
Abstract
The purpose of this study is to investigate the patient’s perspective on physical activity as treatment modality for irritable bowel syndrome (IBS). An interpretive phenomenological analysis (IPA) approach was used to examine the experiences of IBS patients with physical activity, through in-depth interviews with 11 female IBS patients. Experiences with physical activity varied substantially among patients. Patients attributed negative experiences with physical activity to embarrassment, anxiety, inability, and symptom deterioration. Positive experiences with physical activity were attributed to symptom relief and improvements in overall health. Accordingly, patients discussed how they considered the application of physical activity in respect of IBS. Disease activity and the timing, type, and intensity of physical activities all could alter a patient’s response to physical activity. Physical activity seems to relieve complaints in most scenarios; however, a personal approach is required to tailor physical activity to the needs of each patient.
Keywords
IBS is defined as abdominal pain in relation with altered defecation (Brandt, 2009). The global prevalence of IBS is estimated at 9.2% according to Rome III criteria compared with 3.8% according to Rome IV criteria (Oka et al., 2020). Prevalence of IBS is more common among women (OR 1.46; 95% CI = 1.33–1.59) (Lovell & Ford, 2012) and prevalence seems to vary substantially between countries. According to qualitative research, IBS compromises the everyday life of patients, due to limitations in professional, personal, family, and social domains (Harvey et al., 2018). Living with IBS often means that the lived body becomes unfamiliar and unreliable (Sahlberg-blom & Nyhlin, 2009). Pharmacological treatments are often ineffective and cause unwanted side effects (Harvey et al., 2018). Patients seem best supported by recognition of their lived experiences and provided with the opportunity to participate in their own care (Håkanson et al., 2010). Therefore, patients learn to self-manage their condition by modifying their lifestyle, for example, physical activity, sleep and stress management, and dietary strategies (Chey et al., 2015).
Physical activity has been shown to reduce somatic symptoms (Henningsen et al., 2007) and stress (Schumann et al., 2016), improve emotional well-being (Johannesson et al., 2015), and reduce the risk of several gastrointestinal (GI) diseases (Peters et al., 2001). Therefore, increasing the level of physical activity may be effective in relieving IBS symptoms. A thorough perusal of literature reveals that low to moderate intensity physical activities can significantly reduce IBS symptom severity score (IBS-SSS). IBS-SSS is frequently used as clinical parameter to examine the severity and frequency of abdominal complaints and the extent to which IBS interferes with patient’s everyday lives (Francis et al., 1997). Interventions that involve running, jogging, cycling, and swimming cause significant reductions in IBS-SSS compared to their control groups (Daley, Grimmett, Wilson, Corporation, & Roalfe, 2008; Fani et al., 2019; Hajizadeh Maleki et al., 2018; Johannesson et al., 2011). Moreover, one study reports that the significant improvements in IBS-SSS persisted after a mean follow-up of 5.2 years (Johannesson et al., 2015). Similarly, yoga interventions resulted in significant reductions in IBS-SSS (Evans et al., 2014; Kavuri et al., 2015; Schumann et al., 2016; Shahabi et al., 2016). Thus, low to moderate intensities physical activities seem effective for IBS symptom relief.
Quantitative studies help establish the effectiveness of physical activity on IBS symptom relief at group level. However, this does not account for the individual variation in the subjective experiences of patients. Therefore, qualitative research is needed to gain insights into the various patient experiences of physical activity and IBS symptoms. This information is crucial to decide whether, and how, physical activity can be applied as treatment modality.
To our knowledge, only one qualitative study, reported in two articles, examined the experiences of IBS patients in relation to physical activity (Johannesson et al., 2018; Johannesson et al., 2019). Patients report that physical activity can help normalize bowel movements, and improved abdominal pain and gas handling (Johannesson et al., 2018). However, patients also report how IBS limits their capability for physical activity (Johannesson et al., 2019). In this study, all patients had already increased their level of physical activity in a previous intervention study.
Thus, no other study has explored qualitative data on the relationship between physical activity and IBS complaints. Besides, existing literature indicates large heterogeneity among IBS patients’ experiences, which highlights the importance of adjusting research and health care to the individual needs. Therefore, this study aims to examine the experiences of IBS patients who receive standard care, and who are physically active at different levels.
Methods
Choice of Methodology
Interpretive phenomenological analysis (IPA) was chosen as the study design, using semi-structured interviews for data collection. IPA allows for a detailed examination of personal lived experiences rather than describing experiences to existing theoretical preconceptions. It is suitable for examining topics that are complex, ambiguous and emotionally laden (Smith & Osborn, 2015), thus, matching the nature of IBS symptoms.
In order to formulate general claims about experiences with physical activity and symptoms, personal experiences are discussed in-depth. The interviews aim to capture the full range of experiences that result from various diagnostic and treatment journeys. Such experiences may cause patients to hold a certain belief or attitude toward physical activity. A better understanding of these experiences helps create a contextual understanding of how patients construct their beliefs and attitudes toward physical activity. In this way, IPA helps understand how IBS patients ascribe meaning to their experiences in their interactions with their environment.
Recruitment
Five participants were recruited through the IBS-outpatient clinic of Hospital Gelderse Vallei (ZGV). Another six patients were recruited via social media platforms of an IBS patient association. No preconceived recruitment strategy was used in order to gather a diverse study population. Patients were eligible for inclusion if their IBS diagnosis was confirmed by a medical doctor. Patients with an organic GI disorder or former bowel surgery were excluded. Saturation of information obtained from interviewing a heterogenous population usually occurs around 12 participants (Guest et al., 2006). After interviewing eight patients, most responses overlapped or resembled the responses in past interviews, indicating saturation. Therefore, it was decided that 11 interviews were adequate to reach sufficient saturation of information in this study.
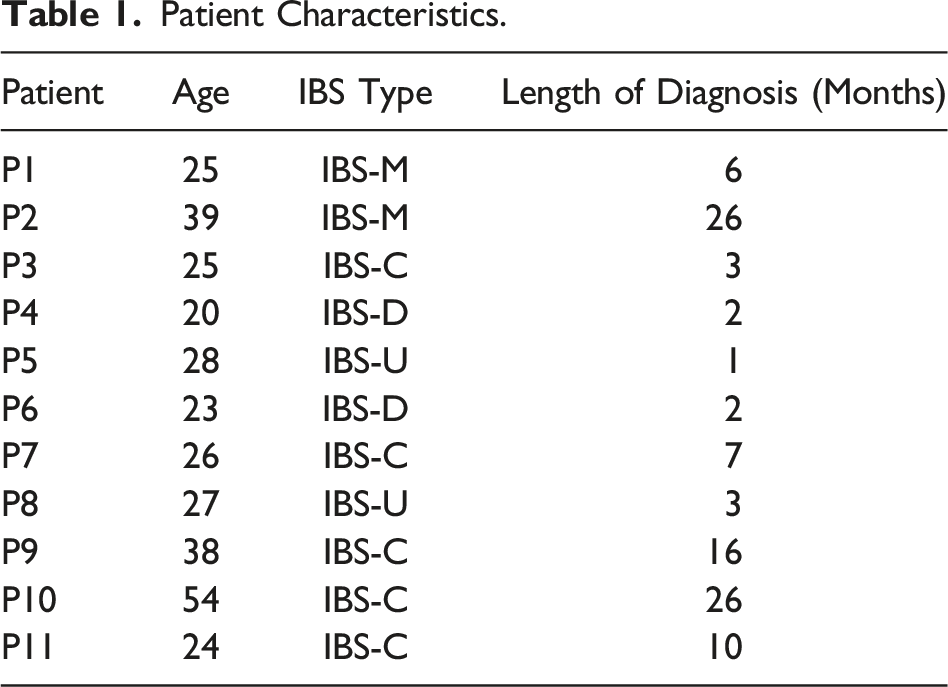
Participants
Patient Characteristics.
Data Collection
Interviews were semi-structured, and the main interview questions (see appendix) were adopted from earlier qualitative research (Johannesson et al., 2018, 2019). The questions were asked to identify the patient’s overall relationship with IBS; the patient’s motives and positive experiences related to physical activity; and the patient’s hindrances and negative experiences related to physical activity. Additional questions about the type and intensity of physical activity were added based on a systematic literature review about the relationship between exercise and abdominal complaints (Costa et al., 2017). Finally, the patient was asked to elaborate on the potential interactions between causative factors related to physical activity that could affect his or her abdominal complaints.
In addition, the interview guide was supplemented in consultation with a gastroenterologist, an IBS caregiver, and an IBS physiotherapist, with questions about the prerequisites for patients to do or enjoy physical activities.
The interview guide was tested in three pilot interviews. Some topics in the interview guide were too specific or irrelevant for patients. Therefore, the interview guide was adjusted to be more in line with the patients’ perspectives, and started by asking “What does IBS mean to you?”
Field notes were made during the interview to summarize the patient’s view. Follow-up probes were used to encourage the patient to exemplify and elaborate, as well as to correct misunderstandings. Interviews lasted approximately 30–90 mins and were audio- and video recorded. Interviews were held online via MS Teams and Zoom to fulfill COVID regulations.
Analysis
Recordings of the interviews were transcribed verbatim with AmberScript and coded in Atlas.ti. A predefined (i.e., deductive) set of codes was based on the interview guide and additional codes emerged inductively during analysis. First, codes were applied for similar phrases, patterns, themes, sequences, and important features. Then, codes were grouped in subthemes. Each subtheme represents a sequence of similar experiences, thoughts, or beliefs. After categorizing the subthemes, three key themes emerged that were typical for all interviews. The key themes and their subthemes are summarized and supported by relevant quotations in the results section. These quotations were translated (Dutch-English).
Ethical approval
Ethical approval was granted for this study by the Medical Ethical Commission of Wageningen University. Patients were informed about their confidentiality and the procedure of the interviews. Before participating in the interview, all patients signed an informed consent for the recording and transcription of the interviews and for anonymous quotation of their responses in this report.
Findings
Interviews
The heterogeneity in the sample resulted in divergent and unique interviews. All patients reported symptom fluctuation over time. Symptoms and flare-ups felt hard to predict. Some patients were very open and talkative. More introverted patients required more follow-up questions and probing. Some patients had great bodily awareness and were able to recall specific experiences about the effects of physical activity on their symptoms. Others could merely describe how they believed physical activity affected their symptoms and health. The majority of the patients developed a sense of alertness and strong will to manage their condition. Two patients felt more dejected by their symptoms.
Interplay Between Physical Activity, Nutrition and Stress
The majority of the patients knew how to modify their lifestyle in order to reduce their symptom severity. Nutrition, stress, sleep, and physical activity were the main lifestyle factors that could interact with IBS. Nutrition was often the major trigger for abdominal complaints. Dietary adaptations such as a diet low in fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAP) were often helpful. However, managing food intake could also be stressful. Furthermore, many patients thought that stress was closely related to abdominal complaints. High levels of perceived or underlying stress could induce flare-ups. Anxiety for or the presence of symptoms could further aggravate stress. Stress could also cause patients to eat unhealthy and exercise less. Moreover, patients emphasized the importance of sufficient sleep and time to relax to reduce perceived stress and GI distress. Physical activity was sometimes reported to cause direct symptom relief. However, relief of symptoms could also be the result of the indirect effects that physical activity exerts on nutrition and stress management.
Key Themes
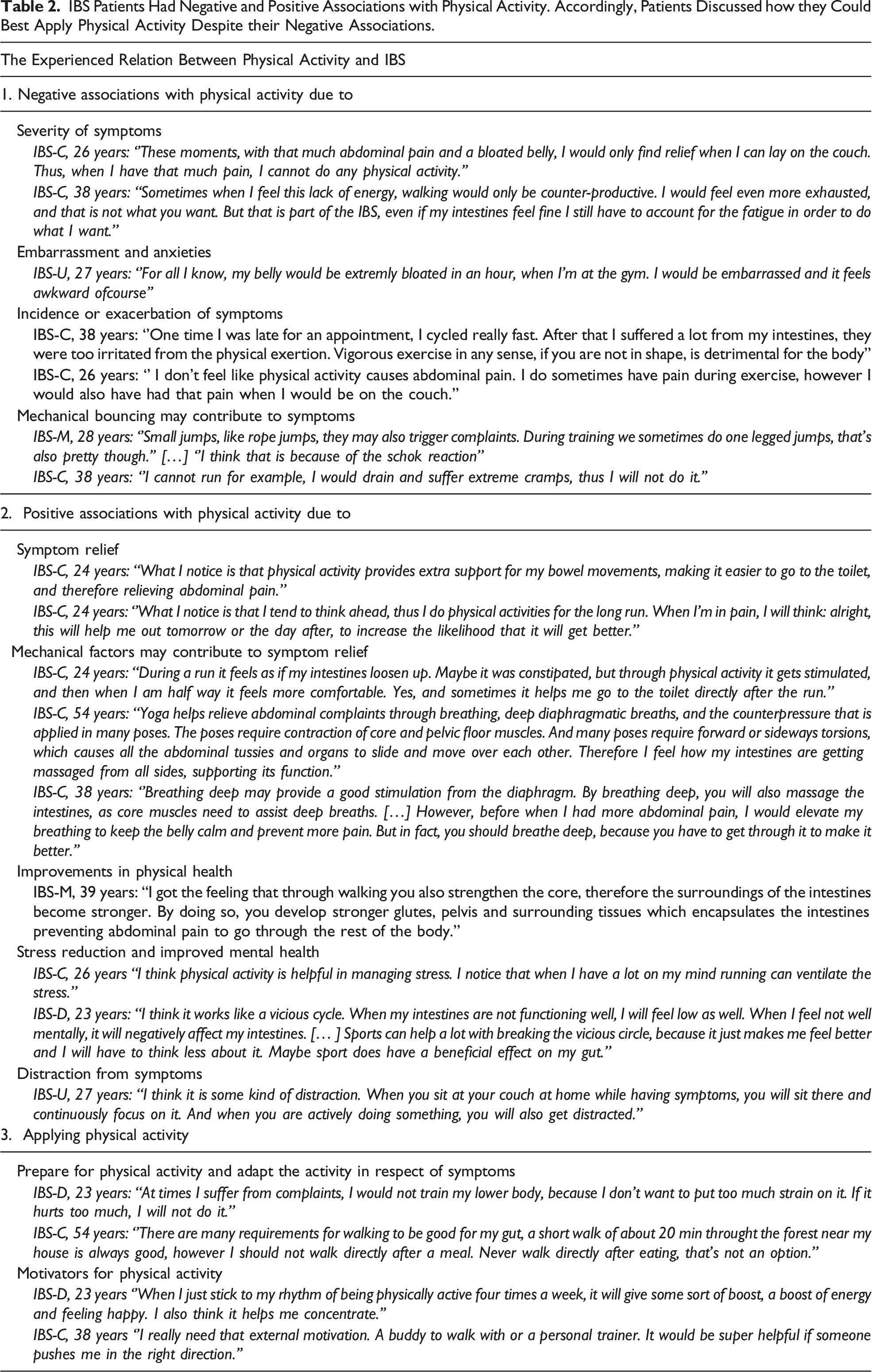
IBS Patients Had Negative and Positive Associations with Physical Activity. Accordingly, Patients Discussed how they Could Best Apply Physical Activity Despite their Negative Associations.
Negative Association Regarding IBS and Physical Activity (Two-Ways)
Most patients were well aware of the health benefits of physical activity. However, IBS was often reported to hinder patients in their capability for physical activity. A few patients explained that physical activity occasionally caused or exacerbated symptoms.
The Severity of Symptoms Can Form an Obstacle for Physical Activity
Several patients reported abdominal pain as a main reason to withdraw from physical activity. In extreme cases, patient could only find relief through resting or sleeping in fetus posture. Rumbling of the belly and frequent bowel movements could also withhold patients from physical activity. Some patients discussed that a lack of energy could withhold them from being physically active. The lack of energy was attributed to constipation and/or disturbed digestion and was distinct from mental fatigue. As a consequence, some patients found it too exhausting to be physically active. In addition, some patients were forced to walk hunched over due to abdominal pain. This caused severe pain in the back in one patient. Another patient suffered from fibromyalgia, a disorder characterized by skeletal muscle pain and fatigue, which often coexists with IBS (Veale et al., 1991). These co-morbidities also limited patients' capability for physical activity.
Embarrassment and Anxieties
Most patients shared how unpredictable symptoms could be. As a consequence, some patients felt anxious for the incidence of symptoms during physical activity. Some patients reported to be embarrassed about their bloated belly, whereas others were afraid of incontinence during a physical activity. While easy toilet access was often a requirement for IBS patients, one patient stressed the importance of privacy at the toilet as bowel movements could be accompanied by awkward noises.
Incidence or Exacerbation of Symptoms During Physical Activity
Some patients recalled how symptoms exacerbated during physical activity. The reason why exacerbation of symptoms occurred was not always clear; however, for some patients, it seemed clear that vigorous exercise could be a trigger. High intensity or prolonged exercise was often reported to induce or exacerbate abdominal complaints. An elite athlete discussed that the intensity of her training regimen could be a causative factor for abdominal complaints. Mainly aerobic interval training, with little rest between the runs, was a frequent cause for complaints during physical activity. In addition, the athlete reported to experience more complaints in preparation to (qualification) races, partly due to competition nervousness. Moreover, the athlete reported to experience fewer or no symptoms during holidays.
Mechanical Bouncing may Contribute to Symptoms
Several patients reported negative experiences with running and jumping. Running was often avoided or rescheduled if mild symptoms were present. Other patients did not share this aversion for running. A few patients believed that up and down movements, typical for running and jumping, could induce abdominal complaints. A patient reported to experience more abdominal complaints related to running if she did not evacuate in advance. Another patient explained to prefer stair walking over treadmill running because the former minimizes up and down movements.
Positive Associations with Physical Activity
Patient motivation for physical activity was often attributed to improvements in physical and mental health. The majority was convinced that physical activity could relief abdominal complaints. However, positive effects of physical activity were not systemic and, in some cases, unnoticed. Unpredictability of IBS and interaction with other causative factors made it hard for some patients to recall how physical activity affected their symptoms.
Physical Activity for Symptom Relief
Several patients explained that physical inactivity could exacerbate or cause symptoms. Sedentary work was believed to negatively affect their symptoms. The majority of patients reported how either walking, cycling, yoga, running, or team sports could help relieve abdominal complaints. For some, physical activity could directly relieve symptoms, whereas others believed it helped them manage their symptoms over time.
Mainly low intensity physical activities including walking, cycling, and yoga could help relieve abdominal complaints. One patient stated that walking was more effective in relieving abdominal complaints than weightlifting. Several patients believed that physical activities of low intensity could enhance digestion, stimulate motility, and induce bowel movements.
Three patients reported that certain stretches, movements of abdominal organs, and applying counter pressure at the abdomen during yoga practice helped to relieve symptoms. Breathing and stress relieve during yoga practice were also attributed as beneficial for gut function.
Some patients claimed that running would be even more effective in relieving abdominal complaints than walking. On the other hand, several other patients reported how running could induce or exacerbate abdominal complaints.
Mechanical Factors may Contribute to Symptom Relieve
Relief of complaints was often attributed to the mechanical stimulations that occur during physical activity. As such, one patient stressed the importance of external stimuli for proper peristalsis of her intestines. Others reported that overcoming a shallow breath by deep diaphragmatic breathing could help reduce stress and relieve abdominal complaints. Breathing was believed to stimulate GI motility via the up and down movements of the diaphragm. Although, abdominal pain may withhold patients form deep breaths, purposeful deep breathing was believed to favor the patients’ symptom severity.
Improved Physical Health
For most patients, it was evident that sufficient physical activity could improve endurance, strength and energy levels. One patient explained why strengthening core muscles could reduce symptoms deterioration. Improvements in fitness level were thought to increase the capability for physical activity. Besides, a better overall health was thought to help reduce symptom severity.
Stress Reduction and Improved Mental Health
The interviews revealed that patients clearly experience a relation between stress and abdominal complaints. Physical activity was often found to be helpful in relieving and managing stress. Many patients reported how physical activity helped them cope with stress and pressure. Besides, patients reported physical activity to contribute to a better mood, better focus, and better overall mental health. In addition, some patients illustrated the relation between stress and abdominal complaints as a vicious cycle. Feeling stressed or feeling low could contribute to symptom deterioration and vice versa. According to some patients, physical activity could be helpful in breaking this vicious cycle, which could potentially relieve symptoms indirectly.
Physical Activity as Distraction for Complaints
Most patients reported how physical activity distracted them from pain and inconvenient feelings in the gut. One patient explained why she thought distraction through physical activity could be the reason for symptoms relief.
Applying Physical Activity in Respect of IBS
Thus, IBS may interfere with the patient’s capability and motivation for physical activity but can also help patients to manage their symptoms. Therefore, patients addressed how they could best apply physical activity with respect to IBS symptoms.
Preparation and Adapting the Activity in Respect of Symptoms
Several patients experienced that food intake in preparation for physical activity could affect the tolerance for physical activity. Eating smaller portions, extending the period between eating and physical activity was found to reduce the risk for abdominal complaints during the activity. Similarly, one patient found that defecating prior to running reduced the risk for abdominal complaints.
Awareness of symptoms and discomforts in the abdomen was often necessary to determine the appropriate physical activity and intensity for that moment. In the presence of symptoms, patients felt better off by doing physical activities that were less demanding for the gut. Therefore, patients often described how they would adapt or reschedule their physical activities according to symptoms or signs of GI distress. For example, patients would avoid running or resistance training of the lower body when they experienced mild symptoms. In some cases, patients would prefer the gym over outdoor running to ensure toilet access.
Moreover, patients reported to lower the intensity of the activity to prevent putting too much strain on the body. Doing low intensity activities at times of mild symptoms would often help to calm down troubling feelings in the abdomen and relieve pain and symptoms. Therefore, some patients stressed that even though they felt troubled with complaints, they knew low intensity physical activity would be helpful. Patients also stressed that when pain and symptoms persisted or exacerbated during an activity, it would be best to stop immediately. In these moments, patients felt as if the activity was to demanding for their body and caused more symptoms then it would solve.
Motivators for Physical Activity
Most patients in our study took pleasure in physical activities, provided they were not hindered by GI complaints. Frequently reported motivations for physical activity were as follows: the joy in a sport or activity, challenging yourself, being outdoors, stress relief, mood improvements, and maintaining or working on overall health. Patients described that in times with plenty physical activity they experienced increased energy levels, improved endurance and strength, fewer symptoms, improved digestion, less stress, better moods, and healthier decision making. In turn, improved mood and fitness was believed to enhance the capability and motivation for physical activity. Therefore, patients believed that frequent and sustained physically activity was key for managing IBS.
Not all patients felt a strong intrinsic motivation for physical activity. For these patients, it was often helpful to seek motivation in the potential health benefits of physical activity or through external motivation. Making physical activity a habit or arranging external motivation (e.g., a personal trainer or membership) was thought to be helpful. Some patients also addressed how social aspects and challenging themselves could help motivate for physical activity.
Discussion
Results of this study display the experiences of IBS patients regarding physical activity. Although patients report diverging experiences, most patients in this study consider physical activity as treatment modality, based on their experiences. All in all, although potentially beneficial, patients also report limitations and obstacles for physical activity. The results are in line with the previous finding that patients require physical activity but may be hindered by IBS symptoms in their capability for physical activity (Johannesson et al., 2019). Therefore, patients were often forced to reconcile physical activity with their symptoms.
Low intensity activities were most often well tolerated and beneficial for symptoms, which is in line other studies (Zhou et al., 2019). Specifically, patients reported that physical activity could help facilitate bowel movements, cause changes in abdominal pain and help handle gas and feelings of bloating (Johannesson et al., 2018). Similar results have been obtained in this study. However, a few patients believed physical activity to be ineffective in relieving symptoms. Although the benefits of physical activity for IBS may seem evident from literature, the experienced effects thus diverge among patients.
High demanding physical activity was often experienced as troublesome by IBS patients. These experiences are in accordance with the theory that the risk for abdominal complaints (except for constipation) increases as exercise intensity becomes vigorous (Peters et al., 2001). Moreover, the increased sensitivity to abdominal complaints may predispose IBS patients to exercise-related GI distress. Increased motor reactivity to stimuli such as stress, impaired transit of bowel gas, autonomic dysfunction, visceral hypersensitivity, cholecystokinin, and altered immune activation could predispose IBS patient to exercise-related GI distress (De Oliveira & Burini, 2009). This may partly explain why patients would recall the least tolerance for intensive physical activity when the gut was compromised.
Mechanical factors such as bouncing of the abdomen, core contractions or rotations, and breathing were believed to affect abdominal complaints. Running and jumping were often poorly tolerated which was attributed to the up and down movements of the abdomen. In literature, this phenomenon is called mechanical bouncing, which can increase intra-abdominal pressure and organ movement (Viola, 2010). Besides, the up and down movements may interfere with prostaglandin release (Gil, Yazaki, Evans St Bartholomew, & Royal, 1998). These alterations are hypothesized to affect intestinal motility and cause exercise-induced abdominal complaints such as runner’s diarrhea (van Nieuwenhoven et al., 2004). The effects of mechanical bouncing may explain why patients have had negative experiences with running and jumping. However, one IBS-C patient experienced greater symptom relief in response to running compared to walking. In addition, patients believed that mechanical vibrations initiated by walking could improve digestion and facilitate bowel movements. Thus, the experiences with mechanical bouncing are divergent and may depend on the intensity of the bounces.
One patient in this study reported how strengthening the core muscles could help encapsulate the intestines preventing pain to exacerbate. A similar finding was reported in another study. This patient had learned that increased tension in the core muscles after training could hold back the perceived bloating (Johannesson et al., 2018). No further literature was found to support the relationship between core training and symptoms reduction in IBS patients. Besides, counterpressure, torsions, and stretches during yoga were also believed to relieve symptoms. Yoga as treatment modality has been reviewed and studies show significant improvements in IBS symptoms (Zhou et al., 2019).
Some patients believed in diaphragmatic breathing to reduce abdominal complaints. There is reason to believe that enhanced breathing may improve vagal and sympathetic functions (Bordoni & Morabito, 2018). Moreover, IBS therapies such as relaxation techniques, cognitive restructuring, emotion-focused coping strategies, yoga, and mindfulness all involve diaphragmatic breathing. However, current data on therapeutic diaphragmatic breathing is lacking (Bordoni & Morabito, 2018).
Clinical Implications and Recommendations
In our study, we see a trend in favor of physical activity as potential treatment modality for IBS, which by no means proves that this is the case for all IBS patients. However, it seems highly relevant for IBS caregivers to consider and discuss physical activity as treatment option. Low to moderate physical activity in particular may offer symptom relief and improve overall health and could be advised to patients that are capable of increasing their level of physical activity. Complications such as fatigue, GI distress, and stress may limit the capability for physical activity. However, regular physical activity itself was often believed to reduce fatigue and stress and could therefore improve a patient’s capability and motivation for physical activity.
In addition, IBS patients have divergent experiences with physical activity. Therefore, clinicians must be well aware of the individual responses to physical activity before consulting patients to increase their level of physical activity. Monitoring symptom severity and creating awareness of the bodily responses to physical activity may help patients to tailor physical activity to their needs. Appreciation of the patients' lived experiences and the opportunity for patients to participate in their own care seems to be key for supportive encounters between patient and clinicians (Håkanson et al., 2010).
Strengths and Limitations
An important study strength is the diversity in levels of physical activity in our study group. The broad range of physical activity levels provided divergent attitudes and experiences with regard to physical activity and IBS. Therefore, the results of this study may cover the experiences of a substantial part of the female IBS patients.
The study also has a number of limitations. First, all participants were female, likely as a result of the female predominance in the prevalence of IBS (Chey et al., 2015). Thus, no data is obtained about male IBS patients. Second, most patients reported constipated symptoms, only a few suffered from recurrent diarrhea. This is in line with the higher prevalence of constipation generally observed in Europe (Peppas et al., 2008). Besides, diarrhea and uncontrolled evacuations may imply more embarrassment and anxieties related to physical activity which may have heightened the burden for IBS-D patients to participate in this study. Interviews in another study revealed that IBS-D patients also experience benefits on bowel movement initiation in response to physical activity (Johannesson et al., 2018). This is remarkable as colonic transit time is believed to accelerate in response to physical activity (Rao et al., 1999). Third, as a result of COVID measures, the interviews were held online. The digital environment is less familiar and safe environment compared to home, which may create an extra burden for sharing sensitive information. Besides, technical issues did sometimes interfere with the quality of the conversation, which could have affected the interpretation and responses at both sides of the interview.
Future Research
Future studies are warranted to further elucidate the potential of physical activity as treatment option for IBS. Future studies may establish which intensities are tolerable and beneficial for patients in the presence or absence of symptoms. Through monitoring symptom severity, level of perceived exertion, heart rate, and markers of intestinal injury during and after physical activities studies may clarify what intensity is best suited for a patient.
Besides, the effects that exercise may have on GI motility remain elusive (Costa et al., 2017). Research may clarify how physical activity and mechanical factors interfere with GI motility. In addition, studies may test the efficacy of therapeutic diaphragmatic breathing and other core movements on IBS symptoms. IBS yoga programs may be developed to promote symptom relief. At last, fatigue can be a huge limitation for the patient’s capability for physical activity. Future research may establish how patients can overcome IBS-related fatigue.
Summary and Conclusion
IBS patients have divergent experiences with physical activity. Physical activity at low to moderate intensities was often perceived as beneficial for symptom relief and overall health. However, IBS may limit patients’ capability for physical activity or cause undesired experiences during activities. In order to enjoy and benefit from physical activity, patients adapt the activity with respect to their symptoms. IBS caregivers must personalize physical activity advice to meet a patient’s capability and increase the likelihood of beneficial experiences. Future research is required to clarify the effects of physical activity for each individual IBS-subtype or symptom. Besides, studies are warranted to clarify how exercise intensity and the degree of mechanical bouncing may induce or relieve abdominal complaints and increase quality of life in IBS patients.
Footnotes
Acknowledgments
We gratefully thank Margreet Jansen; Hans Zwerver (Hospital Gelderse Vallei), and the Dutch IBS-interest organization for their contribution in the recruitment. We also like to thank the patients who volunteered to participate in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
In line with the Dutch ‘Medical Research Involving Human Subjects Act’, the Medical Research Ethics Committee of Wageningen University deemed this study not to be subject to full assessment.
Informed Consent
All patients provided written informed consent prior to enrollment in the study.