
Abstract
This grounded theory study aims to map, conceptualize, and theorize the emotional loss experienced by parents following their child’s pediatric acquired brain injury (pABI). Data were obtained from 47 semi-structured interviews conducted with parents (72% mothers) at least 1 year following pABI. The study’s theory of “concurrent ropes and ladders” emerged from a process of initial in vivo coding followed by focused and thematic coding. Codes were consolidated into five thematic categories capturing parents’ emotional continuous loss experience: (a) comparing life before and after, (b) struggling to construct new realities, (c) recognizing instability and permanency, (d) adjusting and readjusting, and (e) grieving as an emotional shadow. These categories are at work simultaneously in parents’ accounts, thus supporting a model of dynamic concurrency within and across their lived experiences. Recommendations for practitioners were derived from the theory to support parents’ emotional coping with living loss throughout the chronic stage.
Introduction
Pediatric acquired brain injury (pABI) refers to diverse conditions involving damage to the brain that occurs after birth and does not relate to a congenital disorder or degenerative disease. It is a major cause of death and long-term disability among the pediatric population (Lin & DeMatteo, 2013) and can be precipitated by an event with an external cause (traumatic brain injury [TBI]) or an internal cause (e.g., brain tumor, hypoxia, stroke, or brain infections; Chevignard et al., 2010; De Kloet et al., 2013). Sustaining a serious brain injury during childhood results in pronounced impairments in physical, cognitive, emotional, and social functioning, and can, therefore, divert the child’s developmental trajectory (Donders & Warschausky, 2007; Middleton, 2001). Despite variability in recovery outcome (Beauchamp & Anderson, 2013), many children continue to exhibit residual neurocognitive, behavioral, and psychosocial disruptions, which have considerable future implications (Anderson, 2003; Laatsch et al., 2007).
The literature has already acknowledged pABI as a significant event for parents due to the ongoing practical and emotional accommodations it requires throughout the child’s life (Rashid et al., 2014). Alterations in the child’s functioning result in an increased caregiving burden, long-term psychological distress, and changes in the parenting experience (Aitken et al., 2009; Hawley et al., 2003; Micklewright et al., 2012; Wade et al., 2006). Parents’ emotional tasks relate primarily to coping with social isolation, the insecurity of the situation, and the challenges of adjusting to the different roles required in parenting a changed child, as have recently been found in meta-synthesis research (see Tyerman et al., 2017).
Family adaptation to pABI was initially studied through measures of psychological well-being and family functioning (e.g., Rivara et al., 1992; Wade et al., 1998). Documentation on parents’ grieving process, however, gradually increased over the years, albeit sporadically. Zinner et al. (1997) were the first to quantitatively indicate the significant role a child’s behavioral changes play in eliciting parental grief and the fact that grief does not subside with time. Likewise, Collings (2007) described parental loss as an escalating experience, and Brown et al. (2013) showed the patterns of parental emotions to be complex and not moving toward resolution. Similarly, in other qualitative studies exploring post-pABI parenting experiences, parents attest to be “perpetually grieving” (Jordan & Linden, 2013)—an experience that stems primarily from “changes to and loss of the past child” (A. Clark et al., 2008) and the cessation of “normal” family life (Collings, 2007). A two-way emotional experience was also noted: a sense of gratitude that the child survived the injury along with continuous “grieving for the child I knew” (e.g., Roscigno & Swanson, 2011).
These studies attest to a notion of ongoing loss and adaptation coupled with challenges and duality in the parent’s bond with the child postinjury. In most studies, however, parents’ emotional reactions emerged as one dimension of the entire caregiving experience; studies with a fuller conceptual framework addressing parents’ complex processes of grief and loss remain scarce.
Theoretical Perspectives on Grief and Brain Injury
Earlier works outlined the importance of considering models of bereavement and loss in work with families of post-TBI adults (Lezak, 1986; Oddy & Herbert, 2003; Roundhill et al., 2007) or post-pABI parents (A. Clark et al., 2008). To date, such cases of non-death losses are still mainly understood through grief models that address the death of a loved one. However, unlike the five-stage model presented by Kubler-Ross (1969), current models of bereavement emphasize the reworking of the “continuing bond” with the deceased as a central grief-related task. For example, Rubin’s (1999) two-track model of bereavement (TTMB) addresses the bereaved’s biopsychosocial functioning and coping (Track 1) alongside the nature of their bond with the deceased (Track 2). Another model is the dual process model (DPM), which emphasizes an oscillation between a focus on the bereaved’s relationship with the deceased (loss-orientation) and on the tasks of everyday life (restoration-orientation; Stroebe & Schut, 1999). Importantly, existing bereavement models share the understanding that the physical absence of a loved one due to death elicits grief and coping. Navigating these processes results in adjustment to the changed life circumstances and diminished grief, alongside recognition of the adaptive nature of the continuing bond with the deceased (e.g., Bowlby, 1980; Klass et al., 2014; Stroebe et al., 2008; Worden, 1991).
Conversely, following pABI, the physical presence of the changed child enables parental loss to gather significance over time as the memory of the preinjury child coexists with their postinjury child. This results in a “dual” continuing bond along with daily reminders of the loss. Such a key aspect, together with accumulated evidence on undiminished grief reactions (e.g., A. Clark et al., 2008; Jordan & Linden, 2013; Roscigno & Swanson, 2011; Zinner et al., 1997), questions the applicability of bereavement theories to post-pABI parents and to the field of brain injury rehabilitation in general (Harris, 2019; Niemeier & Burnett, 2001).
Turning to existing conceptualizations in the field of non-death loss, Bruce and Schultz (2001) coined the term “nonfinite loss” to denote an enduring loss, usually precipitated by a negative life event after which the source of the loss continues to be present. Such loss manifests itself gradually and is often characterized by a sense of ongoing uncertainty, repeated adjustments, and an unforeseen end (Harris & Gorman, 2011). The term was initially used in cases of children with developmental disabilities or chronic diseases (e.g., O’Brien, 2007; Whittingham et al., 2013). The emotional reaction to nonfinite loss has been termed “chronic sorrow” (Olshansky, 1962; see Coughlin & Sethares, 2017 for review): a set of pervasive and enduring grief reactions that are constantly triggered by painful discrepancies between the present reality and former hopes for the future (see also the concept of “living loss”; Roos, 2002). As an experience with no resolution, family loss in cases of ABI is often termed “ambiguous loss” due to the incongruity between the injured person’s physical and psychological presence, which can be seen to result in “frozen grief” (Boss, 2006). Although the terms “nonfinite loss” and “ambiguous loss” are said to describe cases of non-death losses, their application to parents, following pABI, has not been fully explored. Neither term, however, considers how behavioral and personality changes challenge relational aspects and how the gaps between the “living and developing” child, the “previously known” child, and the “hoped for” child hamper parents’ ability to work through their loss.
A recent quantitative study (Yehene et al., 2021) described parents’ post-pABI grief response patterns and intensity as similar to those previously measured among bereaved parents. However, significant differences were found on scales assessing the continuing bond with the preinjury child; this finding indicates parents’ post-pABI grief as multidimensional and illuminates the interplay between elements characterizing parents’ experiences of nonfinite versus finite loss (i.e., child death).
Such multidimensionality is also evident in psychotherapeutic work with post-pABI parents as the nature of the injury entails constant emotional turmoil for parents and prevents them from making sense of the loss. The “ropes and ladders” trope frames the experience of emotional instability, contrasting with the initial hope for a full recovery. This trope seems consistent with clinical and current research documentation of parents’ loss experiences (e.g., Brown et al., 2013; Jordan & Linden, 2013; Roscigno & Swanson, 2011).
In the overarching spectrum of loss, current models of bereavement and unique conceptualizations in the field of non-death loss do not seem to provide applicable and clinically relevant framing for understanding parents’ non-death child loss. A new direction of investigation would therefore be valuable (see also A. Clark et al., 2008). Furthermore, unlike the lived experience of parents caring for a child with visible physical impairments (e.g., cleft palate syndrome; Nelson et al., 2012), genetic brain impairments (e.g., Down syndrome; L. Clark et al., 2020), or progressive neurodegenerative illnesses (Rallison & Raffin-Bouchal, 2013), the uniqueness of pABI relates primarily to its acquired nature. The onset of the condition, which sometimes takes place years after birth, is usually sudden and occurs after parents have already had significant experiences with their child. In addition, the evolving, albeit everlasting, cognitive and neurobehavioral impairments may sometimes be invisible yet still create a loss of the child’s previous identity and of the shared relationship (interpersonal loss). Considering these distinctive characteristics and their complexity, the aim of the current article is to suggest a separate clinical and theoretical framework to help clinicians working with parents in the process of infinite adaptation. We looked to explore parents’ emotional experiences and to construct a theory on how they understand and conceptualize their living loss reality.
Method
Study Design
Our study follows a constructivist version of grounded theory (Charmaz, 2008). This choice seemed appropriate as our initial interest related to parents’ meaning-making construction of their current loss experience and our aim was to theorize their emotional coping. The study adhered to the premises of constructionism and symbolic interactionism. It also included open-ended, three-phase coding and theorizing as well as typical attributes shared with other versions of grounded theory, such as beginning with a purposeful sample, constant comparisons, and memo writing (Kenny & Fourie, 2015). Parents’ accounts were collected in semi-structured interviews, as part of a larger research project (Yehene et al., 2019, 2021). Ethical approval was obtained from the institutional review boards at the medical center and the academic institution. Verbal and written informed consent was obtained from all participants prior to enrollment.
Setting and Recruitment Strategies
The study was conducted at Israel’s primary children’s hospital, which is located in central Israel, in the country’s largest medical center. Each year, 90 to 110 children are admitted to the rehabilitation department; about 50% of them are post-pABI. A full 3- to 4-month hospitalization is typically followed by 6 to 7 months of day hospitalization (gradually reducing the frequency from four weekly visits to one while returning to school and engaging with relevant services in the local community), and then periodic follow-up visits. These visits take several hours as they involve a multiprofessional clinic, psychosocial assessment/therapy sessions for both the child and the parents, and occupational therapy, physiotherapy, and learning center sessions, as needed. During the period of this study, 223 post-pABI children were seen in outpatient clinics. Of the 60 prospective families who met our inclusion criteria, 47 parents were interviewed; those who declined did so for logistical reasons.
Interviews lasting 45 to 60 minutes were conducted in the outpatient clinics. Parents were invited to participate in the study on the morning of their arrival. They were given initial information and consent forms to review. They were contacted again later in the day by the research team and, if they showed interest, on signing the consent form, the interview was set up for a time when the child was in an assessment/therapy session. Parents were interviewed in a research-designated room (not in use for other parent–staff meetings), keeping the interview in a familiar, supportive, and discrete environment.
In accordance with critiques of power differences in interviews (e.g., Olesen, 1994; Reinharz, 1992), and as we cannot really equalize structural positions in this setting, we took two measures to deal with power differences: (a) complete separation between the regular therapeutic rights of parents and their involvement with the research (parents were informed of the right to refuse or terminate participation at any stage without affecting their medical rights), and (b) using the interviewer’s power to the advantage of the interviewee as much as possible in a hospital setting. Interviews were conducted by an expert clinical neuropsychologist (Einat Yehene), not a direct therapist of any of the participants, who used her knowledge advantage to provide reflective listening, empathic resonance, psychoeducation, and support when the interviewee asked for it. For possible postinterview reactions or concerns, participants were invited to contact the interviewer or the clinic’s psychologist.
A purposeful sample (Palinkas et al., 2015; Patton, 2014) of parents of children diagnosed with pABI was recruited between September 2014 and March 2018. The decision to adhere to a purposeful sample was taken as we wanted to deepen our understanding of parents coping with a specific nonfinite loss before defining further theoretical sampling principles. Purposeful sampling also suited our phase of open coding and testing emergent focused codes and categories (Draucker et al., 2007; Morse, 2007). Responses were good and, by the time we reached saturation (when new interviews did not yield any new information on the parent loss experience), we had a significant volume of rich information, thus allowing us to theorize. Much like Draucker et al. (2007), who refined a typology of life span sexual victimization based on purposeful sampling, we could then refine a typology of parental emotional positions after pABI.
Participants
All the participating parents were primary caregivers of a child who had sustained an ABI between ages 3 and 18 years, which was evident in brain imaging and of sufficient severity to warrant prolonged hospitalization and multidisciplinary rehabilitation. Prior to the ABI, all the children had developed typically with no brain injury, chronic illness, physical disability, or psychiatric condition. We were interested in interviewing parents at least 1 year following pABI as it takes from 9 months to 2 years to realize post-injury loss (Lezak, 1986).
More than two thirds (72%) of the parents were women aged between 33 and 66 years (average education: 14 years; range = 10–19 years). Parents were married (89%), divorced (4.5%), widowed (4.5%), or single (2%). Time since the child’s injury ranged from 1 to 14 years, and the child’s age at the time of injury ranged from 3 to 17 years. Most of the children were male (68%) and the ABI etiology included TBI (60%), cerebrovascular accident (21%), brain disease (11%), and brain tumor (8%).
Data Collection
Our study was looking for information about three main questions (see Online Appendix): (a) Tell me about your child. (b) Tell me what happened to your child. (c) Were there any changes in your child’s behavior post-pABI? If so, please describe those changes. The interview was planned with very few questions to limit intervention and influence over parents’ narratives but to allow for clarification questions about a story or its meaning, requests for detailing, and empathic responses (Josselson, 2013). These questions served as triggers and let parents refer to their child and the ABI event and consequences in any terms they felt comfortable with (Josselson, 2013). Often, only the first or second question was asked as parents shared generously and talked naturally and spontaneously about changes in the child and their family life (the third question).
The interviews were documented in writing. Although we are aware of the taken-for-granted status of audio recording (Nordstrom, 2015), we chose real-time handwriting documentation for four reasons. First, we wanted to avoid interviewees’ hesitation about being audio recorded and, second, to avoid the dilemma of handling “off the record” meaningful data. Our assumption is that interviewees who see the ongoing action of documentation are aware of it and perhaps of what is being documented and hence intentionally choose to share information “on the record.” Third, the interviewer is skilled and experienced in both interviewing and real-time documenting as this is common practice in her regular clinical meetings. Finally, a recent study has shown that there are no omissions of significant information in handwriting documentation when compared with recorded data from the same interviews (Rutakumwa et al., 2020). Immediately after each interview, the interviewer spent time completing and verifying the accuracy of the information. For the purpose of publication, the parents’ texts were translated from Hebrew to English. The standard “forward-backward” procedure was applied by two experts in the field proficient in both languages.
Data Analysis
Morse (2015) called for rigor, reliability, validity, and generalizability as measures of quality in qualitative research methods. She recommends two strategies for semi-structured interview research design, both of which we followed. First, we manually developed a coding system and inter-rater reliability: two of the researchers (a neuropsychologist specializing in brain injury and a psychologist specializing in parent and child therapy) read the transcripts separately, and then developed a set of in vivo codes in the process of initial open coding. Thereafter, by constant comparison, the two researchers developed a set of focused codes (Charmaz, 2006, Chapter 4). This stage yielded six categories. A third researcher (a social anthropologist) read the transcripts anew, applying these six categories. In this coding process, we felt that two of the categories (“comparing past and present” and “comparing present with expected future”) were too intertwined in the parents’ stories. We therefore combined the two into “comparing life before and after,” which related to the lives of both parent and child. The final coding system of five categories and 13 focused codes was refined in team discussions in which attributes of each code were analyzed comparatively. The theoretical model was formalized based on emergent relationships between the categories. Second, we used the peer review/debriefing strategy recommended by Morse (2015). Drafts of coding results and theoretical models were presented to both peers and experts in the children’s hospital and grief scholars in the academic world. Discussions that developed with peers and colleagues added yet another dimension of simultaneity to the analysis and theory development.
The trope “ropes and ladders,” which appears in the title of this article, is an in vivo code (Charmaz, 2006; Glaser, 1978), preserving the meaning and the dynamic of constant emotional instability—a central experience of parenting a child after brain injury. The term “ropes and ladders” helped us move from the initial open coding to a focus on more theoretical codes and categories capturing emotional states/positions that the parents saw as sliding “down” (ropes) and climbing “up” (ladders). It also accentuated their accounts of constant emotional movement.
Results
Concurrent Ropes and Ladders: An Overview of the Theory
The first steps after the injury are drastic and you feel as if you have conquered the world. But with time, you get to understand that it’s more like ropes and ladders . . . I went through a lot of emotional turmoil. There is no serenity or rest. I keep waiting for saturation [meaning: end of constant change] and a stability that will never be.
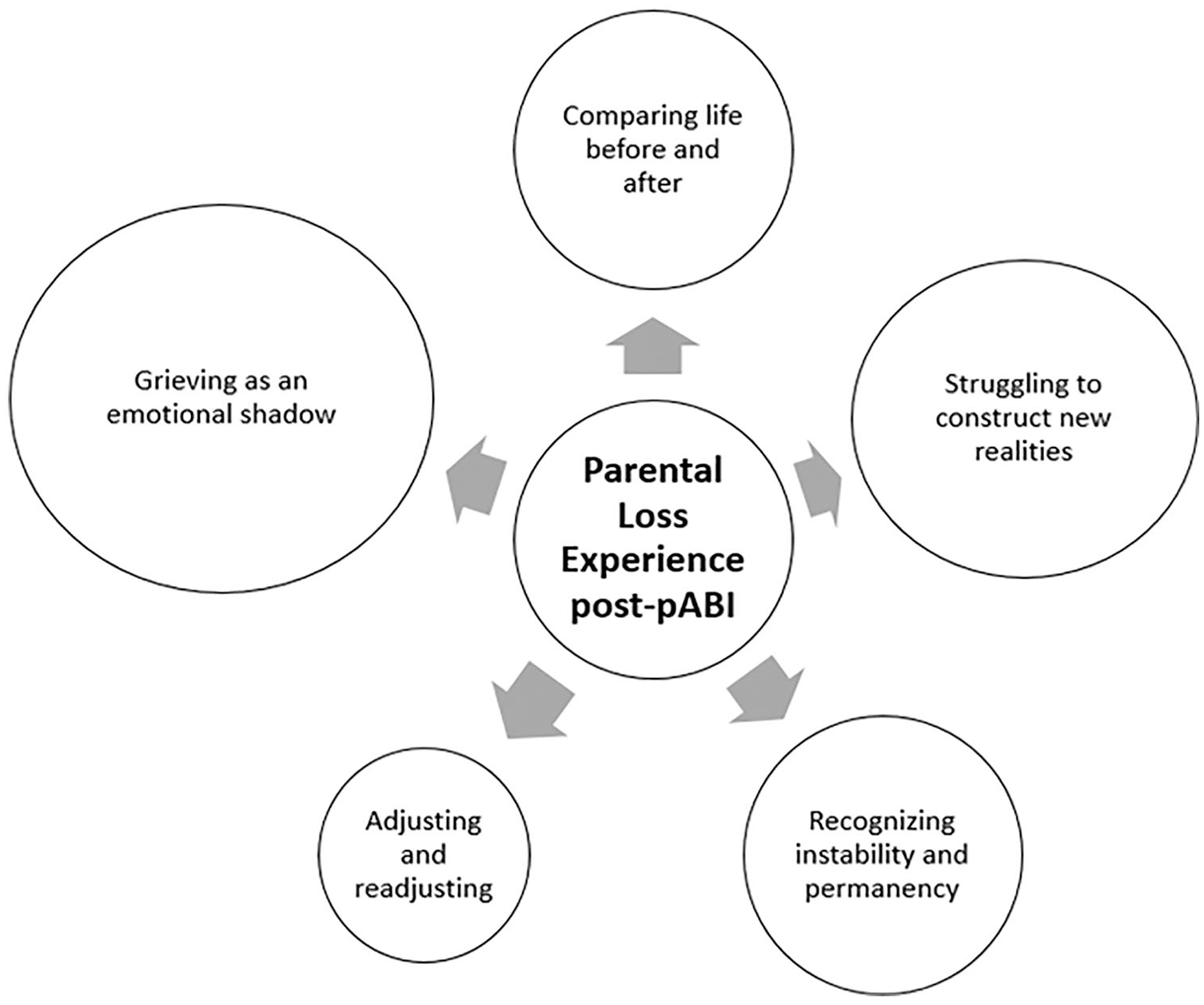
The concurrent ropes and ladders theory comprises three elements:
Five categories of parental emotional positions—(a) comparing life before and after, (b) struggling to construct new realities, (c) recognizing instability and permanency, (d) adjusting and readjusting, and (e) grieving as an emotional shadow;
Concurrency of positions in parents’ lived experiences; and
An integrated model of emotional dynamics and intensity.
The following sections elaborate on each element.
Five Categories of Parental Emotional Positions Post-pABI
The five categories, each based on respective focused codes, often appear intertwined or blurred in the parents’ accounts. They were, nonetheless, found to comprise distinct essence and traits. For the sake of clarity, each of the categories is presented with specifically differentiated excerpts.
Comparing life before and after
The acquired nature of the injury throws parents into an experience of multiple discrepancies between pre- and postinjury visions of child and family. Comparisons become loss defining mechanisms, as they delineate gaps in hopes, expectations, and courses of the lives of both parents and child.
Comparing the child pre- and postinjury
Parents used dichotomous terms to describe postinjury changes in their child alongside an idealizing language describing their preinjury child: “You have an excellent and amazing child who has suddenly become handicapped and needy.” Metaphors such as “day and night difference” were used to describe the gap they experience. A common discursive practice was the listing of the preinjury child’s multiple virtues. For example,
Before the injury, he was curious, a reader, smart, and interested in astronomy. He could name all the flowers, he was an independent normative child, friendly, funny, witty. A happy and loving child. An athlete who played football, basketball, and judo. A very lively and cheerful child. After the injury he became tactless, with temper outbursts, who fails to distinguish between simple situations, who gets easily tired while reading, who lost his areas of interest.
The richness of positive past qualities is altered and narrowed to physical and behavioral postinjury changes. These behavioral changes also challenge the child’s broader relationships:
He was admired by most children in his class from first grade until the accident [six years later]. He was very generous and protective, and now it is gone. It’s all lost. He recovered from the injury but did not return as a whole—the way he was before. He’s a different child.
While parents strive to make sense of the gaps they see between their child pre- and postinjury and watch friends disappear, they also need to provide guidance and mediation to siblings: “His siblings remember the way he was and the way he is now and this gap drives you crazy.” Siblings often mirror the parents’ feelings:
It makes you cry that you had a perfect child and now you don’t . . . His brother says, “Bring me back the old [name].” It’s hard to hear those sentences that actually reflect what we ourselves as parents think and feel.
Discrepancies between the past and present child are intertwined with discrepancies between parents’ present child perceptions and the normative age developmental trajectory. These gaps grow with time, as advances in chronological age and physical development (bodily changes and maturation) do not correspond with mental age and emotional growth, which may remain stagnant or regress:
It’s like having a little child in the house. He is physically a big man. Very tall and impressive, but mentally he is like a little kid. He needs a lot of attention, positive reinforcement. He repeats things, doesn’t calm down, and doesn’t let go until he gets what he wants.
Comparing the parents’ lives pre- and postinjury
pABI is a life-altering event, splitting parents’ life into before and after. Many indicated that it is “the most difficult thing I have ever encountered,” as this event dramatically turns life over, taking away a sense of normality, regularity, and spontaneity: “There is life before the injury and life after it, and there is a very clear line between them.” Equally as prominent as the loss of the preinjury child is the loss of the parental self. The extensive implications of the injury impose changes that affect parents’ daily lived experiences and require their devotion to the injured child: “The major difficulty is that life has changed. I can’t really be free and independent or pursue my studies. It changed the orbit of my career. I lost the ability.” Intimacy between the parents is also severely affected: “Every aspect of our daily life has changed. Even in our marriage everything has reversed, and it is not the same. Our thoughts are always on him and not on us. Our intimacy has gone.”
Struggling to construct new realities
Parents strive to close identified gaps and refer to their efforts in terms of fighting: they hope to “defeat” the impact of the injury and not “surrender” to its permanency.
Fighting to return to “normal.”
Parents invest time and money searching for and trying different therapies, hoping to achieve the child’s perceived recovery potential and to ease their experience: “He is a smart boy. He knows everything. That is why I want us to invest and put the focus on him so he can complete his studies. He has potential.” Parents link their efforts to their child’s pace of recovery and future achievements:
I am afraid he will reach a certain limit from which he will not improve further. Maybe we can still advance him further. I just hope his motivation in rehab will not decline. I’m afraid he will get tired and say that what we have achieved so far is good enough.
Efforts to construct gaps as temporary
Parents construct current time as an “in-between” phase in the hope that it is temporary. During this phase, they try to treat the child “as if nothing really happened.” However, this attitude proves impossible: “We try to treat him as we would a regular child. We try, and it’s not simple, because there’s the understanding that he cannot be a regular child.” Parents also struggle with reconstructing their parental role at this time, debating what they should consider legitimate demands of their child:
I wrangle with him, and then I catch myself and say: “What are you doing? . . . he is not a regular child. What are you thinking to yourself?” . . . I still don’t accept it and I fight over him, and therefore I am less protective of him.
Gaps, as shown here, may be found not only between past and present but also between different constructions of the current situation as transient or permanent. Although reconstructing preinjury life with the child remembered from then may no longer be a viable goal, parents continue to try and fulfill the child’s potential. This perceived potential changes occasionally; hence, construction of the postinjury reality becomes a lifelong mission. The nature of this dynamic is related to the way parents perceive the child’s condition.
Recognizing instability and permanency
A child’s behavioral instability, coupled with an inconsistent line of progression, gradually unravels the stagnant nature of the injury, the permanency of the deficits, and the instability of their manifestation. This recognition and its resulting emotional exhaustion contribute to parents’ need to let go of former hopes and “move on.”
Instability of the child’s behavior
Parents told of facing rapid and dramatic shifts in the child’s behavior: “Now he is golden. But if, an hour from now, he wants a snack and doesn’t get it, he will no longer be this wonderful child.” Triggers for unstable behavior were often reported as unpredictable or untraceable: “In times of anger and frustration, he cries, screams, and lashes out, and it’s difficult to calm him down. It can happen even from invisible and unexpected noises.” Such unpredictability not only impacts their emotional equilibrium and routine but also makes them wonder who their child is now. Ambiguity profoundly hampers their ability to create a cohesive and solid image of the child with whom they try to reconnect, as one mother elaborated, “My child is walking, talking, and smart. But he has a problem whenever he encounters a situation that demands self-regulation . . . . The difference in the child post-injury is not just a changed essence but a disrupted essence.”
Uncertainty about the future
Uncertainty is a salient experience for parents from the first moment of the injury incident. At the point when we met them (at least a year postinjury), uncertainty is related to how life will eventually unfold for the child. Specifically, will the child achieve the future developmental milestones dictated by cultural norms or preinjury hopes? As one parent said, “I think a lot about his future—what will be with him? I really want him to become an independent man, but I don’t live in illusions.” In their effort to replace “illusion” with realistic expectations, parents undergo an internal bargaining process in which they negotiate in their mind what outcome they are willing to settle for: “It is painful and difficult for me that she can’t read. But maybe with time she will. If not, then we will accept it as it is.”
One worry haunting parents relates to the fulfillment of caregiving responsibilities once they themselves are no longer able to provide them: “How many years can I carry on until I see him settling down in his own place living his own life? Who will take care of him? His siblings are not capable of pitching in.”
Permanency and ever-changing orbit
Parents come to recognize that the situation is “endless” with a “no-ending horizon.” Typical phrasing was offered by one of the mothers: “There is injury and deficits and it’s for the rest of our lives.” On being probed for what she foresees continuing for the rest of her life, she continued, “Her difficulties with impulsivity are very prominent. We talk about employing different strategies like using a stop sign cue card, but still this regulation is missing. I must learn about those difficulties and how to cope.” When strategies like the stop sign fail, this mother realizes that it is she who needs to change. Other parents, accounting for the evolvement of their understanding of the situation, told us about extreme mental and emotional efforts: “The understanding that this is not a transient injury that will totally disappear requires from me a lot of energy and mental strength.” It is not only the permanency that parents need to adjust to but also the instability and the ambiguous dynamics in which hope and despair are entangled:
There is a process of discovery. A good day or that one time when the child has been able to control impulsivity is deceiving and makes you think that he will return to his orbit, but then there is another fall. It is endless; this is our life. Everything is dynamic. It’s not something that will stop, and we can say, “that’s it.” Everything is always changing, and there are discoveries for the better or the worse. You go up and down, constant instability . . . . This is until death.
Parents function in an ever-changing reality, making it difficult to hold on to any restoration of their preinjury life.
Recognizing the need for a shift in the definition of the situation
There is an inevitable change in expectations concerning the recovery process and the future of both the injured child and the parent, and hence parents “move on” by coming to terms with the injury and its permanent instable manifestation. Parents adjust their end goals and learn to “accept the situation”:
I was in rehabilitation [accompanying my son] for a long time. After four years, I now need to accept the situation . . . to take a deep breath and embark on a new road; otherwise, it will be difficult. The only difference is that at the beginning, I didn’t want to believe that it was forever and for the long run.
Although such a shift entails internalization of a new spectrum of goals and expectations, parents continue to experience the same endless daily dynamic of ropes and ladders. Thus, although they may “surrender” and change perceptions of their child’s functioning, they continue to aim for the child’s progress with sprouting optimism:
There is a certain point where you say “enough” and you throw your hands up. But we are a coping and functioning family. There are feelings of frustration and despair even today. There is this internalization process, which I define as despair, but sometimes there are also good things, when we work with her and see improvement. Within this despair, I am an optimistic person—if you have no hope, why go on?
Adjusting and readjusting
Adjustment is a continuous process that requires flexibility, openness, and updated accommodations to meet the child’s current functioning. Adjustment means attempt to lean on the good, recognize small successes, and preserve hope. Parents thus act upon their changing expectations while valorizing the good they see in their child’s functioning.
Updating expectations
Parents’ adjustment process includes seeking knowledge about the current abilities of their child and about possible compensation strategies:
For us, it’s definitely something new and something to learn and get used to, but not something impossible. She is the oldest, and we had expectations that she would function as such and assume more responsibilities, but we are constantly adjusting our expectations.
Knowledge obtained and adjusted expectations may lead to providing their children with a better suited environment: “It was difficult to place him in this afternoon sports program for disabled kids. In the beginning, I didn’t want to go there because I said to myself that he’s not like them. Today he is blossoming there.” The processes of reevaluating the powers of the self and the family, reframing the new situation, and accommodating it are often rewarded by watching the child “blossom.”
Valorizing the good
Parents balance their loss perception by capitalizing on the fact that the child has survived the injury or by focusing on their intact abilities or on newfound positive qualities postinjury. This helps them to resolve emotional ambivalence, promote a sense of adjustment, and find meaning in their loss. Some parents rationalized as follows: “Everything is put into proportion when you see what the injury was and what is left. For others, it resulted in death.” Other parents valorized the traits and virtues their child exhibits:
I learned about her strength from the way she copes every single day. She is motivated and has a strong will. In the long run, there are many things that will stay like that. What has not changed is her being a cool girl.
A sense of proportion allows parents to focus on details and to notice some continuation of the preinjury child, thus maintaining hope alongside updated scales of expectation.
Grieving as an emotional shadow
Grief manifests alongside other processes. Parents described grief as a constant invisible “emotional shadow” behind their appearance of adjusted functioning. They reported being occupied with relational active grieving, adaptation with no acceptance, and loneliness.
Relational active grieving
A lack of loss resolution is associated with feelings of acute yearning for the past child, constant preoccupation with memories, and painful thoughts about the “lost” child and relationship, wrapped up in death-related language, such as “The pictures on the refrigerator are killing me and causing a lot of pain. I can barely look at pictures from the past. The way he was and the way he is now.” Another mother talked about both herself and her daughter in similar death-related terms:
My mood is very depressed and pretty much depends on her condition. I am dying within myself . . . It is like you have buried the old [daughter’s name] and got instead the new [daughter’s name]. On the inside, I am constantly grieving. It hurts. There is no single day that goes by without remembering it.
Pictures from the past are “killing” the first mother—she is trapped between the troubling pictures she cannot look at and her inability to remove them from her sight. The second, attesting to a Gordian knot between her emotional state and her daughter’s condition, feels she is “dying within herself.” Permanent grief is, for them, the appropriate framing of their emotional state.
Adaptation with no acceptance
Inherent in the unresolved nature of their loss is the clear distinction parents draw between their ability to cognitively understand the stagnant and irreversible nature of the injury and their emotional readiness to accept it. The constant confrontation with the evolving gaps between past, present, and expected future impedes their ability to make sense of the loss:
I understand that this is what he is capable of right now and that it is what it is . . . and that I cannot change it. But still, it is very hard for me to accept it emotionally . . . . I try to disconnect myself from it, but it is stronger. It’s in front of my eyes. It is emotionally draining for me. I feel like I have aged 20 years.
Parents further elaborated on the burden of grief: the need to constantly suppress emotions and to avoid potential flooding that might interfere with their functioning. In some cases, grief is described as a chaotic, unexpected process that may be triggered by specific moments or incidents and as something encapsulated that parents hope will become better integrated:
On the one hand, something is nesting inside of you, and on the other hand, you function normally on the outside. We aspire to be free from this emotional shadow that weighs on you. Sometimes one incident creates a chain reaction. We want to take what we have been through like another cog integrated into the system that we need to live with and embrace in our current life.
Tensions between cognitive and emotional, inside and outside, and stagnant and dynamic are mediated by actions. Caring for the child and organizing and reorganizing the family’s life amount to a huge but necessary workload. In addition, there is the burden described as “emotional shadow,” which is always there, preventing the family from transitioning to an “integrated system” and overcoming “what they have been through.”
Loneliness
Parents describe their post-pABI life as an experience of isolation and loneliness resulting from differentiating between their real feelings and what they convey to their surroundings. They tried to explain their procedures for establishing borders and finding a balance between the inner and outer self:
I am telling you, it is continuous grief. An inner grief that you cannot convey to your surroundings because you want them to feel good. It’s a chronic sorrow, but you need to survive. Other people cannot really help you. Not even emotionally. You need to be strong yourself. In the beginning, there was a lot of support and help and then, nothing. There is only a hole, and I feel lonely. I cannot find a balance between the inside and the outside.
Parents try to keep their continuous grief reaction inside as an act of survival and thus keep their surroundings happy. However, while doing so, they can cut themselves off from possible supporters, thus deepening the imbalance between their emotional inner and functional outer self.
Parents also talked about disenfranchising aspects of their grief as other people cannot relate to their non-death loss experience due to the ambiguous and sometimes invisible nature of the brain injury:
Everybody who looks at him sees a very sweet and endearing child. But if you spend more time with him, you will understand how big the change is. This entire process and feelings have put me in a very difficult place within myself, but I try not to give up on myself.
As it is difficult for others to grasp what parents are going through, the battle moves inward—into “a very difficult place within myself”—as an act of self-preservation.
Loneliness is also present in the context of the parents’ couplehood. Challenges arising from the postinjury situation, including differences in the emotional processing of the loss, take their toll on their relationship: “I used to be surrounded by supportive people. Now some of them left. Including my husband. Now I am coping all by myself.”
Next, we present another emerging element that might be relevant to understanding the overall feelings of each parent and of the couple as a unit: the interplay of the five categories of emotional positions.
Concurrency of Emotional Positions in Parents’ Lived Experiences
Coding and analyzing yielded multiple categories (i.e., emotional positions) with a common pattern of concurrency or what they described as “at the same time.” Fourteen parental accounts refer to three concurrent categories, another 14 have four such categories, and 19 accounts offer five categories each. Consider, for example, the following account of a father in which we found five categories narratively associated with his present time:
Life is very different [now]. He needs help with everything. From a totally independent child, he now needs help tying his shoelaces . . . . He argues stubbornly all day about every little thing that doesn’t fit with what he thought or wanted . . . . Some days he’s just very sensitive and feels misunderstood. I am not used to seeing him like this. For 10 years, he was an excellent [child/student]. I pay for everything [therapy and assistive activities] privately. I just want him to feel good. There is great difficulty, but one has to move on with life. I see photos from [vacation] a month before the injury . . . it breaks my heart. Friends and family also broke away from us . . . . How long will we be able to be with him like that? If he wants to get married, will he manage? There are always thoughts and worries about the future. I feel like God gifted him to us; our faith grew stronger. I found out that he fights and struggles. It’s hard to think about him negatively.
This father compared his past and present life and child (Category A: comparing life before and after). He described constant arguing and hinted at his struggle against the instability of life routines while understanding the nonstable nature of his child’s injury and uncertainty of the future alongside with the need to “move on” (Category C: recognizing instability and permanency. He continues to invest in therapies hoping to restore age-typical functioning now and in the future (Category B: struggling to construct new realities), while capitalizing on the child’s strength, finding meaning in the loss (Category D: adjusting and readjusting), and lamenting the lost relationship and loneliness (Category E: grieving as an emotional shadow).
Common concurrency of emotional positions (categories) in parental narratives led us to formulate a model of emotional dynamics and construction of reality following pABI. Based on the accounts analyzed here and on existing literature, the following conceptualization is proposed to both enhance understanding of multiple simultaneous emotional processes that parents undergo and to provide a theoretical base for supporting parents’ loss experience in clinical practice.
Model Integration
The ropes and ladders trope refers to a perceived vertical movement, flowing up and down in an emotional metaphorical landscape (Lakoff & Johnson, 1982). Other expressions used by parents, such as “waves” and “ups and downs,” denote similar emotional dynamics. Parents’ attempts to cope and make sense of their loss were thus shown to be either helped or hindered by “ladders” and “ropes,” respectively. These ropes and ladders may be elicited by situations that are momentary (e.g., behavioral regressions and instabilities, the unreliable use of compensatory strategies, or observations of little progress) or conditional (time since injury, life cycle events, perceived pace of recovery, comparisons with peer group, or reflections on progress). Frequent up and down dynamics are reported to differentially influence the intensity of each of the five emotional positions, which might, accordingly, inflate or deflate. Thus, while parents continuously manage the five loss-related positions, certain emotional positions can be at the forefront of their experiences. This depends on their intensity at a given moment and requires a special investment of resources. Hence, following our data analysis, a model of dynamic concurrency is offered to conceptualize parental emotional loss experience post-pABI. Figure 1 illustrates the intensity formation of concurrent emotional positions by describing one parent’s emotional state at a given point in time.
The concurrent ropes and ladders theoretical model.
This dynamic concurrency proposes a within-parent and between-parents variability of intensity for each emotional position throughout the chronic stage. Therefore, conceptually speaking, one can extrapolate how the accumulated intensity of each concurrent element will be graphically presented over time, crafting a personalized monitoring graph for each parent (Figure 2).
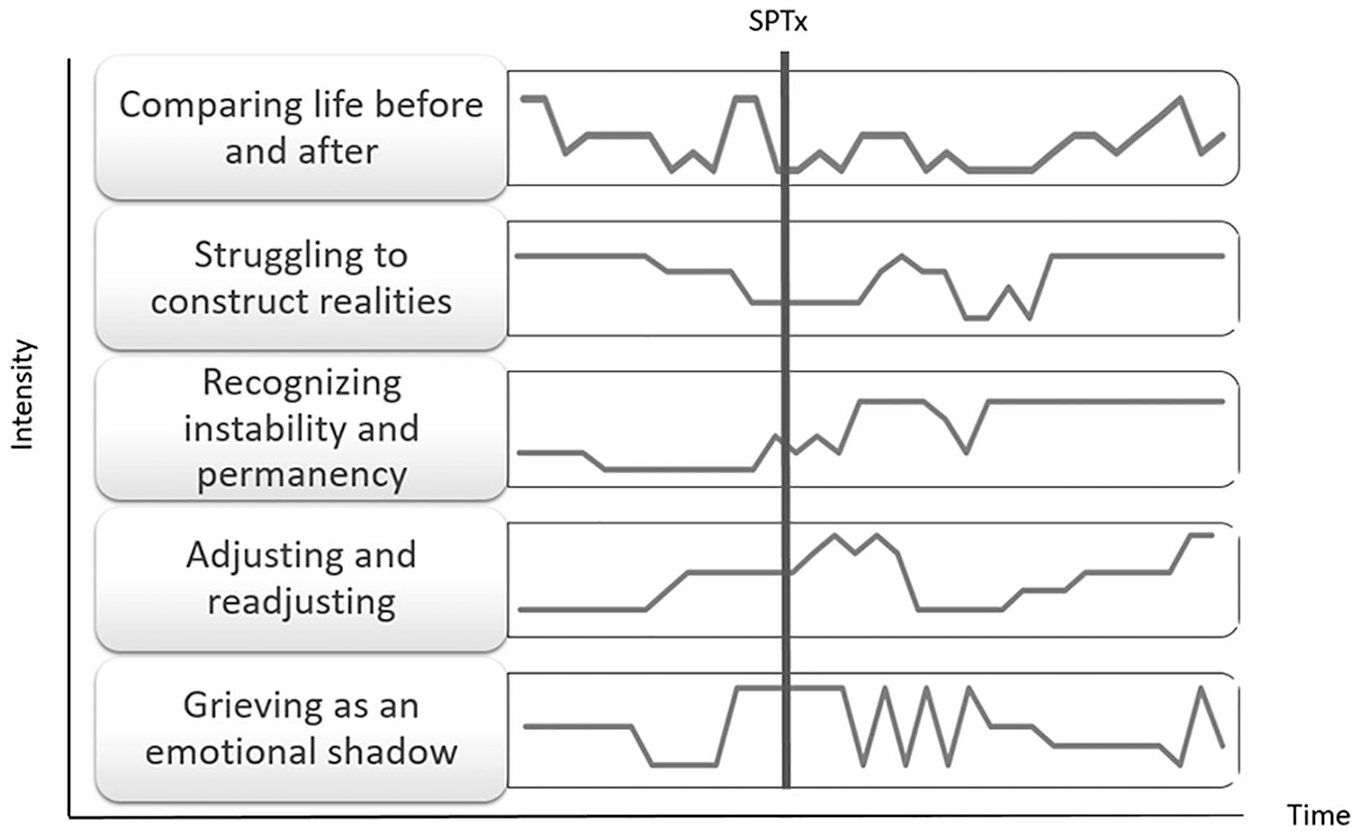
Monitoring one parent’s emotional positions over time.
Discussion
The three elements of the concurrent ropes and ladders theory presented here shed light on the cognitions, emotions, and actions comprising parents’ non-death loss alongside the dynamic and psychological movements they undergo as parents of a post-pABI child.
The first element of the theory maps parents’ loss experience as encompassing the five emotional position categories: (a) comparing life before and after, (b) struggling to construct new realities, (c) recognizing instability and permanency, (d) adjusting and readjusting, and (e) grieving as an emotional shadow. This mapping partially aligns with the initial nonfinite loss conceptualization, as previously defined among other clinical populations (Bruce & Schultz, 2001; Harris, 2019). Overlapping characteristics include painful gaps between reality and imagined future, uncertainty regarding how the loss will unfold during life, changes in the assumptive world, the repeated need to accommodate and adjust to the loss, and the chronicity of sorrow. Parents’ accounts also share some attributes common to caring for a child with chronic illness or permanent disability, emphasizing dealing with ongoing struggles, social isolation, future-oriented concerns, the balance of good and bad times, and striving for acceptance and normalcy (e.g., Coffey, 2006; Lassetter et al., 2007).
Categories identified in this study, which are unique to brain injury, also align with accounts of caregivers of adults with TBI (Petersen & Sanders, 2015) and are consistent with previous qualitative and quantitative research conducted among parents, post-pABI, in Australia, Canada, the United Kingdom, Sweden, and the United States (see Tyerman et al., 2017, for review). Shared themes include a longing for the past child, missing out on a future-imagined child, grieving for the past relationship, adjusting expectations, and an ongoing socially unrecognized grief. The concurrent ropes and ladders theory not only incorporates these experiences but also expands and unites them in one integrative framework conceptualizing parental “living loss” (Roos, 2002), following pABI.
The second element of the theory conceptualizes the construction of parents’ daily experience as encompassing multiple emotional positions simultaneously. This innovative element might contribute to existing knowledge in the still-growing field of emotional reaction to non-death losses and, in particular, nonfinite loss, compared with tangible domains of finite loss (death).
Similar to the theoretical shift in the field of thanatology toward the nonlinearity of grieving, earlier works suggested applying Kubler-Ross’ stages of grief model to TBI (Groveman & Brown, 1985), whereas later works questioned the validity of linear stages in light of a continuous grief reaction among caregivers (A. Clark et al., 2008; Zinner et al., 1997). Despite attempts over the years to conceptualize how grief unfolds for caregivers following ABI, the question has remained partially answered. Recent bereavement models have suggested that grief unfolds through the simultaneity of coping with demands of life and reworking the relationship with the lost person (TTMB; Rubin, 1999; Rubin et al., 2018) or the periodic oscillation between loss and restoration orientations (DPM; Stroebe & Schut, 1999). Yet both models assume grief to subside over time while adjustment and functioning increase. A similar alternating movement between periods of grieving and adjustment was also noted in studies that termed family grieving after brain injury as “mobile mourning” (Muir & Haffey, 1984) or “episodic loss reaction” (Williams, 1991). Roundhill et al. (2007) used a qualitative method to link the DPM with grief in adults with TBI and found only a partial fit, whereas Clark et al. (2008) suggested further examining whether the DPM can be generalized to parents’ post-pABI. Still, these concepts were never further developed or empirically tested with caregivers following ABI. Recently, Harris (2019) suggested an adapted version of the DPM as a generic framework for understanding the reaction to various types of non-death losses. However, our data do not support this appealing theoretical proposition as we found parents’ lived experience to contain five possible emotional positions, not two, and ample evidence for coexistence (which we termed “concurrency”) rather than oscillation between two distinct poles.
A literature review conducted by Coughlin and Sethares (2017) on chronic sorrow in parents of children with chronic illness or disability (other than brain injury) emphasizes its cyclical nature. However, such cyclicality does not align with previous reports on continuous grief reaction in parents of children with ABI (Tyreman et al., 2017; Yehene et al., 2021) or with the way in which the “grieving as an emotional shadow” category in this study emerged as an integral concurrent position in parents’ accounts. Thus, relative to other existing bereavement models and relevant conceptualization in the field of loss, the concurrency offered by the concurrent ropes and ladders theory can be seen to provide a more accurate, experience-near framework for understanding this type of loss.
The third element in this study’s theory refers to the intensity dynamic concurrent elements that parents undergo according to whether they encounter ropes or ladders. While daily ups and downs are common for a period of weeks and months after a significant loss (i.e., “roller coaster”; Doka, 2017), they seem to be central in parents’ loss experience post-pABI, with no dominant strategy. A similar dynamic of peaks and valleys was noted when parenting a child with a chronic disability (e.g., Damrosch & Perry, 1989), emphasizing the role “trigger events” (Eakes et al., 1998) play in the periodic resurgence of chronic sorrow. Conversely, in pABI, cognitive deficits and behavioral instability serve uniquely as triggers, being vivid daily reminders of the loss. Our data show that triggers, momentary or conditional, require ongoing management of the loss and its dictated constraints and derivatives.
Recommendations for Supporting Parents
The model of concurrent ropes and ladders might familiarize practitioners with the concurrent albeit dynamic process that parents undergo, following pABI, and can be a useful framework for interventions designed to ameliorate emotional coping, make sense of the loss, and promote coherence. Given the nonfinite nature of the loss, parents’ emotional experiences should be routinely assessed and addressed in clinical practice. Such a procedure seems valuable, considering parents’ assertions of the need for emotional support in coming to terms with the enduring loss of their former child (Jordan & Linden, 2013; Kirk et al., 2015) and the rarity of clinical interventions attending to their grief (e.g., Hickey et al., 2018) compared with those attending to the child’s cognitive and behavioral outcomes (Laatsch et al., 2020). Suggestions derived from our theoretical model can be coupled with the existing body of literature on parents’ post-pABI and on non-death losses.
Validate the loss
In line with previous studies, our results suggest that parents are grieving a non-death loss, largely unrecognized by society. Such “disenfranchisement” is known to impose complications in the grieving process (Boss, 2006, 2009; Doka, 2002). We therefore suggest that practitioners validate and name with parents the multiple tangible (e.g., relationships, personal habits) and intangible (e.g., dreams, hopes, and autonomy) losses parents encounter post-pABI and enhance their sense of legitimacy to grieve.
Address social context
The category “loneliness” found in parents’ accounts echoes and elaborates on the sense of isolation, misunderstanding, and social withdrawal reported in previous studies (Roscigno & Swanson, 2011; Tyerman et al., 2017). Given the significance of the social context in mourning non-death losses (Doka, 2002), it is important to assist parents in creating a supportive social network. This can be done by means of educating both the caregivers (Petersen & Sanders, 2015) and their surroundings. Education should focus on their emotional loss experience by attempting to promote concordance between the emotions held inside and those conveyed to the outside.
Normalize and integrate conflicting emotions
The second element of the model further supports the notion that the concurrency of contradicting emotional positions should be conveyed to parents as a normal and natural experience. While conflicting emotions are common among parents coping with a living loss (e.g., Coffey, 2006; Lassetter et al., 2007; Rallison & Raffin-Bouchal, 2013), especially when it feels “endless” (see also Harris, 2019), here these emotions dominate parents’ accounts. Thus, integrating various mixed emotions may assist parents in deflating intensity, reducing guilt and shame, and promoting self-coherence. This variety might be illustrated to parents by a personalized graph line similar to that proposed in Figure 2.
Identify and monitor emotional triggers
Creating a personal graph (see Figures 1 and 2) with mothers and fathers in counseling sessions could help trace the intensity of active concurrent emotional positions and identify potential ropes and ladders as triggers (both external and internal) while implementing strategies to manage their impact. Periodically monitoring triggers in therapy might help parents to create a better sense of control over their experience in their quest to achieve emotional equilibrium.
Identify unmet needs
Parents’ various unmet needs at different points in time throughout the recovery process are consistently implicated in the literature (e.g., Armstrong & Kerns, 2002; Kirk et al., 2015). Therefore, mapping parents’ emotional positions might also constitute a revealing intervention, reflecting their perceptions of their family situation and fine-tuning the unmet needs of each parent and within couples. For example, if the personal graph shows a high intensity of loneliness in their grieving process, counselors might suggest active coping strategies and assist parents in seeking social support (e.g., online groups/programs).
Review and reflect on the coping process
Visualization of emotional variability over time through personal graph lines is suggested to enhance strength and hope. The graphs, created together with parents, show that, although all five emotional positions may be permanent, their mastery is within reach by utilizing the graphic illustration (Figure 2), which recognizes times and strategies of controlling emotional intensity. This joint effort might help parents to reduce self-criticism and establish or improve self-compassion (Brown et al., 2015; Germer & Neff, 2013), knowing that it is the unique situation that challenges them rather than limited resilience.
Limitations and Future Directions
The study employed a cross-sectional design, and therefore the current data do not enable us to trace the dynamics of intensity and coping trajectory of each parent over time. In line with the extrapolative nature of Figure 2, future studies should further validate the intensity fluctuations of parents’ emotional process and perhaps also fine-tune its graphic illustration. This can be done either by involving the same parents at different points in time or by involving parents with similar sociodemographic and injury variables at different points in time. Similarly, beyond the dynamic concurrency of the model, the present data corpus do not allow for classifying profiles of parents per factors potentially affecting the intensity of components (e.g., child age, gender, and time since injury). While future studies might also incorporate this direction of theoretical sampling, we recommend exploring the applicability of the model to other child-related nonfinite loss and developing a more inclusive theory. This might require adjustment of the content and dynamic of emotional positions alongside exploring relevance to other members of the family such as siblings and grandparents. In addition, due to parents’ willingness to share their lived experiences, further research might benefit from documentation by recording interviews.
Finally, the categories constructing the concurrent ropes and ladders theory could be transformed into a quantitative assessment tool that can be further utilized in a clinical setting and in quantitative research. Such an approach might also relate to existing conceptualization in the field by linking terms such as nonfinite loss, frozen grief, chronic sorrow, ambiguous loss, and living loss with diverse evidence-based data (qualitative and quantitative).
Conclusion
Caring for a family member undergoing permanent disability or chronic illness has become an ever-growing phenomenon in modern health care. This calls for the development of theories that address the accompanying non-death loss that caregivers encounter, so as to also advance clinical care among professionals. The work presented here, based on parents’ shared experiences, might contribute to research and clinical paths toward understanding and helping parents regain control and continue their life journey while raising a child with ABI. We hope that the concurrent ropes and ladders theory, currently shown to be relevant to parents, following pABI, will be developed further to benefit people experiencing other types of living losses.
Supplemental Material
sj-pdf-1-qhr-10.1177_10497323211012384 – Supplemental material for “Concurrent Ropes and Ladders”: Mapping and Conceptualizing the Emotional Loss Experience of Parents Following Pediatric Acquired Brain Injury
Supplemental material, sj-pdf-1-qhr-10.1177_10497323211012384 for “Concurrent Ropes and Ladders”: Mapping and Conceptualizing the Emotional Loss Experience of Parents Following Pediatric Acquired Brain Injury by Einat Yehene, Pnina Steinberg, Maya Gerner, Amichai Brezner and Jana Landa in Qualitative Health Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.