
Abstract
There is a lack of intervention promoting physical activity targeted toward people living with dementia because their input has not been prioritized in the development of exercise programs. The aim of this study is to investigate motivators and barriers concerning physical activity in people living with dementia in care homes and to give recommendations for intervention development. Qualitative semi-structured interviews were conducted; transcripts were analyzed using qualitative content analysis. Following a tailored procedural model, inductive and deductive category development was applied. The value of Cohen’s κ = .94 indicates the high intercoder reliability of the category system developed. Ten interviewees reported 24 different barriers and 12 motivators concerning physical activity in the context of the social-ecological model. The strong impact of intrapersonal factors and the living environment became apparent. Points of reference for how people living with dementia can overcome barriers and activate their motivators to achieve more physical activity are provided.
Keywords
Introduction
Dementia is characterized by the progressive loss of cognitive functioning and a decrease in activities of daily living (Dilling & Freyberger, 2016; Morais et al., 2019). It is also associated with a decline in quality of life (Bárrios et al., 2013) as well as in social and physical functioning (Allali et al., 2016; Cedervall et al., 2014; Dilling & Freyberger, 2016). Because of these constraints, most models of successful aging exclude people with dementia from the category of successful agers by definition. One popular example is the MacArthur model of successful aging (Rowe & Kahn, 1997) with its three main components: (a) low probability of disease and disease-related disability, (b) high cognitive and physical functional capacity, and (c) active engagement in life. As 152 million people will be living with dementia by 2050 (Alzheimer’s Disease International, 2018), the labeling of so many people as “unsuccessful agers” has to be challenged.
During the last 30 years, there has been particular concern about the multidimensional expansion of successful aging criteria, as well as a request for the inclusion of subjective meanings for successful aging and more inclusive frameworks that could embrace diversity and avoid discrimination (Martinson & Berridge, 2015). However, successful aging literature has scarcely addressed people living with dementia (Nyman & Szymczynska, 2016), and the views of the people concerned have not been considered at all (Cosco et al., 2014). Although people living with dementia are not addressed directly, Tesch-Römer and Wahl (2017) introduced a comprehensive concept of successful aging that includes people with disabilities and care needs. They argue that instead of distinguishing between “healthy aging” and “aging with care needs,” these two categories should be considered as consecutive phases within one life-course. Tesch-Römer and Wahl (2017) propose the inclusion of individual, environmental, and care-related strategies as well as resources and ask for a life-span developmental perspective. With this approach, the goals of interventions to promote successful aging may change from recovery and enhancement to keeping functional abilities stable and slowing down functional losses (Tesch-Römer & Wahl, 2017). In this way, people living with dementia can be enabled to age successfully by enhancing their still existing health resources.
One promising way to do so is physical activity (Laver et al., 2016). Exercise is a promising nonpharmacological intervention with positive effects on cognitive functioning (Du et al., 2018), physical functioning (Zeng et al., 2016), and the activities of daily living. In addition, exercise positively impacts the behavioral and psychological symptoms of dementia (Forbes et al., 2015).
Despite a steadily growing body of evidence in this field of research, it is still unclear how physical activity interventions should be designed to meet the needs of the target group and the practical requirements of diverse care settings. The inclusion of the wishes, needs, attitudes, and beliefs of people living with dementia concerning physical activity is a crucial prerequisite for the development of targeted and successful interventions in the long-term care setting (de Souto Barreto et al., 2016). These aspects have not been discussed in physical activity research so far, and no significant efforts have been made to consider the voices of people living with dementia in care homes concerning the development of exercise programs (Brett et al., 2018; Tak et al., 2015).
The socio-ecological model (McLeroy et al., 1988) provides a multilevel framework for classifying potential factors associated with physical activity behavior in people living with dementia and for identifying potential levels of intervention. The model focuses on individual and social environmental factors as determinants of health behavior and defines five levels of influence: (a) intrapersonal factors, (b) interpersonal factors, (c) institutional factors, (d) community/society, and (e) public policy. Van Alphen, Hortobágyi, and van Heuvelen (2016) used the socio-ecological model in their systematic review to classify motivators and barriers regarding physical activity from the perspective of people living with dementia. The review includes seven studies and identifies 35 barriers and 26 motivators concerning physical activity in people living with dementia within the five levels of the socio-ecological model (van Alphen, Hortobágyi et al., 2016). Health-related conditions are the predominant inhibiting intrapersonal aspects, whereas individual preferences are identified as major intrapersonal motivators for physical activity. On the interpersonal level, people living with dementia face more than twice as many barriers as motivators (van Alphen, Hortobágyi et al., 2016). Specifically, lack of support by caregivers is a major barrier to exercise in this target group. Social identification when exercising with other people living with dementia is the most frequent motivator on this level. No motivators are identified on the organizational, community, and political levels. Bad weather and lack of transportation, time, and dedicated space are common barriers faced by people living with dementia on these levels.
Although van Alphen, Hortobágyi et al. (2016) give a first overview of the motivators and barriers that prevent physical activity in people living with dementia, their results are limited due to the type of data included. The authors did not differentiate between the perspectives of people living with dementia themselves and the perspectives of their informal caregivers. Furthermore, the transferability of the results to a long-term care setting is limited because the authors were not able to identify studies that focus on people living with dementia in care homes, which indicates the absence of studies in this field (van Alphen, Hortobágyi et al., 2016). The specific living environment in care homes impacts the residents’ activities in their everyday lives (Tak et al., 2015) and also influences the intensity and frequency of physical activity (van Alphen, Volkers et al., 2016): people living with dementia spend 72.1% of the day sedentarily in care homes and have, therefore, a 23.5% lower daily physical activity level than community-dwelling people living with dementia.
Bringing together (a) the lack of targeted physical activity interventions in people living with dementia in care homes, (b) the voices of the target group missing from the development of exercise programs, and (c) the incomplete picture of motivating and hindering factors regarding physical activity in people living with dementia in care homes underlines the strong need for further research.
Addressing the research gaps presented, the primary aim of this study is to investigate motivators and barriers concerning physical activity in people living with dementia in care homes in terms of the social-ecological model. Besides facilitating and hindering aspects, the wishes, attitudes, and experiences concerning physical activity are analyzed to get a deeper understanding of the perspectives held by people living with dementia. An additional aim of the study is to make recommendations concerning the promotion of physical activity to facilitate the development of targeted, sustainable, and successful exercise programs for people living with dementia in care homes.
Materials and Methods
Participants
A sample of 10 participants was considered to be appropriate because of the exploratory nature of this research. This assumption is supported by the sample sizes of other qualitative articles which have also applied a pioneering approach regarding dementia research (McParland & Camic, 2018; Mjørud et al., 2017). The following criteria were set for the sampling procedure: five people living with mild dementia (Mini-Mental State Examination [MMSE] value between 20 and 26 points) and five people living with moderate dementia (MMSE value between 10 and 19 points) in long-term care facilities were included. People living with dementia who are cared for in bed, as well as people who are not able to communicate at all, were excluded. Following the gender distribution of people living with dementia in German nursing homes (Schäufele et al., 2013; 78% female), two interviewees out of 10 had to be male. Five nursing homes participated in the study. All nursing homes are located in rural areas of Austria, accommodate 72 residents on average, and have no special dementia care units. All facilities have direct access to gardens and do not offer structured physical activity programs for residents. The nursing home managers of the participating care homes were asked to choose residents—according to the set criteria—who were willing to participate in the study.
Thus, using these predetermined criteria, a convenience sample was recruited. The 10 interviewed people living with dementia had a mean MMSE value of 20.04 (SD = 3.17). The average age of the interviewees was 84.9 (SD = 4.91) years and 80% were female. Three interviewees had no physical impairments, six needed a rolling walker, and one person was a wheelchair user. Half of the participants had experienced at least one fall during the last 12 months. Within the 7-stage care level system in Austria (higher levels indicate a higher need for care), the interviewees had on average Care Level 3 (care needs between 120 and 160 hours per month): one person had Care Level 2 (95–120 hours per month), five people had Care Level 3, three people had Care Level 4 (160–180 hours per month), and one person had Care Level 5 (>180 hours per month).
Data Collection
To enable people living with dementia to share their experiences, wishes, and needs, a qualitative semi-structured interview was conducted (Nygard, 2006). To overcome the obstacles and challenges associated with interviewing people living with dementia (Carmody et al., 2015), specific recommendations were considered when preparing the interview guideline and during data collection. The interview guideline was developed based on comparable studies on physical activity in the oldest old and people living with dementia (Baert et al., 2011; Cedervall et al., 2015; Malthouse & Fox, 2014; O’Connell et al., 2015). The guideline covered the following five topics: (a) motivators for physical activity, (b) barriers to physical activity, (c) physical activity behavior and wishes, (d) biography and importance of physical activity, and (e) effects of physical activity.
The interview started with an introductory statement about the aim and procedure of the interview to provide orientation within the interview situation and to remind interviewees about the general focus of the interviews (Cridland et al., 2016). The interview situation and the questioning and the communication style were continuously tailored to the individual needs of each interviewed person living with dementia. To reduce the complexity, all questions were single-faced, asking just for one aspect at a time (Cridland et al., 2016), for example, What helps you to be physically active? What hinders you from being physically active? Tell me about your current physical activity behavior. Pictures of older people, women and men, making 10 different types of physical activities were used as visual prompts to support the verbal communication (Cridland et al., 2016). The interviews were individually scheduled choosing the most appropriate time of the day for each interviewee (Cridland et al., 2016). As strongly recommended for this target group (Cridland et al., 2016), a pretest was carried out, involving one person living with mild and one with moderate dementia, to test the feasibility of the interview procedure and the interview guideline. The interviews were conducted by Doris Gebhard, who is a researcher with long-standing practical experience working with people living with dementia in care homes. Six interviews were carried out in the rooms of the residents and four in the common area of the nursing homes.
The length of the interviews varied between 6 and 46 minutes, with an average duration of 23 minutes and 10 seconds. Due to their lower communication competencies, interviewees with more advanced cognitive impairments were not able to answer all of the questions through free narrative, but tended to give short answers, sometimes consisting only of one word. Therefore, some interviews were rather short, but the voices of those people were considered equal to the input coming from interviewees who had the ability to answer in a more sophisticated way. Taking into account that there is no minimum recommendation for the duration of interviews with people living with dementia (Cridland et al., 2016; Gove et al., 2017; Samsi & Manthorpe, 2020), but a strong call to involve the people living with advanced dementia in research (Cridland et al., 2016; Gove et al., 2017; Samsi & Manthorpe, 2020), this approach provides added value to the study. All interviews were audio recorded and transcribed verbatim. The entire material comprised 107 pages.
The study is part of the project “Health in Motion 2.0” (ethics approval A 17/15). All participants, as well as their guardians in case of required legal representation, provided written informed consent. Verbal assent for interview participation was gathered directly before the interview; dissent was respected at all times (Nygard, 2006; Scottish Dementia Working Group Research Sub-Group, 2014).
Data Analysis
Transcripts were analyzed using qualitative content analysis based on Mayring (2015). Qualitative content analysis has an established position in nursing research and “is extremely well-suited to analyzing data on the multifaceted, sensitive phenomena characteristics of nursing” (Elo & Kyngäs, 2007, p. 113). Mayring’s concept of qualitative content analysis enables the combination of different analytic methods and provides a systematicand rule-based analysis with a step-by-step procedure. It is strictly controlled and flexible at the same time (Kohlbacher, 2006). Furthermore, qualitative content analysis was applied successfully in comparable interview studies with people living with dementia (e.g., Cedervall et al., 2015; Lindelöf et al., 2017) with the aim of analyzing views and experiences concerning physical activity and can therefore be expected to be suitable for the interview material produced by the target group.
Following the predetermined procedure for qualitative content analysis according to Mayring (2015), a concrete and tailored procedural model of analysis was determined as the first step. This step-by-step model determines the individual steps of the research process and their order in advance, and is constructed especially for the given research question and material (Mayring, 2014). Figure 1 shows the sequences of the inductive and deductive category development within the fitted procedural model.
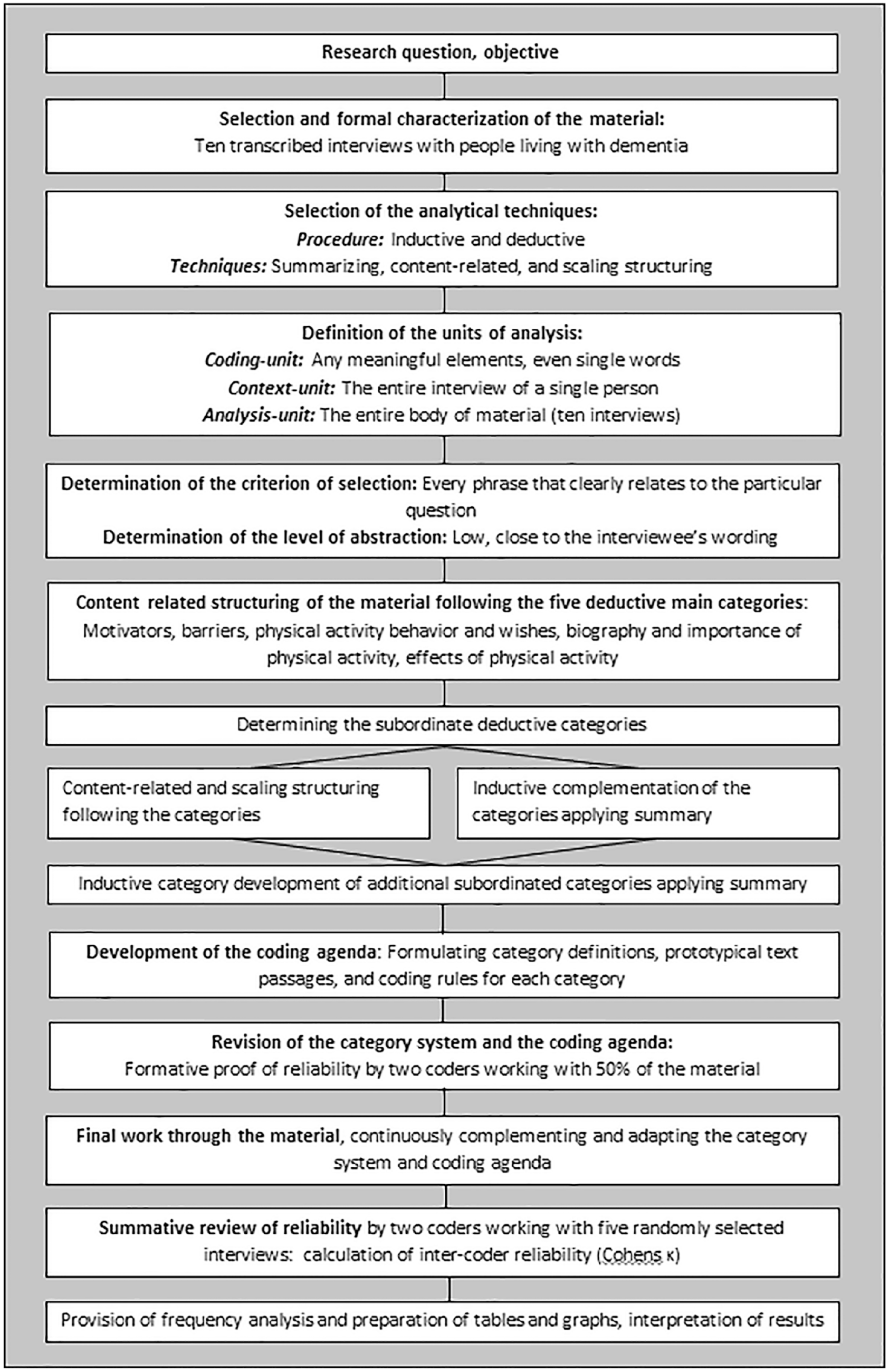
Generated procedural model of qualitative content analysis (Mayring, 2015).
Techniques for summarizing and structuring were applied. Any meaningful element, even if it only consisted of a single word, was defined as coding-unit. The interview of one person built the context-unit; the entire body of the material represented the analysis-unit. Every phrase that was clearly related to one particular interview question was defined as the criterion of selection. The level of abstraction was kept low and therefore close to the interviewee’s wording.
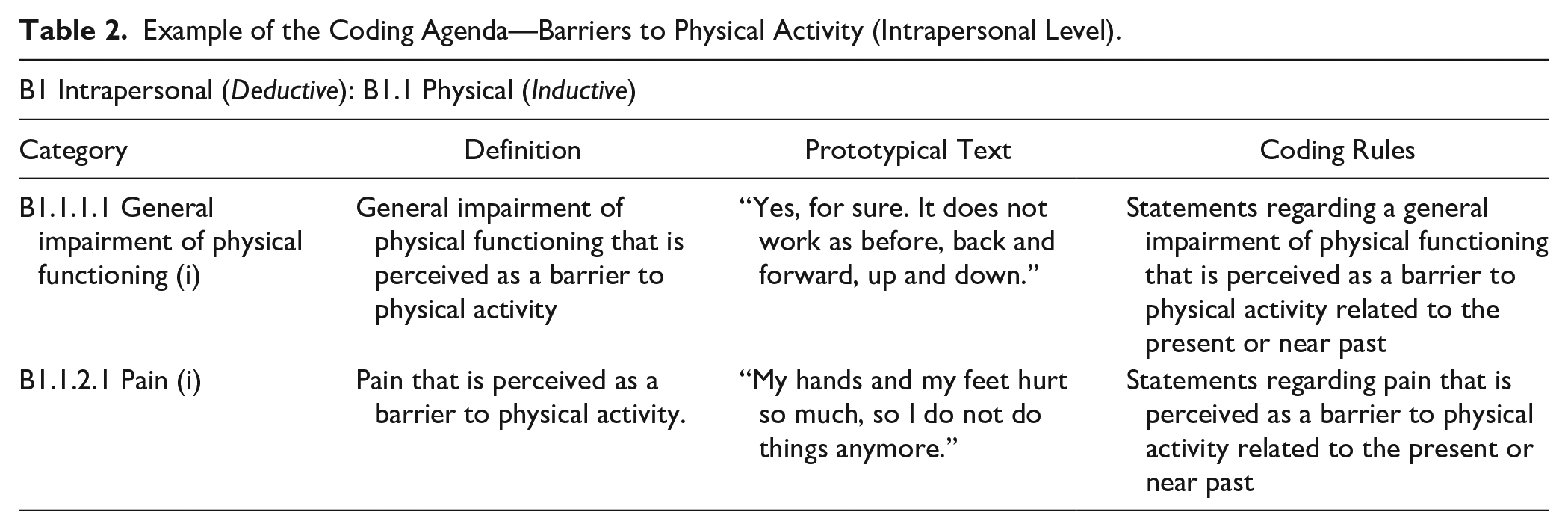
After determining these rules for the coding procedure, the analytical technique of content-related structuring was applied to the material following the five deductive categories which covered the main topics of the interview guideline. Subordinate deductive categories, such as the levels of the social-ecological model within the categories of motivators and barriers concerning physical activity, were defined based on these main categories. Inductive categories complemented those categories within the category system. Parallel to the category system, the coding agenda was developed. This procedure includes formulating the definitions, prototypical text passages, and coding rules for each category (Mayring, 2015). Table 1 outlines the rationale of the category system based on barriers to physical activity. Table 2 provides an example of the coding agenda that focuses on the subsection of intrapersonal barriers for physical activity.
Example of the Category System—Barriers to Physical Activity.
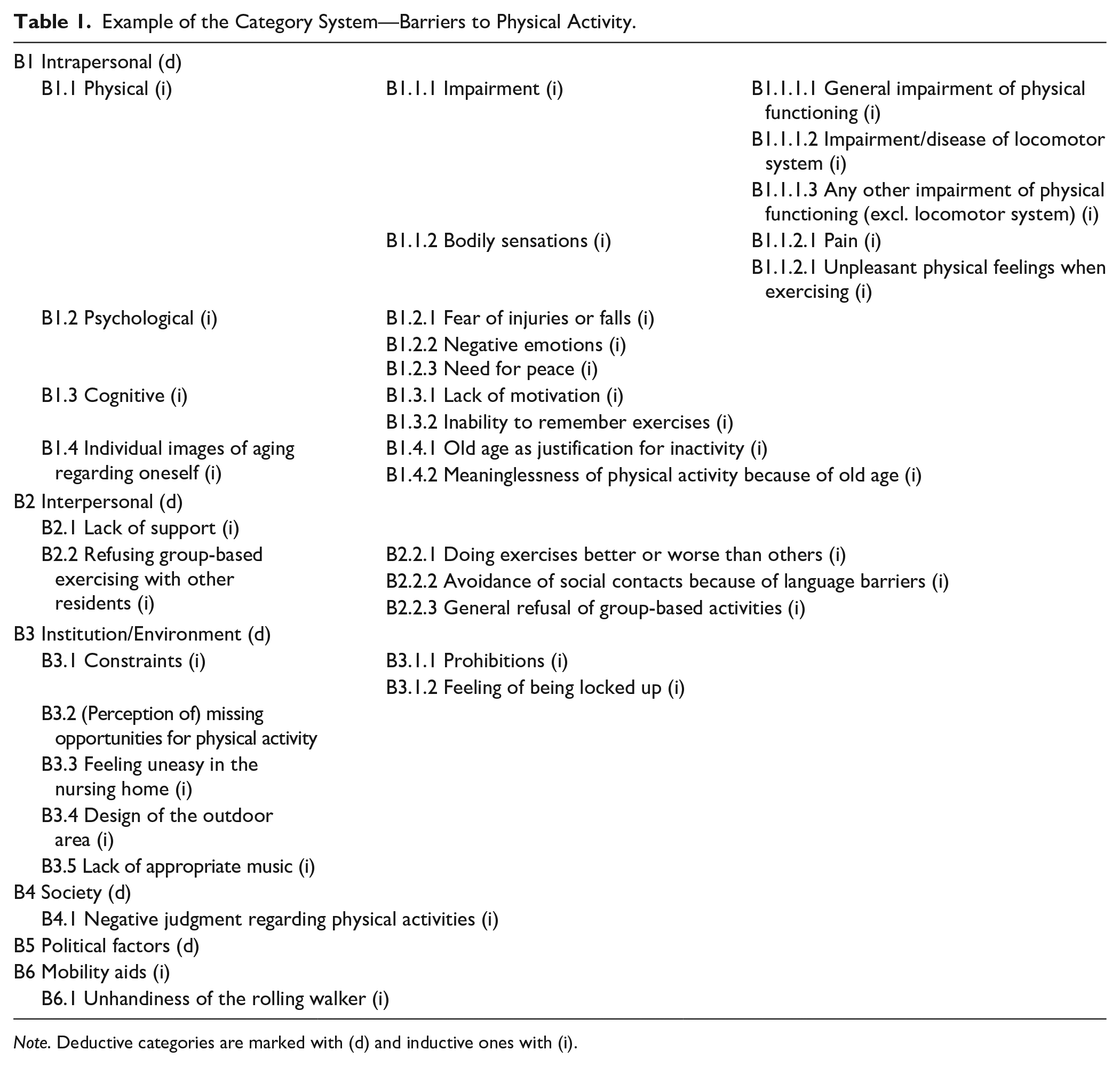
Note. Deductive categories are marked with (d) and inductive ones with (i).
Example of the Coding Agenda—Barriers to Physical Activity (Intrapersonal Level).
The category system and the coding agenda were steadily revised and complemented. In addition, two coders conducted a formative reliability proof of the categories based on 50% of the material. After having categorized the whole material, a summative review of reliability was done. This process was carried out by two coders, who applied the category system independently to five randomly selected interviews. Based on the adjusted accordance of the results, the intercoder reliability was calculated with Cohen’s κ (Fleiss & Cohen, 1973). The resulting value of κ = .94 indicates a very high intercoder reliability of the developed category system (Wirtz & Caspar, 2002).
Finally, the frequencies of the categories were analyzed. This quantitative step of analysis may give added weight to the qualitative results because documenting how frequently a category is reported can give a deeper insight into its meaning and importance as well (Mayring, 2014).
Results
The 10 interviewees identify twice as many barriers as motivators for physical activity along the levels of the socio-ecological model. Moreover, they mention the perceived barriers much more frequently than the motivators. The results indicate that physical activity is part of the past and present, as well as a desire for the future, of the people interviewed. The health-enhancing effect of physical activity is firmly anchored in the interviewees’ perception. The following section is organized by the main topics of the interview guideline: (a) motivators for physical activity, (b) barriers to physical activity, (c) physical activity behavior and wishes, (d) biography and importance of physical activity, and (e) effects of physical activity.
Motivators for Physical Activity
The participants identify 12 different motivators for physical activity. In sum, these motivators are mentioned 37 times. Figure 2 shows the categories’ structure and the number of mentions for each category. The gray boxes represent deductive categories and the white ones inductive categories.
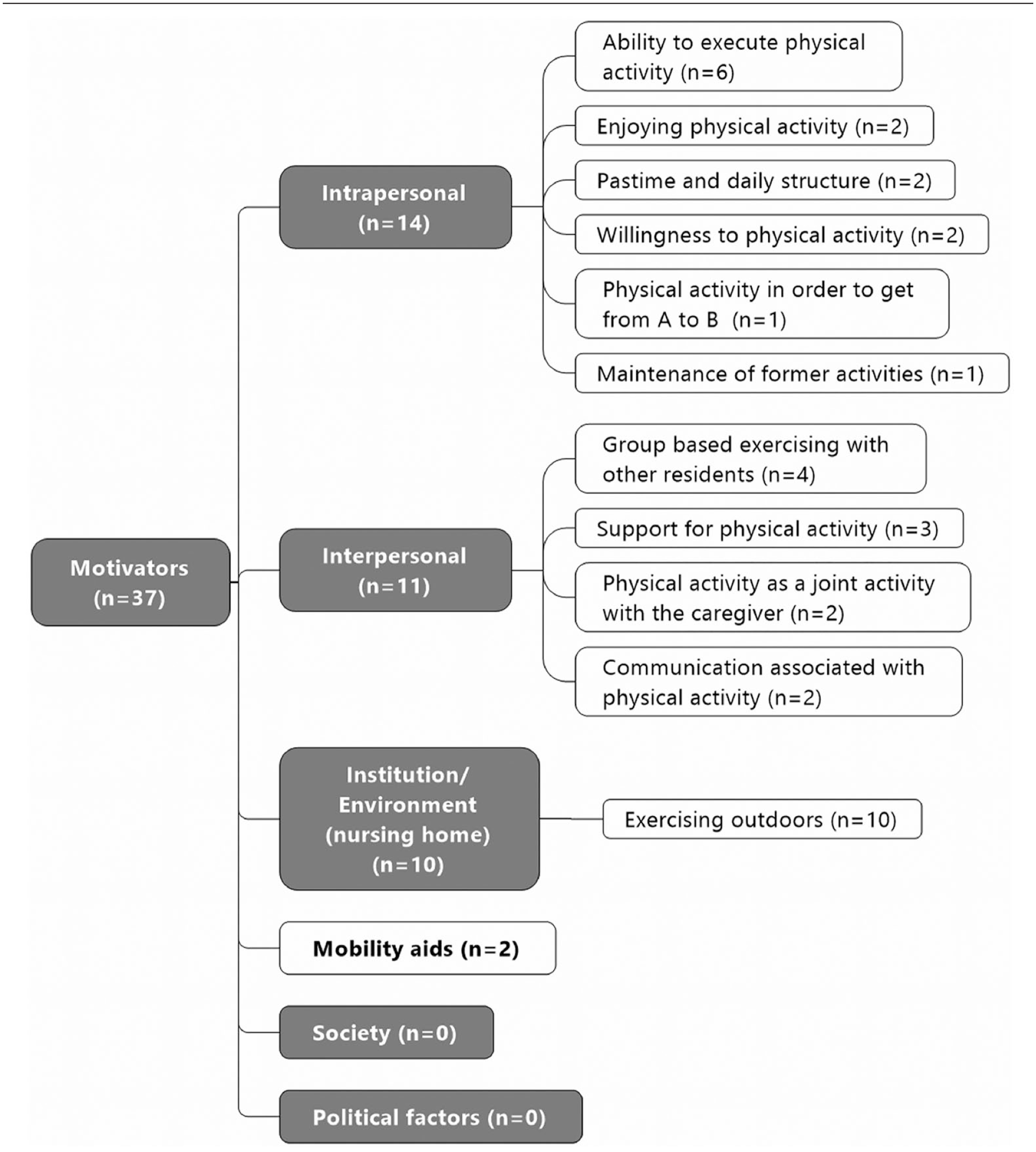
Motivators for physical activity.
Intrapersonal factors are mentioned most frequently (n = 14), followed by interpersonal factors (n = 11) and environmental/institutional factors (n = 10). The inductive category “mobility aids” is mentioned two times as a motivator for physical activity. The still extant ability to engage in physical activity is mentioned most often as an intrapersonal factor (n = 6). Interviewees talk about this ability, for example, as follows: I do it, I do it. I walk as long as I can!
On the interpersonal level, the following statement describes how not only other residents but also the nursing staff are perceived as a motivational factor: Oh, we danced together, Christine and me. She picked me up and we hopped.
All participants perceive the outdoor environment as a motivator on the environmental level as the following statement shows: If we were asked to become physically active, I would prefer exercising outdoors.
The people interviewed do not report any motivators for physical activity on the societal and political level.
Barriers to Physical Activity
Compared with the identified motivators of physical activity, the participants raise twice as many different barriers (24), and the frequency is substantially higher (n = 58). Figure 3 shows the categories’ structure and the number of mentions for each category. Again, the gray boxes represent the deductive categories and the white ones the inductive categories.
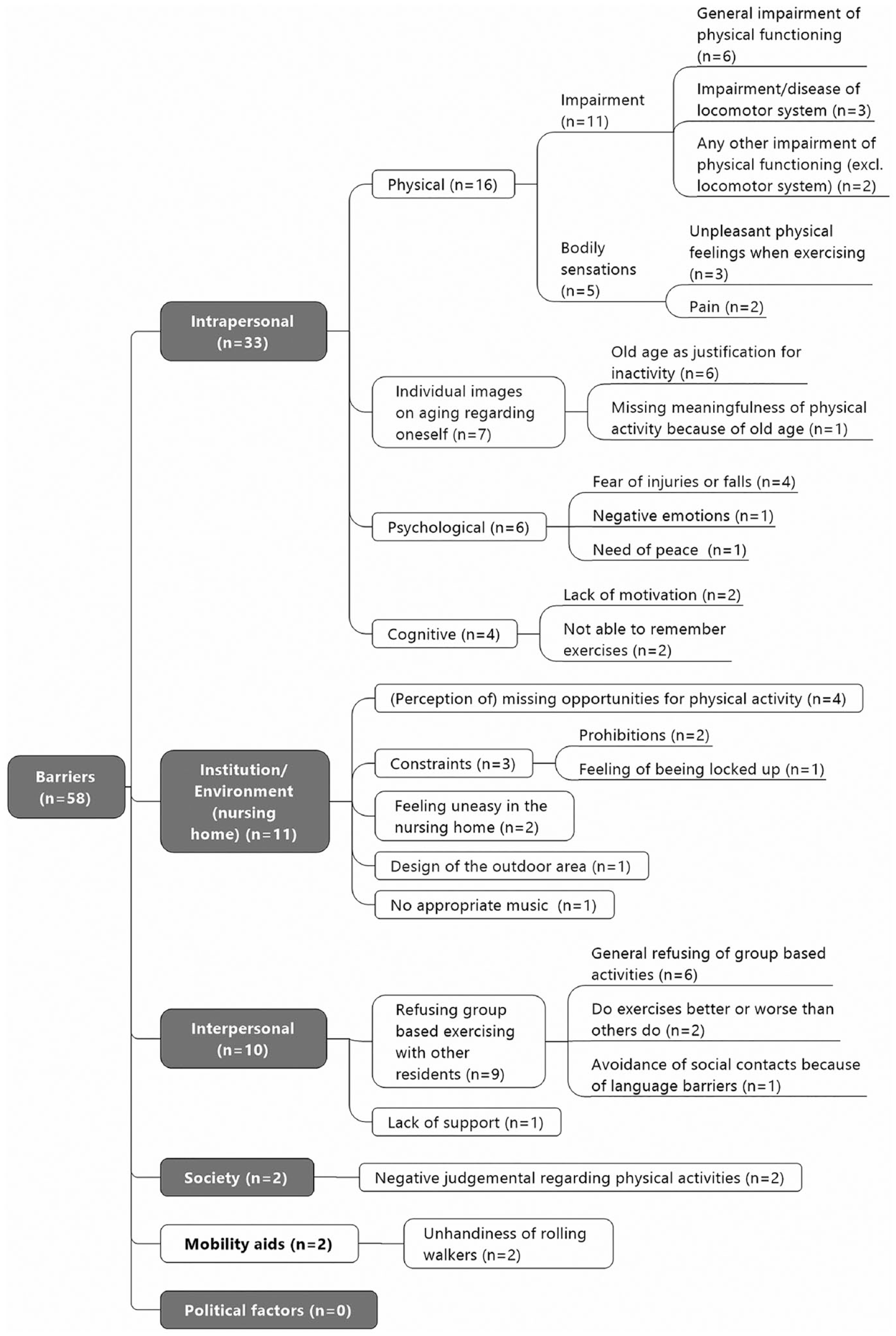
Barriers to physical activity.
As with motivators, intrapersonal factors are mentioned most frequently (n = 33). Within this category, physical barriers are brought up most often (n = 16). One interviewee characterizes the perceived physical restrictions as follows: It goes from bad to worse; I am becoming weaker and weaker because I have fallen three times. Everything decreases, as you can see.
The environmental and institutional level represents the second most mentioned category (n = 11), followed by interpersonal factors (n = 10) and societal factors (n = 2).
In the environmental context, an interviewee states how much she misses her home environment: Here I am only inside; I miss the work in my garden so much. Now I am expected to knit or read this newspaper.
Within the category of interpersonal aspects, two interviewees report their worries concerning different performance levels within an exercise group as follows: Oh, it is so creepy (she is laughing), exercises for old people; they are unable to do anything. I do know, I was already there [before her relocation to the nursing home]—I did not like it. I was wondering if I am really such an old person. Well, there are people who are professionals [he presumes]. They are much better than I am.
One participant depicts the negative judgment of physical activity on a societal level as follows: People from outside, from the neighborhood, might think the old lady is jumping around—in a nursing home! Some have seen me exercising and they said the lady from downstairs was jumping around. That is why I do my exercises when nobody can see me. They all would think, such a fool when I am exercising on my own.
Again, mobility aides constitute an inductively developed category with two mentions. Political factors are not identified as barriers to physical activity.
Physical Activity Behavior and Wishes
Nine out of 10 interviewees answered the question concerning their current physical activity behavior, and all of them are still physically active: eight go for a walk regularly, and one exercises in addition to taking a walk. Five people living with dementia express their wish for further physical activities. Cycling, swimming, and exercises are mentioned once, whereas dancing, going for a walk, and gardening are mentioned twice. Two participants wish for walks outside the building because so far they have only taken a walk on the balcony of the nursing home. The following passage of an interview illustrates how the participants express their wishes for physical activities: Would you still be interested in dancing? Yes, but we do not have such things here. We danced like this (makes dancing movements and laughs). Would you enjoy dancing to traditional music? (Nodding) Yes, if there was an opportunity!
Biography and Importance of Physical Activity
All interviewees give an insight into their biography of physical activity. Cycling (n = 7), dancing (n = 7), hiking (n = 7), and gardening (n = 7) are mentioned most often, followed by physical activity in the occupational context (n = 6), walking (n = 6), household chores (n = 6), winter sports (n = 5), exercises (n = 4), and swimming (n = 4). One person expresses a passion for tennis. The following interview passage gives an insight into the story of one interviewee: Hiking, yes, we often went hiking in the mountains where I come from. We were always there, yes, yes. Very much, everywhere on foot.
Moreover, eight participants stated that physical activity has been an important part of their lives. An interviewee describes her active lifestyle as a farmer and the importance of being physically active, even at an advanced age, as follows: To be honest, I liked working, I never complained. I helped in the cowshed, cleaning it up and so on . . . so in this way I was always physically active. Was it important to you to be physically active? For sure it was—it is true.
Five people living with dementia state that physical activity is still playing an important role in their lives. Two participants for whom physical activity was important in the past are not interested in it anymore, and three participants do not comment on this issue.
Effects of Physical Activity
Nine participants express their ideas about the effects of physical activity. All of them state that physical activity has a positive impact on health, as the following example illustrates: Yes, sure. For sure, it is good. Yes, sure, physical activity is the best thing in any case. Definitely. Well it is healthy!
Three participants share their thoughts concerning the specific effects of physical activity. They say that it has an analgesic effect, stimulates the blood flow, is an effective treatment for swollen legs, is life-prolonging, promotes healthy organs, and helps to keep physical competencies stable or increases them.
Discussion
There are very few studies like this which focus on physical activity from the perspective of people living with dementia in care homes. To the best of the authors’ knowledge, this is the first study that investigates motivators for and barriers to physical activity in this target group.
Merging facilitators and hindrances with the wishes, attitudes, and experiences of people living with dementia lays the foundation for recommendations targeting the development of programs for increased physical activity in care homes. As the results clearly show, physical activity is an important part of the biography of people living with dementia and it is still a relevant topic for them even when living with this chronic and incurable disease. Although the importance of being physically active has decreased in some participants over the years, all try to stay active and some wish for additional activities. The health-enhancing effect of physical activity is deeply embedded in the interviewees’ awareness. The results presented on motivators and barriers concerning physical activity are partly in line with the existing literature about the oldest old (Baert et al., 2011) and community-dwelling people living with dementia (van Alphen, Hortobágyi et al., 2016). The results indicate that people living with dementia face more barriers than motivators where physical activity is concerned.
Intrapersonal Factors
Similarly to the oldest old (Baert et al., 2011) and people living with dementia in the community (van Alphen, Hortobágyi et al., 2016), people living with dementia in care homes also face intrapersonal aspects most often with regard to motivation and hindrances to physical activity. Again, in accordance with the existing literature, health-related conditions are the most frequently mentioned aspects on the intrapersonal level. In contrast to the findings concerning the oldest old (Baert et al., 2011), people living with dementia experience health-related conditions mainly as a barrier. Looking at the physical health status of people living with dementia, this is hardly surprising: Compared with their cognitively healthy peers, people living with dementia have lower physical functioning, higher impairments in balance and gait, and a higher risk of falling, regardless of the age and general health status (Allali et al., 2016; Auyeung et al. 2008; Cedervall et al., 2014).
The results presented confirm fear of falling, lack of motivation, and reduced cognitive functioning as barriers to physical activity on an intrapersonal level also in people living with dementia in care homes (Baert et al., 2011; van Alphen, Hortobágyi et al., 2016). The perception of the interviewees concerning the benefit of being physically active is in line with the results of Malthouse and Fox (2014) and Cedervall et al. (2015), showing that people living with dementia are still aware of the health-enhancing effect of physical activity. Also, Karssemeijer et al. (2018) indicate that the health-enhancing effect is the most important reason for people living with dementia to be physically active. Whether, and how, attitudes concerning physical activity in people living with dementia have an impact on physical activity as behavior is still unclear and requires further investigation (O’Connell et al., 2015).
In contrast to the results of van Alphen, Hortobágyi et al. (2016) and Baert et al. (2011), people living with dementia in care homes rather see the time factor as a motivator and not a hindrance on an intrapersonal level. While community-dwelling people living with dementia complain about the time-consuming aspect of physical activity, exercising regularly helps structure the day in the nursing home setting and offers an opportunity for meaningful activities. Residents living with dementia perceive their everyday lives in nursing homes as boring and have the feeling that time passes slowly (Mjørud et al., 2017; Palacios-Ceña et al., 2016), whereas meaningful activities have the potential to influence the perception of time spent in nursing homes positively (Palacios-Ceña et al., 2016).
Interpersonal Factors
On the interpersonal level, the results presented are comparable to the existing literature. Exercising together with other residents appears to be a motivator as well as a barrier. Three out of 10 people perceive group-based exercise to be exclusively positive, whereas six people refused to participate in a group intervention. Based on these findings, individualized, targeted physical activity interventions can be suggested. However, considering all aspects on the interpersonal level, this conclusion obviously cannot be drawn without some further investigation. The support of others and the socializing effect of physical activity are perceived as additional motivators. Furthermore, one has to bear in mind that initial skepticism regarding group-based exercise programs is quite normal in people living with dementia, as Wu et al. (2015) demonstrate.
Nevertheless, studies also show that these reservations disperse very quickly when people exercise together. The feelings of discomfort and refusal switches to a positive feeling of friendship and companionship within an exercise group (Wu et al., 2015; Yu & Swartwood, 2012). Olsen et al. (2015) report that social relationships within an exercise group for people living with dementia positively affect exercise adherence. Due to the advantages of social cohesion, van Alphen, Hortobágyi et al. (2016) also recommend group-based physical activity interventions for people living with dementia as one conclusion of their literature review.
Institutional Factors
The most significant discrepancy between the results presented and the existing literature about the oldest old (Baert et al., 2011) and community-dwelling people living with dementia (van Alphen, Hortobágyi et al., 2016) appears on the institutional/environmental level. The interviewees raise six different barriers in relation to living environment with a frequency of 11 mentions: Feeling uncomfortable, prohibitions, and lack of opportunities for physical activities characterize the statements.
These results underpin the strong impact of the nursing homes’ living environment on physical activity in people living with dementia (Anderiesen et al., 2014; Benjamin et al., 2014; Tak et al., 2015; van Alphen, Volkers et al., 2016) and are in line with the interview studies of people living with dementia in care homes concerning their experience of lived space (Førsund et al., 2018). People living with dementia describe nursing homes as a low-stimulus environment (Mjørud et al., 2017) and as a place marked by rules and restrictions (Førsund et al., 2018). Even the metaphor of being in prison is associated with the care environment for people living with dementia in care homes (Heggestad et al., 2013). Nevertheless, defining the care environment itself as a barrier to physical activity is a new aspect shown by this study.
The tension between the safety aspects, on the one hand, and the people’s wish for freedom of movement, on the other hand, is obvious: in nursing homes, balancing dementia patients’ risks and autonomy is an enormous challenge, also for people living with dementia themselves (Førsund et al., 2018) as well as for the staff (Evans et al., 2018). The main reason access to the outdoor environment is limited is obviously to prevent falls and ensure safety (Evans et al., 2018). People living with dementia, however, perceive the fact of not being allowed to go outdoors as a restriction on their autonomy (Førsund et al., 2018). According to the interviews conducted, outdoor physical activity is an important issue for people living with dementia and an integral part of their physical activity biographies. The results presented indicate that people living with dementia in care homes have a deep longing to be outdoors and that the outdoor environment is perceived as a motivator for physical activity.
Also, Cedervall et al. (2015) confirm that people living with dementia have positive feelings when being outdoors, and a feeling of freedom results from it. Olsson et al. (2013) found out that people living with dementia—in addition to having this feeling of freedom—perceive outdoor activities as a confirmation of the self. Although there is limited research on the health-enhancing effects of nature on people living with dementia, and studies done so far are rather low in quality, there is some evidence that outdoor activities have a positive effect on agitation, aggression, sleep, well-being, and social interaction, as well as on mobility and preventing falls in people living with dementia (Clark et al., 2013; Gonzalez & Kirkevold, 2014; Whear et al., 2014).
Taking into consideration (a) the physical activity biographies of this generation, who predominately exercised outdoors, (b) the residents perceive a need to be physically active outside, and there is also a (c) supposed additional health benefit of these activities. For these reasons, the outdoor environment should be integrated into physical activity programs for people living with dementia in care homes.
This study has also shown that the absence of motivational music in people’s care environment is perceived as a barrier to physical activity. Moreover, the interviews strongly indicate that music has an impact on physical activity in people living with dementia. For seven out of 10 interviewees, dancing has been an integral part of their lives and they want to continue this activity. Also, in the interviews by McDermott et al. (2014), the impact of music on people living with dementia becomes obvious; music is an emotionally meaningful experience, a part of personal and cultural identity, and it helps people living with dementia build and sustain relationships with others when sharing common memories or singing together.
Furthermore, music has the potential to trigger physical activity. People living with dementia move automatically when they hear familiar music; they seesaw with their legs, clap to the rhythm, or make dancing movements (McDermott et al., 2014). Although there is scant evidence for the effects of music on people living with dementia, a meta-analysis of 34 studies indicates that music has a positive effect on disruptive behavior, anxiety, cognitive function, depression, and quality of life (Zhang et al., 2017). The body of evidence concerning dancing in people living with dementia shows a similar picture; dancing seems to be a feasible intervention, although there is little evidence for the effectiveness of dancing interventions (Mabire et al., 2018). Music is additionally discussed as an effective adherence support strategy that has been used in exercise studies for people living with dementia (van der Wardt et al., 2017).
However, the potential of using music in physical activity programs has not been exploited yet apart from specific dancing interventions. Considering the important role of music for physical activity as shown by this study and the growing body of evidence concerning the positive effects of music on people living with dementia, the inclusion of music in physical activity programs can be strongly recommended.
Community/Society and Public Policy
The absence of motivators on the societal and political levels is again in line with the existing body of evidence about community-dwelling people living with dementia (van Alphen, Hortobágyi et al., 2016). However, the interviewees’ perception that others in society see physical activities in people living with dementia negatively is a new finding. This feeling possibly occurs due to ongoing stigma and stereotypes of people living with dementia, which is experienced as a feeling of shame by those concerned (Alzheimer’s Disease International, 2012; Milne, 2010). Alzheimer’s Disease International (2012) takes a contrary view and argues that showcasing the ability of people living with dementia to remain physically active can help reduce their stigmatization and raise awareness about their existing health resources. Taking the idea of destigmatization into consideration when discussing successful aging and dementia, it becomes clear that physical activity has the potential to break up stigma also in this field—because what can be more strongly associated with active and successful aging than doing sports?
Embedding the results into the introductory discussion on successful aging that is outlined here, it is obviously the wrong approach to label people living with dementia a priori as unsuccessful agers. The results clearly show that even when living with a disease like dementia, which is accompanied by multiple barriers, people perceive health-related resources and their potential on multiple levels. This is in line with the study results of Livingston et al. (2008), which show that people living with dementia have the feeling of aging successfully, disregarding their disabilities. Also, Romo et al. (2013) indicate that most people with late-life disabilities feel that they have aged successfully: their responses to their impairment and the use of adaption and coping strategies determine whether they see themselves as successful agers or not.
This fits perfectly within the selection, optimization, and compensation (SOC) model proposed by Baltes (1997). The SOC model focuses on aging as an adaptive process and consequently on the “how,” whereas the MacArthur model (Rowe & Kahn, 1997) emphasizes a measurable state and the “what.” Both questions have to be considered when developing and realizing interventions for people living with dementia. The spectrum model of aging (Martin & Gillen, 2014) combines these perspectives and enables an individualized, successful aging plan. Based on life-span orientation, the model suggests analyzing the individual status on four interacting quadrants (biological, psychological, social, spiritual) as a starting point to maximize growth and minimize decline. Therefore, this approach asks for the “what” and makes a plan for the “how.” Asking people living with dementia about motivators for and barriers to physical activity provides valuable information for developing tailored interventions considering the “how.”
According to the idea of the spectrum model of aging, this information can be used to offer proactive plans to create a feeling of personal success and unleash untapped potential (Martin & Gillen, 2014). Putting the focus on the given health potential of a person and considering an individual’s position on the health-disease continuum (Antonovsky, 1987) without rating this position as successful or unsuccessful would help society embrace diverse aging trajectories within a salutogenic approach. Consequently the label “successful aging” would no longer only be used to refer to an aging-elite but also to people living with dementia who promote their own health resources as long as possible by being physically active.
Implications for Practice and Research
This study has both practice and research implications. Regarding practice, the following recommendations for physical activity programs can be derived from the study’s results: (a) Design physical activity programs to be adaptable to different mobility levels, and (b) tailor exercises to the individual functional capacity of all participants to overcome barriers due to health-related conditions. (c) Offer physical activity in small groups, and (d) promote the development of social cohesion actively by means of exercises that require the cooperation of the participants. This addresses the desire for social engagement and facilitates training adherence. (e) Meaningful music—according to the participants’ preferences as learned by looking at their music biography—should be integrated whenever appropriate and not only in association with dancing. Therefore, a music biography of the participants should be made and considered when selecting the type of music. (f) The gardens of long-term care facilities and nearby green spaces are the perfect environment for physical activity for people living with dementia because they satisfy the people’s need for a feeling of freedom and their wishes for nature and being connected with it. Moreover, this training environment offers diverse and rich stimuli that have the potential to compensate for the obvious lack of stimuli within the indoor environment of nursing homes. (g) To successfully expand the space for everyday movement for people living with dementia in care homes beyond structured exercise sessions, the access to the outdoor environment needs to be safe. Safety concerns can be addressed by a combination of environmental elements—for example, slip-resistant pathways, handrails, and adequate seating—and sufficient staff who not only have an eye on the residents from inside the facility but perceive the garden as a substantial part of the care environment and therefore as part of their responsibility. (h) The results indicate that people living with dementia are able to give information concerning their physical activity biography. This potential should be used to individualize effective movement patterns for the specific exercise experiences of a person or exercise group by setting thematic foci (e.g., gardening, dancing and sports games). (i) Implementing physical activity in the daily life in nursing homes and (j) empowering people living with dementia to become role models for successful aging may facilitate changes to the individual and societal images of aging (with dementia).
The study’s results also indicate important implications for further research. Whether and how the consideration of residents’ wishes, experiences, barriers, motivators, or attitudes influences the effectiveness and feasibility of physical activity interventions must be evaluated within mixed-methods research designs, including the views of people living with dementia themselves. Until now, many physical activity programs have failed to include the views of the target group in the development and evaluation process. Following Alzheimer Europe’s position paper on involving people living with dementia in research (Gove et al., 2017), methodological ways to engage people living with dementia meaningfully and effectively in the entire research process are now needed.
Strength and Limitations
This is the first study that investigates barriers and motivators concerning physical activity in people living with dementia in care homes using the social-ecological model. Considering that the voices of people living with dementia have so far been excluded from the development of physical activity programs, this study can be seen as a solid starting point for further investigation and it gives—with its detailed presentation of the research methods used—a best-practice example that could be evolved through future research. The main limitations of this study relate to the sample. The ability to generalize the results is reduced by the small sample size, the inclusion of interviews with short duration, the partly convenient selection of the participants through the nursing home manager in his role as gatekeeper, and the predetermined exclusion of people living with dementia who are not able to communicate verbally.
Conclusion
A deeper understanding of motivators and barriers concerning physical activity provides a basis for the development of physical activity programs for people living with dementia in care homes and thus enables programs to be tailored to the people’s needs. With respect to the levels of the socio-ecological model, this study provides points of reference for how people living with dementia can overcome barriers and activate their motivators for physical activity. Using biography-related music and taking advantage of residents’ existing exercise patterns, as well as the use of the facilities’ gardens as a training environment, are some feasible recommendations for practice. Setting the results in the context of successful aging theories emphasizes the potential of physical activity to enable people living with dementia to age successfully. The spectrum model of aging can uncover the given health potential of people living with dementia and the effects of physical activity which help them realize this potential.
Supplemental Material
sj-docx-1-qhr-10.1177_10497323211002822 – Supplemental material for What Moves People Living With Dementia? Exploring Barriers and Motivators for Physical Activity Perceived by People Living With Dementia in Care Homes
Supplemental material, sj-docx-1-qhr-10.1177_10497323211002822 for What Moves People Living With Dementia? Exploring Barriers and Motivators for Physical Activity Perceived by People Living With Dementia in Care Homes by Doris Gebhard and Eva Mir in Qualitative Health Research
Supplemental Material
sj-pdf-2-qhr-10.1177_10497323211002822 – Supplemental material for What Moves People Living With Dementia? Exploring Barriers and Motivators for Physical Activity Perceived by People Living With Dementia in Care Homes
Supplemental material, sj-pdf-2-qhr-10.1177_10497323211002822 for What Moves People Living With Dementia? Exploring Barriers and Motivators for Physical Activity Perceived by People Living With Dementia in Care Homes by Doris Gebhard and Eva Mir in Qualitative Health Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fonds Gesundes Österreich, project “Health in Motion 2.0” (grant no. 2622).
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.