
Abstract
Limited understanding of the psychological challenges experienced by individuals with chronic critical illness hampers efforts to deliver quality care. We used an interpretive description approach to explore sources of distress for individuals with chronic critical illness in residential care, wherein we interviewed six residents, 11 family members, and 21 staff. Rather than discuss physical symptoms, sources of distress for residents were connected to feeling as though they were a patient receiving medical care as opposed to an individual living in their home. The tension between medical care and the unmet need for a sense of home was related to care beyond the physical being overlooked, being dependent on others but feeling neglected, frustration with limited choice and participation in decision making, and feeling sad and alone. Efforts to refine health care for individuals with chronic critical illness must foster a sense of home while ensuring individuals feel safe and supported to make decisions.
Keywords
Introduction
A growing percentage of patients (5%–10%) survive an acute critical illness to develop chronic critical illness (Kahn et al., 2015). Those with chronic critical illness suffer a constellation of complex physiological, metabolic, immunological, neuroendocrine, neuromuscular, cognitive, and psychological disturbances, with repeat episodes of infection and organ dysfunction (Nelson et al., 2010; Wiencek & Winkelman, 2010). Although definitions vary, individuals with chronic critical illness have not recovered to the point of liberation from life-sustaining therapies, with prolonged mechanical ventilation considered a clinical hallmark (Carson, 2012; Nelson et al., 2010). Additional therapies might include organ support with vasopressors, inotropes, and renal replacement therapy, several courses of broad-spectrum antibiotics for ongoing or recurrent infections, and enteral nutrition (Carson & Bach, 2002; Nelson et al., 2010). The chronically critically ill population is expected to increase because of advances in resuscitation techniques, mechanical ventilation protocols, metabolic control, and treatment of sepsis (Nelson et al., 2010). Despite these advances, patient outcomes are poor, with over 50% dead within 1 year and fewer than 19% making it home and independent (Damuth et al., 2015). In Canada, those with chronic critical illness are increasingly discharged to a residential care facility capable of providing ventilator care. In the United States, individuals with chronic critical illness are often cared for in facilities termed long-term acute care hospitals, which are among the fastest growing segments of the health care system (Kahn et al., 2010).
Emerging research suggests that individuals with chronic critical illness experience a high symptom burden and significant gaps in communication (Cox et al., 2009; Nelson et al., 2004, 2007). Furthermore, surrogate decision-makers have overly optimistic expectations for recovery (Cox et al., 2009). In an American study of surrogates of patients receiving prolonged mechanical ventilation, only 26% (33 of 126) of surrogates reported that physicians discussed what to expect for patients’ future survival, general health, and caregiving needs (Cox et al., 2009). In a rare study that examined the experiences of patients and surrogates, Lamas et al. (2017a) documented poor quality of life for patients, surrogate stress and anxiety, optimistic health expectations, poor planning for medical setbacks, and disruptive care transitions. However, Lamas et al., (2017a) exploratory study was conducted in a long-term acute care hospital in the United States. It is unknown whether these findings would be generalizable to other contexts. Moreover, greater detail of the factors that underlie and exacerbate the psychological burden of chronic critical illness is necessary to inform care that meets the unique needs of those with chronic critical illness.
In our prior analysis, a remarkable number of individuals with chronic critical illness who lived in a 22-bed specialized unit in a residential care facility in British Columbia, Canada, experienced unplanned acute care hospital readmissions. Over 2 years (August 2014 to August 2016), there were 105 unplanned acute care visits from residents with chronic critical illness, resulting in a total of 725 acute care hospital days. Through our clinical and research collaborations, residential care facility staff and decision-makers expressed difficulties providing care to these residents and their family members. Staff and decision-makers articulated the clarification of resident distress as a necessary step to improving the care and well-being of this community. Exploration of expectations about health and disease prognosis was also considered a priority. Patient-perspective evidence articulating the challenges experienced by those with chronic critical illness is vital to developing patient-centered interventions and models of care for this unique and rapidly expanding population (Rose et al., 2019). An initial purpose of this research was to examine sources of distress experienced by residents with chronic critical illness related to their disease prognosis and their health care, from the perspectives of residents themselves and their family members. During the study, however, it became evident that the experiences of residents and family members were intertwined with those of health care providers (HCPs), and so we deemed it necessary to also learn from HCPs to construct more comprehensive findings. Thus, we also aimed to describe HCPs’ perspectives of resident distress and their experiences caring for residents with chronic critical illness. We will report on expectations about health and disease prognosis in a future article.
Method
This qualitative interpretive description (Thorne, 2016) research was designed and conducted by our collaborative team of researchers, clinicians, health care administrators, and patient and family partners, in line with the tenets of integrated knowledge translation (Kothari & Wathen, 2013) and patient-oriented research (Alberta SPOR SUPPORT Unit, 2018). Interpretive description was chosen because it is an applied qualitative approach to constructing subjective and experiential knowledge relevant to practice disciplines and clinical application (Thorne, 2016). Consistent with this approach, we considered the reality to be complex, contextual, constructed, and subjective (Thorne et al., 2004). Interpretive description allows for interpretation and explanation that rests upon the epistemological directionality of the applied disciplines, rather than an extant theoretical framework (Thorne, 2016). Using this methodology allows for the articulation of patterns and themes that are relevant and potentially useful for knowledge users in the clinical setting. Thus, this study was conceptualized and designed by our research team of diverse disciplines, expertise, clinical responsibilities, and lived experiences that also represented the intended audiences for study findings. That is, we designed the research, including the research purpose, sampling approach, and data collection and analysis, to generate findings that would meet the knowledge needs of the providers and decision-makers in the facility, with an eye to application. Our team included two critical care clinicians (a nurse practitioner and a physician) who provided outreach to the practice setting; two administrators from the practice setting; two patient and family partners with related lived experience though not in the specific clinical setting; a nurse researcher and a nurse research assistant.
Our integrated knowledge translation (Kothari & Wathen, 2013) and patient-oriented approach (Alberta SPOR SUPPORT Unit, 2018) to this study meant that all team members were considered equal partners in all phases of the research. Integrated knowledge translation, with the focus on partnerships between researchers and decision-makers (clinicians, managers, etc.), and patient-oriented research, with the focus on engaging patient-partners, directed us to promote ongoing involvement of all team members. We participated in regular group meetings typified by open dialogue about study design, evolving data collection, analysis and findings, and individual and group reflexivity. We focused on experiential knowledge, mutual learning, openness, and respect to promote equal partnerships in these meetings (Abma et al., 2009). Team members provided input into all aspects of study design and reviewed study documents, such as consent forms and interview guides, as well as data analysis, as described below.
Beginning at data collection and continuing throughout the analysis, we engaged in group reflexivity as a way to reflect on how we were influencing the data collection and analysis, and ultimately the overall findings. This involved self-reflection, both written and through introspection, and then the sharing of our insights with the larger team during team meetings. For example, at the beginning of data collection, each team member reflected on the following questions, which we then discussed: What are your motivations for being involved in this research? What interests you the most in this research? What are your assumptions about the following: the individuals living at [Facility], the family of individuals living at [Facility]? the care provided at [Facility]? During data analysis, the team members who conducted the initial open coding reflected on and discussed the following: What strikes you as important? What surprises you? What emotions does this evoke? What questions arise for you? During analysis, our larger team also discussed similarities and differences with how each of us was interpreting data. Our reflections and group discussion were structured initially but then evolved such that we discussed our insights regularly in team meetings.
Setting and Study Participants
This research was conducted in a specialized unit in a residential care facility in British Columbia, Canada, which is dedicated to the care of ventilated residents with chronic critical illness. This represents the second largest cohort of individuals with chronic critical illness in a residential care facility in the province. Following approval from the Fraser Health and University of British Columbia Ethics Boards, a member of the resident’s circle of care team approached all residents and a family member designated by the resident, to obtain consent for the research team to invite them to participate in the study. Inclusion criteria for the residents with chronic critical illness included being cognitively intact (as indicated by the attending physician), English speaking, and ventilator dependent but able to communicate verbally, by mouthing words, or through use of adaptive technology. We sought to enroll a family member of the residents who were not cognitively intact or who were unable to vocalize, write, or be understood by the interviewer via spelling board or assistive communication devices. Family members were included who were the designated surrogate decision-maker and spoke English. After potential participants (residents and family members) consented to be contacted by a member of the researcher team, who was not a member of the resident’s health care team, we explained the study and obtained informed consent. Of the eight residents who consented to be contacted by the research team, one declined participation and another passed away. While interviewing residents and family members, it became clear that HCPs figured prominently in their narratives. Thus, we deemed it necessary to also interview HCPs to understand the complexity of experiences. All 45 HCPs employed to provide care on the specialized unit were invited to participate, of which 21 contacted the research team and provided informed consent to participate.
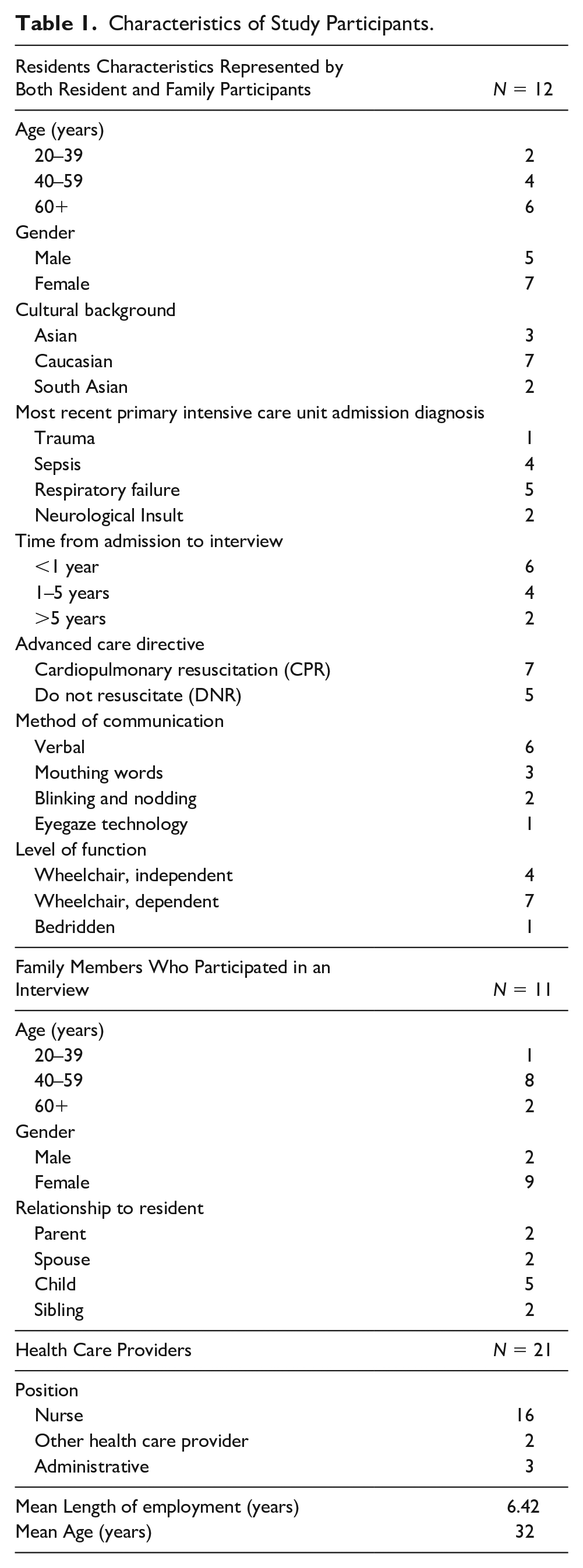
The participants in this study consisted of six residents with chronic critical illness, 11 family members, and 21 HCPs, for a total of 38 individuals. The six residents and 11 family members represented a total of 12 individuals with chronic critical illness who currently or in the past resided in the facility. See Table 1 for participant demographic information and disease characteristics.
Characteristics of Study Participants.
Data Collection
We conducted semi-structured interviews with residents with chronic critical illness, family members, and HCPs. In-person interviews with residents and family were conducted either at the resident’s bedside, in a separate private conference room at the facility, or off-site at a community center, as per participant preference. Interviews lasted 45 to 120 minutes. Family participants were also given the option of a telephone interview to accommodate their busy schedules. We conducted resident and family interviews in locations preferred by participants and that enhanced our ability to maintain their confidentiality. Depending on resident preference, these interviews were either conducted independently or in conjunction with a family member. Two interviewers were present in all interviews including a resident to facilitate interpretation of communication. We developed the interview guides through research team input and also built on Lamas et al., (2017b) conversation guide for chronic critical illness to include questions about sources of distress. These interview guides (see Supplemental File) were constructed to query sources of distress (the research purpose explored in this article) as well as expectations of health and disease prognosis (the research purpose explored and to be reported on elsewhere). Of note, however, these interview guides were not strictly adhered to, but rather, served as a means of facilitating conversation and encouraging participants to communicate their experiences. As such, the interviewers followed the participant’s lead by encouraging elaboration, through prompts and follow-up questions, on aspects of illness and distress that were raised by participants. The interviewers also asked additional questions that emerged through dialogue. We collected resident demographic and medical information from the medical chart after the interviews. HCP interviews were conducted via telephone by a nurse research assistant rather than at the facility to maintain participant confidentiality. The HCP interview length ranged from 30 to 45 minutes. All interviews were audio-recorded, professionally transcribed verbatim, de-identified, and checked for accuracy.
Data Analysis
Our analysis was guided by the applied analytic direction of interpretive description, involved research team input throughout, and was assisted by the data management software NVivo™ version 10. Data collection and preliminary analysis occurred concurrently and iteratively. Following each interview, the two interviewers discussed the insights and experiences shared by participants. Based on these discussions, the interviewers asked additional questions in subsequent interviews as a way of extending and elaborating on earlier interviews. Four research team members, who were not staff at the facility, initially read the transcripts multiple times and used open coding techniques to illuminate data segments in each of the transcripts that were indicative of key ideas, patterns, diversities, and exemplars of resident and family member accounts of distress. This open coding provided the scaffolding to develop our preliminary coding frame. This preliminary coding frame was discussed at length by the larger research team and revised accordingly, resulting in 15 codes. One team member then applied the revised coding frame to resident and family interview data in NVivo. As analysis progressed, three team members used constant comparative techniques to compare pieces of data (an interview, a statement, a code) from data that were extracted for each of the codes. Through group discussion, we grouped and regrouped analytic codes into broader categories (the 15 codes were eventually regrouped into five broader categories), reflecting higher levels of conceptualization, such that key ideas were highlighted with examples and quotes from the data (Charmaz, 2006; Strauss & Corbin, 1998; Thorne, 2016). For example, the individual codes of loss of meaning, loss of purpose, loneliness, boredom, and sadness/depression/despair were combined into the broader category of feeling sad and alone. All team members reviewed the regrouping of codes into five broader categories along with the extracted supporting data (produced through NVivo coding), and as a team we discussed details of these categories and how they fit together. One team member then applied the revised coding frame to the HCP data. We compared and contrasted resident and family data to HCP data because of emerging divergence in their accounts. As the analysis progressed, we refined the analytical categories into themes that represent a descriptive interpretation of sources of distress experienced by residents, from the perspectives of residents, family members, and HCP, as well as HCPs’ experiences of providing care. That is, during a subsequent meeting wherein all team members provided input on the preliminary written findings, we came to a consensus that our five broader categories were best described as one overarching theme (the tension between medical care and an unmet need for a sense of home), which was related to, and explicated in, the four themes specified in the results.
To maintain participant confidentiality, we did not report demographic information when providing examples or quotes. Our research team reviewed the text with the explicit aim of deleting or changing participant details that could identify individuals (e.g., gender, the relationship of a family member to a resident, the type of HCP) in quotes or examples. However, we acknowledge the possibility of deductive disclosure (Kaiser, 2009), wherein an individual with extensive knowledge of the facility, the residents, and the staff could associate individual participants with presented results.
Results
Rather than discuss physical symptoms, such as pain, breathlessness, or fatigue, the sources of distress for residents were connected to feeling as though they were a patient receiving medical care as opposed to an individual living in their home. The accounts of residents, family members, and HCPs suggest that the tension between medical care and an unmet need for a sense of home was related to (a) care beyond the physical being overlooked, (b) being dependent on others but feeling neglected at times, (c) frustration with limited choice and participation in decision making, and (d) feeling sad and alone. In describing each of these four themes below, we draw attention to resident and family perspectives and experiences first to center the results around their accounts and then describe HCP perspectives.
Care Beyond the Physical Being Overlooked
In this theme, we describe the resident and family unmet need for holistic care wherein residents felt known, care beyond the physical wherein residents felt seen, and a physical environment that contributed to a sense of home. We then describe HCPs’ reasoning for, and experiences of, prioritizing medical care and being limited in their ability to provide care beyond physical needs.
The residents and family perceived that on a day-to-day basis, their medical care, particularly concerning their mechanical ventilation, was the priority of the HCPs and the facility. Overall, the residents and family were confident in the “good vent care” and complimentary of the HCPs’ knowledge and skills in managing this aspect of their care. Although acknowledged as necessary, the prioritization of the highly technical medical care was seen by some to be at the expense of HCP recognition and attendance to other symptoms or care needs. Coupled with resident cognitive and communication impairments, some residents and family highlighted the challenges HCPs appeared to face in coming to know the residents in a holistic sense, as individuals with unique personalities, preferences, and care needs. This was exemplified by the following example shared by a family member: The other day the nurse said to me, and it was kind of, the tone of voice I didn’t appreciate really. She was kind of laughing at my mom in a sense that, oh, your mom thinks you’re going to come and get her today. And I said, oh yeah, like that’s normal. But that nurse has been taking care of her for quite a long time now. I’m thinking well why doesn’t the nurse recognize this as normal behavior for her? I certainly do. Sometimes I wonder how much they, pay attention, to her, symptoms, or to her problems. I know that they take care of the trach, fantastic. I’ve no, no problems with that at all. They seem to have that under control one hundred percent, but she has other issues that they don’t seem to take into account.
The absence of holistic care left residents and family feeling that the resident was not known or understood as they would be in a place that engendered a sense of home.
It was widely reported that resident dependence on life-sustaining technology and the complexity of their own and other resident care needs demanded an established daily and weekly routine of care. For some, this routine provided structure to their days and comfort from knowing what to expect. Yet, for others, HCP strict adherence to routine restricted resident choice and participation in meaningful activities, wherein the routine was articulated by a family member to be, “basically it’s just plug her in, because of the vent, and let her sit in one spot.” The “basic,” “simple,” and “little things,” such as bathing, grooming, dressing, and personal care, enhanced resident well-being, contributed to their feeling cared for, and was a resident priority, as conveyed by a family member: She just wants to get comfort care here. I think the most important for her, is that her basic needs are met. You know, combing her hair, changing her clothes. You know she’s really into her appearance. So yeah she likes to try different clothes. And make sure she has her lotion on. Like when she gets a shower, you know even once a week.
These components of care were particularly important because, as one resident stated, they had “lost all else,” and yet, this care was thought to be overlooked at times, which became a source of distress for some. One resident commented that, Getting me up and getting me in my chair, yeah, they do that well. The grooming, not so much. They don’t really care if I look good or feel good. They just care that I’m up and dressed, basic. They don’t take the time. They don’t see who I am. I’m invisible.
When care beyond the physical was overlooked, the residents did not feel cared for, seen, or valued, which detracted from a sense of living in their home.
The residents and family also described the physical environment as reflecting the prioritization of highly technical, medical care, wherein the HCPs could ensure regular and emergency care when required. Individual resident rooms were equipped with lifts, enteral feeding equipment, mechanical ventilator equipment, assistive communication technology, and emergency airway equipment for example, which at times did not leave space for personal items. For some, the physical environment was more akin to a hospital and perceived to conflict with a sense of home, as described by a family member: Her room and even the whole area, has gotten to be more and more, of a hospital. More and more for the benefit of the nurses rather than for the benefit of the residents. Like her room, and they keep tacking stuff on the walls. Like for, emergency equipment, and, all these different things. She had quite a bit of furniture, but they asked me to get rid of some of the furniture because it’s in the way now. And so I did take most of it away. But now they’ve just kind of shoved the rest of the furniture to the side. And, I just, feel that they, they forget that this is where the people live.
The HCPs described the residents as “living on a razor’s edge,” considering their degree of frailty and dependence on life-sustaining technology. They emphasized the need to prioritize medical care, particularly mechanical ventilator care, considering the real risk of death in the event of a miss or mistake. Overall, HCPs were confident and took pride in the “good care” they provided. Following protocols with exactitude enabled them to attend to equipment monitoring and ensure residents were “clean and comfortable.” Some HCPs insisted they had “good staff to patient ratios,” but others provided contradictory evidence wherein they portrayed a routinized “task-oriented” environment in which they struggled due to time constraints. An HCP explained how staff members were required to adhere to a specific care plan, but because “baseline staffing levels were never met,” they felt forced to deny resident requests for anything beyond specifications in the plan. Several HCPs described how they “stretch themselves” by helping a resident send a text or allowing them to take an hour to bathe, but then they worried that deviation from routine would become a “baseline expectation.”
Several HCPs also mentioned difficulties caring for residents who expressed anger and resentment; however, they linked these situations to the challenges of informing a declining resident that more invasive technology would be required daily. One HCP acknowledged that the prioritization of medical and ventilator care excluded any physical or recreational therapy for residents. This participant reflected that “I don’t think we’re residential, we’re sub-acute,” as though reclassifying the facility might better explain the efficiency-based, medicalized environment without any pretense of providing a sense of home.
Being Dependent on Others and Also Feeling Neglected
In this theme, we describe resident and family distress associated with the resident being dependent on others and also feeling neglected. Feelings of neglect undermined resident self-worth, dignity, and sense of safety, which detracted from a sense of home. We also describe the challenges HCPs experience in attempting to meet the multiple competing demands of residents.
All of the residents experienced a loss of independence in almost all aspects of their lives, which contributed to their feeling frustrated, sad, exhausted, and impatient, particularly when their needs were not met. Several residents expressed a desire for greater control in their day-to-day lives. Navigating ways in which to interact with HCPs, upon whom they were entirely dependent, was not always straightforward. A few residents and family members described feeling ignored, dismissed, or neglected by HCPs when their basic or medical care needs were not met, and also when their only interaction with an HCP was related to their need for medical assistance. These experiences undermined their sense of value, self-worth, and dignity. One resident described this suffering: No one comes in, does anything. No range of motion, no anything. And they just, they’re really comfortable basically letting you sit in your, what feels like, just letting you be alone in your room for the rest of your life. That’s what it feels like. And, if I don’t call my call bell, no one will come. Cause they’re always preoccupied. But that’s what it feels like. It feels like, they just left you in a room, room to die.
But the residents and family also acknowledged the complex medical care and demands of providing complete care for residents to be challenging for HCPs, requiring substantial yet unrealistic time and resources. The HCPs were considered to be busy, run ragged, tired, stretched to the limits, and unable to meet the resident’s needs at times, as shared by a family member: It takes 20 minutes to get her into a chair. . . They’re [HCPs] stretched to the limits. It’s not, their fault that they can’t do it. . . And then you can’t get her out of the chair. . . One person covers the whole floor kind of like. So, when she wants to get back out of the chair, she can’t, because there’s nobody to cover, to take her out of the chair. . . . It’s that they are just run ragged.
Cognizant of HCP workload, residents and family commonly reported worrying about being a “nuisance,” “burden,” or “bother” to HCPs, and thus limited their requests for assistance. Other residents noted that because they were not “demanding,” their needs were not attended to by HCPs, as described by a resident: Sometimes I feel like they [staff] aren’t listening because I see other residents being helped because they are more aggressive. And my style isn’t to be aggressive so they ignore me. I just wait and hope.
Moreover, several residents and family members expressed fear and worry that HCPs might not respond, even in the event of an emergency. Not feeling safe detracted from a sense of home. While they recognized their own or their loved ones’ poor prognosis, they did not want death hastened because of a medical mistake or neglect, as explained by a family member: I just hope they’re able to respond to her vent alarm in a timely manner . . . I don’t want her to go like if somebody made a mistake. If they’re not able to respond. Because a couple, like, five times it happened she speed-dialed my number, and I wasn’t able to get a hold of the nurse . . . So I was able to call them. And they, they went there. But that’s my biggest fear. They’re not able to get her in a timely manner. . . . And, uh, it just that’s my biggest fear.
HCPs described an environment in which they perceived it was impossible to provide for various human needs that arise for totally dependent residents unable to turn over, scratch an itch, speak or communicate without a lengthy assisted interaction. HCPs spoke about residents’ competing demands for their attention and the difficulty they faced maintaining residents’ scheduled care (i.e., a regular bath time) as well as spontaneous requests for help. The staff was aware that residents also became frustrated when daily schedules were changed or delayed due to emergencies, illness, or staffing issues. HCP commentaries portray a lose–lose situation, in which some of the residents strategized ways to gain more attention and staff felt the pressures of limited time and deflected or stalled those requests. An HCP remarked that residents relied heavily on staff because “they’re basically isolated in the room and not everyone’s family visits regularly.” These interviews also confirmed the gap between family expectations of individualized care and the gap HCPs confirmed between what residents needed and what the structure of the care permitted them to provide. For instance, an HCP described how routinized protocols dictated her interactions. She said when she entered a room to get the resident up in the morning, “10, 15 minutes are gone, for doing nothing, like open the curtains, close the window . . . come on that side, fix my arm.” Other HCPs expressed more understanding of these everyday human needs and felt the same restrictions juggling residents’ requests. Adding to the challenges, HCPs stated that there were limited physical or psychosocial services that might ameliorate a resident’s frustration living in a locked body.
Frustration With Limited Choice and Participation in Decision Making
In this theme, we describe resident and family frustration with having limited opportunities to make choices and participate in decision making, which were considered as important aspects of a sense of home. We also describe HCPs’ challenges attempting to facilitate resident choice and decision making in the context of complex resident care needs and entrenched medical routines.
Resident communication impairments, difficulties obtaining information, and HCP routines were perceived as interfering with opportunities for the resident to participate in decisions or make choices related to activities of daily living. These activities included bathing, mobilizing, leisure activities, such as doing a puzzle or reading, as well as medical care. The freedom to make choices was considered an important aspect of a sense of home, as shared by two residents: You know if it’s your home, in your home, you have the freedom to choose and to do things that you want to do and that, that’s not necessarily something I feel here. Life is about making choices. And living the way you like to live. I need that. This is my home! Yes, it’s a medical facility, but treat it like my home, where I have a say.
The residents and family described struggling to adapt to communication impairments related to dependence on a ventilator, loss of ability to verbalize, overall weakness and fatigue, and difficulties using assistive technologies, such as tablets or eye gaze technology. These communication impairments limited resident self-expression and the ability of others to help actualize resident choices and decision making. When asked what the resident struggles with most in their day-to-day life, one family stated, That you’re understanding her. Communication wise . . . . I’ve tried a tablet, and I’ve tried a laptop. She doesn’t have the strength, it doesn’t work. It just doesn’t work. Even pointing at letter boards. That doesn’t work. . . . it’s hard, hard time communicating.
As shared by another family member, “I know they [resident] wanted to talk to [staff] the other day. They [resident] just could not tell him [staff], what they wanted to get across. It just wouldn’t come out.” These communication impairments restricted the ability of some residents to engage in conversations necessary to make choices. Of equal importance, communication also required significant time and skills for others to understand what the residents were expressing. This was seen to be time that HCPs did not always have and contributed to the commonly expressed feeling that residents’ choices were not considered because HCPs “do not listen.” Not feeling listened to resulted in the diminishing of the residents’ sense of home. Family members further highlighted resident frustration when the resident did not remember or was confused about their own medical condition or restrictions in their abilities to communicate, mobilize, or perform activities independently for example.
Regardless of resident and family understanding of their medical condition, both commonly reported that they “get the scraps” and had to “bug staff” for updates and information, thereby limiting their ability to consider future medical possibilities or options. A few residents highlighted their desire to choose activities or medical options they understood to be inconvenient for the staff or medically “risky,” such as postponing or changing their medications, changing the type of tracheostomy or ventilator settings, or eating by mouth. In these situations, residents believed that many HCPs did not understand or appreciate their wishes and were unwilling to acquiesce to their choices, as shared by the following resident: I’m aware of the consequences of what I’m asking to try but they don’t listen—or they listen but the next day they have no desire to help me. So they don’t give any consideration to my choice. They make decisions and they don’t tell me why. I have to ask because they don’t even share their intentions.
Being unable to participate in decisions, exercise their autonomy, or take informed risks contributed to some residents feeling as though they had few choices, they were not heard by HCPs, and “things are done to me, not with me.” These feelings culminated in anger and frustration, as well as conflicts with HCPs. As one resident stated, It’s either their way or nothing [for] everything and anything. It’s a vicious setting. I get the silent treatment. It’s really hard cause they’re [staff] mad at me over and over and over.
Another resident explained how they are, “trying to make more noise. I’m getting really angry because I don’t have much time left.”
The commentaries from HCPs offered specific examples of how residents attempted to exert some small measure of control over their daily routines. A staff member conveyed a common situation whereby some residents refused care from new or casual staff, rather than trust an unfamiliar worker who may not understand their particular bodily limitations. This HCP asserted how nursing care should be flexible and adapt to resident needs, changing shower days or times to accommodate resident choices for example. However, it was also clear that the entrenched routines were not flexible and failed to offer residents any negotiation or choice in their day. For this reason—the complete absence of choice in daily life—an HCP remarked, “When you tell them this is their home, how could you possibly . . . [call] this home?” Several HCPs noted that the concept of home was at odds with the lack of choice inherent in the medical routines. Yet, rather than imagining a more flexible approach with some degree of resident choice, HCPs recommended that new residents and their families needed to downgrade expectations and “prepare their mind” for how operations run.
HCPs repeatedly commented on the challenges of learning how to communicate with residents, but over time they described developing confidence and learning the subtleties of communicating with residents unable to speak or gesture. However, communication restrictions could interfere with understanding what residents wanted on a daily basis. Furthermore, as residents deteriorated, communication issues interfered with the resident’s ability to express wishes or make choices about future treatment and care. For example, one HCP described a situation where a resident had communicated that they had wanted full resuscitation but after a respiratory and neurological decline, the resident was no longer able to discuss or revisit their decision not to limit medical treatment. HCPs perceived that most residents were not fully able to realize the trajectory of their illness and instead the residents focused on small day-to-day events. This limited any potential negotiations about significant changes in treatment or care.
Feeling Sad and Alone
In this theme, we describe the resident emotional despair and distress stemming from being chronically critically ill and anticipating a truncated future, feeling lonely and isolated, and not engaging in meaningful activities, all of which diminished the residents’ sense of home. We provide further details from the perspective of HCPs and their suggestions to begin to meet residents’ emotional and social needs.
The residents and family conveyed a sense of deep sadness. They described the residents’ feelings of hopelessness, worthlessness, depression, and despair, which waxed and waned for some, and persisted for others. For many residents, these emotions stemmed from feeling as though life had “lost all importance” and that they “have no future.” One resident shared their despair: I feel like just generally, like if I didn’t have my family I wouldn’t even care to be alive. Like I just don’t even care. There’d be no point in all honesty. It just feels like I’m just a little waste of a resource or, just taking up space.
Unresolved anxiety, frustration, and deep sadness often accompanied setbacks in residents’ health.
Pronounced loneliness and social isolation were common among residents, wherein they described being alone most of the time and having “no one to really help you through things.” This was attributed, in part, to few opportunities to socialize because of immobility and communication impairments, as well as differences in resident interests. Moreover, the limited available activities that resulted in residents “confined to” and often staying in their rooms were reported as distressing, as shared by the following resident: I really learned to be alone. Like I’ve had to learn to be alone. Like it’s like survival, otherwise, I would have broken down, like, out of. I would have died already, or, gone into like, like a psychotic state or something. It’s frustrating. It’s annoying, it’s tough.
For most residents, family members were their only visitors and the primary people with whom they socialized, aside from HCPs. Those whose family visited regularly expressed deep gratitude, yet some family members were unable to visit, and other residents had no family or friends. Overall, feeling lonely, disconnected, and unable to share in meaning-making with others contributed to residents’ diminished sense of home.
Some family reported that their loved one had lost motivation or interest in those things that might help to alleviate their psychosocial distress, such as venturing outside their room, engaging in leisure or meaningful activities (e.g., reading, going to the church service), and/or socializing with others. One family member recounted this decline: She’s not even interested in reading anymore. I found the level of interest has declined as well. She watches television. If somebody would come by and read a book. Say, okay, what kind of novels do you like? Or, read to people, visit people. The violinist. That was lovely. And there was about, oh 50 people, all around, just, you know it was people that were volunteering their time to play. It was nice. She remembers it. It does, it really does [make a difference].
Family members also described the anxiety and distress some residents experienced in relation to these activities, particularly leaving their room or the facility, and fearing that their ventilator or other vital equipment might fail. Past experiences wherein residents had a “close call” when outside the facility (e.g., vehicle lift malfunction, ventilator battery almost empty, unable to hear ventilator disconnection alarm) were recounted and factored into subsequent resident decisions, often resulting in limiting activities, as described by one family member: She’s really choosing to isolate herself to her room. I try, you know when I’m here we’ll try and get her to at least, go for a walk in the courtyard. But that’s a bit stressful for her. So you know usually it’s just a short walk.
And yet, residents and family also spoke about how engaging in leisure and meaningful activities was essential for “feeling human.” The residents yearned for simple experiences with “different stimuli,” such as going for a walk, seeing and interacting with animals, listening to music or to someone reading a book. One family member described this as follows: When I push her out on the street, there’s, there are people walk by with a dog. And they’ll let us touch it. And, it was like, she’ll put her hand out, and like to touch the bush, just when I’m wheeling her just so she can feel something that’s not, in the room, like. The bush looks pretty. She goes, it looks soft. I say, well, you know, and so she’ll try to touch the bush. And it’s just different stimuli.
Again, this reflected the tension between the prioritization of medical care and a sense of home, where home included engaging in meaningful activities and doing things that brought comfort and joy.
The HCPs confirmed that the facility provided minimal psychosocial services or support groups, although a social worker and psychiatrist were available. Nursing staff acknowledged the importance of psychological and recreational support but their skills and workload routines precluded HCPs from providing such activities. Almost all HCPs commented on the need for recreation and/or psychosocial services for residents. A staff member said, “. . . it would be a win-win situation.”
The staff recognized the boredom residents faced when confined to their rooms. They noted that most residents did not have daily contact with family or friends, which meant they lacked support to leave their room or enjoy a simple activity. Several HCPs suggested that residents would benefit from spending time with others, either through the creation of a volunteer program or by expanding a social work program. One HCP stated that everyday residents “get turned [in bed] and watch TV but maybe if they had some different stimulation they would feel better . . .” When asked, HCPs were able to generate various activity ideas that could alleviate the isolation and hopelessness residents faced with no social outlets. A staff member disclosed the guilt she felt not being able to take time for residents: Each time you pass by [residents in front of the TV] you feel kind of guilty because they’re calling you and you can’t go. . .if I have a resident looking at me, staring at me, I know that she looks okay but she just needs somebody to talk to.
Although the limitations of mechanical ventilation overshadowed what staff could envision to improve residents’ psychosocial quality of life, they shared how introducing therapeutic pets, training volunteers in special communication to sit with residents, or incorporating recreation assistants who could play games, music, or read aloud to residents would be a significant improvement—for everyone.
Discussion
This exploratory qualitative study adds to the emerging literature that describes in depth the experiences of individuals with chronic critical illness and their family members, which also includes the perspectives of HCPs. This is also the first to describe individual and family experiences in the Canadian residential care context. The findings from this study suggest that distress among residents with chronic critical illness was connected to the tension between medical care and the unmet need for a sense of home. This tension arose from care beyond the physical being overlooked, being dependent on others and also feeling neglected at times, frustration with limited choice and participation in decision making, and feeling sad and alone. The perspectives of HCPs in this study illuminate the difficulties they encountered in providing care to these unique, medically complex, and vulnerable residents within a specialized, publicly funded long-term care setting.
Physical and Psychological Symptom Burden
Based on prior research, we expected a poor prognosis and the high physical symptom burden to be a significant source of distress for the study participants with chronic critical illness. The uncertain and life-threatening nature of chronic critical illness is thought to elicit states of crisis for individuals and their family systems (Hickman & Douglas, 2010). In an American study by Nelson and colleagues (2004), individuals with chronic critical illness on a tertiary-care respiratory unit self-reported a high physical symptom burden; 40% reported pain at the highest levels, with the majority also reporting shortness of breath, lack of energy, insomnia, dry mouth, and nausea. Yet, prognosis and physical symptom distress were not prominent in the resident, family, or HCP commentaries in our research. Perhaps, if explicitly measured, these would have been highlighted. It is also possible that our sample represents a later stage in the chronic critical illness trajectory when physical symptoms were overshadowed by the more concerning psychological symptoms and challenges related to communication, daily living, and care.
Indeed, Nelson and colleagues (2004) also reported that more than 60% of chronically critically ill participants reported psychological symptoms at the highest levels, as well as feelings of worry, sadness, and nervousness. Ninety percent also reported severe distress due to difficulty communicating (Nelson et al., 2004). In their exploration of the experiences of individuals with chronic critical illness in a long-term acute care hospital and their surrogates, Lamas, Owens, Massaro, Pertsch, Gass, et al. (2017) described poor patient quality of life, noting difficulty communicating, boredom, and poor mobility. Our findings extend these earlier studies by describing in greater detail some of the factors that appear to underlie and exacerbate psychological distress. These were evident in the day-to-day struggles of individuals with chronic critical illness and included their complete dependence on others, limited freedom of choice, not feeling listened to, ongoing grief, inability to participate in meaningful activities, and social isolation. This is similar to the documented experiences of ventilator-dependent individuals, although not necessarily with chronic critical illness, who feel fear and frustration due to dependence on a ventilator, impaired verbal communication, loss of control over their life, and uncertainty and powerlessness in getting their needs met (Carroll, 2007; Tsay et al., 2013). There is sufficient evidence to support the implementation of processes of care that focus on timely, frequent, and empathic communication with individuals and family (Rose et al., 2019).
The incidence and prevalence of anxiety, depression, symptoms of post-traumatic stress disorder (PTSD), and complicated grief remain unknown among individuals with chronic critical illness. Although these psychological sequelae might never be fully understood among those with chronic critical illness and communication impairments, psychological challenges were clearly evident in the narrative accounts of our study participants. One German study did find that 17.6% (23 of 131) of individuals with chronic critical illness suffered from major depressive disorder up to 6 months following intensive care unit discharge (Wintermann et al., 2018). Variables that predicted depression included perceived helplessness, recalled experiences of a traumatic intensive care unit event, symptoms of actuated stress disorder, and the diagnosis of PTSD after intensive care (Wintermann et al., 2018). Therapeutic interventions to address the psychological symptoms experienced by individuals with chronic critical illness are yet to be developed and tested in this population but deserve future research attention. Our study suggests that strategies to enhance communication, elicit and incorporate individual choices in everyday activities, and exposure or participation in activities are important to residents. As our research was conducted in partnership with facility decision-makers who became aware of these resident needs during the study, steps already taken to incorporate meaningful activities into care, particularly recreational therapy, have been implemented with anecdotal reports of benefits to residents and staff. Indeed, the addition of recreation therapists has helped to reduce conflicts between residents and family, and HCPs. There is quite likely an important role for recreational therapists in considering ways of engaging individuals with impaired physical, cognitive, and communication function in meaningful activities.
Importance of Trust and Caring
The importance of trusting and caring relationships with HCPs has been articulated in studies of ventilator-dependent individuals, with HCP patience, empathy, and consistent and reliable care highlighted as key to quality care (King et al., 2019; Tsay et al., 2013). While individuals with chronic critical illness in our study received tremendous reassurance from the competent medical care they received, it was well recognized by residents, family, and some HCPs that trusting, caring relationships with staff were essential, although not always the reality or considered possible. The highly technological care was seen to be incompatible with the more humane, holistic, person-centered care desired by residents. By necessity, the staff prioritized the technological, task focussed care that sustained life and enabled them to attend to the basic medical needs of all residents, with the unintended consequence of crowding out other resident health priorities. In prior research with ventilator-dependent individuals, the ignorance and attitudes of uncaring HCPs created suffering, while deeply committed and competent carers helped to alleviate suffering (Lindahl et al., 2006). Of significance, without regulations, standards, processes, and professional and organizational support that allow for staff flexibility to attend to resident priorities and preferences, HCPs are put in an impossible situation.
Although our study population is somewhat unique, prior research investigating resident–provider relationships in long-term care is particularly relevant. Research suggests that the development of these relationships is crucial to resident thriving, quality of life, and well-being (Bergland & Kirkevold, 2005; Carpenter, 2002; Custers et al., 2012; McGilton et al., 2012), although what constitutes a positive or close relationship and how this is achieved varies. In a Canadian study, residents thought a close relationship included staff acting as their confidants, while family focused on actions staff took to convey a caring attitude and a genuine sense of concern (McGilton & Boscart, 2007). In contrast, HCPs considered close relationships to be primarily about feeling connected with the resident (McGilton & Boscart, 2007). In other research, residents have reported quality of care to include care-as-relating that emphasized the affective aspects of care, wherein care demonstrated friendship and allowed residents to show reciprocity with HCPs (Bowers et al., 2001). Factors found to be important in the development of close resident–HCP relationships relate to characteristics of the resident, such as cognitive status, ability to get along and converse with the provider, and understanding and appreciating that the HCP is doing their best (McGilton & Boscart, 2007; Roberts & Bowers, 2015). Characteristics of HCPs and the facility are also influential in building patient–provider relationships (McGilton & Boscart, 2007; Roberts & Bowers, 2015). Although much research shows the significance of trusting and caring relationships, an important finding that is relevant to those with chronic critical illness is that resident preferences concerning the intensity and role of staff in the relationship vary and ought to be discussed and considered in the provision of care (Custers et al., 2012).
Alternative Approaches to Care
Individuals with chronic critical illness represent a heterogeneous population whose challenges and associated care needs are not fully understood and for whom evidence-based models of care have not been fully developed (Rose et al., 2019). Despite the exploratory nature of our study, the findings suggest that alternative approaches be considered in the future delivery and design of health services for those with chronic critical illness. The Timing It Right framework has been used to conceptualize the four key elements of social support (emotional, instrumental, informational, and appraisal support) across the critical illness survivor care continuum, from the time of intensive care unit admission throughout discharge home or to the community (Czerwonka et al., 2015; King et al., 2019). Although arguably those who progress to chronic critical illness have increasingly divergent support needs than those expected to recover, which require articulation in future research, a method, tool, or questionnaire to identify and document the residents’ greatest needs could help target and ensure consistency in care. Moreover, providing realistic upstream information about the experience of chronic critical illness might enable residents and families to make more informed choices about their care and to communicate their priorities and wishes for the future.
As suggested by others (Lamas et al., 2017), a palliative approach to care would likely be beneficial for individuals with chronic critical illness. This approach emphasizes patient- and family-centered care that focuses on the person and not just the disease, where quality of life is the primary goal (Sawatzky et al., 2016). This approach draws attention to the importance of therapeutic relationships with HCPs, with essential characteristics being (a) the adoption of foundational principles of palliative care and adaptation of palliative care knowledge and expertise to individuals, (b) an upstream orientation that ensures individual and family needs are addressed early and throughout the illness trajectory, and (c) integration and contextualization of this approach across health care systems (Sawatzky et al., 2016). However, there is also emerging evidence that the implementation of a palliative approach might require specific strategies to empower HCPs, primarily nurses at the everyday point of care, as well as practice supports such as educational initiatives (Sawatzky et al., 2017). Sawatzky and colleagues (2017) further suggest that guidelines and pathways for care, as well as means of tailoring the approach to the specific setting and population might be necessary. Arguably, future research into how a palliative approach could be tailored to the unique and complex care of individuals with chronic critical illness is warranted.
Limitations
The findings of this small exploratory research must be considered in the context of the study limitations. Study participants were from one Canadian facility designed to provide specialized ventilator care and we do not claim that our results are generalizable to other care contexts. Moreover, resident participants were cognitively intact, English speaking, and ventilator dependent and able to communicate verbally, by mouthing words, or through the use of adaptive technology. Although we also included family members of residents with chronic critical illness who were unable to participate, these were still proxy accounts and family interpretations might not always align with residents themselves. The HCPs only included staff who were willing to participate and thus might not represent the full spectrum of perspectives. Rather than be generalizable, our findings provide insights that might be relevant to other care environments, other individuals with chronic critical illness, and other HCPs caring for the chronically critically ill. It must also be noted that our study might not have represented the full diversity of experiences of individuals with chronic critical illness, including those expecting to transition home. Instead, our study was bolstered by the depth of information, or information power, garnered through in-depth interviews and interpretation that incorporated clinical expertise (Thorne, 2016).
Conclusion
This study highlights sources of distress for ventilator-dependent individuals in residential care with chronic critical illness that enables a more comprehensive understanding of their challenges, particularly in everyday life, as well as the struggles staff encounter in attempting to meet their complex needs. Although there has been much progress, identifying and implementing strategies to prevent evolution toward chronic critical illness, interventions, and approaches to care that address the unique needs of this population are urgently needed. Future exploratory research across multiple care settings with various models of care and geographic diversity are required to further characterize the experiences of those with chronic critical illness. Further work to develop therapeutic interventions to address psychological challenges and improve relationships with HCPs is also required. Explicit attention to social support needs throughout the illness trajectory and a palliative approach to care appear particularly relevant.
Supplemental Material
sj-pdf-1-qhr-10.1177_1049732320976373 – Supplemental material for Sources of Distress for Residents With Chronic Critical Illness and Ventilator Dependence in Long-Term Care
Supplemental material, sj-pdf-1-qhr-10.1177_1049732320976373 for Sources of Distress for Residents With Chronic Critical Illness and Ventilator Dependence in Long-Term Care by A. Fuchsia Howard, Sarah Crowe, Laura Choroszewski, Joe Kovatch, Adrianne J. Haynes, Joan Ford, Scott Beck and Gregory J. Haljan in Qualitative Health Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Michael Smith Foundation for Health Research.
Data Availability
The data that support the findings of this study are not available on request from the corresponding author nor are they publicly available because they contain information that could compromise the privacy of research participants.
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.