
Abstract
The concept of quality of life (QoL) is used in consultations to plan the care and treatment of children and young people (CYP) with brain tumors (BTs). The way in which CYP, their parents, and their health care professionals (HCP) each understand the term has not been adequately investigated. This study aimed to review the current qualitative research on CYP, parents’ and clinicians’ concepts of QoL for CYP with BTs using meta-ethnography. Six studies were found, which reflected on the concept of QoL in CYP with BTs; all explored the CYP’s perspective and one study also touched upon parents’ concept. A conceptual model is presented. Normalcy (a “new normal”) was found to be the key element in the concept. This study calls for a conception of QoL, which foregrounds normalcy over the more common health-related quality of life (HRQoL) and the need to understand the concept from all perspectives and accommodate change over time.
Keywords
Introduction
The concept of quality of life (QoL) is important for children and young people (CYP) with brain tumors (BTs) in a number of ways. It has figured into outcomes research, into the development of interventions and in clinical trials all of which contribute to the protocols and standards of care used for delivering treatment to these children. Perhaps most important is that it may be used in the decision-making process between CYP, parents and health care professionals (HCPs). Expected QoL is often a key factor in determining whether patients with a life-threatening illness (LTI) or life-limiting condition (LLC) will be given a specific treatment or not (Crane, Haase, & Hickman, 2018; Pellegrino, 2000). This is particularly important in CYP with BTs for whom there are a number of diagnoses, which have a poor prognosis and so have to choose from a number of experimental therapies. Understanding the CYP’s perspective of QoL, as well as that of their parent and HCP, is critical to the success of decision making as a joint venture, especially because parents and HCPs may perceive QoL differently (Janse, Uiterwaal, Gemke, Kimpen, & Sinnema, 2005). Recent movements at the turn of the century to include the child’s perspective in their care and treatment (House of Commons Health Committee, 1997), makes understanding the views of CYP even more pertinent.
Understanding stakeholders’ conceptualizations of QoL is important not just for this application to clinical decision making but to all uses of the concept. These concepts are key to building an adequate theoretical or conceptual framework, which guides the development of QoL instruments. As Haase, Heiney, Ruccione, and Stutzer (1999) stress “without development of theory that is grounded in the experiences of patients, we are likely to continue the ‘shopping list’ approach to HRQL” (p. 130). A search for the conceptual frameworks involved in pediatric QoL measures revealed that most measures have no conceptual underpinning; studies recommend that pediatric QoL research invest time into theory development and evaluation (Davis et al., 2006). Lawford and Eiser (2001) suggest a theoretical model for QoL would clarify the domains and concepts to be assessed in QoL measures (avoiding need for wide range of current measures involving different domains) and understanding how they are related to one another rather than constituting an unrelated list.
The Review
Aim+
To understand CYP, family members and clinicians’ understanding of QoL as they use it in decision making for CYP with BTs through a meta-ethnographic review of research published internationally between 2007 and 2016.
Design
Search Methods
Original peer-reviewed articles presenting research exploring stakeholders’ concept of QoL in CYP with BTs are included in this review. The search is limited to papers published since 2007 (January 2007—February 2016) reflecting the survival curve for CYP with BTs, which has plateaued since the 2002-to-2007 survival rate data for central nervous system (CNS) tumors was published (Gatta et al., 2014; Munro, 2014).
A comprehensive search of the literature was undertaken using the following databases: Medline, PsycINFO, Embase, CINAHL, and Web of Science. Three main search components were used to identify all relevant and available literature: (a) CYP, parents, and HCPs; (b) QoL; and (c) BTs with a fourth search string to ensure the focus was on the CYP’s QoL (not that of the parent or HCP); (d) CYP. A combination of indexed and free text terms were used to reflect these four components. The MEDLINE search strategy is outlined in the supplemental information.
We included English language studies focusing on CYP (aged 0–24 years) with any type of BT, their parents/guardians, and HCPs in charge of their care.
Studies were excluded which:
Did not involve CYP (below 25 years old) or their family or an HCP in charge of their care. Any article with a mixed population, for example involving CYP and adults with BTs, will be excluded unless it is clear that CYPs below 25 years of age were the majority of the sample.
Focused on the QoL of the parent or HCP and not of the CYP.
Did not include BTs in the sample (if it is a mixed sample with other types of tumor this will still be included if data on CYP with BTs are reported separately).
Gave no justification for or did not explore the included dimensions or concept of QoL used in or underlying the article. To be included, studies must state/explore the conceptual under-pinnings of their QoL. We excluded studies, which simply fitted participants’ views into the domains and items of established QoL measures or which looked to operationalize QoL straight from their data without providing participants’ concept of QoL. Applying this criterion required going beyond the language of the articles to understanding at a conceptual level and marks the first application of the translational approach used in this review (see the “Synthesis Methodology” section).
Three reviewers (E.B., E.H., G.B.) screened one third of the abstracts identified and assessed them against the identified exclusion criteria. A second reviewer (J.H.) screened 30% of the abstracts overall to test for interrater reliability, calculated at 80% agreement. Papers identified from the initial database searches were screened for duplicates, which were removed. Citations were then screened for relevance and those that did not meet our inclusion criteria were removed. One reviewer (E.B.) screened all full texts and three reviewers (E.H., G.B., J.H.) screened 10% of the full texts each. Any disagreements over studies to be included or excluded were discussed by the reviewers until a consensus was reached.
Search Results
Of the 2,346 papers returned by the online search, six remained after screening (Figure 1, see supplemental information). No studies reporting on clinicians’ concepts of QoL were found. One of the six studies included parents who acted both as proxies for their deceased children and expressed their own views.
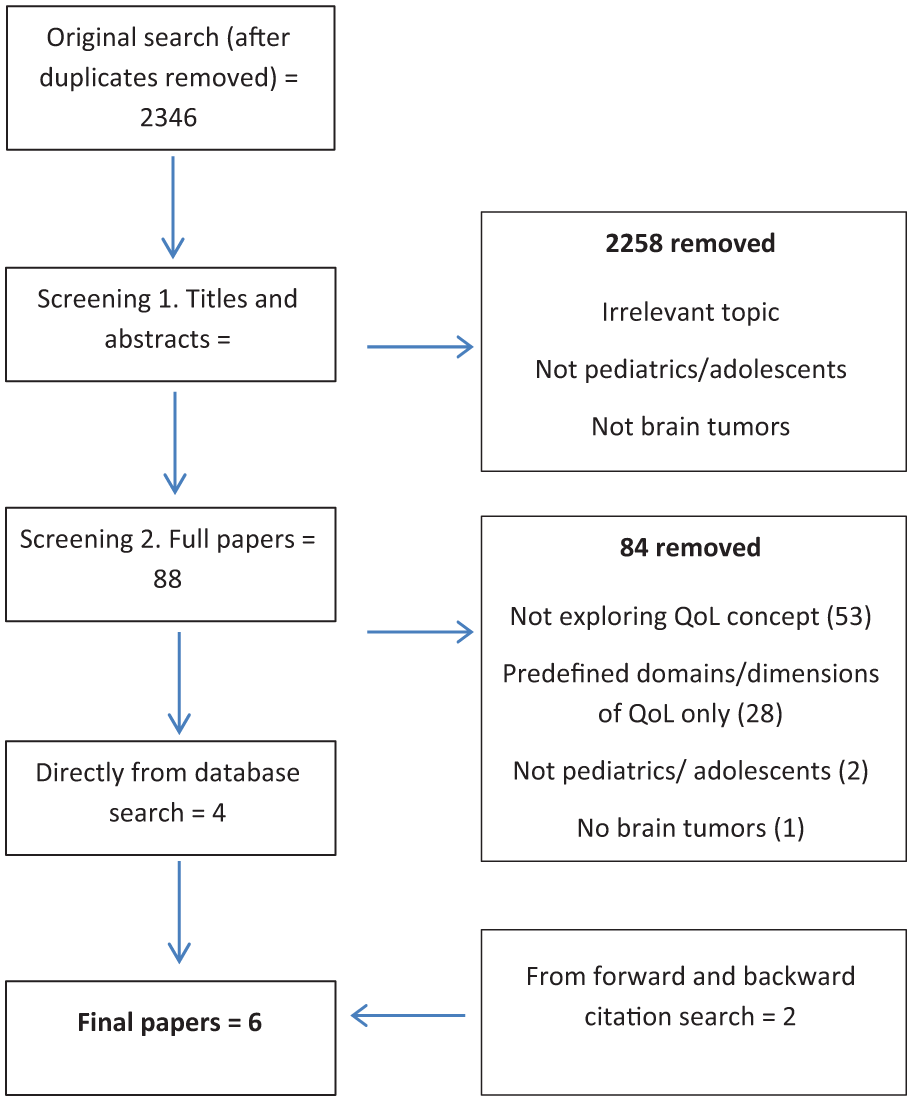
Flow diagram of search and inclusion process.
Quality Appraisal
Guidance for the conduct of systematic reviews recommends the use of quality assessment tools. Included articles were assessed for study quality using two tools. Qualitative research was appraised using recommendations from the Critical Appraisal Skills Programme (CASP) Qualitative Research Checklist (CASP, 2013). Mixed-methods research was appraised using recommendations from Guyatt et al.’s (1993) “Users’ Guides to the Medical Literature II.” Study quality was assessed for all six studies by two researchers (E.B. and J.H.), and any disagreements were resolved by consensus. Ratings are presented in Table 1. The quality appraisal did not yield any information that has led to the elimination of any of the studies, or to interpret their findings any differently.
Study and Patient Characteristics.
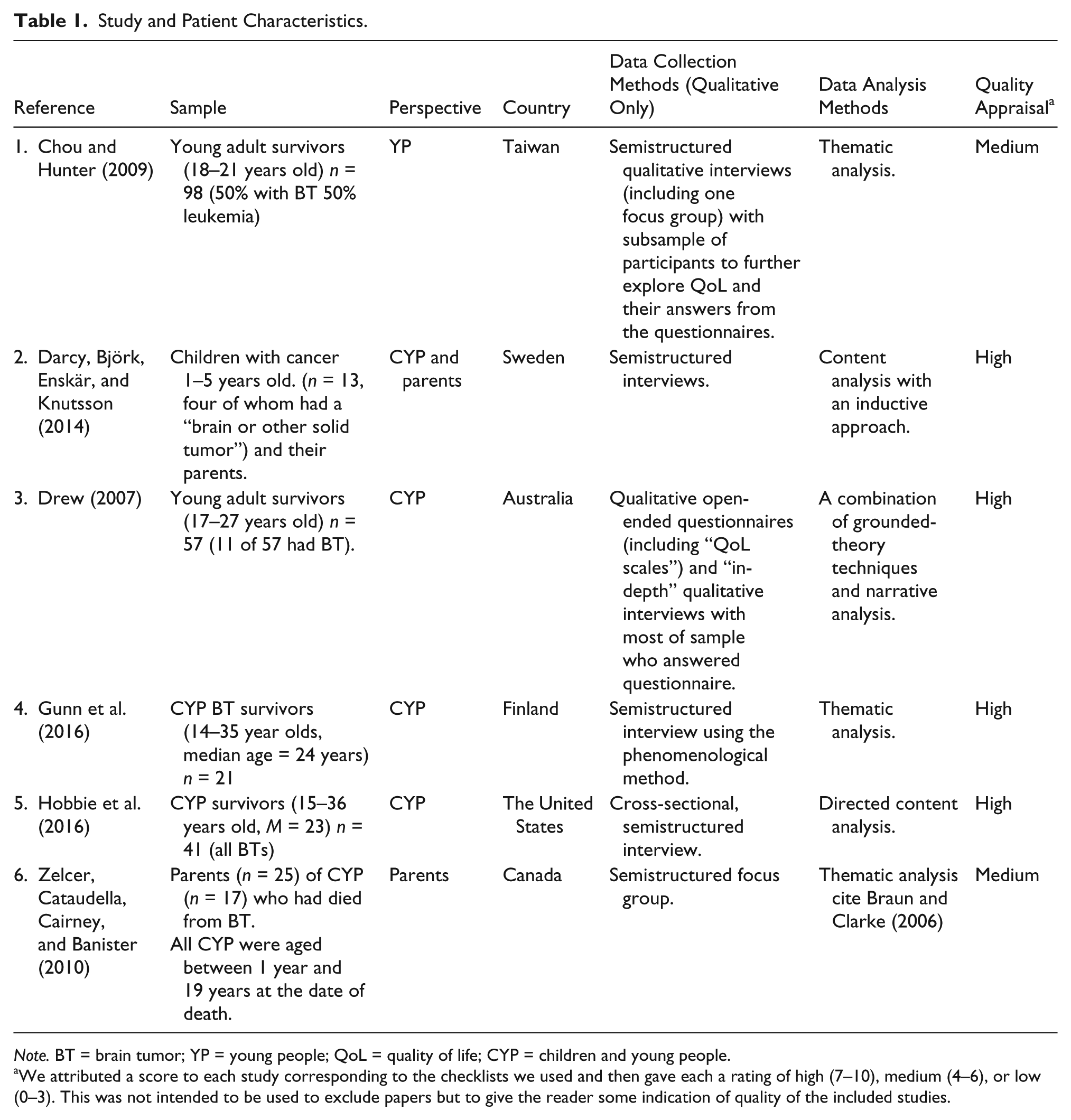
Note. BT = brain tumor; YP = young people; QoL = quality of life; CYP = children and young people.
We attributed a score to each study corresponding to the checklists we used and then gave each a rating of high (7–10), medium (4–6), or low (0–3). This was not intended to be used to exclude papers but to give the reader some indication of quality of the included studies.
Perspectives Represented in the Review
Four studies interviewed YP survivors (Chou & Hunter, 2009; Drew, 2007; Gunn et al., 2016; Hobbie et al., 2016). In one study, both parents and children were interviewed (Darcy, Björk, Enskär, & Knutsson, 2014). Their aim, however, was to capture “children’s experiences as reported by themselves and their parents” (Darcy et al., 2014, p. 610), hence it may be taken as providing the views of children with parents as proxies. The children were below 6 years old and undergoing treatment. Zelcer, Cataudella, Cairney, and Banister (2010) interview bereaved parents both as proxies for the deceased CYP and also as reporting on their own experiences. The findings taken from Zelcer et al. (2010) are limited to ones, which relate to the CYPs experiences rather than to parent’s own issues, for example, competing priorities and choosing place of death.
Synthesis Methodology
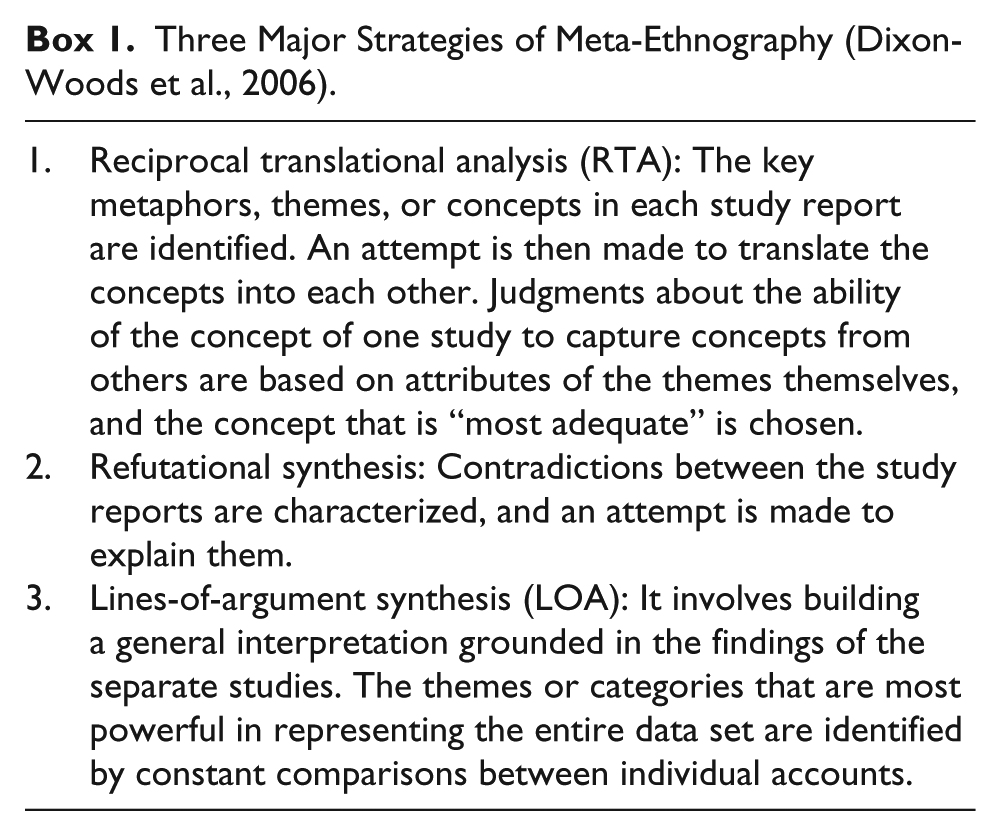
The synthesis employs the method of meta-ethnography, an interpretive form of analysis developed by Noblit and Hare (1988). The fundamental activity of this approach is translation, attempting to “transform interpretations offered by individual studies in such a way that they can be expressed in each other’s terms, thereby enabling a direct comparison of seemingly distinctive pieces of evidence” (Pope, Mays, & Popay, 2007, p. 75–76). We have chosen meta-ethnography as our approach to synthesis for a number of reasons: Although some of the studies in the sample are mixed method, the data which concern us are all qualitative; the sample is small and therefore translating the concepts from each study into the others is a manageable task. In addition, the literature reviewed is relatively coherent. Dixon-Woods et al. (2006) identify three basic strategies in meta-ethnography (Box 1). In this review, we employ two of them, reciprocal translational analysis (RTA) and line of argument.
Three Major Strategies of Meta-Ethnography (Dixon-Woods et al., 2006).
For all studies, we had to identify the key related concepts from the studies by reading closely their reflections on what life is like for the CYP. Identifying related themes and concepts in different studies is an integral part of synthesizing the literature: “studies focusing on similar topics may have conceptual overlaps, even if these are not apparent from the way the results are reported” (Popay et al., 2006, p. 18). Our goal in synthesis was to find these overlaps.
Some of the studies reviewed are mixed-methods studies; however, we are using only the qualitative data presented in them; data which are text-based and derived from semistructured interviews or focus groups. We further restrict our focus to the portions of the articles, which are relevant to stakeholder’s concepts of QoL for CYP with BTs. This extraction of relevant findings from the studies was itself an interpretative task. This review is thus carried out not simply using an interpretive method of synthesis but from an interpretive perspective throughout. Dixon-Woods et al. (2006) highlight the difficulties of using conventional search strategies for an interpretive synthesis. We extended the use of interpretative methodology to the searching and screening process to alleviate this problem (exclusion criterion 4, above). Even at the stage of screening, we needed to move beyond the literal text to determine whether we could find a concept of QoL independent of a measure.
Two reviewers were involved in the analysis and translations of the data (E.B. and R.L.). Both reviewers extracted the data and then compared the translations and any disagreements were discussed and a consensus reached.
Results
Synthesis
Key concepts were extracted from each paper and put into tables to understand the concepts of QoL presented by each paper and to allow the authors to interpret and translate the concepts into one another using meta-ethnography (Tables 2 and 3.).
Overarching Key Concepts Related to QoL for Each of the Included Studies.
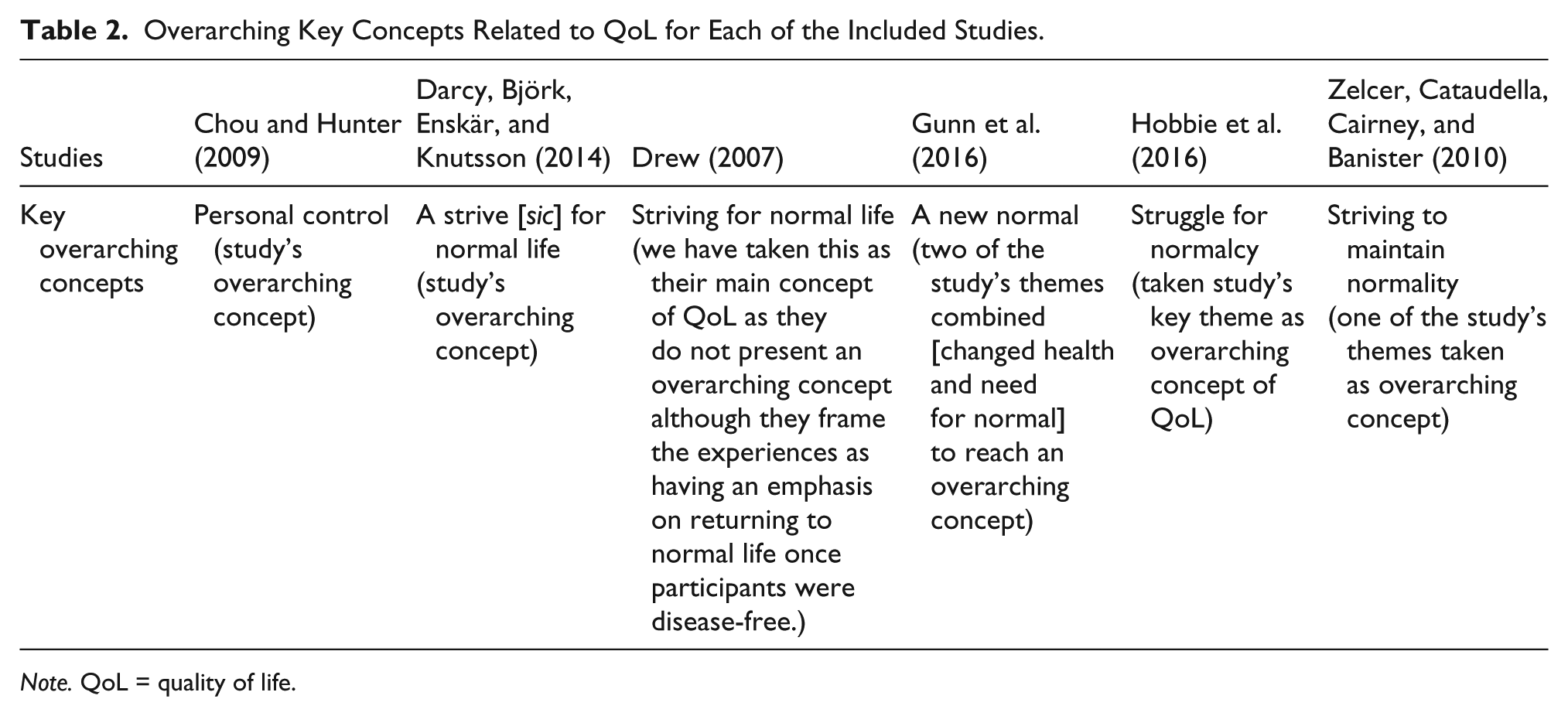
Note. QoL = quality of life.
Translations of Key Concepts in Included Studies.
Note. CYP = children and young people; YP = young people; QoL = quality of life.
RTA
The first task of analysis was to lay out the primary or overarching concept in each paper that was relevant to our research question (Table 2). To be explicit about how the concepts compared with one another, we created a spreadsheet into which we placed the concepts from each paper.
In five studies we found an overarching concept of “normalcy” or variants (Darcy et al., 2014; Drew, 2007; Gunn et al., 2016; Hobbie et al., 2016; Zelcer et al., 2010). Chou and Hunter (2009) present “personal control” as their main concept. Additional key concepts were identified from each paper to compare and translate the studies into one another. The additional concepts taken from the included studies were independence, social functioning, future, success, physical factors, change, and resilience.
We then created Table 3 which we used to translate the concepts into one another, showing how in each paper the relevant concepts overlapped or differed and explained these (Table 3). From this translation process, we arrived at the conclusion that the difference in overarching concepts of normalcy and control is a difference of point of view, of being process oriented or outcome oriented, control being the process and normalcy being the outcome. So, this dyad of “control-normalcy,” process–outcome is the overarching complementary conceptual dyad, which captures a QoL concept underlying all the studies reviewed. Four additional concepts emerged, which provide content to the idea of a new normalcy: personal relationships, independence, success, and a future. These are not simply measurable properties; rather, they identify domains within which survivors must achieve adaptations to realize normalcy and QoL.
In pursuing stakeholders’ concepts of QoL normalcy—a new normal—emerges as the key concept with control alongside as a process to reach and maintain normalcy. In the studies in which normalcy features as the overriding concept there are a number of references to striving for normalcy, clearly joining normalcy to process and to activity (Darcy et al., 2014; Drew, 2007; Gunn et al., 2016; Hobbie et al., 2016; Zelcer et al., 2010). Control is not an abstract concept of keeping one’s life in order. In the study in which it features it is control with a specific purpose: to bring about those things in one’s life which constitute a normal life under circumstances changed by cancer—a new normal (Chou & Hunter, 2009).
We propose then that QoL is something which BT survivors experience in the process of, during the activity of realizing a newly normal life. It is something they experience as a result of the actions which they take. What this indicates that (new) normalcy is not a “static” property as an object’s being of a certain size, shape, or color. Experiencing a measure of (new) normalcy is an achievement which needs to be constantly repeated. Because normalcy is something which applies to one’s life because of activity, we present the concepts of (new) normalcy and control as a dyad.
Line of Argument: A Conceptual Model of QoL as Striving for a New Normal
Three further concepts emerge from our studies: resilience, physical function, and change. These are not components or dimensions of QoL, of what that means to CYP but they nevertheless have fundamental relations to QoL and how that achievement comes about. These three play different roles than do the first six (normalcy, control, independence, social functioning, future, and success) and can be fitted with them to form the beginning of a model in which our concept of QoL is situated.
Change is a fundamental aspect of survivors’ experience and is the context within which they seek and achieve a new normalcy. They experience a changed body and changed relationships. Changes in physical functioning—basic physical abilities and cognitive function—are key elements in this context of change. Again, these are not items which can be straightforwardly measured and compared between individual survivors. These affect survivors’ QoL as they are experienced and interpreted by the individual. Thus, what an external observer might call the same change or degree of change can be interpreted differently by different individuals and thus have a different impact on QoL.
Physical functioning (including neurocognitive impairments) is thus not a part of survivors’ QoL concept, but is something to which BT survivors adapt. It can be seen as something which pushes back against, offers resistance to the control element. These elements are all set against the arena of “change.” All studies reported that CYP with BTs go through some form of change, internal (e.g., physically, emotionally) and external (e.g., in the home, educationally), and this changed life is the context within which CYP strive to achieve a new normalcy. So set against this arena of change the central concept of QoL can be seen to be this idea of “new normal,” striving for a new type of normalcy (Figure 2).
Model of quality of life.
Resilience is something all CYP have in differing degrees and can be seen as influencing the amount of control a CYP has to achieve normalcy. It reflects survivor’s ability to adapt to change and interpret changes in function in a way which allows them to be integrated into a new normal.
Discussion
Key Findings
This review explores the concept of QoL in CYP with BTs from the perspective of two of the stakeholders in decision making about care and treatment. Meta-ethnography is used to synthesize the six studies identified as presenting findings relevant to a concept of QoL in CYP with BTs from a stakeholder perspective. Striving for a new normal is the core concept to come from the synthesis. A related concept, control can be seen as an essentially linked process, as behavior strategically aimed at achieving normalcy. Resilience facilitates control. Elements of social relations/functioning, success, independence and a redefined future emerge as key aspects of the concept of a new normalcy. A changed functioning, which typically includes deficits in neurocognitive functioning, is something which pushes back against or offers resistance to the element of control. These elements are all set within the arena of “change,” a life changed by cancer.
Our Findings and Previous Literature
Previous studies of CYP and families experience with cancer have found striving for normalcy and the establishment of a new normal as a key component of living with and after cancer and chronic illness. Clarke-Steffen (1997) find that life with and after cancer was different but assumed a quality of normality. Parents and CYP had a new “world view.” Stewart (2003) in a study of younger (preadolescent) children undergoing treatment for cancer found that they viewed their lives as routine and ordinary. In reviewing literature on the concept of normalization, Deatrick, Knafl, and Murphy-Moore (1999) report that in normalization, change, and impairment are acknowledged. Normalization, they say, involves both cognitive (definitional) and behavioral (strategies) process and that these two aspects are “inextricably linked.” Taylor, Gibson, and Franck (2008) find that “Young people with a chronic illness strove to overcome social, psychological and physical difficulties to have a normal life” (p. 1828). Earle, Clarke, Eiser, and Sheppard (2007) find that the mothers of CYP with acute lymphoblastic leukemia in their study were all striving to achieve a normal life and had to adjust to a new normal since the diagnosis. Van Schoors et al. (2018) also found families with a CYP with leukemia (or non-Hodgkin lymphoma) were striving for normalcy. In a study of children with developmental delay and cognitive impairment but from illnesses other than cancer, Rehm and Bradley (2005) find that some parents rejected the description of their lives as normal in recognition of the differences in their lives from those of normal families to which they compared themselves and in which there was no illness. Other families characterized their lives as a “crazy normal” or said they were “normal but . . . .”
What this review shows is that achieving this combination of redefinition and normalizing practices brings a sense of quality into the lives of YP and, we suspect, their families as well. QoL is something which results from a combination of cognitive, or meaning making, and behavioral strategies but is not identifiable with these individually. As Deatrick et al. (1999) write “No one attribute can be considered without viewing its context and the attributes as a set. While attempting to clarify the conceptual foundation of normalization, defining attributes are necessarily reductionistic” (p. 213).
In a study published prior to the dates of our search, Hinds et al. (2004) propose a definition of QoL for CYP with cancer based upon interviews with CYP. They define QoL as “an overall sense of well-being based on being able to participate in usual activities; to interact with others and feel cared about; to cope with uncomfortable physical, emotional, and cognitive reactions; and to find meaning in the illness experience” (p. 767). Comparison with our proposed concept (survivors’ concept) is useful and brings to light some basic issues encountered in efforts to define or conceptualize QoL for CYP with cancer and with BTs in particular.
Both our concept and Hinds’ are holistic. Hinds et al. (2004) builds on an overall perception of the CYP’s life; our concept relies upon the YPs overall characterization of their life as normal in a form reassessed post illness. An interesting point of difference is that symptoms and physical function do form a part of Hinds’ concept of QoL whereas from our concept they are part of the model but not of the concept per se. Significantly, in Hinds’ concept the impact of symptoms and function is mediated through the YPs ability to cope with these changes in the YPs life. Thus, on both views the impact of physical changes is not direct, and do not lead inevitably to a decreased QoL. Furthermore, by featuring adaptation, or in our case resilience as well, both concepts allow for positive gains after or during an experience with cancer.
In making this comparison, it is important to note that Hinds et al. (2004) observe that a limitation of their definition is that it is based solely upon views of CYP currently receiving treatment and included no long-term survivors. Our study suffers from a similar type of limitation but in precisely the opposite direction: it is weighted toward the views of survivors.
From the Concept of QoL to Measurement
Good measures of QoL, in addition to having sound psychometric properties, need to reflect issues which are important to YP and families (Eiser, 2004; Hinds, 2010). Despite this agreement in the literature that a need for normality is what families want and how they understand well-being, measures of QoL do not feature normalcy and achievements. Instead they measure deficits in several domains. As Haase et al. (1999) stress, this is a limited way of assessing QoL and without assessing the meaning for the individual CYP. No measure focuses on how far they can live their normal everyday life. The European Quality of Life-5 Dimensions (EQ5D; The EuroQol Group, 1990) approaches this with a domain of how able a patient is able to undertake their “usual activities” be it school, study, or work and the Child Health Utility instrument (CHU9D; Stevens, 2009) with the domain “able to join in activities” but these are one of many domains in the measures.
Our review stresses the primacy of social relationships in achieving normalcy and by inference a good QoL. Hobbie et al. (2016) stress how the importance of families went beyond the resources, structure, and support of their emotional, physical (etc.) functioning and “provided the recognition that they were important beings and their existence mattered to someone” (p. 140, but also featuring in the abstract). They describe the family as a “looking glass,” which enabled survivors to define themselves and enjoy a positive sense of self. Instruments which are sensitive to the concerns of YP and families need to address these aspects of CYP’s concept of QoL.
Different Agendas
It is important to keep in mind that different approaches to QoL, qualitative approaches exploring individual’s appraisal of their QoL versus quantitative approaches using instruments, typically have different purposes. Qualitative studies are important for HCP in their clinical interactions with BT patients and families. Many quantitative studies of QoL are conducted to document a need for continued support for BT survivors. To justify support services, these services need to have measurable impact. Haase et al. (1999) talk of the “pressing need to measure HRQoL as an outcome for children and adolescents” while at the same time they recognize that this “seems to be leading to an acceptance of function-based models without a critical evaluation of the underlying assumptions for both function and meaning as the basis for HRQoL assessment” (p. 125).
This review was undertaken, by contrast, to understand how participants in clinical decision making might understand and use the concept of QoL in those discussions. We are not focused on issues of defining needs for a population and measuring change in QoL over time.
Strengths and Limitations
Although we feel confident about our application of the principles of translational, meta-ethnographic, synthesis to the studies reviewed, we are nevertheless aware of a number of ways in which our results, conclusions, and hypotheses should be qualified. As with any review our results are limited by what was returned by the search. Our search yielded nothing on clinicians’ understanding of or use of the idea of QoL and virtually nothing about parents’.
Each study is from a different country with varying health care systems; one was from a non-Western country. Nevertheless, there was no opportunity to explore the possible impact of social factors at a macro level on understandings of QoL. Such differences may exist within Europe. Radiotherapy is devastating to a young, developing brain. Guidelines about the minimum age at which it should be used vary across different countries in Europe. In the United Kingdom, radiotherapy is avoided in cases of children below 3 years of age. In France, the recommendation is that be avoided until 5 years of age. There is some speculation that this reflects societal attitudes toward disability.
Our approach to these studies has been interactionist, a more microsociological approach, and focused on BT survivors interacting with family and friends to create a new normal life. We recognize that social actors do not create social life ex nihilo. Our analysis can be complemented by analysis from other perspectives, by showing how larger scale social factors influence and support this interactional reality.
Samples in the studies reviewed were purposive or convenience samples; rates of participation of eligible subjects, when they could be calculated (four studies) ranged from 48% to 32%. We cannot know the reasons why a substantial number of eligible participants either refused to participate or simply neglected to do so and whether these decisions or events had an impact on our “data.” It is possible that those most severely affected by treatment for BT more often chose not to participate than other survivors.
We also lack demographic information on participants. Economic resources of the families might affect on the ability of survivors to adapt in these challenging circumstances.
Reporting on the treatment stage of the CYP is a critical component of analyzing a CYP’s experience yet it is regularly ignored in research (Taylor et al., 2008). QoL is dynamic and likely dependent on where in the illness trajectory the CYP is. Hinds (2010) stresses that QoL can vary as severity of treatment changes and continue to do after treatment ends. Our small cohort of studies is composed largely of survivors (213 of the 243 total subjects) some years after diagnosis/treatment. Only Darcy et al. (2014) had CYP participants undergoing active treatment, although nothing they found there conflicted with the other studies. Exploring the concept of QoL of CYP’s who are undergoing active treatment is an area that warrants further investigation.
Conclusion
The clear finding of this review is that BT survivors’ understanding of QoL is based upon adaptation to their changed circumstances. This stands in contrast to a deficit approach to QoL which is typically found in QoL scales and measures. How might the differences between the two approaches be resolved? Should one or the other be regarded as the better understanding of QoL? What are the possible consequences and implications of this difference for CYP with BTs?
Decisions about interventions and treatment protocols may be being made for this population by clinicians and researchers, relying upon deficit-based instruments, whose assessment of the QoL of BT patients and survivors may differ from those of the patients themselves and of their families. Researchers may regard proposed new therapies as resulting in a low HRQoL but patients and families might judge the outcomes to be acceptable. This could slow progress in improving outcomes-survival for BT patients. But, allowing therapies with a higher burden of long-term effects places a new burden on parents and CYP as decision makers. To take such risks, decision makers must clearly envision what survival would be like and what their ability to adapt to and enjoy such a life would actually be. This is something which CYP and their families must do in a context, which is emotionally charged and often beset by uncertainty. As noted above, the understanding of QoL developed here may not reflect the experiences of survivors who have suffered the greatest neurocognitive damage.
One of the uses of deficit-based HRQoL instruments is to document the need for long-term surveillance of BT survivors and the provision of support services. The findings in this review could be taken as presenting advocates for survivors with a dilemma of either renaming their instruments as health status scales or relying more heavily on patient and family subjective assessment of their QoL. However, separating their instruments from the idea of QoL risks making their petitions to policy makers and commissioners for services for BT survivors seem less compelling, about something less important, especially if it is thought that survivors and their families assess their QoL as at least acceptable.
At the same time, it needs to be recognized that while deficit-based instruments may be effective in securing support for BT survivors, they may not be well suited to planning and guiding the services which survivors actually want and need. The adaptive concept of QoL presented here may be better for those tasks. BT survivors find QoL within the milieu which they create with other members of their family. Services need to support this unique unit. Assessments of needs based on external and universal criteria may not be suitable for doing this.
Health-related quality of life (HRQoL) measures have and will continue to have an important role in the lives of BT patients and survivors. Perhaps one outcome of this brief discussion is that it needs to be kept in mind that quantitative measures are instruments, means to ends and not normative judgments.
Clinical Implications
In decision making, support must be provided to clinicians to discuss QoL in understandable terms and whose meaning is shared by CYP and families. Perhaps rather than fixing on the term QoL, clinicians should ask what is important to CYP and their parents and what are their long-term goals.
Clinicians dealing with CYP and families who are undergoing or have completed therapy should be aware of families’ struggle to contain the intrusion of the illness and to maintain normalcy as far as possible. They need to accept that normality and independence are subjective notions and mean different things to different people, CYP and their parents. Excessive emphasis on health status and physical functioning can lead to a neglect of patients’ and families’ understanding of QoL.
Care and service planning should be guided at least as much by what is learned from explorations of the social and subjective dimensions of survivors’ QoL as from studies of the deficits revealed by the application of HRQoL instruments.
Directions for Future Research
This study highlights how little is known about the individual stakeholders’ concepts and understandings of QoL. This is the case even though the terms are often used in clinical consultations in which decisions about care and treatment of YP are made. It is crucial to investigate how different stakeholders in the clinical consultation understand QoL if there is to be clear and meaningful communication between them.
Clinicians are trained to assess patients objectively typically using standardized quantitative instruments. Hence, one might suspect that they place great emphasis on health status and physical function in thinking about QoL, not just HRQoL. We need to determine whether this is the case and what its consequences might be for interacting with CYP and families, and on decision making.
Parents’ understandings of QoL are just as important. Many BTs occur in children below 5 years of age and so have a very limited role in decision making. In such cases, parents become the primary decision makers together with the clinician.
There is a need for an ethnographic longitudinal study that follows families in consultations throughout their illness trajectory to understand what they mean, when QoL is discussed in these consultations. We need to see what is important to CYP and their families and how this changes over time and as the disease changes. Only then will we begin to understand how each of the three stakeholders conceptualizes QoL and how it functions in clinical decision making. This is as essential for designing effective interventions to improve the lives of CYP with BTs as is looking at it from a deficits perspective.
Supplemental Material
QOL_PHD-SYS_REVIEW-Medline_search – Supplemental material for Children’s and Parents’ Conceptualization of Quality of Life in Children With Brain Tumors: A Meta-Ethnographic Exploration
Supplemental material, QOL_PHD-SYS_REVIEW-Medline_search for Children’s and Parents’ Conceptualization of Quality of Life in Children With Brain Tumors: A Meta-Ethnographic Exploration by Emma Beecham, Richard Langner, Darren Hargrave and Myra Bluebond-Langner in Qualitative Health Research
Footnotes
Acknowledgements
The authors would like to thank Dr. Jane Harrington for her help with the quality assessment and screening and Dr. Ellen Henderson and Dr. Gemma Bryan with their help with the screening.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: E.B.’s post is funded by Marie Curie Cancer Care (MCCC-FCO-11-U). D.H.’s post is funded by GOSH Children’s Charity and the National Institute for Health Research Biomedical Research Centre at Great Ormond Street Hospital for Children NHS Foundation Trust and University College London. MB-L’s post is funded by the True Colour’s Trust. This research was supported by The Health Foundation and the NIHR Great Ormond Street Hospital Biomedical Research Centre. The views expressed are those of the author(s) and not necessarily those of Marie Curie Cancer Care, the Health Foundation, NHS, the NIHR or the Department of Health. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.