
Abstract
Care provided by family is the backbone of palliative care in Canada. The critical roles performed by caregivers can at the same time be intensely meaningful and intensely stressful. However, experiences of caregiving can be enhanced when caregivers feel they are making informed and reflective decisions about the options available to them. With this in mind, the purpose of this five-phase research project was to create a Family Caregiver Decision Guide (FCDG). The Guide entails four steps: thinking about the current caregiving situation, imagining how the caregiving situation may change, exploring available options, and considering best options if caregiving needs change. The FCDG was based on available evidence and was developed and refined using focus groups, cognitive interviewing, and a feasibility and acceptability study. Finally, an interactive version of the Guide was created for online use (https://www.caregiverdecisionguide.ca). In this article, we describe the development, evaluation, and utility of the FCDG.
Keywords
Introduction
Globally, people are both aging and living longer with multiple chronic illnesses (Leeson, 2014). Indeed, the number of Canadian seniors above the age of 65 is projected to more than double between 2005 and 2036, placing increasing and unsustainable demands on the health care system (Fowler & Hammer, 2013). Despite the fact that the majority of Canadians die in hospital (Statistics Canada, 2012), most prefer to live at home for as long as possible, which, for many, means dying at home (Stajduhar & Davies, 2005; Wilson, Cohen, Deliens, Hewitt, & Houttekier, 2013). The preference to die at home has also been found in studies conducted in the United States (National Academies of Sciences, Engineering, and Medicine, 2016), England and Wales (Leeson, 2014), Europe (Higginson et al., 2014), and Japan (Fukui, Yoshiuchi, Sawai, & Watanabe, 2011). Regardless of the place of death, the demand for families to provide care at home is increasing. For example, almost three million Canadians aged 45 years and older provide 80% of care for family members with chronic and life-limiting illnesses (Statistics Canada, 2013a, 2013b). One in four Canadians are caregivers and half of them are aged between 45 and 65 years, their peak earning years (Statistics Canada, 2013a, 2013b). This means that more than six million carers are juggling their work and labor-intensive caregiving responsibilities (Statistics Canada, 2013a, 2013b). Caring for an ill spouse requires about 14 hours per week, roughly equivalent to a part-time job (Funk et al., 2010). While caregiving can be rewarding, it is also stressful and can be associated with negative psychological, social, spiritual, and physical consequences (Funk et al., 2010; Topf, Robinson, & Bottorff, 2013). There are also financial implications to caregiving based on reports that caregivers have significant out-of-pocket expenditures (Keating, Fast, Lero, Lucas, & Eales, 2014; Round, Jones, & Morris, 2015; Rowland, Hanratty, Pilling, van den Berg, & Grande, 2017).
The caregiving role becomes even more critical in the advanced and end-of-life phases of illness. Estimates suggest that family caregivers are responsible for 75% to 90% of hospice palliative care provided in the home (Dunbrack, 2005). On average, Canadian family caregivers allocate approximately 54 hours per week to the care of a dying loved one at home (Canadian Hospice Palliative Care Association, 2012). The results of a recent national survey in England indicate that caregiving increases significantly in the last 3 months of life with the median hours of care reaching nearly 70 hours/week for over 50% of family caregivers (Rowland et al., 2017). Responsibilities often include shopping, housekeeping, coordinating, and accompanying their ill family member to medical appointments in addition to attending to their family member’s physical, psychosocial, and spiritual care needs. These additional responsibilities can have immense impacts on family caregivers’ daily lives and put them at risk of compromised quality of life and physical and mental morbidities (Grov, Dahl, Moum, & Fossa, 2005; Williams & McCorkle, 2011). Taking on the role of caregiver is often automatic and unreflected, something that Erlingsson, Magnusson, and Hanson (2012) term “sliding sideways into caregiving.” Caregivers are challenged by lack of preparation, lack of information about what to expect, and inadequate support (Grande et al., 2009; Mastel-Smith & Stanley-Hermanns, 2012; Robinson, Pesut, & Bottorff, 2012). The experience of providing care to an ill family member is well understood, but how to effectively support family caregivers is not (Grande et al., 2009). There is a critical need to develop interventions that enable family caregivers to provide the kind and level of care they are committed to providing, and that the health care system depends upon.
The need to develop interventions to support the valuable work that family caregivers do led to the development of the Family Caregiver Decision Guide (FCDG), a resource designed to help family caregivers make decisions common to their caregiving role. The Guide was developed based upon several studies (Robinson et al., 2012; Topf et al., 2013) where we found family caregivers’ need to provide excellent care was compromised by lack of knowledge about what they were getting into, lack of preparation for the role, lack of understanding about what to expect in terms of illness progression and at end of life, and difficulty accessing professional support as well as critical resources in a timely fashion. These findings are supported by others (Flemming, Atkin, Ward, & Watt, 2019; Oechsle, 2019; Wang, Molassiotis, Chung, & Tan, 2018). In particular, we observed that family caregivers had difficulty identifying the caregiving decisions they had made or needed to make and how to go about making those decisions. Furthermore, although decision aids have been identified as helpful resources, there was no decision aid available to assist them. Therefore, the purpose of this study was to develop and evaluate an intervention to support family caregiver decision making.
Method and Findings
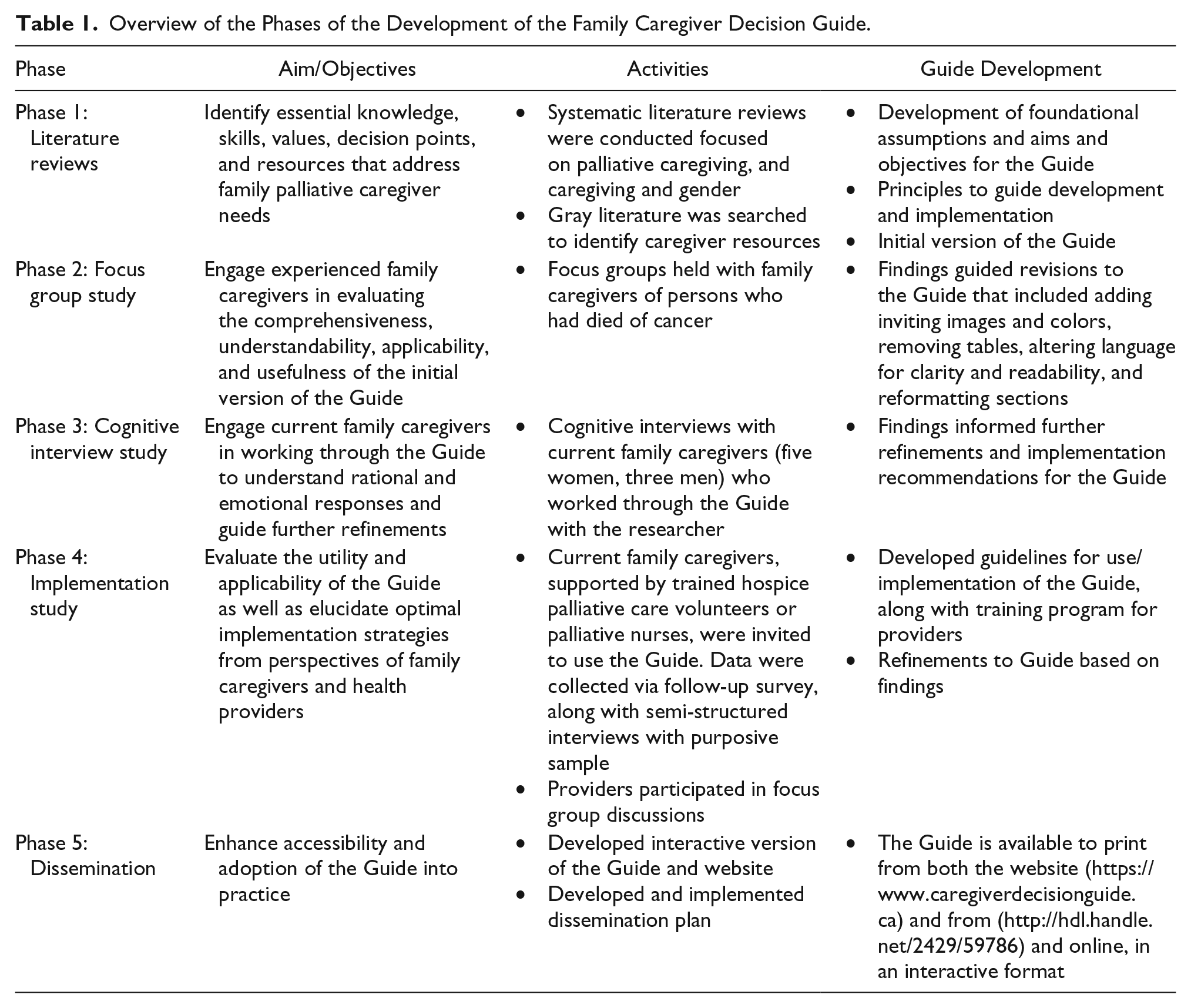
This multiphased study began with a literature review (Phase 1) and was followed by three phases of qualitative research conducted using a sequential multiple method design (Mafuba & Gates, 2012; Morse, 2003). The iterative, user-centered design process involved intended users to create an accessible and effective intervention to support family caregivers (see Table 1). Phases 2 to 4 received ethical approval from the university research ethics board and relevant health care agencies. All participants (caregiver and navigator) provided written consent to participate in the study. Phase 5 focused on development of strategies to support dissemination and uptake of the intervention.
Overview of the Phases of the Development of the Family Caregiver Decision Guide.
Given the wide range of caregiver relationships, we defined family caregiver as whomever provided, or was providing, the majority of unpaid care at home. Family is whoever the ill person identifies as family. This included wives, husbands, partners, mothers, fathers, daughters, sons, and close friends. Support for family caregiver decision making was conceptualized as a palliative intervention. This was based on defining palliative care as focused on quality of life rather than disease that begins with the diagnosis of serious chronic or life-limiting illness and extends across the illness trajectory to end of life.
Phase 1: Development of the FCDG Based on Available Evidence
Phase 1 involved a review of literature, the subsequent identification of foundational assumptions, aims and objectives for the resource, as well as principles to guide development and, finally, initial development of the resource. The review of the evidence focused on three main bodies of literature: palliative caregiving, caregiving and gender, and caregiver resources. In each search, the overall aim was to identify literature that distinguished the essential knowledge, skills, values, decision points, and resources that address family palliative caregiver needs.
The search of empirical palliative caregiving was based on a rapid review strategy (Khangura, Konnyu, Cushman, Grimshaw, & Moher, 2012), prioritizing evidence from quality systematic reviews, and, when relevant, including high-quality primary studies and landmark and/or oft-cited studies. Our search yielded 24 articles that comprised literature reviews (12) and research studies (10 qualitative and two quantitative). Data were extracted in relation to method/sample, major findings, themes, and implications for development of the intervention. Major themes included caregiver decision making, challenges, needs, positive experiences, rural caregiving, and interventions.
Our second search of empirical literature focused on gender and caregiving for the purpose of informing a gender sensitive approach. Twenty-six articles were reviewed and included literature reviews (four) and research studies (18 quantitative, three qualitative, and one mixed method). Data were extracted in relation to women and caregiving, men and caregiving, and implications for development of the intervention. Major findings were summarized within each of those categories (Robinson, Bottorff, Pesut, Oliffe, & Tomlinson, 2014).
Finally, we searched the gray literature for caregiver resources (11) to explore current practices in supporting family caregivers with the aim of identifying best practices, key knowledge and skills being targeted, how the support was being offered, and existing decision aids/supports. Data were extracted in relation to aim of the resource, key components, limitations/concerns, and implications for development of the new resource.
Subsequent to our synthesis of findings, we developed the underpinnings of the FCDG, which included assumptions, aims, objectives, and principles (Table 2) as well as content for inclusion.
Underpinnings of the Family Caregiver Decision Guide.
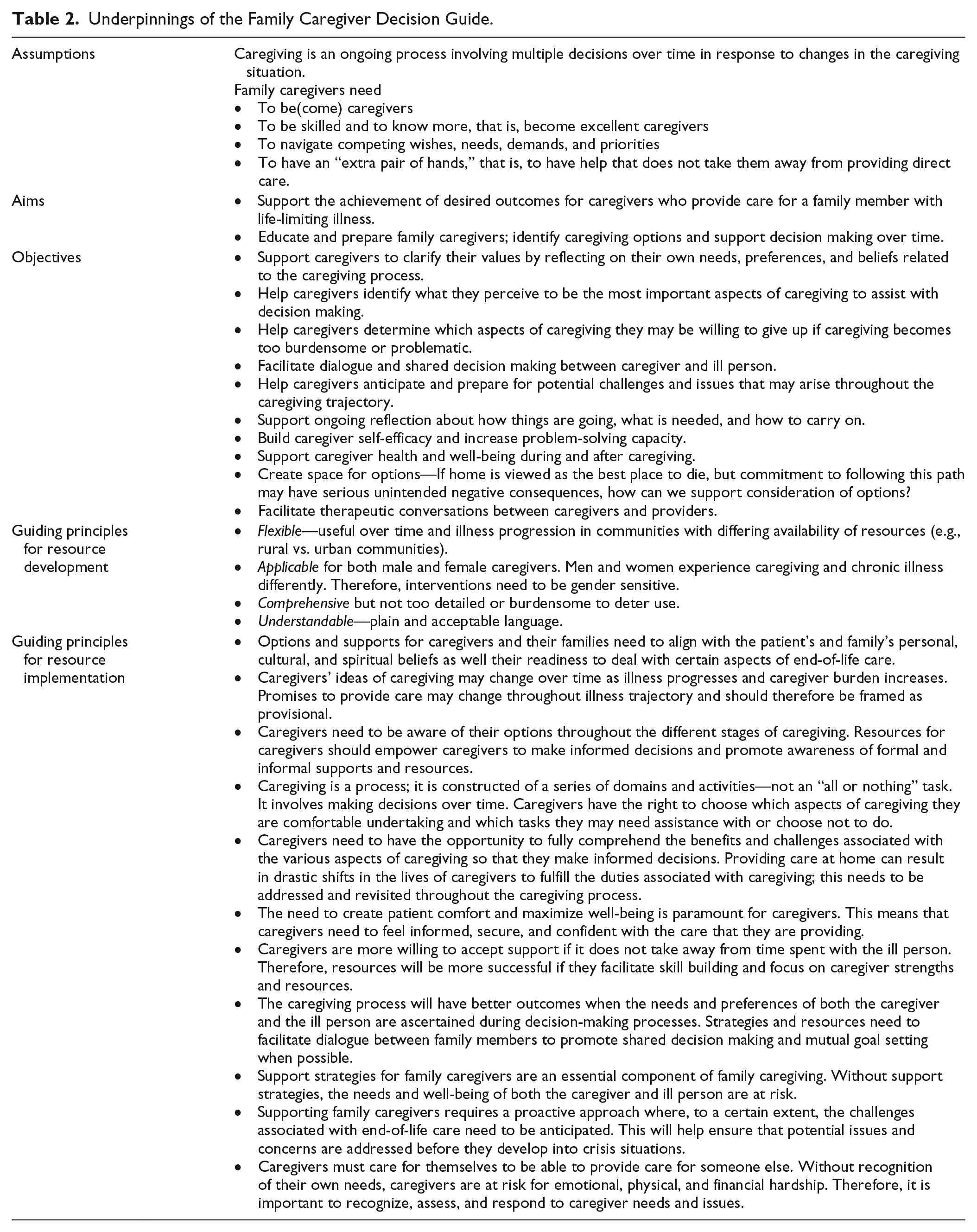
In addition, we took our knowledge of family caregiving acquired from previous studies as well as clinical work into account in development. Despite conceptualizing the resource as a palliative intervention, we were aware of the problematic association of the word “palliative” with death and dying, and the constraints this places on decision making. For example, palliative care is often resisted because of the belief that it is a lesser kind of care offered when there is no hope. Yet the evidence supports that early receipt of palliative care enhances quality of life and may even extend life (Temel et al., 2017; Temel et al., 2010). This led the team to purposely avoid using the word “palliative” in naming and describing the intervention. Instead the term “life-limiting illness” was used, which we anticipated would make the intervention more acceptable, especially prior to the advanced phase of illness and caregiving.
We also recognized the significant challenges to effectively supporting family caregivers, which became apparent in our previous research (Lockie, Bottorff, Robinson, & Pesut, 2010; Pesut, Robinson, & Bottorff, 2013; Robinson, Bottorff, McFee, Bissell, & Fyles, 2017; Robinson et al., 2012; Topf et al., 2013). Family caregivers often prioritized the needs and wishes of the ill person over all other issues, including their own health, preferences, and, at times, safety. For example, a caregiver explained that her husband only wanted to receive care from her but as he was prone to falling, she risked her own physical health in her attempts to get him off the floor. She recounted that she honored his wish until it simply became too dangerous for her to continue. The priority focus on meeting the ill person’s needs, wishes, and preferences, coupled with recognition of limited paid health care provider time, often led to caregiver reluctance to engage health care professionals’ focus and time for their own needs. This was viewed as diverting a precious resource away from the person who needed it most. Furthermore, caregivers reported that they withheld information from health care providers about struggling to provide care for fear of negative judgments about their abilities. They worried that care would be taken from them. Another reported challenge was the professional practice of noting concern for the caregiver but then giving them another job, to take care of their own health and well-being in addition to providing care for the ill person. Although family caregivers often recounted appreciation for expressions of concern, the recommendation of a new job was viewed as nonsupportive and evidence of lack of understanding of the demands of caregiving. The common coping strategy among caregivers of “taking one day at a time,” which prevented being overwhelmed with what might be ahead, also acted to constrain necessary planning and preparing for likely changes. Finally, we were aware of the severe constraint to decision making that occurred when caregivers made an implicit or explicit promise to care at home until death because options were not considered. When a home death did not occur, these caregivers suffered greatly because of the “broken promise” (Martz & Morse, 2017; Topf et al., 2013). All of these constraints challenge our ability to effectively support family caregivers and were addressed in the development phase.
The final factor that influenced development was the unique nature of the decisions that attend family caregiving. Most decision aids are created to facilitate decisions that result in simple yes/no outcomes that are bounded by time. For example, the decision to take a particular cancer treatment at a particular time of diagnosis might be one suitable for a decision aid. However, caregiving decisions are different; the caregiving process changes over time and involves multiple decision points that coincide with changes in the caregiving situation that are ill person, caregiver, or health system related. This necessitated adaptation of the internationally recognized process for decision aid development (Coulter et al., 2013) while following accepted international standards (Elwyn et al., 2006) for decision support tools.
Taking account of these various factors, we developed the first prototype of the FCDG. The FCDG is organized around a four-step process: thinking about the current caregiving situation, thinking about how the caregiving situation may change (this section includes values clarification for both caregiver and care recipient), exploring caregiving options in the area, and best options if the needs for caregiving change. Multiple iterations of the FCDG were reviewed by team members with expertise in palliative research and palliative clinical work until we had a stable version to begin testing. Three phases of testing were conducted following approval by a university ethics committee.
Phase 2: Focus Group Study to Evaluate the First Prototype of the FCDG
In Phase 2, past family caregivers of persons who had died of cancer participated in focus groups designed to evaluate the first prototype’s comprehensiveness, understandability, applicability, and usefulness. We recruited family caregivers who were well into the bereavement period (minimum 6 months postdeath) because we felt they were experienced enough to critique the FCDG and were far enough into the bereavement period that the experience would not exacerbate their grief or be overly burdensome. Eleven women and three men provided informed consent and participated in three focus groups, which were audio-recorded but not transcribed verbatim. Individual participants worked through the FCDG and then engaged in group conversation about their experience prompted by questions about what they liked, did not like, structure and flow of the FCDG, areas lacking clarity, whether their experiences as caregivers were captured, and their assessment of the potential usefulness of the FCDG. Audiotapes were reviewed and detailed handwritten notes were recorded to capture important points made about each section of the FCDG, paying close attention to diverse views, areas of consensus, and suggestions for improvement. Notes were later transcribed, reviewed by the team, and areas for refinement were specifically identified and determined by consensus (Zerr, 2015).
Participants told us that despite containing useful information, they did not think they would access the FCDG based on its appearance. There were too many tables and little aesthetic appeal. This was new learning in relation to the accepted process for decision aid development, which did not prompt us to consider aesthetics. Participants identified many language issues that were either confusing or unacceptable. Furthermore, they requested that the FCDG be more explicit about end-of-life issues including use of the word “palliative” rather than “life-limiting illness” on the cover page. This particular recommendation was not immediately taken up because we were concerned that these participants’ perspective, based on having experienced the death of their ill person, might not be shared by caregivers who were earlier in the caregiving trajectory.
Participants were concerned when the focus of the FCDG was on the family caregiver, specifically their self-care, instead of the ill family member. This de-emphasis of their ill family member, and subsequent emphasis on caregivers’ responsibilities for their own health, disrupted what they described as their connection to the FCDG, which in turn compromised the effectiveness of the intervention. Finally, it was noted that the FCDG was useful in raising many relevant questions but held few answers and participants requested more resources to address those questions. The FCDG was redesigned to include inviting images and colors, tables were removed, language was altered for clarity and readability, sections were reformatted, and resources were added.
Phase 3: Cognitive Interview Study to Evaluate the Second Prototype of the FCDG
This phase involved testing the second prototype of the FCDG with eight current family caregivers (five women and three men) for someone with advanced cancer, using cognitive interviewing (Zerr, 2015). Following informed consent, participants worked through the FCDG alongside a researcher with a focus on understanding rational and emotional responses to the resource. The aim was to further refine the acceptability, understandability, and applicability of the FCDG. We found that the Phase 2 redesign of the FCDG was largely successful. Overall, participants found that the images created a warm, caring, and personal feel to the FCDG. Two images were described as unhelpful (e.g., one showing a man who looked sad) and were subsequently replaced. Lack of ethnic diversity in the images was noted by the caregiver participants. It became clear during our interviews that participants personally and emotionally connected to the FCDG via images that represented them or their situation, which led the team to include more diverse pictures.
Language was viewed by the caregiver participants as understandable and applicable, except in a few instances. When the language did not fit, this caused participants to disconnect from the FCDG, with the thought that the writer of the FCDG clearly did not understand their situation. One example of this was the question of how caregivers were managing with “exercising and staying active.” Similar to the findings in Phase 2 focus groups, participants found the idea of exercising (self-care) made no sense in their demanding circumstances, so this was removed. Two further significant changes involved using first person rather than second person throughout the FCDG (e.g., this Decision Guide is for me rather than you) and to remove the term “loved one” for the recipient of care and replace it with the more neutral term “family member.” We learned in the previous research (Robinson et al., 2017) that love is only one of many motivations behind family caregiving. Furthermore, in contrast to the feedback we got from Phase 2 focus groups with family caregivers in the bereavement period, these participants were not supportive of more explicit language regarding palliation, disease progression, and death and dying because they found it to be too aggressive and upsetting. Finally, participants pointed out that the FCDG was missing a critical piece of caregiving—exhaustion, as one reason why caregiving at home might be curtailed. The FCDG was further refined based on participant feedback. Despite the identified concerns, the overall content of the FCDG was reported to be useful in that it invited reflection and supported planning as well as providing a “map” for essential conversations with the ill family member, which caregivers had not initiated. The FCDG prototype was then professionally redesigned to further enhance its aesthetic appeal and usability.
We concluded that the FCDG showed promise as an effective intervention but that it raised many questions for caregivers and offered very few answers. In addition, caregivers were not likely to seek answers because of fatigue, life demands, or unwillingness to draw attention to themselves. Therefore, we concluded that the FCDG should not be used as a stand-alone tool; instead, it was essential to accompany it with navigational support, particularly in relation to available resources.
Phase 4: Implementation Study of the Revised FCDG
Phase 4 was an implementation study designed to further evaluate the feasibility, utility, and applicability of the revised FCDG in real-world situations and in a broader illness context. In particular, we wanted to determine how navigational support might enhance the utility of the FCDG for family caregivers of someone with serious illness (not limited to cancer and including dementia), as well as identify optimal implementation strategies. The FCDG was evaluated with current family caregivers in a rural setting, who were receiving home care services (20 caregivers), using specially trained hospice palliative care volunteers as navigators and in an urban setting (12 caregivers) using palliative nurses as navigators. An implementation science approach informed by action research was used. The implementation process, including the education (~2 hours) of involved navigators that aimed to build local capacity, was developed and tailored to each setting in consultation with our community-based partners. Both the planning phase of the implementation process and the post-implementation evaluation phase included engagement with local opinion leaders.
After providing informed consent, caregiver participants were introduced to the FCDG by their navigator who then negotiated how the FCDG would be used and how support would be offered based on caregiver preferences. For example, some caregivers wished to work completely through the FCDG on their own and then discuss their thoughts and questions with their navigator. Other caregivers preferred to work through a section at a time with their navigator alongside. All volunteer navigators made at least two in-person visits to the family caregiver and many supplemented these visits with telephone conversations. Nurse navigators made regular, scheduled home visits as part of their care of the ill person.
Data from caregiver participants were collected following completion of the FCDG. Caregivers completed a brief survey focused on the acceptability and usefulness of the FCDG as well as key implementation questions such as when the FCDG should be introduced. Individual, semi-structured interviews were also conducted with four purposively selected key family caregiver informants. Questions explored such things as whether the FCDG was useful and, if so, how; optimal timing for introducing the Guide; most effective process for using the Guide; and perceived outcomes including communication with providers, effectiveness of support, and caregiver well-being. The interviews were audio-recorded, transcribed verbatim, and analyzed using constant comparison.
In addition, appropriateness and utility of the FCDG as well as the implementation process were evaluated from the navigator perspective via focus groups, which were conducted at mid- and end-of-study. The mid-study focus groups were designed to facilitate implementation successes and ameliorate challenges. Topics addressed in the end-of-study focus group included implementation successes and challenges, the FCDG’s usefulness in enhancing communication as well as the understanding of family caregiver values and needs, navigators’ perceived ability to provide effective support, and exploration of the navigator’s role. The focus group discussions were audio-recorded and analyzed thematically.
There was overwhelming consensus among the Phase 4 participants (caregivers and navigators) that the FCDG was feasible, useful, understandable, and comprehensive. Navigators commented that it helped educate and raise awareness for caregivers. They noted that caregivers were grateful for the recognition of their work, concerns, experiences, and burnout—they felt “not so alone.” Some suggestions for additional content were made (e.g., related to financial planning) and the FCDG was modified as appropriate.
All participants stated that the FCDG should be used with support from a trusted, knowledgeable health care provider/navigator. Participants identified many ways that the FCDG could be approached, for example, working through it step by step with a provider, working through all steps independently and then discussing with a provider, or working through a step at a time followed by subsequent discussion with a provider. The majority of participants thought that the FCDG should be introduced as early as possible in the illness experience and used repeatedly as things change. Caregiver participants frequently commented that the FCDG came too late for optimum utility and suggested that family physicians make the initial introduction. Volunteer navigators found the experience rewarding and commented that the FCDG gave their interactions and conversations focus and direction. They got to know their caregiver partners in a deep and meaningful way.
The caregiver participants received the FCDG when they were deep into the illness trajectory, yet even then, they reported the resource to be useful. For example, they found the FCDG to be affirming because it “let’s you know how much you know” and have done. As one woman said, “I know a lot more than I thought I did.” Navigators commented that this gave caregivers comfort. Furthermore, the FCDG solidified previous decisions. “You can see more clearly how you made decisions, and can talk about them more clearly.” Working through the FCDG validated and clarified the path caregivers were on. Even for these experienced caregivers, the FCDG was effective in raising questions such as “Do I know enough about this?”
Implementation advice was specific and helpful. For example, volunteer navigators recommended introducing the FCDG by first recognizing and acknowledging the importance of caregivers’ work and stating that the goal of the FCDG is to support family caregivers in their caregiving and in living life to the fullest by helping them get what they need in their unique situation. Commendations for the caregiver, especially in front of the ill person, were viewed as extremely supportive and it was recommended that providers look for ways to specifically commend the caregiver during the implementation process of the FCDG.
Navigators offered several important tips. Volunteer navigators emphasized that follow-up with caregivers needs to be initiated by the navigator because of caregivers’ reluctance to draw attention to themselves and away from their ill family member. They were particularly effective in this regard. Nurse navigators acknowledged this need but identified how difficult this was for them with their busy schedules. Sometimes family caregivers were exhausted and did not have the energy to make necessary connections or seek required supports (e.g., equipment), so providing information was not viewed as adequate or effective; volunteer navigators often offered to do the work. They noted that simply expecting caregivers to act on new or existing knowledge was unrealistic in the circumstance of exhaustion. In addition, the idea that the FCDG is meant to be revisited over time as things change was confusing to some caregivers. Navigators suggested using different colors for each time the FCDG was completed. They also suggested comparing it with a Will, which people revisit as there are new additions to the family. Most important for the navigators was knowledge about resources that caregivers could reliably access when needed and an appreciation of how the caregiver was faring emotionally.
Phase 5: Dissemination
Phase 5 focused on final refinements to the FCDG, development of an interactive version of the resource for online use, and the creation of a website to enhance accessibility and adoption of the resource into practice (https://www.caregiverdecisionguide.ca). The FCDG may now be used in two formats. Online, caregivers can work through each step in their own time and save as they go to return at a later date, or complete in one sitting. When the FCDG is completed, it can be printed and includes both questions and responses, which can then be used to focus conversations with a trusted health provider. The FCDG is also available to print from both the website and from “http://hdl.handle.net/2429/59786” for people who prefer to work offline or who may not have computer access. It is an open access resource that can be printed by health care providers for caregivers. The FCDG has been successfully implemented in 2-hour, urban and rural community workshops with groups of over 30 people including those with serious illness, current caregivers, and those anticipating becoming caregivers. One key to the success of the community-based workshops was including local health care providers knowledgeable about available resources. In addition, the print version of the FCDG has been translated into Portuguese by the Portuguese Palliative Care Association and made available throughout the country.
Limitations
During the study period, palliative nurse navigators’ caseloads increased significantly, accompanied by a dramatic decrease in patient time on program (less than 6 weeks, which was the duration of study participation). This means that people were accessing palliative care closer to death than had been previously experienced and overall workload intensity increased because patients were sicker. More than half our recruited urban caregivers did not complete the study because their ill person died shortly after the FCDG was introduced. Our belief that optimal implementation of the FCDG should be early rather than late in the serious illness experience was confirmed. The FCDG may assist in preparing caregivers for decisions at end of life, but when introduced for the first time in this phase of the trajectory it was not a useful resource because caregiving was too intense and there were such rapid changes in the ill person’s condition. Furthermore, the nurse navigators had difficulty integrating follow-up with caregivers into their home visits due to the intensity of care for the ill person.
Discussion
The sequential multiple methods study reported here was designed to address the pressing need for interventions to support family members caring for seriously ill people at home. Family was conceptualized as whoever the ill person accepts as family. Following international standards and user-centered, iterative approaches for the development of decision aids, the FCDG was created and subsequently refined. To our knowledge, this is the first intervention for family caregivers that focuses on supporting their decision making in planning care for their family member. The multiphased approach proved valuable in translating evidence into the development of a novel intervention through the engagement of intended users (in this case both caregivers and providers). We were particularly sensitive to the possibility of added burden for caregivers at a time when vulnerabilities may be high and multiple complex issues at play; however, the process proved feasible. The results of each phase determined the focus and methods associated with the next phase. This approach allowed us to make important iterative adjustments and refinements to the intervention as well as implementation guidelines for the FCDG to maximize acceptability and utility. Whereas initial phases focused on caregivers for someone with cancer, the implementation phase expanded to a wide variety of life-limiting illnesses and proved applicable.
The inclusion of family caregivers and providers in the development of interventions has been recognized as important in supporting implementation into practice (Ugalde et al., 2019). Although caregiver interventions have received increasing research attention and randomized control trials report improved outcomes for family caregivers (Ferrell & Wittenberg, 2017), there has been limited focus on the potential for moving interventions into real-world settings. In a systematic review of cancer caregiver interventions conducted by Ugalde et al. (2019), fewer than half of the studies reported on the acceptability of interventions from the caregivers’ perspectives, and only two studies involved caregivers in the development of interventions. The sequential multiple method approach we used in this study provides a model for including family caregivers and providers in the development and use of evidence-informed interventions to support implementation into practice. Others have also suggested that sequential multiple methods designs are more likely to produce valid and reliable knowledge than a single method (Mafuba & Gates, 2012).
Decision aids have been developed to assist people when making difficult choices that require balancing risks and benefits in the light of personal values (O’Connor et al., 1999). Providing care at home for someone with serious illness involves many value-sensitive decisions, particularly when time may be short, which have potential for negative long-term consequences (Topf et al., 2013). These decisions are complicated when caregivers are not aware of their choices or decision making (Robinson et al., 2012). Decision aids aim to address factors associated with suboptimal decision making, such as lack of knowledge, unrealistic expectations, lack of clarity about personal values, unwanted pressure, and inadequate support (Coulter et al., 2013; O’Connor et al., 1999). They are not meant to be used alone, but as part of a process that involves conversation with a knowledgeable health care provider where the discussion can be focused on what is most important to the caregiver (O’Connor et al., 1999). According to our family caregiver participants, the FCDG effectively met the aims of decision aids. Across all the study phases, we consistently found that the FCDG was not sufficient to meet caregivers’ needs on its own. Discussion with providers was required to address gaps in knowledge (e.g., about the anticipated course of illness or about resources) and support as well as unrealistic expectations regarding outcomes. The FCDG has potential to enable focused discussions between caregivers and providers so that priority needs can be identified and the response tailored to the uniqueness of each situation to be most helpful. Given the realities of our cost and time constrained health care environment, the FCDG shows promise in enabling providers to maximize the effectiveness of communication with caregivers.
Rabow, Hauser, and Adams (2004) emphasize the importance of a care partnership between physicians and caregivers that rests on excellent communication, including careful assessment of caregiver beliefs, values, and preferences as well as proactive information to support decision making. Yet caregivers often experience the opposite of partnership—being powerless, invisible, and unsupported (Erlingsson et al., 2012). The FCDG is a time-efficient tool to support the creation of a care partnership where caregivers have an active voice because they can complete it at home and at their own pace or in a group setting. Care preferences may change over time as the illness changes, which supports the idea that communication should begin early in the illness trajectory and be revisited over time. Caregivers often do not know what they don’t know (Rabow et al., 2004; Robinson et al., 2012) and the FCDG was effective in raising caregivers’ questions and concerns. Caregiving circumstances are diverse, which calls for diverse interventions (Chi & Demiris, 2015) to enact truly family centered care through caregiver-centered support (LaValley, 2018). Our web-based interactive version of the FCDG addresses this issue.
Implications for Practice
Study findings indicate that the FCDG should be introduced to family caregivers along with assurances about their valued and essential work. These assurances are particularly important in situations where caregivers are reluctant to divert provider attention from their ill person to themselves. Caregivers can be invited to go through the FCDG at home, with a follow-up visit scheduled by the provider to review and identify needs. Once the FCDG is completed, needs, questions, and concerns can be addressed in relation to their priority to caregiving. The FCDG needs to be introduced early in the caregiving trajectory and revisited at key transitions, such as illness progression, hospitalization, and functional decline. The use of trained volunteer navigators was highly effective, with provider backup and support to address illness-related questions and problems (e.g., pain and symptom management). This makes the FCDG a potentially valuable intervention in settings where the availability of trained palliative care professionals is limited and a strong community-based volunteer system is in place (e.g., in rural settings). Furthermore, the FCDG was applicable to a variety of life-limiting illnesses.
Conclusion
Family caregivers are the backbone of life-limiting illness care. While there is growing recognition of the importance of their work, care for the caregiver remains sadly lacking. The FCDG is a promising intervention designed to assist caregivers to identify their needs, think ahead, and make informed decisions through focused conversations with supportive health care providers.
Supplemental Material
caregiver-guide-nov2018-web – Supplemental material for Development and Implementation of the Family Caregiver Decision Guide
Supplemental material, caregiver-guide-nov2018-web for Development and Implementation of the Family Caregiver Decision Guide by Carole A. Robinson, Joan L. Bottorff, Barbara Pesut and Janelle Zerr in Qualitative Health Research
Footnotes
Acknowledgements
We would like to thank Jamie Tomlinson, Natalia Polchenko, Laura Bissell, Erin McFee, Dr. Elizabeth Andersen, and Dr. Gayl Sarbit for their research assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the University of British Columbia (UBC) Institute for Healthy Living and Chronic Disease Prevention in partnership with Interior Health, The British Columbia Cancer Foundation, and The Peter Wall Institute for Advanced Studies.
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.