
Abstract
While analyzing the narratives of children receiving pediatric oncology treatment and their parents, we encountered three ways to look at their narratives: what was narrated, nonnarrated, and disnarrated. The narrated refers to the actors (characters) and events (scenes) individuals decided to include in the narration of their experiences, the nonnarrated are everything not included in narration, and the disnarrated are elements that are narrated in the story but did not actually take place. We use our reflection to illustrate how an integrative analysis of these different forms of narration can allow us to produce a holistic interpretation of people’s experiences of illness. This approach is still in the early stages of development, but we hope this article can promote a debate in the field and lead to the refinement of an important tool for narrative analysis.
Storytellers shape the world according to the narratives they tell. In health services research, these stories describe the complex constellations of beliefs, values, emotions, intentions, identities, attitudes, and motivations that research participants use to express themselves as individuals and embed themselves within the illness narratives they enact and tell. The research we present here is based on narrative data collected from pediatric oncology patients and their families in Buenos Aires, Argentina. We analyzed the interviews by identifying the primary actors within the illness narrative (i.e., characters) and dominant scenes of activity, organized thematically, based on treatment trajectories.
During the analysis process, we encountered three ways to analyze the narratives of the children and their parents. These included searching for the following: (a) who and what is present in narratives (i.e., narrated), (b) who and what is not present within the story (i.e., nonnarrated), and (c) what is alluded to in the text, yet did not actually happen (i.e., disnarrated). This article presents a reflection of this approach, the contributions it made to the interpretation of the data collected in this study, and its potential application in other research projects.
Illness Narratives
Narrative research is based on the idea that “experience is shared and that experience itself is storied, or it has a narrative pattern” (Sandelowski, 1991, p. 162). Narratives can be both descriptive and explanatory (Groleau, Young, & Kirmayer, 2006; Mishler, 1986; Polkinghorne, 1988). Individuals can implement different formats or narrative types (Frank, 1995; Loseke, 2007; Smith & Sparkes, 2011) to express and deal with events in their lives. These culturally available types of narratives act as guidelines that people adapt or combine to tell their own story (Frank, 1995; Nosek, Kennedy, & Gudmundsdottir, 2012). Narrative types also share common components: narrators, plots, scenes, settings, and characters (Gubrium & Holstein, 2009; Simpson, Heath, & Wall, 2014).
The insight into individual experience that narrative analysis affords is one of the main reasons why this framework is rapidly incorporated in health services research (Hall & Powell, 2011; Hsu & McCormack, 2010; Stenhouse, 2014; Thomas et al., 2009). Narratives are flexible and allow individuals to express their own views about their illness or the care they have received by occupying multiple positionalities and discourses (Mattingly, Lawlor, & Jacobs-Huey, 2002). At the same time, there are certain events in life, such as illnesses, and certain contexts, such as the hospital, which produce specific narrative types (Boaz & Morgan, 2014; Edvardsson, Rasmussen, & Riessman, 2003; Engebretson, Peterson, & Frenkel, 2013; Ewick & Silbey, 1995; Frank, 1995; Thomas, 2010; Tropea, 2012).
In other words, illness narratives have identifiable patterns. They have an inherent temporality (Bruner, 1990; Groleau et al., 2006; Ricoeur, 1984) because they involve sequences of events, feelings, relationships, or spaces (Rapport & Overing, 2000). Therefore, narratives allow the researcher to identify the particularities of the storytellers’ experiences, organize their actions, and make meaning out of a series of events (Park, 2008; Petty, Thomson, & Stew, 2012).
The Narrated, Nonnarrated, and Disnarrated
When looking at what is narrated, the concepts of narrator, character, scene, and plot proposed by Greimas (1966), one of the most famous structuralist literary theorists, are useful categories for classifying, arranging, and analyzing data collected from interviews. Greimas (1966) was interested in the different ways in which story characters perform different functions—a position we think appropriate given the multiple roles of “characters” within our data as children, patients, parents, caregivers, care receivers, and diagnosticians. Stories are not constructed randomly or by chance. Individual storytellers’ narrative decisions—who appears (character) and in what event or action (scene) they appear—are based on the purpose behind telling the story, where the story is told, and to whom it is told (Good, 1994; Riessman, 2003). As Kleinman (1988) has indicated, Patients order their experience of illness—what it means to them and to significant others—as personal narratives. The illness narrative is a story the patient tells, and significant others retell, to give credence to the distinctive events and long-term course of suffering. The plot lines, core metaphors, and rhetorical devices that structure the illness narrative are drawn from cultural and personal models for arranging experiences in meaningful ways and for effectively communicating those meanings. (p. 49)
Such a literary consideration of health narratives entails careful attention to participant roles and identities (Bauman, 1986; Groleau et al., 2006), how performances are expressed and employed (Cosentino, 1982; Riessman, 2003), social norms guiding performance and human relationships (Darnell, 1974; Laslett, 1999; Riessman, 2004), and the series of events that led up to the story (i.e., cultural context; Falassi, 1980; Squire, 2008). However, many times, parts of human experience do not form part of the story (Riessman, 2003). Mattingly (2004), for example, has discussed the construction of narratives in clinical settings as related to the “healing dramas” and “healing possibilities” they reveal (p. 74). Through this lens, she explored how the construction of life experiences are “uneven” making certain moments of intense joy (e.g., cancer remission) or terror (e.g., cancer progression) “more narrative” than others (Mattingly, 2004, p. 74).
Researchers elsewhere have categorized the potential inability of narration to touch on those more routine or everyday moments as “failure of the grammar of the ordinary” to describe how we experience daily life (Das, 2007, p. 7). How narratives are expressed and employed becomes only one facet of the story, and that which occurred, yet was not narrated, also deserves consideration. Prince (1992) has argued that the segments that are left out of a story can be visualized as, Everything that according to a given narrative cannot be narrated or is not worth narrating—either because it transgresses a law, or because it defies the powers of a particular narrator, or because it falls below the so-called threshold of narratability. (p. 28, emphasis in original)
Narrators choose to leave out elements that threaten their ability to tell a story as well as issues they do not consider sufficiently important or interesting. This last point includes all of the daily, and often taken for granted, activities that are present in the events being narrated, which might be implied, but are not specifically told because they would make the story tedious or repetitive (Prince, 1992).
In addition to what is narrated and nonnarrated, there are other events that storytellers include in their story that play a different role—disnarrated events. The disnarrated refers to “all the events that do not happen though they could have and are nonetheless referred to (in a negative or hypothetical mode) by the narrative text” (Prince, 1992, p. 30, emphasis in original). For example, when the text mentions the possibility of an event happening such as “he saw the envelope on the table but did not open it.” Here, disnarration functions to create specific effects on the reader such as suspense, surprise, an advance of what could happen (but does not), the presentation of a parallel and alternative reality, and the deception of the reader (Prince, 1992). As Lindholm (2003) argued with regard to the use of the disnarrated in the short story genre, “the disnarrated allows its readers to delve into the hopes, possible directions, dreams and fears of the focalized character” (p. 208).
This technique is also common in face-to-face communication, appearing in phrases such as “I wonder what would have happened if . . .” or “if I had to do it over again, I would . . ..” The disnarrated in this sense can be used to express regret, hopefulness, plans for the future, or critiques of past decisions. The search for the disnarrated in texts or interview transcripts becomes a useful analytic tool when we seek to answer questions such as the following: If this event did not happen, why does the narrator mention it? Why does the narrator need to include it in the story? If story making is “fashioned to convince others to see and comprehend some part of the reality in a particular way so that what happens follows from the way things are portrayed to be” (Garro & Mattingly, 2000, p.261), what role in the convincing process are these hypothetical events playing?
The lifework of Rita Charon (1993, 2001, 2004, 2006, 2009, 2011) and Maura Spiegel (Charon & Spiegel, 2003; Spiegel & Charon, 2006, 2009), who are part of the core faculty of the Program in Narrative Medicine at Columbia University, provide us with questions for understanding the disnarrated stories encountered while conducting pediatric oncology research. In seeking to understand the intimate connections between sick bodies and the norms guiding how those bodies are medically treated—usually as either disembodied reminders of Cartesian division or embodied selves that bridge mind and body—they propose, “seeking for what comes after loss . . . might be another way of trying to understand, more simply, what comes before it” (Charon & Spiegel, 2003, p. 135). Structuring the narrative in this manner is less about communicating one’s personal experience to others (for the event did not actually occur), and more about interrogating how potential futures can be reconciled with past and present illness experiences.
A common criticism for analyzing illness narratives has been that analysts tend to overemphasize their privileged access to personal experiences leading to “inappropriate assumptions concerning human actors and social action” (Atkinson, 1997, p. 325). For example, in the narrative agenda proposed by Mishler (1984, 1986) to use personal narratives of illness as a therapeutic and emancipatory tool for patients, Atkinson (1997) questions whether this “Romantic agenda” (p. 334) and “surrogate form of liberal humanism” (p. 335) can provide a solid methodological foundation for theory building.
Other authors argue that in explaining human behavior only in terms of meaning systems, this framework tends to represent individuals as causal in their own right and contributes to the obfuscation of social structures and power relations in clinical settings (Baer, Singer, & Susser, 2003; Lewellen, 1983; Singer, Baer, & Lazarus, 1990). More recently, Atkinson and Delamont (2006) caution that qualitative researchers might be too quick to celebrate narratives rather than subject them to systematic analysis. While we understand the basis for these critiques, we believe that the analysis of individual illness narratives, when grounded in a research design devoted to rigorous methodology as hinted by Atkinson and Delamont (2006), holds significant explanatory power to search for the meaning of not only what was narrated but also what was not narrated or disnarrated.
The Study
Data presented in this article were collected during three research projects conducted in Buenos Aires, Argentina, from 2008 to 2010. In all occasions, the research was carried out in collaboration with Fundación Natalí Dafne Flexer (Natali Dafne Flexer Foundation or FNDF), a local non-governmental organization that provides medical and other forms of assistance to pediatric oncology patients and their families. The interviews and other activities with participants were carried out at FNDF’s facilities. Multiple methods were utilized for data collection: interviews, four different types of child drawings, participant observation, and historical and public policy document analysis. This article reflects only data derived from interviews. Information collected by using other research methods can be accessed in previous publications (Johnson, Pfister, & Vindrola-Padros, 2012; Vindrola-Padros, 2012; Vindrola-Padros & Whiteford, 2012). A total of 70 interviews (35 with parents and 35 with children) were recorded and transcribed.
Interviews
Audio-recorded, open-ended, semi-structured interviews were used to obtain illness and treatment histories and narratives from child patients and their parents. The interviews were organized to obtain disease and treatment histories for each child and their family’s experience. They were divided into two sections. The first section started with the following instruction: “Tell me how everything began.” The study participant was then prompted to continue the story. This portion of the interview created narratives that were then analyzed according to the inclusion (or exclusion) of characters and scenes.
The second section was organized according to the following areas: description of diagnosis, description of treatment, travel to Buenos Aires, resettlement, perceptions of medical treatment, perceptions of the health care system, and demographic information. The participants were asked questions about family and household composition and their main sources of income as well as their ideas toward health care in Argentina, their advice for other children/parents in the same situation, and their reflections on how pediatric oncology treatment could be improved. The questions in this section of the interview guide were open ended to allow the participants more freedom in their interpretation. Answers were used to contextualize the treatment and migration narratives constructed by children and parents and to understand the particular characteristics of each household.
Process of Data Analysis
The first author (Cecilia Vindrola-Padros) transcribed the interview recordings in Spanish (with selected quotes translated to English) and compiled the field notes from participant observation into one file. The content of each narrative was analyzed in the following ways. First, the main actors (also referred to as characters) were identified. In the case of this study, the two main actors were the children and their parents. Their stories served as the base for identifying the other actors involved in the situations described during the interviews (i.e., doctors, nurses, siblings, volunteers).
Second, the main scenes described during the interviews were identified and organized into categories. It is important to take into consideration that the scenes described by the children and parents were structured by the dynamic of the interview guide that delineated a temporal and sequential arrangement based on the treatment protocol. However, not all of the participants adhered to this structure. Many changed the questions to their liking, skipped stages, critiqued the questionnaire, and suggested new questions for its improvement. In other words, even though the narration is heavily influenced by the interview setting and questionnaire, parents and children played active roles in fashioning a narrative that represented their lived experiences.
The patterns found in the representation of actors and scenes were used to create a list of codes. These codes were discussed with another researcher who was also familiar with the transcripts to reach consensus on a final list of codes. ATLAS.ti qualitative computer software (ATLAS.ti Scientific Software Development, 2006) was used to help manage the data and codes assigned by Cecilia. A list of the topics not included in the stories was also made to compare the nonnarrated issues in parents and children’s narratives. Information collected on the characteristics of each household was summarized into brief vignettes on each family, and portions of these descriptions were used to understand the processes of narrative construction.
Sample
As described above, the three research projects generated a convenience sample of 35 families from areas outside of Buenos Aires whose children (ages 5–17) were undergoing cancer treatment in four public hospitals in the capital city. These hospitals were selected because the families who frequented FNDF’s headquarters received treatment in these medical facilities. Only one parent refused to participate in the research project. Children in different stages of treatment were asked to participate to obtain a better understanding of how perceptions change through time. Participants from different provinces of the country were selected to document greater diversity in travel experiences.
Ethics Review
The research protocol, information sheets, and consent and assent forms were approved by the Institutional Review Board (IRB) at the University of South Florida. The President of FNDF also reviewed these documents. Cecilia handed the age-appropriate information sheets in Spanish to the parents and children explaining the contents of the study, potential risks and benefits, the voluntary nature of their participation, and the possibility of withdrawing at any point. No personal or identifiable information was collected during the interviews or observations. Each participant was assigned a code, and they are referred to in all publications by pseudonyms.
The Narrated
As mentioned earlier, the narrated refers to everything that happens explicitly in the text and is told as a factual component of the story. One way of analyzing the narrated was to ask the following question: Who was represented in the text? This question allowed us to look for the main characters that form part of the person’s illness story: the people, groups (e.g., patient groups, online support groups), or institutions and organizations (e.g., the hospital, the health care system, the government) the storyteller deemed necessary to include in the story. We identified and typified the characters in one individual story to understand how it is constructed and to compare these types across and among groups to identify patterns. For instance, in our study on pediatric oncology treatment in Argentina, each individual child narrative was analyzed by asking, “Who was represented?” All of the characters in the children’s stories were compared and then these were associated with the characters appearing in the parents’ stories. The result of these comparisons is presented in Figure 1.
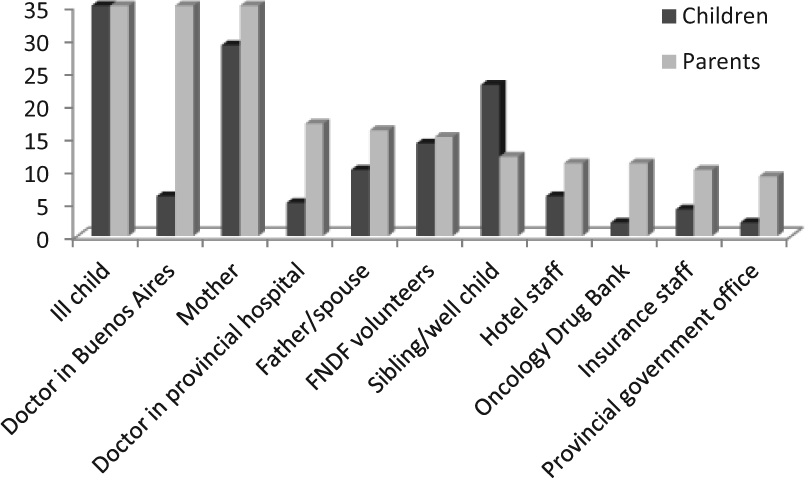
Characters identified by children and their parents.
The results of the study indicated that children tended to talk more about close family members such as their mothers (82% of the participants, the other 18% mentioned grandmothers or other family members), siblings (65%), and fathers (29%) and less about their doctor in Buenos Aires (17%) or the doctor in their provincial hospital (14%). The children also identified a wide variety of other actors with whom they had contact on a daily basis. Hospital volunteers and the staff of the hotel where they stayed when they were not hospitalized were the most prominent ones.
Individuals in charge of providing medical and non-medical services for children appeared more frequently in the parents’ stories when compared with the children. The doctors in Buenos Aires appeared in all 35 interviews, and the doctors from provincial hospitals were mentioned in 47% of the stories. Other included professionals were hospital volunteers (43%), the Oncology Drug Bank (31%), hotel staff (31%), insurance personnel (29%), and the local government office (28%). Family members were also present in the stories and the ill child appeared in all 35 interviews. The spouse was mentioned in 46% of the stories and the well sibling(s) in 34%. The greater frequency of appearance of these professionals in the parents’ narratives was probably because the accompanying parents were the ones in charge of securing medical and non-medical services. Throughout the treatment process, parents obtained information on the institutions and individuals capable of providing assistance (often from various sources outside of the hospital sphere).
Provincial doctors were mentioned less frequently than those in Buenos Aires. This could be explained by the fact that some families traveled to Buenos Aires without a provincial referral, while others had a referral from health care professionals they encountered in the emergency room or children were referred by specific provincial doctors and their parents avoided mentioning the doctors. Family members were not missing from the parents’ narratives, but they were not the main characters. This could be explained by the fact that most of the children included in the study traveled to Buenos Aires with only one parent, and families seldom had relatives in the city.
We also asked, “What was represented? This question prompted us to search for events that are self-contained, that is, events that in some way had a beginning and an end (similar to a scene). The scenes identified by children and parents are shown in Figure 2. In all cases, the parents’ stories began with the symptoms that led them to believe their child was not well. The stories then moved on to describe the processes of obtaining diagnosis. This was often not an easy process because it required parents to surpass obstacles produced by poorly trained personnel, unsuitable hospital policies, a lack of medical resources, and excessive bureaucracy.
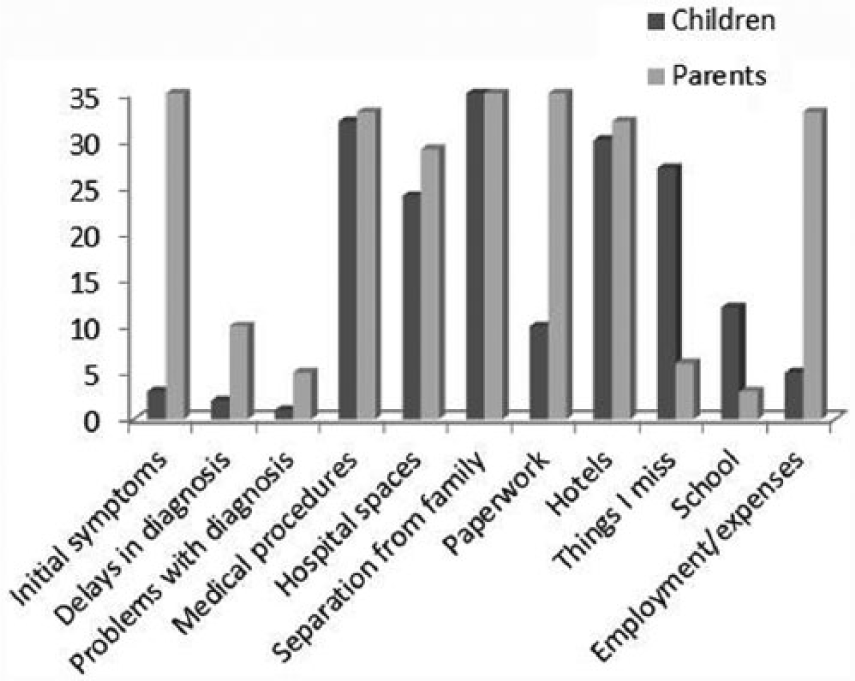
Narrative scenes identified by the children and their parents.
While parents described the details of obtaining a diagnosis, only one child focused on this stage. One possible explanation for this is that children did not see diagnosis as a separate stage. Many children were also in critical health condition during this time and, when asked specifically about it in the second section of the interview, they did not remember the steps their family took to obtain their diagnosis. When the children talked about hospitalization, they focused mainly on specific medical procedures such as lumbar punctures, chemotherapies, or blood transfusions. One of the reasons for this could be that the prompt given by Cecilia included the term treatment, which might have limited their interpretation to biomedical procedures. Parents also talked about these events, but they included a discussion on the daily activities that took place at the hospital, including eating, taking showers, and entertaining their children. Parental stories contained in-depth descriptions of the paperwork they completed to secure medical services for children, issues with employment and travel expenses, and the obstacles they encountered when traveling around a new city or dealing with paperwork delays.
The Nonnarrated
Events or individuals can be erased from stories because of the stress or anxiety their presence created, the unimportant or irrelevant role they played, or the fact that they might have represented a menace to the plot of the story or the storyteller’s ability to tell the story. Analysis of what was not narrated was carried out in close connection with the narrated and disnarrated as well as through other methods such as observations. We analyzed the individual child or parent story in connection with our knowledge of their daily routines of treatment or life outside of the hospital to determine what participants included in their stories.
When we asked “Who is not represented?” during our analysis, it was clear that children decided to erase health care professionals from their narrative. Our knowledge of the daily lives of children undergoing oncology treatment made us question this erasure knowing children are in constant contact with medical personnel. Parents rarely talked about the activities or things they missed from their place of origin, while these figured prominently in children’s stories. When talking about the place of origin, parents chose to focus on the people they left behind (e.g., spouse, other children, extended family) or the issues they were experiencing with employment, child care (for their other children), or the upkeep of the house.
The nonnarrated also emerges when comparing children’s stories according to specific variables such as the hospital where the child receives care, their age or gender, and the distance they travel to obtain treatment. In the case of this study, when the hospital scenes were analyzed together, we were able to see that “What was not represented?” varied according to the services available in each hospital. For instance, children who did not have a hospital school included scenes of school or education in their stories while those who did have access to these facilities did not talk about them. The children who included the scenes of school did so because the interruption of their education was a source of worry and concern.
The Disnarrated
The disnarrated is what is included in the text but did not actually take place in the experience the person is narrating. The disnarrated added another dimension to the analysis in which we identified characters, scenes, or issues that were narrated but the way in which they were narrated gave us an idea of the purpose behind the narration and the emotions involved in its verbalization. A clear example of the disnarrated was present in the quote transcribed below. This quote came from a young participant who was receiving oncology treatment.
Sometimes I feel like stopping all of this.
The treatment?
Yes, I mean, look at my family, we get 150 pesos from Plan Jefas [a government assistance program] and we have to spend all this money so that I can come here to get the treatment. I have two brothers and they have kids, my mom, and my dad and we are paying for the bus ticket for me, and the hotel. We put in the papers for a pension like 8 months ago and haven’t gotten anything.
In this part of her story, Adriana used the disnarrated, that is, she talked about an action (stopping treatment) that did not take place, but that she had contemplated. When prompted by Cecilia, she provided a more in-depth description of why she would stop treatment, commenting that she felt like a burden to the rest of her family and desired a change in the family’s financial situation. Rodrigo’s mother also used the disnarrated in her story when she said, Sometimes I think of how different things would have been because you go there and can come back in two hours, but the thing is that the excellence is here [Buenos Aires], and you go where you can find the best to cure your child.
Here, Rodrigo’s mother talked about the possibility of getting oncology treatment in a hospital closer to their home, only 2 hours away.
The disnarrated functioned to make the audience visualize an alternative reality, not migrating for treatment, and obtaining care closer to home. However, after this alternative was expressed, the storyteller reasserted her decision to migrate by expressing her original reason for doing so—obtaining what she considered to be the best quality medical treatment for her son. In both cases, a focus on the disnarrated facilitated a glimpse into an additional dimension of the story. By alluding to an alternative reality, that is, something that did not happen but could have happened, Adriana and Rodrigo’s mother were able to express their feelings regarding the medical situation of their children. Adriana communicated feelings of guilt about the burden her treatment represented to her family, while Rodrigo’s mother used a fictional scenario to reassert that her decision about her child’s treatment was correct.
Conclusion
The concepts of the narrated, nonnarrated, and disnarrated allowed us to look at different forms of telling a story, thus providing greater insight into experiences of illness. The narrated dimension shed light on the issues that were explicit in the text, the nonnarrated pointed to what was erased or missing, and the disnarrated let us see what could have happened or what could happen in the future. In the case of the study presented here, the combination of these three ways of looking at children’s and parents’ narratives highlighted issues or themes (such as the time and energy parents spent arranging paperwork to secure their child’s care, the stress children experienced when they were not able to continue with their education, or parents’ need to reassure to themselves they were making correct choices) that we would have otherwise missed in our analysis.
This approach, however, is not without problems or shortfalls. The concepts of character and scene might seem too rigid for the analysis of some stories and might need adaptation depending on the research context. Not all narratives included disnarrated events; thus, this dimension might not always be relevant. In the analysis of what was nonnarrated, the reasons for effacing characters and scenes from the story can become misconstrued. In other words, the researcher might come to the conclusion that the storyteller has erased part of the story or failed to include certain details in the story because they created discomfort, when, actually, the storyteller thought they were irrelevant to the plot.
The construction of the stories could also be influenced by the context in which they are told or the audience to whom they are directed. Within health services settings, researchers are likely embedded in clinical environments where health care professionals distinguish between the patient as either a “good historian” whose illness narrative confirms the scientific evidence of laboratory results or, alternatively, as “bad historians” whose narratives confuse, falsify, underreport, or distract from diagnostician evidence of illness (DasGupta, 2006). Social norms guiding narrative construction in these medicalized settings, specifically in reference to nonnarrated events, might have been influenced by previous interview experiences. That is, stories that were discouraged, delegitimized, doubted, or ignored (Gubrium & Holstein, 2009) as non-relevant details for medical science might not have been recovered during the retelling of an illness narrative.
One way to deal with this situation could be to combine different research methods, allowing research participants to construct their stories in multiple ways. Another idea is to work with research participants during data analysis to continue to obtain their input regarding interpretation of their narratives. This stage of “participatory analysis” could continue to generate useful data regarding the participants’ views of the narrated, nonnarrated, and disnarrated in their own stories and could help reduce researcher bias during interpretation. Despite its limitations, we hope this approach sparks discussion in the field of health service research toward continuing to improve the tools we use to explore the storied nature of human experiences of illness.
Footnotes
Acknowledgements
We thank the families who participated in the study, FNDF for allowing us to carry out the interviews in their facilities, and Anne E. Pfister and Bruno Vindrola-Padros for commenting on earlier versions of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and or publication of this article: CONACYT, Fulbright-Garcia Robles, ISLAC, and the University of South Florida funded the doctoral research carried out by Cecilia Vindrola-Padros in Buenos Aires, Argentina.