
Abstract
Student-led clinics, defined as those in which services are delivered by students under supervision of qualified educators (Briggs & Fronek, 2020), provide a unique service model and student education. Over the past two decades there has been a steady growth of student-led clinics in providing not only preventive services, but also specialized care (Peoples et al., 2025). Although many student-led clinics target underserved communities (Peoples et al., 2025)—populations that social work primarily focuses on—the presence of student-led clinics in social work remains limited (Briggs & Fronek, 2020; Sanders et al., 2024).
Established in 2021 during the COVID-19 pandemic as a response to the increased need for mental health support in the community and the heightened demands for quality social work field placements, the Talk It Out Counseling Clinic at the University of Toronto's Factor-Inwentash Faculty of Social Work is a student-led clinic where Master of Social Work (MSW) practicum students, under close supervision of qualified supervisors, provides free telemental health services to residents of the Greater Toronto Area including communities facing multiple systemic challenges as well as Black and other racialized communities. Originally launched as a pilot program, the Clinic has continued to operate post pandemic, offering short-term counseling services (8–12 weekly sessions typically) online or over the phone to clients aged 16 and older with mild to mental health concerns.
A detailed description of the Clinic, including its development, service model, clientele, and student training, has been described elsewhere (Fang et al., 2024a, 2024b). Briefly, the Clinic operates from a trauma-informed, anti-oppressive lens. Although the Clinic was envisioned and designed by a faculty member and its operation and infrastructure are supported by the school of social work, all services are delivered by MSW students under supervision. Referrals are received exclusively through community partners, which include neighborhood centers, community health centers, legal aids services, homeless shelters, immigrant and settlement organizations, and elder abuse navigation services. As a student-led clinic, the Clinic provides services to individuals experiencing a range of concerns, including anxiety, depression, stress, loneliness and isolation, grief and loss, and relationship challenges. Given its training-based structure and scope of services, the Clinic does not have the capacity to support individuals experiencing acute suicidal ideation or those with serious mental illness or substance use issues who also require a higher level of care. Operating within a continuum-of-care model, our community partners partake in warm handoffs when appropriate and remain involved throughout the duration of the counseling services. This collaboration allows the Clinic to better support clients by complementing their existing support networks, connecting them with external resources, and ensuring continuity of care upon discharge from our services.
All clients referred to the Clinic are informed by both the referral provider and Clinic staff that services are delivered by MSW students under supervision. The Clinic accepts 12–15 MSW students annually, with practicums lasting 5–7 months. All students have an individual supervisor and additional supervisory support, and typically maintain an active caseload of six to eight clients. Students undergo extensive orientation, ongoing training, and regular individual and group supervision (Fang et al., 2024b). Except for the clinic manager who usually supervises up to three students, other supervisors supervise one to two students at a given time. A supervisor attends intake and assessment sessions to confirm client eligibility and provide real-time support via text messaging, while also assessing students’ readiness to conduct counselling independently. Students typically see clients independently after these sessions, unless specific learning needs require the supervisor's online presence.
All students receive training in solution-focused brief therapy at the Clinic, and many also complete additional coursework in cognitive behavioral therapy, narrative therapy, and emotion-focused therapy as part of their MSW program. These approaches are generally well suited to short-term counseling (McGuinty et al., 2016). Given the diversity of client presentations, no single therapeutic modality is prescribed. Instead, under close supervision, students integrate interventions based on systematic assessment and case formulation. As such, students do not adhere to a single manual and may draw on multiple therapeutic approaches to meet client needs.
The current study aims to contribute to the emerging literature on client outcomes for social work student-led clinics. Despite the availability of supervised student-led clinics and the rich learning opportunities they provide (Peoples et al., 2025), these clinics often lack a strong social work presence (Warren et al., 2017), and few studies have assessed client outcomes associated with these services (Briggs & Fronek, 2020; Liberman et al., 2011; Warren et al., 2017). Among the limited studies reporting clients’ mental health outcomes, Canada et al. (2021) presented descriptive data from 46 clients who attended free telemental health services provided by social work and psychology students through the Integrative Behavioral Health Clinic at the University of Missouri before and during the first three months of the COVID-19 pandemic. Their findings suggested that clients’ levels of depression and anxiety remained stable throughout the service period. It should be noted that the purpose of this study was to describe clients’ mental health symptoms during the study period rather than to evaluate service outcomes. In another study of 627 clients, Moncrief-Stuart et al. (2024) found that clients who attended a community-based mental health program in suburban Virginia and Washington, D.C. staffed by social work, counseling, marriage and family therapy, and clinical psychology students showed improvements in depression, anxiety, and overall global severity scores. Lastly, Roseborough et al. (2023) found clinical improvements on a session-by-session basis among 421 clients who attended a free clinic in which counseling services were delivered by social work and psychology practicum students at a private Midwestern university in the United States. Taken together, these results suggest that social work student-led clinic may provide services conducive to client's mental health, while highlighting the needs for further research examining client outcomes in these settings.
Given that many of student-led clinics provide services to communities that lack resources and face systemic barriers (Peoples et al., 2025), evaluating their performance is vital to ensure that these communities receive effective and high-quality care. Such evaluation is essential to ensure that these models do not inadvertently perpetuate a two-tiered system in which marginalized populations receive lower-quality care under the guise of increased access. The need for evaluation is further underscored by the limited empirical research on social work student-led clinics, with existing literature drawing on samples with limited racial and ethnic diversity (Canada et al., 2021; Moncrief-Stuart et al., 2024; Roseborough et al., 2023). Moreover, because counseling services at the Clinic are delivered entirely online and by phone, this evaluation also contributes to the growing literature on telemental health services.
To address these gaps and to advance the knowledge of social work student-led clinics, the study has three objectives. First, the study evaluates the extent to which clients’ mental health symptoms change from intake to termination at the Clinic. It is hypothesized that clients who completed services at the Clinic will demonstrate significant improvements in their mental health outcomes compared to baseline. Second, the study will also explore factors associated with improvements in mental health outcomes. Previous research shows that gender, baseline mental health severity, and number of sessions are associated with client outcomes (Andersson et al., 2019; Barkham et al., 2012; Duong et al., 2025; Hedman et al., 2012). Accordingly, we hypothesize that women and individuals presenting with greater baseline symptom severity will demonstrate greater improvement in mental health outcomes. The number of sessions attended is also examined as a potential factor associated with client outcomes, as greater treatment exposure may provide increased opportunities for therapeutic engagement and symptom change in student-led clinics (Powell et al., 2022). In addition, given the recent establishment of the Clinic and its unique model, clientele, and focus on telemental health services, we followed the practice of past research on student-led clinics (Moncrief-Stuart et al., 2024; Powell et al., 2022) to conduct exploratory analyses to assess the relationship between demographic variables, the medium of service delivery (video, phone, or both) and clients’ mental health improvements. As there is limited evidence on outcomes in social work student-led clinics, these analyses can generate preliminary insights to inform future research and program development. Third, the study assesses clients’ feedback on the care they receive using a structured tool. Within trauma-informed and anti-oppressive frameworks, service effectiveness is understood not only in terms of symptom reduction but also in terms of clients’ experiences of safety, respect, voice, and empowerment within the service environment.
Method
Study Design and Data
The study employed chart reviews and a post-service client feedback survey of clients who completed services between September 2022 and September 2025. Data were extracted from client chart records and administrative logs. In addition, to better understand clients’ service use experiences, the anonymous Virtual Client Experience Survey (VCES) (Crawford et al., 2025) was emailed to all clients who attended at least one intake assessment session after completing services at the Clinic, regardless of termination type.
Ethics Statement
The University of Toronto's Health Sciences Research Ethics Board reviewed the scope of this study and determined that it constituted quality improvement and program evaluation. Clients were also advised prior to providing consent for counseling services that their clinical records might be used for supervision, program evaluation, and quality improvement activities, and that any information used for reporting would be anonymized and presented only in aggregate form.
Measurements
The chart records reviewed contained clients’ demographic characteristics, reasons for seeking services, self-rated mental health at intake, and anxiety and depression scores at both intake and service completion. Administrative logs were also examined to obtain information on service utilization, including the occurrence of the warm handoff, the number of sessions attended, and reasons for service termination.
Demographic Characteristics
Demographic variables included clients’ gender, age, partnership status, education, and race.
Reasons for Seeking Services
Clients provided reasons for seeking counselling services from the following 12 categories: anxiety, depression, stress, trauma, family issues, relationship challenges, loneliness and isolation, grief and loss, violence, identity exploration, bullying, and racial distress. Reasons that did not fall under any of these categories were coded as “other.”
Baseline Self-Rated Mental Health
During the intake assessment, clients rated their general mental health on a 5-point scale ranging from 1 (poor) to 5 (excellent).
Mental Health Outcomes
We assessed client's level of anxiety and depression during the intake (baseline) and termination sessions. Anxiety was measured by the Generalized Anxiety Disorder-2 (GAD-2) scale (Plummer et al., 2016). Clients reported how often they had experienced the following two symptoms over the past 2 weeks: (1) “feeling nervous, anxious, or on edge” and (2) “not being able to stop or control worrying.” Depression was assessed using the Patient Health Questionnaire-2 (PHQ-2) scale (Staples et al., 2019), in which clients indicated how often they had experienced the following symptoms over the past 2 weeks: (1) “little interest or pleasure in doing things” and (2) “feeling down, depressed, or hopeless.” Both GAD-2 and PHQ-2 are 4-point Likert scales ranging from 0 (not at all) to 3 (nearly every day), producing a total score from 0 to 6. A cutoff score of 3 was used on the GAD-2 to indicate probable clinical anxiety (Kroenke et al., 2007; Plummer et al., 2016) and on the PHQ-2 to indicate probable depression (Kroenke et al., 2003; Staples et al., 2019). GAD-2 demonstrates acceptable discriminative validity (Staples et al., 2019) and moderately high balance of sensitivity and specificity identifying generalized anxiety disorders (Plummer et al., 2016). Similarly, PHQ-2 has an excellent discriminative validity and an optimal balance of sensitivity and specificity (Staples et al., 2019). Both scales have good test–retest reliability and internal consistency (Staples et al., 2019). Beyond facilitating higher client response rates because of their brevity (Kroenke et al., 2009; Plummer et al., 2016), both measures have shown to be viable tools for screening and monitoring symptoms of anxiety and depression (Andersson et al., 2019).
Service Utilization
Service utilization variables included clients’ preferred method of counselling (video, phone, or both), whether they had a warm hand-off session before intake (no or yes), the number of service sessions, and the client's service termination type (premature or planned). Premature termination referred to clients who exited the services without mutual agreement with their therapist, whereas planned termination was defined as successful completion of services followed by a scheduled termination session (McGovern et al., 2024; Rabinowitz et al., 2025).
Client Experience and Service Quality
We assessed clients’ perceptions of their services using the adapted VCES, administered anonymously through an online survey. Demographic information such as gender, age, and race, was also collected as part of this survey. The VCES has an established content validity, well-supported factor structure, and high construct reliability (Crawford et al., 2025). Our adapted VCES, maintaining the same structure as the original version, consisted of 17 Likert-scale items assessing multiple aspects of virtual care, including: access to services; efficiency and timeliness; client-centeredness; safety; effectiveness of service delivery; and overall satisfaction. Although VCES is guided by the Institute of Medicine (2001) health care quality framework, several of its domains, particularly access, safety and client-centeredness, are compatible with the Clinic's trauma-informed and anti-racist practice orientations (Levenson, 2020; Substance Abuse and Mental Health Services Administration, 2014; Umogbai & Walji, 2024). A sample item is “I was involved as much as I wanted to be in decisions about my treatment services and supports.” Each of the 17 items was rated on a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). The Cronbach's alpha for the adapted VCES in the current study was .89, indicating good reliability (Tavakol & Dennick, 2011).
Statistical Analyses
Descriptive analyses such as frequencies and percentages were used to describe the client population, reasons for seeking services, mental health, service utilization, and service experience. Bivariate analyses examined relationships between client characteristics and service termination status, as well as between their demographic characteristics and service experiences. Given the small sample size, Fisher's exact test (for 2 × 2 tables) or the Fisher–Freeman–Halton test (for larger tables) was conducted between categorical variables and termination status, and independent samples t tests were conducted between continuous variables and termination status. For relationships between clients’ demographic characteristics and service experience, independent samples t tests and analysis of variance (ANOVA) were conducted.
We hypothesized that: (1) clients receiving clinic services would show significant improvement in GAD-2 scores and (2) PHQ-2 scores from pretest to posttest. Pre-post differences were examined using paired-samples t tests for continuous scores, and McNemar's chi-square tests for scores based on established clinical thresholds. In addition, to examine factors associated with pre-post score changes (posttest minus pretest), we conducted independent samples t tests, one-way ANOVAs, and Pearson correlations, as appropriate. Given the limited sample size and the need to maintain a parsimonious model, only variables significant in bivariate analyses were included in the repeated measures models for interaction analyses. All analyses were conducted in SPSS 31. Listwise deletion was applied to handle missing data.
Results
Client Demographics, Baseline Mental Health Status, and Service Utilization
As shown in Figure 1, a total of 328 clients were assessed between September 2022 and September 2025, and 236 clients attended at least the one intake assessment session. Among them, 144 (61.0%) successfully completed services with a planned termination and 92 (39.0%) ended services prematurely. The primary reasons for premature termination were inability to contact the client after three attempts (n = 51, 55.4%), followed by client-initiated withdrawal (n = 24, 27.1%), and scheduling conflicts (n = 8, 8.7%).
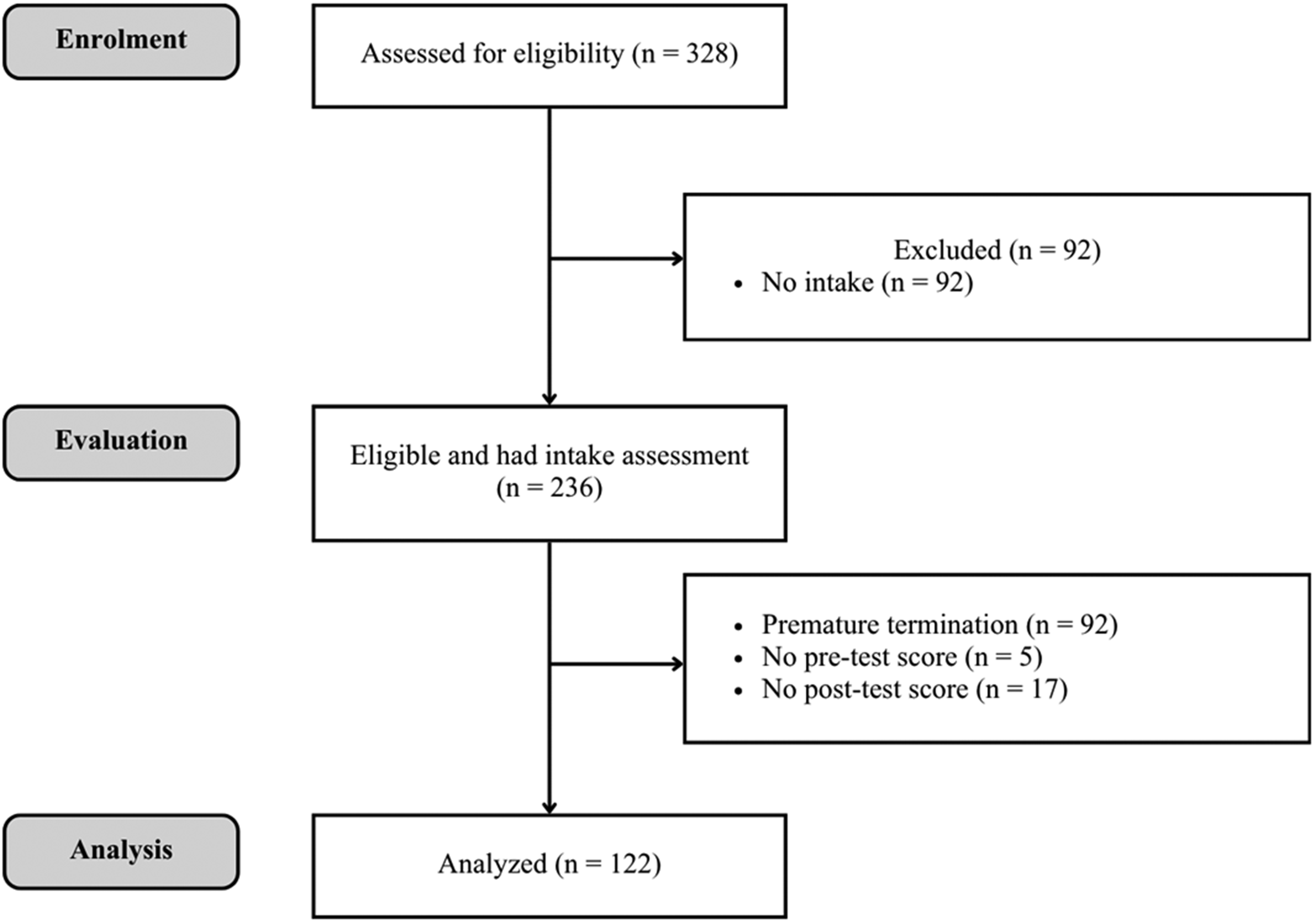
CONSORT flow diagram for the single-arm evaluation.
Table 1 presents the demographic characteristics and baseline mental health status of 236 clients who had at least one intake session, including both who successfully completed services and those who terminated prematurely. The age of clients ranged from 15.24 to 76.70 (M = 37.72, SD = 14.46), and most clients self-identified as women (67.2%) and as Black, Indigenous, and people of color (BIPOC; 63.1%). Most clients sought services for anxiety (67.4%), depression (57.2%), and stress (56.4%). At intake, 72.4% of clients rated their mental health as “poor” or “fair” (M = 2.11, SD = 0.94). Over two-thirds (68.4%) of clients met the cutoff score of GAD-2 (M = 3.73, SD = 1.82), and 57.0% of clients met the cutoff score on the PHQ-2 (M = 3.01, SD = 1.76).
Client Characteristics by Termination Status (N = 236).
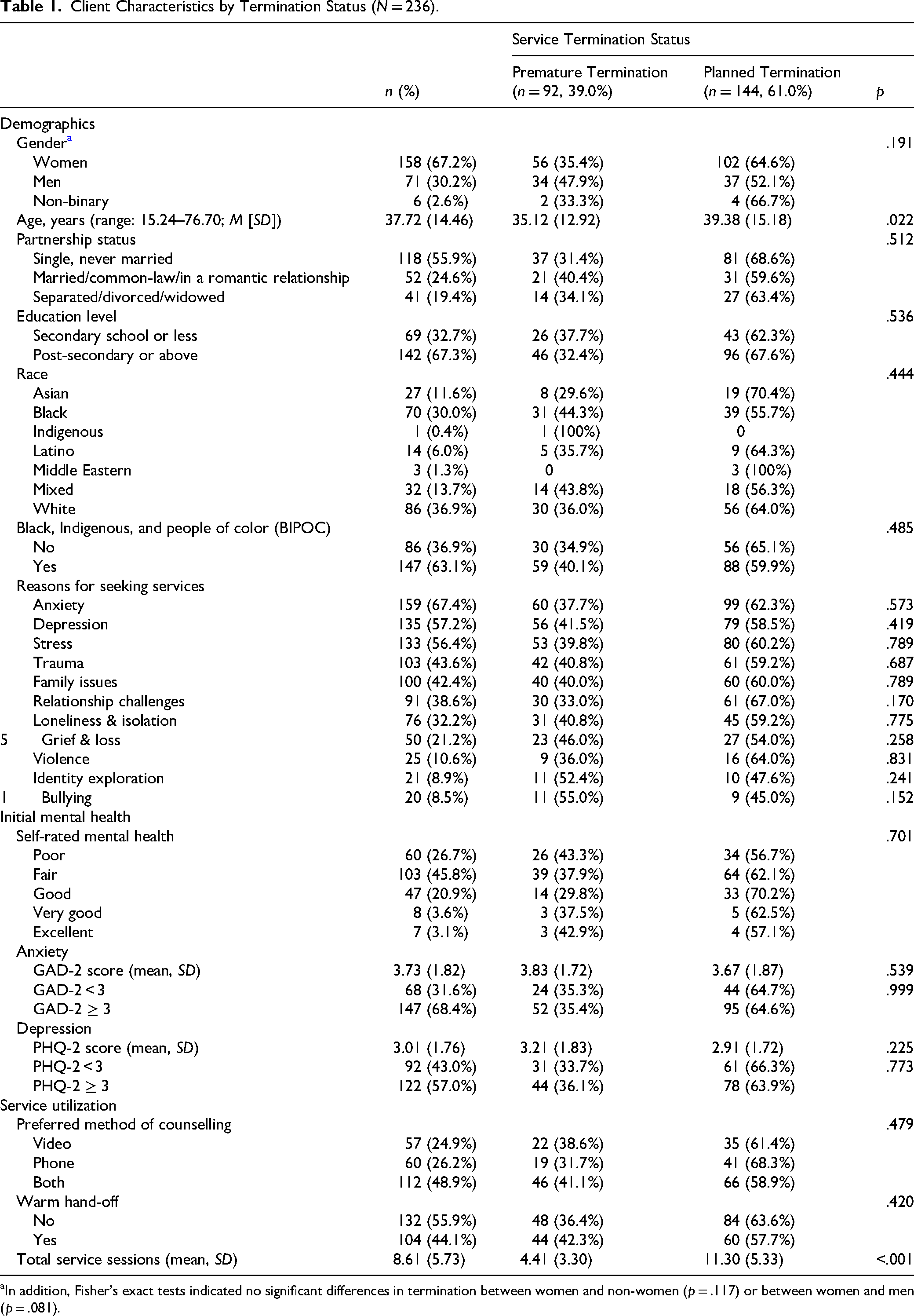
In addition, Fisher's exact tests indicated no significant differences in termination between women and non-women (p = .117) or between women and men (p = .081).
We found no significant differences in baseline demographic and mental health characteristics between clients who had a planned termination and those who terminated prematurely, except for age (p = .022). Clients who had a planned termination were older (M = 39.38, SD = 15.18) than those who terminated prematurely (M = 35.12, SD = 12.92). On average, clients with planned termination attended 11.30 sessions (SD = 5.33), compared with 4.41 sessions (SD = 3.30) among those who ended services prematurely (p < .001).
GAD-2 and PHQ-2 Scores from Baseline to Termination
We hypothesized that clients who completed services at the Clinic would demonstrate significant improvements in their anxiety and depressive symptoms from baseline to termination. Shown in Figure 1, among the 144 clients who successfully completed services, five were missing pretest scores and 17 were missing posttest scores, resulting in a sample of 122 for within-group analyses. Significant improvements were observed in GAD-2 and PHQ-2 scores in this sample. As shown in the paired t test results, clients’ mean GAD-2 score decreased from 3.57 (SD = 1.83) at baseline to 2.32 (SD = 1.84) at termination, t(121) = 7.10, p < .001, d = 0.64, 95% confidence interval (CI) [0.45, 0.83], indicating a medium-to-large effect size (Ellis, 2010). Similarly, the mean PHQ-2 score decreased from 2.84 (SD = 1.77) to 1.73 (SD = 1.42), t(121) = 5.87, p < .001, d = 0.53, 95%CI [0.34, 0.72], reflecting a medium effect size (Ellis, 2010).
McNemar's chi-square tests on dichotomized scores indicated significant reductions in the proportions of clients meeting the cutoff for both anxiety and depression. The proportion of scoring above the GAD-2 cutoff decreased from 68.0% to 36.1%, χ2(1, 122) = 29.47, p < .001, φ = 0.49, suggesting a near-large effect size (Ellis, 2010). The proportion scoring above the PHQ-2 cutoff decreased from 54.1% to 26.2%, χ2(1, 122) = 17.02, p < .001, φ = 0.37, indicating a medium-to-large effect size (Ellis, 2010).
Client Baseline Characteristics and GAD-2 and PHQ-2 Change Scores
We hypothesized that women, individuals with greater baseline symptom severity, and those who attended more sessions would demonstrate greater improvements in GAD-2 and PHQ-2 scores. In addition, we explored whether age, race, education level, and preferred counseling modality were associated with therapeutic gains. Bivariate analyses (Table 2) revealed that gender and initial self-rated mental health were the only factors significantly associated with changes in symptom scores. Gender was associated with both GAD-2 and PHQ-2 change scores. Compared with men (MΔGAD−2 = −0.58, SD = 1.93), women (MΔGAD−2 = −1.48, SD = 1.90) showed greater reduction in anxiety symptoms, t(115) = −2.24, p = .027. Similarly, women reported a larger decrease in depressive symptoms (MΔPHQ−2 = −1.43, SD = 2.14) than men (MΔPHQ−2 = −0.48, SD = 1.79), t(115) = −2.20, p = .030. Repeated measures analyses comparing scores from baseline to termination demonstrated that time-by-gender interactions were significant for both the GAD-2, F(1, 115) = 5.02, p = .027, and the PHQ-2, F(1, 115) = 4.82, p = .030. The interaction plots suggested that women have higher levels of anxiety (Figure 2) and depression (Figure 3) than men at baseline experienced greater improvement over time.
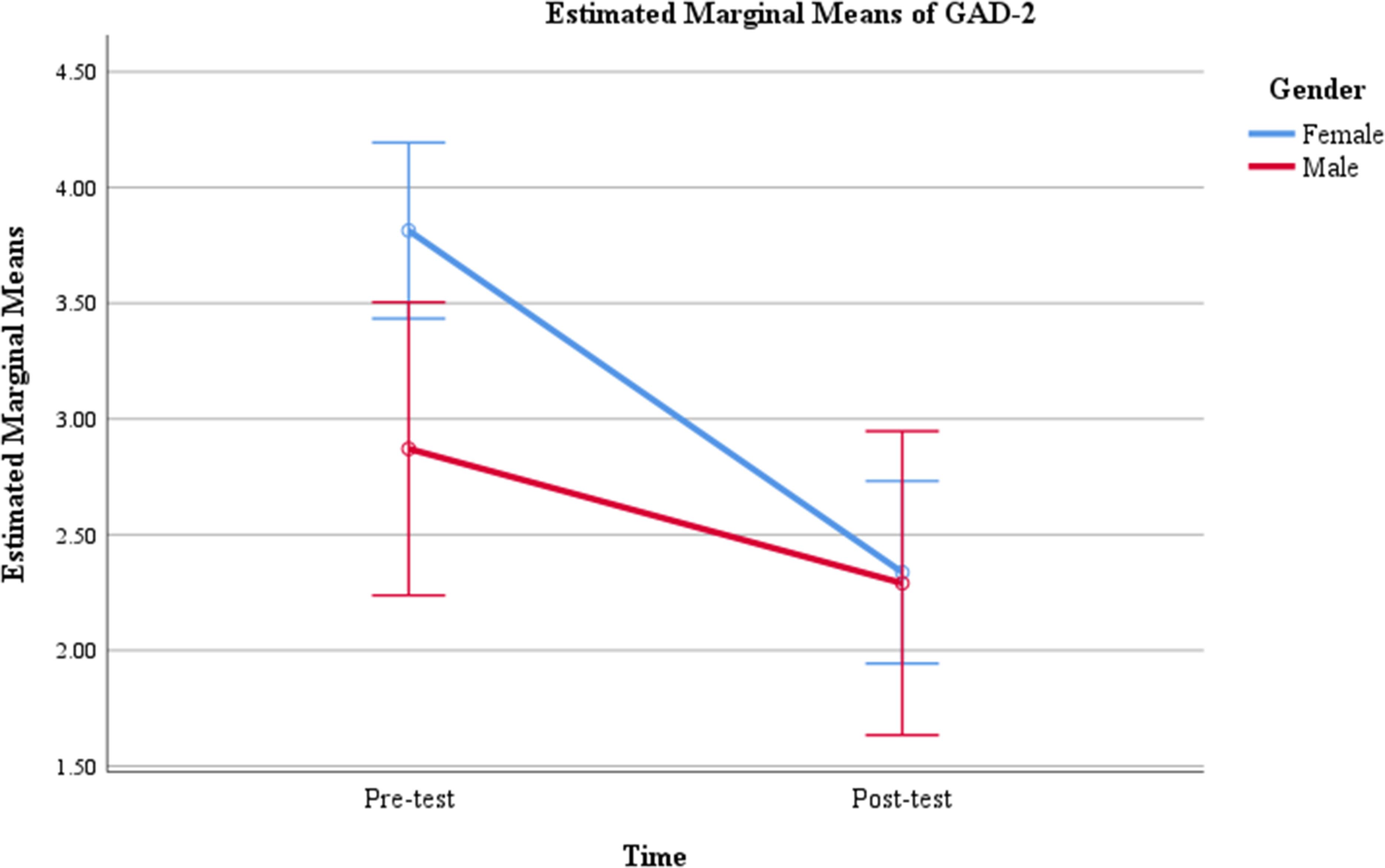
Repeated measures results of GAD-2 scores by gender (N = 117).
Bivariate Results of Client Characteristics and GAD-2 and PHQ-2 Change Scores (N = 122).
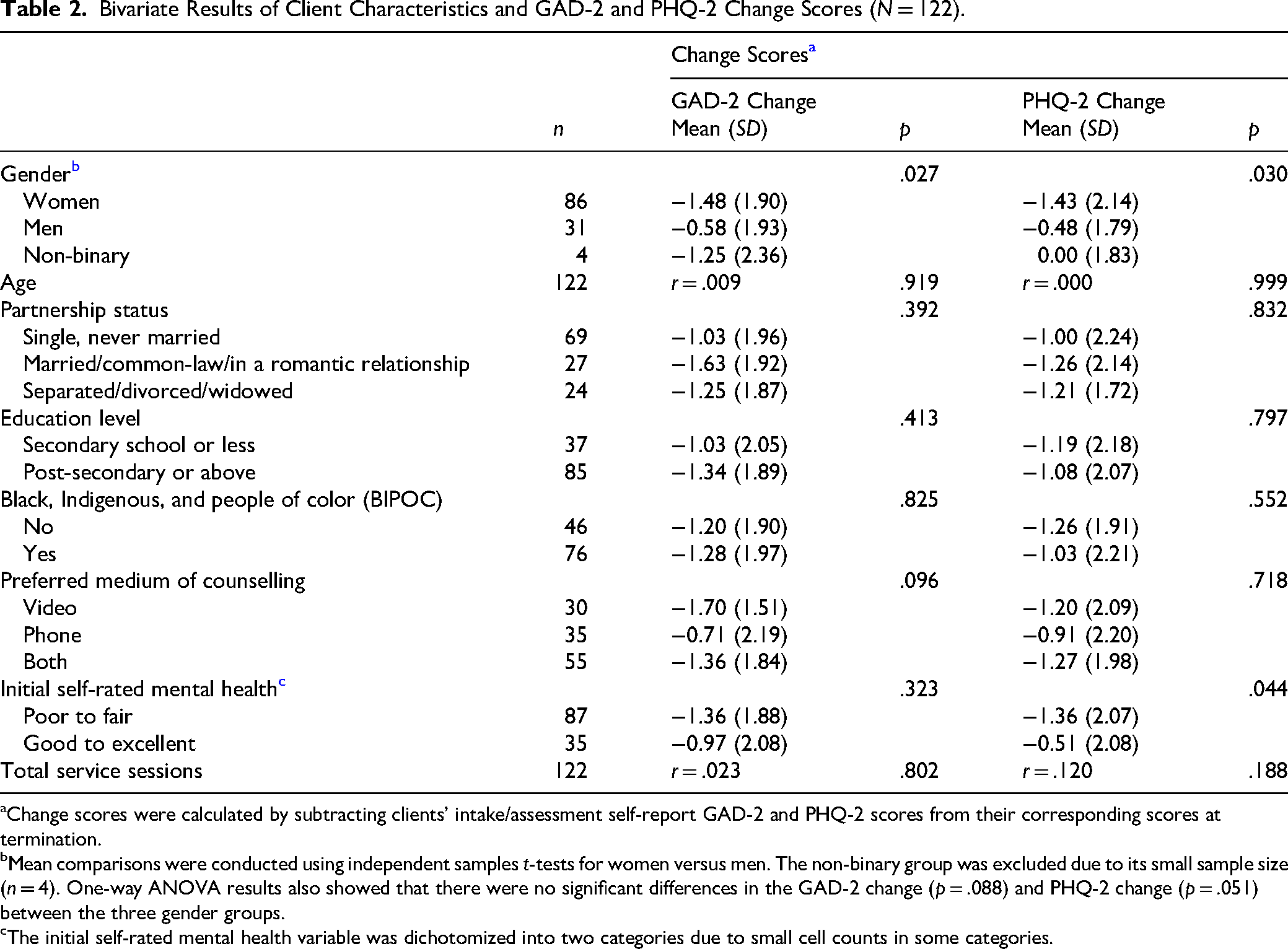
Change scores were calculated by subtracting clients’ intake/assessment self-report GAD-2 and PHQ-2 scores from their corresponding scores at termination.
Mean comparisons were conducted using independent samples t-tests for women versus men. The non-binary group was excluded due to its small sample size (n = 4). One-way ANOVA results also showed that there were no significant differences in the GAD-2 change (p = .088) and PHQ-2 change (p = .051) between the three gender groups.
The initial self-rated mental health variable was dichotomized into two categories due to small cell counts in some categories.
Client's self-reported initial mental health status was significantly associated with PHQ-2 score changes, t(120) = 2.03, p = .044. Clients who rated their mental health as poor or fair experienced more improvement (MΔPHQ−2 = −1.36, SD = 2.07) than those who rated their mental health as good to excellent (MΔPHQ−2 = −0.51, SD = 2.08). Repeated measures analysis shows that the interaction between time and self-rated mental health was significant for the PHQ-2, F(1, 120) = 4.13, p = .044. The interaction plot (Figure 4) suggested that clients who reported poor or fair mental health had higher levels of depressive symptoms at baseline and experienced greater improvement over time compared with those reporting good-to-excellent mental health.
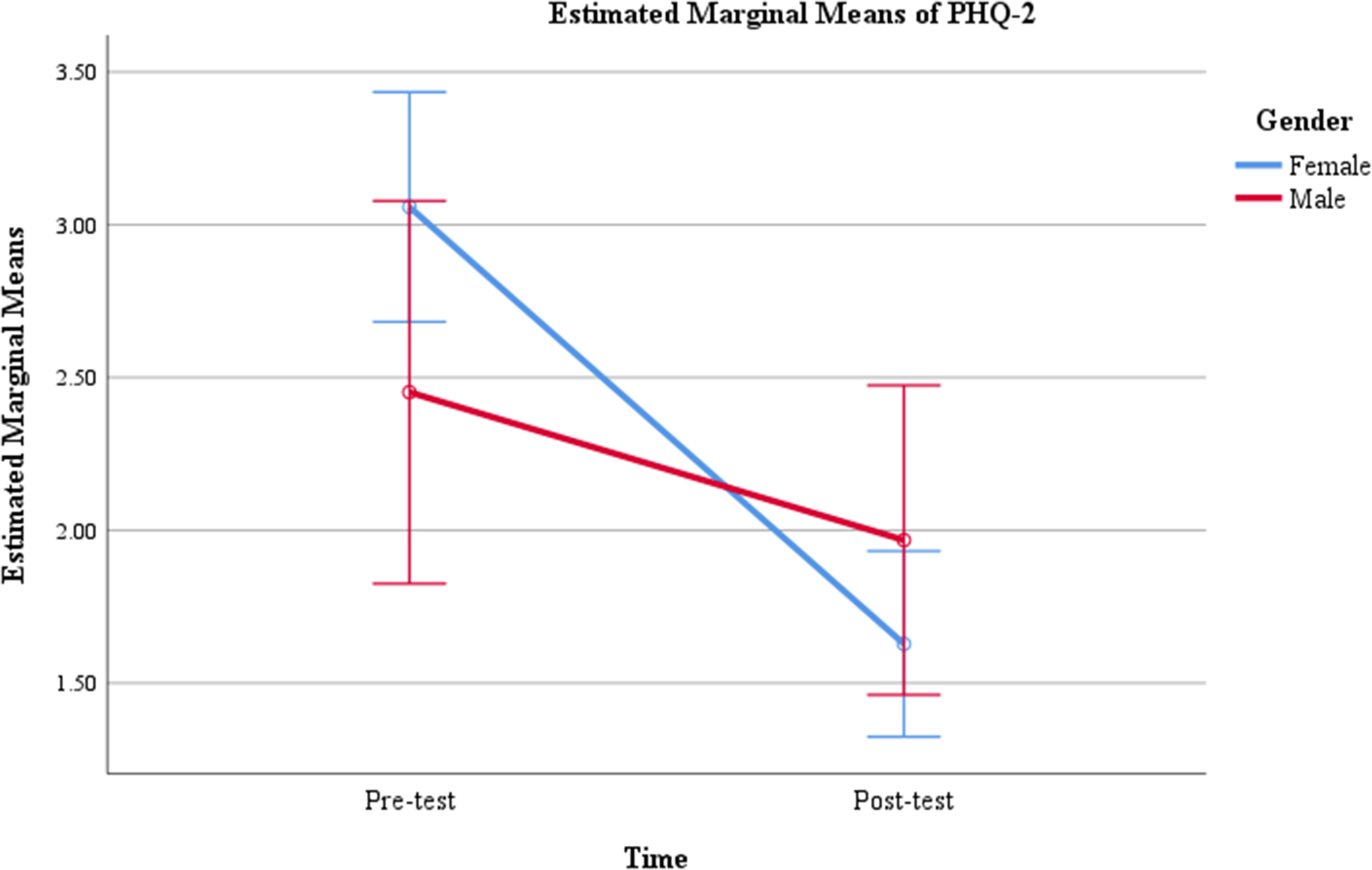
Repeated measures results of PHQ-2 scores by gender (N = 117).
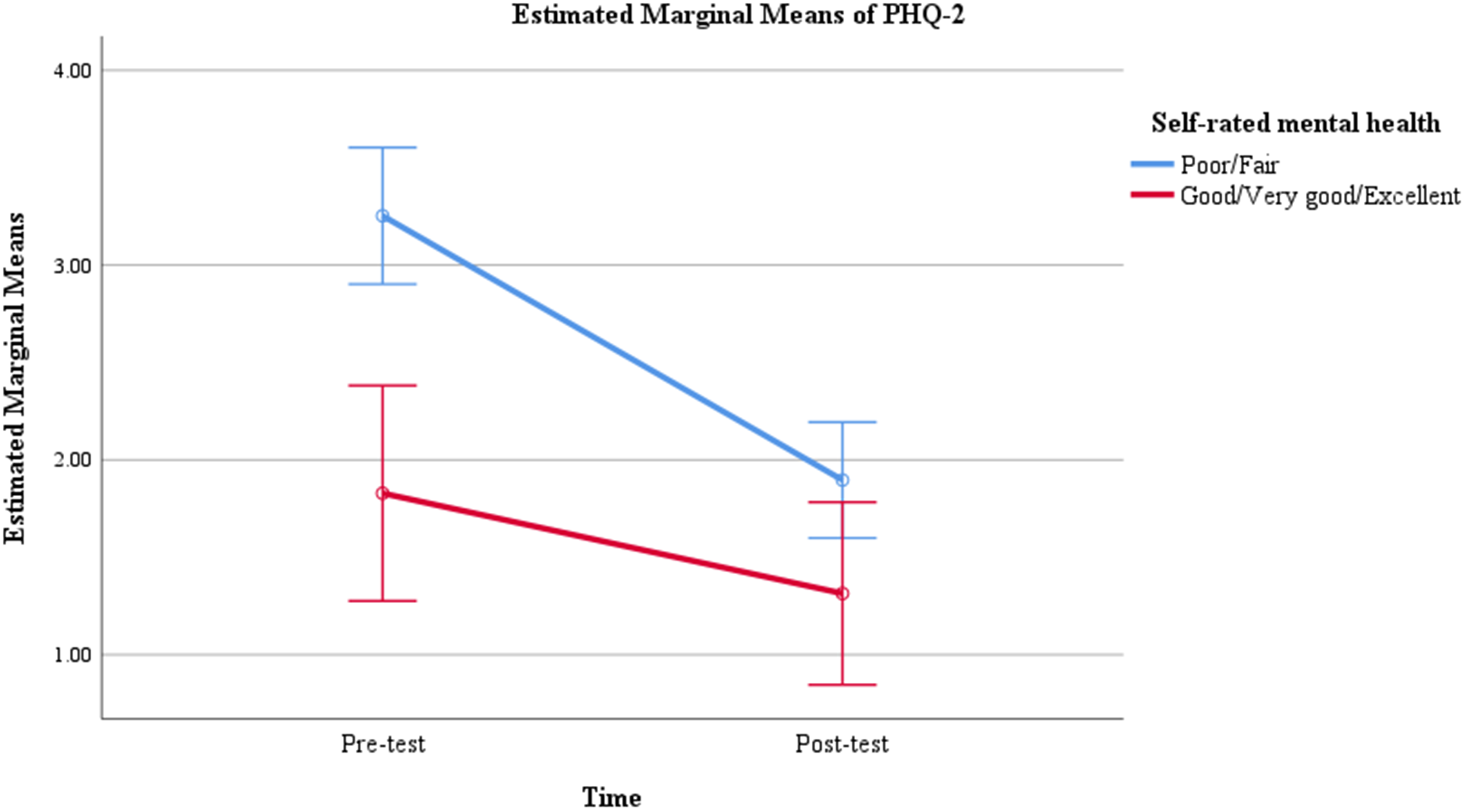
Repeated measures results of PHQ-2 scores by self-rated mental health (N = 122).
Client Experiences and Service Quality
The anonymous VCES was sent to all clients who had at least one intake assessment session after completing services and had an email address. Out of the 236 clients serviced between September 2022 and September 2025, 188 met the eligibility criteria to receive the VCES. A total of 87 clients provided a valid response, resulting in a 46.3% response rate. As presented in Table 3, most respondents were women (n = 63, 77.8%), and the largest age group was 35–44 years (n = 22, 27.5%). The majority of respondents identified as Black, Asian, Latino, or mixed race (n = 43, 53.1%), while 46.9% (n = 38) identified as White.
Demographics of VCES Respondents (N = 87).
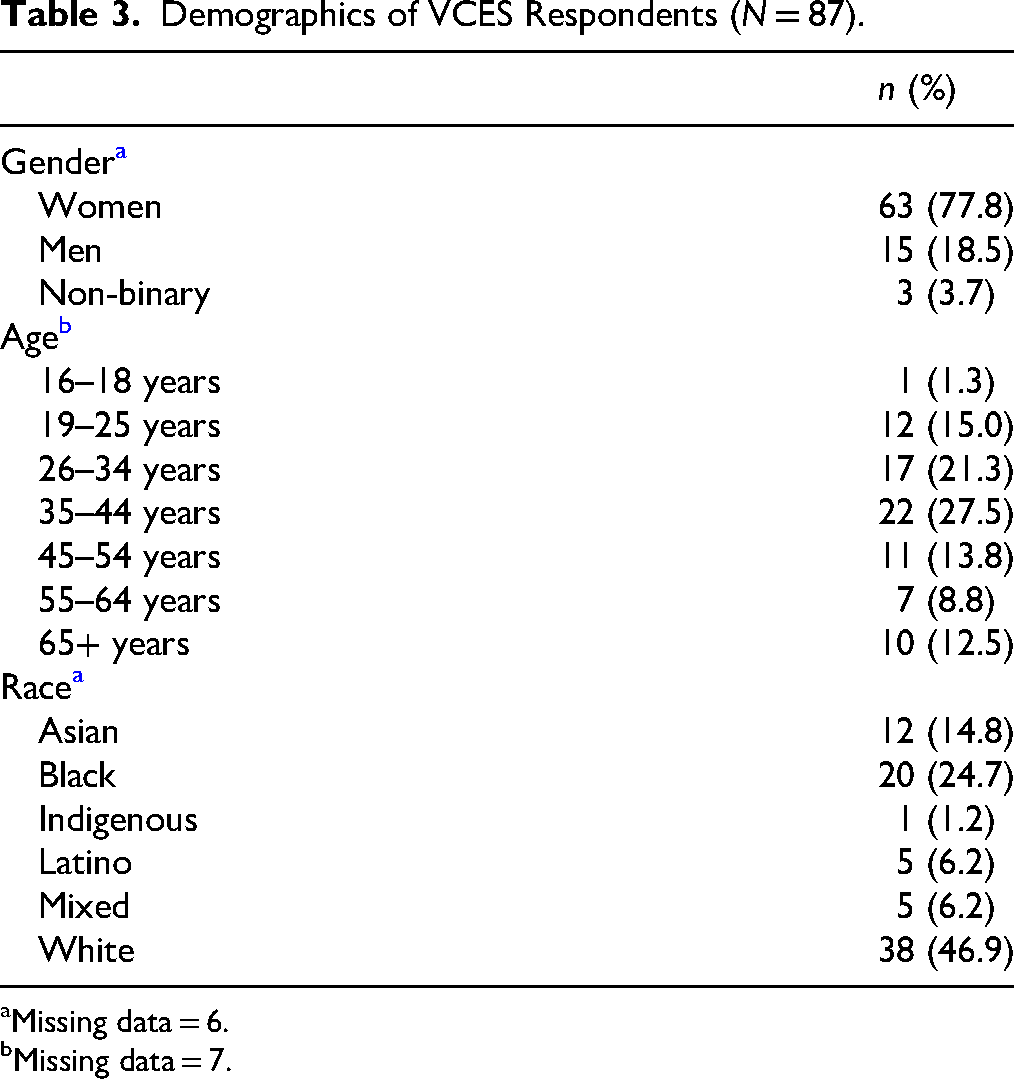
Missing data = 6.
Missing data = 7.
Responses indicated positive experiences and high quality across various service domains (Table 4).
Client Experience Results Using the VCES (N = 87).
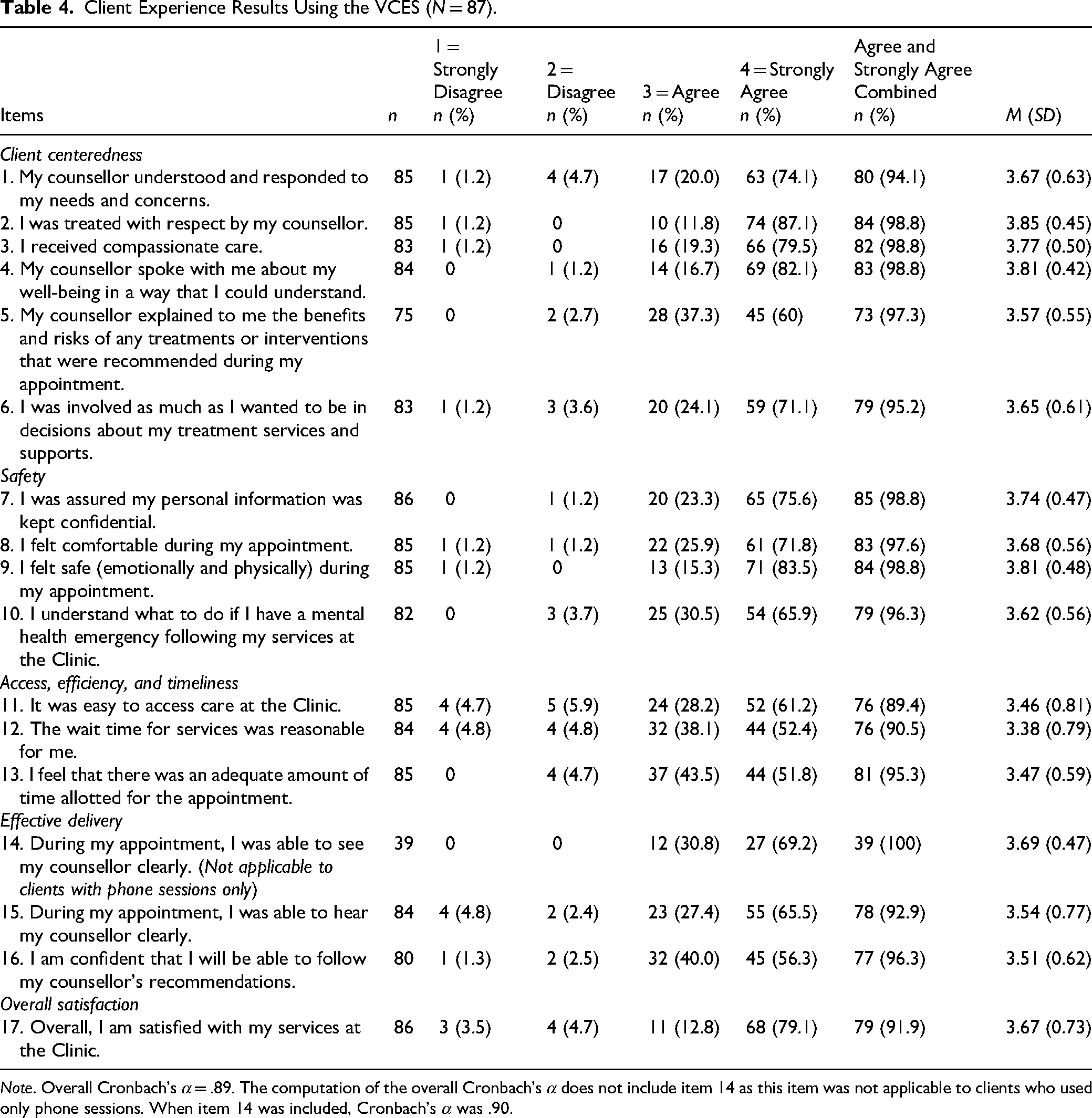
Note. Overall Cronbach's α = .89. The computation of the overall Cronbach's α does not include item 14 as this item was not applicable to clients who used only phone sessions. When item 14 was included, Cronbach's α was .90.
Client Centeredness
Almost all respondents agreed or strongly agreed that their counsellor treated them with respect (98.8%), communicated in an understandable way (98.8%), provided compassionate care (98.8%), and explained any benefits and risks (97.3%). Most clients reported that their counsellor involved them in decision-making sufficiently (95.2%) and responded to their needs (94.1%). Mean scores ranged from 3.57 (SD = 0.55) (benefits and risks explained) to 3.85 (SD = 0.45) (being treated with respect), reflecting clients’ highly positive perceptions of client-centered care.
Safety
Nearly all respondents felt that their personal information was kept confidential (98.8%), that they were safe (98.8%) and comfortable (97.6%) during services, and that they understood what to do in case of a mental health emergency (96.3%). Mean scores ranged from 3.62 (SD = 0.56) (understanding what to do in an emergency) to 3.81 (SD = 0.48) (feeling safe), reflecting clients’ highly positive perceptions of safety.
Access, Efficiency, and Timeliness
Most respondents agreed or strongly agreed that sessions were of adequate length (95.3%), that the wait time was reasonable (90.5%), and that it was easy to access care (89.4%). Mean scores ranged from 3.38 (SD = 0.79) (reasonable wait time) to 3.47 (SD = 0.59) (adequate session length), suggesting opportunities for improvement in this domain.
Effective Delivery
All (100%) respondents who attended video sessions reported being able to see their counsellor clearly, and 92.9% of respondents agreed that they could hear their counsellor clearly. Additionally, 96.3% felt confident in following their counsellor's recommendations. Mean scores ranged from 3.51 (SD = 0.62) (following recommendations) to 3.69 (SD = 0.47) (seeing clearly), reflecting clients’ appreciation for effective delivery of virtual services.
Overall Satisfaction
Overall, 91.9% of respondents agreed or strongly agreed that they were satisfied with their services at the Clinic (M = 3.67, SD = 0.73).
Client Experience and Demographic Characteristics
We examined whether clients’ experiences differed by demographic characteristics, including age, gender, and race. No significant differences were found.
Discussion and Applications to Practice
Monitoring client progress and using their feedback to improve service outcomes is widely recognized as important but rarely implemented in practice (Jensen-Doss et al., 2018), despite being central to services operating within trauma-informed and anti-racist frameworks. This evaluation study contributes empirical evidence on client mental health outcomes and care experiences within a social work student-led clinic grounded in these principles. As a clinic that delivers services exclusively via telemental health, and works with a large proportion of BIPOC clients, these findings extend the existing literature by contributing evidence from more diverse and underrepresented client populations.
Over a 3-year period, findings suggest that the majority of our clients screened positive on the GAD-2 and PHQ-2 scores at intake and completed counseling services as planned. Moreover, those who completed the services showed significant improvement from baseline to termination, along with positive client experiences of care among a largely racialized client population. The study results contribute to the emerging literature on client outcomes from student-led health services (Broman et al., 2022) and virtual counseling services (Novella et al., 2022), with particular relevance to the field of social work.
Client retention is a key element for treatment effectiveness and quality care. In the present study, 61.0% of clients had a planned termination and 39.0% terminated prematurely. Reviews on termination in psychotherapy shows that 12–53% of the terminations are due to goal achievement (Rabinowitz et al., 2025), and premature termination rates typically range from 20% to 50% (McGovern et al., 2024; Swift & Greenberg, 2012; Wierzbicki & Pekarik, 1993). Although literature on community-serving student-led clinics is limited and tends to emphasize engagement and attendance rather than comparable post-intake dropout rates (Elizabeth et al., 2022; Powell et al., 2022), available evidence suggests that our premature termination rate compares favorably with rates reported in university psychology training clinics, estimated at 60–69.9% (Al-Jabari et al., 2019; Callahan et al., 2014; Cukrowicz et al., 2011). Clients at the Clinic who terminated the services prematurely tended to be younger, a finding consistent with literature (Bowker et al., 2025), although the difference in age was modest (35.12 vs. 39.38 years). The primary reasons for premature termination were inability to contact and client-initiated termination. While some of the clients served at the Clinic have no fixed address and the transient nature of their lives may contribute to the premature termination, it is important for the Clinic to continue working with our partners, monitoring client progress, identifying client barriers to service engagement (Hanevik et al., 2023), and implementing targeted strategies to enhance client hope and motivations (Bowker et al., 2025).
In addition, a meta-analysis found that client dropout rates are significantly higher among trainees than among experienced clinicians, suggesting that therapists may become more skilled at engaging clients and improving outcomes as their move beyond basic training (Swift & Greenberg, 2012). As such, the Clinic should continue to enhance its in-service training and support for student therapists’ professional development, which may in turn improve client engagement and retention beyond the initial sessions. One area for student therapists’ growth is role induction, which refers to the process of orienting clients to psychotherapy by providing education and expectations about the therapeutic relationship (Swift et al., 2023). Role induction has been shown to improve client engagement following assessment (Swift et al., 2023). However, student therapists often appear hesitant to offer such orientation, as they are new to delivering psychotherapy and may feel uncertain about the direction of services. To enhance client engagement and reduce early dropout, strengthening training and supervisory guidance around role induction may help student therapists communicate the purpose and process of therapy, clarify the respective roles of therapists and clients, and more confidently address client ambivalence (Lawrence et al., 2017; Swift et al., 2023).
Among clients who had a planned termination, we observed a medium-to-large (d = 0.53–0.64) significant and meaningful reduction in anxiety and depression symptoms, as reflected in improvements in GAD-2 and PHQ-2 scores. These results are comparable to those reported in the small number of published studies examining psychotherapy delivered in student-staffed clinics within community routine-care settings (Moncrief-Stuart et al., 2024; Roseborough et al., 2023). Moreover, studies have suggested that brief telemental health treatments in routine care by professionals typically produce moderate-to-large within group effect sizes (d = 0.50–0.90) (Fernandez et al., 2021; Forand et al., 2025; Kenwright et al., 2025). The magnitude of improvement observed in the present study falls within this range, although toward the lower end, suggesting that clients receiving services at the Clinic experienced levels of symptom reduction broadly comparable to those reported in studies of professionally delivered telemental health interventions. Given that services at the Clinic are delivered by student clinicians within a training context, these findings are notable and suggest that meaningful improvements in mental health symptoms can be achieved within supervised student-led clinical settings. The somewhat smaller effect sizes may reflect differences in clinical experience, the routine practice setting, or the use of brief measures such as the GAD-2 and PHQ-2, which are designed to detect symptom change but provide less detailed assessment than longer instruments.
We further analyzed demographic and clinical characteristics that may help explain these clinical outcomes. Our analysis shows that only gender and self-rated mental health at baseline were associated with changes in symptom scores. Interaction analyses suggest that these improvements were more pronounced among women (for both GAD-2 and PHQ-2 outcomes) and among clients who self-rated their mental health as poor to fair at baseline (for PHQ-2 only). A close examination of the interaction plots suggests that these groups had greater symptom severity at baseline. These results are consistent with findings from meta-analyses showing that greater baseline symptom severity is associated with stronger improvement following psychotherapy (Andersson et al., 2019; Scholten et al., 2023), and suggest that services provided at the Clinic may particularly benefit clients with higher symptom severity and poorer self-rated mental health at baseline. From a practice perspective, these results underscore the importance of systematic and measurement-based assessment to identify clients who may benefit most from brief therapeutic interventions. These findings also provide preliminary evidence that supervised trainee-delivered services can produce meaningful improvement among clients presenting with elevated distress.
Notably, although prior studies have found that a greater number of sessions is associated with symptom improvement in student-led services (Powell et al., 2022), we did not observe this association in our study. Structural differences between student-led clinics may affect both the number of sessions delivered and the pattern of symptom change over time. For example, clinical services provided in Powell et al. (2022) included assessment, pharmacological, supportive counseling, and individual psychotherapy, whereas the Clinic focuses on assessment and brief psychotherapy only. Moreover, in the context of a student-led clinic, the brief and goal-oriented nature of services may allow clients experience meaningful improvement within a limited number of sessions (Żak & Pękala, 2025).
Given that the Clinic serves a large number of BIPOC clients, it is important to note that we also did not find a significant relationship between race and outcome improvements. While racial disparities in mental health outcomes continue to exist (Eack & Newhill, 2012; Olfson et al., 2023), the absence of differences in the present study may suggest that the Clinic's trauma-informed and anti-racist practice approach has potential to support equitable outcomes across client groups. Future research should further examine how service models guided by these orientations influence outcomes across diverse populations.
Continued monitoring of client feedback related to services is essential to guide service improvements and enhance overall quality. This study used a validated tool for virtual practice, the VCES, to assess client experiences with the Clinic's services. To capture a broad range of client perspectives, the survey was distributed to both clients who completed services as planned and those who terminated services prematurely. However, survey respondents differed somewhat from the broader clinic population with respect to gender and race, suggesting non-response bias. Specifically, VCES respondents included a higher proportion of women (77.8% vs. 67.2%) and a lower proportion of BIPOC clients (53.1% vs. 63.1%). These differences highlight the importance of considering strategies, such as offering multiple modes of survey completion, reinforcing the purpose and anonymity of client feedback, and ensuring that feedback processes are accessible and culturally responsive (Anhang Price et al., 2022; Keusch, 2015).
Results indicate that over 90% of respondents agreed that the Clinic performed well across the domains of client-centeredness, safety, efficiency, timeliness, and effective service delivery. These findings are encouraging as client-centeredness (including respect and collaboration) and safety are pivotal to trauma-informed practice (Levenson, 2020), which guides the Clinic's approach. Access was the only area with agreement below 90%, with 10.6% of respondents indicating that it was not easy to access care at the Clinic. Further analyses indicated no significant associations between gender, race, or age and agreement with this and other items. Although virtual counselling services are often promoted for their accessibility (Lattie et al., 2022), student-led clinics face unique structural constraints. In our Clinic, service availability is limited by student practicum schedules (i.e., 3 days a week), which may restrict access for some clients. The Clinic has been transparent about these scheduling limitations with community partners and clients from the outset. To further improve access, future strategies may include strengthening referral pathways for clients requiring more immediate or ongoing support and enhancing the continuum of care by more actively engaging referral partners to support clients’ needs.
Several limitations warrant consideration when interpreting the study findings. First, the evaluation employed a pre-post design without a control group due to the naturalistic service setting. The absence of random assignment poses threats to internal validity and limits causal inferences, as the design cannot control for passage of time, maturation, placebo effects, and desire to please the therapist. Second, although the study included clients seen at the Clinic over a 3-year period, the overall sample size remained relatively small, which limited statistical power and precluded more detailed subgroup analyses. Third, the representativeness of the sample may be limited. Clients were referred to the Clinic through community partners, which may introduce selection bias and limit the generalizability of the findings. Generalizability may also be constrained by the specific context of the Clinic, which operates as a student-led service in a metropolitan area in Canada with a unique partnership model. Fourth, therapist effects should be acknowledged. Services were delivered by students whose placements lasted from one to two academic semesters, and their levels of clinical experience and skills varied. Students were encouraged to integrate therapeutic approaches based on comprehensive case assessments and formulations. As well, because the specific treatment modality used for each client was not recorded, it was not possible to examine associations between treatment modalities and client outcomes. Fifth, the study lacked follow-up data. Without longer-term follow-up, it is unclear whether the observed improvements could sustain over time. Sixth, measurement limitations should be considered. Given the burdens on clients of administering longer measures in a routine, virtual practice, particularly among individuals experiencing structural inequalities, we opted to use brief tools such as GAD-2 and PHQ-2 to reduce client burden and improve accessibility. Although prior research indicates that the GAD-2 and PHQ-2 demonstrate sensitivity comparable to the GAD-7 and PHQ-9, respectively (Staples et al., 2019), the limited scoring range of these brief measures may reduce variability and constrain the detection of outcome differences compared with longer assessments. Lastly, the anonymous VCES was distributed only to clients with a valid email address, which may have limited access for some individuals. The Clinic has since implemented a procedure whereby administrative staff not directly involved in client care contact clients without email access by phone to complete the survey.
Despite its limitations and preliminary nature, this evaluation study provides valuable evidence on client outcomes and experiences within a unique social work student-led clinic that serves a high number of racialized clients. By integrating analyses of symptom change, predictors of improvement, and client experiences of care, the study contributes to the limited literature on social work student-led clinics and provides support for the effectiveness and acceptability of student-led and virtual service models. While the student-led model may facilitate trauma-informed and anti-oppressive practices through its emphasis on supervision and relational care, further research is needed to examine this relationship directly. As well, given the role of client-therapist matching in therapeutic engagement and outcomes (Ilagan & Heatherington, 2022; Kim & Kang, 2018), future research should incorporate clinician demographic and training variables to better examine their influence. Ongoing evaluation efforts will strengthen student training and supervision, inform organizational infrastructure and support, and in turn, enhance service quality and effectiveness, ultimately benefiting the communities served.
Footnotes
Acknowledgments
The authors would like to thank Yu Lung, Nelson Pang, Angela Lee, and Zihui (Cynthia) Ni for their contributions to the maintenance of the Clinic's database.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Talk It Out Counseling Clinic is supported by donors and sponsors whose contributions to the Factor-Inwentash Faculty of Social Work, University of Toronto, make its operations possible. This research was supported by the Bertha Rosenstadt Trust Fund in Health Research, Factor-Inwentash Faculty of Social Work, University of Toronto (grant number N/A).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.