
Abstract
Although factors associated with HIV/sexually transmitted infection (STI) testing among gay, bisexual, and queer (GBQ) men are well-established in the literature, few studies have attempted to delineate the processes underlying different patterns of testing. We conducted a qualitative study involving 35 semistructured interviews with a purposive sample of GBQ men in Singapore from October 2017 to July 2018. Topics explored included formative sexual experiences, relationships, and experiences of HIV/STI testing. Interviews were audio-recorded, transcribed, coded, and analyzed through inductive thematic analysis. A typology comprising four distinct HIV/STI testing patterns was identified from the data, categorized based on the regularity of testing, relative to internal or external factors that motivate testing behaviors. These include triggered episodic testing, influenced episodic testing, institutionalized regular testing, and value-based regular testing. The typology highlights the preconditions that underlie different testing patterns and provides a framework for developing interventions that promote HIV/STI testing among GBQ men.
Keywords
Introduction
Gay, bisexual, and queer (GBQ) men are disproportionately affected by HIV and other sexually transmitted infections (STI), relative to the general population. However, studies across different settings have consistently found varying proportions of GBQ men who reported no prior testing experiences for HIV (Berg, 2013; Brito et al., 2015; den Daas, Doppen, Schmidt, & Op de Coul, 2016; Li et al., 2016). Early diagnosis and initiation of antiretroviral therapy among HIV-positive individuals have shown to improve one’s life expectancy and delay the onset of any serious AIDS-related events (Insight Start Study Group et al., 2015; Nakagawa et al., 2012). Furthermore, with the advent of novel, effective biomedical technologies and prevention strategies including HIV pre-exposure prophylaxis (PrEP) and treatment as prevention (TasP), early knowledge of one’s own HIV status may consequently have an impact on primary prevention efforts in the context of HIV as well (Cohen et al., 2011; Cohen et al., 2016; Grant et al., 2010).
Factors that are correlated with HIV testing among GBQ men have been established through several large quantitative epidemiological studies. Individual factors such as increasing age, educational attainment, and indicators of risk behaviors, such as a history of STI and increasing number of sexual partners, have been found to be positively associated with both ever and regular testing for HIV/STI among GBQ men (Guadamuz, Cheung, Wei, Koe, & Lim, 2015; Holt et al., 2014; Machouf et al., 2011; Noble, Jones, Bowles, DiNenno, & Tregear, 2017; Visser, Heijne, Hogewoning, & van Aar, 2017). Sexual identity has also been shown to be significantly correlated with ever testing for HIV testing among GBQ men, with those who identify as gay being more likely to have had ever tested for HIV, as opposed to those who identify as bisexual or heterosexual (Guadamuz et al., 2015; Noble et al., 2017; Pham et al., 2017; Witzel, Melendez-Torres, Hickson, & Weatherburn, 2016). Furthermore, positive associations between degrees of sexual orientation disclosure or “outness” and HIV/STI testing behaviors have been established by several studies (den Daas et al., 2016; Pachankis et al., 2015; Wilkerson, Fuchs, Brady, Jones-Webb, & Simon Rosser, 2014).
At the end of 2018, a total of 8,295 incident HIV infections among Singapore residents have been notified to the Singapore Ministry of Health. In 2011, yearly reported cases of HIV transmitted through male “homosexual or bisexual” modes exceeded that of “heterosexual” modes for the first time and that trend has persisted since (Ministry of Health Singapore, 2019). Despite the increasing prevalence of HIV among GBQ men in Singapore, little has been published on HIV/STI testing among GBQ men in Singapore and the risk factors that drive the spread of HIV in the present setting. This may be attributed to negative attitudes toward GBQ men among the general population (Mathews, Gee, Chiang, & World, 2015), and the existence of Section 377A of the Penal Code, which criminalizes sexual relations between men with penalties of imprisonment for a term that may extend up to 2 years. These sociolegal factors make discussion of health issues and rights among GBQ men challenging in the present setting.
In Singapore, HIV/STI testing is available at both government-run or private health care institutions and at a list of “anonymous” test sites. Under the Infectious Diseases Act, all positive test results for HIV, along with the identities of those who test positive, must be reported to the Singapore Ministry of Health within 72 hours of diagnosis (Singapore Government, 2003). Considering this law, the anonymous testing scheme was introduced in 1991 in a bid to encourage testing without the fear of being identified. At the end of 2018, there were a total of 10 anonymous testing sites for HIV in Singapore, comprising nine general practitioners and a volunteer-run community-based clinic (Ministry of Health Singapore, 2018). These clinics designate special timings to operate anonymous testing services, where interested individuals may get tested for HIV without having to provide any personal identifiers (Health Promotion Board Singapore, 2018).
Although the factors associated with the frequency and recency of HIV or other STIs among GBQ men are well-established through epidemiological studies, fewer studies have sought to critically examine how these factors intersect with social realities that enable or restrict HIV/STI testing-related behaviors or delineate the processes that underlie different types of testing patterns among GBQ men. Several typologies relating to HIV testing behaviors have been proposed in the extant literature. Boydell, Buston, and McDaid (2017) propose three patterns of HIV testing among young gay and bisexual men in Scotland, including habitual testers who test as a personal or community responsibility, reactive testers who test in response to exposure to sexual risk or to new relationships, and ad hoc testers who are motivated to test but experience barriers or disruptions to regular testing schedules. Similarly, Hussen and colleagues (2013) propose a typology of four testing patterns among Black men who have sex with men (MSM) in southeastern United States, namely, maintenance testers who test regularly as a responsibility to self, risk-based testers who test as a result of sexual behavior or new relationships, convenience testers who test as and when opportunities arise, and test avoiders who test irregularly or do not follow up on results.
Notwithstanding the aforementioned effective typologies posited by other scholars, we believe that this study extends such work by fleshing out the processes that underpin different patterns of HIV/STI testing among GBQ men. The approach also builds on the existing typologies by emphasizing the experiences of rather than types of individuals. This approach aligns with the call to transcend biomedical, behavioral, social, and structural distinctions toward HIV prevention and for the development of holistic HIV prevention interventions “that engage with the everyday lives of people and be integrated into their social relations and social practices” (Kippax & Stephenson, 2012, p. 789). Moreover, we note how participants in this study displayed the ability to switch between patterns of testing based on the psychosocial, contextual, and economic resources that are available to them at the point of testing, and simultaneously employ different pathways to testing within a certain time frame. As such, examining motivations to test and the social and structural factors that enable them more accurately represents the realities that participants constructed in the sharing of their past testing experiences. We believe that such a typology would serve as a useful tool to derive health promotion interventions and recommendations that specifically aim to bolster or address these underlying factors through separate but complementary efforts to promote the uptake of HIV or other STI testing in the GBQ community.
Situating GBQ Male Identities in Singapore
Singapore society has largely held negative perceptions of and attitudes toward lesbian, gay, bisexual, and transgender (LGBT) individuals. Nationally representative surveys across the past decade have consistently found that Singaporeans perceived sexual relations between two adults of the same sex as being wrong, are intolerant of homosexual content in the media, are against the idea of gay marriage, or are not in favor of the repeal of Section 377A, the law that criminalizes sexual relations between men (Chua, Su, Tan, & Jie, 2017; Detenber et al., 2007; Mathews et al., 2015; Panchapakesan, Li, & Ho, 2014). The media in Singapore has played an instrumental role in propagating and reproducing such stigma toward LGBT individuals, and in particular, GBQ men in Singapore. This has manifested through the negative portrayal of GBQ men (Atkins & Project, 2012), the censorship of media content that normalizes same-sex relationships (Yue & Zubillaga-Pow, 2012), as well as blaming GBQ men for the spread of HIV in Singapore (Goh, 2008).
These negative attitudes and the institutional structures that reproduce them undoubtedly have an impact on sexual health seeking, and specifically, HIV/STI testing among GBQ men. A recent study by Tan and colleagues (2019) has posited how this sociocultural milieu that pathologizes the GBQ male identity, alongside the potential criminal implications of being identified as gay, bisexual, or queer, disincentivizes GBQ men being seen at sexual health care institutions, and subsequently impacts the uptake of HIV/STI testing among GBQ men in Singapore. Another published study by Tan and colleagues (2019) corroborates this with evidence that GBQ men in Singapore who are more “out,” or have disclosed their sexual orientation to others to a greater extent, are more likely to engage in both recent and frequent HIV/STI testing. Against this sociolegal backdrop that disincentivizes HIV/STI testing, it is thus imperative for us to take a critical, in-depth exploration of the motivations to test for HIV/STI for GBQ men, and delineate the pathways that individuals may take to engage in such sexual health-seeking behaviors.
Method
We drew on an interpretivist epistemology in designing this qualitative study. Interpretivism takes human interpretation as the starting point for the construction of knowledge in the social world (Prasad, 2018) and is employed as a means of accessing and generating knowledge in this study. An interpretivist approach serves as an appropriate means of accessing the varying meanings, perceptions, and motivations that underlie testing-related behaviors among participants in this study and is thus useful for developing a typology of HIV/STI testing patterns and corresponding recommendations for interventions in the given social context or setting.
Participants
This study was conducted among 35 self-identified GBQ men from October 2017 to June 2018. Ethics approval was obtained from the institutional review board at the National University of Singapore (NUS IRB Reference Code S-17-181) prior to recruitment. Eligibility criteria for the sample included participants who self-identified GBQ men, aged 21 and above, and who were Singapore citizens or permanent residents at the point of recruitment. Recruitment of participants was done through a recruitment message posted on and shared through social media, tapping on both personal and community group networks. Participants were purposively sampled based on age, educational attainment, and self-reported past diagnoses of HIV/STI. This was done so that our interviews captured a diverse range of participant accounts reflecting experiences across socioeconomic backgrounds, birth cohorts, self-perceived risk, and experiences of attending sexual health services. Recruitment ceased after thematic saturation was achieved, or when no new codes, themes, or patterns emerged from the data.
Data Generation
The lead author, who is a trained qualitative researcher, identifies as a gay cisgender male, and volunteers for peer-led support groups among drug-using and HIV-positive GBQ men in the local GBQ male community, conducted all interviews. All interviews were conducted in the English language, took between 45 and 90 minutes to complete, and took place at a conducive location. All participants were provided with a participant information sheet and provided verbal consent to participate. All interviews were audio-recorded and subsequently transcribed verbatim, except for one interviewee who refused audio-recording, and detailed field notes were taken instead. Each participant was reimbursed SGD50.00 (~USD36.00) for their time. All interviews were semistructured, and a topic guide was employed to steer the interview process, while allowing for deeper investigation of certain themes that arose during the interviews. The topic guide covered topics of sexual identity formation and development, formative sexual experiences, relationships, HIV/STI testing experiences, experiences with health care institutions and other community-based organizations, and lived experiences of HIV/STI diagnosis and acquisition. A summary of participants’ demographic characteristics is given in Supplemental Table S1.
Data Analysis
Data were analyzed by both the lead and second authors, adopting the six-stage process to conduct thematic analysis (TA) as prescribed by Braun and Clarke (2006, 2013). TA is a theoretically flexible method of analysis that can generate rich, detailed, and complex accounts of data. An inductive TA approach was adopted to identify themes within the study’s interpretivist approach, where both semantic and latent themes were generated from the data without a pre-existing framework. In the first stage of analysis, both researchers read through the transcripts and familiarized themselves with the data prior to coding. In the second stage, both authors proceeded to conduct line-by-line and complete coding of initial transcripts to develop a list of codes. The initial list of codes was then used by both the lead and second authors to independently code a randomly selected transcript, and new codes as well as discrepancies in coding were discussed to ensure that codes and developing themes were adequately fleshed out. This process was done iteratively to develop a third and final coding frame, which both authors felt adequately covered the range of semantic and latent codes and themes for the dataset, and was subsequently used to code the remaining transcripts. In the third stage, we began to consolidate our codes and started to draw stronger links between codes and developing themes. As we were still coding transcripts at this point, a recursive method and process of comparing new codes with the existing codes and themes as well as themes with the data was employed to improve the rigor of our inductive approach (Braun & Clarke, 2013). In the fourth and fifth stages, both authors met several times throughout the process of coding, as well as at the end of the coding process to iteratively review, define, and name the themes and to develop conceptual maps between themes, subthemes, and our codes. It was at this stage when the typology began taking shape as we grouped our themes of factors influencing HIV/STI testing across two broader, overarching axes based on the regularity of testing, relative to internal or external factors that motivate testing behaviors. In the final stage, we presented our findings as written in the “Results” section of this article and proposed interventions and recommendations that were subsequently derived from our typology. Data from the coded transcripts were organized using NVivo 11 software (QSR International Pty Ltd, Melbourne, Australia).
Data Quality and Trustworthiness
Throughout the data collection process, care was taken to ensure that trustworthiness and quality of the data was maintained (Lincoln & Guba, 1985). The interviewer, as a member of the GBQ male community, acknowledged not only his own shared position with the participants but also his privileged position as a member of the research team. The interviewer sought to mitigate the impact of any pre-conceived biases and theoretical positions through the process of memo-writing following each interview, which was done iteratively and reflexively to reflect on the style of the interview, reactivity in participants’ responses, and emerging themes. Contents of the memos were not reported in the results of this study, but served instead as opportunities for reflexive reflections by the interviewer and as references during the coding process in the development of codes and themes.
The lead author took several measures to improve the credibility of the study findings. The lead author, as the main interviewer for all participants, first adhered to the institutional review board’s suggestions to warn participants about the potential risk of criminalization that sharing experiences around sexual relations with other men would entail. However, the interviewer also began the interview with self-disclosure of his own identity as a GBQ man, sharing more on his motivations for the study as a member of the community, and by assuring participants of his independence from any health care institutions or government-related institutions. This helped to establish rapport and trust between the participants and the interviewer, and that the interviewer had no ill intentions in conducting the interviews and had the participants’ and the wider community’s interests at heart. Furthermore, participants were assured of the confidential nature of the study, and that no personal identifiers would be collected at any point. The interviewer also told participants that any instances where participants may have accidentally disclosed their own names or other identifiable information would be redacted from the eventual transcripts. To improve dependability of the results, the lead author and interviewer also collaborated with an additional coder and data analyst who does not identify as a GBQ male to improve the rigor of the coding discussions (Barbour, 2001). Transferability of the study’s findings is maintained through a detailed description of the study methods and a thick description of participants’ accounts of their sexual health-seeking behaviors.
Results
Typology of HIV/STI Testing Behaviors
Table 1 summarizes the typology of HIV/STI screening behaviors among the GBQ men who participated in the study. Participants described four distinct patterns of testing that could be categorized along the following two defining factors: first, based on the regularity of testing (episodic vs. regular) and second based on the source of the motivation to test (internal vs. external). These four patterns of testing included triggered episodic testing (episodic testing, internal motivator), influenced episodic testing (episodic testing, external motivator), institutionalized regular testing (regular testing, external motivator), and value-based regular testing (regular testing, internal motivator). Participants also described unique sets of individual, interpersonal, and contextual factors that precipitate or serve as preconditions to each testing pattern.
Typology of HIV/STI Testing Patterns by Regularity of Testing Relative to Factors Motivating Testing Behaviors.
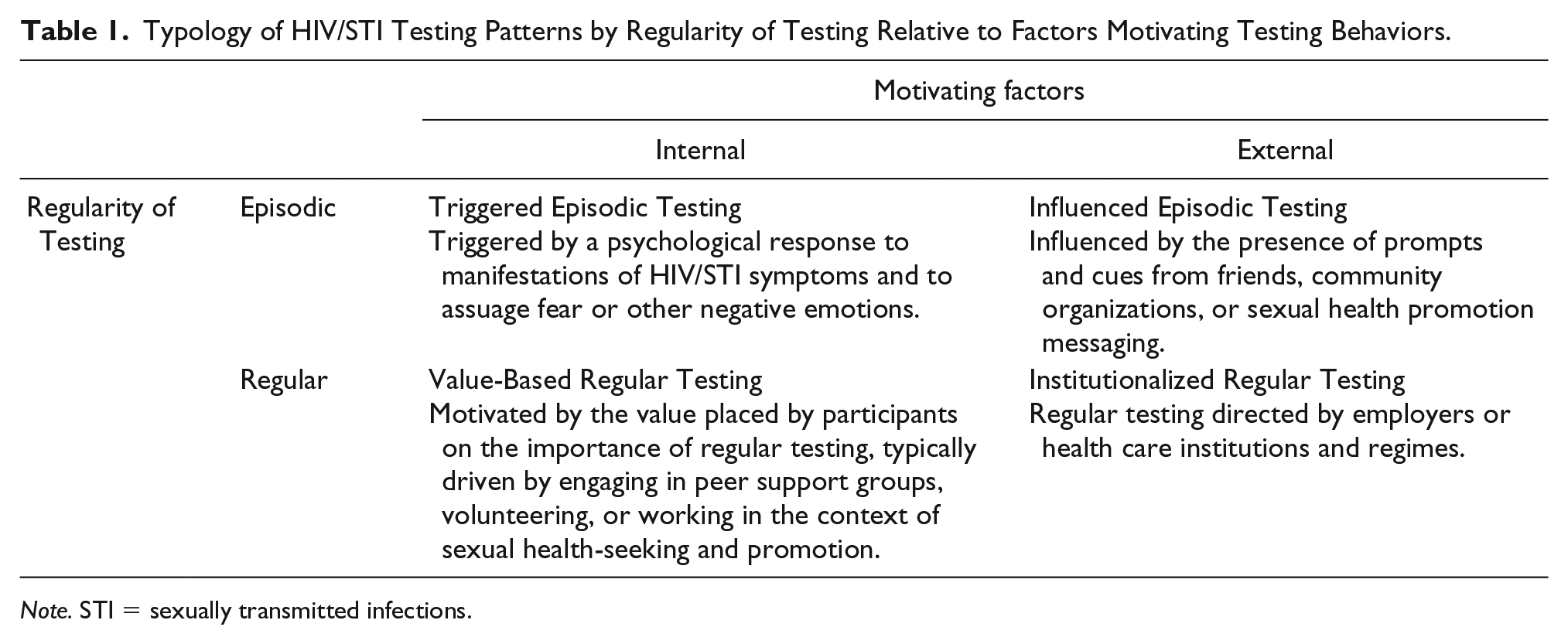
Note. STI = sexually transmitted infections.
Triggered Episodic Testing
Triggered episodic testing is defined by testing behaviors that are triggered in response to a heightened sense of one’s own HIV or STI acquisition risk, following discrete risk-defining events or events that cause an individual to reevaluate one’s own perceived risk following such events. Specifically, participants described how the experience of fear may be immediate, delayed, triggered, or even absent—to the point where testing was eventually precipitated by physical manifestations of HIV or STI symptoms. The first form of triggered episodic testing is characterized by experiences of fear over the prospect of having acquired HIV or other STIs immediately following sexual experiences that are perceived to be high risk in the context of HIV or other STI acquisition: So, my first STI test was after a risky exchange . . . I guess a bit of cruising happened, we ended up in the toilet, and then one thing led to another . . . And after that I was like, okay I have to wait a few weeks, because I know [about] the window period . . . So I went to get a test, one month and then three months later, I did the syphilis test together with HIV. (30- to 39-year-old gay male, previously diagnosed with other STIs)
This participant described how a “risky exchange” had taken place at a public gym toilet, which involved insertive anal intercourse without the use of condoms. Following this event, the participant talked about being aware of the risk of acquiring HIV or STI through unprotected anal sex as the insertive partner and had subsequently planned to get tested for both HIV and syphilis in accordance with the window period for HIV testing: 1 month, and 3 months later for a confirmatory test.
Unlike the aforementioned participant, whose articulation of events reflected a good grasp of sexual health knowledge, an understanding of the risks associated with specific sexual practices, and the psychological capacity or motivation to get tested, other participants described being only confronted with the fear of having acquired HIV or other STIs from past risk or exposure events after a considerable period: I guess the trigger event happens when you think that, or you read something, and then you go like, oh shit. Maybe I should go test myself—I haven’t tested myself in awhile. You think there might be a slight chance you get exposed? I haven’t tested for the past 18 months already, and then you just happen to be talking to somebody . . . , or I kissed that guy, you know, and there might have been some minor lacerations in my mouth, maybe I should go get tested. (30- to 39-year-old gay male, previously diagnosed with other STIs)
This situation illustrates how each sexual event may serve as a source of distress in the context of acquiring HIV or other STIs and requires resolution by means of getting tested and confirming of one’s own HIV/STI status. This participant had described how his feelings of fear associated with past risk events were initially suppressed, but were eventually brought to the forefront of his consciousness upon being exposed to trigger events that allowed him to reevaluate his perceived risk of HIV/STI acquisition.
Finally, several participants spoke about how they eventually tested for HIV or other STIs in response to physical manifestations or symptoms that they perceived to be associated with the potential acquisition of HIV or other STIs: But the thing is . . . I had high fever for a week, I was very worried, because I have never had high fever for that long before. That’s when I was hospitalized and uhm . . . I ask the doctor to help me check for HIV, and that’s when I was diagnosed. (20- to 29-year-old gay male, previously diagnosed with HIV)
In contrast to the aforementioned first two participants, who spoke about going for testing in response to immediate or delayed fear, or a heightened sense of risk in the context of exposure to HIV or other STIs, this participant articulated how he had not felt the need to get tested until he experienced symptoms that were incongruent with his usual experiences of illness and attributed these symptoms instead to the possible acquisition of HIV.
Influenced Episodic Testing
Influenced episodic testing is defined by testing behaviors that are influenced by prompts or cues related to the initiation or promotion of sexual health-seeking behaviors. Specifically, participants described these prompts as typically originating from friends, who provided emotional support and encouragement to get tested, or directly from community-based organizations via outreach efforts or sexual health promotion messages in GBQ-specific venues: Like, ‘hey there’s a free HIV test coming up for this place at this date, do you want to go, or not?’ You know, that kind of stuff. Or like, ‘hey, since you are going clubbing, there’s a free HIV test, why not just go for it?’ Or like, their friends who are volunteering for [HIV/AIDS-related NGO] will be like, “hey, do you need a free HIV test?” (20- to 29-year-old bisexual male)
This participant, who described his social network as comprising individuals who actively engage in social activities in the GBQ community, talked about how his friends would often notify him of events in the community whenever free, anonymous HIV, or other STI testing are available. As the cost of anonymous testing for HIV or other STIs is high in the present setting, free and anonymized testing is a significant incentive to test for individuals like this participant, who described himself as being an undergraduate who was not earning any income but was sexually active.
In contrast, another participant spoke about how his friends who did not identify as GBQ men influenced his testing behaviors, by providing him emotional support and encouragement as he navigated the fears that he had toward getting tested: I shared with two of my close friends from secondary school who knew about [my sexual orientation] that I never ever had an HIV test done, because I was so afraid of what I would find. It was all the avoidance, I couldn’t get out of the fear. And then they told me that, two of them told me that, okay, we will give you by the end of the year—if you don’t do it, we will all go with you. But before that, I also told one of my course mates who was also gay, and he was like, okay, we are going to do it next week. So he brought me to the test center to get tested. (20- to 29-year-old gay male)
Most participants who participated in activities that took place in social spaces in the local GBQ community talked about being exposed to sexual health messaging or services from community-based organizations that operate or advertise in such spaces. These spaces included both online venues such as GBQ-specific Internet forums, geosocial networking mobile apps, and other GBQ-specific websites, as well as brick-and-mortar venues such as sex-on-premises venues, bars, and clubs. Another participant illustrates this point by describing how he got tested for HIV on two separate occasions, once at a club, and then once at a sauna (sex-on-premises venue) where community-based organizations were holding outreach programs: I think like it was the [NGO] van outside [club]? That was the first time I tested . . . But it was when I went to the club. I think once was at the. . . I mean like I don’t really go to the sauna, but I went to sauna and there were these three people trying to ask me to test, and so I tested. (20- to 29-year-old gay male, previously diagnosed with HIV and other STIs)
Institutionalized Regular Testing
Institutionalized regular testing is defined as regular testing as influenced by institutions such as employment or other health care organizations. It is similar to influenced episodic testing, in that the motivators to test stem from external sources, but regularity is imposed on patterns of HIV or other STI testing due to institutionalized processes. Such institutionalized processes included being participants in research studies and opt in testing as part of other regular checkups. However, this form of testing is the least common among participants, as it presupposes the presence of an organization or institution influencing participants’ testing behaviors on a regular basis: Coincidentally it was part of my regular check-up. At my previous check-up they were asking me if I want to participate in a study for them, like the catch is that I have to come back for regular testing which I said okay . . . that’s when I got, I was diagnosed positive there. Now, whenever I come by for my [regular HIV] check-up, at the hospital, I will just opt-in for STD screening too. (20- to 29-year-old gay male, previously diagnosed with HIV)
This participant presents a unique case of how he had to test for HIV according to a schedule, as a result of his participation in a research study that took place at a government-run specialist sexual health clinic. However, like most other participants who had previously been diagnosed with HIV and are presently attending regular health checks with an HIV physician, he then proceeded to highlight how he regularly takes the opportunity to voluntarily screen for other STIs, aside from his regular blood tests: Yah, I test regularly for HIV—I’m actually on PrEP [pre-exposure prophylaxis] right now? But I’m on on-demand PrEP [a form of PrEP where dosing occurs on an event-driven basis; this is in contrast to daily PrEP where dosing occurs on a daily basis]. I just switched over. So I have to do my regular three-monthly check, but since I’m on on-demand, so my Hep B and kidney function tests are every six months. (20- to 29-year-old bisexual male)
As HIV PrEP was only recently rolled out in the present setting, only a few participants described themselves as being on PrEP at the point of being interviewed. Like the participant quoted earlier, all participants who talked about being on PrEP also described testing regularly for HIV as part of their regular checkups with their health care provider.
Value-Based Regular Testing
Value-based regular testing is defined as regular testing driven by the value that participants place on the importance of regular testing. Participants described how these values were fostered or nurtured typically through past engagement with peer support groups, volunteering for HIV/AIDS-related nongovernmental organizations (NGOs), or working in the context of sexual health-seeking and promotion. Several participants highlighted how working in the context of sexual health care or volunteering with HIV/AIDS-related community-based organizations helped them shape their perceptions and attitudes toward sexual health: At my previous workplace, I was also working for a healthcare organization . . . when I started here [at a healthcare organization], it became a regular thing, then I thought that it was just simply part of my routine . . . Ironically, I was working with people living with HIV . . . so, so it made me see the importance of regular testing, especially for someone who has, has a lot of sexual partners. (30- to 39-year-old gay male, previously diagnosed with HIV and other STIs)
The aforementioned participant’s explanation of how his employment at a health care organization shaped his attitudes toward regular testing is echoed in the experiences of most participants who talked about volunteering or working for organizations in the health care sector. However, beyond directly shaping an individual’s attitudes toward sexual health practices, a minority of participants illustrated how volunteering for organizations that provide comprehensive and holistic education and support for sexual identity issues indirectly impacted their attitudes toward sexual health as well: It was that whole volunteering experience . . . I gained a lot of self-acceptance through them . . . Because back then I kept thinking that being gay is bad, being gay is wrong . . . I guess I began to realize that you know, maybe what the media portrayed as gay sex being like a sin . . . and then gradually you learn that—okay so now you know that this thing is not bad, how do you go about engaging in it safely for yourself? (20- to 29-year-old gay male)
This participant explained how volunteering at a community-based organization allowed him to gain “self-acceptance” in the context of his sexual identity as a gay man. He articulated specifically how this acceptance of self and his reframing of “gay sex” as something that was not “sinful” was instrumental toward approaching sex in a safe manner. The preceding quote illustrates a possible mechanism of how sexual identity development and acceptance may impact sexual health practices, where stigma and the unconstructive labeling or moralizing of “gay sex” create a false binary or what is, in the case of this participant, whether it is a “sin” or not. Essentially, this labeling eclipses the potential for meaningful discussion or internalization of sexual health knowledge, and corresponding sexual health-seeking behaviors.
Discussion
The proposed typology of testing patterns among GBQ men provides a framework to better understand the various mechanisms and pathways through which participants may decide or act on different types of testing behaviors for HIV/STI. It explains how participants may test for HIV/STI through these four proposed mechanisms, which are not mutually exclusive for a given individual, but are precipitated by unique sets of motivators. Furthermore, participants illustrate the ability to switch between types of testing patterns or combine patterns of testing based on their existing psychosocial and contextual resources.
Triggered episodic testing patterns highlight how risk assessment plays an instrumental role in influencing HIV or other STI testing behaviors among GBQ men. This finding stands in contrast to the extant literature that finds no clear relationship between HIV risk perception and an individual’s frequency or recency of HIV testing. A study among Cambodian MSM found that those who had a higher perceived risk of HIV acquisition were significantly more likely to have had tested for HIV in the last 6 months than those who had lower risk perceptions (Yi et al., 2015), whereas a study among MSM in Peru found an inverse association between HIV risk perception and recent HIV testing (Vargas et al., 2018). On the contrary, a cross-sectional survey among MSM in Germany found that there was no statistically significant association between HIV risk perception and decisions regarding HIV testing (Marcus, Gassowski, & Drewes, 2016). Participants in this study highlighted how the assessment of risk varies from person to person and may fluctuate or shift following exposure to risk-defining events, or other factors that shape an individual’s own risk assessment strategies, which warrants further research.
Influenced episodic testing patterns illustrate the role of social capital in driving HIV or other STI testing behaviors as well. Our findings specifically delineate the ways in which having within-group and between-group social capital, through friendships within the local GBQ male community or with individuals who are not identified as GBQ, may influence testing through prompts or a sense of social support. This is aligned with Putnam’s (2000) conception of bonding and bridging social capital, which are defined as the existence of within-group and between-group network ties, respectively. Although the impact of both bonding and bridging social capital on health care access remains inconclusive due to issues relating to the lack of uniformity in their measurement (Derose & Varda, 2009), or may pose as a health liability depending on the social context (Kawachi, Subramanian, & Kim, 2008), our findings highlight specific nuances in how within and between-group social capital may operate to positively impact HIV/STI testing among GBQ men.
Our findings are supported by studies that reported both positive and negative associations between measures of within-group or bonding social capital among MSM, and the recent HIV testing (Grover et al., 2016; Scott et al., 2014). We believe that our findings also highlight the mechanism through which perceived connectedness to the GBQ community or acceptance of one’s own sexual identity, and correspondingly being comfortable with participating in social spaces that are linked to the GBQ male community, may influence HIV or other STI testing. This is because exposure to sexual health messaging in the GBQ male community, or more specifically, in online or brick-and-mortar venues where GBQ men typically meet, presupposes individuals being present in those spaces, as described by most of our participants. This position is supported by the extant literature which finds that identifying as gay relative to being bisexual or straight, and degrees of sexual orientation disclosure or “outness,” is positively associated with both the frequency and recency of HIV testing among MSM (den Daas et al., 2016; Guadamuz et al., 2015; Noble et al., 2017; Pachankis et al., 2015; Pham et al., 2017; Wilkerson et al., 2014; Witzel et al., 2016). The impact of between-group or bridging social capital on HIV/STI testing has been less well-established among GBQ men, and thus warrants further study.
An alternative explanation for the impact of sexual orientation disclosure or sexual identity on HIV or other STI testing would be a position that is proposed by participants who shared more about their value-based regular testing patterns. Specifically, that self-acceptance of one’s sexual identity may promote feelings of self-worth, and consequently facilitate health-seeking behaviors that may align with a more positive view on one’s perceived self-esteem. This finding is consistent with studies that similarly found that the positive association between sexual identity development and sexual health-seeking behaviors may be mediated by greater psychological well-being among the MSM sampled (Mimiaga et al., 2015; Riggle, Rostosky, Black, & Rosenkrantz, 2017; Wagner et al., 2012; Whitman & Nadal, 2015).
Table 2 summarizes the recommendations and interventions proposed to increase the uptake of HIV or other STI testing behaviors among GBQ men, by the patterns of HIV or other STI testing. Participants who experience either triggered episodic testing behaviors or institutionalized regular testing may provide an opportunity for health care providers and community-based testing services to provide HIV/STI-related education and risk assessment of GBQ men who attend such services. Unlike value-based regular or influenced episodic testing patterns, those who test in response to a heightened sense of one’s own HIV/STI acquisition risk or as part of regular institutionalized routines may comprise GBQ men who might not be connected to the GBQ male community or are not “out” about their sexual orientation. This presents a ripe opportunity for health care providers to provide these men with more important information and support on not just sexual health knowledge but also sexual identity development. Health care providers, especially those who provide testing services to GBQ men who test regularly as part of institutionalized processes, should also consider extending information and services related to HIV or STI prevention strategies such as PrEP and TasP for HIV-positive or HIV-negative GBQ men, respectively.
Proposed Interventions to Increase Uptake of HIV and Other STI Testing Among GBQ Men, by Patterns of Testing.
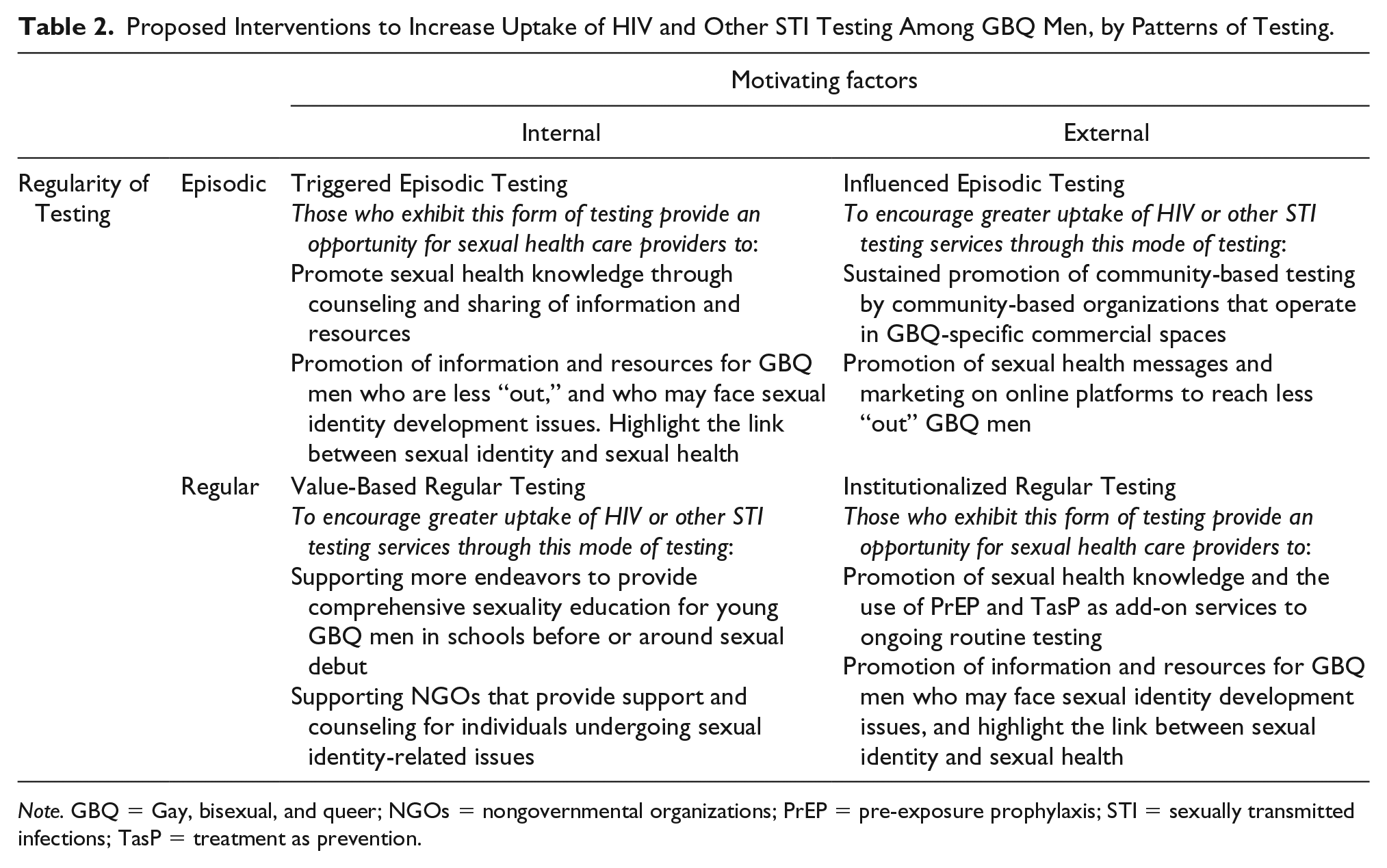
Note. GBQ = Gay, bisexual, and queer; NGOs = nongovernmental organizations; PrEP = pre-exposure prophylaxis; STI = sexually transmitted infections; TasP = treatment as prevention.
To encourage influenced episodic testing, community-based messaging and testing should be carried out and sustained by community-based organizations, as most participants highlighted this as an influential driver of HIV/STI testing behaviors. Given the presupposition that such services only reach GBQ men who participate in activities where such community-based organizations operate, such as in GBQ-specific commercial venues, more initiatives and funding could be directed toward reaching GBQ men who may be less “out,” likely through online venues that accord these men a comfortable level of anonymity. Finally, the values that drive testing behaviors among GBQ men who exhibit value-based regular testing behaviors tend to overlap or interact with a positive self-concept and self-esteem. Early intervention programs can positively impact identity formation processes for young GBQ men and incorporate sexual health education. Greater care may be made to not stigmatizing GBQ men who may not be comfortable openly identifying as gay, bisexual, or queer.
Although societal attitudes toward GBQ men remain largely negative and most Singaporeans do not support the repeal of Section 377A of the penal code, participants in this study exhibited resilience as manifested through their sexual health-seeking strategies, and offer perspectives on how they are able to engage in HIV/STI testing in spite of the perceived costs of doing so in such a sociolegal backdrop. The proposed typology thus highlights opportunities for sexual health-seeking among GBQ men, as well as the importance of nevertheless maintaining channels for information and sexual health-seeking behaviors, building social capital, and expanding funding of sexual identity development-related resources to motivate and enable engagement in HIV/STI testing among GBQ men.
We are mindful of the study’s limitations. First, the typology focused mainly on the drivers or facilitators of testing patterns but does not capture the complex nature of the barriers to HIV or other STI testing that GBQ men face in the present setting. Nevertheless, its focus on individual or contextual resources allows us to better understand the tangible and intangible resources required by diverse GBQ men to overcome the barriers that may impact health-seeking behaviors. Furthermore, in spite of our best efforts to purposively recruit participants based on their age, educational attainment, and previous diagnoses of HIV/STI, the laws that criminalize gay sex and prevailing negative societal attitudes toward GBQ men in the present setting may prevent those who are less “out” or more uncomfortable with their sexual identities to participate in this study. However, we were mindful of ensuring that all recruitment advertisements reiterated the anonymous and confidential nature of this study, and that no personal identifiers would be collected at any point.
Conclusion
This study adopted an inductive approach to generate a typology of HIV or other STI testing among GBQ men in Singapore, which serves as a useful framework for deriving a range of interventions to promote regular testing for HIV/STI among GBQ men. It also highlights the preconditions or resources that underlie different types of testing behaviors, which enable the targeting and position of various interventions. As GBQ men are diverse and may possess varying levels of social, psychological, and economic resources at a given point in time, greater care should be made in differentiating health promotion messaging and interventions to maximize their impact among GBQ men.
Supplemental Material
Supplementary_File_S1_-_QHR-2018-1116.R1 – Supplemental material for Developing a Typology of HIV/STI Testing Patterns Among Gay, Bisexual, and Queer Men: A Framework to Guide Interventions
Supplemental material, Supplementary_File_S1_-_QHR-2018-1116.R1 for Developing a Typology of HIV/STI Testing Patterns Among Gay, Bisexual, and Queer Men: A Framework to Guide Interventions by Rayner Kay Jin Tan, Nashwinder Kaur, Mark I-Cheng Chen and Chen Seong Wong in Qualitative Health Research
Footnotes
Acknowledgements
The study team is indebted to all the participants who took part in the study. We would also like to thank all our community-based partners for their assistance in recruiting participants for the study, as well as Dr. Priscilla Ho Lai Peng and Mr. Muhamad Alif Bin Ibrahim for their comments. We would like to thank the editors and anonymous reviewers for their constructive and invaluable comments.
Authors’ Note
Chen Seong Wong is also affiliated with Yong Loo Lin School of Medicine, National University of Singapore, Singapore.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Saw Swee Hock School of Public Health, National University of Singapore. This publication was supported by the Singapore Ministry of Health’s National Medical Research Council under its Centre Grant Programme (NMRC CGAug16C021).
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.