
Abstract
There is increased emphasis on adopting positive health and aging policy goals for heterogeneous older populations, and recognition of the role that participatory research approaches can play in supporting their implementation. However, questions remain about how to represent the marginalized experiences of some older populations within such processes. With a focus on older Irish ethnic Travelers and older homeless adults as two vulnerable populations in Ireland, this article presents and critically discusses a participatory approach developed to integrate marginalized older adult perspectives on positive health and aging in a multistakeholder research and development process. The qualitative methodology is first detailed, incorporating methods that harness collaboratively derived views and individual narratives (e.g., focus groups; consultation forums; in-depth interviews). Critical reflections on research implementation and specific considerations relevant to these populations are presented (e.g., trust building; one-to-one facilitation), with lessons then drawn for the design of multistakeholder participatory approaches with marginalized older populations.
Keywords
Introduction
The increasing need for cohesive policy on older people and health and social care has been recognized as a political priority in recent years (European Commission, 2021), and is reflective of a greater push towards positive health and aging (PHA) concepts, such as healthy, active, and positive aging. With significant emphasis now placed on person-centered values, policies must be cognizant of heterogenous older populations’ multifaceted needs (Carlsson & Pijpers, 2021; WHO, 2015). This is in the face of established critiques of the homogenizing effects of some PHA constructs (Foster & Walker, 2015), neglecting the interests of sub-groups, and rendering interventions ineffective. As such, there is growing interest and pressure to engage in research-led processes that incorporate participatory approaches to elucidate the diverse health and social contexts of older adult lives. This is in addition to having to account for professional stakeholders’ views so as to generate a holistic understanding of challenges, and solutions. Whether the concentration is on research, or service improvement programs, more structured forms of co-production, and public engagement and patient involvement with older people are now evident (Greenhalgh et al., 2019; Schilling & Gerhardus, 2017).
Notwithstanding these developments, representing the marginalities of lived experiences of some older populations, and the intersectionality of their identities, has been recognized as a significant challenge to operationalize (Cush et al., 2020; Littlechild et al., 2015). It is this challenge that is the focus of this article. We present and critically discuss a participatory approach developed to capture and integrate diverse, marginalized older adult perspectives in a multistakeholder research and development process. Consideration here is given to co-producing PHA understandings and recommendations with older Irish ethnic Travelers and older adults experiencing homelessness as two vulnerable populations in Ireland, whose voices are largely absent from research, policy, and practice spheres (Gibney et al., 2019), who developed indicators for positive aging for Irish Travelers, and Walsh (2013), who explored aging and dying amongst the Irish homeless population, are two exceptions to this from the grey literature. First, the relevant literature on participatory approaches in health research, and the general challenges in capturing perspectives of older populations is reviewed, followed by a short description of the older Traveler and older homeless populations in Ireland. Next, we detail the methodology developed for this research, and summarize specific considerations for these populations. We then provide critical reflections based on the implementation of the methodology. We close the article by drawing out lessons for the future development of multistakeholder participatory methods with marginalized older populations.
Participatory Approaches and Marginalized Older Populations
Participatory health research (PHR) approaches are credited with securing a range of benefits for health and social care research that targets innovation. This includes harnessing different forms of knowledge; the co-development of insightful methods; and the creation of impactful outputs (Fitzgerald & Walsh, 2017). PHR refers to a broad family of traditions and strategies which have been developed to enhance the real-world applicability of health research, in tandem with empowering participants to articulate their own needs/views (ICHPR, 2013). Maximizing the participation of target groups in all research stages, PHR harnesses equitable partnerships for wider societal transformation, and fairer resource allocation (Roura et al., 2021). When embedded in co-produced implementation models, these strategies can bolstered service reform, and enhance self-directed care (Flemig & Osborne, 2019). The international literature testifies to a multitude of different frameworks (e.g., Participatory Learning Action) that support participatory approaches (Flemig & Osborne, 2019), with many targeting marginalized populations (Kyoon-Achan et al., 2018; O’Reilly-de Brún et al., 2018), and some considering the specific position of older people (Hallett et al., 2017; Rudnicka et al., 2020; Sandholdt et al., 2020).
The application of these approaches, therefore, to the concerns of marginalized older adults in multistakeholder processes would seem to hold significant value. Systemic life-course disadvantage, and inconsistencies in access to health services, can reinforce entrenched forms of exclusion (Chau & Yu, 2010), and poorer outcomes for some groups of older people (Haas & Rohlfsen, 2010; Northwood et al., 2018). This is the case for older Irish Travelers and older homeless adults, who both can experience significant individual level risk and systemic marginalization from mainstream societal institutions (e.g. Cush et al., 2020). For such sub-sections of the population it is critical to recognize the intersectionality of experiences that can stem from group categorization and experience, and aging processes and constructions (Cronin & King, 2010). Participatory health research approaches may be a useful means to account for the range of needs and experiences across and within groups. This is in addition to the barriers that these strategies typically attempt to address, for example, supporting those with literacy issues and cognitive impairment (Liljas et al., 2017; Lourenço et al., 2021), and equalizing power differentials within research processes (Cook & Klein, 2005; Pratt, 2019).
However, co-methods are less developed for aging populations, with some older people likely to encounter challenges to participation (Cowdell et al., 2020; Schilling & Gerhardus, 2017). Reflecting, in relative terms, a wider paucity of research on older populations and participatory approaches (Cowdell et al., 2020), questions remain as to how to best support the involvement of marginalized aging populations in multistakeholder participatory research and development processes, where the need for impactful provisions is most present (Pratt, 2019). This is despite the recognition that policy and practice, and the research that supports it, must reflect older people’s lives to secure equitably PHA outcomes (Rudnicka et al., 2020).
At a base level, concerns persist about how to sufficiently represent diversity within older adult groups. Recruitment of marginalized older people for research is often challenging (Sandholdt et al., 2020), and can be due to a number of physical, social, psychological or structural factors (Lourenço et al., 2021). There can also be significant internal heterogeneity within sub-populations that requires specific consideration. As Machielse (2015) describes for socially isolated older people, there is a “…diversity of circumstances, ambitions and possibilities…” (2015, p. 338). For older homeless adults, this might include the reasons for, and the timing of becoming homeless (Grenier et al., 2016). For older Travelers, this might include generational variations in life experiences, for example, education, which may lead to different expectations (Jong et al., 2012). Similarly, accounting for the differential capacities and agencies within groups within a single study design can be problematic. Additionally, the optimum way to centralize the lived experiences of such groups in agenda-setting health research is unclear (Roche et al., 2020). Building trust—particularly among those who have experienced discrimination—can be a barrier to participation (Pratt, 2019). Fostering confidence so that participants voice their views can also be challenging, especially when professional “experts” are present (De Freitas & Martin, 2015). Furthermore, low expectations, and a relative appreciation for health status and services, or a hesitance to express dissatisfaction, can dilute the effectiveness of deliberative processes and their goal of reform.
These challenges result in the continuation of research approaches which neglect the most marginalized perspectives, hindering transformative change, and exacerbating inequities due to the promotion of the most dominant voices (De Freitas & Martin, 2015).
Older Travelers and Older Homeless Adults in Ireland
Older Irish Travelers in this research refer to people aged 50 years and over “…who are identified…[by themselves and others]…as people with a shared history, culture and traditions including, historically, a nomadic way of life” (Equal Status Act Ireland, 2000, Sec 2 (1)). Due to government policy to settle the Traveler community in the mid-1960s, the Traveler nomadic lifestyle was greatly limited, and while the vast majority are no longer nomadic, nomadism is viewed as vital to Traveler culture (Joyce, 2018). The majority of Irish Travelers now live in private dwellings, but only 20% own their own homes (68% in the general population) and 3% live in caravans and temporary structures (CSO, 2016), with repeated concerns that accommodation standards are a pressing issue for Traveler well-being. There are estimated to be 2639 older Travelers resident in Ireland. The Traveler community received official recognition as an indigenous ethnic minority in 2017. In this research, older adult homelessness refers to people aged 50 years and over who are currently or who have recently experienced rooflessness, houselessness, or inadequate and insecure accommodation (Amore et al., 2011). It is estimated that there are 1069 older homeless adults in Ireland (CSO, 2016). While the age structure of both groups are younger than the general population in Ireland (aged 65 or older: Travelers, 2.5%; wider population, 13%; older homeless people over 50 years, 15%), the two populations are increasing in size in line with demographic aging, and patterns for homeless populations and indigenous ethnic groups internationally (e.g., Woolrych et al., 2015). As with similar populations in other jurisdictions, both groups have lower life expectancies and higher rates of comorbidities, and are more likely to experience inequalities with respect to service access and social, economic, and health outcomes (Cush et al., 2020; Gibney et al., 2019; Woolrych et al., 2015).
Approach and Study Design
The study utilized a qualitative, participatory voice-led methodology, which was focused on capturing and promoting the “insideness” of the perspectives of older Travelers and older people experiencing homelessness. The methodology aimed to redress the deprivation of opportunities for these groups to guide work on this topic, and to embed their concerns as the central spine within the research design. In line with participatory health approaches’ emphasis on interdisciplinarity (Greenhalgh et al., 2019), the research team comprised of colleagues from social gerontology, public and primary health, and health policy. Project collaborators comprised of national health services, social inclusion organizations, an aging advocacy organization, and groups working with the two populations. Collaborators provided project oversight, assisted in accessing professional stakeholders, and advised on outputs.
The approach adopted principles of a participant-voice framework for the inclusion of marginalized populations in multistakeholder research processes (Fitzgerald & Walsh, 2017) Based on an applied program of work on community participation involving older people, children, and youth, and people with disabilities, the framework aims to support processes that create shared understandings of challenges and required responses. With a focus on understanding social context, ethical engagement, and the importance of real-life experiences, emphasis is placed on the emergence of different forms of knowledge from, in this case, older Irish Travelers, older homeless adults and professional stakeholders. The study approach was also informed by the social determinants of health, and life-course theoretical perspectives. The former guided consideration of how the methodology needed to gather insights into how differential impacts of structural forces and conditions of daily lives may drive PHA inequalities for the two groups (Sadana et al., 2016). The latter guided an emphasis on capturing how PHA trajectories may be derived from early-life experiences, transitions, and events (Alwin, 2012; Dannefer, 2003).
Recruitment considered age, gender, accommodation status, urban-rural location, health status, ethnicity, and for older homeless adults, the timing of homelessness. Recruitment protocols were developed with collaborators to ensure ethical and representative recruitment and was facilitated by gatekeepers (charities; representative groups; service providers) and supplemented with snowball sampling. However despite this and specifically targeted efforts, the study was not successful in recruiting homeless older adults currently living on the streets, and nomadic older Travelers. Although the samples did include individuals who had past and recent experiences of these circumstances, this is a study limitation and reflects the very hard to reach nature of sub-sections of the groups. Ethical approval was granted from the authors’ institution’s Ethics Committee, and informed consent was given by all stakeholders.
Consideration was also necessary in relation to the choice of specific methods. First, attention was given to older adult stakeholder backgrounds, bio-demographic characteristics, and the degree to which data collection techniques (e.g., focus groups; interviews) were likely to require adaptation. This included integrating approaches that could respond to differential education levels and literacy (especially for older Travelers), potential cognitive health issues (especially for older homeless people), and possible mis-trust amongst participants. Second, it was necessary to incorporate professional stakeholders’ views, while accounting for how their roles may alter power dynamics within group discussion methods (Cornwall, 2002). It was thus important to consider methods that could be both used in a consistent way with all stakeholders, but that were sufficiently flexible to support the participation of two heterogeneous older adult groups. Practical steps in this regard are outlined in the next section.
Data Collection and Methods
With reference to Figure 1, the study involved five data collection strands. Given our interest on multistakeholder processes, and the inter-stakeholder dialogue that arises during these processes, critical reflections presented in this article focus on strand 1—focus group discussions, strand 2—Consultative Forum 1, and strand 5—Consultative Forum 2. Each of these strands involved multistakeholder discussions and data collection, and brought people together to share and debate views and agree actions collaboratively for the research team to progress. These strands therefore provided a means of channeling perspectives into a decision-making structure that shaped the direction of the research, namely, (a) what topics to research—from strands 1 and 2, and (b) what recommendations to focus upon—from strand 5. As strands 3—peer research projects and strand 4 in-depth life-course interviews did not involve multistakeholder interactions and were designed to collect individual, in-depth experiences and views, reflections presented in this article are not based on these methods. However, as these strands provided the evidence-base for the recommendations derived in Consultative Forum 2, it is important to outline in brief the details of each method, and the sort of research data they collected, to provide a description of the overall methodology. Empirical findings from these strands, and further details on these methods, will be published in full in future articles. The majority of fieldwork took place in 2019 and early 2020, prior to the COVID-19 pandemic. Strand 5 (Consultative Forum 2) was conducted in December 2020 during the second wave of the outbreak in Ireland. Data collection strands (about here).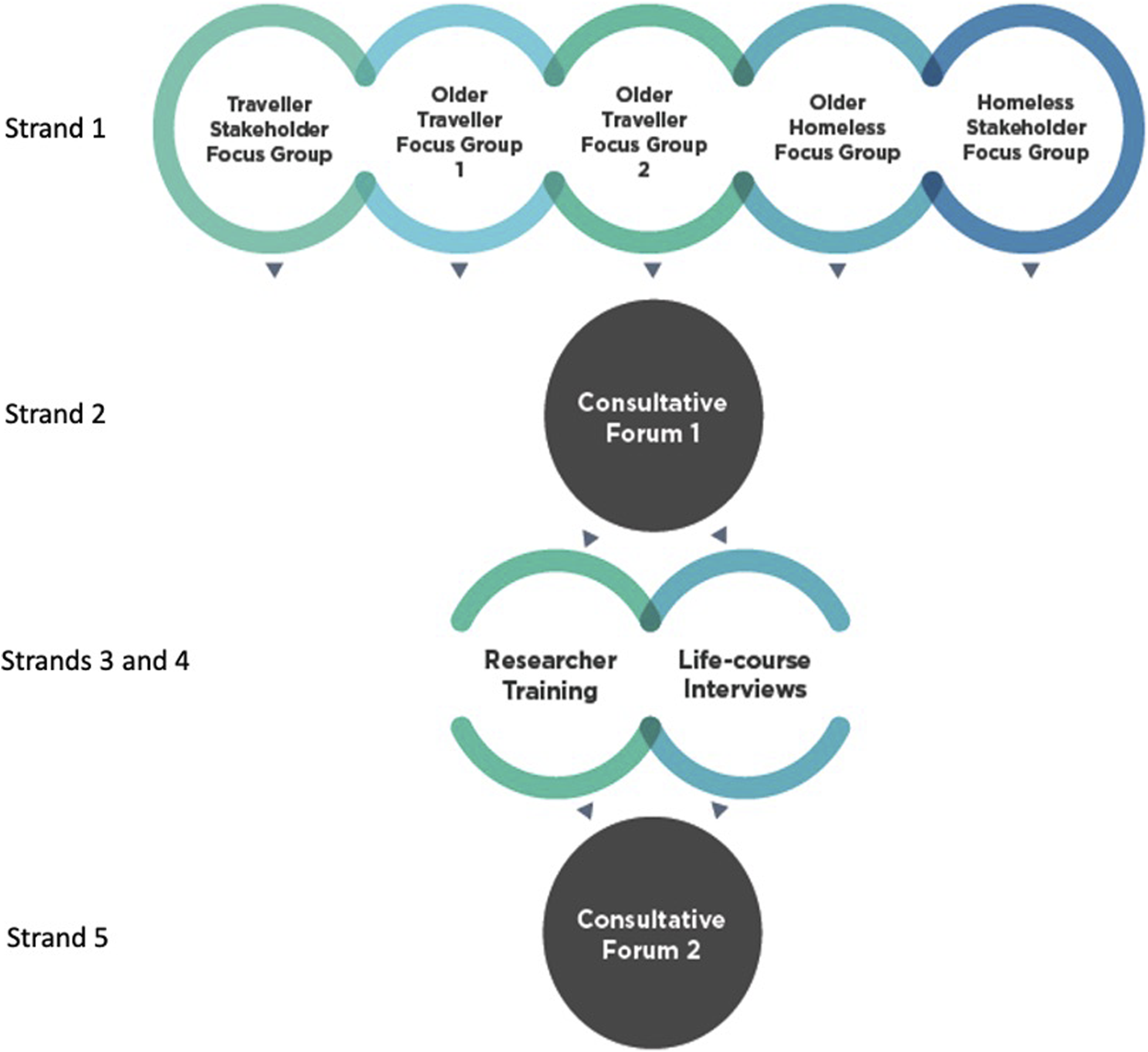
Strand 1—Focus Group Discussions: To contextualize challenges and opportunities encountered by the populations, five focus group discussions were conducted with: older homeless people (n = 5); older adult Travelers (two groups; n = 11 overall); and professional stakeholders working with and representing older homeless adults (n = 7), and older adult Travelers (n = 7). The professional stakeholders included representatives from public and third sector care providers, primary health organizations (charitable bodies), and advocacy groups. Discussions were held separately to establish each group’s perspective, the diversity of views within that perspective, and to build trust between individuals, and participants and researchers.
Semi-structured guides were developed to probe on three main topics: (1) meanings of good health, and positive aging; (2) life experiences and structural factors as determinants of later-life inequities; and (3) health and social care provision. While focus groups with professional stakeholders focused on sector-wide implementation issues, discussion with older stakeholders centered on lived experiences. To help ensure representation of voice amongst participants, Participatory Learning and Action (PLA) techniques were employed. Based on the work of Chambers (2007), PLA offers practical approaches where power asymmetries may exist.
These techniques were designed to bring individual and collective voice into discussions (graphical aids; structured individual and ranking exercises; timelines) so as to equalize power between groups (Chambers, 2002; O’Reilly-de Brún et al., 2018). For topic 1, a flexible brainstorm exercise was used to elicit participants’ responses. To counter possible literacy issues, general stock images on health and aging were displayed for participants to select pictures that supported their answers. In addition, and where appropriate, key points with one-word descriptors were noted on Post-it notes by participants or a member of the research team. These notes were then placed either on a flipchart or on a table alongside the images. For topic 2, and only for older participants, a timeline exercise was used to support responses to questions on life-course and structural factors. This involved facilitators drawing a life stage timeline, on a flipchart. Participants were encouraged to use images/Post-its and place these along the timeline. All discussions were audio-recorded and transcribed. Data were analyzed using an inductive thematic approach (Braun & Clarke, 2006), where a general coding structure was first developed from the initial reading of transcripts. The coding structure was discussed and agreed amongst the researchers who supported completion of the focus groups (typically three researchers per focus group), and refined iteratively through a re-reading of transcripts.
Strand 2—Consultative Forum 1: A Consultative Forum, which drew together older stakeholders and professional stakeholders from the focus groups, was conducted (n=9: 2 older homeless; 4 older Travelers; 3 professionals (homeless)). The Forum’s purpose was to review the findings of strand 1 and to agree priority areas to be investigated in the remaining strands. The forum drew out a collaborative perspective from across the groups, elaborating differences and similarities and supporting the emergence of shared understandings. A summary of findings from each focus group was first presented. This allowed participants to confirm/query the findings from their own group discussion, as well as to hear about the findings from other discussions. Participants were then divided into two small groups facilitated by a researcher and comprising a mix of professional and older stakeholders. The groups were asked to discuss two questions: “To what extent do the findings represent what is most important for PHA?” and “What are the common PHA issues/opportunities facing older Travellers and older homeless adults?” Individual responses were summarized on Post-it notes by participants or the facilitator, and later fed into a general plenary discussion. The final portion of the forum summarized common themes as areas that needed to be investigated further strands 3 and 4.
In strands 1 and 2, careful consideration was given to the accessibility of physical venues and discussion materials. Understandable language was a core element of both methods as was finding an appropriate means of framing questions that engaged older and professional stakeholders alike. To support full participation of older participants, one-to-one facilitation, and third-party assistance (from personal assistants) was used where appropriate.
Strand 3—Peer researcher Training: Supporting the empowerment of inclusion to tackle health inequities (Commission on Social Determinants of Health, 2008), five older Travelers and older homeless adults were trained as peer researchers to provide a systematic means of advancing their voices. Supported by three workshops, participants conducted their own projects using photo elicitation on research questions that reflected the common themes from Consultative Forum 1. Projects addressed identity and belonging, and care environments, and were the basis of two researcher briefs that peer researchers co-produced with the research team. Please see (Abushark et al., 2020) and (Sweeney et al., 2020) for full details of this training and the research projects.
Strand 4—Life-Course Interviews: In-depth life-course interviews were conducted with 22 older Travelers (8 male; 14 female) and 27 older homeless people (22 male; 5 female) (n = 49). Interviews lasted approximately one hour and consisted of three parts: (1) an open narrative portion which focused on a single question about health experiences; (2) an in-depth, semi-structured portion based on common themes agreed in the Consultative Forum; and (3) two life-path exercises where participants worked with the researcher to map out their health biography of positive and negative experiences, and their residential history.
Strand 5—Consultative Forum 2: The Consultative Forum was reconvened for the purpose of reviewing findings from strands 3 and 4, and agreeing policy/practice priorities and recommendations. The Forum involved nine participants (2 older homeless; 1 older Traveler; 6 professionals), and although it was due to take place one year after the first Forum, it was postponed due to the COVID-19 pandemic. The Forum was held virtually, 20 months after the first event. This introduced two major challenges. First, the membership of the forum had partially changed. Some professional stakeholders had moved posts and were replaced with representatives from the same organization. Some older Travelers and homeless participants were cocooning due to health vulnerabilities and without the ability to access online platforms were unable to take part. Second, significant efforts were required to ensure the accessibility of the online forum. Reminders of the research aim and methods, as well as summaries of findings (which had been organized into three thematic sections) were circulated in advance. The materials were made available both in document form and through three short videos (3–4 minutes in length each). The videos were sent to participants or to gatekeepers working to support older participants via phone message, or emails. Pre-test calls were organized with older Travelers and older homeless stakeholders, and facilitated by gatekeepers to troubleshoot technical challenges. In some instances, gatekeepers also provided more direct technical support, for example, one homeless participant attended via a video-link set up in a charity’s offices.
The Forum involved a recap presentation of the research rationale, aims and methods. This was followed by the presentation of findings in three parts: PHA meanings; PHA determinants; experiences of and preferences for health and social care. Each presentation was followed by an open discussion, with a focus on distilling priority areas and recommendations to inform future directions for PHA for the two groups. Draft suggestions were used to stimulate discussion if needed. A short break was provided between the presentations. During the discussions, each participant was in turn invited to comment on the findings and the conclusions, as well as contributing their own novel recommendations.
Research outputs
Research outputs were designed to reflect the co-production values of the project. In addition to the two peer researcher briefs, three briefing reports which featured the findings, and the recommendations arising from the Consultative Forum were produced.
Observations and Analysis for this Article
Critical reflections presented in this article are drawn from three sources of information for strands 1 (focus group discussions), 2 (Consultative Forum 1), and 5 (Consultative Forum 2). First, observation notes were made by at least one researcher, typically the same person, for all group discussions and forums. Along with recording insights related to the main research questions, researchers made notes on the following dimensions: aspects of each method that were successful and those that were problematic; the sort of adjustments that were made to circumvent these issues during implementation; and any observations regarding the nature of exchanges between participant groups during discussions. Second, all researchers involved in the focus groups and the consultative forums (in the majority of cases, comprising three researchers) were asked to reflect on these same dimensions. These reflections, along with the researcher notes, were then discussed at team debriefings post implementation to agree key observations. Third, audio recordings and transcripts were where possible used to validate these observations with quotations and exchanges identified that supported researchers’ notes.
Capturing Lived Experiences in Multistakeholder Processes: Critical reflections
We present critical reflections on the capacity of the research design to integrate the “insider” perspectives of marginalized populations, in a multistakeholder process that aimed to inform evidence-based PHA priority areas and recommendations. Reflections are grouped into six considerations based on observations. Participant quotations from strands 1, 2, and 5 are used to support these considerations and the key messages arising from each.
Harnessing curiosity and opportunities for critical reflection
One of the primary benefits to emerge from bringing the different groups together was the curiosity that was exhibited towards the other participant groups. Both older Travelers and older homeless individuals were interested to hear about their respective life experiences with respect to aging, inequities and service utilization. Hearing other individuals, from a different background, speak about their experiences helped participants from the two groups to understand each other’s position on the margins of society. For example, the following excerpt captures an exchange between the two groups in relation to Traveler ethnicity:
This learning, however, also helped to cement participants’ understandings of their own position and the fundamental issues challenging their PHA. For example, disconnection, displacement and the importance of creating a stable sense of home became strong themes for both of the groups, and emerged through their own recognition of this common ground. I think when you have a space, it doesn’t really matter how big the space is … you will make it a home, no matter how bad things are… (Male older homeless participant, focus group). …you’ll never have good health with the accommodation that there is Travellers living in… (Female older Traveller participant, focus group).
This helped each group to explore wider cross-cutting issues that had served as drivers of their experiences. The process illustrated how such multi-group interactions can capture significant processes of reflection with respect to aging, vulnerability and health. What also emerged was that some older participants never had the opportunity to meet and converse with peers in similar situations previously, which was especially evident during the focus group with older homeless adults, all of whom were male. While initially participants were hesitant to contribute, the reciprocity in dialogue emerged strongly, helping to sustain a commitment and interest amongst participants in the research and in returning to meet each other again. …you just don’t get meetings like this at all that I’m aware of and it has been helpful, very helpful for me and I think also for [other male homeless participant]… you find out where you stand for want of a better term. (Male homeless participant-speaking about returning for the Consultative Forum).
Reflecting inter-and intra-group heterogeneity and common concerns
The participants in this study consisted of a range of actors with significantly different life experiences. One of the challenges to emerge from working with such a diverse group was trying to identify a basis for fostering group rapport and encouraging the sharing of views. Particularly evident in the Consultative Forums, older participants were positioned at different points on a continuum of exclusion and integration, and possessed different degrees of experience with respect to participating in research, and consultation processes. However, these differences were not simply divided along group lines (older Travelers versus older homeless adults), with the diversity of experiences also apparent within both communities—even in these small samples. For example, some older homeless adults who lived a large proportion of their lives on the street had significantly different experiences to those who first became homeless in later life. Older Travelers, typically members of younger cohorts, living within settled accommodation had very different experiences to those who spent much of their lives in halting site or in roadside accommodation. Finding common ground was not straightforward, nor always necessary. But to help illuminate the potential for shared understandings of PHA, and policy actions that might address shared and differential needs, periodic reminders that these groups were participating as diverse populations were necessary. In this study, emphasizing aspects of potential marginalities and environmental uncertainty helped participants to think critically on how their perspectives were relevant to each other and the research.
Expressing collective versus individual voice
During the Consultative Forums the articulation of group perspectives sometimes gave rise to a power differential, and a dominance of one group’s voice—namely, older Travelers. The dynamic however did not emerge from a competitive attempt to exert a particular set of views over another. Instead it arose as a consequence of older Travelers possessing a more organized and unified voice. This was in part because these participants already knew each other (difficult to avoid in small ethnic community populations), and in part because of a more developed collective understanding, and literacy, around the marginal position of Travelers within society—reflecting a well-established discourse on Traveler rights at a grass-roots level. Some Traveler participants possessed significant confidence in this regard: …I wouldn’t care who they were and who they weren’t, I was talking to them anyway… If I’m campaigning for [Travellers’ rights] I know it’s the truth, you know what I mean… Let it be the corporation, let it be the local authority… or whoever it is, I know myself they can’t say: “Well [participant name], that’s not true, you don’t know that”, because I knows it’s true and I need it. So you built up your confidence from here. And you’re able to say what you’re able to say, what you want to say…. (Female older Traveller participant, focus group).
While in the wider study it was evident that this was not generalizable across all older Travelers, it was still a dynamic that had to be negotiated—especially relative to the more fragmented voices of older homeless participants, where understandably identities and experiences were less tied to group membership. The small group exercises, and the adapted PLA techniques assisted in this regard: participant groups were broken up; group moderation was easier with the smaller number of participants; and individual voice could be recorded (on Post-its) or expressed after direct requests for individual views. In addition, there was self-policing of behavior within group discussions. For instance, one older Traveler woman—an influential member of the community—asserted there were other voices that needed to be heard in the discussion. The following Consultative Forum excerpt, where a homeless participant is asked about accommodation challenges, helps to illustrate these sorts of exchanges:
Older Stakeholder-Professional Stakeholder Dynamics
Facilitating both older stakeholders and professional stakeholders in the same discussion illustrated other forms of power relations that also had to be accounted for in conducting this work. The documented potential for professional stakeholders to dominate group forums (Cornwall, 2002) was, as described, a concern in designing the Consultative Forums and resulted in a strong focus on providing specific space for older participants to express their views. However, unexpectedly, the potential for dominant voices appeared in some instances to be reversed. Professional stakeholders were careful not to assert their views in sessions, and seemed hesitant to articulate the strong opinions they had expressed within the professional stakeholder discussion, emphasizing instead the importance of the older participants’ voice. This is likely to have been a reflection of the social justice ethos that underpins the work of many community-based services and organizations within these two sectors. Professionals were conscious that these groups had few opportunities to inform development in this space: I think we tend to, we’re still very much top down in that we don’t listen enough… and I think there is a fear as well of people being assertive. They [homeless people] feel that they can lose their beds. That they can be excluded in some way, that they won’t be listened to. Or maybe they’re just is not a confidence you know that they have been here before. (Professional stakeholder, focus group).
Some stakeholder participants seemed to actively constrain themselves to ensure participants from the two communities had control of the session. These participants would have also directly engaged older adults, from both groups, to draw out their views and opinions in an effort to explore potential commonalities in experiences. Such constraint threatened to undermine the aim of the Consultative Forum, which was to promote an equality of dialogue, and maximize diverging viewpoints, in order to deliberate across perspectives and consolidate understandings. To counter this, facilitators would sometimes refer back to professional stakeholder focus group themes, and request stakeholders to explain or expand on these views.
Group and Individual Characteristics and Circumstances
A range of factors associated with the bio-demographics and life experiences created specific, although expected, challenges during implementation. First, low-literacy levels amongst some participants meant that individuals were not in a position to engage with text-based aspects of group exercises. Literacy issues were especially evident for older Traveler participants, and reflected long-standing structural barriers limiting participation in formal education. And then if you go in they’re giving you all these forms and you’re looking at them as if you have 10 heads or whatever… And that’s the way it is with a lot of older Travellers. And it’s embarrassing as well. (Female older Traveller participant, focus group).
While greater emphasis was placed on image-based exercises, and the role of facilitators in noting responses, literacy levels did challenge some of the adapted PLA techniques, such as ranking and timeline exercises. A number of participants appeared to find it difficult to follow, or lost interest in, these task as they involved some (albeit minimal) text annotation and labeling. Second, recruitment and retention of older Traveller and older homeless participants sometimes posed difficulties. Although gatekeeper recruitment was fundamental to the success of the study, it meant that the majority of participants were connected into existing services, shaping the sort of perspectives that featured in the research: …but they [homeless keyworker] came and they were saying to me… ‘I'm not here [participant’s name] to tell you what to do, I’m only here to tell you what we have to offer. If you want them all, you can have them all…’ And I think the service that they provide is a great service. (Male older homeless participant, focus group).
That said, and even with this sample bias, the logistics of conducting the study were often complicated by the extent of the challenges that faced members of these groups. Some participants never turned-up, or in one case left before a session commenced due to anxiety. A number of participants also withdrew due to complications relating to physical health. The engagement of other individuals was compromised by having chronic pain, and required personal care assistance during sessions. All of these factors, combined with the delay in hosting the second Consultative Forum, contributed to higher attrition rates, and was a reminder of the multi-morbidities that faced both groups. But issues of attrition were not solely concentrated amongst older adults. As with the first Consultative Forum, retaining the involvement of professional stakeholders could also be a challenge, particularly as their organizations were often under resourced. One stakeholder stated that their manager would not permit involvement in a second session (Consultative Forum 1) due to workloads. Finally, and with respect to gathering views on enablers of PHA, low expectations amongst older stakeholder participants appeared could create more favorable assessments of circumstances. My own father is 91 and… he won’t question anything… He won’t challenge it, and it’s like that with a doctor, a priest or a guard. They were seen as the people in authority. Particularly with a Traveller person… They’re just going to accept it. (Professional stakeholder, stakeholder focus group). So me personally, I shouldn’t be saying this, should I. But me personally, I think there’s almost too much that gets put into the servicing of people like us. (Male older homeless participant, focus group).
The focus on surviving from one day to the next, typically those from the homeless community, also meant that some participants had difficulty in projecting into the future and voicing preferences on the basis of likely need. This limited the aspirational nature of recommendations and was, as this stakeholder describes, reflective of challenges encountered in practice: They really don’t see two days ahead of themselves… But a lot of people just live right now this second. Survival. (Professional stakeholder, focus group).
COVID-19 and Capacities for Participation
Although, technically only impacting on one strand of the research design, the outbreak of the COVID-19 pandemic compromised the participatory and co-production value of the methodology in a number of different ways. First, and as already referenced, the pandemic delayed the hosting of the second Consultative Forum, compromising the momentum of the study, compounding issues of participant retention, and delaying closure and feedback for participants. Second, the need to conduct this Forum virtually functioned to exclude or added additional challenges for older participants. All older participants did not readily have access to communication technologies or online platforms. Due to social distancing and cluster outbreaks of COVID-19, older individuals could also no longer rely on their familial and community support networks for assistance. This was especially evident amongst the Traveler community, where high infection rates were prevalent in Traveler group housing schemes and halting sites. Such circumstances meant many gatekeeper stakeholders had to engage in significant efforts to provide technologies (e.g., SMART phones for older Travelers; access to office personal computers for older homeless adults), and virtual and face-to face technical support. Even for those who could participate in the Forum, the online medium of engagement stifled interactive dialogue and stripped older participants of a confidence in participation. Third, and finally, the pandemic impeded the engagement of the research team with project collaborators. Because of the outbreak, and the particular accommodation and care needs of these groups, collaborators were often on the front line of support during the pandemic. This compromised their capacity to engage in deliberations around dissemination and final outputs.
Concluding Remarks
This article set out to respond to a significant deficit regarding a lack of strategies for embedding the experiences of marginalized older populations in multistakeholder research and development processes. From the outset, it is important to acknowledge three limitations in the execution of the methodology itself, which compromises our capacity to appraise its effectiveness and transferability. First, this research did not capture the perspectives of homeless older adults currently living on the streets, and older Travelers who continue to live nomadically—although the samples did include those who had past and recent experiences of these circumstances. Second, and due to the impact of the COVID-19 pandemic, the study timeline extended beyond a duration that is conducive to sustained in-depth engagement. Third, participants were not directly canvassed as to their views of this methodology, and their assessment of its effectiveness in integrating their voices within the research process.
Notwithstanding these limitations, we argue this article holds valuable insights that may help advance the development of participatory approaches for marginalized sections of the aging population. The article’s central contribution, informed by theoretical concepts, is its illumination of six sets of considerations linked to supporting inter-group, and inter-sector dialogues that privilege the voices of these populations. This is not to over-emphasize the degree of innovation in the approach, or to purport to the novelty of its component methods, or indeed its messages. Many of these are well-established, and many of the supporting tools (i.e. PLA techniques) have been applied extensively to diverse populations (c.f. O’Reilly-de Brún et al., 2018). The combination of approaches, however, and the flexibility the design offers in capturing and integrating collaboratively derived views (of those who may be more connected), with individual (and perhaps more marginalized) narratives is valuable. So too we would argue is the establishment of these attributes within a central, evidence-based, decision-making study structure. In addition, there are four lessons that can be drawn from the analysis which may help to assist in developments outside of these specific groups, and outside of the Irish context.
First, the challenges encountered in operationalizing these sorts of methodologies for such older populations are likely to reflect to some degree the disadvantages that have accrued to these groups. In this study, education levels and literacy, mistrust, structural uncertainties, deficient material resources, and depleted capacity for engagement disrupted past and present integration levels for individual participants. In effect, these deprivations functioned as design criteria with regard to what this study’s methodological features had to account for, where possible. As others have noted for these and similarly populations (Greenhalgh et al., 2019; Woolrych et al., 2015), appreciating the life-course context of individual lives, and the historic circumstances of such groups within society is fundamental within participatory approaches. This is both in terms of embedding real-life positionalities within outputs, and in designing a process that is compensatory and empowering proportionate to the disadvantage encountered by participants. While not in all cases, the scale of marginalization can be more pronounced for older members of these groups, given their duration spent in precarious conditions. In line with universal proportionalism (Marmot et al., 2010), multistakeholder approaches must be elevated as a mechanism to ameliorate entrenched forms of exclusion in older age.
Second, a continuous process of critical reflection, and structured observation/appraisal, is required within implementation phases to identify methodological elements that are working for, and against the participatory research process. The broad PHR ethos, and the PLA techniques in this study employed were valuable assets. They informed the design of the approach, the fieldwork’s execution, and individual method adaptations. Nevertheless, and as described, challenges with some exercises still persisted. Illustrating that no one approach is a straightforward panacea, these techniques could not address all participant needs. Researchers cannot be complacent even when using “specialized” approaches designed to promote voice. While the challenge of accommodating specific needs at a group level is substantial, responding to the diversity of difference at the intra-group level is perhaps more even more so.
Third, there is a demonstrable need for further investment in voice and engagement platforms for marginalized older adult groups in policy/practice spheres. For older Travelers and older homeless adults, one of the most significant challenges remains the lack of opportunities to influence decision-making, and the lack of channels to express voice as older members of these groups. Again, this emphasizes the role that participatory methodologies can play in addressing such deficits, even on an incremental, fixed term basis. But it also illustrates the need for more sustained mechanisms. In Ireland, advancements have been made in relation to inclusion health, and public and patient involvement with marginalized groups. However, specific provisions for older adult Travelers and older homeless adults are largely absent. As elsewhere, this reflects a wider deficit concerning the underdevelopment of a cohesive voice for “mainstream” older populations—a deficit that became more evident during the COVID-19 pandemic (c.f. D'cruz & Banerjee, 2020). The strength of Travelers’ voices in this study shows the benefits of grass-roots investment in capacity building, but it is an investment that is yet to be evident on the basis of age, not to mention intersectional identity.
Fourth, and finally, the collaborative, cross-sector approach embedded within the governance and design of this study created buy-in and ownership that was instrumental to any of the successes that were achieved in this process. However, this level of in-depth engagement was disproportionate to the project’s limited scope, and stemmed from the commitment of these agencies to improve the lives of older Travelers and older homeless adults. Due to the scale of this project, the research team were perhaps not in a position to fully translate the value of this collaboration. As demonstrated across the international literature (Cowdell et al., 2020; Liljas et al., 2017), these kinds of participatory processes are frequently small-scale, posing a challenge to achieving meaningful and sustainable outcomes. More concerted and coordinated efforts in research, policy and practice are required to scale up these processes and to leverage tangible improvements in the lives and inclusion of such groups. Otherwise, and as reflected throughout the various research strands, representing the diversity of experiences is always likely to be a challenge within these sorts of studies, with these sorts of populations.
Some of the observations within this article are likely to be specific to the older Irish Traveler and older homeless populations, and the jurisdictional and temporal context within which the original study was conducted. Nevertheless, and as we hope to have illustrated in the presentation of critical reflections, the general themes surrounding the engagement of these populations within multistakeholder fora are likely to hold relevance for other marginalized groups of western aging societies. Whether other international homeless or displaced populations, or First Nations or indigenous ethnic groups, the accumulation and intersection of risk arising from life-course experiences, socially constructed categorizations, and structural opportunity constraints are likely to present similar challenges to inclusion for these aging groups, albeit diversified across individual members of these populations. While the demographic aging patterns of these populations are becoming more prominent, so too are the deficits in the opportunities for the inclusion of their voice and concerns in research and policy. It is only through a more concerted effort at advancing participatory approaches can these aspects of unequal aging begin to be combatted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Services Executive, Department of Health and Atlantic Philanthropies through the Healthy and Positive Ageing Initiative (HaPAI) partnership