
Abstract
The prevalence of HIV-associated neurocognitive impairment (H-NCI) is concerning. Individuals on effective antiretroviral therapy (ART) may still be at risk for H-NCI as they experience longer life expectancies. There are, however, few professionals with knowledge and skills to identify H-NCI, in low- and middle-income countries. We explored qualitatively, primary healthcare workers’ knowledge and views of H-NCI, in the era of effective ART, particularly their views toward task-sharing of H-NCI screening from specialists to mid-level or lay healthcare providers. The first phase of data collection involved two focus group discussions (FGDs) 23 primary healthcare workers from two facilities in the Western Cape participated in the FGDs. In the second phase of data collection12 individual, in-depth interviews were conducted in KwaZulu-Natal. Using thematic analysis, several key themes emerged. Although healthcare providers were unable to specifically identify H-NCI, they described several HIV disease and treatment related or mental health comorbidities that could be responsible for the symptoms. Despite healthcare workers reporting low frequencies of H-NCI, they favoured receiving training to screen for H-NCI with a view toward providing holistic care.
Keywords
Introduction
In the past decade, HIV has evolved into a manageable, multi-system, chronic illness, following the development of effective antiretroviral therapy (ART) (Milanini & Valcour, 2017; Sanford et al., 2019). However, HIV-associated neurocognitive impairment (H-NCI) remains a concern even among people with HIV (PWH) on ART (Underwood et al., 2019). Although the prevalence of H-NCI vary significantly across countries, a meta-analysis exploring the global prevalence and burden of H-NCI found that sub-Saharan Africa, which is home to the largest population of PWH, may also have the largest number of adults living with H-NCI (Wang et al., 2020).
HIV has the ability to invade the central nervous system during acute infection causing inflammation which may result in a range of cognitive, motor, and/or mood problems among people with HIV (Carter et al., 2003). H-NCI varies in clinical course as well as in signs and symptoms, ranging from subtle cognitive and motor impairments to mood disorders including depression, or more severely as dementia (Mohamed et al., 2020; Watkins & Treisman, 2015). Typically, individuals with H-NCI may experience functional impairment (Sacktor, 2018) which includes difficulties with learning, attention, problem-solving and decision-making, as well as functional challenges with tasks required for daily living (de Jager et al., 2015; Heaton et al., 2011). Individuals with H-NCI may be at an increased risk for chronic treatment non-adherence, leading to a myriad of adverse outcomes, including opportunistic infections, poor quality of life and early mortality (Kamal et al., 2017; Meade et al., 2011). Despite significant declines in the incidence of severe H-NCI, the prevalence of milder forms may persist as PWH now experience longer life expectancies (Simioni et al., 2010; Terpstra et al., 2018).
The diagnosis of H-NCI is a diagnosis of exclusion, requiring healthcare workers to be aware of confounding or contributing factors (Milanini & Valcour, 2017). An H-NCI screening tool is administered once these factors have been ruled out. However, few trained professionals possess the necessary knowledge and skills to screen and diagnose H-NCI in low- and middle-income countries (Cettomai et al., 2011). Furthermore, these specialists seldom provide healthcare services at a primary healthcare level, where the majority of PWH access care (Cettomai et al., 2011; Dube & Uys, 2016; Mall et al., 2013).
Healthcare services are mainly provided by nurses, adherence counselors, pharmacists and a small number of medical doctors, at a primary healthcare level (Joska & Sorsdahl, 2012). These facilities often experience high patient volumes, as well as staff shortages (Sibeko et al., 2018). Due to these challenges, South Africa adopted the World Health Organization’s (WHO) recommendation of ‘task-sharing’ of mental health services (Department of Health, 2013). These services are shared from specialised doctors to non-specialist physicians, followed by nurses, nursing assistants, as well as other community healthcare workers, such as adherence counselors (Department of Health, 2013; Remien et al., 2019). Although task-sharing has been beneficial in improving general mental health services, it is unclear whether task-sharing of H-NCI screening at primary healthcare facilities will be equally beneficial (Cettomai et al., 2011; Remien et al., 2019). There is also a paucity in literature describing H-NCI training interventions targeting primary healthcare workers. This is despite previous cross-sectional surveys highlighting H-NCI knowledge gaps and uncommon screening practices in South Africa (Gouse et al., 2020; Munsami et al., 2021).
To our knowledge, there have been no in-depth reports on H-NCI knowledge and skill gaps among nurses, adherence counselors and medical doctors. This article expands on previous research by qualitatively exploring primary healthcare workers knowledge, understanding and perceptions of H-NCI in the era of effective ART. We further explore their views towards acceptability and feasibility of integrating H-NCI screening into primary healthcare services, suggestions for tool administration and perceived needs for capacitation.
Methods
Study Design
In this descriptive qualitative study, we conducted focus group discussions (FGDs) and in-depth, individual interviews with medical doctors, nurses and adherence counselors providing HIV services at primary healthcare facilities (Hunter et al., 2019). The facilities were in the Western Cape and KwaZulu-Natal provinces, South Africa. The University of Cape Town, Faculty of Health Sciences, Human Sciences Research Ethics Committee (HREC 624/2018), the Western Cape Department of Health and the KwaZulu-Natal Department of Health approved this study. All participants signed informed consent before continuing with the interviews.
Participant Selection
Operational managers were approached and once they were agreeable healthcare workers were invited to voluntarily participate. The healthcare workers were informed that the FGDs would explore healthcare services provided to PWH accessing care at the facility. All who were approached for the FGDs agreed to participate, while three healthcare workers declined to participate in the in-depth interviews due to time constraints. Two participants who initially agreed to participate deceased prior to the interview taking place.
Procedure
Between July 2019 and August 2019, two FGDs were conducted by the first author with the participants in the Western Cape Province. The first author is a female researcher and has postgraduate qualifications, and previous training.
The FGDs were conducted first, to allow the opportunity for the individual interviews to further explore key themes that emerged. After obtaining informed consent, the in-depth, individual interviews were conducted in English with healthcare workers from two hospitals and three primary healthcare clinics, between December 2020 and January 2021. The in-depth interviews were conducted by the first author. We aimed to ensure that our sample was representative of the staffing profile of primary healthcare facilities in South Africa, to be able to explore any variations between cadres that emerged from the data.
The FGDs and in-depth interviews were conducted at the facility during the scheduled weekly staff meetings, to avoid removing healthcare workers from the facility, limiting disruptions to patient services. Only healthcare workers who agreed to participate were present during the FGDs. The FGDs followed an interview schedule that included questions pertaining to non-adherence among PWH, H-NCI symptoms, H-NCI screening at a primary healthcare level and future training. The complete interview schedule is provided in Appendix 1. The FGDs lasted between 60 and 80 min and were recorded using a voice recorder and field notes which were made by the first author.
Following the initial analysis of the FGDs, 12 individual, in-depth interviews were conducted, to further explore and describe healthcare workers’ understanding of H-NCI among PWH. Only healthcare workers’ who provided informed consent were interviewed. Each in-depth interview lasted approximately 45–60 min and was conducted during times where there were few patients at the healthcare facility. The in-depth interviews were conducted until saturation was reached.
To facilitate this discussion, the semi-structured guide was supplemented with a vignette. A vignette is a short, hypothetical story, commonly used in qualitative and quantitative research to explore real-world, patient-based scenarios (Aujla, 2020; Gourlay et al., 2014; Sampson & Johannessen, 2020). Given that milder forms of H-NCI may be complex to identify, we presented a vignette that describes severe H-NCI.
Vignette
A 35-year-old man who works at the local grocery store has come to the clinic following difficulties at work. His supervisor suggested that he see a doctor after noticing that he has been losing track of time and as a result he does not complete his daily tasks. He has also been finding it more difficult to concentrate and has greater difficulty in remembering the instructions that have been given to him by his supervisor. For example, which shelves need to be re-stocked. He informed the counsellor that he missed his last clinic visit because he has trouble remembering things, such as appointments, unless he is reminded by his wife. He tested positive for HIV recently and was initiated onto ART. His CD4 count at the time of testing was 25 cells/mm3 and his viral load was 260,862 copies/mL. He missed his last scheduled clinic appointment and has been without his ARVs for more than a month. His viral load (190,052 copies/mL) has not improved since being initiated onto treatment.
Data Analysis
Inductive thematic analysis, an approach which focuses on identifying, analysing, organising, describing and interpreting patterns of meaning within qualitative data, was used to analyse the data (Braun et al., 2012; Nowell et al., 2017). The analysis was facilitated using NVivo 12, a qualitative data analysis software. The data was recorded and transcribed by the first author who conducted the initial review or familiarisation, and identification of major themes with a second researcher. The first author and a second researcher coded two FGDs and four in-depth interviews independently, before meeting to review the codes. The intercoder reliability coefficient was 0.83. All discrepancies were discussed until consensus regarding the coding was achieved. The remaining interviews were then coded using the agreed upon codes. The researchers resolved all differences through discussion.
Results
After describing participant characteristics, we present synthesised findings that emerged from the FGDs and in-depth interviews. H-NCI knowledge and screening practices among primary healthcare workers in South Africa were influenced by (1) existing knowledge and understanding of H-NCI, (2) views on the perceived acceptability and feasibility of screening at primary healthcare level and (3) opinions on the appropriateness of training healthcare workers at primary healthcare facilities to identify H-NCI.
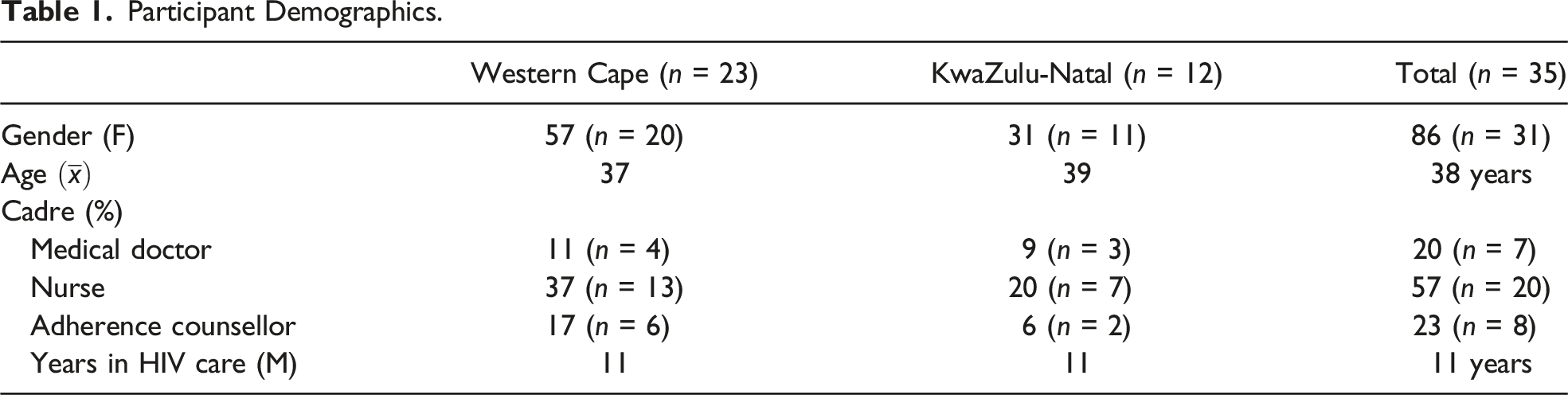
Participant Characteristics
Participant Demographics.
Healthcare Workers’ Knowledge and Understanding of H-NCI
When asked to provide a broad description of the effects that HIV may have on the brain, several nurses and doctors specifically mentioned co-morbidities, opportunistic infections or described common mental disorders, particularly depression. Although a few doctors and nurses specifically mentioned dementia due to HIV impacting the brain, the term HIV-associated dementia (HIV-D) was not mentioned specifically. When describing the symptoms of dementia caused by HIV, the providers tended to describe quite severe clinical symptoms. This is illustrated by several participants who said: [Patients with dementia] can get this apathy, insomnia, hallucinations, sleep disturbances, depression. (Medical doctor, participant 25) In the older patients where they are restless, and they often forget things. It is like when they have dementia. (Nurse, participant number 31)
When prompted specifically about whether they had heard of H-NCI, only one doctor responded with ‘now that you mention it, I remember hearing something’, while all the providers ‘were only hearing about it now’. Upon further probing with the use of the vignette describing a typical patient living with H-NCI, only one healthcare provider mentioned that the person in the vignette could be living with ‘HIV encephalopathy or AIDS dementia complex’.
The healthcare providers did not specifically diagnose the individual described in the vignette with H-NCI. However, they did describe several factors that could be responsible for the symptoms. These were primarily HIV disease and treatment related causes or a result of a mental health problem. First, HIV specific causes, including non-adherence, side effects of ART low CD4 cell count and late-stage disease, were mentioned by a few doctors and nurses in the sample. You get mental manifestations due to advanced stage of disease. People have confusion, and this is most times in the low CD4 or late stages [of HIV]. (Medical doctor, participant 24)
All providers described how poor adherence to medication could explain the symptoms. We have seen people with confusion then they are not taking their treatment [causing] general neuropsychiatric manifestations of HIV. (Medical doctor, participant 25)
Several healthcare professionals among all cadres, described side effects frequently experienced by PWH who are on Efavirenz, a drug that forms part of older ART regimens that could be contributing to the symptoms described in the vignette. Patients on first line, Efavirenz, they are going to have confusion, lucid dreams and neuropsychosis. It is a side effect of that drug. (Medical doctor, participant 13)
Efavirenz usually acts on the central nervous system which usually affects our patients causing acute confusion. (Nurse, participant 29) In addition to HIV disease and treatment related causes, mental health problems were described by several healthcare providers as not only contributing to patient non-adherence to ART but could be a direct cause of the symptoms described in the vignette.
Depression has those same physical symptoms. So maybe it is also related to depression. (Nurse, participant 33) [Confirm] if its only memory problems or a concentration problem maybe anxiety related issues because with HIV you are already thinking about death. (Medical doctor, participant 25)
When asked about the frequency of HIV patients presenting with symptoms described in the vignette, the doctors and nurses highlighted that they were common prior to the roll-out of ART, but they ‘do not really see these symptoms’ in the era of effective ART. Medical doctors and nurses regarded H-NCI as a historic problem, which declined following widespread use of ART. This is illustrated by several healthcare providers who said: It is not often. It is not so prevalent mainly because we started initiating [early]. Remember in the years before we used to start people at a certain level of low immunity. So those manifestations were prevalent when they [patients] used to have low CD4 count. (Medical doctor, participant 24) We saw a lot of that in the beginning in the eighties and the latter part and the nineties. It is not as bad as before. Now you find it rarely. (Nurse, participant 29)
Healthcare Workers’ Views on the Acceptability and Feasibility of H-NCI Screening
Screening at Primary Healthcare Facilities
Given that healthcare workers in this study reported that they did not screen for H-NCI, we explored current care practices for patients who report problems with memory loss or confusion. Adherence counselors suggested that patients with these problems would ‘need to be referred to the nurse’. Some nurses suggested that they would ‘refer to the doctors and maybe the doctors would refer to the psychologist’, while several doctors stated they would ‘refer the patient to a psychologist’.
Among the doctors and nurses who reported that they would investigate the symptoms further, these individuals stated that they would administer ‘the mental health screen which was started in primary healthcare clinics’ by the Department of Health in South Africa. The tool was described a brief set of ‘questions about mood disorders and fears or phobias’.
Nurses indicated that forgetfulness or difficulties with memory were investigated to determine treatment adherence. Adherence counselors referred patients to a nurse if they reported challenges with their attention or memory. We ask about the medication, using protection and being safe. I never really thought to ask about the other things [like H-NCI]. (Nurse, participant 27)
The Acceptability and Feasibility of Screening for H-NCI at a PHC
Despite having reported low frequencies of H-NCI, all cadres still felt it was within their role to identify H-NCI among PWH accessing care at their facilities and responded positively to having access to an H-NCI screening tool. They also considered it feasible to administer an H-NCI screening tool at a primary healthcare level. Adherence counselors agreed that screening for H-NCI ‘would be very good’. Having this tool would allow us to recognize them at an early stage. Not when they are at a stage of possible irreversibility or requiring admission or something. (Medical doctor, participant 24) I think it will benefit patients a lot. Because the more we identify early the better. It will be better to identify early and prevent it if it is happening. (Nurse, participant 30)
Healthcare workers expressed alternate views when asked which cadre of healthcare worker should be equipped to screen for H-NCI. Medical doctors and nurses agreed that patients provided more detailed and honest information to the adherence counselors or nurses during counselling, compared to information provided to medical doctors during a physical examination. The counselors might know more because patients tell us different things, and then something else to the nurses. The counselors also see the patients more frequently than us [doctors]. (Medical doctor, participant 2) The nurses would be central because they see more patients than a doctor. Counselors are the entry point they help a lot and can be helpful. (Medical doctor, participant 24)
Several nurses reported that medical doctors would be more suitable to administer screening tools as further treatment and management decisions lie with the medical doctors. It will be better because then the medical doctor will know how to manage the patient better than we will have to wait to know from the medical doctor, and this can create delays. (Nurse, participant 30)
The majority of healthcare workers felt that all cadres should be equipped to screen for H-NCI as each cadre has a different role to fulfil in terms of patient care. I think that everyone needs to be trained, because if a medical doctor or nurse screens a patient, the reinforced counselling provided by counselors will also become important. (Medical doctor, participant 1) It is all of us. We all have a part to play. (Nurse, participant 29)
When asked to suggest suitable times at which H-NCI screening could be conducted, the following points in the clinic flow were suggested: adherence clubs, during waiting time at the facility and annual check-ups, for ongoing monitoring of H-NCI as highlighted by the following statements: We can talk about neurocognitive impairment during the adherence clubs. (Adherence counsellor, participant 5) It will be feasible at this facility because we have much standing time sometimes while patients are waiting to be seen. The other thing is at their first test, maybe it is possible and annually after that when they come for CD4. (Medical doctor, participant 2)
Perception of Training in H-NCI Screening and Diagnosis
All cadres reported that they had attended training to provide HIV services. However, the medical doctors indicated that they had ‘not been for any training’ focussing on HIV and cognition or H-NCI. In most cases, healthcare workers had attended courses many years ago and did not receive refresher training thereafter. As a result, they were unsure if they had received information on H-NCI in previous training. Remember we did nursing school very long ago. We maybe cannot remember things that were mentioned. We know the focus. Check viral load check CD4 count check these things. (Nurse, participant 27) It has been like 13 years since I completed my medicine. I do not remember other [disorders] to be honest it has been a very long time. (Medical doctor, participant 26)
All three cadres of healthcare workers were open to receive training on H-NCI and the use of screening tools. However, there were mixed views on the best method of delivery for the training programme. Several healthcare workers preferred traditional methods of training such as didactic, face-to-face lectures. We have tried the online training here at this facility. It has had a lot of issues and people do not really pay attention, they are in and out because no one can see you. So maybe face-to-face. (Medical doctor, participant 25)
Others preferred a combination of shorter brief workshops over multiple sessions or ongoing, online training which could be accessible after clinic duties but were concerned about network or connectivity issues as illustrated below: Personally, I think online you can log in at any time. As you came today its quiet so I would login and learn instead of having to go and sit for hours to do this. (Nurse, participant 30) I like to face-to-face because you have a question you can ask. Sometimes online it will be connecting, and they cannot hear you. (Adherence counsellor, participant 35)
Discussion
To our knowledge, this is the first paper to use qualitative methodology to report on primary healthcare workers’ knowledge and understanding of H-NCI and, perceptions, towards H-NCI screening at this level of care and attitudes towards received H-NCI training. Between the three cadres, we found that healthcare workers did not identify H-NCI specifically but attributed symptoms to HIV treatment related causes or a result of an underlying mental health condition. Medical doctors and nurses viewed H-NCI as a historic problem, suggesting that H-NCI was uncommon among PWH accessing care at primary healthcare facilities, while many others expressed not knowing enough about this disorder. All cadres had no prior experience in screening for H-NCI. Despite primary healthcare workers suggesting a low prevalence of H-NCI among their patients as a result of effective ART, they were in favour of receiving training to screen for H-NCI. This, with a view towards providing holistic care for PWH accessing care at this level. There were differing views on the method of training best suited for primary healthcare workers. Certain individuals favoured traditional, didactic, face-to-face training, whilst others favoured flexible, online training sessions. There were no differences in knowledge and views between the two provinces.
Although our findings illustrate that healthcare workers were not able to identify H-NCI and were unaware of the spectrum of impairment caused by HIV, a few were aware of dementia due to late-stage disease among PWH. Several healthcare workers attributed symptoms of H-NCI to treatment related factors such as poor treatment adherence, low CD4 count or resulting from common mental disorders, such as depression. Similar to findings from previous studies in South Africa, the majority of healthcare workers had never heard about H-NCI, especially adherence counselors (Gouse et al., 2021; Munsami et al., 2021). Many believed that H-NCI had declined since the advent of ART and only existed in rare cases. This may be true for the incidence of severe H-NCI such as HIV-D that has declined over the years; however, the prevalence of milder H-NCI may still increase as PWH accessing ART experience longer life expectancies (Simioni et al., 2010). Reports on the prevalence of H-NCI vary and remain a debatable topic (Valcour et al., 2011). It is, thus, unclear whether H-NCI is indeed uncommon in the current context, or whether primary healthcare workers’ lack the appropriate knowledge to identify milder forms of H-NCI among individuals accessing care.
The attribution of neurocognitive and functional impairment in PWH to co-morbid factors, for example, the side effects of the drug Efavirenz, or low CD4 cell count, is still positive. This, as the first stage of H-NCI diagnosis, is the exclusion or optimal management of other contributing factors (Milanini & Valcour, 2017). Therefore, our findings show that if milder forms of H-NCI are prevalent, primary healthcare workers may be able to identify these symptoms among PWH, if future training differentiates between H-NCI and other commonly occurring co-morbidities, such as depression.
The paucity of primary healthcare workers administering H-NCI screening tools is consistent with reports on mental health screening among HIV service providers in this context (Mall et al., 2012). Medical doctors were the only cadre that were aware of common H-NCI screening tools such as the International HIV Dementia scale, although they had never used a screening tool outside of their undergraduate medical training. All cadres were in favour of learning to administer an H-NCI screening tool, to improve patient outcomes at their facilities and agreed that it would be feasible to administer a tool at this level of care.
There is still controversy about the clinical utility of screening for H-NCI, especially in low- and middle-income countries, as well as potential false positive diagnoses which could cause increased anxiety among PWH (Nightingale et al., 2014; Winston & Spudich, 2020). There are also questions around which healthcare worker cadre should screen, who should be screened and when screening should occur, due to high patient volumes, staff and resource shortages. Our findings show that should screening at a primary healthcare level be deemed appropriate, healthcare workers considered a combined effort from all cadres to be the best approach towards integration of H-NCI screening. Mall et al., (2013) highlight that the burden of care often falls to non-clinical healthcare workers due to time constraints and linguistic similarities. Similarly, medical doctors in this study suggested that counselors and nurses may be in a better position to ascertain important and accurate behavioural information during adherence counselling sessions or while patients wait to see a medical doctor, which could trigger the use of an H-NCI screening tool. In contrast, nurses in this study viewed medical doctors to be better suited to administer screening tools as patient management is determined by clinical healthcare workers. Our findings highlight that adherence counselors often referred patients when there were problems with memory or attention, suggesting that this cadre may be able to flag patients for screening and diagnostic confirmation by a medical doctor. Primary healthcare workers also suggested that ongoing monitoring for neurocognitive decline among PWH with functional impairment could take place during routine, annual visits.
Although medical doctors, nurses and adherence counselors predominantly provide healthcare to PWH, none had ever received training on H-NCI. There were mixed views on appropriate training methods among the different cadres. Previous H-NCI training targeting healthcare workers in South Africa are limited. In a Kenyan study, Cettomai et al., (2011) developed a one-day H-NCI training module for healthcare workers who were not medical doctors. This training utilised didactic lectures conducted by a trainer, group discussions and case studies. Several nurses and counselors preferred traditional face-to-face workshops similar to the training conducted by Cettomai et al., (2011), while some medical doctors and nurses favoured online learning. There were a range of factors that influenced these preferences, including time, resources and workload. Online training requires access to a computer, access to the Internet as well as strong Internet connectivity, which can be costly and not always readily available or accessible in low- and middle-income countries. Online training would, however, allow healthcare workers to access training at a convenient time without impacting on patient services. Face-to-face, didactic training has been widely recognised as a traditional approach to continued education present challenges as these sessions are hosted away from the facility for several hours at a time. As a result, healthcare workers would have difficulties attending due to patient volumes and staff shortages. Considering these challenges, healthcare workers favoured brief training sessions spread over several days or weeks. Determining the best method for training among primary healthcare workers in low- and middle-income countries require further investigation.
Methodological Considerations
There were several methodological considerations in this study. Firstly, our data were collected at the healthcare facility, resulting in distractions or disruptions during the discussion. The initial FGDs could not exceed the scheduled weekly staff meeting time, which was 90 min, to allow staff to continue providing services to patients accessing care at the facility. In-depth interviews were conducted to supplement the brief FGDs. Finally, our findings rely on healthcare worker self-reports only as we did not observe the practices of healthcare workers.
Recommendations
There is a need to disseminate information regarding the varying degrees of severity of H-NCI and the potential adverse outcomes experienced by PWH with functional impairment. Training targeting medical doctors, nurses and adherence counselors focussing on H-NCI and skills to successfully use a readily available H-NCI tool, could have potential benefits in this setting. Our findings show all cadres desired training to implement H-NCI screening services to improve care. It is, however, unclear how screening for H-NCI should be implemented and distributed amongst the different primary healthcare cadres, thus requiring pilot research to explore the appropriateness of each of the three groups in administering an H-NCI screening tool. Assessments of feasibility and acceptability, reflective of current practices in a primary healthcare facility, may then be conducted to inform decision-making for future programmes and potential integration into primary healthcare services.
Conclusion
There is limited knowledge of H-NCI screening tools among primary healthcare workers, and screening practices were uncommon. There is also a paucity in previous training for cadres providing frontline HIV healthcare services in South Africa. Our findings show that H-NCI training is desired; however, there are few programmes available in this setting, especially for primary healthcare workers who do not receive specialist training. In-field training targeting healthcare workers in this setting would be useful to equip healthcare workers with knowledge to recognise the signs and symptoms of H-NCI as well as the skills to administer screening tools at this level of care. Training healthcare workers at a primary healthcare level, where most people living with HIV access care, would be useful to understand the feasibility of H-NCI screening at this level of care. This should be followed by research examining the appropriateness and acceptability of H-NCI screening among the various cadres providing services at these facilities to determine which cadres are best suited to administer an H-NCI screening tool.
Footnotes
Acknowledgements
The authors wish to thank the Department of Health for their assistance, all facilities and healthcare workers who participated in the study. The doctoral candidate places on record her thanks to the South African Neurocognitive Association (SACNA), The National Institute for Human and Social Sciences (NIHSS), in collaboration with the South African Humanities Deans Association (SAHUDA) and the David and Elaine Potter Fellowship programme for their continued support.
Author Contributions
All authors contributed to the development, revision, and final review of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.