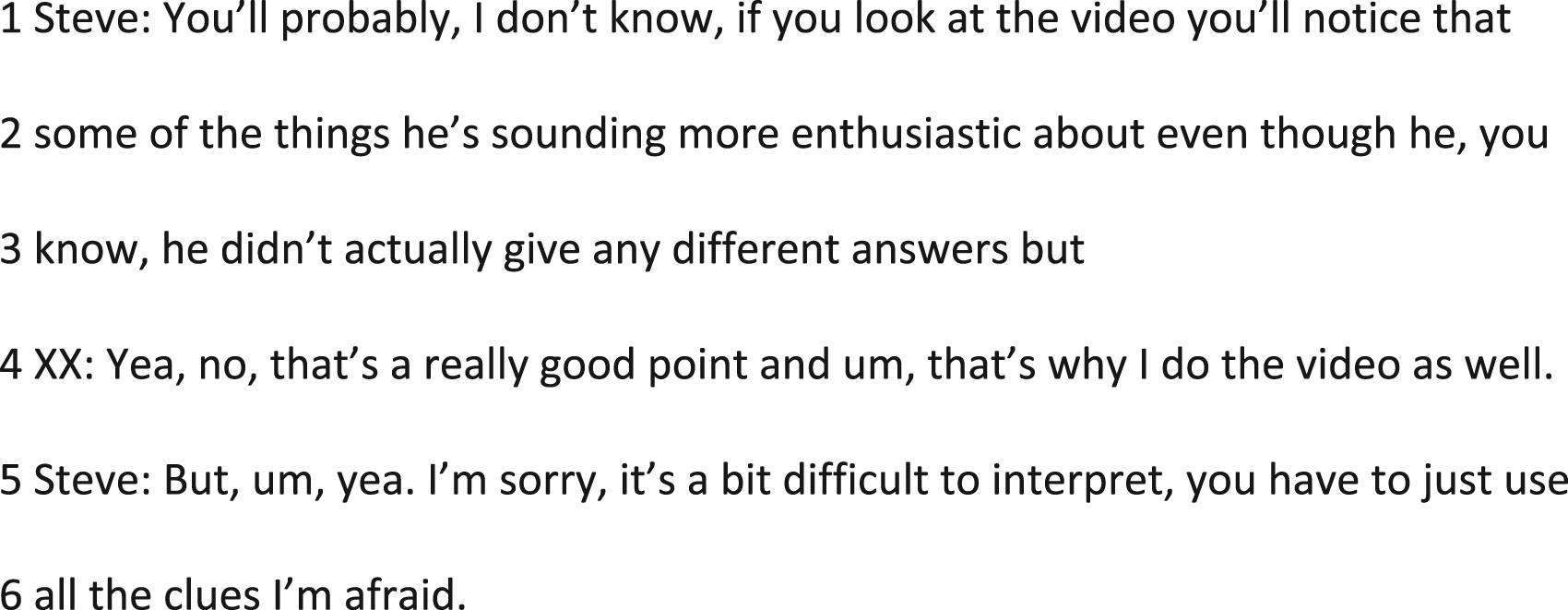
Excerpt B (Figure 2) further exemplifies both Steve and Jane’s insight into the communication needs of Dave. Steve’s use of the idea of being ‘on his wavelength’ (Figure 2, line 1) suggests the notion of tuning in, or attending to signals, and of being an actively engaged listener. This responds to the ideas of Shotter about the relational-responsiveness of dialogue; of sensing and being alert to aspects of the wider landscape that are shaping the current moment. Jane reiterates the idea of the context either shaping or eclipsing meaning (Figure 2, lines 3–4), but focuses on Dave’s expressions rather than the reactions and responses of other actors. Jane goes on to scaffold the interview through her anticipation of Dave’s needs; her actions allow him to perform. She wants him to participate through the generation of messages to give information, and by implication her actions could serve to direct the interview towards these explicit messages. Excerpt B, interview 1.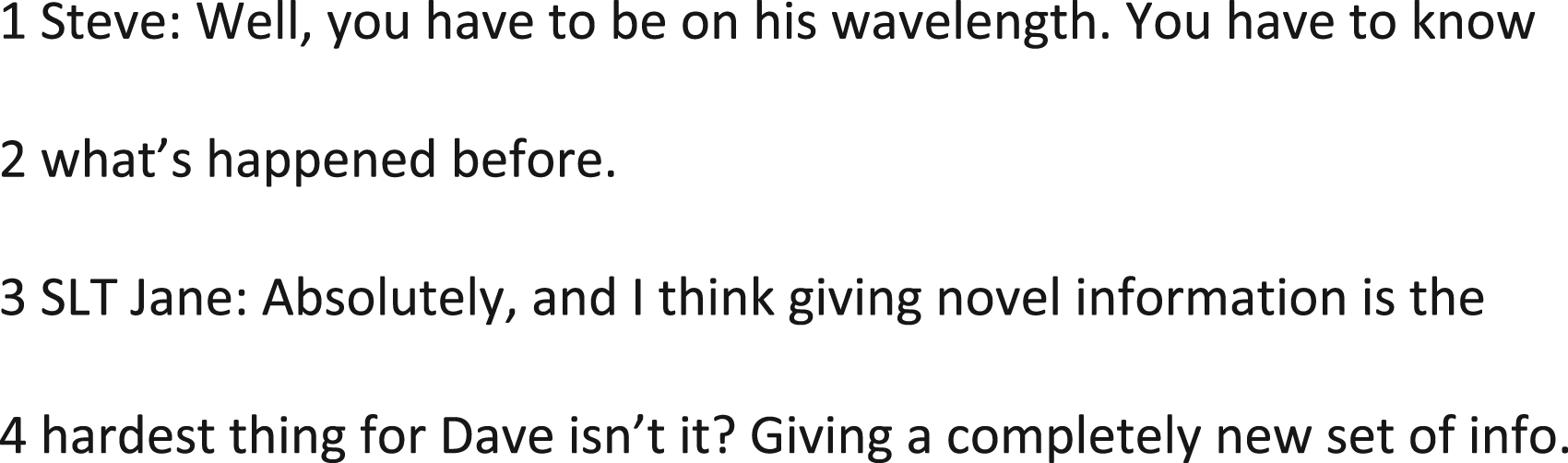
Excerpt C (Figure 3) comes from interview 3, after Dave has been issued with an AAC device which has some pre-programmed phrases within it and has a synthetic voice output (a VOCA). Steve and Jane are asking Dave specific questions to which he is responding. Dave is using a combination of his natural speaking voice and the synthetic voice (transcribed in capital letters) on his VOCA to participate. There are other communicative signals noted in the transcript, such as Makaton™ signs and facial expressions, being used by Dave and his conversation partners (Steve and Jane) which provide some additional information. Excerpt C, from interview 3.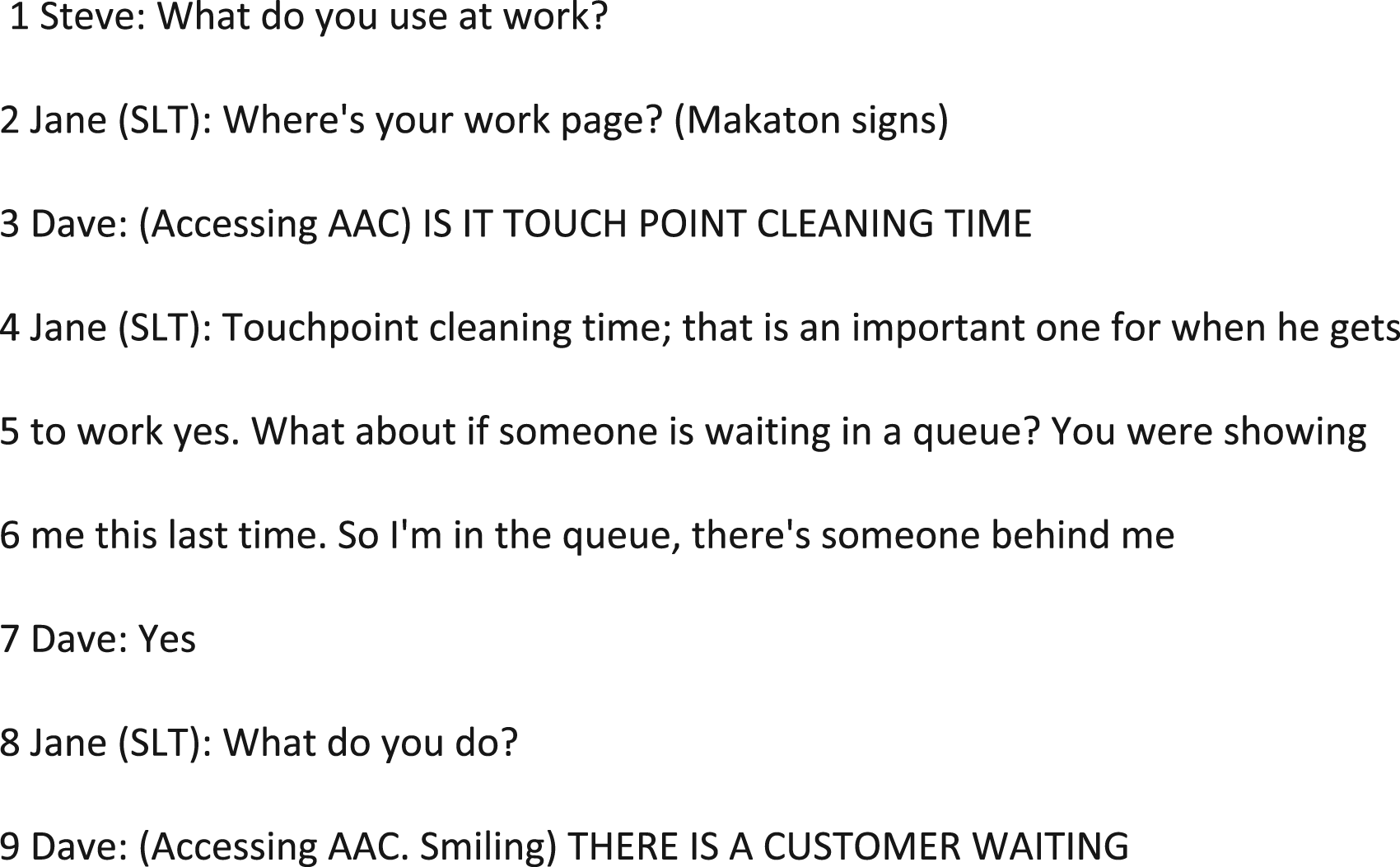
Close attention to Jane’s responses in excerpt C highlights the challenges presented by analysing only the explicit communicative signals. Rather than respond to the question, Jane points Dave towards specific pages on his VOCA (Figure 3, line 2) and then she goes on to create a scenario to which she seeks a reaction (Figure 3, line 6). Dave responds by selecting a prestored phrase from his AAC device which is then produced in synthetic speech. Jane’s response to Steve’s question: ‘where’s your work page?’ (Figure 3, line 2), is not directed to Steve (in response to his question) nor is it intended to express her own perspective, but rather to facilitate Dave to participate in the interview. She uses Makaton™ to support Dave’s understanding of the question. In pointing Dave towards his work page, she is anticipating his response and he responds by recognising the intention of her suggestion. Jane contextualises Dave’s response, ‘IS IT TOUCHPOINT CLEANING TIME’ (Figure 3, line 3), with her use of a clarifying phrase ‘that is an important one for when he gets to work’ (Figure 3, line 4–5). Her reaction signals a deeper understanding of the nature of the context in which Dave’s response is used in the workplace. Jane then facilitates Dave to build on his contribution to the interview by providing a scenario that she knows that Dave has a prestored phrase in his VOCA that he can respond with: ‘what about if someone were waiting in the queue?’ (Figure 3, line 5). Jane’s actions are not intended to contribute to the to-and-fro discourse of the interview, but to enable Dave’s participation using his VOCA. It is in the convergence of her perception of her role in the interview, her background knowledge of the VOCA and of the workplace in which it is used, that Jane helps to construct the meaning being voiced in this excerpt.
KB made reflective fieldnotes to comment on poetic moments or arresting events that she noticed both directly after the interview takes place, and during a later process of analysing interview videos and transcripts. Excerpt D (Figure 4) evidences the reason she was drawn to the moment in excerpt 3; it represented how she interpreted meaning being created beyond words. Her knowledge and experience of meeting with Dave, Jane and Steve in previous interviews shaped her understanding of the nature of Dave’s communication and the relationships between the three other actors. This living knowledge – experience that informs future embodied responses – drew attention to excerpt 3 because she recognised the movements that were behind the words in Dave’s VOCA which were shaping the emergent voice. Through attending to such moments in the video and transcript, and to what feelings they arouse, becomes part of the interpretative process in the dialogue. It is in noticing of specific events, or moments, both during the interview itself and during post-hoc appraisal and reflection on the interview video that the concepts which inform the interpretation of meaning are elicited. Excerpt D from reflective fieldnotes written by XX directly after interview 3 took place.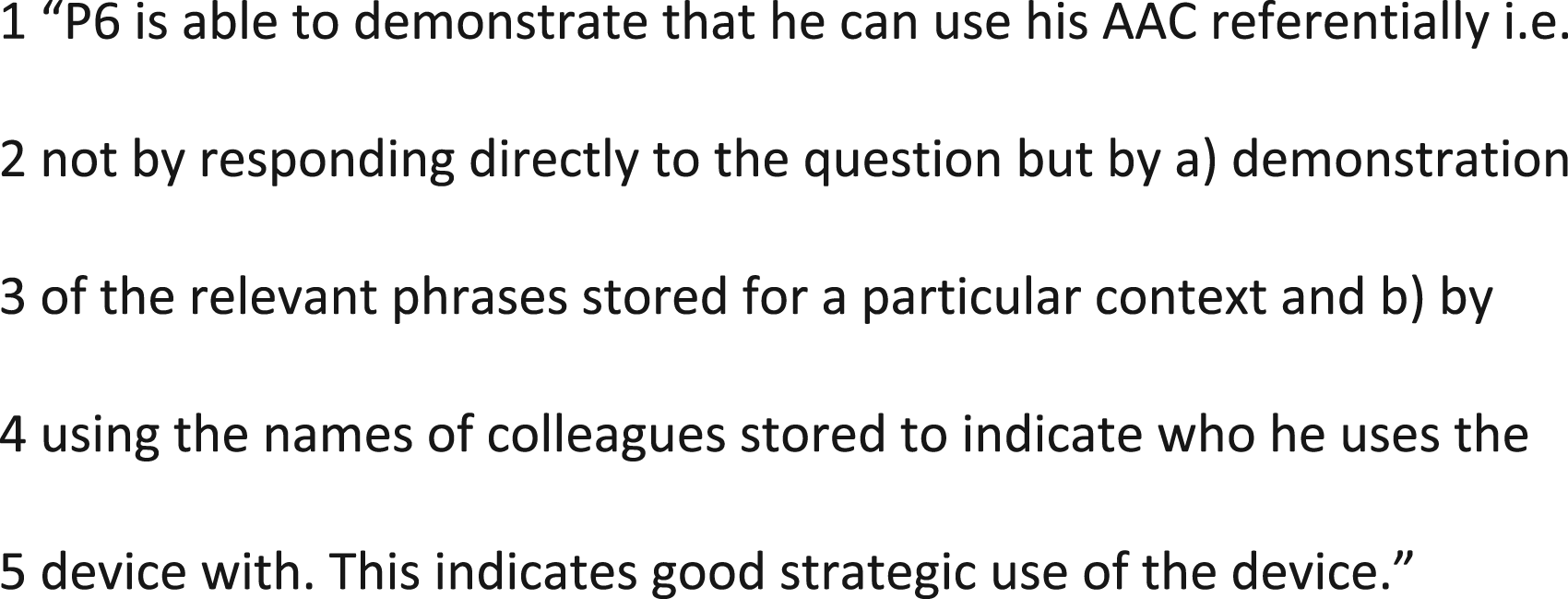
Discussion
The data excerpts presented from the Unspoken Voices Project provide some insight into the scarcity of linguistic richness and the multimodal nature of communication for people who have communication difficulties. This serves to elucidate some of the challenges of qualitative data analysis with this population. Linear, transactional models of communication provide insufficient frameworks from which curious SLT clinicians and researchers can investigate the multimodal and dynamic features of communication (Wadnerkar et al., 2012), and wonder at the nuance and complexity that exists beyond speech and language during communication.
Engaging sociological and philosophical, rather than psycholinguistic, conceptualisations of the nature of human interaction and communication theory enabled us to reimagine voice and where it emerges in dialogue with people who use AAC. We were also able to position ourselves, and our own experiences as clinical academic researchers within the co-construction of meaning making within the data collection interview and subsequent dialogic analysis.
Concepts of Communication and Voice
The communication chain is a model that allows practitioners to consider the impact of speech and language on communication. In the data presented, the AAC device has expanded Dave’s communication toolkit from Makaton™ signs and dysarthric speech to include a physical, intelligible voice which can transmit words and phrases. However, a transactional interpretation of excerpt C does not enable us to adequately understand how Dave uses AAC to facilitate his participation in the interview as he does not have a direct response to the question pre-stored within his AAC device. Nor does it adequately explain the roles that Jane and Steve are playing in the interview and how their behaviours and actions within interaction shape meaning making. The communication chain tends towards positivist (where reality is exclusive of context), or pragmatic (where reality is informed by individual ‘patient’ experience) informed praxis. In clinical practice, it directs SLTs towards objectivity and problematising functions or behaviours within the individual, which they may or may not be able to alter (Korvarsky 2014). In research, it directs researchers in communication disability towards identifying how communication is affected by impairments to the speech or language mechanisms that underpin it.
Expanding on the nature of communication from being a string of linguistic signals to incorporating aspects of the interactional dynamics allows researchers to attend to the discursive features that shape our understanding of data. Detailed analysis of discourse using a tool such as CA can capture the distinct features of the interaction that support and/or inhibit how meaning is generated through the various behaviours and activities of those involved (Wilkinson, 2010). This can be a valuable tool in clinical practice as it moves clinical focus away from the individual and their communication impairment and towards aspects of communicative activity that are inhibiting conversations. However, understanding the nature of the interaction process does not necessarily enable qualitative researchers to engage with the pith of individuals’ experience of communication; how do these interactive features of discourse coalesce with wider aspects of their lived experience? To understand how the meaning being shaped by the personal histories and lifeworld’s of people we found that we needed to apply a different theoretical lens, and to reconceptualise voice and where it emerges.
Qualitative researchers have used philosophical and sociological theory to refocus the conceptualisation of voice away from the physical and towards the figurative voice (Teachman et al., 2018; Wickenden, 2011). Teachman et al. (2018) present a critical dialogic methodology used in research with people who use AAC, to explicate the idea of multivoicedness, where voice is located between speakers. By considering this idea of multiple messages interacting with one another to construct voice dialogue is reimagined as a mediated and co-produced interaction resulting in meaning which is ‘dynamic, relational and always uncertain’ (Teachman et al., 2018, p 38). This concept of multiple voices interacting orients us towards the idea that dialogue is driven by anticipation; discursive actions connect the dialogue to the past and/or direct the shape of the interaction going forward. Conversation analysis can illuminate the mechanisms through which the direction of the interaction progresses or is disrupted in the moment. It can also explicate how multiple voices create meaning from the linguistic and semiotic signals observable from outside of the interactive discourse. But what of the less evidently explicable responsiveness of actors in the interaction? During data collection and analysis in the Unspoken Voices Project, we noticed over time that our attention was drawn to instances in the data (e.g. excerpt C) because of what we had observed, learned, and experienced during previous interviews. We also wondered the extent to which our own professional training and personal histories informed how we interacted with the data. We sought a theory of dialogue that would help us understand what and why we were alerted to these moments.
In critiquing the concept of voice, we recognised the activity of the clinician and researcher/interviewer in the multi-voiced data from the Unspoken Voices Project. We noticed when reviewing the data for this project that KB’s embodied experience, or living knowledge, was useful in facilitating interviews and was drawn upon in the creation and representation of the experiences of participants. Attending to the embodied responses of agents in dialogue allowed us to get closer to understanding how meanings are co-created within and between the actions observed in an interaction. Shotter uses the phrases ‘withness-seeing’ and ‘withness-thinking’ (2011, pp100–101) to describe how one can get inside the dynamics of an interaction by active listening; observing all signals that are being generated but also by attending to our embodied senses and how we are physically responding to the messages in the moment. Being ‘inside the moment’ of acting and speaking (Shotter, 2016, p127) allowed us to attend to and notice our embodied responses in dialogue and to respond relationally to the needs of the interaction and to the needs of the other. He describes the role of intuition in the ‘spontaneous performing’ (Shotter, 2016, p131) that our expressions arouse, both in ourselves and in all those to whom they are addressing, to generate both ‘feelingful thoughts and thoughtful feelings’ (Shotter, 2016, p131). Shotter’s theory enabled us to situate ourselves within the interview interaction as active agents in meaning making while also attending to the actions that suggested ways of knowing beyond explicit signals and messages during data analysis. We were able to delve into the detail of the interactions within interviews and zoom outwards to notice the significance of specific actions within the wider context provided by the whole of the dataset. This interaction with the data allowed us to draw out conceptual interpretations from the range of verbal, non-verbal, visual and reflective information gathered during each individual interview and look across the cohort data set for resonance and dissonance across the experiences of other participants.
Shotter’s dialogic lens offered us the conceptual tools to create visual and embodied understandings from our data that transcended concrete, semantic meaning and were more representative of the multiplicity of interacting information we encountered. The excerpts presented above provide a snapshot; they exemplify the essence of how we dialogically moved between the detail of the interaction, the historicity of the interview and actors within it, and the embodied reactions we noticed in ourselves and others to move towards a sense of co-created, shared meaning.
Critique
In this paper, we have attempted to condense some expansive theoretical ideas into a conceptual toolkit that we applied to our data with the intention that it might be useful to others. In the process of doing so, we anticipate that there might be appetite for greater debate about, and critical engagement with these theories and ideas. We have read great philosophical, sociological and academic works in developing our interpretation and application of Shotter’s dialogism yet only alluded to them within this manuscript. We accept that further critique and discussion of these ideas would add greater depth and further insight to their application in the field of communication disability research, and to SLT training and praxis.
We recognised that there is a gap between the complex, dynamic and nuanced dialogue inherent in interactions with people who have communication difficulties and the current theories that inform the research and clinical practice of SLT. In conducting research with people who have communication difficulties, we found that the scientific paradigm in which we train was not a helpful foundation from which to explore more philosophical ideas about experience and lifeworld. Shotter’s work has been applied in the field of family therapy (Shotter, 2015) which, like SLT, has a specific interest in interaction and relationships. In applying the concepts discussed in this paper, we found that they provided a platform from which we could better attend, listen and attune to all the responses and reactions we experienced during data collection and analysis. We argue that engaging with sociological and philosophical theory, though potentially disruptive, can provide rich sources of inspiration for creative and socially motivated practice.
Finally, there was further dialogue that could have, and arguably should have, taken place with the data presented here. What may have happened if we presented our interpretations back to the participant? How would further dialogue have shaped our interpretations in a different way? One of the attractions of this theoretical lens is that it opens-up the idea of possibility and potentiality. Shotter uses the analogy of a river, being shaped by the contours of the surrounding landscape and interpretations are ‘embedded within the larger flow of things’ (Shotter, 2016, p44). We entered the river at one point and exited at the other, acknowledging that there are different possible exit and entry points further up- and down-stream. This may be dissatisfying or alluring to our readership, depending on your perspective.
Conclusion
Speech and language therapists are not trained or professionally rooted in the social sciences, which influences the epistemological nature of our clinical research. This paper presents a provocation to our field: do we have the conceptual tools that adequately reflect the demands of research praxis and clinical practice with people who have communication difficulties?
We have found Shotter’s dialogism to be a useful theoretical lens through which to explore the life worlds of people who have communication difficulties; one that has allowed us to listen and engage with data in a different and more expansive way. Dialogism is a lens that needs to be looked through by agile and reflexive practitioners who can enter into the world of others while maintaining connection to their own history and lived experience. A dialogism that engages SLT researchers and clinicians with their background, skills, and their role within an interaction enables praxis that transcends the traditional boundaries imposed by linear communication models and works with multiple perspectives and sources of information to generate a negotiated representation of shared understanding. Through dialogic engagement with the data, we reconceive voice as polyphonic and mercurial, emerging in dialogue where the past, present, and possible future coalesce to inform meaning-making. Engaging a theory that better represents the activities of agents in dialogue with people who have communication difficulties will help the SLT profession, as well as other practitioners working with this population, better reflect and articulate the complexity and wonderment that is inherent in these interactions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Katherine Broomfield (Clinical Doctoral) This Research was supported by the National Institute for Health Research (NIHR)/ Health Education England (HEE) for this research project and Research Trainees Coordinating Centre (ICA-CDRF-2016-02-061). The views expressed are those of the authors and not necessarily those of the NHS, NIHR or the Department of Health and Social Care, UK.