
Abstract
Stress urinary incontinence is common and sometimes embarrassing. New, simple, and easily accessible treatments are needed. We telephone interviewed 21 women who participated in a randomized controlled study comparing two treatment programs based on instructions for pelvic floor muscle training. One program was Internet-based and included email support by a urotherapist; the other was sent by post. There was no face-to-face contact in either program. Our main aim was to explore the women’s experiences of the Internet-based treatment. Grounded theory analysis revealed three categories: hidden but present, at a distance but close, and by myself but not alone. These were incorporated in a core category: acknowledged but not exposed. The leakage was often a well-hidden secret, but the study treatments lowered the barrier for seeking care. In the Internet group, a supportive patient–provider relationship developed despite the lack of face-to-face contact. Internet-based treatment programs can increase access to care and empower women.
Use of the Internet to obtain health-related information is increasingly common. In 2011, 88% of the Swedish adult population had access to a computer with an Internet connection, and 67% of Internet users aged 12 years and older reported using the Internet for health-related information (Findahl, 2011). In the United States, 59% of the population had sought health-related information on the Internet at some point in 2010 (Fox, 2011). Commonly mentioned reasons for using the Internet instead of turning to ordinary health care include a personal or stigmatizing condition, a wish to remain anonymous (Powell, Inglis, Ronnie, & Large, 2011; Young, 2005), and dissatisfaction with previous health care providers (Tustin, 2010). Those using the Internet for health-related information are more often women, have a higher education, and are younger than the population average (Powell et al., 2011).
Internet-based treatments have been developed for various conditions such as chronic pain, headache, and irritable bowel syndrome (Andersson, Ljotsson, & Weise, 2011). Treatment via the Internet has been found to be convenient, flexible, and time-sparing (Beattie, Shaw, Kaur, & Kessler, 2009; Sanchez-Ortiz et al., 2011). However, the patient–provider relationship might be negatively influenced by the lack of visual cues and by difficulties with text-based communication (Beattie et al., 2009). In addition, the help-seeking barrier might be different for an Internet-based treatment compared to ordinary health care. In a qualitative study of Internet-based cognitive behavioral therapy for eating disorders, some participants described the treatment as a first option, something to try before seeking ordinary health care (Sanchez-Ortiz et al., 2011).
Urinary incontinence (UI) affects one in four women. Stress urinary incontinence (SUI), that is, the leakage of urine during sneezing, coughing, or exertion, accounts for about half of all female UI (Hannestad, Rortveit, Sandvik, & Hunskaar, 2000). Quality of life might be decreased depending on type of incontinence and severity of symptoms (Kwon, Kim, Son, Roh, & You, 2010; Monz et al., 2005). The leakage can affect many different modalities of quality of life, such as the ability to work, physical activity, travel, mood, energy, and sleep. Sexuality and intimacy might also be affected (Barber, Dowsett, Mullen, & Viktrup, 2005; Nilsson, Lalos, Lindkvist, & Lalos, 2011). The recommended first line of treatment for SUI is pelvic floor muscle training (PFMT), which brings improvement or cure in about two thirds of women (Shamliyan, Wyman, & Kane, 2012).
Despite the existence of effective treatment for SUI, fewer than 40% of affected women seek care for their leakage (Koch, 2006). One reason for not seeking care might be that the woman does not regard the leakage as a major problem. Severe symptoms and high impact on quality of life make women more prone to seek help (Samuelsson, Victor, & Tibblin, 1997), but there are other factors that influence help-seeking behavior. UI is a stigmatized condition (Elstad, Taubenberg, Botelho, & Tennstedt, 2010), and fear of humiliation and shame might prevent women from seeking help (Hagglund & Wadensten, 2007; Kinchen et al., 2003).
In addition, a postmodernist feminist analysis suggests that the bodies of women are regarded as having an inherent leakiness (Shildrick, 1997), and there is a risk that incontinence will be neglected and dismissed as yet another leakage from the female body (Peake & Manderson, 2003), in addition to monthly blood, discharges, breast milk, and tears. Furthermore, access to care might be variable, depending on location and health care system. Once having sought care, some women perceive that the subject of UI embarrasses their doctor and the condition is sometimes not taken seriously (St John, James, & McKenzie, 2002). Instead of seeking care, women might develop strategies to cope with their symptoms, and accept and adjust to the situation (St John, Wallis, Griffiths, & McKenzie, 2010).
New methods for the delivery of nonpharmacological treatment for SUI, such as Internet-based or self-management treatments, have been identified as an important research field (Shamliyan et al., 2012). In a recent randomized controlled trial (RCT), two treatment programs for SUI based on self-instructions for PFMT were compared: one Internet-based and one sent by post (Sjöström et al., 2013). The Internet group received email support from an urotherapist, whereas the postal group completed training on their own. There was no face-to-face contact in either program. Highly significant and similar improvements in both symptom scores and quality-of-life scores were seen with both programs, but the Internet-based treatment group reported higher self-perceived improvements, a larger reduction in the use of incontinence aids, and a greater satisfaction with the treatment program, compared to the postal group.
In the present parallel qualitative study we asked the women to elaborate on their experiences of the treatments and on some aspects of living with incontinence. The main aim of the present study was to explore women’s experiences of an Internet-based treatment program for SUI. We also wanted to explore how a postal treatment program for SUI was perceived and how the tendency to seek care and the patient–provider relationship were affected by the type of treatment given.
Method
Our study was a qualitative study of 21 semistructured individual telephone interviews. We analyzed data according to grounded theory principles (Corbin & Strauss, 2008). We chose this method because it is a constantly ongoing process that works with recruitment, interviewing, analysis, and development of new research questions in parallel, and it is applicable when exploring a previously uninvestigated field.
We conducted the study in Sweden in 2011. The interviewed women had all participated in the previously mentioned RCT, comparing the effect of an Internet-based treatment program for SUI with the effect of a treatment program sent by post (Sjöström et al., 2013). We recruited 250 participants for the RCT via the project’s Web site. This Web site provided information on the research group and the urotherapists, including names and photographs. All participants in the study were women aged 18 to 70 years and had SUI at least once weekly. We diagnosed them using self-assessed validated questionnaires, 2-day bladder diaries, and a telephone interview with a urotherapist.
After randomization, both groups had 3 months of treatment, mainly based on instructions for PFMT. The Internet group received individually tailored support from a female urotherapist via asynchronous encrypted email contact, whereas the postal group completed the training on their own. We performed the first follow-up after 4 months through self-assessed postal questionnaires, including open-ended questions on the experience of each treatment program.
Shortly after the followup, we approached a selected sample of the women by email and asked if they were willing to elaborate on their experiences in a telephone interview. We used a strategic selection aiming for diversity of age, location, and group allocation. Because experiences of non-face-to-face treatment for UI are sparsely described, we chose to interview women in the postal group as well as the Internet group. In Figure 1 we summarize the study population and recruitment method. The mean age of the participants interviewed was 47.6 years (range = 30 to 69). The participants were located all over Sweden, representing rural areas, smaller towns, and larger cities.
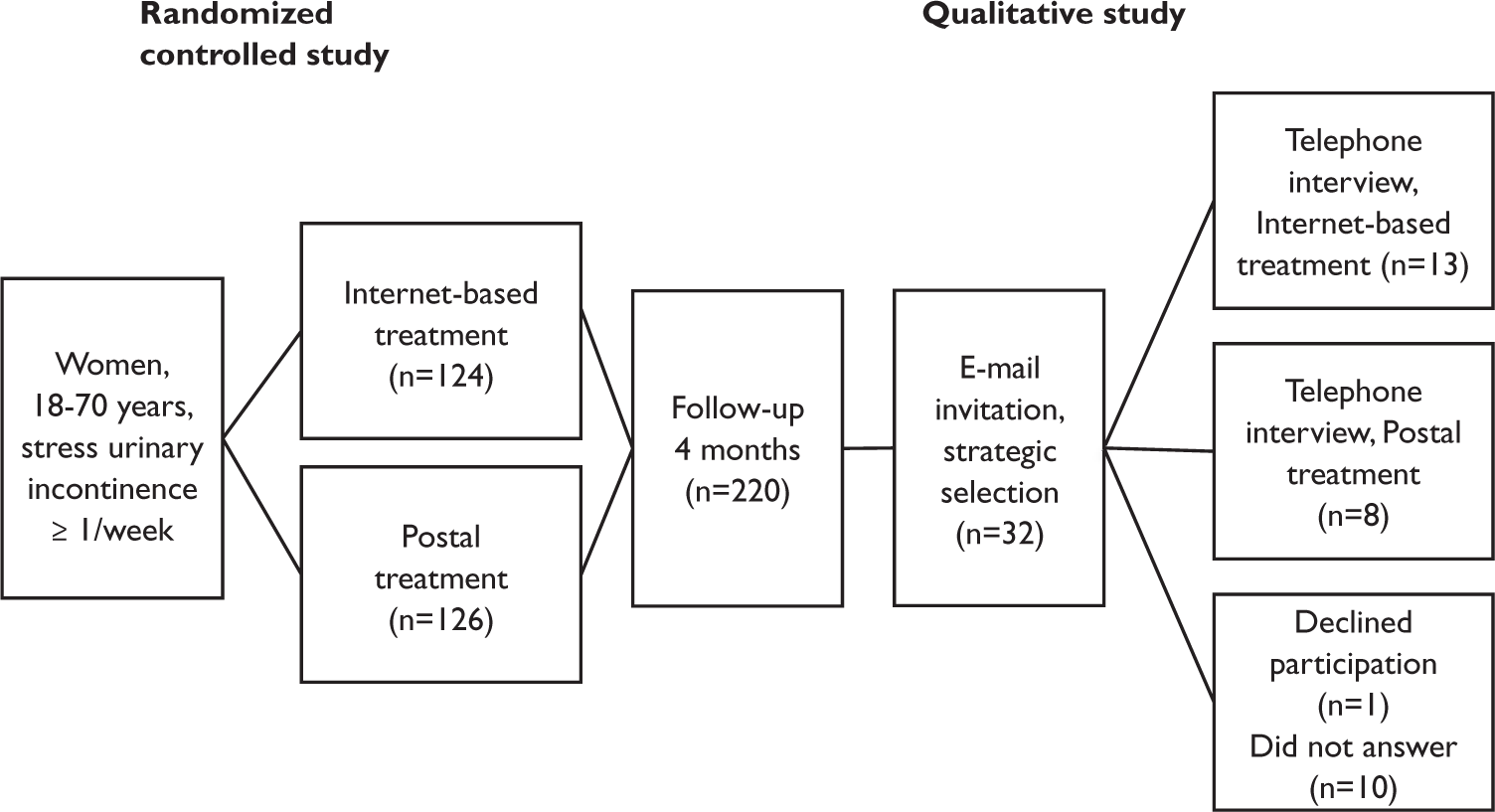
Population and recruitment.
Data Collection
As preparation for constructing the interview questions, we coded the open-ended questions used in the 4-month RCT followup and used the emerging preliminary categories from this process to compose a semistructured interview guide. The questions in the guide were open ended. We intended the questions to give a deeper understanding of several factors: what led to participation in the study (“Why did you join the study?”), aspects of living with incontinence (“Could you describe your symptoms before joining the study?”), feelings experienced during the treatment (“How did you experience the treatment?”), treatment effect (“In what way has the treatment altered your incontinence symptoms?”) and, when applicable, the relationship with the urotherapist (“How was your contact with the urotherapist?”).
The first author (a woman) conducted all of the telephone interviews. During each interview, she encouraged the participant to talk freely about her experiences, and at the end of the interview asked her to raise any subject not yet covered. For better preunderstanding, the first author read the encrypted email contact between the participants and the urotherapist before interviewing women in the Internet group. The mean interview time was 23 minutes (range = 11 to 45 minutes). The first author recorded and transcribed verbatim 19 of the 21 interviews. One woman did not want the interview to be recorded, and one interview could not be recorded because of technical problems. Instead, the first author took notes during and after these two interviews.
Data Analysis
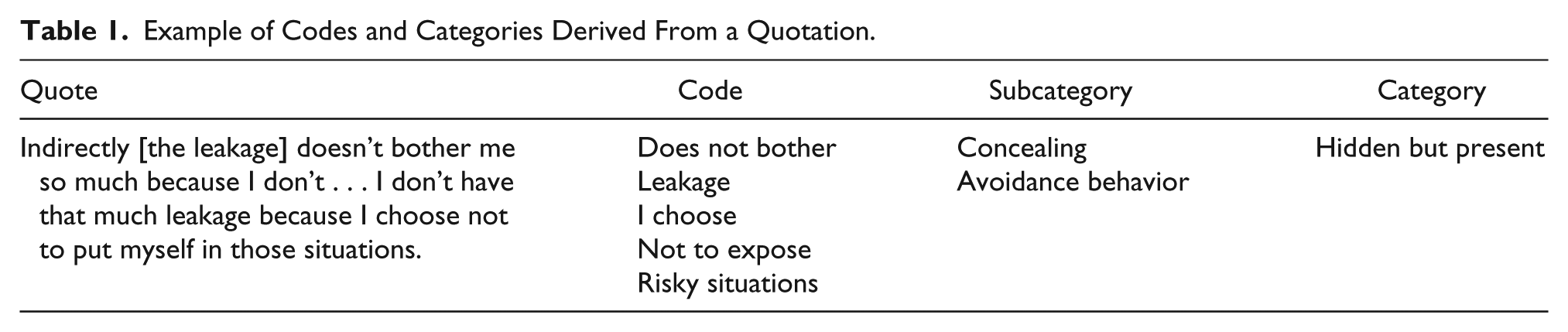
Data collection, transcription, and preliminary analysis proceeded simultaneously. All authors contributed to the analytical process. We compared and discussed the codes, and identified new topics for further elaboration in forthcoming interviews. As with the codes, we continuously discussed the emerging categories within the research group, and we made constant comparisons between the new findings and the raw material in the transcribed interviews. In Table 1 we give an example of how we derived codes and categories from a quotation.
Example of Codes and Categories Derived From a Quotation.
We continued the interviews until no new categories emerged (i.e., until we had reached saturation). During the preparation of this article, we kept close contact with the transcripts. We also wrote memos throughout the whole process. To check the trustworthiness of our analysis, a group of researchers participating in a qualitative research course coded and discussed one part of an interview. These researchers, who were not involved in our study, recognized and thereby confirmed our findings. We received ethical approval from the Regional Ethical Review Board. All participants provided informed consent, and we gave no reimbursement.
Results
We grouped the results into three categories. “Hidden but present” covered aspects of life with incontinence and the factors that led to participation in the RCT. “At a distance but close” covered experiences of the treatment programs and the patient–provider relationship that developed. “By myself but not alone” covered the sense of empowerment experienced by many women during and after treatment. The concepts of motivation, ambivalence, and shame recurred in all three categories. Finally, a core category—“acknowledged but not exposed”—emerged to describe and summarize the results of the categories (see Figure 2).
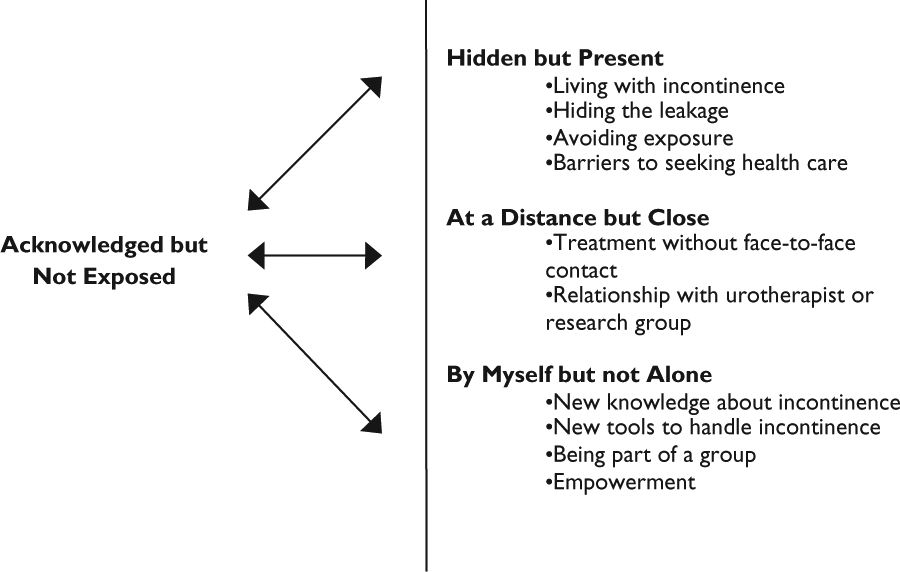
Core category in relation to the main results of the study.
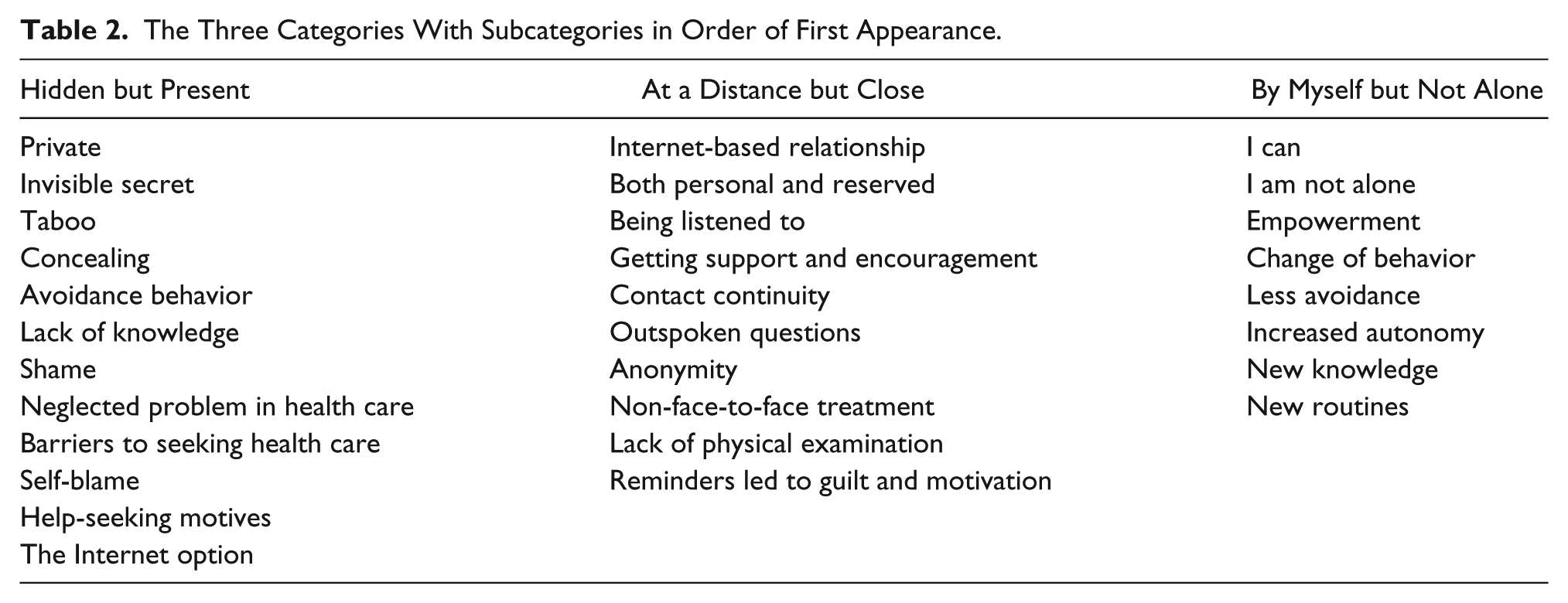
We have marked the quotations in this section with the letter I to denote women in the Internet group and the letter P to denote women in the postal group. Table 2 provides a reader’s guide, listing the subcategories in the text in the same order as they appear in the article. The results are presented in chronological order: before, during, and after the treatment.
The Three Categories With Subcategories in Order of First Appearance.
Hidden but Present
“I am relatively young, still just thirty-one at the moment, but I thought, am I supposed to live with an invisible but very real problem for the rest of my life, then, if I don’t do anything about it?” (I). This category contains descriptions of symptoms, some experiences of living with SUI, and barriers for seeking help from women in both treatment groups. Most women did not define their incontinence as a major health problem: “Well, it does affect me, even though I haven’t exactly suffered, it affects me” (I). Still, living with an ever-present concern of leaking urine was described as a private and usually well-hidden secret that might result in awkwardness and embarrassment. Most of the women described their incontinence as shameful, and something they disclosed to no one or to very few other people: “Yes. You can talk about almost anything else I think, all kinds of matters considering your genitals and . . . but not this, this I think is very taboo” (I).
Before joining the study, a majority of the women had lived with incontinence for many years. The women described how they had adjusted to their circumstances instead of seeking help, for instance by avoiding leakage-provoking activities such as jogging, jumping, or energetic play with their children. Another reason for not seeking care was a lack of knowledge about the treatments available for SUI. Some women expressed a wish for health care providers to talk more openly about incontinence and what to do about it. The women were uncertain whether SUI was a treatable condition or just a consequence of giving birth and a part of the normal aging process: “You get to a point of acceptance. Well, well, I am sixty-eight years old, and you get some ailments. Yes, and then you get some pads and you settle for that” (I).
Most women had an explanation for the etiology of their leakage, and for some of them this was associated with guilt. They blamed themselves for the leakage, and for not doing enough PFMT: “So, I didn’t have the kind of problems where I would have looked for the usual health care help. Because I know it’s because of my bad training routine, that’s clear” (P). Some of the women said that talking about SUI with a health care provider face to face was embarrassing and exposing. The Internet treatment offered an opportunity to seek help with less embarrassment.
Having sought care on previous occasions, some women felt they had not been taken seriously or had even been ignored. On mentioning their incontinence, they had experienced a dismissive and sometimes embarrassed attitude from health care providers: “Well, I haven’t explicitly looked for it, but since I was there I asked them and told them about my problems, but they didn’t think there was much to be concerned about” (I). Overall, many of the women described the barrier for seeking help as relatively high. The more impact the leakage had on everyday life, the greater the motivation for seeking help. One woman said that a reason for seeking help was the limitation of not being able to play with her children any more.
The barrier to applying for the non-face-to-face treatments offered in the RCT appeared to be lower than for ordinary health care. The women perceived the treatments as a possibility to do something about the leakage on their own. They also saw the treatments as time-sparing and easily accessible, which was appealing;
I saw it in a newspaper and thought it was a good idea, because I didn’t have the kind of trouble where I would have sought help from the ordinary health care providers. I didn’t think I had that much of a problem. (I)
Other reasons for joining the study were the possibility to remain anonymous, the need for motivational support, curiosity about Internet-based treatments, and having been on the verge of seeking help when they saw an advertisement for the study.
At a Distance but Close
One could say, had she been sitting in front of me like anybody else, then I would not have asked in the same way. . . . Yes, I thought so. It felt natural in a way, I did not feel as exposed and vulnerable. (I)
This category mainly focuses on the experiences from the 13 women in the Internet group. The reflections from the 8 women in the postal group are summarized at the end. Most women in the Internet group experienced the establishment of a relationship with the urotherapist. They described the relationship as both personal and distant, and said that it gave them a sense of being acknowledged and supported without being exposed. They mentioned many factors as important for the development of the relationship, including the fact that someone seemed genuinely interested in their concerns, gave them praise when they were doing well, and supported them when their motivation was low. The women had contact with the same urotherapist throughout the treatment period, and they experienced this as a positive aspect that enhanced the patient–provider relationship, which in turn increased their motivation to do PFMT.
The lack of face-to-face contact had both positive and negative consequences. Some women experienced the relationship as more harmless and less potentially judgmental, compared to a face-to-face relationship, and this made them feel freer to talk openly about the leakage:
I mean, I think I developed a close relationship with her anyway. I mean, just because I could ask about things more directly than I normally would. And you got an answer the next day, she didn’t try to escape. She was there, it was a comfort to have her there. And I knew that if I needed to ask about something, I could email her. (I) No, and that’s why it felt good on the ‘net [Internet]: You’re an anonymous person. Because I would think, I’ve been thinking about this for quite a while and thought that it’s a bit hard to go to a health care center or doctor with these problems. So, I think I thought that this anonymity was comfortable. (I)
Some aspects of the relationship were lost or became more superficial without face-to-face contact. For example, small shifts in facial expressions, body language, or intonation were missed, and for some women this led to an experience of a less-close patient–provider relationship. As a consequence, these women also felt less motivation to do PFMT:
It is easier to cheat, what should I say, if you don’t have a physical meeting. It gets more distant and it can be easier to skip, if you don’t feel really engaged, because it becomes a more impersonal contact that hasn’t got the same weight. (I)
A few women said that it was more difficult to explain complex situations and feelings in written text than face to face. One woman expressed the ambivalence like this:
Sometimes it can be tough to have a contact, get to the contact, sit face to face, and go there every week. It feels demanding and it takes too much time, so that was really positive. Sometimes it is good, though, to have someone to look you straight in the eyes and tell you what to do. It is easier to take it seriously. But I thought that the contact over the Internet worked really well. (I)
A few women also expressed a wish for a physical examination at the start of treatment. They wanted reassurance that everything looked normal, and also confirmation that they were using the right muscles when performing PFMT.
Women in the Internet group reported on their completed training each week by email to their urotherapist. If they did not report on time, the urotherapist sent a reminder; some women experienced this as stressful. Many women also mentioned a sense of guilt because of the inconsistency between their own goals for the training and their actual achievements.
These women placed high demands on themselves, and wanted to do the right thing to meet the expectations they perceived from the urotherapist:
Yes, toward the end there was a negative pressure. But it wasn’t because of the emails I got, but because I felt that I should have done more, and this was important for me. And then I felt guilty about it and chose not to answer, because I felt that, no, I have to do the exercises properly now for a week before I can answer. (I)
Conversely, many women said they needed the reminders to maintain their motivation for training: “It is in my own interest to do this, but it still feels like I need to have someone to keep an eye on me so that I do the training” (I).
The women in the postal group expressed a lack of communication and support. They wanted someone they could tell about their progress, and they wanted help with motivation and reminders to do PFMT. They found it difficult to retain motivation over a long period without support. One woman described the PFMT as follows:
It is so boring to do. I really felt motivated when I joined. I figured it was now or never, but then three weeks go by, and then you’ve lost your motivation. You don’t talk about it with anyone. It’s not like when you’ve been out jogging five kilometers and brag about it; this is something you’re quite alone with. (P)
Women in the postal group talked less about guilt and negative pressure than women in the Internet group, and more often described their participation and contribution with purely positive words. They also expressed a sense of loyalty toward the research team, and took responsibility for their participation in the study. It is likely that this also helped them maintain their motivation for training: “It felt like, like I was, the participation in a study like this, like my contribution was important, and all of these questionnaires, it felt important to do. And I think that my motivation to do this also increased” (P).
By Myself but Not Alone
“And when you know how, then it is easier to do it” (I). One effect of the Internet-based treatment, and to some extent also of the postal treatment, was an increased awareness of how to handle the incontinence. The majority of the women felt empowered by the treatments. Almost all women in both groups expressed a change in their ability to control the leakage, and not necessarily by using their previous technique of avoiding certain activities. After treatment, the women thought about their leakage more often, but in a more constructive way, and believed they were one step ahead in their mind. Many of the women said they had learned how to contract their pelvic floor muscles to prevent the leakage, and as a consequence their level of activity had increased.
One part of the Internet-based treatment program focused on cognitive behavioral therapy assignments for lifestyle change, and for the identification and minimization of avoidance and redundant security measures. Some of the women said that this part was helpful, and a few clearly expressed that it helped them avoid negative patterns: “I think it was good that you included those things, because then you gained awareness. At first I thought, I don’t do any of those things, but then I thought again and oh, yes, actually I do” (I).
For some women, the treatment did not improve the leakage; however, most of these women expressed a positive experience of the treatment because they had gained new knowledge, increased their awareness, and received tools to work with in the future: “Even though it hasn’t happened that much during the study time, I got a little bit better. I have gained a tool to use when I get time and decide to do this” (I). Participation in a study in which incontinence was openly discussed also helped to break down some of the shame barriers. One woman described how she was now brave enough to bring the topic up:
Yes, I have noticed that since I said that I joined this study, both at work and among friends, that people have said, “No, so should I. That’s exactly the way it is.” Well, I didn’t know it was that common a thing, I had thought it was mostly just me. (P)
In both groups, women described how their motivation to do PFMT was correlated with the severity of the leakage. They found it motivating to decrease the leakage to a certain point, but the better the leakage got, the more difficult it was to remember the training. Women who remembered to do PFMT in the long term described how they connected the training with preexisting activities; hence, the training became a part of their daily routines:
I still try to do some training. I did it for so long that it became a routine. You sat there in the car contracting your muscles. Once, I sat on the couch and my daughter said, “Are you still doing your contractions?” Well, yes; the whole couch moves. Well, okay. It became a little bit like that; my whole family was dragged into this. (P)
Acknowledged but Not Exposed
During the analytical process, a core category emerged that described the results in all three categories: acknowledged but not exposed. This core category included a number of aspects, as follows. A woman living with a condition she perceives as embarrassing might feel alone and exposed. Many of the women wished that SUI would be more recognized and openly talked about instead of being a well-hidden secret. Some of the women were afraid of exposing themselves, and this led them to adapt their daily activities and sometimes deterred them from seeking health care. Participation in a treatment program made the women feel acknowledged and supported, and it helped them to retain control and gave them a feeling of less exposure. The women were empowered by the treatment programs; the discovery that they were not alone made them see themselves as part of a group, and this new knowledge helped them feel less exposed in their everyday lives.
Discussion
In this qualitative study, we interviewed women treated for SUI with two different treatment programs without face-to-face contact. The results fell into three categories: hidden but present (living with incontinence and barriers to seeking help), at a distance but close (experiences of the treatment programs and the patient–provider relationship), and by myself but not alone (how the women were empowered by the treatments). A core category eventually emerged: acknowledged but not exposed.
Living with SUI is a state of ambivalence for many women. Most women in this study considered themselves healthy, but at the same time thought they had a hidden handicap. Many described their leakage symptoms as quite moderate, but the leakage still had consequences for their everyday lives and made them avoid certain situations. Moreover, they were unsure of the dignity of their condition, and felt alone and ashamed. Contradictions like these, associated with UI, have also been described by other researchers (Peake & Manderson, 2003). These ambiguities might emanate from a social and cultural context in which the bodies of women are referred to as leaky, and set in contrast to the bodies of men, which are hard and dry (Peake & Manderson; Shildrick, 1997). In this context, female UI might be considered normal, even if it has severe implications for everyday life, and deter women from seeking help.
The social and cultural context described above permeates the entire society, and so there is a risk that health care personnel will not take women with UI seriously, and that symptoms will be minimized once the woman seeks care. A few women in our study described how they had previously tried to talk about their incontinence with a health care provider but had been met with a dismissive response, a result confirmed in other studies (St John et al., 2002). The offer of an Internet-based treatment program might make it easier to seek care (Sanchez-Ortiz et al., 2011); many of the women described how they considered their participation in the RCT as a way to manage the leakage on their own and were not sure they would have sought help from the ordinary health care system.
Even though they never met, the women in the Internet group developed relationships with the urotherapists. The lack of face-to-face contact can have a dual impact: It might make it easier to communicate about sensitive issues (Suler, 2004), but the loss of some communicational aspects might lead to a superficial relationship (Beattie et al., 2009). However, most of the women described the relationship with their urotherapist as an important motivating factor.
This relationship, along with revealing the leakage and the gradually increasing exercises, induced the feeling of being acknowledged both as an individual and as part of a group. The anonymity offered by an Internet-based treatment program might become a motivating factor via an increased sense of control, because the patient might feel more free to dictate the pace and the focus, compared to more traditional treatments (Donkin & Glozier, 2012). Comparably, the women in the postal group expressed a wish for more support during treatment and said that they found it difficult to maintain the motivation to continue PFMT over a longer period.
In a previous review of success factors for Internet-based treatment programs, the authors concluded that individually tailored support is important (Schubart, Stuckey, Ganeshamoorthy, & Sciamanna, 2011). Such support has been shown to induce self-discipline and increase learning (Gerhards et al., 2011). Women in the Internet group often expressed gratitude toward the urotherapists, but they also talked more about guilt and feelings of negative pressure than women in the postal group. The occurrence of UI is sometimes considered to be caused by bodily neglect and lack of self-discipline (Peake & Manderson, 2003), and it is possible that, at a more or less conscious level, the reminders from the urotherapists induced feelings of insufficiency and self-blame instead of being supportive. The difference between support and blame is a balancing act; this is important to keep in mind when developing new treatment strategies—even those taking forms such as instructions for PFMT.
After treatment, most women in our study were more aware of how common SUI is, and they had also achieved a greater knowledge of how to perform PFMT. Some women said they had started to talk more freely about their leakage with friends and relatives and described how this led to less shame. When under treatment, the women believed they were being taken seriously, and this made them feel empowered. Malterud (2010) pointed at the responsibility of health care providers to “recognize the suffering of patients, identify their strengths, and prevent further marginalization due to power inequality” (p. 140) as a part of empowerment. This was achieved in our study, even though the patient and the health care provider did not meet. For many of the interviewed women, the treatments contributed to a shift from containing, restricting, concealing, and modifying strategies as described by St John et al. (2010) to an increased sense of autonomy and empowerment in everyday life.
Strengths and Limitations
We chose to analyze our material according to grounded theory because Internet-based treatment of SUI is a new development and women’s experiences of this treatment form have not been explored previously. Grounded theory makes it possible to adjust later interviews in accordance with findings in interviews that have already taken place, and after discussions in the research group our emerging results led to shifts of focus and themes in the remaining interviews. One of the authors conducted all of the interviews, and this author’s preconceptions might have meant that some aspects were more thoroughly penetrated than others. However, this also gave the interviewer the opportunity to quickly adjust the process and explore new themes. Another strength of the study is that women from both intervention groups were interviewed in parallel, which made it possible to mirror the emerging results.
A limitation of the study is that the interviewed women cannot be seen as representative of women with SUI in general because all of them had completed an online application for participation in the RCT. It is possible that women with an interest in Internet-based treatment have a more positive attitude toward Internet interventions than do women in general. In addition, a treatment program without face-to-face contact demands good skills in comprehensive reading and writing, and this might have excluded women who prefer oral communication.
The process of conducting in-depth interviews by telephone has its own limitations, which might be reflected in our relatively short interview time. Because visual cues are lost, it can be more difficult to reach sufficient depth. Conversely, not sitting face to face with the interviewer can make it easier to talk about sensitive topics. Another potential limitation is the risk that a semistructured interview guide, unless carefully used, might constrain the dialogue.
Conclusion
In this article we have shown that treatment programs for SUI without face-to-face contact were well accepted and seemed to lower the barrier for seeking care. Most of the women participating in the Internet-based treatment program felt supported and acknowledged without exposure, and a patient–provider relationship developed despite the lack of face-to-face contact. Our analysis was descriptive rather than critical. Nevertheless, our results reveal issues that are important to understand when developing new treatment strategies.
SUI is a common condition, yet one that is often difficult to talk about. It is classified as a minor condition both in a cultural context and medically, and women might find it difficult to claim as problematic. Some women are ashamed of and embarrassed by the leakage, and beliefs about the etiology can induce feelings of guilt. In all, this might delay care seeking among women who want treatment. There is also a risk that the health care system might exacerbate the stigma and the silencing of women with incontinence and induce feelings of insufficiency or self-blame. There is a delicate balance between carrot and stick—between being supportive and potentially blaming—which should be kept in mind in all treatment programs for incontinence based on PFMT. Ideally, new treatments should be easily accessible, individualized, supportive, and nonblaming.
The Internet and other technical solutions such as smartphones offer extended possibilities, and treatment without face-to-face contact is likely to increase in the future. An Internet-based treatment program for SUI is an alternative to ordinary health care that can increase access to care and empower women.
Footnotes
Acknowledgements
We thank the participating women for sharing their experiences, urotherapists Eva Källström and Annika Andreasson for support to women in the Internet group, and our research assistant Susanne Johansson for coordinating the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from the Swedish Council for Working Life and Social Research, Västernorrland County Council, Jämtland County Council, Västerbotten County Council (ALF), and Visare Norr, Northern County Councils, Sweden.