
Abstract
Guidelines advocate a combined physical and psychological approach to managing non-specific chronic low back pain (NSCLBP), referred to as psychologically informed practice (PIP). PIP is underpinned by patient-centered principles and skilled communication. Evidence suggests that a physiotherapist-focused style of communication prevails in physiotherapy. There is a recognized need for observational research to identify specific communication practices in physiotherapy interactions. This observational study explored the interactional negotiation of agenda setting following a PIP training intervention, by identifying and describing how physiotherapists solicit and respond to the agenda of concerns that patients with NSCLBP bring to primary care initial encounters. The research setting was primary care. Nineteen initial physiotherapy consultations were video-recorded, transcribed, and analyzed using conversation analysis, a qualitative observational method. These data revealed a patient-focused style of communication where trained physiotherapists demonstrated a collaborative and responsive style of verbal and nonverbal communication to solicit, explore, and validate patients’ concerns.
Keywords
Guidelines advocate combined physical and psychological approaches to managing non-specific chronic low back pain (NSCLBP) (Foster et al., 2018; National Institute for Health and Care Excellence [NICE], 2016), referred to as psychologically informed practice (PIP) (Keefe et al., 2018). Patient-centered principles and communication between the patient and health care provider are central to PIP (Beneciuk et al., 2019; Keefe et al., 2018; Main et al., 2012; O’Sullivan et al., 2018). This is characterized by greater patient-physiotherapist collaboration and a facilitating style of interaction to incorporate the patient’s perspective, including their concerns, ideas, and feelings (Mead & Bower, 2000; Stewart et al., 2003). Although effective verbal and nonverbal communication skills are considered important prerequisites to such positive interaction, and to build therapeutic alliance (Pinto et al., 2012), the empirical foundations for communication practice in physiotherapy are lacking (Hiller et al., 2015).
Patient–practitioner interaction has also been characterized by more practitioner dominance (Schoenthaler et al., 2018), and existing studies of communication in musculoskeletal physiotherapy demonstrate a physiotherapist-centered style of communication where physiotherapists demonstrate difficulties balancing their own “professional” agendas with those of the patient (Cowell, McGregor, et al., 2019; Hiller et al., 2015; Opsommer & Schoeb, 2014). This physiotherapist-centered communication style has been attributed to the traditional biomedical focus of undergraduate training programs (Cowell et al., 2018; Hiller et al., 2015) and lack of postgraduate training in communication skills (Cowell et al., 2018; Daluiso-King & Hebron, 2020; Synnott et al., 2015). This is consistent with recent qualitative studies in which physiotherapists express a need for communication training (Cowell et al., 2018; Holopainen, Simpson, et al., 2020; Sanders et al., 2013; Synnott et al., 2015).
Soliciting patients’ agenda of concerns comprehensively is key to patient-centered communication (Epstein et al., 2008) and can improve patient satisfaction (Rodriguez et al., 2008). Effectively incorporating the patient’s agenda as part of a PIP interview can establish the patient’s psychosocial concerns (Keefe et al., 2018; Nicholas & George, 2011), yet it is not clear how well physiotherapists can do this in current practice.
Our previous observational study analyzed physiotherapists prior to undergoing training in PIP and demonstrated how physiotherapists do not always engage verbally and nonverbally with cues reflecting patient’s concerns about pain and incapacity (Cowell, McGregor, et al., 2019). It also highlighted that physiotherapists typically dominate the interactional agenda resulting in lost opportunities for patients to disclose and develop their agenda of concerns. To date, there has been no study exploring how physiotherapists explore patients’ concerns following PIP training.
This study explores the interactional negotiation of agenda setting by analyzing the extent to which physiotherapists solicit and respond to the agenda of concerns that patients with NSCLBP bring to primary care initial encounters following a training program in Cognitive Functional Therapy (CFT) (O’Sullivan et al., 2018). CFT is a psychologically informed physiotherapy-led intervention that targets physical, lifestyle, and psychological barriers to help patients self-manage low back pain (LBP) (O’Sullivan et al., 2018). Central to CFT is building a strong therapeutic alliance, which is underpinned by a reflective, empathetic, and validating communication approach (O’Keeffe et al., 2016).
The aims of this study were to identify (a) physiotherapists’ questioning strategies for soliciting patient concerns and (b) to explore how physiotherapists respond to patients’ presentation of concerns. These analyses did not focus on soliciting patients’ complete agendas of concerns but gave focus to sequences in which patients express their concerns specifically about symptom attribution and the future consequences, and their emotional agendas (Barry et al., 2000) due to loss of capacity and pain.
Conversation analysis (CA) is an inductive observational method (Maynard & Heritage, 2005) and was chosen as the research method for the study to allow for close microanalysis of the real-time interaction. The dyadic interpersonal communication model describes the dynamic interactive process that takes place between two people and has been used to characterize the interdependence of patient and provider communication (Bylund et al., 2012). CA views patient-provider communication as a dyadic process that gives equal consideration to both partners (Maynard & Heritage, 2005) and has been used previously to describe different types of interdependent patient–provider communication, which can either inhibit or promote patient participation (Collins et al., 2005; Cowell, McGregor, et al., 2019). In this study, CA was employed to explore how “concerns talk” was accomplished and co-constructed by the physiotherapist and patient. By illustrating the possible communication practices employed by physiotherapists in real-life interactions following training, this study provides empirical insights into how embedded physiotherapist-centered communication is in current practice (Cowell, McGregor, et al., 2019; Hiller & Delany, 2018; Hiller et al., 2015; Josephson et al., 2015).
Method
Setting
The setting for this study was two outpatient physiotherapy departments in primary care in North East London Foundation Trust (NELFT). One of the authors was employed by NELFT, and although his perspectives provided insight into the processes in the research setting and its place within the wider organization, it is acknowledged that may have had an influence on the sequences selected for inclusion in the article and the interpretation of the data. Three of the authors have a clinical and research interest in PIP and the management of LBP, and these multiple perspectives may also have consciously or subconsciously had an influence on the findings and interpretation of the data. Nineteen initial physiotherapy consultations were video-recorded (10 physiotherapists and 19 patients). The recorded assessments ranged in duration from 48 minutes to 1 hour. The lead researcher (I.C.) was present at the recorded assessments to adjust the camera as required, but he had no discussion with the physiotherapist or patient during or directly after each recorded assessment. The encounters were recorded in private treatment rooms consistent with usual practice in the research setting. The images included in this article reflect the typical physiotherapist–patient orientation during the interview phase of an initial encounter and were not manipulated for the purposes of the research.
Participants
Ten physiotherapists (three females and seven males) who had completed a formal training program in CFT were included in this study. They ranged in years qualified from 4 to >14. The years working in a musculoskeletal setting ranged from 3 to >14. Previous postgraduate bio-psychosocial training ranged from 0 to 12 days. Twenty-three patients, reporting NSCLBP >3 months, including a range of risk profiles for developing persistent LBP, were identified in two NELFT physiotherapy departments from either the triage clinic or the musculoskeletal clinical assessment and treatment service. Two patients declined to participate due to work commitments, and two patients elected for “usual care,” as they did not want to be video-recorded, leaving 19 patients included in the study (12 women and seven men). The ages of the patients ranged from 19 to 68 years (mean of 40.8 years). The patients completed several questionnaires, which included the Ørebro Musculoskeletal Pain Screening Questionnaire (ØMPSQ; Boersma & Linton, 2005), the Roland and Morris Disability Questionnaire (RMDQ; Roland & Morris, 1983), and the STarTBack Screening Tool (Hill et al., 2008), and a measure of pain intensity on a 0–10 pain numerical rating scale (NRS). The ØMPSQ scores ranged from 83 to 150 (mean score of 112.3). The RMDQ scores ranged from 2 to 21 (mean score of 9.1). The patients’ estimated risk profile for developing persistent LBP measured on the STarTBack screening tool included eight patients at low risk, six medium, and five high. The NRS scores ranged from 4 to 9 (mean score of 6.3).
Multifaceted Training Program
This observational study was nested in a larger study, conducted over a 3-year duration, examining the training requirements for the implementation of CFT. The multifaceted CFT training program is presented in detail in Supplemental Appendix 1. The training program included a mix of theoretical and experiential learning approaches and was informed by the physiotherapists’ own data from a pre-training observational phase (Cowell, McGregor, et al., 2019). The communication component of the training program gave explicit focus to encouraging physiotherapists to produce active displays of recipiency to facilitate patients to pursue their agenda and voice their concerns. We acknowledge that presenting post-training data from a non-randomized design such as this cannot be used to determine the effectiveness of such a training program or to interrogate the mechanisms through which clinical behavior might change. Instead, the training program simply allowed us to observe whether agenda setting and patient concerns were explored to a greater extent than that previously described (Hiller & Delany, 2018; Hiller et al., 2015; Josephson et al., 2015) and observed in our own previous (pre-training) data (Cowell, McGregor, et al., 2019).
Analysis
All data were analyzed using CA, a qualitative data-driven inductive method based on empirical observation of communication practices (Collins et al., 2005). This method of analysis is predicated on the supposition that talk, in its ordinary and institutional form, is sequentially organized, and the meaning of each turn of talk depends on how it is understood in the next turn by the participant rather than rely on the views or interpretations of the analysts (Maynard & Heritage, 2005). There are several “intersecting machineries” of practice required for conducting the analysis (Hoey & Kendrick, 2017, p. 153), and the focus in this study was on the following aspects: turn-taking (how turns of talk are taken by the speakers and how this is locally managed within the talk), structural organization (overall “map” of the interaction in terms of analysis of different sections of interaction (e.g., opening—greeting, problem initiation, closing), sequence organization turn-organization (how successive turns link up to form coherent courses of action), turn-design (how turns are designed to perform actions, e.g., soliciting patients’ agendas of concerns), lexical choice (analysis of vocabulary), and forms of asymmetries during the interaction (Heritage, 2004; ten Have, 2004, 2007) (analysis of participation).
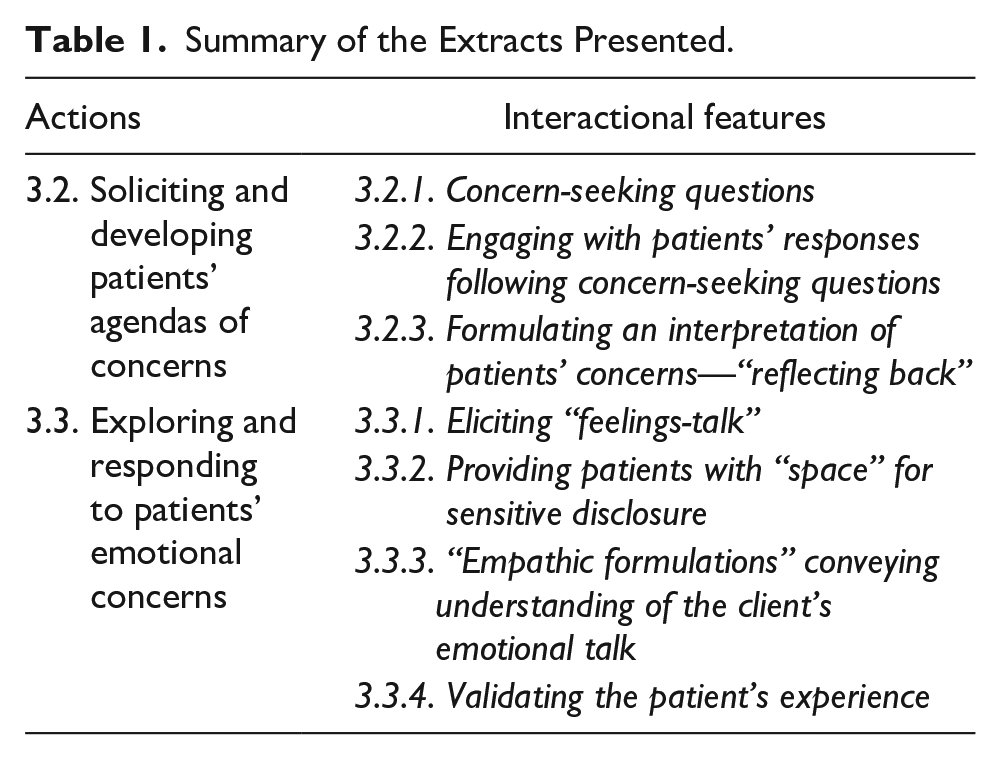
Initially, these post-training data were transcribed verbatim, and two members of the research team (I.C. and R.P.) independently analyzed each transcript with the accompanying video recordings. Sequences related to patients’ concerns were identified, viewed, and presented to the research collaborators to refine the direction for further analysis (Cowell, McGregor, et al., 2019). Shorter extracts of these events were then transcribed in more detail using the standardized transcription conventions for verbal and NV activity (Jefferson, 2004). 1 NV aspects of communication during talk in which patients revealed their concerns were described in brackets. These shorter extracts were presented to the research collaborators for discussion at data workshops to support the analysis. The video recordings allowed for repeated scrutiny and provided access to the fine details of both talk and NV activity. Table 1 provides an overview of the extracts presented in this study.
Summary of the Extracts Presented.
Question Formats
These findings illustrate particular types of questions that can be classified as either Yes/No (Y/N) questions (Raymond, 2003) or Wh-questions (WH-Qs; Stivers, 2010), concern-seeking questions (Robinson, 2006b), and candidate questions:
Y/N questions, or polar questions, are designed to encourage a brief “yes” or “no” response. These have been referred to as “closed” questions in that they typically limit the contributions that patients make to interactions (Boyd & Heritage, 2006). We identified two kinds of Yes/No questions: Yes/No interrogatives (YNIs) and Yes/No declaratives (YNDs), which have been differentiated in the literature in terms of how they convey the questioners’ access to information (Heritage, 2010).
Wh-questions are questions using words such as “what,” “why,” “when,” “who,” “where,” and “how,” and are considered less constraining than yes/no questions (Wang, 2006), providing more space for patients to design their response and describe their experience in their own terms (Peräkylä & Vehviläinen, 2003).
Concern-seeking questions are categorized on their content rather than grammatical form, in that they are explicitly formatted in ways that allowed for the relevance of concerns to be solicited (Robinson, 2006b).
Candidate questions are classified on their content and provide a model type of answer and are a common method of information-seeking (Pomerantz, 1998).
Ethics
The local research ethics committee approved the study (reference Number: 2352), and it was successfully reviewed by the East Midlands-Nottingham 2 National Research Ethics Service (NRES) committee (14/EM/1045). All patients and physiotherapists who agreed to participate provided written informed consent prior to participation in this study, which also included authorization to use their transcripts and images in scientific articles. Video-recording live interaction has the potential to threaten privacy and confidentiality, and, therefore, the videos once collected were then kept on a password protected external hard drive, which was only available to the research team. The decision was taken to blur the faces of the participants to preserve anonymity, although it is acknowledged that this will have a detrimental impact on the presentation of the data (Parry et al., 2016), in that patients’ subtle facial expressions will be reliant to some extent on the description rather than the images.
Results
These findings enabled insight into the identification of typical patterns of behavior and communication practices that were found in the different consultations following a multifaceted PIP training program.
Soliciting and Developing Patients’ Agendas of Concerns
“Concern-seeking” questions
This extract starts with the patient expressing her concerns that she is having to use her own judgment to manage her back pain and is unsure as to whether she should be working through the pain or not. This concern is built over multiple turns reflecting the patient’s perception that she caused damage previously by working through the pain:
Engaging with patients’ responses following concern-seeking questions
This extract starts with the patient reporting that a previous magnetic resonance imaging (MRI) scan had revealed degenerative changes. The physiotherapist’s concern-seeking question—
Formulating an interpretation of patients’ concerns—“reflecting back”
This extract starts with the patient describing the impact of his LBP and how he now avoids sports he previously enjoyed because of concerns about making the condition worse. The physiotherapist’s so-prefaced YNI question that follows includes candidate answers (Lines 03–05) and appears to be positioned and constructed to better understand whether his avoidance of sporting activities is based on worry/expectation of pain or the actual experience of activity-provoked pain. The patient’s response,
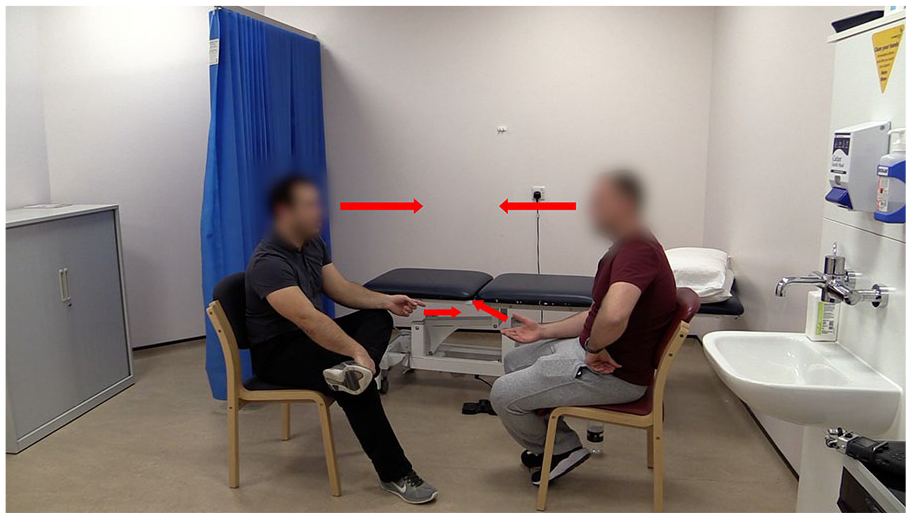
The arrows denote synchronized hand gestures and aligned eye gaze (physiotherapist on the left).
Exploring and Responding to Patients’ Emotional Concerns
Eliciting “feelings-talk”
At the start of this extract, the patient reports that his spinal consultant has suggested that he should expect a future of ongoing pain:
Providing patients with “space” for sensitive disclosure
This extract starts with the patient describing the impact of her back pain and includes an explicit reference to her emotional distress:
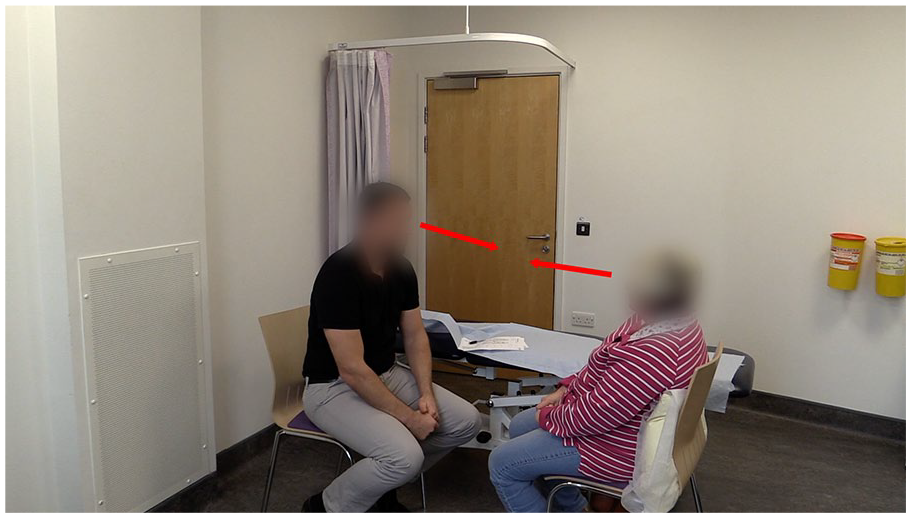
Physiotherapist’s body orientation and eye gaze toward the patient communicating engagement.
“Empathic formulations” conveying understanding of the client’s emotional talk
This extract starts (Lines 01–04) with the patient describing her concerns for the future, predicting with some certainty that her back pain will deteriorate and ultimately
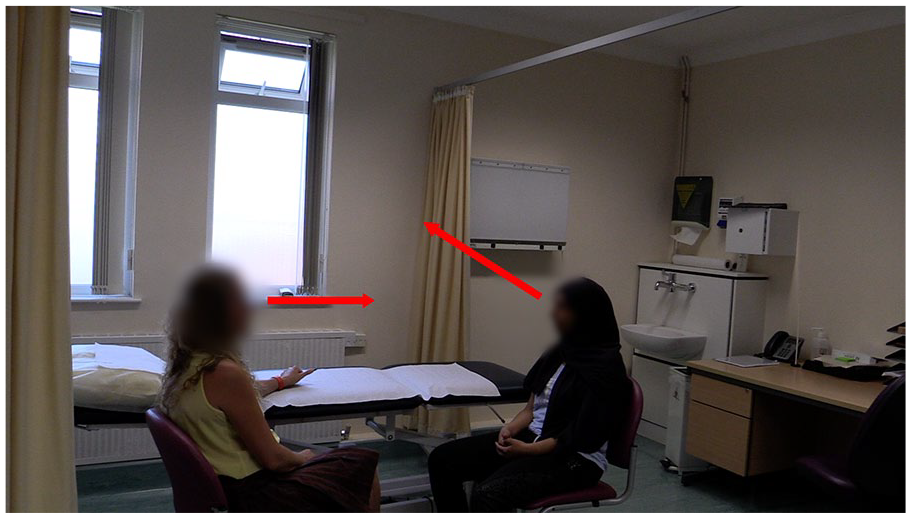
Patient looks away toward the window and the physiotherapist maintains eye contact with the patient.
Validating the patient’s experience
This extract is a continuation of Extract 1 and starts with the physiotherapist (Lines 01–03) attempting to elicit why the patient feels her back is damaged. The response produces the patient’s main concern,
Discussion
Overview
In these findings, the physiotherapists “actively” solicited and explored patients’ concerns and were responsive to patients’ implicit and explicit cues. The key aspects of these findings will now be discussed in more detail.
Exploring Patients’ Concerns
Patients’ concerns were prioritized explicitly by the frequency of concern-seeking questions (Extract 1, Lines 23–24). Physiotherapists do not always engage with patients’ responses following concern-seeking questions, preferring to pursue their own agenda (Cowell, McGregor, et al., 2019). By contrast, here the physiotherapists consistently engaged with patients’ responses by employing secondary questions. These secondary questions were typically WH-Q’s, for example,
Physiotherapists preserved the patient’s concerns-displays as a legitimate topic for discussion by providing minimal responses, such as
The physiotherapists’ responsiveness was also reinforced by their attempts to interpret patients’ previously expressed concerns. Such “reflecting back” or formulating the meaning of the patients’ earlier statements (Antaki, 2008; Heritage & Watson, 1979) is consistent with recommended patient-centered interviewing techniques (Hashim, 2017; Main et al., 2010). While formulations can close topics (Heritage & Watson, 1979), in these findings, the formulations “fixed” the topic on the patients’ concerns, and patients mostly oriented by providing elaboration (see Extract 3, Lines 23–25), as previously observed in psychotherapy, medical, and physiotherapy data (Beach & Dixson, 2001; Bonnin, 2017; Cowell, McGregor, et al., 2019).
Exploring Patients’ Emotional Concerns
There is good evidence that emotional distress impedes recovery for patients with persistent back pain (Crombez et al., 1999; Foster et al., 2008; Pincus et al., 2002). Despite recommendations that physiotherapists identify and target these risk factors (Foster et al., 2018; NICE, 2016), there is little interactional evidence supporting physiotherapists’ willingness or ability to do so. The limited available data suggest that physiotherapists rarely question patients with LBP on the emotional impact of their condition (Roussel et al., 2016), despite patients seeing this as key to “good” clinical interaction (Laerum et al., 2006). While physiotherapists recognize the importance of addressing patients’ emotional factors, they often feel uncomfortable addressing sensitive topics, reporting a lack of training and guidance in this regard (Cowell et al., 2018; Fritz et al., 2018; Holopainen, Simpson, et al., 2020). Recent evidence has demonstrated how some physiotherapists acknowledge but fail to explore patients’ emotional concerns in preference for pursuing their own agenda (Cowell, McGregor, et al., 2019; Josephson et al., 2015).
In contrast, these findings strongly suggest that physiotherapists viewed patients’ emotional concerns as an integral aspect of physiotherapy interaction. They frequently initiated feelings talk by employing feelings-formulated questions (Extract 4, Lines 05–06), or candidate questions, which included emotions as model answers (Extract 4, Lines 13–14), making patients’ feelings a relevant next topic. Patients typically orientated to the opportunities to reveal their emotional concerns, displaying how these were interactively produced in a physiotherapy context. The patients’ affective displays were marked here as sensitive through hesitations, hitches and perturbations, laughter particles, prosodic shifts in pitch and volume, and through emotional expressions such as
The physiotherapists’ sensitivity and engagement with the patient in these emotional sequences was reflected by their minimal responses, which had a different quality and seemed to resonate with patients’ quiet emotional disclosure (Fitzgerald & Leudar, 2010), for example,
The physiotherapists’ responsiveness to patients’ emotional talk was also demonstrated by their attempts to represent the patients’ emotional experience by employing empathic formulations (Fitzgerald & Leudar, 2012). These formulations provided a sensitive way to orient to the patient’s emotional talk, for example,
Nonverbal Behaviors
Very little focus has been given to NV communication in physiotherapy interaction (Parry & Brown, 2009). In our previous observational study, prior to the CFT training intervention, we observed how some physiotherapists demonstrated a lack of direct body orientation and abrupt withdrawal of eye gaze, communicating a reduced state of engagement with the patient (Cowell, McGregor, et al., 2019).
In contrast, these findings were characterized by the physiotherapists’ consistent body orientation, eye gaze, and hand gestures toward the patient, communicating a framework of engagement (Robinson, 2006a). Such behaviors communicated that the patient was the dominant focus and enabled physiotherapists to detect patients’ facial expressions and bodily displays expressing their symptoms and distress (Heath, 2002). Patients also displayed their orientation to these nonverbal displays through their own body behavior, with illustrations of synchronized patient-therapist hand gestures (see Extract 3; Figure 1) and reciprocal head nodding.
Using documentation during the interaction is a widely recognized barrier to effective communication (Cowell, McGregor, et al., 2019; Schoeb & Hiller, 2018). In these findings, the physiotherapists’ sensitivity to the intrusive nature of documentation was manifest in their body comportment and eye gaze away from the documentation and toward the patient (Robinson, 1998). This is consistent with self-promotional goals theory (Goffman, 1979; Jones & Pittman, 1982) and wanting to communicate an expression of interest to the patient.
We have observed in these findings how key communication features could influence the disclosure of patients’ expression of concerns. Such verbal and NV communication features provide tangible empirical examples of the recommended skills of patient-centered communication required to develop the therapeutic relationship (Bedi & Duff, 2014) and are at the heart of PIP approaches (Main et al., 2012; O’Sullivan et al., 2018).
Strengths and Limitations
These findings seem observably different from data from previous studies, including our own pre-training data (Cowell, McGregor, et al., 2019; Hiller et al., 2015; Josephson et al., 2015); however, the design precludes specific conclusions being made about the effects of the training program. Consequently, further research using quantitative methods is needed to determine the effectiveness of this training model in changing physiotherapists’ communication practice. Future work might also consider including patients with higher levels of disability as it is acknowledged that patients at high risk of poor outcome have higher levels of emotional distress (Hill et al., 2008; Main et al., 2012). Validation of the findings was strengthened by a strong commitment to naturalistic description of the interaction and ensuring that the researchers’ analyses were aligned to how the interactants themselves locally interpreted the interaction, by closely analyzing how the next speaker treats the preceding action (Silverman, 2004). However, the video recordings were undertaken in two settings in primary care only; therefore, no representation of practice can be claimed. It is also acknowledged this is a relatively small sample size and, therefore, the findings discussed are suggestive of the possible types of practices employed by physiotherapists in real-life interactions, yet perhaps not representative of all physiotherapists’ practices following this type of PIP training (Peräkylä, 2011). It is recognized that using video recording might have had an influence on how participants behave (Parry, 2010) and that the presence of the lead author may have disrupted natural interaction. This PIP training program was experiential, extensive, and multi-staged over an extended period of time, which has clear practical implications in terms of the resources needed for wide-scale implementation. Health reform is also needed to better align funding with evidence-based practice (Foster & Delitto, 2011; Keefe et al., 2018), as short appointment times make delivering PIP challenging (Cowell, O’Sullivan, et al., 2019; Holopainen, Piirainen, et al., 2020). We also observed in these findings how physiotherapists integrated documentation tools to limit their intrusive nature when addressing patients’ concerns. Being able to integrate physiotherapy documentation to limit its intrusive nature when addressing patients’ concerns may be difficult in current practice given an increasing move toward the use of computerized documentation (Schoeb & Hiller, 2018). It has been suggested that the structure of documentation tools may need reconsideration so that they align more seamlessly with the flow of the conversation (Schoeb & Hiller, 2018).
Practice Implications
We observed how key verbal and NV communication features helped solicit and validate the disclosure of patients’ concerns. These findings may help physiotherapists to reflect on the elements of communication, such as levels of bodily engagement, actively listening, accurately summarizing and empathizing with patients’ expressed concerns, not being incorporated into their current practice. This process of reflection on practice may be enhanced by expert observation and feedback on physiotherapists’ communication practice, as used in this training program. These findings illustrate the importance of multimodal communication in patients’ emotional displays and demonstrate how physiotherapists’ empathic responses are important in allowing patients to disclose and build their emotional displays.
Conclusion
Following a training program in CFT, we observed how physiotherapists were prepared to share control of the interactional agenda and prioritize patients’ concerns. The physiotherapists were responsive to patients’ “talk,” employing key verbal and NV communication behaviors to support patient disclosure and allow the exploration and validation of patients’ concerns. This contrasts with recent studies that have consistently demonstrated a more physiotherapist-focused style of communication, including with the same physiotherapists prior to this training. This suggests that the communication behavior of physiotherapists may be amenable to change.
Supplemental Material
sj-pdf-1-qhr-10.1177_10497323211037651 – Supplemental material for Physiotherapists’ Approaches to Patients’ Concerns in Back Pain Consultations Following a Psychologically Informed Training Program
Supplemental material, sj-pdf-1-qhr-10.1177_10497323211037651 for Physiotherapists’ Approaches to Patients’ Concerns in Back Pain Consultations Following a Psychologically Informed Training Program by Ian Cowell, Alison McGregor, Peter O’Sullivan, Kieran O’Sullivan, Ross Poyton, Veronika Schoeb and Ged Murtagh in Qualitative Health Research
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.O., K.O. and I.C. receive fees for speaking at conferences and providing clinical workshops for health care professionals in the management of musculoskeletal disorders.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Authors would like to acknowledge Funding support was received from from the Private Physiotherapy Educational Foundation and the Musculoskeletal Association of Chartered Physiotherapists.
Supplemental Material
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.