
Abstract
Community-based participatory research has been seen to hold great promise by researchers aiming to bridge research and action in global health programs and practice. However, there is still much debate around whether achieving authenticity in terms of in-depth collaboration between community and academic partners is possible while pursuing academic expectations for quality. This article describes the community-based methodology for a qualitative study to explore intimate partner violence and HIV/AIDS among women in sex work, or female sex workers, and their male partners in Karnataka, South India. Developed through collaborative processes, the study methodology followed an interpretive approach to qualitative inquiry, with three key components including long-term partnerships, knowledge exchange, and orientation toward action. We then discuss lessons learned on how to pursue authenticity in terms of truly collaborative processes with inherent value that also contribute to, rather than hinder, the instrumental goal of enhancing the quality and relevance of the research outcomes.
Keywords
Introduction
Community-based participatory research (CBPR) has been gaining wider appreciation and application as part of an epistemological shift toward viewing community members and organizations as integral partners in the inquiry process (Israel, Schulz, Parker, & Becker, 1998; Rhodes, Malow, & Jolly, 2010). Common conceptualizations of CBPR emphasize the need for partnerships that are aimed toward health action, which Minkler (2005) has described as
[A] collaborative process that equitably involves all partners in the research process and recognizes the unique strengths that each brings. CBPR begins with a research topic of importance to the community with the aim of combining knowledge and action for social change to improve community health and eliminate health disparities. (Minkler, 2005, p. ii3)
In line with this definition, there are principles that many have agreed should characterize community-based research in practice, such as shared decision-making and co-ownership of the research products among partners; co-learning and reciprocal transfer of knowledge in a self-reflective manner; strengthening of research and program development capacity; and relevance to locally identified needs (Buchanan, Miller, & Wallerstein, 2007; Israel et al., 1998; Rhodes et al., 2010). As a pragmatic approach to research, CBPR aligns particularly well with interpretive forms of inquiry that employ qualitative methods to explore elements of social phenomena (Lincoln & Guba, 2000; Minkler, 2004).
Researchers have agreed that CBPR represents an overarching methodology that involves partnering with communities where research is undertaken. CBPR has roots in a variety of traditions, including Kurt Lewin’s work on action research in social psychology, and Paulo Freire’s process of conscientization that involves cycles of co-learning through dialogue on sources of oppression and structural discrimination, and action for social change. CBPR has been further adapted by feminist, post-colonialist and post-structuralist scholars who desire to give primacy to community narratives and their visions of change (Delemos, 2006; Minkler, 2005).
Past literature focused heavily on the definitions of CBPR and the important ethical considerations raised by CBPR (Buchanan et al., 2007; Campbell-Page & Shaw-Ridley, 2013; Delemos, 2006; Israel et al., 1998; Jamshidi et al., 2014; Minkler, 2004, 2005; Schaffer, 2009). There has been less attention to date devoted to understanding the organizational capacities required to support CBPR (Salimi et al., 2012), or critical considerations around the authenticity of community participation, power balances, and unexpected consequences of studies that take this approach (Elliott, Watson, & Harries, 2002; Guta, Flicker, & Roche, 2013). Some researchers have cautioned against the neutralization of CBPR’s transformative potential through its increasing uptake by more utilitarian or mainstream researchers as primarily a means of accessing knowledge on the health of marginalized groups (Guta et al., 2013; Minkler, 2004). To contribute to these discussions, first we will describe the CBPR methodology that we developed to qualitatively explore intimate partner violence (IPV) among women in sex work and their male partners in Karnataka state, South India. Then we will discuss how through these methods we aimed to enhance “authenticity” both through the processes of community-based decision-making and knowledge exchange, and in the quality of outcomes on relevant health and social issues (Delemos, 2006; Lincoln & Guba, 2000; Salimi et al., 2012; Wallerstein & Duran, 2010).
Study Background
Increasingly in public health research and programs, there is an understanding that women who sell sex, or female sex workers (FSWs), can face high degrees of different forms of violence, not only from clients or police but also from their intimate partners (Panchanadeswaran et al., 2008; Shannon & Csete, 2010; Shannon et al., 2014; Shaw & Pillai, 2012). Intimate partners of FSWs in India can include regular or long-term clients, “husbands,” non-paying partners or “lovers” who provide financial, non-monetary, or emotional support (Beattie et al., 2009; Karandikar & Próspero, 2010; Orchard, 2007; Panchanadeswaran et al., 2008; Panchanadeswaran et al., 2010). A large proportion of women in sex work in northern Karnataka, India, identify (either formally or informally), as part of the Devadasi community. Traditionally, Devadasi women have not been allowed to marry; instead, they were dedicated to a god or goddess as part of a regional socio-cultural tradition and expected to perform religious duties, including providing sexual services for temple priests (Dalrymple, 2009). Their sex work has become increasingly commercialized and covert after the Devadasi tradition was banned by the Indian government in the 1980s — policy change found to have increased stigma, socio-economic exclusion, and violence against Devadasi women, and exacerbated the HIV and other health vulnerabilities they face (Blanchard et al., 2005; Decker, McCauley, Phuengsamran, Janyam, & Silverman, 2011).
We undertook a qualitative study based on a CBPR model to better understand violence and lack of condom use among FSWs and their male intimate partners in a northern district of Karnataka state, India. The study was initiated through collaboration between non-governmental partners in India, including the Karnataka Health Promotion Trust (KHPT) in Bengaluru, and the community-based organization (CBO) Chaitanya AIDS Tadegattuva Mahila Sangha, with researchers at the University of Manitoba (UM), and the London School of Hygiene and Tropical Medicine (LSHTM). KHPT is a non-governmental organization (NGO) that was formed as a partnership between UM and the Karnataka government to lead programs and research across Karnataka on HIV prevention and maternal, neonatal, and child health. In 2001, Chaitanya Mahila Sangha was established as a collective by women in sex work in Bagalkot, and since then has grown to achieve membership of over 80% of FSWs in the district. They have worked on a range of projects since 2003 with KHPT, and its predecessor the India–Canada Collaborative HIV/AIDS Project (ICHAP), on targeted programs for HIV/AIDS prevention through peer education, condom promotion, and sexually transmitted infection (STI) services. These programs continued to be supported as part of the Bill and Melinda Gates Foundation’s Avahan project involving HIV and violence care and counseling, crisis management, community mobilization, and self-help groups providing micro-credit (Chaitanya Mahila Sangha, 2013). Chaitanya is one of the most active and long-standing FSW CBOs in the region, now also applying for and implementing government-funded programs, making it a natural step to start working more closely as partners on research.
Discussions between partners on the potential for a CBPR study with Chaitanya were held in 2012 in which community leaders had expressed that their top research priority was to better understand IPV facing their members. At this time, KHPT, UM, Chaitanya, and LSHTM were collaborating with other partner organizations, in a project called “Tackling the Structural Drivers of the HIV/AIDS Epidemic” or STRIVE. As part of STRIVE, these four groups collaborated to undertake a 3-year evaluation of Samvedana Plus, designed to reduce violence and increase condom use within the intimate relationships of FSWs in Bagalkot district and one other pilot district. This convergence of interests led to a longitudinal qualitative case study adopting a CBPR model to be included in the STRIVE evaluation of Samvedana Plus. The research methods described here pertain to the baseline exploratory study that was completed within the evaluation, involving 38 in-depth semi-structured interviews with 13 individual FSWs, five individual intimate partners of FSWs but not partnered with study participants, and 10 couples interviewed separately (i.e., FSW and her intimate partner).
Our CBPR study employed novel methods that aimed to enhance “authenticity” in both process and outcome while navigating the challenges others have raised such as balancing power dynamics, strengthening the existing organizational context, and preserving the transformative potential of the CBPR approach (Minkler, 2005; Montoya & Kent, 2011; Salimi et al., 2012; Wallerstein & Duran, 2010). To this end, the study incorporated three key interrelated components that we developed through our collaborative planning processes, including (a) the development and maintenance of long-term partnerships designed to encourage equitable involvement at all stages, (b) incorporation of ongoing training and knowledge exchange, and (c) an orientation for action on relevant health and social issues.
Ensuring Long-Term, Equitable Partnerships
Research Topic Selection
During meetings in June 2012 with UM and KHPT, Chaitanya leaders expressed an interest in being more involved in research and identified IPV as the most pressing issue to study. They determined the following as important research questions:
Development of Ongoing Researcher–Community Partnerships
This study was embedded within the wider organizational commitment of long-term partnerships between Chaitanya, KHPT, and academic organizations. Initial meetings were conducted in early 2013 with 15 leaders from Chaitanya to determine study objectives, criteria for selecting members of a community Research Committee, a timeline, and selection criteria for both potential participants and community research investigators (CRIs). A community Research Committee was then formed by women in sex work who volunteered to be involved with good verbal skills, knowledge on the issues, and some previous involvement in research. Seven women joined the Research Committee as a representative body for the CBO. After some attrition due to migration and time constraints in the first year, the remaining members of the Research Committee decided that consistent attendance would solidify membership, while new members would be selected democratically through votes by the CBO Board of Members.
Roles and Responsibilities
Important in the initial stages was the determination of the roles and responsibilities of all partners. Each of the partners expressed their expectations from the others, and agreed on what they could contribute so as to build on each other’s strengths, as Israel et al. have recommended (Israel et al., 1998). For example, the community Research Committee felt that they had knowledge in the topical areas, ethical and logistical considerations, and were experienced with recruiting participants for other studies. In return, the Research Committee members viewed training and guidance by the other partners on methods for data collection, analysis, and writing of reports as a renewable resource that would strengthen their involvement in this and future studies. Sometimes the diverse partnerships caused confusion and language barriers, but these were addressed through close involvement of program field staff from KHPT who could ensure the training processes were conducted in local dialects.
Methods of Training and Knowledge Exchange
Interview Question and Tool Development
An important component of CBPR to which our team committed much time was training and knowledge exchange (Israel et al., 1998). The NGO and academic researchers provided the community Research Committee training on evaluation and CBPR research processes and methods at multiple points in the study. To begin, KHPT program directors and AKB held training workshops for the Research Committee on research principles and processes in July 2013 in Bagalkot, followed by workshops to develop the questions, tools, and ethical protocol.
Interview tool development involved multiple stages: We discussed a range of issues involved in understanding IPV; the Research Committee decided key areas that could form themes for the interview guide, and specific questions were constructed for each theme. Simultaneously, the researchers worked to streamline the tool with an eye toward the evaluation outcomes. The final interview guide included the following theme areas: (a) important relationships; (b) personal qualities, self-esteem, hopes, and dreams; (c) life problems and coping mechanisms; (d) intimate relationship history, feelings, expectations, relationship with family; (e) IPV experiences, norms/acceptance, and methods to address; (f) condom use experience and norms; and (g) exposure to the intervention and knowledge of laws on domestic violence. As part of the CRIs’ training, it was important to identify the precise questions in the local dialect through role-plays. For example, questions around women’s self-esteem were framed in terms of what they liked or disliked about themselves, rather than about good or bad personal “qualities” as in English. Through pilot-testing with two women in sex work, the CRIs and KHPT staff further refined the interview questions into a pictorial tool with brief prompts to allow for more natural dialogue.
Ethical Protocol and Approval
Numerous ethical issues are important in a CBPR study, such as cultural appropriateness of methods, feasibility of timelines, training for community partners or interviewers, and the joint use of data for program and research outputs (Buchanan et al., 2007; Campbell-Page & Shaw-Ridley, 2013; Jamshidi et al., 2014; Schaffer, 2009). We worked as partners to determine the ethical considerations for each stage, which was formed into a protocol for all to follow. Important elements that the Research Committee identified were (a) safe means of approaching participants and concealing their identities; (b) a sensitive and relevant interview guide; (c) participant counseling if requested, and debriefing with CRIs; (d) awareness by the CRIs of the neighborhood context; (e) interviews with men by an external interviewer, after consent by and separately from the FSW participant; and (f) participants’ honoraria equivalent to but not beyond travel costs, to ensure fair and voluntary participation. Although concerns were raised by some academic partners regarding couple interviews, recent experience has suggested that this could be conducted ethically if precautions were observed (Dandona et al., 2006; Enosh, Eisikovits, & Gross, 2013; Karandikar & Gezinski, 2012; Kostick, Schensul, Singh, Pelto, & Saggurti, 2011; Luke, Schuler, Mai, Vu Thien, & Minh, 2007; Panchanadeswaran et al., 2012; Sikweyiya & Jewkes, 2011). Research Committee members stated that interviewing both members of a couple separately was feasible because Devadasi women usually lived independently with their own incomes and many of their partners did not belong to the same village as them.
To obtain informed consent, the CRIs used a “vague first contact” approach toward potential female participants (Sikweyiya & Jewkes, 2011) in which the study was introduced generally as a health study to potential participants. If they showed interest, this was followed by a full informed consent process both for interviews and for contact with their intimate partners. A concern of the community Research Committee was that participants would benefit from doing the interviews, which is a key ethical consideration. As part of consent, the CRIs told the women that through the interview they may gain more courage or peace of mind, but it would ultimately help the CBO to move ahead in addressing the wider community issues related to IPV and HIV/AIDS.
To ensure confidentiality, all the interviews were one-on-one and the locations were determined based on the interviewees’ preferences (e.g., home, a neighbor’s home, a public place, or CBO office), with a code to stop talking if others approached. During analysis, interviews were de-identified and discussed individually between external researchers and the interviewers first, then aggregately with the Research Committee, and KHPT as a whole. Ethics approval for the study was obtained by all partners, including the St. John’s Medical College to KHPT in Bangalore, the LSHTM’s Research Ethics Board, and UM’s Human Research Ethics Board (H2014:108).
Training With CRIs
Chaitanya selected a pool of potential CRIs from within the FSW community. In December 2013, the CRI candidates were trained on qualitative research and interviewing skills. The workshop was followed by numerous role-plays and “fish-bowl” exercises to practice skills, where pairs of women practiced interviewing each other with a set of questions in front of the group. Observers provided feedback on the importance of open body language, facial expressions, clear questioning, probing, and the need to give time for longer answers. Through role-plays, the phrasing of the interview questions in Kannada was determined, and allowed increased familiarity with the questions by the CRIs. The final selection and hiring of two CRIs was made jointly by the Research Committee and academic researchers.
Sampling Strategy
The Research Committee suggested that important and ethical criteria for sampling included: participants from villages that the CRIs are not from; those who reported experience of chronic events of IPV in last 12 months; those having a single intimate partner (for the couples, to ensure clarity of their accounts and safety for participants); participants from different age groups(those both below age 25 and 25 or above); representation of home-based FSWs as well as all other typologies of sex work; and women both with and without children. The sample was selected by KHPT researchers in Excel from their “line-listing” of women registered in the Samvedana Plus intervention in 2012 to maximize variation on the abovementioned characteristics. In total, the CRIs and male RI interviewed 38 participants, including 13 individual FSWs, five individual intimate partners, and 10 couples (FSWs and their intimate partners), which will likely preserve a sufficient sample for further rounds.
Data Collection
The CRIs made initial contact and obtained informed consent. Though all partners agreed on the importance of maintaining confidentiality by ensuring the CRIs went to villages they were not from, this caused initial challenges for logistics and discomfort for the CRIs that they had to overcome through further training. The community Research Committee and KHPT staff were central in supporting the CRIs throughout, especially as it was a completely new process, involving extensive travel and perseverance to contact the interviewees. The main difficulties in data collection for the CRIs occurred in recruitment, mostly due to migration or deaths of the participants in the initial sampling frame, wariness on the part of the participant of being recorded, and fear of identifying as Devadasi if they were a part of the Government’s Devadasi Rehabilitation Programme. 1 Male participants were more difficult to recruit due to transient work, suspicion around recording, and the topic of violence itself. After informed consent, interviewers completed one-on-one, semi-structured in-depth interviews using digital recorders, as well as taking written field notes before, during, and after each interview. Field notes included the process of consent, the manner in which the questions were answered, and any occurrences outside the recorded interview that provided insight (e.g., when an intimate partner interrupted, or body language in the interview). The most difficult aspect of the interviews was in broaching sensitive topics, particularly around condom use. The CRIs stated that if it had been an outside interviewer, the topic would have been difficult to broach. However they were able to assess through the way the participant answered whether they were being open or not. The field notes and interviews were transcribed verbatim by KHPT RIs and the CRIs, and translated by KHPT’s trained local translator who was familiar with the interview guide and data collection process. SGN read through each transcript for accuracy and completeness in English before analysis, consulting interviewers where needed.
Orientation for Action
Collaborative Data Analysis
Because few CBPR studies have reported on the involvement of community partners in interpreting results, we undertook a process of “meaning-making” that involved a novel combination of analytic methods in multiple steps (Cashman et al., 2008; Ellsberg & Heise, 2005; Lorway et al., 2014; Miles & Huberman, 1994). First, AKB coded the interviews with a set of “nodes” developed with SGN in NVivo 10.0, in light of the interview questions and STRIVE’s evaluation outcomes. Shortly thereafter, AKB and SGN met in Bagalkot to discuss with the CRIs and male RI what they found to be the most important findings from each interview, and then to identify main points for each of the interview guide sections across participants.
In a subsequent workshop, these main descriptive points were translated into Kannada and presented in PowerPoint by the CRIs to the community Research Committee and KHPT intervention team. This was the basis for a collaborative “meaning-making” exercise that adapted card-sorting and causal flow diagram methods used elsewhere in qualitative violence research (Ellsberg & Heise, 2005). Specifically, we formed two groups composed of one CRI and KHPT or UM researcher, with half of the Research Committee members in each. Each of the main points from our descriptive analysis was written on small cards of paper in Kannada, which were enumerated to correspond with a list of points in English. A copy of each was given to the two separate groups. The groups arranged the sheets on a poster board to show which points related to one another, with violence and condom use as the central, though not sole, outcomes of interest. The groups decided which points were most closely related to IPV and condom use outcomes, and which were less important and placed further to the periphery. There was much dialogue to prioritize, debate, and rearrange the cards before the final placements. A representative from each group shared why they arranged the diagram that way, leading to a general discussion between the groups. The cards in Kannada were turned over to be photographed and decoded to produce an English version (as shown in Figures 1 and 2, respectively). We used these diagrams to consider the prioritization of and relationships between the NVivo coding of interviews, which helped form themes to answer the research questions.
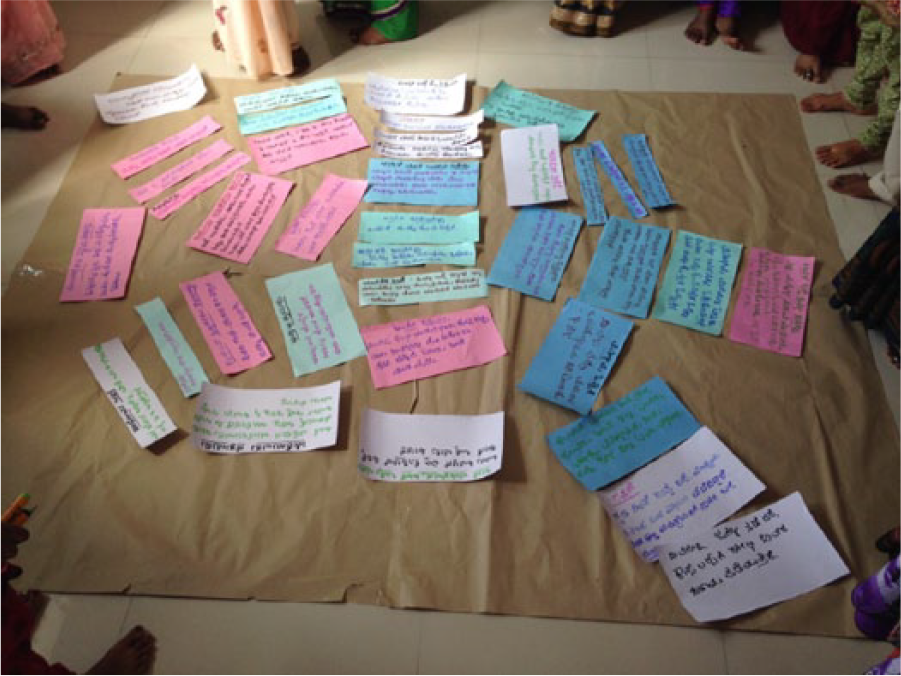
Example of a collaborative “meaning-making” analysis diagram (Kannada language).
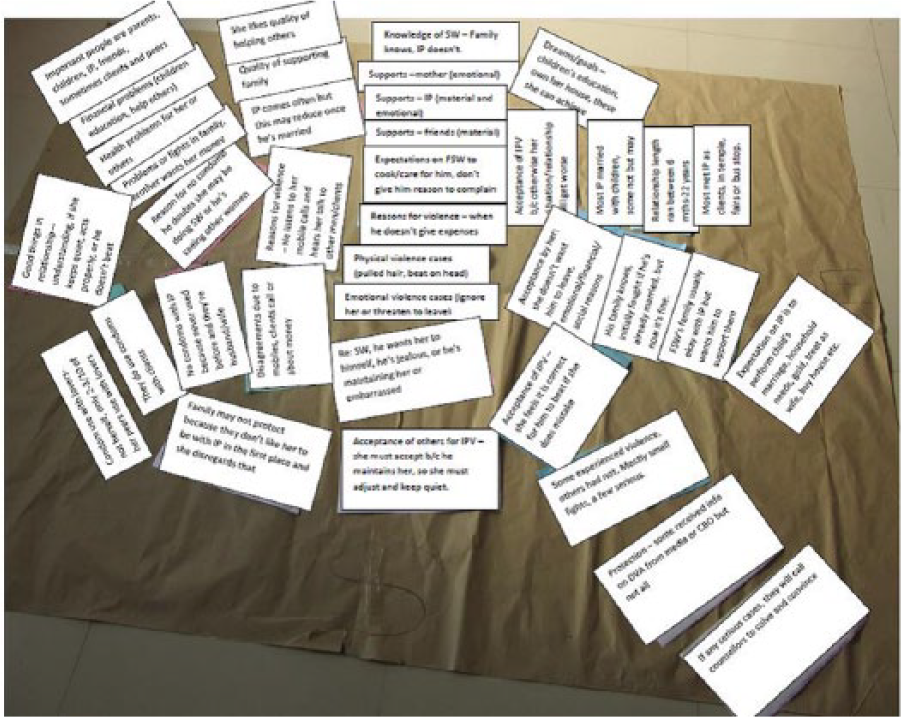
Example of a collaborative “meaning-making” analysis diagram (English language).
Action and Application of Results
Our interpretations of the findings on IPV have fed into a cyclical process of research, implementation, and evaluation, with both inherent and instrumental benefits. The CRIs and Research Committee members shared that being involved in the study was beneficial. For example, one member stated that the analytical process encouraged her own personal reflection: After joining the Research Committee, because our women express how there is violence with them, I felt it is like that for me also. Then I started understanding . . . I am personally experiencing this. Now I know what is right and what is wrong. Earlier if he beat me, scolded me also I didn’t say anything to him, I wouldn’t answer back. Now I feel, why does he talk like that?
Many female participants also said that they found the process helpful, as one CRI reported back: “At the end [of the interviews] we asked, ‘by talking to us did you find any problem?’ They said, ‘[my] mind became lighter’.” Similar reflections were shared by a respondent at the end of the interview: Thank you very much, see you. It is okay. You also share some good things with us if we meet like this. Moreover, you are here to help the people like us. So we have to respect you. We usually keep everything inside, now you made me feel quite relaxed as I expressed everything openly. That is also a kind of help from your side. (Female sex worker, aged 26)
This approach continues to have instrumental benefits by informing programs and facilitating future CBPR research, as one Research Committee member expressed, Because this is important research, people from other countries are also involved. Such studies are very few . . . What we have learnt here may be useful to others . . . Still, more research should take place about other topics. It should involve our community members . . . We can prepare them [researchers]; on who should be there, what questions should be there and all . . . We have taken training, we can ask questions. We know how to go stepwise [in research processes] . . . If we do research about a new topic then it will be more learning for us. We will come to know about other methods.
The Research Committee has continued to meet regularly with KHPT in the development of the tools for the second round of the evaluation study. The tools for the next round will delve deeper into complex and relevant issues that were raised in the baseline study, such as how differing degrees of intimacy and dependency in intimate relationships, and the associated gender role expectations, together shape levels of violence. This is based on the common finding that it was acceptable for male partners who were consistently providing financial support to use violence as a form of discipline, as one woman shared, Do you mean that men beat the women when they make a mistake? Yes, he beats her because he gives money to her; if someone goes to stop the fight he argues with them that he has that right because he gave money to her. That is why no one will interfere in such issues. (Female sex worker, aged 42)
A male partner affirmed this by saying that he was not supporting her and therefore would not fight with her if she went outside without permission: Don’t you ask her why she went to other places? Why should I bother about that? I am not maintaining her, she has her own life. I cannot maintain [financially support] her life, then why should I create a problem? (Male intimate partner, aged 34)
Another area that was identified for further exploration in the second round was the social meaning of being a Devadasi, and how this is reconciled with the social expectations for monogamous male–female relationships. The acceptance of violence was seen as a sign of love as in a marriage, but the aspiration to be like a marriage was heightened by the changing legal and social environment in which the Devadasi tradition has been criminalized and blamed for the spread of HIV/AIDS: [T]hey [intimate partners] have to be like married couples if they want to continue their relationships . . . they [government] told us not to continue this observance of tying the righteous pearls to women [dedicating women as Devadasi sex workers] since dangerous infections are spreading. Awareness is being created among the families of our community to re-establish their lives. If there are any unmarried lovers, they are getting married. (Female sex worker, aged 26)
The knowledge gained on reasons for IPV and condom use from the study has also continued to inform KHPT and Chaitanya’s implementation of the Samvedana Plus program. Specifically, a major finding in the study was around the level of suspicion and infidelity in the FSW-intimate partner relationship as a trigger of violence. The analysis showed that the relationship was based on gender role expectations to be like a marriage, leading women to stop or at least conceal their involvement in sex work: I forgot that [sex work] profession. We are living like married couples. He and I are like wife and husband and the whole village knows it . . . (Female sex worker, aged 33)
Furthermore, violence was justified when expectations for fidelity were contravened either through sex work or other forms, as one man stated, She [female partner] should not have any contact with other men, because I have taken the responsibility of her life. So I will beat her if she commits a mistake. I will be like a husband with [lover’s name] as how you [interviewer] are with your wife. (Male intimate partner, aged 31)
The Samvedana Plus curricula for counseling female and male intimate partners have therefore been revised to be more sensitive to addressing triggers of violence like jealousy and trust in the context of gender role expectations to be like a marriage. The information on complex social dynamics in intimate relationships that the baseline study provided will help to strengthen the work of Chaitanya Mahila Sangha and KHPT on Samvedana Plus both methodologically and programmatically.
Discussion
The collaborative process we developed in our qualitative study in South India on IPV and HIV/AIDS vulnerability among women in sex work contributes to current discussions on optimizing authenticity in CBPR literature. To pursue authenticity in terms of an inherently valuable process, we built on long-standing relationships between community, NGO, and academic partners (Israel et al., 1998). In practice, most examples in the literature show that community partners are involved in initial problem identification, recruitment of participants, and sometimes interpretation of the results (Salimi et al., 2012). Less often have they been involved in the technical aspects of methodology, data collection, and particularly the analysis; these require extra resources and have sometimes been seen as a challenge to scientific rigor (Carlisle & Cropper, 2009; Cashman et al., 2008; Elliott et al., 2002; Lorway et al., 2014; Shannon et al., 2007). In line with the purposes of CBPR, we found that working within an existing organizational context surrounding a program of research and across the research cycle was inherently valuable both for ongoing mutual development of skills, and as a platform for the application of results within the Samvedana Plus intervention (Minkler, 2004; Salimi et al., 2012; Schaffer, 2009).
As a key part of authentic community-based processes, we aimed to create a space for co-learning and capacity-building through cyclical, rather than unidirectional knowledge translation; this corresponded with the CBO’s interest in understanding and applying the results directly in their programs (Israel et al., 1998; Stack, 2013). The involvement of peer interviewers carried inherent value by buttressing the work and relationships of the CBO to address the daily issues affecting their community. The CRIs will continue to be an asset to the CBO’s engagement in ongoing research by conducting interviews in the future. In addition, the importance of orienting CBPR partnerships toward future action was embodied in the Research Committee’s desire to continually meet together and, with KHPT, discuss relevant issues of research, inform the next stages of data collection, and participate more fully in establishing related study and ethical protocols.
Essential for an authentic process in CBPR, we sought to uphold the fundamental ethical tenet of equality in the partnership (Israel et al., 1998; Minkler, 2005; Montoya & Kent, 2011). As discussed elsewhere, we found that to better overcome the inevitable power-related issues required constant consideration, especially with respect to time, money, and decision-making power (Guta et al., 2013; Lorway et al., 2014). On a few items like sampling, input from the community Research Committee could have been sought first rather than after the evaluation framework was externally designed to prevent any disjointed decision-making; yet because the study design was flexible, these inputs were still largely able to be incorporated. Another issue of control and power was that of finances; because of the CBO’s strong relationship with KHPT, the leaders of the Research Committee were able to obtain more control over the finances and increased salary for the CRIs over the course of the study. Through extended engagement and involvement, the community Research Committee felt that they had greater responsibility for the process than any previous research involvement: “If there were any problems we would solve them . . . [If] we get the result or don’t get the result, we are responsible for everything.” The power held by the Research Committee was maintained through their ability to inform decisions, express opinions, and choose to continue being involved in the research or not.
Much literature on ensuring rigor in qualitative research encompasses debate on whether universal, or at least guiding, criteria for quality of results could or should be established (Denzin, 2009; Gordon & Patterson, 2013; Hatch, 2006; Lincoln & Guba, 2000; Seale, 1999; Tracy, 2010). Though the role of community in this has been seldom discussed to date, we tried to use a process that built on, yet contextualized, general guidelines for quality as Lincoln and Guba (2000) have promoted for interpretive approaches. In this view, the question of authenticity of the results (i.e., ‘are they isomorphic to some reality’) relates both to how one approaches the methods and the interpretations in research (Lincoln & Guba, 2000). First, in our methods, the processes of co-learning and sharing language throughout aimed to prevent disconnect between academic and community discourses or ways of knowing. Many of the considerations that the RC members raised, though resonant with past literature on IPV, were also very context-specific and based on a strong understanding of the community. An example is the important discussions that we shared on the appropriate local phrasing needed in the questions, which the CRIs stated and the transcripts reflected were understandable to and well-received by participants. It became apparent upon analysis that through collaborative planning and tool development, the interviews provided an array of in-depth perspectives.
The involvement of CRIs was another aspect of the qualitative methods that could contribute to the authenticity of results. There was some initial concern that there were insuperable trade-offs of involving CRIs in the study, particularly for gaining in-depth and trustworthy accounts. Thus, we committed increased time and effort on training. With support from the community Research Committee and KHPT’s trained research investigators as mentors, the interviews became longer and more in-depth. As found in other contexts (Carlisle & Cropper, 2009; Elliott et al., 2002), it was evident that the initial challenges were outweighed by the local knowledge and position that CRIs had, as one of the community interviewers reflected, Someone else interviewing them and us interviewing our own women, there is a lot of difference. The difference is, we introduce about ourselves also—I am also a sex worker, I also have a lover. My situation and circumstances are also like yours, so she agrees [to share]. If someone else comes then they talk saying “you, you” . . . But we say “our, our” when we talk.
Furthermore, they were able to ask questions that were not directly in the guide, exploring relevant aspects that only they would think to ask by sharing similar life circumstances. A number of participants expressed that they were disclosing something sensitive to the CRI, especially if they had to conceal their involvement in sex work from their partner. The enhanced rapport and expressed benefit to participants suggests that this increased the trustworthiness of the accounts.
As another aspect of achieving rigor, the collaborative thematic analysis approach that we developed aligns with Lincoln and Guba’s (2000) assertion that “meaning-making” activities are central both for achieving trustworthy interpretations and for shaping action in interpretive inquiry. Being an exploratory study aimed at understanding social phenomena from a range of perspectives, our approach was consistent with the view that criteria for knowledge is not separate from the knowers, but must be made comprehensible through meaning-making as a social process (Israel et al., 1998). CBPR has been said to acknowledge subjectivity while maintaining the search for patterns and contribution to theory (Israel et al., 1998). Throughout our qualitative analysis, the creation of space to share dialogue and multiple viewpoints on the interview results was aimed at enhancing the relevance, ownership, and applicability of results. For example, our analytical discussions reflected important debates in the theoretical and empirical literature on IPV (Shahidullah & Derby, 2009; Venning, 2010). In many of the interviews among women and particularly men, and some of the Research Committee members’ views, an individual-level lens was reflected when unmet expectations for behavior in the intimate relationship were seen as “mistakes” that justified violence. This led them to suggest that women should change behavior to avoid “mistakes.” Conversely, there were some women in the study and members of the community Research Committee with the view that violence was never acceptable. They identified how justification of IPV based on “mistakes” appeared to be rooted in broader social issues like economic exclusion, stigma, and gender norms. Our collaborative meaning-making processes to prioritize and interpret the results will continue to be useful for informing the Samvedana Plus IPV program and can contribute to broader theory and practice (Cashman et al., 2008; Lorway et al., 2014). The authenticity of these results should be further strengthened through triangulation with subsequent rounds of this qualitative study. Hence ongoing interpretation and refining of our understandings will be possible through ongoing dialogue between the community, academic, and NGO partners in the coming years.
Conclusion
Throughout this qualitative CBPR study on violence and HIV/AIDS among women in sex work and their intimate partners in Bagalkot, South India, we aimed to create a shared space for dialogue on appropriate research questions, methods, ethics, and quality that would help us to pursue authenticity in both process and outcome. While it has sometimes been argued that the purpose of optimizing authentic community partnerships with inherent value must pose a trade-off with the quality of the research outcomes, this study drew on an interpretive approach that allowed us to view both as mutually supportive aspects of authenticity. In line with broader principles of CBPR, we pursued this goal by incorporating three main components, including first, long-term partnerships between academic researchers, community representatives, and local organizations; second, multi-directional training and knowledge exchange; and third, a strong orientation toward action for improved health and well-being. Our methodological framework may offer encouragement for future qualitative community-based research endeavors to pursue truly collaborative methodologies that can also effectively develop knowledge and engage in action to improve health and reduce disparities globally.
Footnotes
Acknowledgements
The study would not have been possible without the involvement and support of many from the Chaitanya AIDS Tadegattuva Mahila Sangha and Karnataka Health Promotion Trust program teams in Bagalkot and Bengaluru, India. The authors sincerely thank the participants for their valuable time and willingness to participate.
Authors’ Note
For more information on related research materials for this study, please contact the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful for the support from the STRIVE research program consortium for this research, which is funded by the Department for International Development (PO 5244).