
Abstract
In this study we explored the factors that affect assistive technology (AT) provision within the Navajo Nation using a qualitative approach to inquiry. Focus groups were held in which AT users discussed their awareness of AT and their need for, use of, and satisfaction with AT devices and services. Twenty-eight individuals who used wheelchairs, orthotics or prosthetics, hearing aids, communication aids, vision aids, and other AT participated in one of seven focus groups. Seven AT providers discussed the facilitators and barriers that affect AT provision. The findings revealed six themes common to both stakeholder groups and two additional themes for AT users. The central theme for AT users centered on (not) feeling understood; the central theme for AT providers revolved around the processes, activities, and roles the providers engaged in at times for different clients. Activities to increase awareness and to promote successful AT provision and satisfaction with AT devices were proposed.
Keywords
The World Health Organization (WHO, 2011) estimated that 15% of the world’s population, or one billion people, have a disability such as spinal cord injury; mobility disability; or auditory, visual (blind, low vision), communication (speech), or cognitive/learning impairment. Population statistics show that the number of individuals with disabilities worldwide is increasing because of population growth, medical advances, and the aging process; it is estimated that with life expectancy exceeding 70 years, individuals will spend an average of 8 years living with a disability (United Nations, 2006). Vulnerable populations such as those in resource-limited environments, those who are less educated, and those who are unemployed have a higher prevalence of disability, and individuals with disabilities are less likely to have opportunities for education and employment.
Assistive technology (AT) is any device, piece of equipment, software, or other tool that is used by individuals with disabilities to perform activities that might otherwise be difficult or impossible because of their disability. 1 AT provides an interface between the person and environment, enabling individuals to improve their functional abilities and become more independent; increase their potential to go to school, gain employment, participate with family and community; and to generally exercise human rights. Appropriate AT meets the user’s needs and environmental conditions; provides proper fit when relevant; is of high quality (safe, durable, and effective); and is available and can be accessed, maintained, and sustained in the country/region at the most economical and affordable price. 2 Appropriate AT has been found to be one of the most important factors in supporting activities and participation of individuals with disabilities (Borg, Lindström, & Larsson, 2009).
According to the United Nations Development Program (2007), 80% of people with disabilities (800 million) live in developing countries or resource-limited environments in which the infrastructure (material/physical, human, and financial resources) is underdeveloped or inadequate to support the provision of some or all AT products and services. Although the United States is a highly developed country, some areas in the country, such as tribal lands, qualify as resource-limited, with disparate disability statistics. For example, in the 2002 Survey of Income and Program Participation, Steinmetz (2006) reported that 18.1% of the United States population had some level of disability, compared to prevalence rates of 24.3% for American Indian/Alaskan Natives. According to the World Disability Report (WHO, 2011), the employment rate for Americans with disabilities was 38.1% compared to the overall employment rate for the working age population of 73.2%. In resource-limited environments, employment rates are probably even lower because it is often assumed that individuals with disabilities are unable to work, or that working environments are not accessible.
Navajo Nation
The Navajo Nation (NN) is geographically the largest Native American nation in the United States, encompassing more than 27,000 square miles in Arizona, New Mexico, and Utah, with a population greater than 173,000 (Arizona Rural Policy Institute, n.d.). Compared to the United States as a whole, the NN population is relatively younger, poorer, and unemployed; households are typically multigenerational or multifamily; and houses are generally smaller and in need of repair, often lacking basic utilities such as plumbing, electricity, and phone service. There are no urban areas on the reservation; population centers are generally clusters of housing around chapter houses (local governance units), schools, hospitals, and trading posts. Most roads remain unpaved and many people live more than 50 miles from the closest population center with a hospital. The estimated prevalence of disability within the NN ranges from 15% (RPI Consulting, 2011) to 30% of adults between ages 21 and 54, and 70% for those above 64 years of age (Landry, 2012). Ninety-one percent of Navajo individuals with disabilities are low-income, and 51% are unemployed (RPI Consulting).
The NN is a sovereign nation with its own governance structure, divided into 110 chapters and grouped into five agencies (administrative districts). The 88-member Navajo Nation Council (the government’s legislative branch, hereafter Tribal Council) is responsible for enacting policy, including disability policy, on behalf of constituents in the 110 chapters. Because of its sovereignty status, the general belief is that the NN does not have to comply with the Americans with Disabilities Act of 1990 (ADA, 2008), which prohibits discrimination against people with disabilities. However, in 1984, the Tribal Council enacted the Navajo Vocational Rehabilitation and Opportunities for the Handicapped Act (Navajo VR Act, 1984), which states that all Navajo people are entitled to fully participate in the economic, social, cultural, and political life, regardless of a person’s disability.
The health care delivery system in the NN is complex and convoluted, divided into eight health service units in which the main facility operates under the Navajo Area Indian Health Services (IHS) or is established as an independent, tribal hospital (“638 hospital”) under the Indian Self-Determination and Education Assistance Act (ISDEAA) to assume responsibility for health care previously offered by the federal government (ISDEAA, 2004). Not all facilities offer the same services. The Navajo Division of Health, the Navajo government public health authority, currently implements 14 programs, including a community health representative (CHR) program that provides outreach health care assistance and education at the community level. Navajo people can also seek services from a few private health providers or from a traditional medicine man.
Despite the significant impact AT can have for individuals with disabilities, 47% of American Indian and Alaska Natives reported unmet needs for AT; 40% had an assessment for a device but only 20% reported acquiring a device (Schacht, Gahungu, & Gallagher, 2002). Estimates of the need for AT devices and services in resource-limited environments contrast sharply with the capacity to provide AT, which is limited by several factors, including inadequate numbers of personnel to provide AT devices, service providers’ lack of awareness of AT, lack of maintenance and repair facilities, and lack of funding to support AT devices and AT services.
We know little about the availability of devices and services within the NN, about whether individuals with disabilities know what exists, about best practices, and about the quality and appropriateness of devices and services as perceived by AT users. Several reviews have included Navajo individuals with disabilities in larger American Indian population studies to understand disability and assess health care needs (Waldman, Perlman, & Kucine, 2006; Wall & Walz, 2003), with a focus on education, vocational rehabilitation, and independent living (Kauffman et al., 2003; Wall & Walz); strategies to promote more culturally appropriate rehabilitation and health care for American Indians with disabilities (Chino & DeBruyn, 2006; Lomay & Hinkelbein, 2006); or policy for individuals with disabilities (Dwyer, Fowler, Seekins, Locust, & Clay, 2000; Manson & Buchwald, 2007; Native American Disability Law Center [NCLC], 2007). Other studies have focused on factors contributing to vocational rehabilitation outcomes (Guy, 2009) and independent activity functioning in Navajo elderly (Fitzpatrick, Alemán, & Van Tran, 2008).
Few research studies have focused on multiple types of AT. Schacht et al. (2002) examined AT use, barriers to use, and consumer satisfaction regarding a variety of AT devices to improve employment outcomes. Quality of life for Navajo individuals who use wheelchairs (Overman, Knoki-Wilson, & Petri, 2009; Rothman, 2004), or who have visual impairments (McClure, Choi, Becker, Cioffi, & Mansberger, 2009), have also been studied. Stuart and Parette (2002) examined cultural considerations in the provision of communication aids from the perspectives of AT users, family, and service providers. Still, little is known about the needs and satisfaction of individuals with disabilities, or the important factors that influence AT outcomes from either the user or provider perspective.
A clear understanding of individuals with disabilities’ needs for, awareness of, and satisfaction with AT devices and services is an essential piece in learning how to improve the provision of AT so the greatest number of individuals with disabilities have access to AT and ultimately acquire it. Knowledge about the current situation is important for future advocacy and action; without this knowledge it is impossible to develop cost-effective strategies to improve conditions for individuals with disabilities (Øderud, Loeb, Eide, & Tyrmi, 2003). Thus, the purpose of our study was to explore factors that contribute to successful AT provision within the NN. Our main objectives were (a) to identify factors associated with AT manufacturing and distribution, or AT service provision that might influence the success of AT provision within the NN; and (b) to identify factors that might influence Navajo individuals with disabilities’ awareness of, access to, and acquisition of AT devices, and their use of and satisfaction with AT devices and services.
Methods
Research Design
Because we were interested in learning about the ways that individuals with disabilities within the Navajo Nation construct meaning of their experiences, we employed a social constructionism approach to inquiry (Crotty, 1998). We embraced the viewpoint that multiple realities exist and that participants would be able to orally share the meaning of their individual and collective experiences in accessing and using AT. We utilized focus groups as a method of data collection because they provided the opportunity for participants to explain their ideas and to build off of the ideas of others who held some shared experiences (Warr, 2005). Specifically, we selected a culturally appropriate form of focus groups—talking circles—to explore participants’ views about assistive technology provision within the Navajo Nation (Daley et al., 2010; Struthers, Hodge, Geishirt-Cantrell, & De Cora, 2003).
Drawing from community-based participatory research practices, we partnered with ASSIST! to Independence, a Navajo-owned independent living center located on the reservation. Partnering with ASSIST! allowed us to conduct the project with Navajo staff to ensure that the project was community-driven and culturally appropriate (Caldwell et al., 2005; Strickland, 1999). In collaboration with the ASSIST! board of directors, we sought to conduct the study in both Arizona and New Mexico, to include both IHS hospitals and independent (638) hospitals, and to include individuals with disabilities living close to and far from services. Four service units were selected according to their geographic location and type, as follows: Crownpoint, Chinle, Kayenta, and Tuba City. Selection of these four service units allowed us to recruit from 49 of the 110 NN chapters.
This project was approved by the Navajo Nation Human Research Review Board and also by Ethical and Independent Review Services, West Coast Division, Corte Madera, California. All research staff received training on the protection of human research subjects as well as training on conducting focus groups. All participants provided informed consent.
Participant Identification and Recruitment
Key stakeholders in the provision of AT include individuals with disabilities, AT designers, AT manufacturers, AT distributors, and AT service providers. On the Navajo reservation, transportation providers and CHRs also play key roles in AT provision. AT users were considered to be the primary stakeholder group able to identify factors that influence AT provision, and use and satisfaction with AT devices and services. Because they have direct interaction with AT providers, we also sought AT providers’ perceptions to allow us to identify the most important barriers to and facilitators of successful AT provision as perceived by both groups. Finally, we sought the input of other stakeholders (representatives of organizations and Navajo and United States government programs) to ensure that our findings were interpreted within the contexts in which they were created.
We utilized a variety of recruitment strategies for AT users that included collaboration with CHRs, posting flyers at chapter houses, making radio announcements and providing a toll-free telephone number, attending clinics at the hospitals, posting flyers at public community locations, attending social gatherings such as flea markets and sporting events, and mailing recruitment letters to clients of our local partner. Inclusion criteria were an adult or an adult caregiver of a child who used one or more AT and lived in one of the chapters within the selected health service units. The participant also had to be able to attend at the location of the focus group. The one exclusion criterion was a cognitive impairment, which would preclude providing informed consent or focus group participation.
We recruited manufacturers, suppliers, and service providers, including physical and occupational therapists, audiologists, ophthalmologists, and other related disciplines through departments at local hospital facilities and community clinics. We also invited transportation service providers as well as CHRs. The inclusion criterion was anyone directly involved in one or more aspects of AT provision within the NN.
AT-User and AT-Provider Focus Groups
Chinle, Arizona, was selected as the location of all focus groups. We held focus groups in either Navajo or English for individuals who used wheelchairs, prosthetics, orthotics, hearing or communication aids, vision aids, and other types of AT such as canes, walkers, and ramps. We organized AT-user focus groups to be composed of individuals who used similar types of AT. We also conducted two focus groups for AT providers to assess their perceptions about the current state of AT provision.
After obtaining informed consent, we completed the demographic forms for AT-user participants in an interview fashion; AT providers completed demographic forms independently. To maintain anonymity, we assigned a number to each participant. Following brief introductions, group facilitators led discussions guided by questions for AT users (see Supplemental Appendix SA, available online at qhr.sagepub.com/supplemental) or for AT providers (see Supplemental Appendix SB, available online at qhr.sagepub.com/supplemental). One cofacilitator noted key discussion points on a flip chart throughout the session. After discussing all questions, participants ranked their most important needs for successful AT provision, and AT users also ranked the items that most affected their satisfaction, based on the key discussion points. We sought group consensus on ranking where possible. All focus groups were audiotaped (primary method) and video-recorded (for review during transcription). All focus group discussions lasted approximately 4 hours, with a short break for lunch. One cofacilitator took field notes to record the tone of the focus group, the nature of the discussion, and nonverbal communication among focus groups participants.
Data Analysis for AT-User and AT-Provider Focus Groups
Audio recordings and focus group notes from the English-speaking focus group sessions were transcribed verbatim and reviewed by a second individual for accuracy. Data collected from the AT-user focus groups conducted in Navajo were simultaneously translated to English and transcribed. To ensure accuracy of our transcriptions, one Navajo-speaking staff member transcribed the Navajo focus group discussions and a Navajo-speaking professional transcriber subsequently reviewed the transcripts.
The process of data analysis was guided by interpretive description, as described by Thorne (2008). We coded each focus group transcript, guided by the question: What is this about? (Hunt, 2009; Thorne, Kirkham, & O’Flynn-Magee, 2004). Initial coding remained data-near (Sandelowski, 2010) to avoid premature interpretation of findings. Codes were then reread and grouped into patterned topics (Sandelowski & Barroso, 2003) addressed in individual focus groups. We constructed a narrative summary for each focus group that identified the latent theme(s) of the group. Using constant comparative methods (Thorne, 2000), we compared findings within and between groups, guided by the question: How are these themes/experiences influenced by being an AT user in the Navajo Nation? Finally, we integrated participants’ demographic data into the data analysis to examine and understand unique patterns. Specific comparisons were made to identify unique themes or experiences for specific subsets of participants (AT user vs. AT provider groups, AT type, rural/remote location of residence, socioeconomic status, and service unit).
To gain a visual understanding of travel involved for individuals with disabilities to receive AT services (i.e., within their service unit vs. other service units vs. off reservation), we reviewed transcripts for mention of travel for services and recorded each location for each participant. We then mapped each participant’s travel from his or her home to each service location on a map of the Navajo Nation using Microsoft Word’s drawing tools feature. Three maps were generated to depict participant travel: wheelchairs; orthotics and prosthetics; and hearing, speech, and vision.
Results
Group Composition
Three Navajo project staff conducted four focus groups for AT users who spoke Navajo: wheelchair (n = 6), orthotics/prosthetics (n = 2), hearing (n = 5), and other AT (n = 3). Three focus groups were conducted by the first author for AT users who spoke English: wheelchair (n = 4), orthotics/prosthetics (n = 4), and hearing/vision (n = 4). Overall, we had AT users from the selected service units as follows: Chinle (n = 22), Kayenta (n = 1), Tuba City (n = 4), and Crownpoint (n = 1).
Across all AT-user focus groups, 15 women, 12 men, and 1 parent of a child who used AT participated. The mean age for adult AT users was Mage = 59.5 years, with age ranges as follows: 20 to 40 years (n = 3), 41 to 60 years (n = 11), and greater than 60 years (n = 13). Across all groups, participants reported their primary AT as follows: manual wheelchair (n = 8), power wheelchair (n = 2), prosthesis (n = 2), orthosis (n = 4), hearing AT (n = 7), vision AT (n = 3), and other AT (e.g., cane or walker; n = 2). The participants’ experiences with AT provision ranged from several months to more than 45 years (< 1year, n = 3; 1 to 5 years, n = 5; 6 to 10years, n = 5; 11 to 20 years, n = 4; 21 to 30 years, n = 7; and more than 45 years, n = 4; Myrs-diagnosis = 15 years); 3 participants reported being disabled since birth.
The first AT-provider focus group (n = 5) included representatives from audiology, prosthetics and orthotics, and two transportation providers. All participants of this group provided a service directly to the AT user. The second AT-provider focus group (n = 2) represented vendors/suppliers of AT devices, including wheelchairs, walkers, crutches and canes, and durable medical equipment. One participant represented a large national company with a local presence near the reservation; the second participant represented a smaller local company.
AT providers reported a general lack of awareness of other providers on the reservation. The first AT-provider group was aware of some other providers (e.g., skilled nursing facilities, the CHR program, funding programs, Children’s Rehabilitative Services, Navajo Area Agency on Aging, or other transportation providers) but unaware of programs such as independent living, vocational rehabilitation, AT loan programs, and disability-specific programs, both on and off the reservation. The AT suppliers in the second AT-provider focus group identified other suppliers that provided AT within the NN but were located off the reservation; however, they were not aware of the CHR program.
Findings
Living with a disability
AT users provided rich descriptions of how they experienced life with a disability within the NN. Most participants described an acquired rather than a congenital disability, and thus the experience of disability was a sudden loss and change from a previously active life. Living with a disability limited participation in daily life and affected their roles, activities, and relationships. They expressed frustration, loss, and depression at their inability to be active and contribute to family or social activities, which led to a feeling of uselessness. One individual with a hearing impairment remarked, “You see others visiting and you sit there and not participate.” Some participants perceived they were a burden to family, felt abandoned by their family members, and described the despair and loneliness that accompanied the sense of abandonment: Sometimes I just start crying and then I get so frustrated and I say, “Why do I have to be the one that is hurt all the time?” Nobody around, no family. Nobody to care for me. This is just too hard for me.
Although living with a disability took an emotional and physical toll on participants, the additional financial costs exacerbated the experience. Many participants described the difficult choices they needed to make between paying for needed medication or AT supplies or purchasing food when income was severely limited. More than 70% of participants (20/28) reported an income of less than $10,000/year, which was below the 2012 United States poverty line. Some participants were unable to continue to work, or had lost their job, yet needed to purchase AT through their own means.
Despite challenges, participants highlighted ways they addressed adversity, often describing a turning point in their attitude when they came to accept there was “life beyond disability.” Being active and involved in family and community life, (re-)engaging in meaningful activities, and developing a sense of self-reliance were ways that participants addressed the challenges of living with a disability. Some participants created new meaning and purpose for themselves through reciprocity and caregiving for others.
Disabled by the inadequate infrastructure
Eighty-six percent of participants reported living in a rural community (n = 9) or remote/rural area (n = 15), with 57% living more than 20 miles from the closest town. For AT users, the lack of infrastructure and the environmental barriers were the fundamental source of disablement. Participants described how the lack of basic communication systems, impassable unpaved roads, and inaccessible public environments created barriers to their participation in their community and society. Participants expressed that improved built-environment accessibility would improve their community participation and engagement: “Like a lot of them want to go voting but they don’t have that access—to vote or to go be a part of the chapter meetings.” However, the most pervasive infrastructure issue was inadequate housing; homes were in a state of disrepair, with many lacking running water and electricity: We have a house but we don’t have a shower, so that is one of the other needs we have. The house has water piped in and has plumbing and all the bathroom fixtures, but no water to shower with or flush the toilet with. We don’t even have a water barrel or water tank.
Many participants needed a basic ramp installed to safely enter and exit their home. Inside the house, inaccessible spaces precluded access to essential spaces, such as the bathroom, and safety equipment such as handrails in the bath or shower was absent. Many AT-user participants experienced lengthy waits for repairs, upgrades, or a move to an accessible home. When home adaptations had been completed, some expressed concern about the quality of the work (“The installers did a shoddy job”), and thus equipment designed for safety became a safety hazard. Most perceived a lack of available funding for essential housing modifications, that their efforts to request modifications were futile, and that others were prioritized for housing. Overall, AT-user participants were frustrated and disheartened by the inability to use their home in safe and functional ways: Where I live right now is a house that we are renting from NHA [Navajo Housing Authority]; there is nothing. In the bathroom, when I take a shower, there is nothing to hold on to. I get scared when I go in there. I have a chair so I can use that, but the bathroom is very unsafe for people like us.
AT providers described the compounding effect of inadequate infrastructure. For example, one AT provider explained that lack of clean running water affected the hygiene of those with amputations; this resulted in an inability to keep stump socks clean, led to skin breakdown and infection, and ultimately resulted in the need for further amputation.
For AT providers, lack of effective communication channels and limited all-weather road access were viewed as the most challenging infrastructure issues, because this meant difficulty in locating the whereabouts of clients when the driver arrived with their device, and challenging navigation of the terrain when rain or snow made dirt roads impassable. AT providers shared that roads were unmapped and street signs were nonexistent.
AT meaning, use, and benefits
AT-user participants described a pragmatic approach to AT use, choice, and selection; they primarily focused on usefulness, comfort, and fit within their environment. Participants were grateful for and greatly valued their AT because it served to restore lost function and promote their independence, autonomy, and self-confidence: “So I think a lot of the devices I have really enhanced being able to be more independent, and that really helps my self-esteem, because if I can do more things by myself then I can capture the world.” Participants described how AT promoted activity engagement and participation; for example, one individual with a prosthetic leg reflected, “This leg has helped me out a lot. . . . So now I can go outside and walk around and watch the kids [children] outside.”
Whereas most participants embraced the functional benefits of their AT, the experience of hearing aid users was one of unmet expectations related to hearing aid durability and effectiveness: “This device that I have, that is in my ear now, I liked it when I received it. Now I feel it is just in my way. When everyone’s talking right now it seems everyone has a pitched voice.” Hearing aids they received did not function well in all situations, and participants were still unable to participate in certain social events, such as large group meetings.
AT–person–environment appropriateness
The challenge of finding appropriate AT to address the environmental conditions was highlighted by all AT-user participants: “I cannot use my wheelchair in bad conditions, like when it’s icy, muddy, or snowing.” A prosthetic user emphasized the challenges: “I can’t really walk on the sand and the rocks.” Those who tried to use their device in the outdoor environment expressed concern for their safety; for example, one power wheelchair user described how she had to crawl home after getting stuck in soft dirt. The lack of appropriate AT led to underutilization or nonuse of the device, resulting in limited ability to engage in community life.
Recognizing the lack of compatibility between AT and the environmental conditions, decisions had to be made about the best choice. For example, participants discussed how “stickers” caused flat tires on their wheelchair, and thus although solid tires were better in that situation, air-filled tires were better for surmounting rocks. Experiential learning and considering the trade-offs were required when deciding on the most appropriate technology. AT providers described how they used knowledge of their clients’ context to supply AT: I don’t think we ever did a myoelectric device on anyone because, first of all it’s too expensive, and for what people normally do around here it is not appropriate. It needs to be cleaned daily and a lot of our patients do not have electric or running water, and also they do a lot of rough things like chop wood and that kind of stuff.
Out-of-context AT assessments (e.g., in larger urban centers) resulted in an incongruence between the AT–person–environment; for example, one visually impaired participant was taught to use a white cane in an urban context, but he was unable to use it when he returned home. Participants recommended that extended, in-context trial periods with AT be required: “It might be appropriate for the cities where it is paved, but if they really want to test it out they should give it to someone to use for like a whole year out here.”
Policies dictating replacement cycles for AT disregarded environmental conditions; for example, a replacement cycle for wheelchairs was every 5 years, and participants of both groups believed that policies were designed for those living in cities where the environmental conditions are entirely different. One AT provider commented, “We see some people bring wheelchairs that are six months old. They beat the heck out of them. After six months it looks like it was hit by a car.” While AT-user participants expressed keen interest in acquiring new, more appropriate AT, this was tempered by the AT providers (suppliers) because they indicated that they would only be able to source more-appropriate AT if it was requested by the tribe, and if they could bill for the product.
AT service and maintenance
All focus groups raised AT maintenance and service issues; however, the AT-user and AT-provider groups differed in their perspectives on the quality and nature of the service provided. AT-user participants with a longer history of disability noted how previously existing, useful programs had been cut back. In the past, services had been local and easily accessible: “When we had our appointments with physical therapy a representative is on site here to fix everything: brakes, tires, realignment. This setup was ideal and convenient for us, and again this service is no longer available.”
AT devices often were provided without ensuring that regular maintenance or supplies were available. The financial cost associated with hearing aid repairs and batteries was a specific point of concern raised by those with hearing loss: If I don’t have extra [batteries] on hand, then I have no hearing aid because I purchase my batteries from Gallup (New Mexico). It takes us a while to go into Gallup . . . I have to make a special trip. This device takes a lot of upkeep.
When repairs were needed, the approval process was lengthy and fraught with restrictions and delays. Although some participants reported completing minor repairs themselves, those devices with more complex parts and electronics required specialized service, and a local maintenance person was identified as an important need.
Although some AT users received education and training on device use, it often occurred out of context and thus had limited applicability. A few AT users had received education on device use upon initial receipt; one participant valued the context-specific mobility training he received from a blind peer, who “came around [into his own environment] to teach me”; however, many indicated an overall lack of training or explanation received on device use and maintenance.
In contrast, AT providers perceived that they went to great lengths to provide client-focused services. AT providers stated they provided choice when possible, worked to be responsive to needs and concerns, tailored their education on device use (using pictures and educating the family) and provided extra service (e.g., staying open late to accommodate individuals who had traveled for their appointment). Although waiting lists were commonplace, AT providers perceived that waiting was because of a lack of service providers.
Overall, a lack of attention to maintenance because of inability to afford costs or access maintenance supplies meant being left without their AT. Although the groups differed in terms of their perceptions of available services, both groups agreed that additional local services would be beneficial to reduce the travel demands on clients, to ensure more in-context and timely service provision, and to reduce the “downtime” of AT use.
Changing and limited insurance coverage
Participants discussed how differences existed in eligibility depending on whether one lived on the New Mexico or Arizona side of the reservation. Differing policies resulted in complex, fragmented application processes that participants had to negotiate for equipment access, replacement, and repair, and case managers added complexity and time to the process. Furthermore, AT users reported that recent changes and reductions in eligibility were not well conveyed, resulting in eligibility confusion and frequent denial of equipment or services: “If you live on the res [NN reservation], you have to go this way, that way, this way, just to get to where you want—just to get something done.”
A funding eligibility paradox was discussed in the AT-user focus groups: Participants explained that if they tried to be financially independent they were no longer eligible for some things, yet the income they received was not adequate to cover disability-related expenses. Eligibility for care assistance was found to be equally challenging. Approval for care assistance was based on an external assessment of independence; assessment criteria did not consider the individual’s self-perceived assessment, nor did it address the additional needs that emerged when aging with a disability. A pattern of being “not quite” disabled, poor, sick, mobility-challenged, or old enough to qualify for support continued to weave itself through many situations, including access and eligibility for AT, transportation, home care, and food stamps. AT providers also identified issues related to changing eligibility criteria and reduced services. They reported that policies and eligibility requirements were device-, age-, and state specific and underwent continuous changes, creating an ongoing perception that priorities were driven by cost containment.
AT user participants described the innovative ways they sourced AT. Whereas some people reported receiving their equipment through traditional means (e.g., hospital or vendors, paid for by government or insurance companies), others reported purchasing their devices second hand at flea markets, receiving them as a donation from their church, or acquiring them from a deceased relative.
Transportation
Transportation was viewed as a necessity on the reservation, where people are geographically dispersed and live primarily in rural and remote locations. Of the AT-user participants, only 10 (36%) owned their own car; others utilized a driver (including transport service), borrowed a car, walked, or hitchhiked. Reductions in transportation services were detrimental because transportation was seen as a crucial link for individuals with disabilities living on the reservation seeking to engage in their community. Many participants shared how they were no longer eligible for medical transport based on income or health condition. One said, “They tell me I cannot get a ride to the clinic because I make too much money. It is very frustrating because I have a total disability with my vision.” Another said, “Yes, there is medical transport but our hearing doesn’t qualify us for it. . . . For appointments for hearing and eye clinic it doesn’t qualify you for medical transport.”
AT providers supported the AT-user assertions about transportation challenges faced by individuals with disabilities, and identified that the limited reimbursement available for longer trips to see specialists resulted in companies making financially based decisions not to take on those bookings. Routine situations were perceived to become urgent and costly because of a lack of available transport services: The whole reason for nonemergency transportation is for them to get their medication, for them to get to their follow-up appointments. If they’ve missed their medication, [or] if they’ve missed their follow-up appointments because they don’t have transportation, a month later they might end up in the ER [emergency room].
Importance of (need for) local, consistent, culturally appropriate health services/businesses
Both stakeholder groups highlighted the crucial need for local, culturally appropriate services. Although both groups spoke about the importance of Navajo fluency and ease of access, the AT-user group added a desire for health provider consistency, colocation of services, and easier access to expertise. Previously existing services that met these criteria had been discontinued because of a lack of funding, and participants lamented the loss of expert knowledge, convenience, and holistic care they had received. Throughout the focus groups, concern was raised about the lack of consistency with on-reservation physicians that precluded the development of trusting, long-term relationships. The participants explained that they needed to explain their situation to each physician: They say, “How painful is it? Can you feel this?” and I’m like, I thought you were a doctor. You should know I’m a quad [quadriplegic] and I can’t feel to a certain point on down. But it’s like that all the time, every time.
Most participants felt that the CHR program did not meet their needs. AT-user participants reported that CHRs visited only certain people, and that requests to be added to the visitation list were denied. Some participants were told they were ineligible because they had family support, even though the family was not always available. The few participants receiving services through the CHR program felt that visits were hurried and insufficient, not lasting long enough to discuss their issues.
Culturally relevant health providers and options were desired, including access to Navajo healing ceremonies, a medicine man, translators fluent in different Navajo dialects, and care providers familiar with the needs of American Indians. Even though participants preferred local health care access, the quality of off-reservation health care service was generally felt to be superior, providing more immediate assistance with their needs. Conversely, accessing on-reservation services meant waiting (e.g., waiting all day at the pharmacy to pick up medicine).
AT providers believed that the need to travel for health services negatively affected their clients’ quality of life. Sometimes providers felt there to be a lack of awareness of existing local services, resulting in referrals off reservation and unnecessary travel. Traveling long distances to other health service units on the reservation, and to health care facilities off reservation to receive AT services and/or devices was reported by AT users in all focus groups. Although there was an identified need for local businesses, AT providers described barriers to this: First of all, where will we be located there? We have to deal with our building restrictions as far as all the permits, water, and everything else. So I think that’s why you do not see providers on the reservation.
Alongside the need for local business expansion, participants expressed the need for more AT providers, because increased business development without concomitant AT provider availability would simply serve to increase already long waiting lists. One necessary element to increase local business development was to ensure that reimbursement for services was forthcoming and timely.
Central Theme for AT-User Focus Groups: (Not) Feeling Understood
Overall, the central theme that underscored the AT-user participants’ discourse was the issue of (not) feeling understood (see Figure 1). Not feeling understood meant that others (i.e., society, government, insurers, health providers) lacked understanding of the individuals with disabilities’ needs, issues, and concerns, and demonstrated this by not taking action or fulfilling promises. This lack of understanding was linked to a lack of awareness by others. There was the sense that if (when) others became aware of their needs, issues, and concerns, they (others) would understand, and participants would then feel understood. There were two variations of this cycle: lacking awareness–not understanding–not feeling understood, and awareness–understanding–feeling understood. Although the majority of discourse around this central theme revolved around the former, there were specific incidents, people, and efforts that exemplified the latter and specific suggestions and indications of how the cycle of awareness–understanding–being understood might be fortified and reinforced.
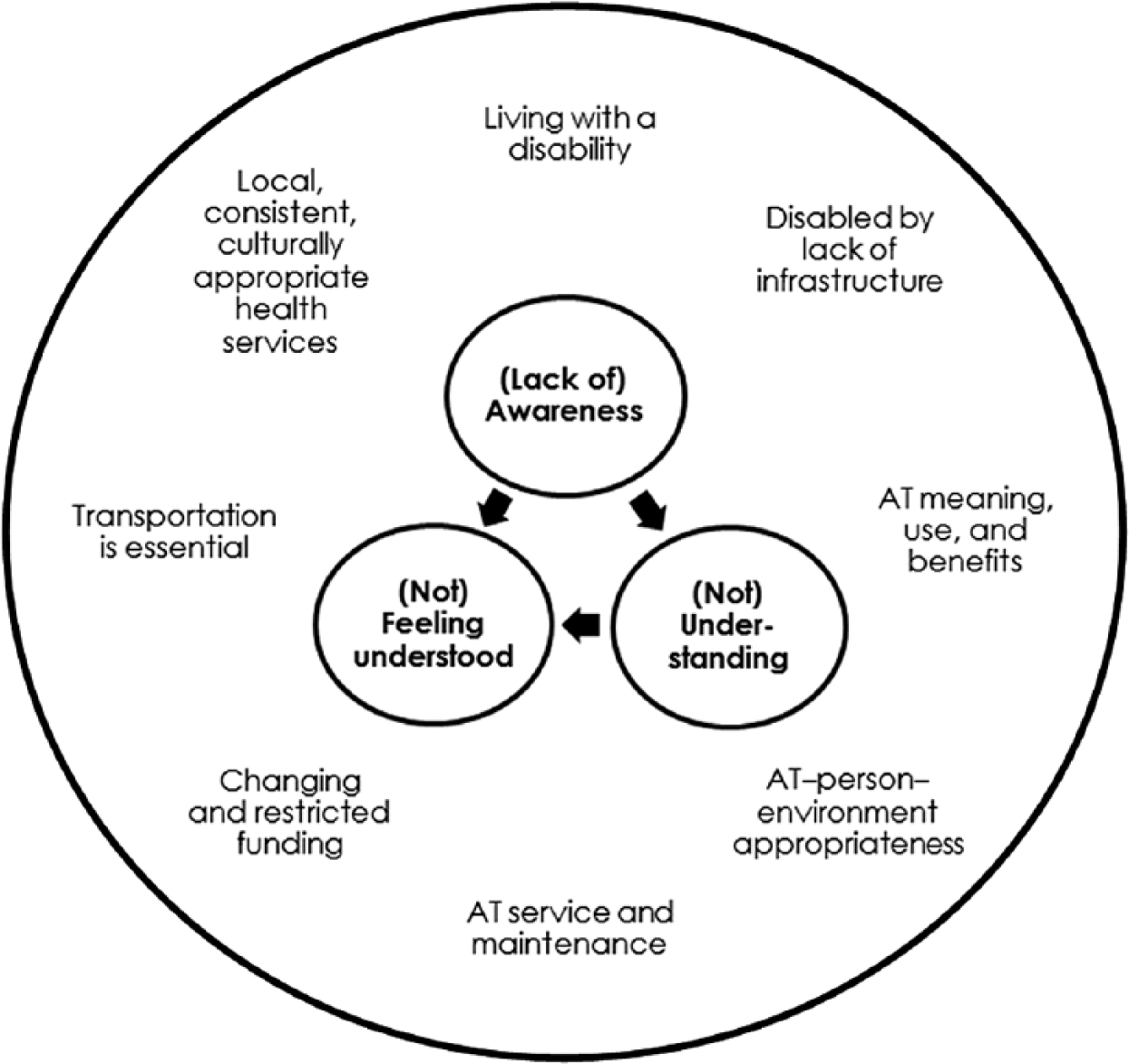
Model depicting central and supporting themes for assistive technology (AT) users.
Lack of awareness–not understanding–not feeling understood
Participants discussed how, despite what the authorities said, their actions did not match their words. AT-user participants felt they were not always understood or prioritized in society: Government [Navajo] says disability is priority but does not follow through with money, help, or assistance for those with low income. They usually say in every chapter meeting that disability is their first priority. Whenever money is allocated to the chapter house we usually get left out. Not enough for the disabled.
AT users felt overlooked and misunderstood by society in general, and actions taken by others demonstrated a lack of awareness and understanding. Participants believed they were not understood at a local level, in part because tribal authorities did not always hear their concerns: Even the tribe, I don’t know if they can do something about it. You ask them to do things like this and they will never help you. They don’t listen to you, they just ignore you. That is how they are.
Even though they wanted to be self-sufficient and independent, when society and officials were not aware of and thus did not understand their issues, individuals with disabilities could not receive the help they felt they needed. Participants expressed a sense of futility when they had asked for assistance but were denied.
Participants felt they lacked opportunity to voice their concerns, in part because they felt disempowered as individuals with disabilities. Furthermore they felt that in the past they had the opportunity to express their concerns, but recent changes in chapter structure meant they lacked the opportunity to express their voice in local government matters: The officers . . . are the ones that are the core at the chapter meetings, and no one from the audience or outside can speak unless one of these people put you on the agenda about two or three weeks ahead. . . . The chapter officials are the ones that control the meetings, and that control the funding and give out different services.
AT-user participants felt that they lacked decisional autonomy to get their needs met; for example, some providers made decisions about the type of mobility device provided while disregarding individual requests and needs: I feel it’s very important the doctors listen to our concerns. I have expressed to my doctor that I am in a need of a wheelchair. Once darkness comes it’s hard for me to move about in my home, and I desire a wheelchair. I think I can move about my home in a lightweight and narrow wheelchair. I need it for those purposes. I make a request to get a narrow wheelchair so I can get easily around my house. They don’t listen to me; they tell me I don’t need it. In reality, I do.
Despite holding out hope that their concerns would be heard by officials, they felt disillusioned by unfulfilled promises of help and support, which had resulted in a lack of trust in the word of authorities. Some participants felt that although the NN government was able to apply for targeted federal funds, those funds were not allocated to the people themselves: Apparently they [NN government officials] would say that they are getting money from this place and that place for the elderly and for the disabled, but what happened to the money? People don’t get help. Disabled people don’t get help.
The participants wanted transparency in funding availability and decision making, and overall, some felt that the tribal government could do more to support the needs of persons with disabilities.
Awareness–understanding–feeling understood
The cycle of lack of awareness–not understanding–not feeling understood was clearly contrasted in a few situations. For the most part, these contrasts were not programs or policies, but rather specifically named individuals who were aware of the issues faced by the AT-user participants, had a personal connection with an individual with a disability, were disabled themselves, or lived on the reservation. For example, the understanding of one AT provider was described as follows: [Name] used to do all the maintenance out here. She lives on the reservation. She knows how difficult it is. She understands because she has a nephew in a wheelchair. So she understands the need for it and she understands how hard it is when our chairs break down, so she goes out of her way to fix our stuff.
People who understood demonstrated caring through behaviors such as being sensitive and responsive to the unique needs of individuals with disabilities and treating individuals with disabilities with respect, even if it meant not following rules and procedures. For example, participants contrasted different medical transport drivers, some who were rule-bound and inflexible and some who understood (e.g., respecting their need to eat while traveling). Furthermore, AT devices designed by someone with a disability were deemed more appropriate because that person understood: The stuff that is made by people that are disabled, like you’re saying this chair was made by someone with a spinal cord injury. I think that is more appropriate than somebody that is just producing [wheelchairs] and they are not disabled themselves.
AT-user participants described the advocacy, education, and peer-support strategies they undertook to enhance the cycle of feeling understood: Tomorrow I go back to Tuba City. I’m going to speak to the Tuba City administration and raise my voice. If I have to take a malpractice suit I will. This is what we need. Advocacy. We need as handicap people to have some kind of advocacy. It would help in the Navajo system.
Others believed that advocacy efforts needed to be developed in collaboration with others, and that advocacy coalitions needed to be distinct from government.
Educating others and increasing societal awareness of the issues was a second strategy used to feel understood. Some felt that media attention would be useful in calling awareness to the issues: “Somehow I hope that the concerns that we are expressing here will come up in the papers, all over the media. . . . That is the only way that a lot can be done.”
Finally, participants discussed the lack of opportunity to discuss the issues they faced with others who could empathize. The opportunity to discuss issues with their peers in the research focus groups opened up the possibility that this would be a useful strategy for feeling listened to and understood: When I talk to someone, you know someone that will listen, I will feel better. Sometimes it is hard for me to talk to somebody because nobody’s never around. . . . But today I feel better. I’ve enjoyed being here. I enjoyed talking. This way we learn things from one another and who did what to get better.
Central Theme for AT-Provider Focus Groups: Roles and Responsibilities
The two AT-provider focus groups differed in their focus and priorities. One group consisted of front-line AT providers and representatives of a locally owned and operated medical transport company who strove to meet the needs of their clients (individuals with disabilities) rather than the funder. Participants in the second AT-provider focus group represented AT-device supply companies who clearly stated that the ease, predictability, and speed of reimbursement was necessary for the success of their business. Thus, the latter group viewed service providers (e.g., doctors, therapists) as their primary clients, although at times individuals with a disability became their primary clients. The central theme of the AT-provider focus groups revolved around the processes, activities, and roles the providers engaged in at times for different clients (see Figure 2).
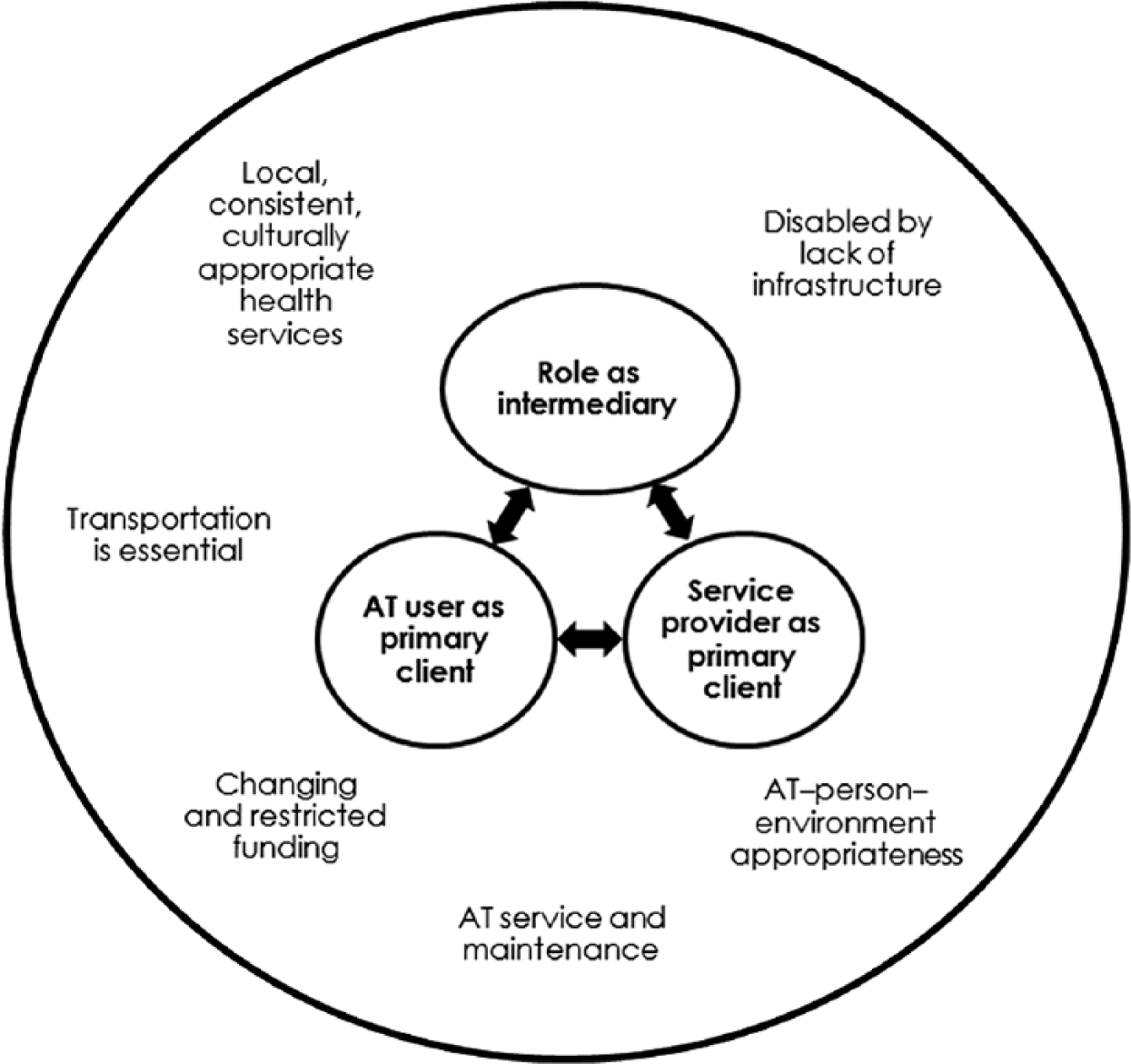
Model depicting central and supporting themes for assistive technology (AT) providers.
Individual with a disability as primary client
Those who provided direct services strove to be client focused; responding to client needs was viewed as a key to success. They modified their operating hours, traveled to the individual with a disability, employed Navajo-speaking staff, conducted thorough assessments to provide the most appropriate AT device, provided choice of AT whenever possible, and educated clients. Flexibility in policy application was important; for example, one participant described how her department provided services beyond the warranty period, and wouldn’t deny service to people from other health service units. Customer service overrode profit, as described by a transportation company representative: We do courtesy rides when they’re prearranged and we don’t get reimbursed from anybody. If we are in the area and we do have a driver . . . if the facility calls then we will do that, courtesy rides.
Finally, ensuring that they were able to meet regulatory, safety, ongoing education, and credentialing requirements was an important contributor to their business success.
Service provider as primary client
For those who viewed service providers as their primary client, profit and financial viability of the business was the priority. As for-profit companies, their primary role was to deliver and set up the equipment prescribed by the service providers, and thus any other needs of or requests from the individual with a disability were secondary: I would say communication with the client [referring to the individual with a disability] is on the low end because most of them . . . . That’s unfortunate that the discussion of what the patient really needs is the bottom. Nobody really looks at that because we’re trying to impress more of the doctors and staff that are doing the orders, than what the patient really needs. . . . You have to get the doctor to buy in first.
A successful business was defined by financial viability. Participants relayed how it might take up to 2 years to receive payment for a claim while insurance and health plan providers battled over responsibility for payment. Often, service provider requests and accompanying documentation were incomplete, creating further delays.
The role of intermediary
In many instances, the AT providers took on the role of intermediary between the client (individual with a disability) and others (insurers, health care providers); for example, some relayed how they would deliver equipment ordered by a doctor, but the client would be unaware that the request had even been made. Sometimes, the AT-provider participants provided referral services and education about available resources, based on their observations: A lot of the drivers, they do observe [the client], and let’s say if they do have an elder who cannot help herself or can’t do anything for herself, they will let us know. . . . We will call the home health care agency and let them know that this person probably needs somebody. Either that, or we will let the client know that there are services or resources out there that they can utilize.
The AT providers were caught in the middle of policies developed at a systems level. Although not responsible for insurance eligibility or funding cuts, the AT providers often became the point of contact for conveying these situations to the clients. Because of ineffective communication mechanisms between insurers and insured, AT providers served an important and unrecognized role as a communication link between the insurers/payers and the individuals with disabilities, having to explain the complexities of eligibility: “And so a lot of times what our people do is they have to explain to them [clients] what kind of services are covered under their insurance, and they don’t understand, a lot of them.”
Discussion
This study provided a unique examination of the experiences and opportunities AT users face living within the NN, with supporting evidence provided by the AT providers. The central themes of the two sets of focus groups intersect in several key ways. The experience of feeling understood described in the AT-user groups referred to the importance participants placed on feeling validated and recognized as a unique person with unique needs. Participants felt understood when others listened to them, treated them with respect, responded to expressed needs, and demonstrated they (others) were trustworthy. Often, the individuals with disabilities felt most understood when others held some similarity to them in life experience (e.g., lived on the reservation, had a disability).
The central theme of individual with disability as client emerging from the AT-provider groups complemented the AT users’ feeling understood theme in that AT providers strove to understand their client (individual with disability) by responding to individual needs, demonstrating flexibility in services, and attempting to be responsive in their service provision. The role of intermediary in the AT-provider groups linked closely to the theme of awareness and understanding in the AT-user groups: The AT providers tried to share their understanding of policies and eligibility through their intermediary role, and in doing so tried to raise the awareness and understanding of the individuals with disabilities.
The results of this study align with other studies related to rehabilitation and/or AT provision on the Navajo reservation or in other resource-limited environments. It is clear from our study that the use of AT was an important means of enablement for individuals with disabilities. AT was valued for its pragmatic role in replacing lost function or enhancing existing function. Similar to other studies on the meaning of AT (Boschen, Tonack, & Gargaro, 2003; Brandt, Iwarsson, & Stahle, 2004; Ripat & Woodgate, 2012), AT was viewed as a means to engage in activities of choice and meaning. The importance of AT as a means to inclusion and equality of human rights has been well established (Borg, Lindström, & Larsson, 2009; United Nations, n.d.), and participants in our study shared how they used AT as a tool for inclusion in family, conversations, and community.
Despite the importance placed on AT in the lives of individuals with disabilities within the NN, significant challenges around awareness of, access to, and acquisition of AT were highlighted by the multiple stakeholders. The current study findings concur with the findings of Schacht et al. (2002), who identified limited awareness, affordability, and availability of AT devices and services for the broader population of American Indian/Alaska Natives.
Even those who do acquire AT devices might have limited use of them because environmental conditions often affect the usability of AT products. Consistent with other literature about resource-limited environments, the lack of accessible infrastructure (physical, natural, built, institutional, policy, financial, governmental, and communication) curtails access to and use of AT. From a social determinants of health framework, it was clear that many inequities existed in the AT-user participants’ lives. Inadequate housing, poverty, food insecurity, and limited access to health care were identified as areas of concern by participants, and they were limited in their ability to draw on the social factors that contribute to overall health (Public Health Agency of Canada, 2001; WHO, n.d.).
Rothman (2004) identified that individuals with disabilities in the NN face many challenges, including lack of available public transportation, long distances to receive services, inadequate housing, lack of utilities, lack of basic communication, poverty, lack of health care providers, and lack of culturally appropriate services. According to a 2009 survey, more than 34,000 new homes were needed in the NN because of overcrowding and because homes were dilapidated and beyond repair (RPI Consulting, 2011). More than 51% of the households surveyed reported lacking complete bathroom facilities, and more than 55% reported lacking complete kitchen facilities. Electric service was available to 80% of the homes, although this was well below the national average of 98%. Landline telephone service remains available only near population centers, and cellular service is sporadic. It is disconcerting that almost a decade later, these issues were found to still exist, impacting the lives and curtailing the opportunities afforded individuals with disabilities in the NN.
Barriers to access to and acquisition of AT by individuals with disabilities represent only one aspect of the problem; without an AT provision system designed for the specific context, it is impossible to appropriately meet the needs of the individuals it must serve. Extant literature highlights a few attempts at the creation of AT services and programs within the NN; for example, Norton (2002) described the development and evaluation of Navajo-ABLE, an AT loan program targeted at provision of AT devices and services to children with disabilities within the NN. Although evaluation results were promising, it is unclear whether this program was sustained. Rothman (2004) described the value Navajo individuals with disabilities found in a support group; programs such as this would provide valuable social and peer support for individuals with disabilities, as highlighted by the participants in our study. He also discussed the value of a multidisciplinary team approach to health care, just as some of the participants in our study praised the spinal cord injury clinics as the exemplar of the desired services.
AT access and use issues also intersected with the larger, system-wide health care infrastructure challenges. Lack of coordination among complex, multiple health and social service systems has been highlighted as a particular challenge (Overman et al., 2009; Rothman, 2004). Off-reservation referrals and missed home visits might have been caused, in part, by the provider participants’ limited awareness, and speaks to the continued need for better communication and more coordination of efforts between AT providers. Prohibitive transportation costs and limited availability (Guy, 2009; Overman et al.), and long distances to receive services (Rothman) prevented individuals with disabilities from accessing timely and needed AT services. Issues related to difficulty with repair and maintenance and limited counseling and support services (Overman et al.) were also emphasized by the participants.
Similar to our findings, the importance of accessible housing and communities was identified in a study of First Nations individuals living on a reservation in Canada, where lack of access precluded ability to engage in important cultural community activities (Wearmouth & Wielandt, 2009). Lack of enforcement of disability legislation (as cited in Rothman, 2004) continues to be a challenge, as reported by participants in our study and confirmed by other stakeholders within the NN. There is a need to overcome the obstacles faced by Navajo individuals with disabilities, because of both the environmental conditions that exist within the NN and those that exist within the health care system, to improve AT provision and provide individuals with disabilities within the NN increased access to more appropriate AT devices and services.
Our findings are consistent with the literature on delivering culturally appropriate AT services (Chino & DeBruyn, 2006; Lomay & Hinkelbein, 2006). Participants in our study highlighted the importance of being “known,” and identified culturally congruent elements of AT service provision that would promote effective AT use by Navajo individuals with disabilities: communication in native language and dialect, access to traditional medicine, consistent medical personnel, education delivered in various formats, in-context training, and inclusion of both client and caregiver opinions in AT device selection.
Devices need to be available that are appropriate for the unique geographical challenges of living on the reservation. There are some research reports accounting challenges with existing AT devices and efforts at designing appropriate technology for use in resource-limited environments (Lysack, Wyss, Packer, Mulholland, & Panchal, 1999; Pearlman, Cooper, Chhabra, & Jefferds, 2009; Stuart & Parette, 2002; Zipfel, Cooper, Pearlman, Cooper, & McCartney, 2007). Similarly, in future research it would be prudent to explore the environmental appropriateness of devices with respect to the challenging terrain, geographical isolation, and lack of infrastructure on the Navajo reservation.
Knowledge Translation: Dissemination of Research Findings
The findings of our study were disseminated to numerous stakeholders within the NN: the Navajo Division of Health Directors; the Health, Education, and Human Services oversight committee of the NN Tribal Council; the NN Advocacy Council on Disability, 3 the Navajo Area Indian Health Services chief medical officer, and the four boards of directors for the service units selected for this study. Dissemination to these other stakeholders provided an opportunity for additional input and interpretation of findings.
Studies bringing to light the barriers faced by those in the forefront of AT provision are important in creating awareness and bringing about changes in policy and practice. Research findings of the Navajo Advocacy Council on Disability overlap with the findings of our study: housing issues, including inaccessibility at home; inaccessibility in public locations; health care at Indian Health Service facilities that do not meet the needs of individuals with disabilities; and that people with disabilities are poorly understood by communities, including tribal leaders (Native American Disability Law Center, 2007). In response to the policy-related issues identified in our study, the Health, Education, and Human Services oversight committee indicated that they would utilize our research findings to take action related to housing issues and accessibility of all public buildings on the reservation, and to facilitate communication with and oversight of relevant divisions and programs involved in AT provision (Navajo Post Reporter, 2013).
According to the chief medical officer, Navajo Area Indian Health Services is bound by United States regulations regarding the provision of certain AT, and the reality of health care within the Indian Health Services system is that there is significant need for providers in all areas of medicine that must be filled by contracted doctors. Until recruitment and retention of qualified doctors can be achieved, the high turnover of doctors will continue.
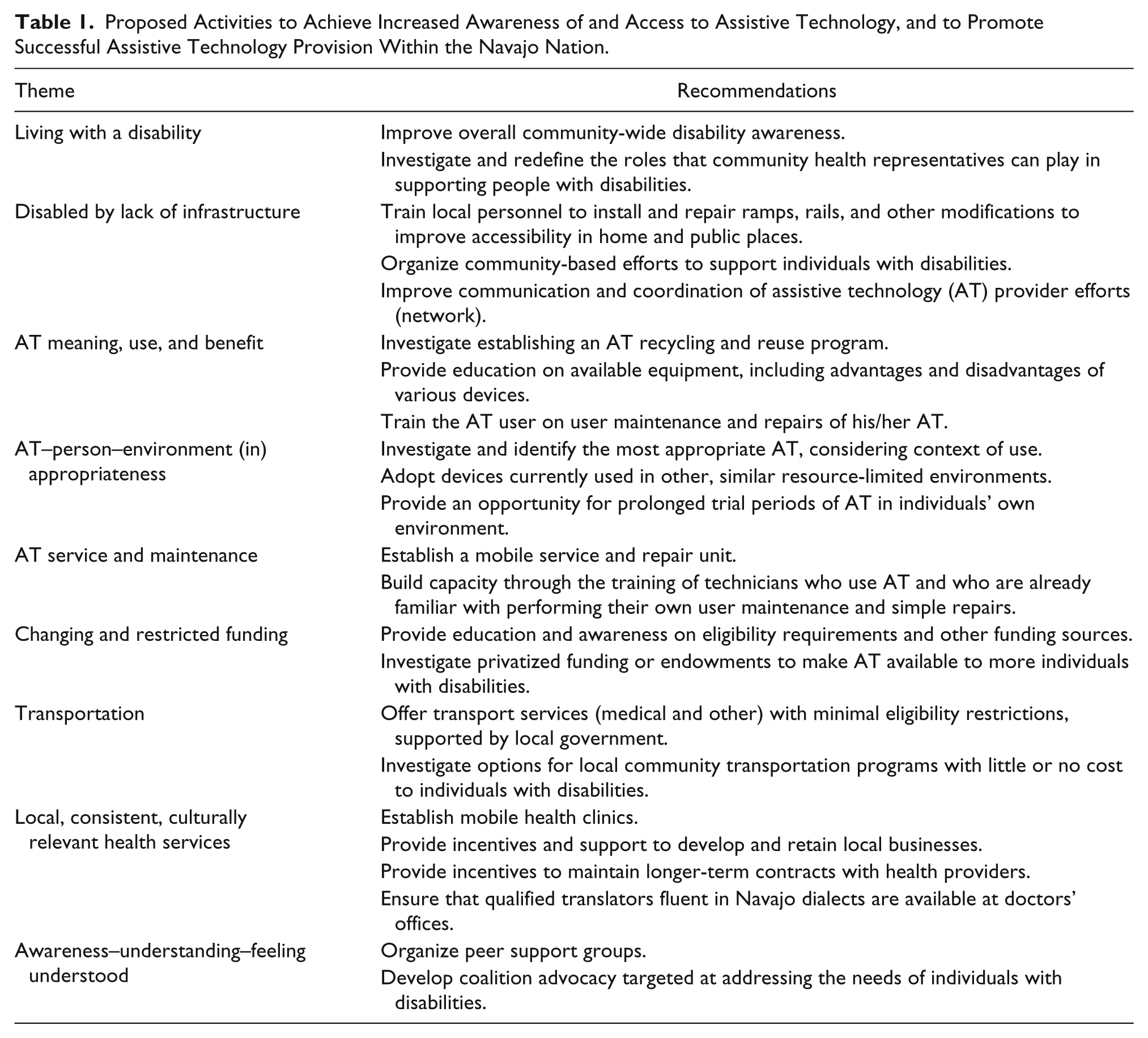
Recommendations: Opportunities for Change
Bringing about awareness of all stakeholders is crucial to creating change and improving AT provision within the Navajo Nation. Suggestions by focus group participants and review of the findings indicate opportunities for various stakeholder groups to improve the current state of AT provision in the NN (see Table 1).
Proposed Activities to Achieve Increased Awareness of and Access to Assistive Technology, and to Promote Successful Assistive Technology Provision Within the Navajo Nation.
Limitations, and Future Research
The main limitations of this study relate to inadequate researcher presence on the reservation, communication barriers, and delays in obtaining local community support, which prohibited recruitment from all four service units simultaneously and caused us to fall short of our recruitment goals in terms of number of participants and group demographics, including a lack of involvement of individuals who used augmentative and alternative communication technology. Within each focus group we sought to have 2 or 3 participants from each service unit, with 1 or 2 participants being caregivers of children who used AT. Because we were unable to achieve our desired group composition we cannot generalize findings to all of the reservations in both Arizona and New Mexico, or to type of service unit. Nor were we able to compare results between adult AT users and caregivers of children who used AT. Although we did not achieve our recruitment goals, we did achieve data saturation within and between AT-user focus groups for the themes discussed above.
Similarly, we did not achieve our AT-provider recruitment goals. We intended to recruit at least 1 manufacturer or supplier and 1 service provider for each of the AT types, 1 transportation provider, and 1 CHR, for a total 10 to 12 participants per AT-provider group. We had no representation from manufacturers for any type of AT, nor did we have service providers of wheelchairs, vision aids, or speech aids. Thus, we were unable to compare AT users’ and AT providers’ perspectives by type of AT.
Overall, there were few age-related issues brought forward for discussion. Future focus groups with younger cohorts (ages 18 to 40) would be beneficial for drawing out other age-related concerns. Some tentative areas of difference included culturally relevant health services, importance of peer support, and advocacy efforts.
Conclusions
Improving awareness of, access to, and acquisition of assistive technology in resource-limited environments has been a goal of stakeholders both domestically and internationally. We held focus groups to assess the current state of AT provision within the Navajo reservation as perceived by individuals who use AT and as perceived by AT providers to identify factors that contribute to the success of AT provision, and that affect the use of and satisfaction with devices and services. Separate groups were conducted for individuals with disabilities who used different types of AT and for the AT providers. We identified several common themes among the AT users and the AT providers, and identified opportunities to improve specific aspects of AT provision in the Navajo Nation.
Footnotes
Acknowledgements
We thank all focus group participants for sharing their stories and experiences. We acknowledge the support and efforts of Nancy Geiger, our Navajo partner ASSIST! to Independence, and all Navajo project staff who helped in conducting this study.
Authors’ Note
This article was reviewed and approved by the Navajo Nation Human Research Review Board (NNHRRB) for submission to QHR. The results of this study were presented at the NNHRRB research conference October 23–24, 2013, in Window Rock, Arizona.
Declarations of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the U.S. Department of Education, National Institute on Disability and Rehabilitation Research (Grant # H133A090020).
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.