
Abstract
Understanding the challenges of professionals in addressing child adversity is key to improving the detection, protection, and care of exposed children. We aimed to synthesize findings from qualitative studies of professionals’ lived experience of addressing child adversity. Through a systematic search, we identified eight qualitative studies and synthesized them using metaethnography. We generated three themes, “feeling inadequate,” “fear of making it worse,” and “facing evil,” and one overarching metaphor, “walking children through a minefield.” The professionals felt that they lacked the means necessary to explore child adversity, that they were apprehensive of worsening the child’s situation, and that their work with child adversity induced emotional discomfort. This metasynthesis indicated that the professionals’ efficiency in exploring abuse relied upon their ability to manage emotional and moral distress and complexity. To support children at risk, we propose developing professionals’ ability to build relationships, skills in emotion regulation, and proficiency in reflective practice.
Keywords
Introduction
Over the last two decades, a large body of multidisciplinary research has been conducted to document the prevalence and long-term effect of adverse childhood experiences (ACEs), including psychological, physical, or sexual abuse; violence against mothers; or living with household members who were substance abusers, mentally ill or suicidal, or ever imprisoned (Felitti et al., 1998). The findings have revealed that ACEs are a common pathway to social, cognitive, and emotional impairments, leading to an increased risk of unhealthy behaviors, violence, physical and psychological disease, disability, and premature mortality (Van Niel, Pachter, Wade, Felitti, & Stein, 2014). The prevalence of adverse and potentially traumatizing events in childhood appears to be high in Europe and the United States (Finkelhor, Turner, Shattuck, & Hamby, 2013; Janson, Jernbro, & Långberg, 2011; Thoresen, Myhre, Wentzel-Larsen, Aakvaag, & Hjemdal, 2015).
The early identification of ACEs and intervention with children may produce stronger effects than attempting to modify health-related behaviors or provide health care in adulthood (Anda, Butchart, Felitti, & Brown, 2010). Still, it appears that few of the children exposed to ACEs who have developed ongoing distress receive effective treatments (La Greca et al., 2009; Steinberg et al., 2014). Furthermore, we need to identify and address children’s adversities to be able to reduce their exposure to stressors and/or to diminish the biological effects of stressors. Therefore, a major contributing factor to our failure in helping abused children may be that professional caregiving for these children rarely includes routine exploration of traumatic exposure (Blount et al., 2008; Cameron & Guterman, 2006; Reigstad, Jørgensen, & Wichstrøm, 2006).
Professionals’ inadequacy in disclosing child adversity may be related both to the professional as an individual and to the norms and practices of institutions and programs. Taylor, Daniel and Scott (2012) concludes in a review of quantitative research that there is sufficient evidence on the identification of, and response to, neglected children to guide practice. Despite this evidence, professionals’ willingness to explore and identify childhood adversity seems limited. This finding raises the question of what contributes to the reluctance of practitioners to explore psychological trauma with children. Plitz and Wachtels’s (2009) review of quantitative research found nurses’ identification and reporting of suspected child adversity to be dependent on individual factors such as knowledge, experience, fear of perceived consequences, lack of emotional support, and low opinion of child protective services (CPS). To recognize why today’s competence is inadequate and to enable future interventions to efficiently alter practice, we need to increase our comprehension of professionals’ experiential world. To our knowledge, no metasynthesis exists on this subject. Thus, we aimed to synthesize qualitative studies of professionals’ lived experience of addressing child adversity. Professionals’ lived experience includes screening, assessment, identification, and reporting behaviors, as well as intrapersonal (e.g., attitudes, values, beliefs, knowledge, and biases) and contextual factors. We anticipate that the findings will guide improvements in professional practice.
Method
Sandelowski (2012) defined qualitative metasynthesis as a form of scientific inquiry in which research findings in completed qualitative studies are summed up or integrated to make them more applicable to inform practice, policy, or future research. The main purpose is to compare, contrast, translate into each other, and synthesize empirical, qualitative findings from individual studies to gain new insight, overarching meaning, and a deeper understanding of a topic; this process avoids the possibility that these studies remain isolated pieces of a large puzzle (Zimmer, 2006). Noblit and Hare’s (1988) metaethnographic comparative method is the most frequently applied metasynthesis method in health care sciences, allowing us to interpret qualitative findings from diverse settings and cultures into higher order understanding. We applied this method and followed its seven recommended steps: isolate a research question to explore with qualitative data; identify relevant studies through literature review; read the studies thoroughly; find how the studies are interrelated; translate the studies into each other and extract overarching themes; synthesize translations; and communicate findings.
Search Strategy and Inclusion Criteria
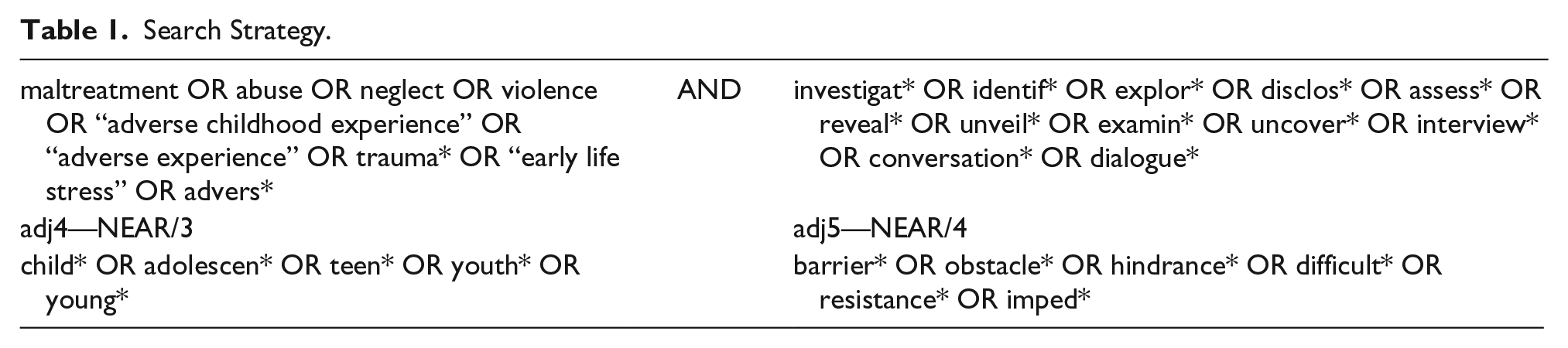
We chose to include peer-reviewed, empirical, qualitative studies that examined professionals’ experiences addressing ACEs in interviews with children and adolescents published in English or Norwegian. Due to the sparse number of records available, we chose to include all established qualitative methods studying all groups of professionals who work with children and adolescents’ health and well-being. We developed a search strategy outlined in Table 1 with guidance from an expert academic librarian and searched the following databases through January 2015: PsychInfo, Medline, Embase, Web of Science, and ProQuest (11 databases, including ERIC).
Search Strategy.
The initial search resulted in 904 records after duplication removal in EndNote. We conducted a supplementary hand search, including a search in the Norwegian databases IDUNN and NORART, and in the reference list of relevant articles, resulting in seven potential articles. Finally, we found two more articles through contact with experts at the 9th Nordic Conference on Child Abuse and Neglect in Stockholm. To counteract the risks of researcher bias and of overlooking studies, we avoided having an a priori theoretical framework guiding our search and practiced reflexivity. Supplemental Figure 1 outlines the search process.
The screening process was carried out in four phases primarily performed by Albaek. An initial screening based on the title for concurrence with inclusion criteria reduced the records from 904 to 203. Next, reading the abstract reduced the number of possibly relevant records to 76. We then read the full text of the remaining 76 records, along with the seven records identified by the hand search and the two records identified by expert contact. In cases of doubt, all authors read the article and discussed its fit with the inclusion criteria. Finally, we scrutinized the final cut of articles together to ensure agreement and ended up with eight studies.
Quality Assessment
We opted not to apply appraisal checklists to assess the quality of the articles partly due to the controversy regarding the use of rule-based judgments in qualitative research in general (Barbour & Barbour, 2003) and partly due to the vast amount of proposals for quality checklists that reveal several incompatible positions (Dixon-Woods, Shaw, Agarwal, & Smith, 2004). Instead, we checked the relevance and proficiency of the articles with two screening questions suggested by Campbell et al. (2003): “Does the article report findings of qualitative research involving qualitative methods of data collection and analysis and are the results supported by the participants’ quotes?” and “Is the focus of the article suited to the synthesis topic?” (p. 674). Through this process, we excluded four articles, although we kept two articles only partly compatible with the requirements (i.e., they lacked participants’ quotes), as the findings were relevant and applicable. We discovered no major methodological or ethical flaws in the final sample of articles.
Sample
We have summarized the main attributes of the included studies in Table 2. Three studies were conducted in the United States; two, in the Netherlands; two, in Sweden (these were based on the same data material and informants); and one, in Great Britain. Six articles were published in medical or health journals, and two articles were published in thematic journals on abuse. The data collection methods used in these studies included in-depth and semistructured interviews (three studies), semistructured focus-group interviews (three studies), questionnaire with open-ended questions combined with in-depth interviews (one study), and small group seminars with open-ended questions and case discussions (one study). All studies covered responses from 172 professionals, including men and women, with varying work experience and different levels of education. Only some of the studies listed gender; hence, we could not quantify gender distribution. The professionals worked with children or adolescents in physical health care (four studies), school nursing (two studies), CPS (one study), and counseling (one study).
Main Attributes of the Included Studies.
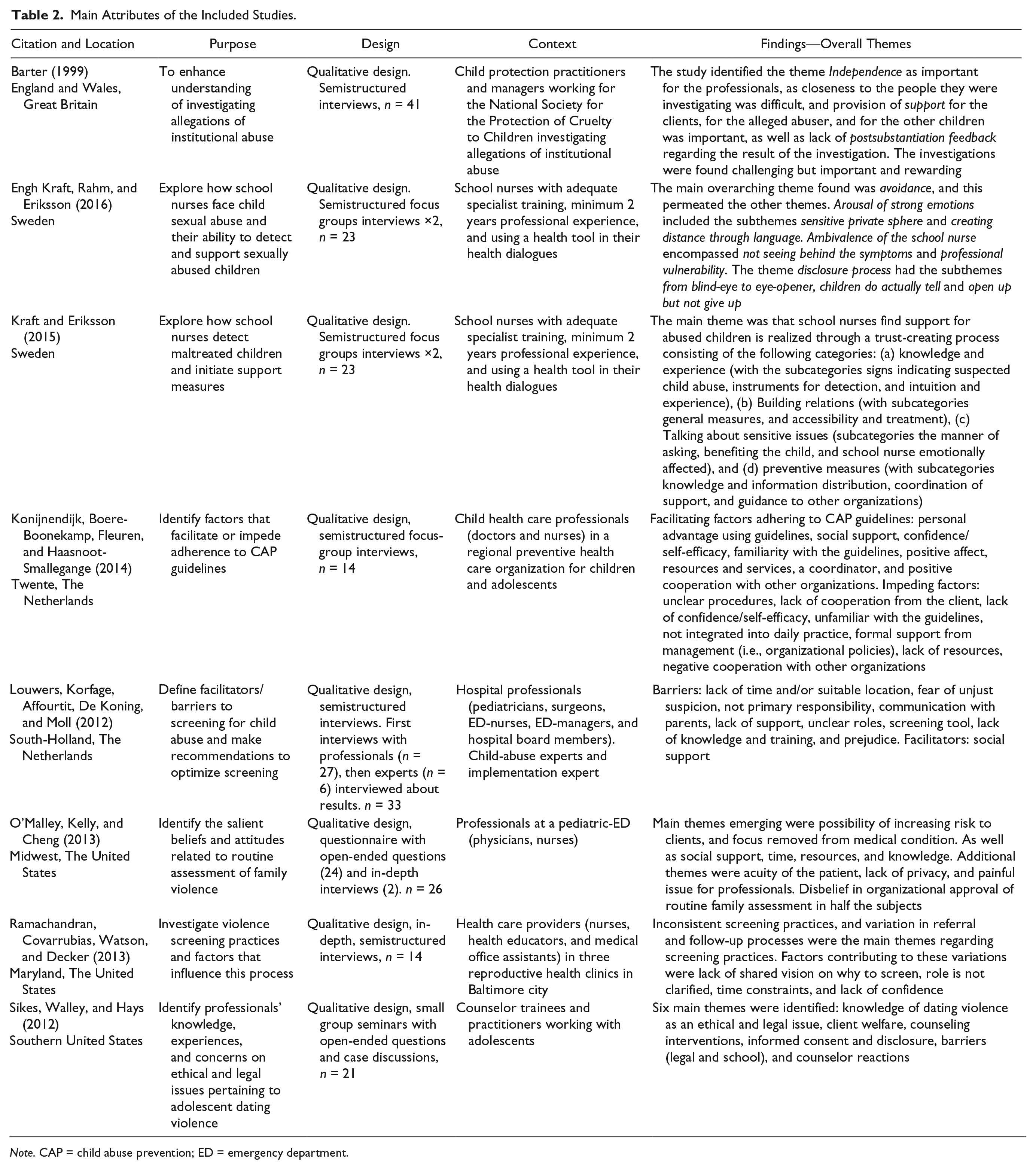
Note. CAP = child abuse prevention; ED = emergency department.
Researchers
Albaek is an organizational psychologist and is experienced in competence development for professionals in social and health services, with specialisation in psychological trauma. Kinn is an associate professor in occupational therapy and has published research on vocational rehabilitation for people with severe mental illness in international journals. Milde is an associate professor in biological and medical psychology and a specialist in clinical psychology. She has published research on stress and trauma in international and Scandinavian journals.
Analysis and Synthesis
Adhering to Noblit and Hare’s (1988) method, Albaek summarized the results section of each study with metaphors and participants’ quotes and distributed this information to Kinn and Milde. Thereafter, we grouped the findings into three categories: individual factors, factors related to the ACE, and organizational factors. Next, all authors of this study participated in a creative process in which we compiled a list of the concepts, themes, and key phrases from the individual studies. We juxtaposed the themes or ideas to understand how the studies could be interrelated and searched for findings confirming each other and findings that seemed to refute each other. Our list of findings appeared to concur with each other, although they addressed different aspects of our synthesis topic. In the next phase, we therefore chose to further our analysis through reciprocal translations of the findings by principles of thematic analysis and interpretative translation. We discovered several reoccurring themes, and we used key concepts from one study and translated them into findings of the other studies to deepen our understanding of the meaning behind the themes. Three overarching categories of themes emerged through these translations: external barriers, concern for the welfare of the child, and the participants’ emotional discomfort. Finally, we conducted a line-of-argument synthesis to make inferences about the entire topic using meaningful metaphors or concepts. Through continued translation and synthesis, we developed three themes and a metaphor.
Results
We developed an overarching metaphor, “walking children through a minefield,” to create a coherent comprehension of how our three themes were interrelated. We will outline this metaphor, along with the following three themes, below: (a) “feeling inadequate,” (b) “fear of making it worse,” and (c) “facing evil.”
“Walking Children Through a Minefield”
The metaphor “walking children through a minefield” illustrates the participants’ lived experiences of addressing ACEs. We chose this metaphor because the participants felt they lacked the competence and means necessary to address child adversity, similar to maneuvering through a minefield without maps of safe routes or tools to defuse mines (i.e., feeling inadequate). Moreover, the participants feared their attempts to help could hurt the child, much like having to walk individuals into an unknown minefield and risk stepping on hidden mines (i.e., fear of making it worse). When the participants faced child adversity, they experienced emotional discomfort that induced avoidance patterns, parallel to how stepping into a minefield and risk injury would create fear and evasion (i.e., facing evil).
“Feeling Inadequate”
In all the included studies, the participants felt inadequate and unequipped to work with child adversity due to insufficient competence, organizational culture, and/or system attributes. The participants shared how they experienced a lack of agency over their practice and its outcome, which reduced their confidence in their ability to walk children through the minefield and their willingness to step into the minefield themselves. In addition, even if the participants chose to do so, they felt less optimistic about the likelihood of positive outcomes for the child.
In most studies, the participants identified sufficient competence (e.g., “knowledge,” “training,” “self-efficacy,” and “confidence”) as key to working efficiently with ACEs. The participants in two studies (Engh Kraft, Rahm, & Eriksson, 2016; Kraft & Eriksson, 2015) underlined their calls for satisfactory competence addressing child adversity; in four studies (Engh Kraft et al., 2016; Konijnendijk, Boere-Boonekamp, Haasnoot-Smallegange, & Need, 2014; Kraft & Eriksson, 2015; Louwers, Korfage, Affourtit, De Koning, & Moll, 2012), for identifying ACEs; and in six studies (Engh Kraft et al., 2016; Konijnendijk et al., 2014; Kraft & Eriksson, 2015; Louwers et al., 2012; O’Malley, Kelly, & Cheng, 2013; Ramachandran, Covarrubias, Watson, & Decker, 2013), for responding to ACEs. As a participant claimed, “You can’t just go and ask these questions without having some sort of previous knowledge. . . Otherwise it can go really wrong” (Engh Kraft et al., 2016, p. 5). This quote illustrates that many participants found it difficult to know how and when to ask children about ACEs. They believed that professionals had to possess the knowledge and specific skills to address adversity in a way that would benefit the child, and they doubted whether professionals with insufficient competence should ask about ACEs (Engh Kraft et al., 2016; Kraft & Eriksson, 2015). However, the included articles reported mixed messages about this issue. Ramachandran et al. (2013) described that some participants always asked about adversity without ruminating on how or when to ask: “Every time I see a patient, regardless of what the visit is for . . . I ask them if he or she is nice to them, and if they hit or kick or punch them, and if they feel safe” (p. 858). Differing opinions of tasks and responsibilities may explain this discrepancy. The participants in Ramachandran et al’s study (2013) perceived their job to entail screening and registering ACEs and not a responsibility for improving the child’s overall situation. As this participant said when asked how he or she followed-up on positive screens, “I don’t, unless it’s a patient that follows up with me” (Ramachandran et al., 2013, p. 858).
The participants in four studies (Engh Kraft et al., 2016; Konijnendijk et al., 2014; Kraft & Eriksson, 2015; Louwers et al., 2012) found it difficult to identify child adversity, as they had to interpret the child’s signs with ingenuity. One participant explained, “It is not easy to see. You have to develop spectacles to see. Extremely hard” (Engh Kraft et al., 2016, p. 5). The participants underscored how intuition and relational skills were essential to recognizing ACEs. Although experience could refine these skills, the participants believed that the professional’s intentions and ethics were the ultimate origin of proficiency in recognizing child adversity. As said by one participant, “What we say is part of our profession. How we should act comes from within us” (Kraft & Eriksson, 2015, p. 356). This quote shows how the participants felt that their actions defined them and their worth as professionals and fellowmen. Therefore, these participants invested more into identifying adversity and helping children than the participants who limited their duties to asking about ACEs.
The participants in six studies (Engh Kraft et al., 2016; Konijnendijk et al., 2014; Kraft & Eriksson, 2015; Louwers et al., 2012; O’Malley et al., 2013; Ramachandran et al., 2013) felt inadequate and insecure, as they did not know how to respond to a child’s disclosure. As expressed by one participant, “. . . But then someone says yes and then you’re like, oh no, because now I really have no idea what to do with them” (Ramachandran et al., 2013, p. 860). These participants felt insecure about how to act in the interview setting and how to respond with supportive measures, both of which made the participants question whether a walk into the minefield would be worthwhile. One participant described not knowing how to respond after losing their on-site social worker: “When I do see a patient, we’re supposed to ask them, have they experienced any violence, or so and so . . . but no one has said yes, so I haven’t been forced to figure out what we’re going to do” (Ramachandran et al., 2013, p. 858). As shown in this quote, the participant felt ambiguous toward screening with no plan for a positive response, and the ambiguity conveyed may account for the lack of disclosure from patients.
In all studies, the participants felt frustrated and inadequate due to system failure, as shown in this participant’s complaint: “On many, many occasions, the child’s anxiety landed in our lap” (Kraft & Eriksson, 2015, p. 357). After a child’s disclosure, the participant felt as if she were left alone with a scared and hurt child without any support measures to offer. Such incidents tended to discourage the participants from reporting ACEs and sometimes from even screening: “Naturally, I should have reported my concern to the CPS but the question is what they would have achieved” (Engh Kraft et al., 2016, p. 6). Deficient cooperation with the legal system and/or CPS made the participants feel incapable and upset to see children treated unfairly:
. . . It doesn’t seem that the law—this is the legal side—it doesn’t seem like they do much about it. But you have to report it a number of times, before they step in. And I don’t think that’s fair. (Sikes, Walley, & Hays, 2012, p. 1483)
In five studies (Konijnendijk et al., 2014; Kraft & Eriksson, 2015; Louwers et al., 2012; O’Malley et al., 2013; Ramachandran et al., 2013), the participants thought organizational culture influenced their ACE exploration in the form of insufficient guidelines, unclear roles and responsibilities, lack of social support, and disagreement about the screening tool. The participants in all studies requested clearer guidelines and better assessment tools to handle their uncertainty in working with child adversity. Although, in one study, the participants handled doubt with experience-based intuition: “My years of service and experience mean that I am not so scared anymore but I feel that I can rely on my gut feeling” (Engh Kraft et al., 2016, p. 6).
In three studies (Louwers et al., 2012; O’Malley et al., 2013; Ramachandran et al., 2013), the participants did not think it was their primary objective or responsibility to screen for ACEs, as exemplified by this quote: “We’re too busy with STDs (sexually transmitted diseases)” (Ramachandran et al., 2013, p. 857). Similarly, two studies reported that the participants perceived unclear roles and division of labor, which hindered their exploration of ACEs (Louwers et al., 2012; Ramachandran et al., 2013). Quotes from two participant colleagues may be illustrative: “I would say that clinicians would be able to identify it a little bit better. . . ” and “[screening] is a social work issue” (Ramachandran et al., 2013, p. 859). Due to their feelings of inadequacy, the participants seemed to think that other professions were more skilled to detect ACEs.
In all studies, the participants felt challenged by insufficient system attributes important for their practice and its outcomes, such as time, resources, workload, support measures for the child, and cooperation with CPS and legal authorities. Moreover, in five studies (Engh Kraft et al., 2016; Kraft & Eriksson, 2015; Louwers et al., 2012; O’Malley et al., 2013; Ramachandran et al., 2013), the participants experienced a heavy workload and/or a lack of time, which impeded ACE screening. One participant shared how addressing ACEs required difficult priorities:
I hate opening up a door to someone and then being like I am not going to deal with it… unfortunately, when you’re really busy, knowing that, you know, a certain conversation could make this an hour long visit, and you have three more people on your door. . . (Ramachandran et al., 2013, p. 860)
This quote exemplifies that the participants could choose not to enquire if they felt unable to respond properly to disclosure. Otherwise, exploring ACEs would come at the expense of other clients. With a lack of time requiring harsh prioritization, the participants felt inadequate, powerless, and guilty: “. . . we just can’t save everyone. You can’t get involved in any case” (Engh Kraft et al., 2016, p. 6).
“Fear of Making It Worse”
This theme captures the participants’ fear of taking a child into the minefield where they could trigger a mine and hurt the child. As the participants felt unable to predict the consequences of their actions, they felt anxious that their attempts to help would make the child’s situation worse (Engh Kraft et al., 2016; Kraft & Eriksson, 2015; O’Malley et al., 2013; Sikes et al., 2012).
The participants were afraid of making it worse for several reasons. First, they were scared of inflicting harm upon the child by causing fear, as illustrated in this quote: “The pupil had been so scared and said ‘I don’t know where I am going after school, whether I can go home or not’. . . Threats are so awful. . . ” (Kraft & Eriksson, 2015, p. 357). The participants were also afraid of exposing the child to added abuse, as explained by this participant: “You could inadvertently trigger violence if the abuser finds out about the disclosure” (O’Malley et al., 2013, p. 276). Second, the participants expressed worry that interviewing a child about ACEs could introduce new hardships into the child’s life. These hardships included ruptured relationships within the child’s family (O’Malley et al., 2013), unjustified suspicions posed to parents or legal authorities (Louwers et al., 2012), or the parents could deny the child further contact with the professional (Engh Kraft et al., 2016). Third, the participants in all studies doubted they had sufficient resources to help the child: “If we ask about abuse but then are not able to do much when the answer is yes, things could get much worse at home” (O’Malley et al., 2013, p. 276). Implicitly, the participants’ stories embedded their fears of entering an unchartered minefield, in which they could never trust that their actions would be beneficial or at least not harmful.
In three studies (Engh Kraft et al., 2016; Kraft & Eriksson, 2015; Sikes et al., 2012), the participants described how revealing ACEs could catch them in a dilemma between different ethical and legal standards. An example from Kraft and Eriksson’s study (2015) is the contradiction between upholding client confidentiality and their legal obligation to report uncovered ACEs. Given no correct answer, any action would breach one set of ethics. Moreover, when the participants could not help a child after reporting ACEs, they felt they had deceived the child and given false hope, as revealed by one professional:
. . . if someone came and they were in a relationship of violence or something, and they trusted us to do something about it . . . in a way they might feel you are betraying their trust because you have to report it. So you do that, and then it’s like, if nothing happens, you’ve just betrayed their trust and nothing happened. (Sikes et al., 2012, p. 1481)
The next quote shows how unpredictability caused the participants to feel caught in a “catch-22” situation: “This is something you always bear in mind when you start something. How will it benefit the child? However, there is no other way. . . All the same, you look at the pros and cons” (Kraft & Eriksson, 2015, p. 357). If the participants chose not to explore ACEs, they could not initiate any support measures. In contrast, if the participants addressed and reported ACEs and could not protect the child, the participants risked losing the child’s trust and exposing the child to more danger.
In five studies, participants doubted if they should lead the child into the minefield if they were unsure they could walk the child to safety (Barter, 1999; Engh Kraft et al., 2016; O’Malley et al., 2013; Ramachandran et al., 2013; Sikes et al., 2012). One professional explained the situation as follows: “You can’t just give child abuse or domestic violence a prescription and make it better; you can’t scan it away, radiate away, so they won’t ask” (O’Malley et al., 2013, p. 277).
Interestingly, in one study, the participants claimed that they always explored what they interpreted as “obvious signs of child abuse” (Kraft & Eriksson, 2015, p. 357). Another study reported that participants had low self-efficacy when they based their suspicion of ACEs on vague and ambiguous signals (Konijnendijk et al., 2014). It seems that the participants were more willing to walk the child through the minefield if they felt certain that a child was a victim.
The participants in all studies searched for ways to increase the predictability of their actions and reduce their fear of making it worse. In addition to improved competence, the participants requested follow-up information after reporting to CPS in three studies (Barter, 1999; Konijnendijk et al., 2014; Kraft & Eriksson, 2015). Information about outcomes of their actions could help the participants maneuver through a similar minefield in the future. Moreover, the participants in three studies (Engh Kraft et al., 2016; Konijnendijk et al., 2014; Kraft & Eriksson, 2015) believed that accumulating experience with ACEs would help them overcome self-doubt and fear. As one professional explained, “. . . then you will become increasingly skillful and tend to experience less fear of making poor decisions” (Konijnendijk et al., 2014, p. 421).
“Facing Evil”
In all included studies, the participants described how facing potential child adversity (facing evil) induced emotional discomfort, such as frustration, despair, anger, guilt, and shame. The participants’ reactions to the emotional distress of facing evil evoked several types of avoidance patterns on varying levels of cognitive awareness: suppression, avoidance of talking about it, disbelief, and fear of negative reactions.
The participants displayed the effects of facing evil with their emotional reactions to the horrors of child adversity, as illustrated in this quote: “It is such a taboo area. It is so awful if it is true” (Engh Kraft et al., 2016, p. 4). In two studies (Engh Kraft et al., 2016; Kraft & Eriksson, 2015), the participants shared how these reactions also made it challenging to suspect someone of child abuse: “Thinking of someone in these terms is very harsh” (Engh Kraft et al., 2016, p. 4).
In Engh-Kraft et al.’s study (2016), the participants initially suppressed their recall of their experiences with sexual-abuse cases: “I had completely forgotten about it. I have even been to the district court as a witness” (p. 5). As this quote shows, the participants kept painful experiences of facing evil away from their everyday awareness. Another participant explained it in this way: “We who are right on the edge push it (child abuse) to the back of our minds because it is unpleasant” (p. 6).
The participants in four studies (Barter, 1999; Engh Kraft et al., 2016; Kraft & Eriksson, 2015; Louwers et al., 2012) expressed how talking about ACEs was emotionally challenging, as described by one participant: “It is extremely difficult to ask about abuse. It really is” (Engh Kraft et al., 2016, p. 4). They tended to avoid talking about abuse, and if they did, they created distance through language (Engh Kraft et al., 2016). For instance, they would use vague terms and periphrases, as exemplified by this quote: “It wasn’t consummated then, but in another way. I don’t want to. Ugh, it’s tough talking about what had happened in detail. But it was then, you know” (Engh Kraft et al., 2016, p. 4). Markedly, in four studies (Engh Kraft et al., 2016; Konijnendijk et al., 2014; Kraft & Eriksson, 2015; Ramachandran et al., 2013), the participants referred to a child’s ACEs in several ways, including “it,” “the case,” “their situation,” “that,” and “awful thing.” Moreover, the participants used circumlocutions despite their belief that children need and want direct questions. Utility of distant language could be a method for the participants to protect themselves from facing evil through objectifying adversity and detaching it from human suffering. If they failed to do so, the participants could lose control over their emotional involvement, as this participant said, “A warning sign for the counsellor may be that—you are extremely upset. Something happened to her—you’re going to have to distance yourself. Kind of transference” (Sikes et al., 2012, p. 1483).
The participants in two studies (Engh Kraft et al., 2016; Kraft & Eriksson, 2015) described how their disbelief or oblivion toward the presence of evil in their daily practice disrupted their ability to identify ACEs. This phenomenon was described by one professional as follows: “You find what you want to see, you don’t look for what this might stand for, do you? Many times, seeing it is tough, although you don’t realize you are resisting” (Engh Kraft et al., 2016, p. 6). As this quote shows, the participants had to intentionally search for ACEs and become aware of implicit personal issues preventing them from reading signs of adversity. Six studies (Barter, 1999; Engh Kraft et al., 2016; Kraft & Eriksson, 2015; O’Malley et al., 2013; Ramachandran et al., 2013; Sikes et al., 2012) mentioned such issues including preconceptions, defensive attitudes, identification with parents, avoidance, denial, and personal experiences, as exemplified in the following quote: “I think this counselor may be able to resolve their own experiences from the past, before they take on this individual” (Sikes et al., 2012, p. 1483).
The participants in six of the studies expressed fear that facing evil would expose them to negative reactions and cause emotional discomfort (Barter, 1999; Engh Kraft et al., 2016; Konijnendijk et al., 2014; Kraft & Eriksson, 2015; Louwers et al., 2012; Sikes et al., 2012), as expressed by this participant: “This mother has an aggressive boyfriend . . . When I am at the mother’s house, I hope that her boyfriend will not show up. When I mention the word CPS, they will burst with anger” (Konijnendijk et al., 2014, p. 421). In addition to dreading negative reactions from caregivers, the participants also worried about critiques from their colleagues and from the legal system, as illustrated by this quote: “You are in a stronger position when you have discussed the case with professional colleagues, and this will also give you greater legal protection if your decisions are challenged” (Konijnendijk et al., 2014, p. 421).
Even with a general perception that addressing ACEs was challenging, six studies had participants who said they often screened for abuse (Barter, 1999; Engh Kraft et al., 2016; Konijnendijk et al., 2014; Kraft & Eriksson, 2015; Ramachandran et al., 2013; Sikes et al., 2012). Some of the participants reasoned that they addressed adversity because of their commitment to help exposed children, as said by one participant: “doing what’s best for the client” (Sikes et al., 2012, p. 1480). To overcome their self-protection from emotional discomfort and choose the child’s best interest, the participants had to exert drive and courage. They believed that although screening was tough, it was necessary for helping the child, as illustrated in this quote: “. . . even when the answer is awful, you have shown you can take it” (Kraft & Eriksson, 2015, p. 357). The participants who perceived their actions to be beneficial and efficient found it meaningful and worthwhile to address adversity. Barter (1999) explained it in the following way:
Despite the fact that many participants felt these investigations were particularly challenging, they also spoke about how rewarding and important they were. For many, their involvement in these investigations was seen as a substantial contribution to the safety and protection of children. (p. 401)
Discussion
We aimed to synthesize findings from qualitative studies of professionals’ lived experiences of addressing child adversity and revealed that professionals experience emotional discomfort, fear of doing something wrong, and feelings of inadequacy when they address ACEs. In our analysis, we found an interesting discrepancy between how professionals experienced addressing ACEs and what professionals described as causes for difficulties in exploration, as well as their suggested interventions/improvements. The professionals’ experiences of exploring ACEs were categorized into the themes “facing evil” and “fear of making it worse,” referring to personal and emotional issues, whereas the professionals’ descriptions of causes for hardships in addressing adversity and requested amendments were categorized into the theme “feeling inadequate,” referring to instrumental, often organizational, issues. The professionals’ stories of work with ACEs were often emotional and personal, revolving around intrapsychic conditions and relationships with children. Still, the professionals did not ask for interventions to help them regulate emotional discomfort or strategies for handling dilemmas and uncertainty. Rather, the professionals requested guidance, knowledge, guidelines, and enhancement of external factors, such as time, workload, facilities, and role clarity. The professionals solicited knowledge about ACEs, how to ask about adversity, and the actions to perform if they revealed ACEs. With the narratives being so emotionally loaded and personal, the professionals’ expressions of causes and desired interventions seem like externalizations. Our finding is similar to Killén’s (1996) findings, in which CPS workers protected themselves from the emotional distress of working with abusive families using the mechanisms of problem displacement and simplification. In problem displacement, professionals fixated on one aspect of the situation, such as a child’s developmental delay, instead of the ongoing abuse. In our study, we found problem displacement exemplified by the professionals’ focus on inadequate external factors. In simplification, professionals protected themselves using simplified methods that were inadequate to encompass the complexity of the task. A method was more popular the more it created distance between the professionals and the emotional pain of families. We found simplification in the professionals’ desire for standardizations in form of guidelines and assessment tools, although they would be unable to capture the complexity of exploring ACEs.
The professionals described ethical and moral challenges addressing child adversity in our themes “feeling inadequate” and “fear of making it worse” and felt incapable of helping children either due to moral distress or moral dilemma. Our findings in “feeling inadequate” concur with findings from other studies showing moral distress in pediatric health care providers (Trotochaud, Coleman, Krawiecki, & McCracken, 2015), nurses (Burston & Tuckett, 2013), and social workers (Mänttäri-van der Kuip, 2016). Moral distress occurs when constraints hinder a person from performing actions he or she considers morally appropriate (Jameton, 1984). Constraints can be both individual (i.e., knowledge, skills, and confidence) and site specific (i.e., resources, workload, organizational culture, and interagency cooperation). These ideas are in line with our findings that professionals felt distressed because of unsatisfactory competence, organizational culture, and system attributes. Burston and Tuckett (2013) revealed that moral distress made nurses feel powerless and prone to inaction. Similarly, in our study, constraints made the professionals feel discouraged, and they became less inclined to address or report ACEs. In the “fear of making it worse” theme, professionals experienced moral dilemma, defined as a choice between options with differing values without a correct answer. As in the case of moral distress, we found that the professionals facing moral dilemmas experienced doubt and found it difficult to act. Both moral distress and moral dilemma have cognitive, emotional, and behavioral aspects, but the central aim and desired outcome of addressing these issues is to enable professionals to engage in moral action. The professionals in our metasynthesis requested knowledge, coaching, and improved organizational resources to facilitate their work with ACEs. Burston and Tuckett (2013) concur and suggest education and coaching to facilitate moral action, and add the need for communication practices to increase ethical awareness and relieve moral distress. Tiedje (2000) proposed that professionals need awareness of moral distress and need empowerment to believe they can make a difference to improve quality of care.
We found a discrepancy between studies in terms of findings and work role. Four studies presented more findings included in the theme “feeling inadequate,” in which the authors interviewed professionals in health polyclinics performing physical examinations (Konijnendijk et al., 2014; Louwers et al., 2012; O’Malley et al., 2013; Ramachandran et al., 2013). The other four studies included more findings encompassed in the themes “fear of making it worse” and “facing evil” and included professionals working in CPS or in counseling (Barter et al., 1999; Engh Kraft et al., 2016; Kraft & Eriksson, 2015; Sikes et al., 2012). This discrepancy could reflect a divergent primary focus in their work. Work aimed at improving children’s psychological health over time may evoke deeper emotional involvement from professionals compared with short-term work with physical examinations.
Our themes “facing evil” and “fear of making it worse” incorporate the strong negative emotions professionals experienced when working with potential child abuse, and “walking children through a minefield” illustrates the professionals’ anxiety-evoking journey. Similarly, Diamond and Allcorn (1985) outlined how events perceived as unpredictable caused anxiety in professionals. This anxiety threatened the professionals’ existence and identity and motivated them for anxiety-reducing actions, either attempting to control the environment or to control feelings. The professionals in this metasynthesis handled anxiety by trying to control environmental factors while repressing their feelings.
Diamond (2008) introduced the concept “unthought known,” defined as “unconscious thoughts and feelings as known, but not thought or communicated to oneself or others in any meaningful form” (p. 351). “Unthought known” could explain the contradiction we revealed between the professionals’ emotional accounts of addressing child abuse, and their external attribution of causes and suggested remedies. The professionals were aware of their emotional reactions, but because they suppressed their emotions, they became masked to both themselves and others. Thus, their emotional reactions were absent from their daily work discourse. An example of unthought known is the situation in which professionals suppressed recollection of their experiences with sexual-abuse cases.
Our theme “facing evil” incorporates the negative emotions evoked in professionals when working with ACEs. However, we infer that “facing evil” also includes existential challenges because recognizing people’s potential for evil-doing disturbed the professionals’ view of people as essentially good. To be able to reveal abuse, the professionals had to accept that malevolent acts exist and that the people they met could commit them. The professionals in our study felt discomfort thinking of parents as potential perpetrators. Similarly, Killén (1996) found that professionals’ overidentification with parents made them look for alternate explanations for potential abuse and minimize or ignore negative aspects of parents. Looking further into the existential dimension of “facing evil” for professionals, May (1982) proposed that seeing evil in others challenges our basic narcissism and self-worth if we lack an integrated view of human nature as both good and evil. Thus, the professionals in our study could feel like “facing evil” threatened their basic self-worth and explain the emotional distress and avoidance they exhibited. Zimbardo (2007) agreed we must accept human nature as prone to evil as most people are capable of inflicting serious harm upon others under compelling circumstances. More importantly, Zimbardo stressed that awareness of human’s potential for evil and our individual choice to engage in harmful or heroic acts are the keys to fighting evil. Self-protection from the emotional distress of facing people’s potential for cruelty may have left us with professionals who struggle to accept evil as an inherent part of their work.
Implications for Practice
The professionals in this metasynthesis requested experience, counseling, knowledge, training, and guidelines to work efficiently with ACEs. Warner-Rogers, Hansen, and Spieth (1996) challenged the notion that experience with ACEs facilitates exploration of abuse and found no significant difference in abuse identification between medical students and experienced practicing physicians. Likewise, Chow et al. (2015) found that therapists’ number of years of experience was unrelated to positive client-reported outcome. The benefit of experience appears to be dependent on conditions such as the quality of experience and professionals’ learning outcomes. For instance, the professionals presented here who thought their actions had worsened a child’s situation were less inclined to repeat these actions. Ericsson, Krampe, and Tesch-Romer (1993) claimed that effortful activities (deliberate practice) and coaching lead to expert performance, and Chow et al.’s (2015) findings, where therapists with the best client outcomes spent the most time on deliberate practice, support this claim. In addition, Joyce and Showers’s (2002) review found that ongoing on-site coaching was crucial to alter job performance. In this study, many professionals believed that work experience facilitates exploration. Thus, the beneficial effect of experience could depend on deliberate practice and coaching to ensure that professionals learn from experience. Ericsson, Nandagopal, and Roring (2009) highlighted the need for immediate objective feedback on performance and outcomes at work to achieve deliberate practice, and argued such feedback often is difficult to obtain for professionals in health care and CPS. This is congruent with our finding that the professionals requested feedback on the child’s situation after their involvement and felt that lack of follow-up information was a barrier for exploration.
The professionals in this metasynthesis wanted more and improved guidelines. Koijnendijk, Boere-Boonekamp, Fleuren, Haasnoot, and Need (2016) found that child health care workers’ adherence to guidelines was low even when they viewed them positively, indicating that guidelines may not improve professionals’ screening for ACEs. This supports our conclusion that efforts to improve efficiency in ACE exploration need to address the professionals’ emotional distress and the complexity of abuse cases rather than offer simplified solutions such as guidelines and assessment tools.
We were unable to find empirical studies of interventions that increase professionals’ efficiency in exploring ACEs. Conventionally, professionals acquire theoretical knowledge on ACEs, methods/tools for exploring adversity, and guidelines for a systemic chain of action. Our findings lead us to suspect these interventions cannot resolve challenges such as emotional discomfort and complexity-induced fear of making it worse.
In this study, the professionals thought that organizational support would facilitate addressing ACEs, in the form of both social support and role clarity. Implementation studies concur with these findings, showing that to improve competence, we need enabling organizational contexts (Meyers, Durlak, & Wandersman, 2012), which entails adaptive leadership and purposeful retailoring of organizational culture, roles, structures, and functions (Fixsen, Naoom, Blase, Friedman, & Wallace, 2005). Diamond (2008) claimed that denial and repression can be part of organizational culture, where members share resistance toward unwanted realities, thus preserving the status quo. A requirement for change is therefore to acknowledge difficult issues openly, which fits with our finding that talking to colleagues about difficult issues was helpful for professionals.
This metasynthesis focused mainly on professionals’ experiences rather than organizational attributes. However, Stevens and Hassett (2007) revealed that when anxiety-evoking events occur, organizations tend to seek simplified solutions, much as professionals do. Our findings support the need to counteract anxiety-based responses from both professionals and organizations. Hence, we must move past simple linear thinking and connect factors in complex causal relations to find interventions that can improve professionals’ efficiency in addressing ACEs.
Methodological Reflections
The heterogeneity of the included studies covered diverse organizational settings and different countries, and the studies’ participants varied in professions, roles, educational level, and experience. However, the three themes and overarching metaphor of our metasynthesis emerged with little evidence of data that would refute the essence of that interpretation. We therefore believe that this diversity is a strength in terms of the transferability of results.
In qualitative analysis and synthesis, researchers engage in a creative and intuitive process of meaning-making and interpretation (Kinn, Holgersen, Ekeland, & Davidson, 2013). Naturally, these exploring and synthesizing developments are susceptible to researcher bias. Albaek and Kinn have focused on organizational and work environment in their career, and Albaek and Milde have specialized in psychological trauma. Consequently, the authors could be sensitized to reveal contextual influences and individual emotional reactions. In the analysis, we therefore took care to be as open-minded as possible and to expand our interpretations beyond our preconceptions, for instance by exploring existential challenges, relational aspects, and case complexity. In addition, we used verbatim quotations for validation, and Albaek safeguarded the intersubjectivity of interpretation by feeding the second- and third-order results back to the coauthors who confirmed the congruence with their interpretations.
Suggestions for Future Research
Based on our findings, we propose searching for effective interventions improving professionals’ emotion-regulation skills and self-awareness to advance efficiency in handling emotional discomfort. In addition, interventions improving professionals’ relationship-building and communication skills may boost their self-efficacy in addressing sensitive issues with children. Finally, we recommend exploring interventions to increase professionals’ capacity to accept and tolerate complexity and dilemmas, as well as interventions to improve their reflection skills in complex situations.
Footnotes
Authors’ Note
Ane U. Albaek is also affiliated to Department of Psychosocial Health, University of Agder, P.O. Box 422, N-4604 Kristiansand, Norway.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Figure is available for this article online.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received financial support from the Southern Norway Resource Center for Psychological Trauma.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.